Back to Journals » Advances in Medical Education and Practice » Volume 13
Perceptions and Motivation Regarding Performing Research in Physicians Specializing in Care for Older Adults Involved in a Mandatory Evidence-Based Medicine Training Study: A Mixed-Methods Study
Authors van der Steen JT ![]() , Tong WH
, Tong WH ![]() , Groothuijse J, Ommering BWC
, Groothuijse J, Ommering BWC ![]()
Received 10 November 2021
Accepted for publication 23 February 2022
Published 8 March 2022 Volume 2022:13 Pages 217—224
DOI https://doi.org/10.2147/AMEP.S348735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Jenny T van der Steen,1,2 Wing H Tong,1,3 Janneke Groothuijse,1 Belinda WC Ommering4
1Department of Public Health and Primary Care (PHEG), Leiden University Medical Center, Leiden, the Netherlands; 2Department of Primary and Community Care, Radboud university medical center, Nijmegen, the Netherlands; 3Argos Zorggroep “DrieMaasStede”, Center for Specialized Geriatric Care, Schiedam, the Netherlands; 4Center for Innovation in Medical Education, Leiden University Medical Center, Leiden, the Netherlands
Correspondence: Jenny T van der Steen, Leiden University Medical Center (LUMC), Department of Public Health and Primary Care (PHEG), Building 3, Hippocratespad 21, PO Box 9600, Leiden, 2300 RC, the Netherlands, Email [email protected]
Purpose: Evidence underpinning treatment of older persons with complex conditions is often sparse, and involving more early career physicians committed to optimizing care for older adults may help increase a relevant evidence base. We examined perception of and motivation to conduct research in physicians (residents) specializing in care of older adults.
Subjects and Methods: Residents of an academic medical centre in the Netherlands enrolled in a 3-year training programme. The programme includes a mandatory evidence-based medicine (EBM) training study on pain and discomfort in cognitively impaired nursing home patients, in which residents perform their research over the 3-year duration of the programme. We employed a mixed-methods design with survey and qualitative interviews (December 2019–April 2020). The survey included validated scales with agreement response options rated 1– 7. Qualitative interviews were underpinned by interpretative phenomenological analysis.
Results: Of 38 invited residents, 23 (15 females) participated. The mean score on perceptions of research was 4.1 (SD 0.8); on intrinsic motivation 4.8 (SD 1.0); on extrinsic motivation 4.3, with a higher SD of 1.4. Eight interviews also showed diversity in the extent to which residents felt equipped to conduct the mandatory EBM training study, and research more generally, which was related to previous experiences performing research. The residents generally did not anticipate conducting research themselves despite recognizing the benefits of training in research.
Conclusion: Perceptions and motivation of the residents specializing in care of older people to conduct research, although considered relevant to their practice, were not very positive. The study results in recommendations to motivate physicians in geriatrics training to conduct research, eg through personalized boosting of self-efficacy. This is crucial to motivate future physicians to contribute to research relevant to older people in more ways than just delivering data for research conceived by (non-clinical) researchers.
Keywords: nursing home, medical education, core competences, curriculum, research activities
Introduction
In long-term care, evidence for treatment that meets treatment goals is often sparse or less applicable to older adults with multimorbidity,1–3 except perhaps for trialled novel stand-alone dementia-care interventions.4 Physicians who are skilled in research in long-term care and older populations can help move the field forward in terms of professionalization and enhanced quality of care, contributing to a relevant evidence base.
Indeed, physician-scientists are well-positioned to conduct scientifically innovative translational research for patient benefit, as they bridge the gap between clinical practice and science while both fields undergo increased specialization.5,6 Residency research may thus help promote evidence-based medicine and quality patient care, and also enhance residents’ analytical skills and develop critical thinking.7 Further, conducting research contributes to residents’ ability to understand research, which in turn supports evidence-informed decision making in current and future practice, for instance through increased capacity to critically appraise trial effects.8,9
To reinforce motivation,10 it is important to understand medical residents’ perceptions and motivation regarding engaging in research. Recent research among medical students suggests that intrinsic motivation relates to actual research involvement, while extrinsic motivation does not.11 We examine perception and motivation regarding conducting research of novice physicians specializing in care for older adults, when exposed to the mandatory conduct of research as part of evidence-based medicine (EBM) education.
