Back to Journals » Journal of Pain Research » Volume 19
Percutaneous Endoscopic Lumbar Discectomy Serves as a Valuable Minimally Invasive Surgical Option for Adolescent Lumbar Disc Herniation: Mid-Term Outcomes from a Retrospective Cohort Study
Authors Zhang B ![]() , Zhou Q, Zhong C
, Zhou Q, Zhong C ![]() , Huang X
, Huang X ![]() , Hu Z, Zhao Q, Wang B, Zhu Z, Qiu Y, Sun X
, Hu Z, Zhao Q, Wang B, Zhu Z, Qiu Y, Sun X
Received 19 February 2026
Accepted for publication 26 May 2026
Published 28 May 2026 Volume 2026:19 604244
DOI https://doi.org/10.2147/JPR.S604244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Bolu Zhang,1 Qingshuang Zhou,1 Chao Zhong,2 Xingcheng Huang,2 Zongshan Hu,1 Qinghua Zhao,1 Bin Wang,1 Zezhang Zhu,1 Yong Qiu,1 Xu Sun1
1Division of Spine Surgery, Department of Orthopedic Surgery, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China; 2Division of Spine Surgery, Department of Orthopedic Surgery, Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Xu Sun, Division of Spine Surgery, Department of Orthopedic Surgery, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Objective: To compare perioperative outcomes, mid-term clinical efficacy, and sciatic scoliosis correction after percutaneous endoscopic lumbar discectomy (PELD) versus mini-open fenestration discectomy (MOFD) for adolescent lumbar disc herniation (ALDH).
Methods: This retrospective cohort study reviewed 174 patients aged ≤ 21 years who underwent single-level L4/5 or L5/S1 discectomy between January 2021 and December 2024. Patients were grouped by procedure: PELD (n=83; TELD 44, IELD 39) or MOFD (n=91). Perioperative outcomes, VAS, ODI, EQ-5D, modified MacNab results, complications, recurrence, and radiographic correction of sciatic scoliosis were compared.
Results: Baseline characteristics were comparable between groups. Compared with MOFD, PELD had a smaller incision (0.9± 0.3 vs 3.7± 0.7 cm; p< 0.001), lower blood loss (13.6± 12.1 vs 48.2± 51.5 mL; p< 0.001), no postoperative drainage, and shorter postoperative hospital stay (2.7± 1.0 vs 4.5± 1.6 days; all P< 0.001). Operative time did not differ significantly. Both groups showed sustained improvement in VAS, ODI, and EQ-5D. The only between-group clinical difference was lower VAS back pain on postoperative day 1 after PELD, which did not persist. Excellent/good MacNab outcomes were similar (94.0% vs 94.5%). Same-level recurrence occurred in 3.6% and 2.2%, respectively. Among 63 patients with sciatic scoliosis, both procedures achieved comparable Cobb angle and AVT correction, with satisfactory radiographic and clinical correction in 95.2%.
Conclusion: In this retrospective cohort, PELD provided less surgical trauma and faster early recovery than MOFD while achieving comparable mid-term functional outcomes and sciatic scoliosis correction. These findings support PELD as a valuable minimally invasive option for ALDH patients.
Keywords: adolescent lumbar disc herniation, percutaneous endoscopic lumbar discectomy, mini-open fenestration discectomy, sciatic scoliosis, minimally invasive spine surgery
Introduction
Lumbar disc herniation (LDH) is one of the most common degenerative spinal diseases in adults and a major cause of low back pain and radiating pain in the lower extremities.1,2 Although adolescent lumbar disc herniation (ALDH) accounts for only 0.5–6.8% of surgically treated LDH cases, it poses distinct clinical challenges.3–7 Different from adult degenerative diseases, the etiology of ALDH often has a traumatic or genetic predisposition with intensive physical activity being common contributors.8–10 Adolescents are at a critical phase of spinal growth and development, characterized by incomplete maturation of both bone and soft tissue structures. This ongoing developmental process usually continues until around 21 years old with the closure of the vertebral epiphysis.11–13 This unique biological context makes it necessary to have substantially different clinical management strategies for ALDH compared to adults. Accordingly, determining an appropriate surgical strategy is particularly important in adolescents requiring operative treatment.
ALDH often causes marked functional limitation and may be accompanied by postural abnormalities, particularly sciatic scoliosis.14 Sciatic scoliosis is generally considered an antalgic compensatory posture caused by nerve root irritation, radicular pain, and paraspinal muscle spasm.15 This trunk shift may temporarily reduce nerve-root tension and relieve pain.16 This deformity is usually flexible and non-structural, but persistent disc compression may prolong asymmetric loading of the immature spine and impair daily function. Therefore, in adolescents, the correction of sciatic scoliosis after decompression is not only a radiographic outcome but also an important indicator of pain relief, functional recovery, and restoration of spinal balance.
Conservative therapy is the primary treatment for ALDH, including activity modification, strict bed rest, and physical therapy modalities such as intermediate frequency physiotherapy, analgesics, muscle relaxants, and epidural steroid injections.17–19 However, surgery should be considered for those with significant neurological compromise, such as motor weakness, cauda equina syndrome, or intractable pain that does not improve after exhaustive conservative management for a recommended duration.20,21
Mini-open fenestration discectomy (MOFD) has traditionally been regarded as a conventional and widely used surgical approach for LDH.22 It enables a direct view of neural structures, provides well-established efficacy, and has demonstrated satisfactory long-term outcomes in clinical practice.23 However, the extensive tissue that has to be dissected out including paraspinal muscle dissection, partial removal of vertebral bone and ligamentum flavum, and significant nerve root retraction may contribute to prolonged postoperative recovery, persistent low back pain, and potential iatrogenic instability.24–26 These limitations are particularly relevant in adolescents because preserving spinal mobility and growth potential is crucial.
In recent years, with the advancement of minimally invasive spinal endoscopic techniques, PELD has been increasingly adopted for the surgical management of LDH. Improvements in endoscopic visualization, working-channel systems, continuous saline irrigation, and specialized instruments have expanded the feasibility and safety of endoscopic decompression in clinical practice. This minimally invasive procedure is performed through a small working channel either transforaminal (TELD) or interlaminar (IELD) under continuous saline irrigation and endoscopic magnification.27 By achieving neural decompression with less disruption of posterior musculoligamentous structures, PELD may preserve lumbar anatomy and biomechanical stability, which is particularly relevant for adolescents.
Although MOFD and PELD have been compared in adults with LDH, evidence specific to adolescents remains limited.25,28–31 Furthermore, the impact of these techniques on the improvement of sciatic scoliosis has not been adequately evaluated. Therefore, this study aims to systematically compare MOFD and PELD in the treatment of ALDH, with particular focus on perioperative parameters, short- and mid-term clinical outcomes, functional recovery, and the resolution of sciatic scoliosis. We hypothesized that PELD would provide clinical and radiographic outcomes comparable to those of MOFD, while reducing surgical trauma, accelerating postoperative recovery, and achieving effective improvement of sciatic scoliosis.
Methods
Study Design and Patient Population
This study was approved by the ethics committee of Nanjing Drum Tower Hospital (2025–1273-01). We conducted a retrospective analysis of patients younger than 21 years with single-level L4/5 or L5/S1 LDH who had received surgical treatment in our center between January 2021 and December 2024. The diagnosis of ALDH was established according to clinical history, physical examination and lumbar magnetic resonance imaging (MRI). The detailed patient selection process is shown in Figure 1. Given the retrospective and non-randomized nature of this cohort study, treatment allocation was based on clinical decision-making rather than a predefined randomization protocol. Therefore, the possibility of selection bias and confounding by indication cannot be fully excluded.
