Back to Journals » Journal of Pain Research » Volume 15
Percutaneous Release of the First Extensor Tendon Compartment in De Quervain’s Disease by Acupotomy with US-Guidance: A Cadaveric Study
Authors Shen Y ![]() , Zhou Q
, Zhou Q ![]() , Sun X
, Sun X ![]() , Li S, Zhang W
, Li S, Zhang W ![]()
Received 27 May 2022
Accepted for publication 6 October 2022
Published 22 December 2022 Volume 2022:15 Pages 3995—4005
DOI https://doi.org/10.2147/JPR.S375309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Yifeng Shen,1,2 Qiaoyin Zhou,1,3 Xiaojie Sun,4 Shiliang Li,1,3,4 Weiguang Zhang5
1College of Traditional Chinese Medicine, Fujian University of Traditional Chinese Medicine, Fuzhou, People’s Republic of China; 2Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 3Key Laboratory of Orthopedics & Traumatology of Traditional Chinese Medicine and Rehabilitation (Fujian University of TCM), Ministry of Education, Fuzhou, People’s Republic of China; 4Department of Acupuncture and Moxibustion, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 5Health Science Center, Peking University, Beijing, People’s Republic of China
Correspondence: Shiliang Li, Department of Acupuncture and Moxibustion, China-Japan Friendship Hospital, Beijing, People’s Republic of China, Email [email protected] Weiguang Zhang, Health Science Center, Peking University, Beijing, People’s Republic of China, Email [email protected]
Background: De Quervain’s disease is a painful stenosing tenosynovitis of the first dorsal compartment of the hand affecting the tendons of the abductor pollicis longus and extensor pollicis brevis. This study aimed to evaluate the safety and efficacy of percutaneous first extensor compartment releases performed on embalmed cadaveric models by acupotomy operation with or without US guidance.
Methods: Percutaneous release was performed with an acupotomy on 59 wrists of cadavers; 23 wrists were operated with US guidance, and 39 wrists were operated without US guidance. Each arm was dissected and assessed regarding the amount of release as well as the extent of neurovascular and tendon injury. Anatomical structures were also observed in this study.
Results: Twenty cases (87%) were successfully released with ultrasound-assisted techniques, and 27 cases (75%) were successfully released with blind techniques. No neurovascular injury occurred in any arm, regardless of technique. No significant tendon injury was seen in any arm. Although minor surface scratches were visualized in 11 cases, they occurred in 3 cases (13.04%) with ultrasound assistance and in 8 cases (22.22%) with blind techniques. There was no statistically significant difference between the two groups in the measurement of the distance from the incision marks to the blood vessels and nerves. A fibrous septum and bony protrusions were found in the first dorsal compartment, which may be anatomical factors affecting the success of treatment.
Conclusion: Both traditional and US-guided percutaneous release by acupotomy of the first extensor tendon compartment can be performed for all wrists. US-guided techniques can improve the success rate and reduce damage during acupotomy operations.
Keywords: de Quervain’s disease, tendonitis, acupotomy, acupuncture, ultrasound guidance, anatomy
Introduction
Stenosing tenosynovitis of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) in the first extensor compartment of the wrist, also known as de Quervain’s disease (dQD), is a common disorder. Its treatments include local steroid injection, open, and endoscopic surgery.1 By histopathology, de Quervain’s disease is not characterized by inflammation but by thickening of the tendon sheath and most notably by the accumulation of mucopolysaccharide, an indicator of myxoid degeneration.2 These changes should be pathognomonic of dQD. It has been suggested that dQD is likely to be a result of intrinsic degenerative mechanisms rather than extrinsic inflammatory ones. The primary pathogenic structure in radial stenosing tenosynovitis is the bony fibrous canal on the lateral aspect of the radial styloid process. The development of stenosing tenosynovitis is closely related to the local anatomic features, and the pathogenesis of the disease is more closely related to the physical entrapment produced by its local anatomic structures, including the condition of the tendon, the presence or absence of a septum, and the presence of a bony ridge at the base of the first carpal compartment that can affect tendon gliding and produce inflammation. These anatomical structures increase the friction between tendons and between tendons and bony channels. Short-term friction or minor injuries can be recovered by local tissue interstitial lubricating fluid and self-repair, while prolonged and repeated mechanical friction will produce chronic sterile inflammatory edema and congestion between tendons and tendon sheaths, and inflammatory exudation will lead to local fibrosis, which will aggravate the stenosis symptoms.3
Some studies have reported that needle tip percutaneous tenotomy can be performed effectively and safely in de Quervain’s disease.4,5 Acupotomy applies a miniature surgery instrument consisting of a handle, needle body and blade (Figure 1). Acupotomy has been widely used clinically by doctors of traditional Chinese medicine and in orthopedics and pain departments in China,6 and the use of acupotomy for percutaneous release has become a routine procedure in dQD that can effectively avoid the creation of unsightly scars caused by open surgery.7 However, the traditional acupotomy operation is carried out without ultrasonography (US) guidance as a blind technique, so the operator needs to have high anatomical knowledge, and there might be some operational risks.8 This study evaluated the safety and accuracy of ultrasound-guided and nonultrasound acupotomy in the treatment of dQD and proposed an anatomical reference.