Methodology
Study Design
Mixed-methods study with survey (December 2019) and subsequent qualitative interviews (January–April 2020). We adhered to the General Data Protection Regulation procedures (EU 2016/679). The Netherlands Association for Medical Education (NVMO) approved the study protocol (16 October 2019; number 2019.7.7). The participants provided informed consent, part of which was consent to publish anonymized responses.
Setting
The study was conducted in the Netherlands, where so-called “elderly care” (older adults) medicine represents an important specialization.12 The 3-year resident training programme comprises practical training and a 1-day-a-week training at the University. Physicians should be able to adequately interpret research results,13 but the Leiden University Medical Center curriculum additionally features a mandatory EBM training study14 to acquire competencies to plan and conduct research (more information in Supplementary Box S1). The training study covers the breadth of contributing to a fixed, but broad, data collection on pain and discomfort in the cognitively impaired nursing home patients under their care, and group work with two to four peers. Residents generate a research question, perform analyses, and report results in an article and paper presentation in the third year. Most classes for the training study are scheduled in the first year.
Participation
We invited residents of three groups in year 1 or 2 of their 3-year certification curriculum. We explained the study and provided informed consent forms to return at the residents’ convenience, with options to participate in the survey, an interview, or both. We e-mailed two reminders and teachers reminded residents during classes.
Survey
The survey comprised open-ended and closed items, and included perception, intrinsic and extrinsic motivation for research scales with agreement rated 1–7 based on Self-Determination Theory15 validated in medical students.11 We adapted phrasing for residents specializing in care for older adults where needed (Supplementary Tables S1–S3).
Interviews
Semi-structured individual interviews with residents were conducted by WHT (male PhD and resident of non-invited group) and HJAS (female postdoctoral fellow, psychologist) guided by an interview guide (Supplementary Box S2). To fit with our aim to understand people’s experiences, “interpretative phenomenological analysis” (IPA) underpinned the design, conduct and analysis of the qualitative interviews.16,17 The “phenomenon” under study was the experience of the development of a professional identity, with a focus on perceptions and motivation regarding research. “Interpretation” referred to the meaning making of residents reflecting on research and the EBM training study in particular.
Analysis
We calculated mean item and total scores for the scales, substituting with item means if less than 30% missed. We compared scores between interviewees and non-interviewees with a t-test to verify possible selective participation. Quantitative data were analysed using IBM SPSS Statistics version 25 for Windows (2017). JTvdS, WHT and JG coded open-ended survey items inductively.
Before the interview, the interviewer reviewed the respondent’s completed survey to inspire questions additional to those in the interview guide, and afterwards noted impressions in a log. The interviews were audio recorded and transcribed verbatim; the researchers verified accuracy of the transcripts. JTvdS started stepwise analysis with gaining an understanding of individual experiences,16 focusing on instances of reflection on what experiences meant to the resident, marking transcripts and writing memos on each interview. Next, narratives of individuals were linked to common points of reflections, which were linked to striking quotations marked in earlier phases. In case of doubts regarding meaning making, the audio recording was listened to again. Finally, text snippets as large as quotations were coded around the central points throughout the full transcripts. JG analyzed two interviews independently and discussed meanings with JTvdS. Further, WHT and JG provided feedback on interim analyses, which enriched the double hermeneutics of meaning making.
Results
Of 38 invited residents, 23 (61%) completed the survey; 18 were in the first year of their training, and five in the second year. Mean age was 31.7 years (SD 6.6) and 15 (65%) were female.
The mean score on perceptions of research was 4.1 (SD 0.8), on intrinsic motivation 4.8 (SD 1.0) and on extrinsic motivation for research 4.3 with a higher SD of 1.4 (Table 1). The item scoring lowest across scales referred to capability to conduct research independently being necessary (mean 3.1, SD 1.2). Further, “I think that doing research could help me to get a good job in the future” scored low (mean 3.4, SD 1.8; extrinsic motivation scale), and on the perceptions scale, “a scientific educational programme is important for me” (mean 3.7, SD 1.1). The item scoring highest by far (≥5) across scales was the only item not referring to science, “I like solving puzzles and problems” (intrinsic motivation, mean 5.8, SD 0.8). The open-ended comments indicated a balance of positive and negative aspects of the EBM training study; none of the 23 residents provided exclusively positive or negative feedback. Most criticized was the organization of the training study, with instructions being unclear, little protected time and fragmented classes making dedication to doing research very difficult. The content, expressing interest in increasing EBM competencies, and dedication of staff were appreciated the most.