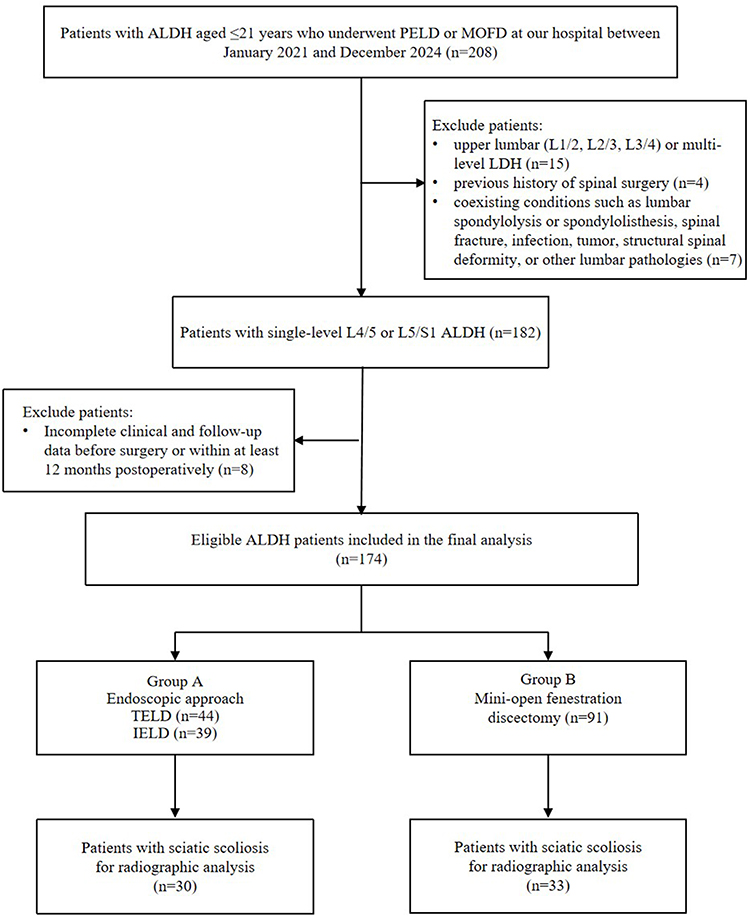 |
Figure 1 Study flow diagram showing the inclusion and exclusion of patients. |
The inclusion criteria were as follows: (1) patients who underwent surgery under the age of 21 years; (2) MRI-confirmed single-level LDH at L4/5 or L5/S1 with no improvement of symptoms after 6 weeks of conservative treatment; (3) presence of significant symptoms and signs consistent with the radiographic findings; (4) treatment with either MOFD or PELD; (5) complete follow-up data available for at least 12 months after surgery.
The exclusion criteria included: (1) upper lumbar (L1/2, L2/3, L3/4) or multi-level LDH; (2) previous history of spinal surgery; (3) coexisting conditions such as lumbar spondylolysis or spondylolisthesis, spinal fracture, infection, tumor, structural spinal deformity, or other lumbar pathologies.
According to the surgical procedure they received, patients were divided into two groups: patients who underwent PELD (including TELD and IELD) were assigned to Group A, and those who underwent MOFD were assigned to Group B. TELD and IELD were combined because both are PELD approaches with the same endoscopic decompression goal, and approach selection was indication-based rather than randomized; therefore, separate subgroup comparison was not performed to avoid selection bias and limited statistical power.
Surgical Techniques
All procedures were performed by senior spinal surgeons (X.S. Z.Z. and B.W.) who have extensive experience in both open and endoscopic techniques. The surgical approach (TELD, IELD, or MOFD) was selected by the treating surgeon after evaluation of disc level, herniation morphology, anatomical feasibility, anesthesia tolerance, and patient-specific clinical factors. In Group A, the selection between the TELD and IELD approaches was mainly based on the level of herniation and patient’s ability to tolerate anesthesia. Generally, TELD was chosen for herniations at L4/5 and was performed under local anesthesia with conscious sedation in suitable patients, whereas IELD was often preferred for L5/S1 or central herniations and was generally conducted under general anesthesia. The three procedures share similar elements in terms of patient positioning and sterilization. The patients were placed in a prone position for surgery, with their hips and knees moderately flexed and supported by pillows or positioning pads to maintain the posture.
Transforaminal Endoscopic Lumbar Discectomy (TELD)
Under C-arm guidance, the skin entry point was marked approximately 8–12 cm away from the middle line of the target intervertebral space. After local infiltration with 0.5% lidocaine was given and a needle was then advanced to the outer foramen under fluoroscopy. Guidewire insertion, followed by a 0.7 cm incision. Sequential dilators were used to place a working cannula. The spinal endoscope (TESSYS, Joimax, Germany) was introduced, and the anatomy was visualized under saline irrigation. The surgical field was cleared using a bipolar radiofrequency probe and nucleus forceps. If necessary, foraminoplasty was performed with a trephine, drill, or osteotome. The herniated disc was exposed and removed, along with any compressive material ventral to the nerve root and within the foramen. Adequate decompression was confirmed by free pulsation and mobility of the traversing nerve root and thecal sac. After hemostasis, the cannula was withdrawn and the incision closed without drainage.
Interlaminar Endoscopic Lumbar Discectomy (IELD)
A standard interlaminar approach, directly facing the pathological level, was used. Entry point was checked by fluoroscopy, followed by a 1.2 cm skin incision and soft tissue dilation. The large-channel endoscope (iLESSYS-Delta, Joimax, Germany) was inserted through the cannula. Under endoscopic vision, a limited laminotomy and medial facetotomy were carried out so as to have access to the spinal canal, taking care to maintain spinal stability. Then, the ligamentum flavum was opened and part of it was removed, exposing the dural sac and the compressed nerve root. The herniated disc fragment was clearly identified anteriorly or axillary to the nerve root, and was carefully removed using endoscopic forceps. Decompression considered satisfactory following confirmation of free nerve root movement and strong dural pulsations. Finally, the endoscope and cannula were withdrawn, and the incision was closed without placement of a drain.
Mini-Open Fenestration Discectomy (MOFD)
A midline longitudinal incision, approximately 3–5 cm in length, was centered over the target spinal segment. Subperiosteal dissection of the paraspinal muscles allowed exposure of the laminae and the facet joints at the target level. Then a fenestration was done with a Kerrison rongeur to perform a partial laminectomy, which involved resecting the inferior edge of the lamina of the cephalad vertebra, the superior edge of the lamina of the caudal vertebra, as well as the medial portion of the facet joint. The ligamentum flavum was removed so that the thecal sac, the compromised nerve root, and the herniated disc material were fully visible. The herniated nucleus pulposus was carefully removed, along with any loose disc fragments within the intervertebral space. Upon verification of adequate neural decompression and free nerve root mobility, a surgical drain was placed. The wound was then irrigated and closed layer by layer.
Postoperative Management
All patients received standardized postoperative care. Patients in Group A were instructed to start sitting and ambulating with the support of a lumbar brace after 24 hours of bed rest. In Group B, the surgical drain was routinely removed within 24 hours after the operation, then movement started under identical brace protection. During the first postoperative month, all patients were instructed to avoid activities involving heavy lifting, or excessive bending or twisting of the trunk. Moderate intensity lumbar and back muscle strengthening exercises regimens were also incorporated into the rehabilitation program during this time for slow muscular recovery. Follow-up assessments included standing whole-spine radiographs and quality of life (QOL) evaluations at 3, 6, and 12 months to assess coronal balance and clinical outcomes. MRI was performed at 3 and 12 months postoperatively and last follow-up to evaluate the degree of decompression and disc status.