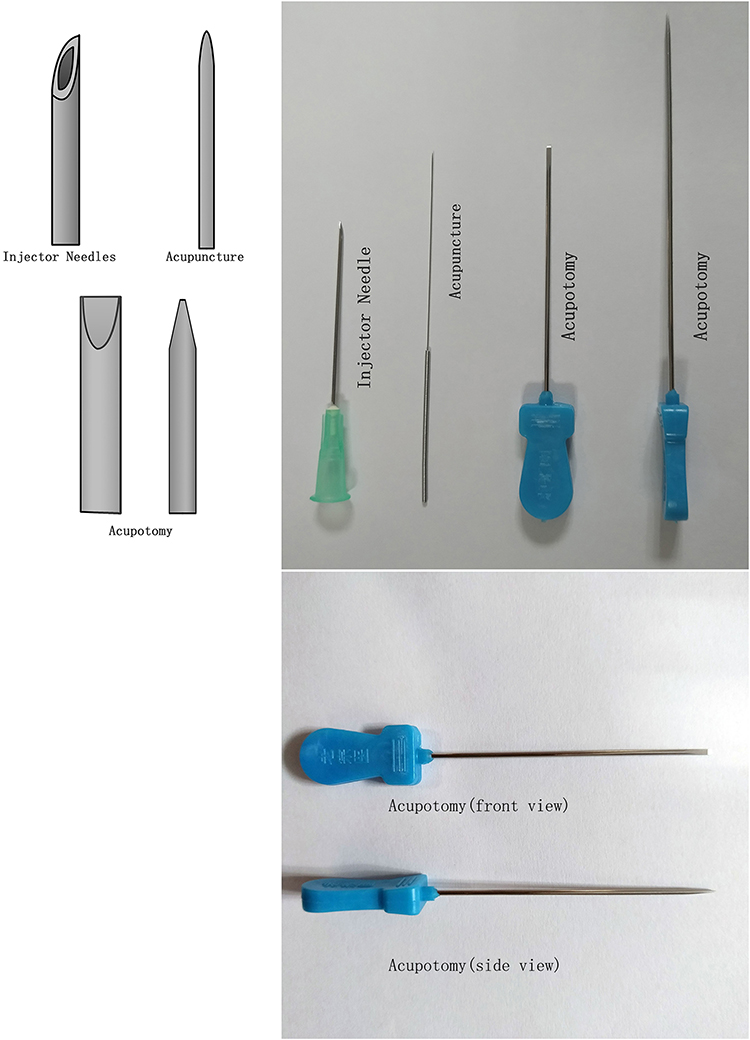 |
Figure 1 Schematic diagram of the acupotomy. |
Materials and Methods
Fifty-nine embalmed cadaver arms were selected. They had not been dissected and had no major wrist or hand injuries. This study was approved by the Ethics Committee of Peking University School of Medicine for human research (FITCM IACUC 2021077). According to whether the water content of the specimens could be displayed by ultrasound images, the specimens were divided into 23 cases in the ultrasound group (U Group) and 36 cases in the blind group (B Group). A 1.00 mm-acupotomy 50.00 mm in length was used. The experiment was completed by two trained operators: one doctor (Shen Yifeng) was responsible for the operation of the ultrasound and needle knife, and the other doctor (Zhou Qiaoyin) was responsible for the dissection and measurement.