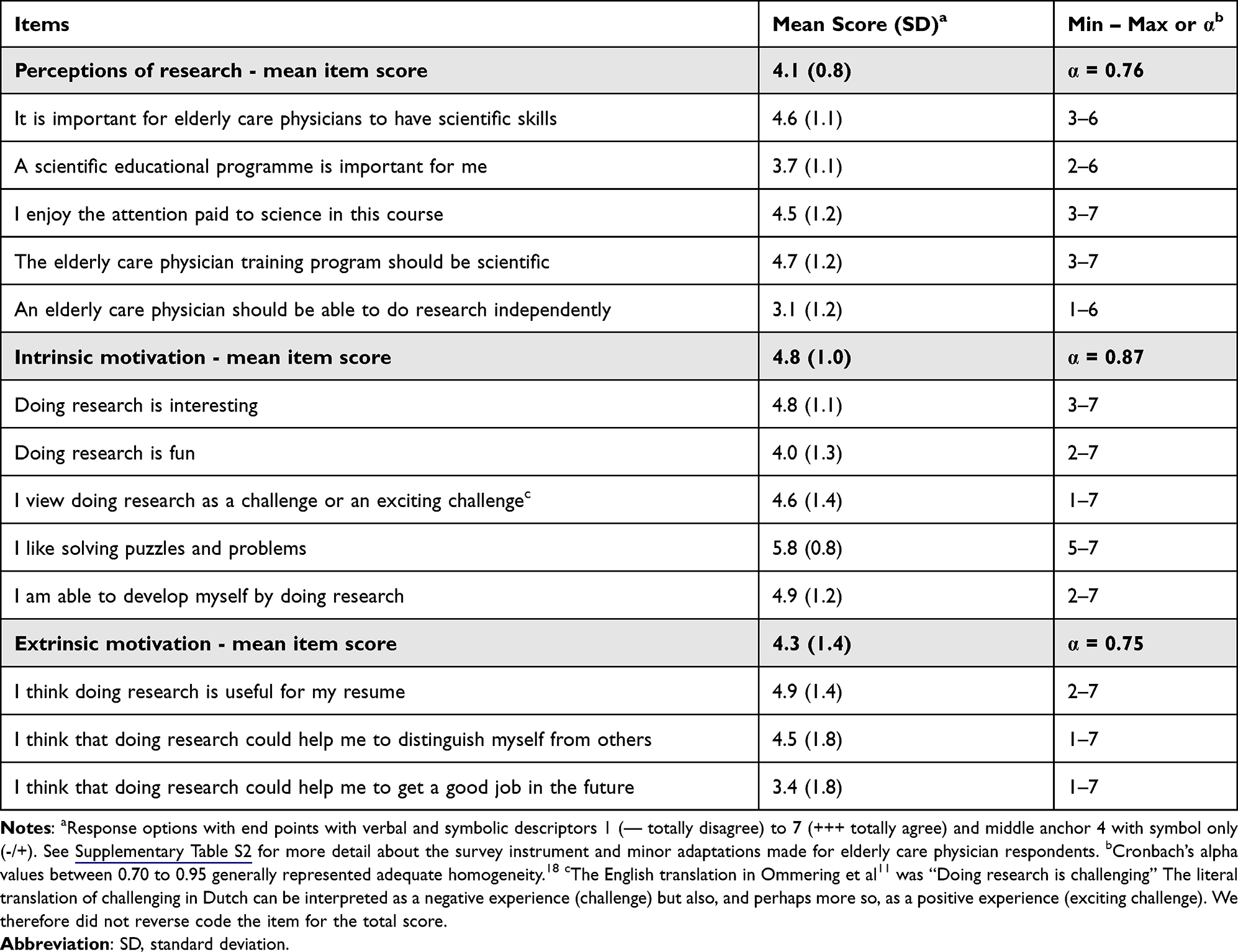 |
Table 1 Perceptions of Research and Motivation to Conduct Research Item Scores (N=23 Residents “Elderly Care” Medicine) |
Nine residents consented to an interview, and we interviewed eight (five females). Interviewee motivation scale scores were similar but perceptions were more favourable (mean 4.6 SD 0.7) compared to non-interviewees (mean 3.9 SD 0.8; P=0.045). The interviews lasted 31–50 minutes; five were face-to-face; in their nursing home (4) or at the university (1) according to their preference, and the last 3 interviews were by Zoom due to COVID-19 measures. Residents’ research experience was highly variable, ranging from almost absent to a PhD (exempt from the training study but reflecting on own and communicated peer experiences). Expectations regarding the EBM curriculum (burden, difficulty, benefits) also varied.