Evaluation Metrics
Clinical data were obtained from the hospital information system, with follow-up QOL data collected via telephone or face to face interviews. The collected dataset included patients’ demographic information, disease duration, herniation side, and perioperative metrics such as operative time, incision length, intraoperative blood loss, postoperative drainage, and postoperative hospitalization days. Complication identification data sources comprised operative notes, anesthesia and nursing records, along with clinical, radiographic, and patient-reported outcomes from follow-up visits.
Patient-reported outcomes, such as Visual Analog Scale (VAS) scores for back and leg pain, the Oswestry Disability Index (ODI), and the European Quality of Life-5 Dimensions (EQ-5D) questionnaire were systematically collected preoperatively and postoperatively. Overall treatment satisfaction was assessed using the modified MacNab criteria at the last follow-up. Additionally, MRI was performed to evaluate the completeness of resection of herniated nucleus pulposus fragments.
For patients with sciatic scoliosis, the resolution of spinal curvature was evaluated by comparing preoperative and follow-up standing radiographs, specifically measuring changes in apical vertebral translation (AVT) and Cobb angle.
Statistical Analysis
All statistical analyses were done with SPSS Statistics (version 26.0; IBM Corp., Armonk, NY, USA). Continuous variables’ normality of data distribution was tested by the Kolmogorov–Smirnov test. Continuous variables including age, body mass index (BMI), duration of symptoms, AVT, Cobb angle, operative duration, blood loss, postoperative drainage, postoperative hospital stay, and VAS/ODI scores were approximately normally distributed, so they were expressed as the mean±standard deviation (SD). Categorical variables, such as gender, operative level, side of herniation, and modified MacNab criteria, were expressed as numbers and percentages. For comparisons between Group A and Group B, continuous variables were compared using the independent-sample Student’s t-tests, and categorical variables were compared using either the Chi-square test or Fisher’s exact test as needed. For between-group comparisons of continuous outcomes, mean differences with 95% confidence intervals (CIs) were calculated, with Group A minus Group B defined as the direction of the difference. All figures, including histograms and line charts, were generated using GraphPad Prism software (version 9.0; GraphPad Software, San Diego, CA, USA). A two-tailed p-value of less than 0.05 was considered statistically significant. Because this was a retrospective cohort study, no formal a priori sample size calculation was performed before patient enrollment. All eligible patients during the study period were included. A post hoc sensitivity analysis was subsequently performed to assess the adequacy of the available sample size. The results indicated that the current sample size was sufficient to detect moderate between-group differences in continuous perioperative and functional outcomes, but the study may have been underpowered to detect differences in uncommon complications or recurrence.
Results
Patient Demographic Data
A total of 174 adolescent patients were included in the final analysis with 83 patients assigned to Group A and 91 patients to Group B. In Group A, the specific endoscopic approaches included IELD in 39 cases and TELD in 44 cases. The follow-up time ranged from 12 to 60 months, with a mean follow-up time of 33.2±11.0 months in Group A and 31.3±14.1 months in Group B. The preoperative demographic and clinical characteristics of both groups are summarized in Table 1. There were no statistically significant differences between the two groups in terms of age, gender distribution, BMI, herniation level, side of disc herniation, and duration of disease. Sciatic scoliosis was present in 30 patients (36.1%) in Group A and 33 patients (36.3%) in Group B, with no significant difference in incidence between the groups. Furthermore, the mean duration of follow-up was comparable between Group A and Group B.
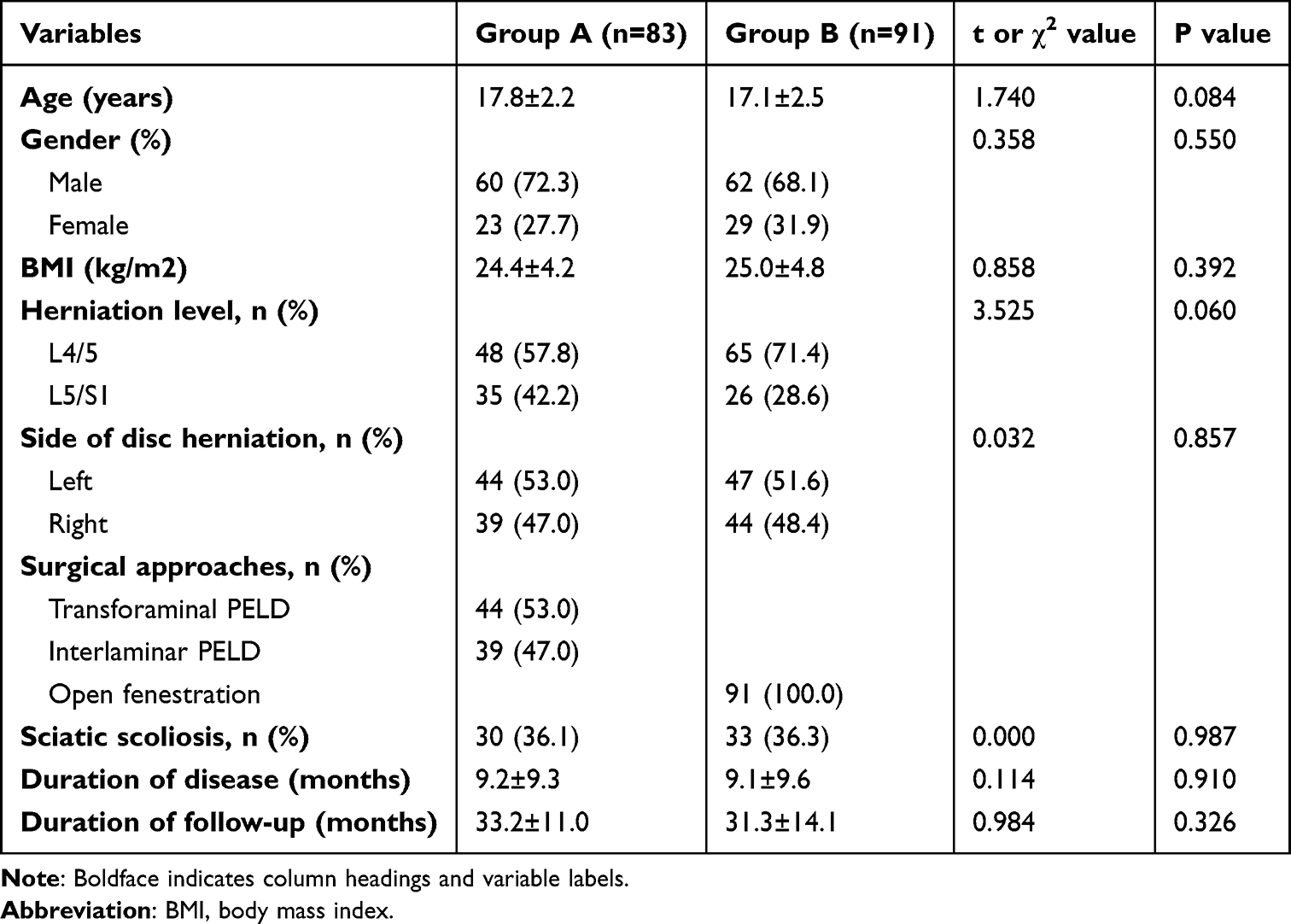 |
Table 1 Demographic and Clinical Characteristics of 174 ALDH Cases |
Perioperative Outcomes
The comparison of perioperative parameters is presented in Table 2. No significant difference was observed in the duration of surgery between the two groups. The incision length was markedly smaller in Group A. Additionally, as no drainage tube was placed in Group A, the postoperative drainage volume was significantly lower than in Group B. Patients in Group A also experienced substantially less intraoperative blood loss. Furthermore, Group A demonstrated a significantly shorter postoperative hospital stay.