The forearm specimen was placed in a neutral position, and the wrist was kept ulnar to facilitate needle insertion. The high-frequency ultrasound probe was placed on the surface of the radial styloid process, and the first compartment of the wrist was identified by transverse scanning. The operation procedure is as follows: the needle is inserted in the plane, the needle body and the skin are at an angle of 15°, and the knife surface is perpendicular to the skin. The ultrasound image shows that when the needle knife penetrates the skin and reaches the surface of the tendon sheath, it is pushed and released once, and it can be clearly felt during the pushing and cutting process. There is a feeling that the tough tissue is cut under the needle knife, and the needle is retained (Figure 2A).
 |
Figure 2 (A) Ultrasound-guided acupotomy manipulation of a forearm specimen; (B) Blind acupotomy manipulation on a forearm specimen. |
The blind operation group also used the same method to insert the needle without ultrasound assistance. First, the highest point of the radial styloid process was touched by hand for anatomical positioning, and the needle insertion point was located at the distal end of the radial styloid process. It is located between the two bony ridges of the radial styloid process and is flush with the proximal transverse crease of the wrist. The other operations were the same as those in the ultrasound group (Figure 2B).
A magnifying glass was used to observe the superficial branch of the radial nerve, radial artery, and tendon for cuts and injuries. Tendon injuries were assessed using the following methods: tendon injury (none; minor injury: superficial minor injury or injured tendon thickness <10%; severe injury: tendon rupture or injured tendon thickness >10%). The following distances were measured using an electronic Vernier caliper: the shortest lateral distance (L1) of the incision from the radial branch of the superficial branch of the radial nerve. The shortest lateral distance (L2) of the incision from the ulnar branch of the superficial radial nerve. The shortest longitudinal distance from the incision to the bifurcation of the superficial branch of the radial nerve (L3). The shortest lateral distance from the incision to the radial artery (L4) and the shortest longitudinal distance from the incision to the radial artery snuff fossa (L5). We observed whether the position of the acupotomy incision was located on the surface of the first sheathing canal at the radial styloid process or deviated from the target release area. The length of the acupotomy incision (L6) was measured, and the full release and partial release and the number of unreleased cases were recorded. Anatomical structures for manipulation are also observed and measured. The incision approach, length and morphological classification of the bony and fibrous canal of the first carpal compartment, fibrous septum and bony protrusions in the radial styloid groove were observed in this study (Figure 3).
 |
Figure 3 Schematic diagram of the release traces and anatomical structure of the radial styloid process with acupotomy 1 (red line) needle-knife release trace (L6); 2 superficial branch of the radial nerve; 3 radial artery; 4 radial artery snuff fossa; 5 extensor pollicis brevis; 6 abductor pollicis longus; 7 radial wrist retina; L1, the shortest lateral distance of the incision from the radial branch of the superficial branch of the radial nerve. L2, the shortest lateral distance of the incision from the ulnar branch of the superficial radial nerve. L3, the shortest longitudinal distance from the incision to the bifurcation of the superficial branch of the radial nerve. L4, the shortest lateral distance of the incision from the radial artery. L5, the shortest longitudinal distance of the incision from the radial artery snuff fossa segment. |
All data were analyzed by SPSS 20.0 statistical software. The count data such as success rate and injury rate were expressed as percentages (%). Chi-square test was used for comparison between groups, and P < 0.05 was considered statistically significant. Anatomical data and other measurement data were expressed as mean ± standard deviation (x ± s), independent samples t-test was used for comparison between groups, and P < 0.05 was considered statistically significant.