Key experiences regarding the EBM training study included enjoying the study and learning experiences while recognizing its pragmatic approach, and frustration about slow progress. Developing an exciting research question with no overly obvious answer and relevant to practice was described as an enjoyable experience. The fixed data collection reduced the choice of research questions, but it also offered a framework appreciated by the most inexperienced residents. Structured detailed observation of patient behaviour for data collection was mentioned as an educational experience directly relevant to practice. Navigating peer research group dynamics was perceived as educational, even if frustrating due to slower than aimed for progress over the years. The residents commonly related inefficient work and learning experience to lack of protected time, problems scheduling classes and peer group work. They found that maintaining focus is required for their research to progress.
There was great diversity in how equipped residents felt to conduct the EBM training study and research more generally. The meaning they attached to their experiences emerged through the lens of previous experiences conducting research themselves or collecting data for others. The interview itself was instrumental in making sense of their experiences; several residents reflected on it when concluding the interview (Box 1, quote a).
The residents considered the value they attached to research personally, in clinical work and career. Their reflections centred around five issues (Box 1, quotes b–j).
(1) Self and medical practice ideals. The residents would become an MD who navigates complexities creatively, a communicative team player engaging in long-term relationships.
(2) Value of research for my profession. They perceived the evidence underpinning their profession as rather weak and saw a need to enhance the evidence to support decisions in complex cases.
(3) Value of EBM and research training for my own practice. The residents felt they needed to master the EBM way of thinking and update their knowledge. However, they felt that communication skills mattered more, as excellent communication is what really makes a good doctor.
(4) (Not) anticipating conducting research myself. The residents generally would not do research themselves in the near future, as they prioritized becoming a good MD. Doing research well would take too much time; they might reconsider later, if allowed by academic practice environment, support and private circumstances.
(5) (Variable) self-efficacy to practice EBM and to conduct research. Beliefs varied greatly depending on earlier exposure and experiences with research.
Trade-offs and choices of time investment emerged from the residents’ reflections, regardless of self-efficacy. They were strongly motivated to use highly valued and enjoyable creative teamwork skills for the purpose of becoming a good doctor rather than for the purpose of doing research. Research was perceived to take much competing time relative to its benefits. One resident with much research experience explained it dominates life, as do responsibilities for long-standing relationships in nursing home practice compared to hospital practice (Box 1, quote k). Although they recognized benefits of understanding research for the complex clinical decision-making and communication with family and other disciplines they encounter in practice, they would therefore not engage in research themselves.