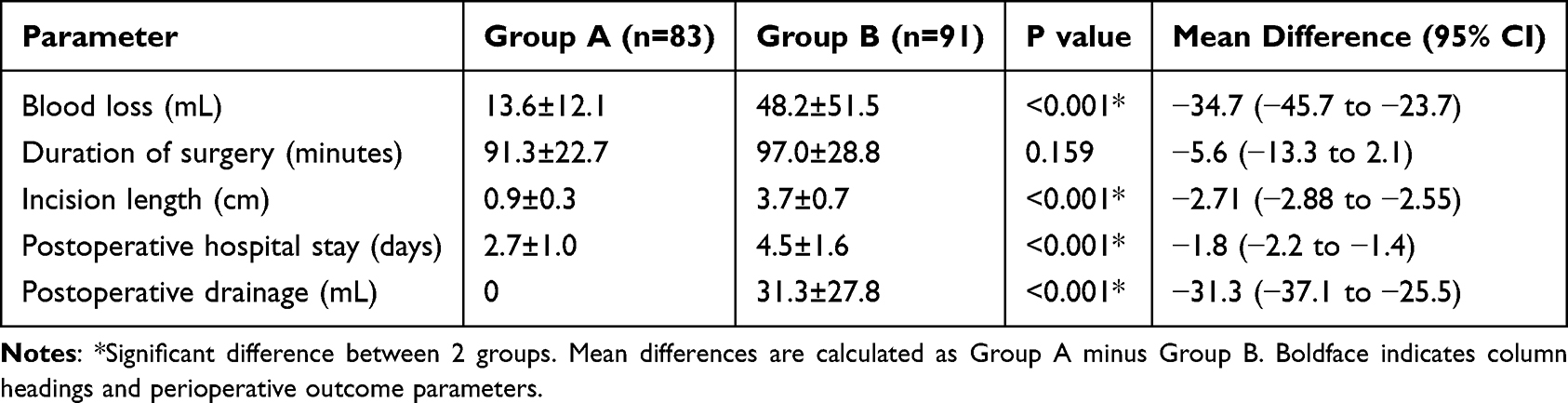 |
Table 2 Comparison of Surgical Information Between the Two Groups |
Clinical Results
Patient-reported outcomes are detailed in Table 3 and Figure 2A–D. Both surgical techniques led to significant and sustained reductions in VAS scores for back and leg pain and improvement in ODI scores at all postoperative time points. A notable early finding was that patients in Group A reported significantly lower VAS scores for lower back pain on postoperative day 1 compared to Group B. However, this inter-group difference was transient and no longer evident at the 3-month, 6-month, or final follow-up assessments. Similarly, there were no significant differences in VAS scores for leg pain or ODI scores between the groups at any other postoperative time point. Both groups demonstrated similarly significant improvements in EQ-5D scores at the final follow-up, with no significant difference between them. At the final follow-up, the rate of “Excellent” or “Good” outcomes according to the modified MacNab criteria was similarly high in both Group A (94.0%) and Group B (94.5%).
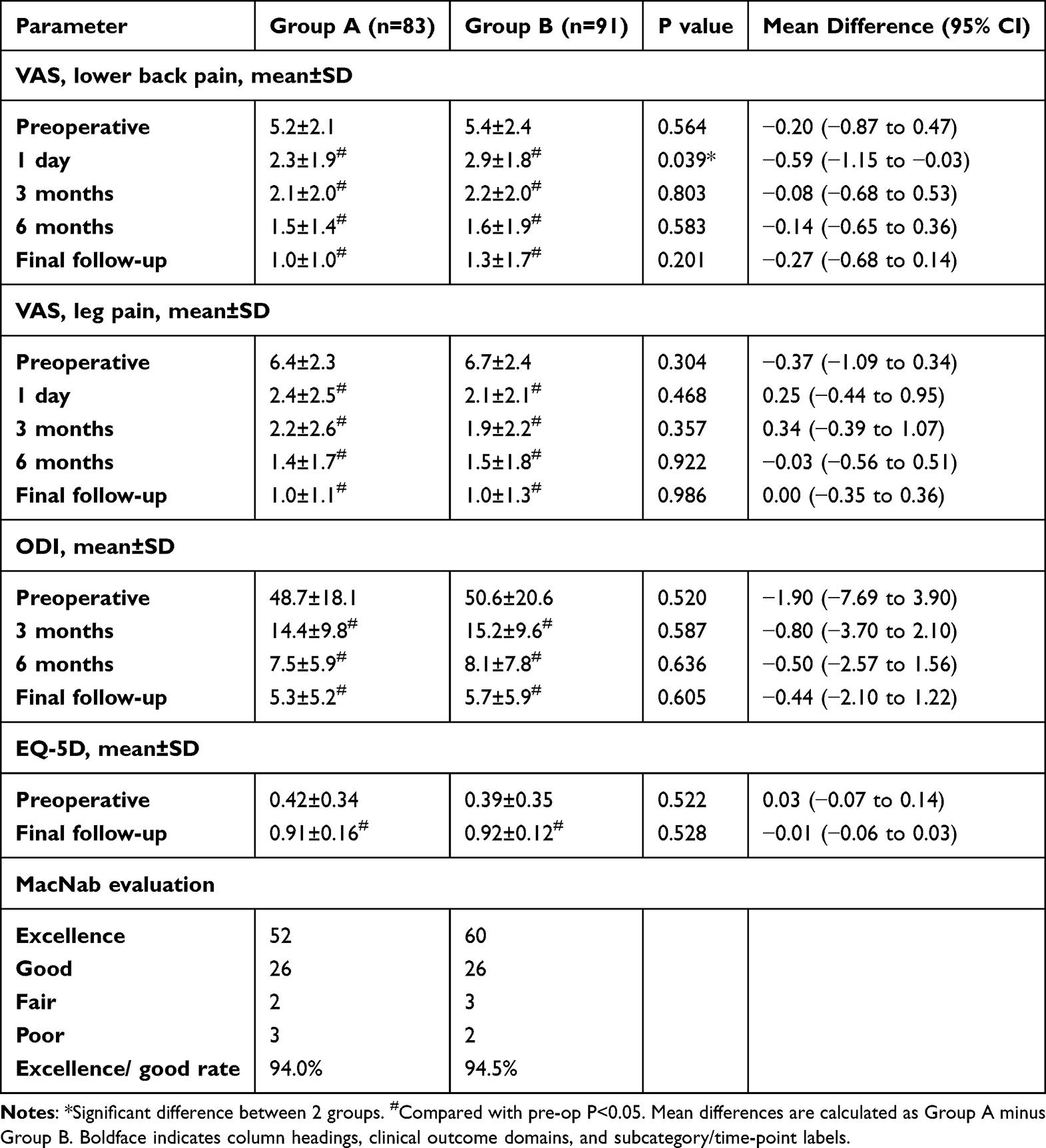 |
Table 3 Comparison of Changes in Clinical Outcomes Between Two Groups |
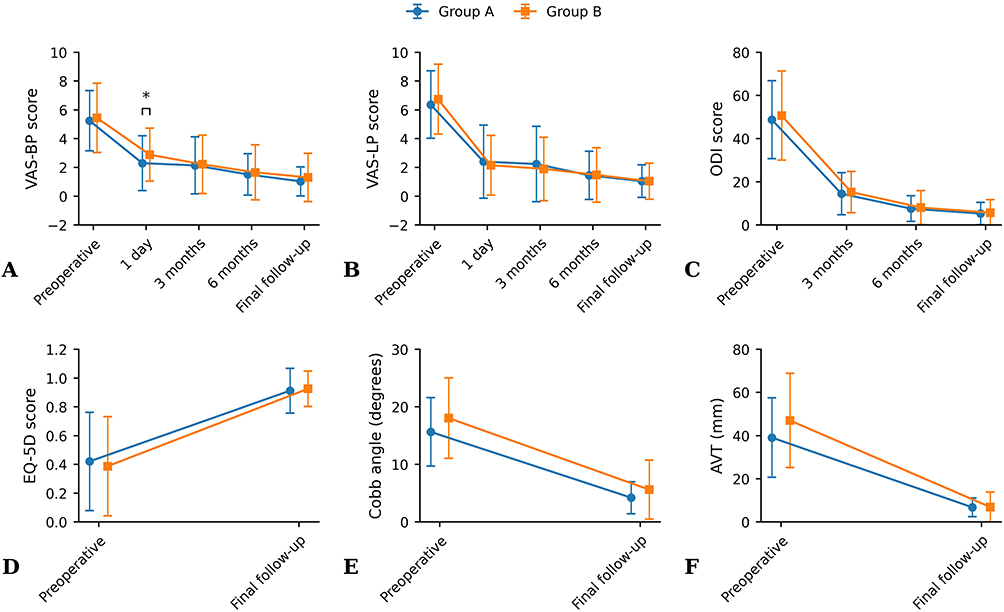 |
Figure 2 Comparison of pre- and postoperative clinical outcomes and imaging measurements in MOFD and PELD group. (A) Changes in VAS-BP score; (B) Changes in VAS-LP score; (C) Changes in ODI score; (D) Changes in EQ-5D score; (E) Changes in Cobb angle; (F) Changes in AVT. |
Spontaneous Correction of Sciatic Scoliosis
Among the 174 patients, 63 presented with sciatic scoliosis preoperatively. Radiographic outcomes are shown in Table 4 and Figure 2E–F. Both PELD and MOFD resulted in marked correction of sciatic scoliosis, with significant improvements in Cobb angle and AVT at final follow-up. The degree of correction was comparable between the two groups. Overall, 60 of 63 patients achieved satisfactory radiographic and clinical correction. A representative case is shown in Figure 3.
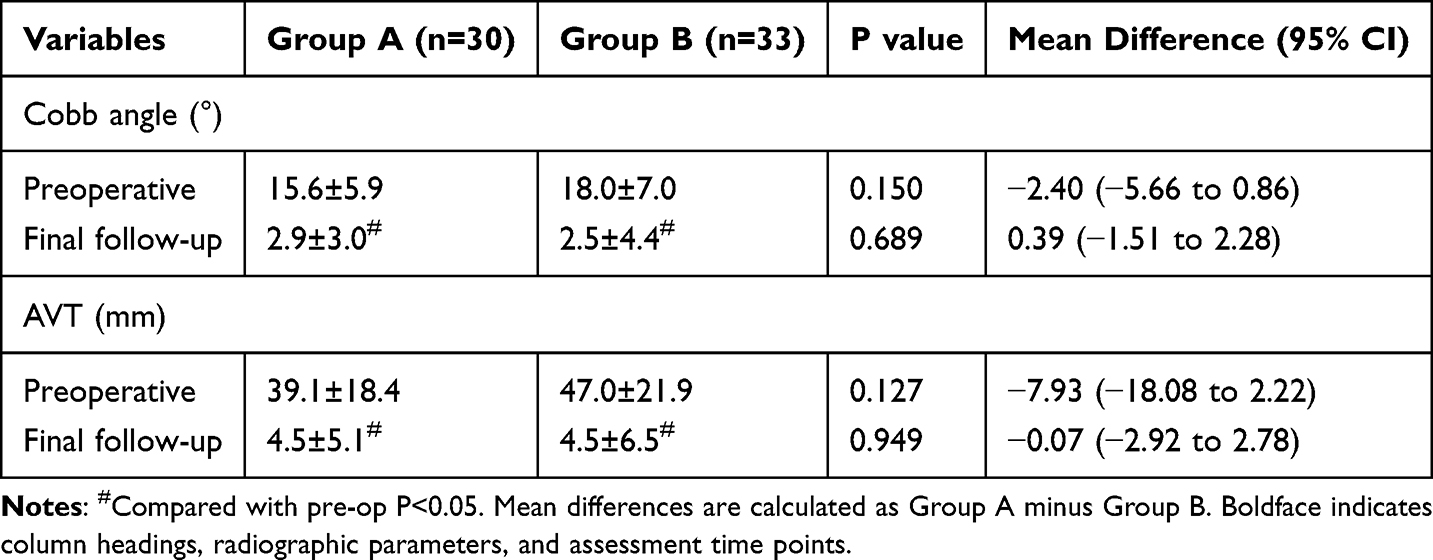 |