Results
Ultrasound Images
After placing the ultrasound probe on the radial styloid process with one end of the probe approximately flush with the proximal wrist crease (Figure 4A), on the ultrasound images, the tendon fiber bundles were continuous cord-like hyperechoic layers, the synovial layer of the tendon sheath adjacent to the tendon was cleft-like hypoechoic, and the densely structured tendon sheath fiber layer was hyperechoic on the outside. The needle knife showed a high signal, and the puncture and cutting process at the radial styloid process could be clearly visualized in real time in the longitudinal scanning plane. The radial styloid process bone ridge and the radial bone surface showed high-brightness signals and left sound shadows below. Fat and superficial fascia showed a strong echo reflex (Figure 4B).
 |
Figure 4 (A) Scanning plane schematic diagram of ultrasound-guided acupuncture treatment of dQD; (B) Ultrasound image of longitudinal section scanning of dQD treated with acupotomy under ultrasound guidance. Abbreviations: EPB, extensor pollicis brevis; APL, abductor pollicis longus; Triangle, acupotomy. |
Success Rate and Injury Rate
As shown in Table 1, the complete release rates were similar to those of ultrasound-guided and blind-sighted procedures, but the missed rate of ultrasound operation was only half that of the blind operation (3 of 23 [13.04%] in the U group versus 9 of 36 [25%] in the B group). Dissection revealed no nerve or vascular injury to the manipulation in either the ultrasound operation or the blinded operation. No flexor tendon laceration or severe injury of suspected clinical importance was seen in the tendon, although minor surface scratches were visualized in 11 cases (18.64%), including 3 cases (13.04%) in the US-guided acupotomy operation and 8 cases (22.22%) in the blind acupotomy operation (Figure 5A). The distances from the nerves and blood vessels between the two operations are shown in Figure 5, and the difference was not statistically significant (P > 0.05) (Figure 5B, Table 2).
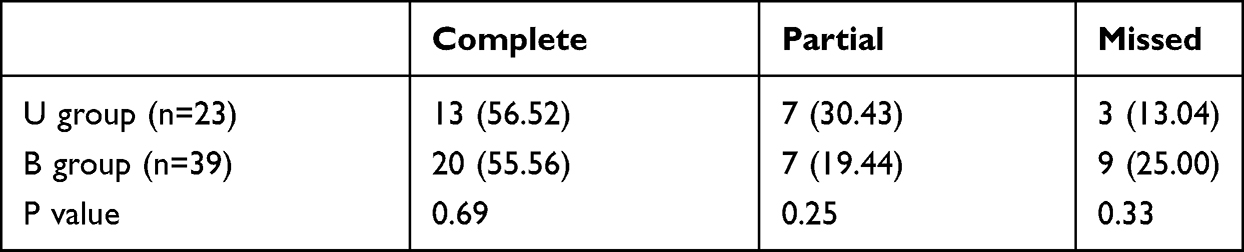 |
Table 1 Success of Percutaneous Release of the First Extensor Tendon Compartment by Method (n, %) |
 |
Table 2 The Distance from the Needle Knife Incision to Blood Vessels and Nerves and the Length of the Incision (mm) |
 |
Figure 5 (A) Success rate and injury rate; (B) Distance of the incision from nerves and blood vessels. |
Anatomical Findings
The acupotomy approach was from the skin to the superficial fascia to the tendon sheath. After puncturing the skin, it penetrates the subcutaneous fat and superficial fascia and reaches the surface of the first extensor tendon compartment of the wrist. The surface of the tendon sheath is pushed and sloped using the vertical blade surface without going deep into the first extensor tendon compartment of the wrist or piercing the inside tendon (Figure 6).
 |
Figure 6 Acupotomy release on the surface of the first extensor tendon compartment of the wrist. |
The length of the bone fibrous sheath in the first extensor tendon compartment of the wrist was 23.23 ± 3.01 mm, and the length of the volar bone crest of the radial styloid process was 9.65 ± 1.67 mm (6.23~15.70 mm). According to the distance between the fibrous sheath in the radial styloid process and the distal wrist rasceta, it can be separated into 3 types: Type I: The fibrous canal extends to the distal wrist crease in 35.59% (21/59). Type II: The fibrous canal extends to the distal wrist crease and radial styloid process, 47.46% (28/59). Type III: Vascular extension to the radial styloid process 16.95% (10/59) (Figure 7).