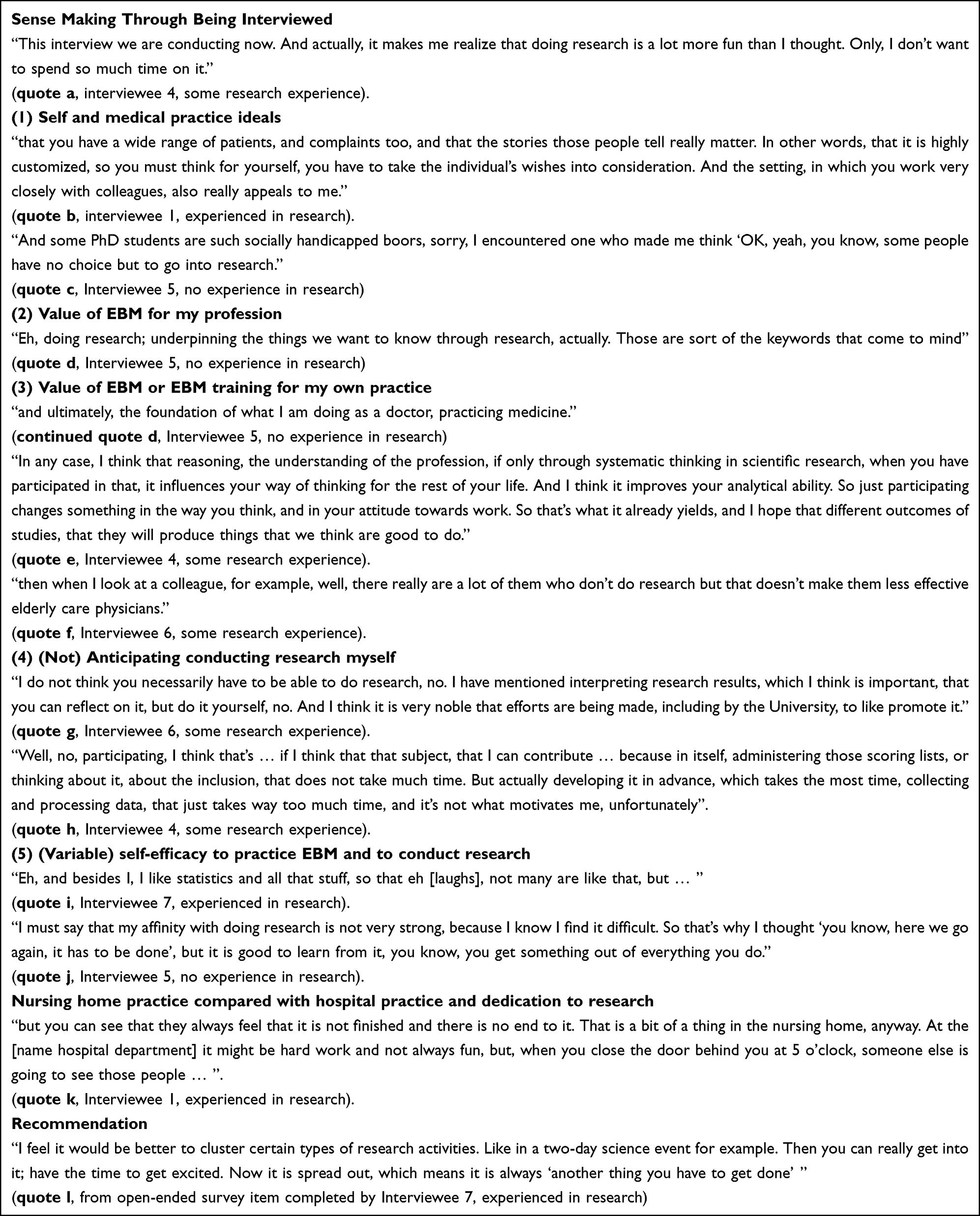 |
Box 1 Citations from Interviews and Open-Ended Survey Questions |
Discussion
Perceptions of research were not very favourable, motivation to conduct research was modest, and self-efficacy highly variable among residents specializing in care for older adults involved in a training study covering all phases of conducting research across their 3-year programme. The residents perceived (quantitative) research as distant from empathic care practice. Protected time and focus needed for research competed with their motivation to learn to become a good physician, which they prioritized. However, they valued understanding research as it directly improved care for their patients.
Table 2 summarizes more general lessons from our mixed-methods study that may help in setting up a training study. The main lessons, such as personalizing research (recommendation 2),5 resonate with research among medical students and physician-scientists.