Table 4 Comparative Radiographic Outcomes of Sciatic Scoliosis Correction Between Groups |
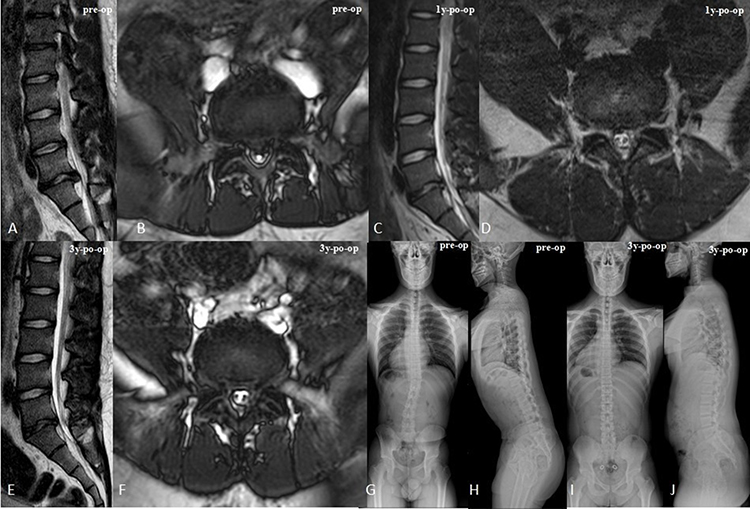 |
Figure 3 A 15-year-old boy with ALDH presented with sciatic scoliosis. Preoperative MRI in the sagittal (A) and axial (B) planes revealed a left-sided L5/S1 disc herniation. Postoperative MRI obtained at 1 year post-surgery in the sagittal (C) and axial (D) planes confirmed complete removal of the herniated disc. Postoperative MRI obtained at 3 years post-surgery in the sagittal (E) and axial (F) planes further confirmed complete removal of the herniated disc. Preoperative X-ray images in the coronal (G) and sagittal (H) views demonstrated sciatic scoliosis in the coronal plane and imbalance in the sagittal plane. The patient underwent an interlaminar endoscopic lumbar discectomy. Corresponding 3-year postoperative X-ray images in the coronal (I) and sagittal (J) views illustrated recovery of both coronal and sagittal spinal alignment, along with resolution of sciatic scoliosis. |
Complications
The overall complication rates were low in both groups, with no statistically significant differences observed between them (Table 5). Neither group was observed with cases of nerve root injury, facet joint injury, dural tear, or surgical site infection. In Group B, one patient experienced delayed wound healing, which was resolved with conservative local wound care. Transient leg pain or numbness occurred in one patient in each group, both of which were successfully managed with a short period of medication. During TELD surgery, one patient with spinal rotational deformity secondary to scoliosis presented initial difficulty in puncture needle placement; this was resolved through intraoperative adjustment, and the procedure was subsequently completed without further incidents. Regarding the follow-up complications, none in either group experienced segmental instability, but symptomatic recurrence of disc herniation at the same surgical level was observed in three patients (3.6%) in Group A and two patients (2.2%) in Group B.