 |
Figure 7 Three types of fiber tube extensions a, Distal wrist rasceta. b, radial styloid process. |
A total of 32.20% (19/59) of the first extensor tendon compartment had a fibrous septum, 6 cases had a complete fibrous septum length with extension of the entire tendon, and 13 cases had an incomplete fibrous septum with a length of 6.78 ± 2.91 mm (2.45–10.88 mm). It was observed that 18 of the 59 upper limb specimens had bony protrusions in the radial styloid groove, and the rate of bony protrusions was 30.51% (Figure 8). Fifteen specimens had a bone crest, of which 12 specimens had a bone crest with fibrous septa, 3 specimens had a bone crest but no fibrous septum, and 6 specimens had no bone crest but a fibrous septum. There were obvious differences between the bony protrusions in the radial styloid groove and the flat radial styloid groove (Figure 9).
 |
Figure 8 First extensor tendon compartment with a fibrous septum. *Fibrous septum; #Bone fibrous sheath; EPB (extensor pollicis brevis); APL (abductor pollicis longus). |
 |
Figure 9 Differences between the bony protrusions in the radial styloid groove (left) and the flat radial styloid groove (right). *Bony protrusions. |
Clinical Application Discovery
We found that both ultrasound-guided acupotomy operation and blind acupotomy operation for dQD have good clinical results, but ultrasound guidance can reduce the bleeding rate of the procedure, which may be related to the blood vessels above the area of the first extensor tendon compartment (Figure 10) and the avoidance of subcutaneous vessels by ultrasound Doppler.
 |
Figure 10 The blood vessels above the area of the first extensor tendon compartment. |
Discussion
In this study, the clinical anatomical method was used to verify that ultrasound scanning can clearly visualize the acupotomy treatment area at the radial styloid process and clearly visualize the puncture and release process of the acupotomy. The ultrasound-guided acupotomy operation for dQD was superior to the blind operation in accuracy, possibly because the ultrasound-guided operation could be monitored and accurately positioned on the surface of the first bony fibrous sheath of the radial styloid process. This allowed avoiding the release of the superficial fascia of the fibrous tube or piercing the first extensor tendon compartment without releasing the fibrous sheath. However, there was a similar complete release rate between the two operation methods, indicating that the blind operation also has a high success rate under the premise of a skilled practitioner. Ultrasound-guided acupotomy treatment is widely accepted by clinicians. Ultrasound-guided acupotomy release has a good curative effect in the treatment of dQD,9 and ultrasound-guided acupotomy is better than palpation and positioning operations.10 This shows that the safety of ultrasound-guided acupotomy is similar to that of the blind operation. There was no radial nerve or radial artery injury in either group. The tendon injury rate of the ultrasound-guided group was lower than that of the blind group, but the difference was not significant. Ultrasound can locate the depth of the bony fibrous canal in the first extensor tendon compartment of the wrist, avoiding more tendon scratches. At the same time, ultrasound can identify anatomical variations and reduce the risk of operative injury.