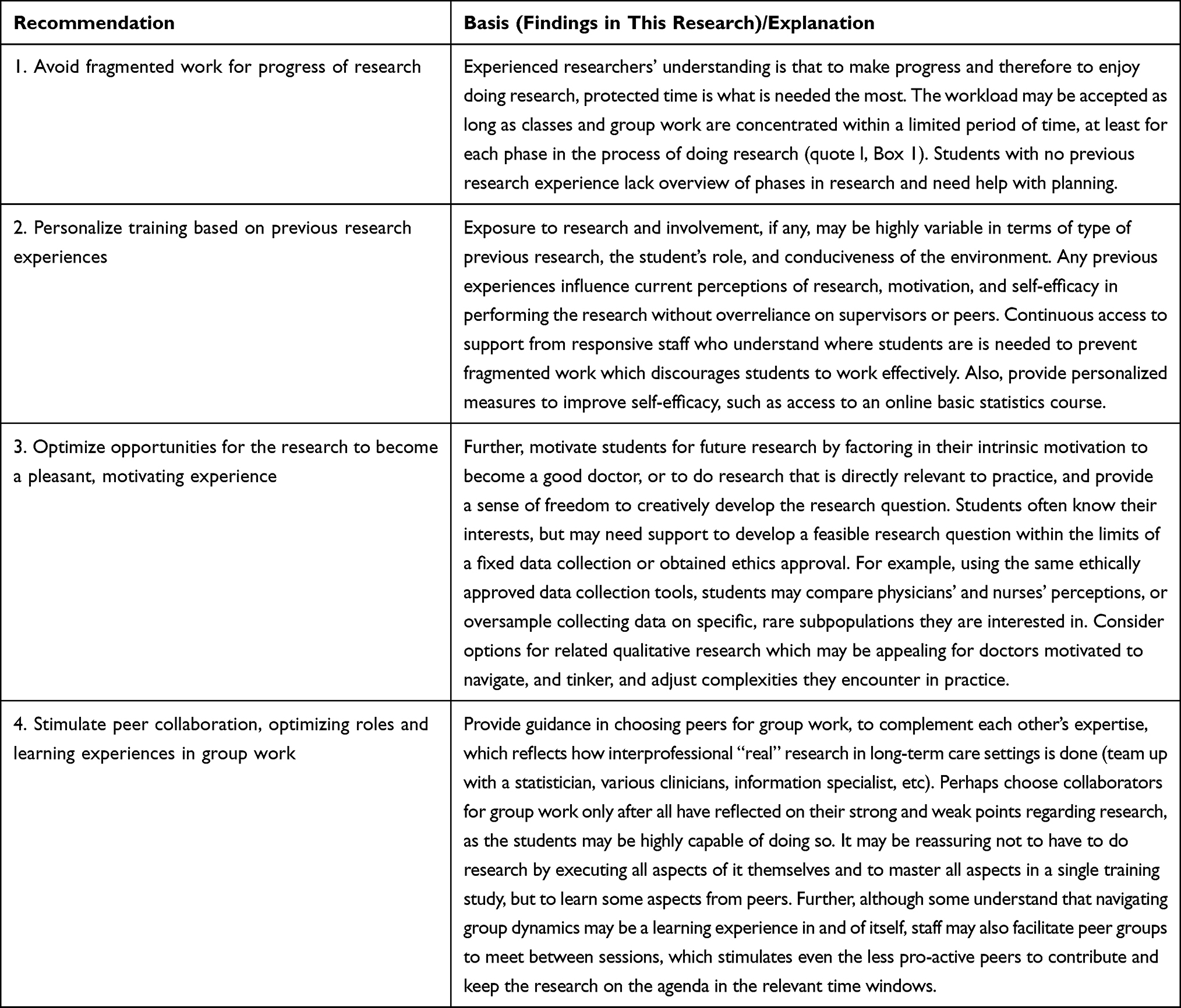 |
Table 2 Recommendations for Training Studies for Those Specializing in Medical Care for Older Persons or in Long-Term Care Settings |
The residents practiced in settings where nursing home staff include physicians, which may explain their perception of a good physician foremost as an excellent communicator taking a central position in the web of long-standing relationships with colleagues, nursing staff and family. This finding, along with low extrinsic motivation for research to benefit careers, may not translate fully to ambulatory geriatrics or acute care settings. Other findings on perception and motivation to conduct research may relate to interest in navigating complexities in caring for older persons, diversity in residents’ backgrounds and earlier exposure to research, and the design of the educational programme around the particular EBM training study.