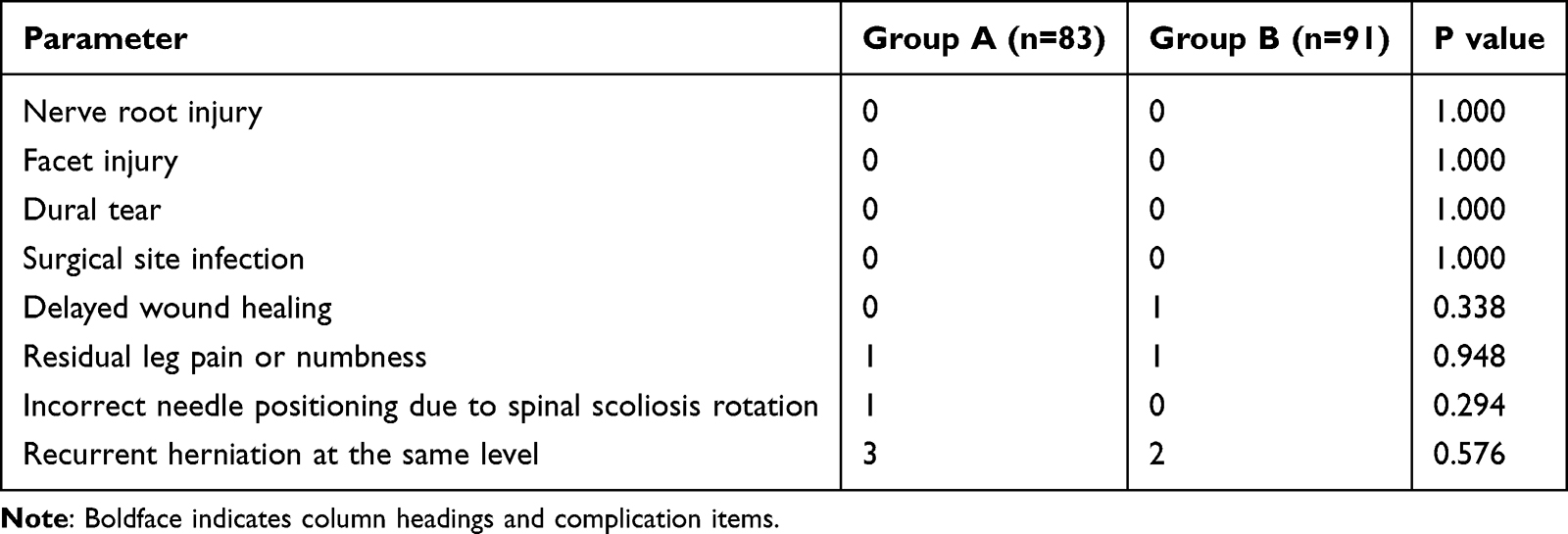 |
Table 5 Complications Collected from MOFD and PELD Groups |
Discussion
This study compared the perioperative outcomes and mid-term clinical effectiveness of PELD and MOFD for ALDH and it is the first study to compare the different effects of these two surgical approaches on the resolution of sciatic scoliosis in ALDH. Our results show that both techniques had similar and good mid-term functional outcomes, and were equally effective at correcting sciatic scoliosis, but PELD had better perioperative metrics. More specifically, the PELD approach led to notably less surgical trauma, lower intraoperative blood loss, shorter hospital stays, and quicker pain relief right after surgery.
Given the close association between ALDH and spinal developmental status, and considering that vertebral growth plates typically fuse around the age of 21, our study established an upper age limit of 21 years. Adolescent patients require effective neural decompression with maximal preservation of developing spinal structures. Although MOFD remains a reliable conventional approach, it requires wider soft-tissue dissection and partial removal of posterior elements. In contrast, PELD uses a limited working corridor and endoscopic visualization, which may explain the lower blood loss and absence of drainage observed in the present cohort.
In our study, we observed that PELD possesses numerous benefits compared to MOFD in treating ALDH. The significantly lower intraoperative blood loss in Group A may be explained by its smaller working channel, reduced soft-tissue exposure, and endoscopic radiofrequency-assisted hemostasis, which together minimize bleeding from paraspinal and posterior ligamentous structures.32–34 PELD’s other main advantage is no postoperative drainage, which fits its less invasive profile. Conversely, MOFD generally necessitates drainage because of the extended incisions and broader dissection of the common surgery procedure in traditional operations. Furthermore, PELD patients experienced a significantly shorter postoperative hospital stay, which is in line with previous studies that highlight the faster recovery associated with minimally invasive techniques.35,36 These advantages, including smaller incisions, reduced tissue trauma, and lower early postoperative back pain, may be particularly relevant for adolescents, in whom rapid recovery and preservation of developing spinal structures are important.
Anesthetic management may be another important factor contributing to the early postoperative differences between groups. Unlike IELD and MOFD, which are normally done with general anesthesia, where a patient is intubated through an endotracheal tube, TELD can be successfully carried out with local anesthesia and conscious sedation. This technique is not performed under general anesthesia, which eliminates the associated risks of airway manipulation and potential side effects including postoperative nausea, sore throat, respiratory complications, and potential cognitive effects, all of which are particularly relevant to the adolescent population. More importantly, the patient’s ability to stay awake and provide real-time feedback during the surgical procedure enhances safety by allowing for timely alerts about nerve root irritation, which helps mitigate the risk of iatrogenic neural injury.37 These anesthesia-related advantages may facilitate earlier postoperative alertness, mobilization, and discharge readiness. Therefore, although the reduced surgical trauma of PELD remains an important explanation for early recovery, the observed differences in early back pain, mobilization, and postoperative hospital stay may also be partly attributable to the anesthetic approach.
In our research, both PELD and MOFD showed a significant positive transformation in pain relief and functional recovery, with comparable outcomes in terms of VAS scores for back and leg pain, ODI scores, and modified MacNab criteria. Nevertheless, distinct benefits of PELD were observed during the initial postoperative phase since the VAS scores of patients with PELD reflected lower back pain level on the first day after the surgery as compared to those who received MOFD. This early benefit may be related to the less invasive nature of endoscopic surgery, including reduced paraspinal muscle injury, smaller incisions, less postoperative inflammatory response, and may also be partly influenced by differences in anesthetic management. However, this early advantage did not translate into long-term benefits, indicating that the clinical outcome of the two procedures ultimately depends on sufficient neural decompression, rather than the surgical entry method.
Nevertheless, previous studies have not uniformly demonstrated superior outcomes with minimally invasive or endoscopic discectomy. A Cochrane review reported that minimally invasive discectomy may be associated with less favorable leg pain relief, low back pain relief, and rehospitalization outcomes than microdiscectomy or open discectomy, although the absolute differences were small and the overall quality of evidence was limited.38 Similarly, Teli et al39 found higher rates of dural tears and recurrent herniation after micro-endoscopic discectomy than after open discectomy. Gibson et al40 reported comparable 2-year functional outcomes between transforaminal endoscopic discectomy and microdiscectomy, but noted more repeat MRI examinations and revision procedures in the endoscopic group. These findings suggest that reduced soft-tissue disruption alone does not necessarily translate into superior clinical outcomes. Limited visualization, a narrow working corridor, a steep learning curve, and the possibility of incomplete decompression may offset some advantages of minimally invasive approaches. Therefore, the major benefit of endoscopic discectomy may lie in reduced access-related trauma and faster early recovery, whereas durable pain relief and functional improvement depend primarily on complete neural decompression, surgical safety, and appropriate patient selection.