Acupotomy treatment of dQD has been widely used in clinical practice, but there are potential safety hazards due to a lack of basic knowledge of anatomy and irregular operation protocols. In our study, we found that ultrasound-guided blind acupotomy for the treatment of dQD was less likely to damage blood vessels and nerves, and any injury was mainly along the tendon. Two cases of iatrogenic injury of dQD treated by irregular acupotomy have been reported.11 Within 2 months after the acupotomy treatment, the patient had a “clicking” sound at the radial styloid process when he held a heavy object. The ruptured APL tendon was sutured during surgery and was found to be cauda equina. We simulated deep penetration of the needle knife into the tendon on a wrist specimen, and a cauda equina break at the tendon was found (Figure 11). In the treatment of dQD with acupotomy, it is necessary to avoid transverse dissection and the bone surface in-depth operation to avoid tendon injury.12 Although there have been no clinical reports of needle knife injury to the nerves and vessels at the radial styloid process, clinical malpractice of local steroid injections into the superficial branches of the radial artery resulting in finger necrosis is still noteworthy.13,14 The superficial branches of the radial nerve are susceptible to medical injury due to their course and the design of the surgical incision.15 Patients who undergo surgery for dQD may suffer from postoperative complications such as nerve loss, transient or permanent sensory dullness, and neuroma.16 When acupotomy is performed for dQD, the palmar and dorsal 2 bony crests of the radial tuberosity and their highest points should be touched first. Above the line of the highest point of the crest and within 1 cm from the 2 highest points between the two crests is a safe treatment area; operations outside this area will increase the risk of injury to the superficial branch of the radial nerve, radial artery, cephalic vein, and tendon.17
 |
Figure 11 Simulated deep penetration of the acupotomy into the tendon results in a cauda equina break. |
The wrist radial extensor support band forms the first chamber of the wrist between the two bony crests at the radial styloid process, which forms the fibrous wall layer of the tendon sheath and serves to fix the ABL and EBP. The bone groove formed between the palmar and dorsal crests of the radial styloid process has little space for movement, and the wrist joint and thumb are under great tension during movement. The bony fibrous canal of the first chamber of the wrist at this location can be released by acupotomy to relieve the restrictive local anatomical structure of the causative agent. In this experiment, the length of the palmar crest of the radial tuberosity was measured to be 9.65 ± 1.67 mm (6.23~15.70 mm), so it can be completely loosened by pushing and cutting approximately 1 cm. At the same time, the extensor support band crosses the palmar crest longitudinally, and there is a distance of approximately 1 cm at both the proximal and distal ends, which can play a fixed role in preventing slippage of the tendon to a certain extent.
The fibrous septum is located within the bony layer of the first compartmental compartment of the wrist and manifests as a localized septum that does not extend along the entire length of the first compartmental compartment of the wrist. The development of radial stenosis tenosynovitis may be related to the presence of a fibrous septum. A septum at the radial styloid process increases the sliding resistance of the EPB during wrist flexion in biomechanical experiments.18 The presence of a fibrous septum may increase the susceptibility to dQD and failure of nonsurgical treatment.19 Eighty-six percent of patients with dQD had a septum completely separating the APL and EPB tendons.20 The septum might be a pathological state in which the septum progresses from incomplete to complete and may depend on the chronic inflammatory response of the synovial membrane produced by multiple APL and EPB tendon stenoses.21 In this study, 32.20% (19/59) had a fibrous septum, 6 cases had a complete fibrous septum accompanying the entire tendon extension, and 13 cases had an incomplete fibrous septum length of 6.78 ± 2.91 mm (2.45 to 10.88 mm). The fibrous septum in the fibrous sheath canal mainly wraps around the EPB tendon, making the space for the EPB tendon narrower.22 Surgical release of only the subspaces of the EPB tendon has also been clinically effective.23 The number of APL tendons ranges from 1 to 5, and the number of EPB tendons ranges from 0 to 3.24 Humans commonly have 2 or more APL tendons and 1 EPB tendon.25 Acupotomy can be considered to incise the subinterval of the EPB tendon by entering the ulnar side of the first carpal compartment, but considering that the EPB tendon is thin and small, it is prone to damage and rupture during the operation, and such an operation needs further research.
From the data of this experimental study, the rate of appearance of the bone crest in the bone groove of the radial styloid process was 30.5%, and the appearance of the bone crest reduced the sliding space of the tendon in the bone groove of the radial styloid process. The use of modified total tenosynovectomy and cystectomy for recurrent refractory radial stenosing tenosynovitis had satisfactory results and effectively prevented recurrence and complications,26 indicating that the crest is also a factor to be considered in the treatment of radial stenosing tenosynovitis. Measurements were performed on 284 Chinese cadaveric dry radius intact distal limb specimens, and the most common tissue was found to be type I (extensor sulcus divided into two grooves by a bony ridge) in 181 specimens, accounting for 63.73% of the total. Type II (a single groove of the extensor sulcus without bony ridges) was found in 79 specimens (27.82%). Type III (flat type) accounted for 24 cases (8.45%).27 This study used CT images to observe sex differences in the radial grooves of the first extensor compartment and found that 19.8% of men and 33.3% of women showed grooves with bony ridges in the first extensor groove of the wrist, suggesting that bony ridges are more common in women. This may also be one of the reasons why radial stenosis tenosynovitis is more prevalent in women.28
The study still has limitations. First, due to the limitation of the number of specimens and its conditions, there is the different water content between two groups, which may affect the results of the operation. The difference is not statistically significant, but some advantages of the ultrasound procedure can still be seen. Second, formalin-fixed human specimens differ from patients in tissue composition and morphology. We will further use clinical randomized controlled trials to observe the efficacy.