Connecting research to practice is imperative7,19 (recommendation 3) and also motivated first-year medical students of the same academic centre,20 but the residents’ perceptions of research and motivation were lower.11 We did not quantify self-efficacy, but the interviews demonstrated that previous experiences strongly coloured confidence in capacity to conduct research. This is consistent with Social Cognitive Career Theory and research in medical education which asserts that early experiences such as successes shape and influence self-efficacy and positive outcome expectations, and training programmes must therefore accommodate differential backgrounds.21 Further, Self-Determination Theory suggests that intrinsic motivation (doing research out of interest) is enhanced by feelings of competence, by offering autonomy and feelings of (social) connectedness.15 Indeed, a mixed-methods study found that competence, autonomy and relatedness all motivated medical students to do research, and completing compulsory projects–especially when conducted in groups (recommendation 4)–led to effective learning about research and higher future research intentions.19
The interviews and IPA approach offered a rich understanding of experiences of the residents who are used to reflecting on their learning experiences and group dynamics; indeed, phenomenological research is suitable with more eloquent individuals.17,22 The residents also disclosed experiences of their peers about local supervisors in the nursing home not offering protected research time, a well-known barrier to combining research with clinical and educational duties (recommendation 1).5–7,19,23 Interviewing and analysis of interviews was conducted by researchers with diverse backgrounds, which helped appreciate rich responses, including in one case brief responses and the interviewer reflecting on difficulty connecting.
Our study was limited to experiences in an early phase of a particular training study, and further longitudinal research should quantify self-efficacy (Supplementary Table S3). We believe saturation was reached and eight interviews falls within a typical range for IPA analysis of experiences of 4–10 individuals.16 The interviews were mostly exploratory24 although conducted in parallel as in a convergent design.25 IPA’s flexibility lends itself to combining with findings obtained within other paradigms.22
Conclusion
Our mixed-methods study informed specific improvements. Building on previous research experience and empowering residents to conduct research, emphasizing creative, non-linear aspects of doing research relevant to practice is key to favourable experiences which motivate future physicians in long-term care to contribute to, but also to conduct research themselves.
Data Sharing Statement
Supplementary Materials are available: Boxes S1 and S2 and Tables S1–S3. De-identified survey data are available from the authors upon reasonable request.
Acknowledgments
We thank the medical residents for participating in the research, and Brian Yothers, BSc for his assistance. We gratefully acknowledge Hanneke JA Smaling, PhD for interviewing. This work was supported by the Department of Public Health and Primary Care, and the Center for Innovation in Medical Education, Leiden University Medical Center, Leiden, the Netherlands. Belinda WC Ommering is currently affiliated with HU University of Applied Sciences Utrecht, Utrecht, the Netherlands.
Disclosure
The authors report no financial, personal or any other potential conflicts of interest in this work. This work was supported by Leiden University Medical Center (LUMC), Leiden, the Netherlands. The sponsor of the study, LUMC, had no role in the design, methods, subject recruitment, data collections, analysis or preparation of paper.
References
1. Smith SM, Wallace E, O’Dowd T, et al. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2016;3(3):CD006560. doi:10.1002/14651858.CD006560.pub3
2. Muth C, Blom JW, Smith SM, et al. Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: a systematic guideline review and expert consensus. J Intern Med. 2019;285(3):272–288. doi:10.1111/joim.12842
3. Damarell RA, Morgan DD, Tieman JJ. General practitioner strategies for managing patients with multimorbidity: a systematic review and thematic synthesis of qualitative research. BMC Fam Pract. 2020;21(1):131. doi:10.1186/s12875-020-01197-8
4. Pham T, Bugeja L, Holmes A, et al. Systematic review of randomized controlled trials in Australian nursing homes from 2000 to 2018. J Am Geriatr Soc. 2021;69(4):1086–1093. doi:10.1111/jgs.16944
5. DeLuca GC, Ovseiko PV, Buchan AM. Personalized medical education: reappraising clinician-scientist training. Sci Transl Med. 2016;8(321):321fs2. doi:10.1126/scitranslmed.aad0689
6. Harding CV, Akabas MH, Andersen OS. History and outcomes of 50 years of physician-scientist training in medical scientist training programs. Acad Med. 2017;92(10):1390–1398. doi:10.1097/ACM.0000000000001779
7. Rothberg MB. Overcoming the obstacles to research during residency: what does it take? JAMA. 2012;308(21):2191–2192. doi:10.1001/jama.2012.14587
8. Ommering BWC, Haramati A, de Jong PGM. Teaching to develop scientific engagement in medical students. In: Huggett KN, Quesnelle KM, Jeffries WB, editors. An Introduction to Medical Teaching: The Foundation of Curriculum Design, Delivery, and Assessment.