A particularly noteworthy aspect of this investigation is the evaluation of sciatic scoliosis resolution. Sciatic scoliosis is common in ALDH and is generally considered a flexible antalgic posture caused by nerve-root irritation.41 In our study, we found that 36.2% (63 /174) of ALDH patients presented with sciatic scoliosis, an incidence rate consistent with previous studies on scoliosis in this group of people.16 Both procedures were associated with significant improvements in Cobb angle and AVT at final follow-up. PELD and MOFD did not significantly differ in the correction of sciatic scoliosis, which means that the postural imbalance that accompanies ALDH can be reversed to a substantial extent after proper decompression regardless of the type of surgery that is adopted. The restoration of coronal alignment further demonstrates that sciatic scoliosis in ALDH is primarily a compensatory mechanism rather than a fixed structural deformity.
In terms of safety, both PELD and MOFD demonstrated favorable safety profiles. No nerve-root injury, dural tear, facet injury, surgical-site infection, or postoperative segmental instability was observed. Minor symptoms, including transient leg pain or numbness, resolved with conservative treatment. One case of delayed wound healing occurred in Group B and healed after local wound care. It is noteworthy that one case of difficult needle placement due to remarkable vertebral rotation secondary to deformity occurred during the TELD surgery. This indicates that for ALDH patients with significant scoliosis, it is necessary to plan the puncture trajectory before surgery. During follow-up, disc herniation recurrence was observed in both groups. The same-level recurrence rate was 3.6% (3/83) in Group A and 2.2% (2/91) in Group B. Although the rates were slightly higher in Group A, there was no statistically significant difference between the two groups. These recurrence rates are similar to what has been reported in previous studies of adolescent lumbar disc herniation.42,43 These findings suggest that recurrent herniation remains a clinically relevant concern in active adolescent patients, regardless of surgical technique.
This research has several limitations. First, this was a retrospective, non-randomized cohort study. Although a relatively large adolescent cohort was included, surgical procedure selection was based on clinical decision-making and may have been influenced by surgeon experience and preference, introducing potential selection bias and confounding by indication. Future prospective randomized controlled trials with larger sample sizes are needed to validate these findings. Secondly, the limited follow-up duration does not allow for a reliable evaluation of the long-term durability of the surgical outcomes and the actual recurrence rate of ALDH. Therefore, further research with extended follow-up period is required to clarify the long-term efficiency of both surgical procedures, their impact on spinal growth and development, as well as the precise recurrence risk.
Conclusion
For the treatment of ALDH, endoscopic surgery showed minimally invasive advantages, including less blood loss, a smaller incision, and a shorter postoperative hospital stay, while achieving comparable mid-term outcomes in pain relief, functional recovery, and overall safety to traditional fenestration discectomy. These findings suggest that endoscopic surgery may serve as a safe and effective minimally invasive alternative for ALDH patients, although further prospective studies are warranted to validate its long-term efficacy and safety.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Statement
Ethics committee approval by the Committee of Nanjing Drum Tower Hospital (2025-1273-01). The study was performed in accordance with the principles of the Helsinki Declaration of 1964 and its later amendments. All patients provided informed consent for participation in the study and research publication. For patients below the age of 18 years, informed consent was obtained from their parent or legal guardian.
Consent for Publication
We hereby consent to the publication of the paper and confirm that all authors have approved the final version of the manuscript. No part of the paper has been published elsewhere.
Acknowledgments
We appreciate the contribution of all patients, their families, the investigators, and the medical staff.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by fundings for National Natural Science Foundation of China (82502962), fundings for National Natural Science Foundation of China (82302781), fundings for Development Project of Nanjing Science and Technology Commission and Foundation (ZKX24024), and Clinical Trials from Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University (2024-LCYJ-MS-04).
Disclosure
The authors declare no competing interests in this work.
References
1. Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. Lancet. 2021;398(10294):78–13. doi:10.1016/S0140-6736(21)00733-9
2. Deyo RA, Mirza SK. Herniated lumbar intervertebral disk. N Engl J Med. 2016;374(18):1763–1772. doi:10.1056/NEJMcp1512658
3. Ozgen S, Konya D, Toktas OZ, Dagcinar A, Ozek MM. Lumbar disc herniation in adolescence. Pediatr Neurosurg. 2007;43(2):77–81. doi:10.1159/000098377
4. Lee JY, Ernestus RI, Schröder R, Klug N. Histological study of lumbar intervertebral disc herniation in adolescents. Acta Neurochir. 2000;142(10):1107–1110. doi:10.1007/s007010070037
5. Feldman DS, Hedden DM, Wright JG. The use of bone scan to investigate back pain in children and adolescents. J Pediatr Orthop. 2000;20(6):790–795. doi:10.1097/00004694-200011000-00018
6. Epstein JA, Lavine LS. Herniated lumbar intervertebral discs in teen-age children. J Neurosurg. 1964;21:1070–1075. doi:10.3171/jns.1964.21.12.1070
7. Bhatia NN, Chow G, Timon SJ, Watts HG. Diagnostic modalities for the evaluation of pediatric back pain: a prospective study. J Pediatr Orthop. 2008;28(2):230–233. doi:10.1097/BPO.0b013e3181651bc8
8. Battié MC, Videman T. Lumbar disc degeneration: epidemiology and genetics. J Bone Joint Surg Am. 2006;88(2):3–9. doi:10.2106/JBJS.E.01313
9. Papagelopoulos PJ, Shaughnessy WJ, Ebersold MJ, Bianco AJ, Quast LM. Long-term outcome of lumbar discectomy in children and adolescents sixteen years of age or younger. J Bone Joint Surg Am. 1998;80(5):689–698. doi:10.2106/00004623-199805000-00009
10. Zhang J, Zhang W, Yue W, Qin W, Li Z, Xu G. Adolescent lumbar disc herniation: etiology, diagnosis, and treatment options. J Orthop Surg Res. 2025;20(1):605. doi:10.1186/s13018-025-06024-3
11. Silvers HR, Lewis PJ, Clabeaux DE, Asch HL. Lumbar disc excisions in patients under the age of 21 years. Spine. 1994;19(21):2387–2391. discussion 2392. doi:10.1097/00007632-199411000-00002
12. Ferrante L, Mastronardi L, Lunardi P, Puzzilli F, Fortuna A. Lumbar disc herniation in teenagers. Eur Spine J. 1992;1(1):25–28. doi:10.1007/BF00302138
13. Jiang L, Du X, Pan Z, Yuan Y, Battié MC, Wang Y. Lumbar disc herniation in juveniles: a case–control study of MRI characteristics and etiological insights. J Orthopaedic Res. 2023;41(12):2685–2693. doi:10.1002/jor.25598
14. Tu Z, Wang B, Li L, et al. Early experience of full-endoscopic interlaminar discectomy for adolescent lumbar disc herniation with sciatic scoliosis. Pain Physician. 2018;21(1):E63–E70.
15. Zhao Y, Qi L, Ding C, et al. Characteristics of sciatic scoliotic list in lumbar disc herniation. Global Spine J. 2024;14(3):894–901. doi:10.1177/21925682221126123
16. Zhang Y, Li W, Xu L, Jiang E, Qiu Y, Zhu Z. Sciatic scoliosis evolution after lumbar discectomy: a comparison between adolescents and young adults. Pain Physician. 2019;22(5):E457–E465.