Conclusions
Both traditional and US-guided percutaneous release by acupotomy of the first extensor tendon compartment can be performed for all wrists. US-guided techniques can improve the success rate and reduce damage during acupotomy operations.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Author Contributions
YS and QZ contributed equally to this work and are co-first authors. YS and QZ contributed to data collection and verification. XS contributed to the methodology. YS and QZ contributed to the data analysis. YS contributed to writing the original draft. SL and WZ contributed to review and editing. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work is supported by National Natural Science Foundation of China (Youth Science Foundation Project; 82104886), Natural Science Foundation of Fujian Province (2021J01932), and China Scholarship Council (CSC).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Pensak MJ, Bayron J, Wolf JM. Current treatment of de Quervain tendinopathy. J Hand Surg Am. 2013;38(11):2247–2249. doi:10.1016/j.jhsa.2013.06.003
2. Kay NR. De Quervain’s disease. Changing pathology or changing perception? J Hand Surg Br. 2000;25(1):65–69. doi:10.1054/jhsb.1999.0277
3. Abate M, Silbernagel KG, Siljeholm C, et al. Pathogenesis of tendinopathies: inflammation or degeneration? Arthritis Res Ther. 2009;11(3):235. doi:10.1186/ar2723
4. Lapegue F, Andre A, Pasquier BE, et al. US-guided percutaneous release of the first extensor tendon compartment using a 21-gauge needle in de Quervain’s disease: a prospective study of 35 cases. Eur Radiol. 2018;28(9):3977–3985. doi:10.1007/s00330-018-5387-1
5. Gulec A, Turkmen F, Toker S, Acar MA. Percutaneous release of the first dorsal extensor compartment: a cadaver study. Plast Reconstr Surg Glob Open. 2016;4(10):e1022. doi:10.1097/GOX.0000000000001022
6. Yoon SH, Kim YS, Jo HG, Kwon CY. Current usage of terminologies related to acupotomy: a literature research and standardization suggestion. Chin J Integr Med. 2019;25(2):147–150. doi:10.1007/s11655-018-3015-1
7. Shen YF, Zhou QY, Li SL. Research progress of stenosing tenosynovitis of radial styloid process based on anatomical structure. Zhongguo Gu Shang. 2019;32(5):479–484. doi:10.3969/j.issn.1003-0034.2019.05.018
8. Kwon CY, Yoon SH, Lee B. Clinical effectiveness and safety of acupotomy: an overview of systematic reviews. Complement Ther Clin Pract. 2019;36:142–152. doi:10.1016/j.ctcp.2019.07.002
9. Chen P, Xiao D, Guo R, Yan MZ. Clinical observation of ultrasound-guided small acupuncture in the treatment of radial stem stenosis tenosynovitis. Clin Res Tradition Chin Med. 2017;9(21):41–42.
10. Zhu T, Jiang W, Wang K, Shanshan Y. Ultrasound-guided drug injection combined with acupuncture for radial stem stenosis tenosynovitis. Chin J Interv Imaging Ther. 2018;15(8):465–468.
11. Xu WX. Complications and management of tenosynovitis treated with small acupuncture. J Pract Hand Surg. 2003;3:186–190.
12. Wang L, Li YK, Liu Q. Problems in the treatment of radial stenosis tenosynovitis with acupuncture. Chin J Rehabil Med. 2011;26(03):275–277.
13. Wang BA, Li CL, Wang EF. A case of finger necrosis due to closure of radial stenosis tendinitis. Chin J Bone Joint Inj. 2010;25(01):88.
14. Zuoren Z, Dianfa F, Guohui L, Zhao Q. Finger necrosis due to local closure of radial stenosing tenosynovitis (with 3 case reports). Chin J Orthop Surg. 2005;5:72.