9. Vandiver DM, Walsh JA. Assessing autonomous learning in research methods courses: implementing the student-driven research project. Act Learn High Educ. 2010;11(1):31–42. doi:10.1177/1469787409355877
10. Amgad M, Man Kin Tsui M, Liptrott SJ, et al. Medical student research: an integrated mixed-methods systematic review and meta-analysis. PLoS One. 2015;10(6):e0127470. doi:10.1371/journal.pone.0127470
11. Ommering BWC, van Blankenstein FM, Wijnen-Meijer M, et al. Fostering the physician-scientist workforce: a prospective cohort study to investigate the effect of undergraduate medical students’ motivation for research on actual research involvement. BMJ Open. 2019;9(7):e028034. doi:10.1136/bmjopen-2018-028034
12. Koopmans RT, Lavrijsen JC, Hoek JF, et al. Dutch elderly care physician: a new generation of nursing home physician specialists. J Am Geriatr Soc. 2010;58(9):1807–1809. doi:10.1111/j.1532-5415.2010.03043.x
13. Richardson D, Oswald A, Lang E, et al., editors. The CanMEDS 2015 Scholar Expert Working Group Report. Ottawa:The Royal College of Physicians and Surgeons of Canada; 2014. Report.
14. van der Steen JT, Klapwijk MS, Achterberg WP. Palliative care and impact of the COVID-19 pandemic on nursing home residents with dementia. Riv It Cure Palliative. 2020;22(3):129–139. doi:10.1726/3439.34275
15. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi:10.1037//0003-066x.55.1.68
16. Smith JA, Flowers P, Larkin M. Interpretative Phenomenological Analysis: Theory, Method and Research. Sage Publications; 2009:
17. Tuffour I. A critical overview of interpretative phenomenological analysis: a contemporary qualitative research approach. J Healthc Commun. 2017;2(4):52. doi:10.4172/2472-1654.100093
18. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
19. Rosenkranz SK, Wang S, Hu W. Motivating medical students to do research: a mixed methods study using self-determination theory. BMC Med Educ. 2015;15:95. doi:10.1186/s12909-015-0379-1
20. Ommering BWC, Wijnen-Meijer M, Dolmans DH, et al. Promoting positive perceptions of and motivation for research among undergraduate medical students to stimulate future research involvement: a grounded theory study. BMC Med Educ. 2020;20(1):204. doi:10.1186/s12909-020-02112-6
21. Bakken LL, Byars-Winston A, Wang M-F. Viewing clinical research career development through the lens of social cognitive career theory. Adv Health Sci Educ Theory Pract. 2006;11(1):91–110. doi:10.1007/s10459-005-3138-y
22. Noon EJ. Interpretive phenomenological analysis: an appropriate methodology for educational research? J Perspect Appl Acad Pract. 2018;6(1):75–83. doi:10.14297/jpaap.v6i1.304
23. Chang Y, Ramnanan CJ. A review of literature on medical students and scholarly research: experiences, attitudes, and outcomes. Acad Med. 2015;90(8):1162–1173. doi:10.1097/ACM.0000000000000702
24. Mayoh J, Onwuegbuzie AJ. Toward a conceptualization of mixed methods phenomenological research. J Mix Methods Res. 2015;9(1):91–107. doi:10.1177/1558689813505358
25. Curry LA, Krumholz HM, O'Cathain A, et al. Mixed methods in biomedical and health services research. Circ Cardiovasc Qual Outcomes. 2013;6(1):119-123. doi:10.1161/circoutcomes.112.967885
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.