17. Haidar R, Ghanem I, Saad S, Uthman I. Lumbar disc herniation in young children. Acta Paediatrica. 2010;99(1):19–23. doi:10.1111/j.1651-2227.2009.01460.x
18. Kuzu Ş, Jawad SR, Canli M, Özüdoğru A. Investigation of efficacy of high and low intensity laser therapy in patients with lumbar disc herniation: a randomized controlled trial. J Med Biol Eng. 2025;45(5):738–744. doi:10.1007/s40846-025-00989-6
19. Kuzu Ş, Canli M, Valamur İ, Özüdoğru A, Alkan H, Hartavi A. Effects of aerobic exercise in addition to core stabilization exercises on functional capacity, physical performance and fall risk in geriatric individuals with chronic non-specific low back pain. BMC Sports Sci Med Rehabil. 2025;17(1):218–228. doi:10.1186/s13102-025-01271-7
20. Karademir M, Eser O, Karavelioglu E. Adolescent lumbar disc herniation: impact, diagnosis, and treatment. BMR. 2017;30(2):347–352. doi:10.3233/BMR-160572
21. Lagerbäck T, Kastrati G, Möller H, Jensen K, Skorpil M, Gerdhem P. MRI characteristics at a mean of thirteen years after lumbar disc herniation surgery in adolescents: a Case-Control Study. JBJS Open Access. 2021;6(4). doi:10.2106/JBJS.OA.21.00081
22. Schoenfeld AJ. Historical contributions from the Harvard system to adult spine surgery. Spine. 2011;36(22):E1477–1484. doi:10.1097/BRS.0b013e3181f2d52c
23. Li WS, Yan Q, Cong L. Comparison of endoscopic discectomy versus non-endoscopic discectomy for symptomatic lumbar disc herniation: a systematic review and meta-analysis. Global Spine J. 2022;12(5):1012–1026. doi:10.1177/21925682211020696
24. Bokov A, Isrelov A, Skorodumov A, Aleynik A, Simonov A, Mlyavykh S. An analysis of reasons for failed back surgery syndrome and partial results after different types of surgical lumbar nerve root decompression. Pain Physician. 2011;14(6):545–557. doi:10.36076/ppj.2011/14/545
25. Majeed SA, Vikraman CS, Mathew V, AT S. Comparison of outcomes between conventional lumbar fenestration discectomy and minimally invasive lumbar discectomy: an observational study with a minimum 2-year follow-up. J Orthop Surg Res. 2013;8(1):34. doi:10.1186/1749-799X-8-34
26. Fritsch EW, Heisel J, Rupp S. The failed back surgery syndrome: reasons, intraoperative findings, and long-term results: a report of 182 operative treatments. Spine. 1996;21(5):626–633. doi:10.1097/00007632-199603010-00017
27. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–56.
28. Li T, Zhang J, Ding Z, Jiang Q, Ding Y. Percutaneous endoscopic lumbar discectomy versus open fenestration discectomy for lumbar disc herniation: a retrospective propensity score-matched study with more than 5 years of follow-up. J Orthop Surg Res. 2024;19(1):753. doi:10.1186/s13018-024-05239-0
29. Li Q, Zhou Y. Comparison of conventional fenestration discectomy with Transforaminal endoscopic lumbar discectomy for treating lumbar disc herniation:minimum 2-year long-term follow-up in 1100 patients. BMC Musculoskelet Disord. 2020;21(1):628. doi:10.1186/s12891-020-03652-0
30. Tang Y, Li H, Qin W, et al. Comparison of percutaneous endoscopic interlaminar discectomy and conventional open lumbar discectomy for L4/5 and L5/S1 double-segmental lumbar disk herniation. J Orthop Surg Res. 2023;18(1):950. doi:10.1186/s13018-023-04361-9
31. Zheng S, Zhao Q, Hu Z, et al. Large-Channel interlaminar endoscopic discectomy for highly migrated lumbar disc herniation: effectiveness and safety. JPR. 2025;18:3821–3832. doi:10.2147/JPR.S537181
32. Zhu X, Zhao Y, Liu K, Zhang Y, Cheng L. Clinical outcomes of fenestration discectomy and iLESSYS-Delta interlaminar endoscopic system for treatment of LDH: a single-center retrospective cohort study. Sci Rep. 2024;14(1):20087. doi:10.1038/s41598-024-70973-8
33. Choi G, Lee SH, Raiturker PP, Lee S, Chae YS. Percutaneous endoscopic interlaminar discectomy for intracanalicular disc herniations at L5-S1 using a rigid working channel endoscope. Neurosurgery. 2006;58(1 Suppl):ONS59–68. discussion ONS59-68. doi:10.1227/01.neu.0000192713.95921.4a
34. Wang L, Guo X, Song Z, Tang H, Guo H, Li Y. Comparison of perioperative blood loss of three different posterior nonfusion decompression operations for single-segment lumbar disc herniation. Front Neurol. 2025;16:1551742. doi:10.3389/fneur.2025.1551742
35. Phan K, Xu J, Schultz K, et al. Full-endoscopic versus micro-endoscopic and open discectomy: a systematic review and meta-analysis of outcomes and complications. Clin Neurol Neurosurg. 2017;154:1–12. doi:10.1016/j.clineuro.2017.01.003
36. Zhang B, Liu S, Liu J, et al. Transforaminal endoscopic discectomy versus conventional microdiscectomy for lumbar discherniation: a systematic review and meta-analysis. J Orthop Surg Res. 2018;13(1):169. doi:10.1186/s13018-018-0868-0
37. Alexander N, Gardocki R. Awake transforaminal endoscopic lumbar discectomy in an ambulatory surgery center: early clinical outcomes and complications of 100 patients. Eur Spine J. 2023;32(8):2910–2917. doi:10.1007/s00586-023-07786-2
38. Rasouli MR, Rahimi-Movaghar V, Shokraneh F, Moradi-Lakeh M, Chou R. Minimally invasive discectomy versus microdiscectomy/open discectomy for symptomatic lumbar disc herniation. Cochrane Database Syst Rev. 2014;2014(9):CD010328. doi:10.1002/14651858.CD010328.pub2
39. Teli M, Lovi A, Brayda-Bruno M, et al. Higher risk of dural tears and recurrent herniation with lumbar micro-endoscopic discectomy. Eur Spine J. 2010;19(3):443–450. doi:10.1007/s00586-010-1290-4
40. Gibson JNA, Subramanian AS, Scott CEH. A randomised controlled trial of transforaminal endoscopic discectomy vs microdiscectomy. Eur Spine J. 2017;26(3):847–856. doi:10.1007/s00586-016-4885-6
41. Suk KS, Lee HM, Moon SH, Kim NH. Lumbosacral scoliotic list by lumbar disc herniation. Spine. 2001;26(6):667–671. doi:10.1097/00007632-200103150-00023
42. Lee DY, Ahn Y, Lee SH. Percutaneous endoscopic lumbar discectomy for adolescent lumbar disc herniation: surgical outcomes in 46 consecutive patients. Mt Sinai J Med. 2006;73(6):864–870.
43. Feng F, Zhao R, Dong H, et al. Full-endoscopic lumbar discectomy for lumbar disc herniation in young adults: 199 consecutive cases treated by a single surgeon with a mean 3.7-year follow-up. J Neurosurg Spine. 2024:1–9. doi:10.3171/2024.4.SPINE231011
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.