15. Robson AJ, See MS, Ellis H. Applied anatomy of the superficial branch of the radial nerve. Clin Anat. 2008;21(1):38–45. doi:10.1002/ca.20576
16. PernoIoanna D, Papaloïzos M. Une approche globale incluant une nouvelle technique d’élargissement pour prévenir les complications du traitement chirurgical de la tendinopathie de De Quervain. Hand Surg Rehabil. 2016;35(3):183–189.
17. Liu X, Zhang JJ, Jing YJ, Liao LQ. Anatomical study of the safety zone of radial stem stenosis tenosynovitis treated with acupuncture. Tradition Chin Med Orthop. 2018;30(02):7–9.
18. Kutsumi K, Amadio PC, Zhao C, Zobitz ME, An KN. Gliding resistance of the extensor pollicis brevis tendon and abductor pollicis longus tendon within the first dorsal compartment in fixed wrist positions. J Orthop Res. 2005;23(2):243–248. doi:10.1016/j.orthres.2004.06.014
19. Sato J, Ishii Y, Noguchi H. Ultrasonographic evaluation of the prevalence of an intracompartmental septum in patients with de quervain’s disease. ORTHOPEDICS. 2016;39(2):112–116. doi:10.3928/01477447-20160222-05
20. Gousheh J, Yavari M, Arasteh E. Division of the first dorsal compartment of the hand into two separated canals: rule or exception? Arch Iran Med. 2009;12(1):52–54.
21. Hoch J, Fritsch H, Lewejohann S. [Congenital or acquired disposition of the separate compartment of the extensor pollicis brevis tendon associated with stenosing tendovaginitis (de Quervain’s disease)? Macroanatomical and fetal-plastinationhistological studies of the first compartment of the wrist]. Ann Anat. 2004;186(4):305–310. German.
22. Xiao L, Liu Q, Li YK. Anatomical and morphological typing of the radial styloid process and its clinical significance. Chin Med Clin Anat. 2010;28(05):507–509.
23. Yuasa K, Kiyoshige Y. Limited surgical treatment of de Quervain’s disease: decompression of only the extensor pollicis brevis subcompartment. J Hand Surg Am. 1998;23(5):840–843. doi:10.1016/S0363-5023(98)80160-3
24. Alemohammad AM, Yazaki N, Morris RP, Buford WL, Viegas SF. Thumb interphalangeal joint extension by the extensor pollicis brevis: association with a subcompartment and de Quervain’s disease. J Hand Surg Am. 2009;34(4):719–723. doi:10.1016/j.jhsa.2008.12.015
25. Kulthanan T, Chareonwat B. Variations in abductor pollicis longus and extensor pollicis brevis tendons in the Quervain syndrome: a surgical and anatomical study. Scand J Plast Reconstr Surg Hand Surg. 2007;41(1):36–38. doi:10.1080/02844310600869720
26. Qian X, Shiping J, Rui-Long X. Surgical treatment of radial stem stenosis tenosynovitis. J Clin Mil Med. 2014;42(03):325.
27. Xiao L, Li YK, Ye GH, Yang XW. Variations in the extensor grooves on the radial styloid process in Chinese population. Surg Radiol Anat. 2013;35(1):49–53. doi:10.1007/s00276-012-0995-y
28. Gurses IA, Turkay R, Inci E, et al. Sex differences in the radial grooves in the first extensor compartment. Skeletal Radiol. 2016;45(7):955–958. doi:10.1007/s00256-016-2381-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Traditional Chinese Non-Pharmacological Therapies on Knee Osteoarthritis: A Narrative Review of Clinical Application and Mechanism
Liu ZF, Zhang Y, Liu J, Wang YY, Chen M, Liu EY, Guo JM, Wang YH, Weng ZW, Liu CX, Yu CH, Wang XY
Orthopedic Research and Reviews 2024, 16:21-33
Published Date: 26 January 2024
Acupotomy for Musculoskeletal Pain: Exploring Therapeutic Potential and Future Directions
Hu J, Tong H, Zhang J, Jiang L
Journal of Pain Research 2025, 18:3027-3036
Published Date: 17 June 2025