Back to Journals » Patient Preference and Adherence » Volume 16
Perceptions and Motivating Factors Regarding COVID-19 Vaccination in Latinx Older Adults in Chicago: A Local, Qualitative Perspective
Authors Light SW ![]() , Pack A
, Pack A ![]() , Vela A, Bailey SC, Zuleta A, O'Conor R, Wolf MS
, Vela A, Bailey SC, Zuleta A, O'Conor R, Wolf MS
Received 17 June 2022
Accepted for publication 9 August 2022
Published 25 August 2022 Volume 2022:16 Pages 2321—2333
DOI https://doi.org/10.2147/PPA.S378081
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sophia W Light,1 Allison Pack,1 Alyssa Vela,2 Stacy C Bailey,1 Andrea Zuleta,1 Rachel O’Conor,1 Michael S Wolf1
1Division of General Internal Medicine, Northwestern University Feinberg School of Medicine, Chicago, IL, USA; 2Department of Surgery, Northwestern University Feinberg School of Medicine, Chicago, IL, USA
Correspondence: Sophia W Light, Center for Applied Health Research on Aging (CAHRA), Division of General Internal Medicine, Northwestern University Feinberg School of Medicine, 750 N. Lake Shore Drive, 10th Floor, Chicago, IL, 60611, USA, Tel +1(312)503-5015, Email [email protected]
Purpose: Historically marginalized communities disproportionately impacted by the pandemic are demonstrating lower uptake of COVID-19 vaccines. To facilitate the development of culturally tailored, language concordant educational materials promoting COVID-19 vaccination, we first explored older Latinx adults’ awareness, attitudes, and beliefs about COVID-19 vaccines and factors involved in vaccination decisions within their communities.
Patients and Methods: Individual, semi-structured interviews were conducted with 15 participants who self-identified as Latinx/Hispanic, aged 50 and older, and living in Chicago. Eight interviews were conducted in English and seven in Spanish. Thematic analysis was used to analyze participants’ responses.
Results: Participants revealed four key factors influencing vaccination decisions: 1. protecting oneself and loved ones (against COVID-19 (n=14), or from perceived dangers of the vaccine (n=9)); 2. trust in authorities (trusting information (n=9), or worrying the vaccine is being manipulated (n=5)); 3. access and availability (gratitude to live in a country where vaccines are available (n=5), or fear of going to vaccination sites due to immigration and insurance status (n=4)); and 4. Employment and semblance of normalcy (vaccination to create opportunities (n=6), or concern about missing out due to side effects (n=9)).
Conclusion: Our findings illuminate key factors influencing decisions for COVID-19 vaccination among Latinx older adults in Chicago. Vaccination information aiming to increase vaccination rates among this important population may benefit from leveraging collective pronouns and spirituality, language concordance, low-tech options, building trust, and addressing insurance and immigration doubts. Next steps include developing educational materials based on these themes, followed by dissemination and evaluation. Lessons learned may be of interest to public health experts responding to the ongoing pandemic and other public health crises experienced by historically marginalized communities.
Keywords: qualitative, COVID-19 vaccines, COVID-19, Latinx, older adult
Introduction
The impact of the COVID-19 pandemic in the United States (US) has been drastic and far-reaching, especially for older adults and those with underlying health conditions, who are at greater risk for infection as well as adverse outcomes if infected.1–3 Moreover, the pandemic has disproportionately affected historically marginalized racial and ethnic groups, including Black, Hispanic/Latinx (hereafter referred to as Latinx), Asian, and Native American/Indigenous populations.4 Due to longstanding structural and societal inequities that have affected economic opportunity, access to healthcare, and overall health status, many such communities have been placed at greater risk of harm from the very onset of the outbreak.5,6 Further, individuals who are at the intersection of these two disproportionately affected communities, being of older age and members of historically marginalized communities, may be at a multiplicative risk for adverse consequences.7
Widespread access and timely uptake of preventative vaccines is vital to halting the spread of the COVID-19 virus and minimizing the consequences of new variants.8,9 Vaccine hesitancy, defined as either the refusal of or the delay in the acceptance of vaccination despite availability,10 threatens not only to attenuate progress made in the fight against COVID-19, but also to exacerbate health disparities. Recent cross-sectional surveys have demonstrated the relatively lower rates of COVID-19 vaccine acceptance in historically marginalized racial and ethnic communities compared to predominantly White communities in the US.11,12 Importantly, vaccination rates may be influenced by mistrust of the medical system, due to a long history of unethical research practices on historically marginalized racial and ethnic groups, as well as generations of exposure to and anticipation of discrimination.13 In addition, logistical challenges, including transportation barriers or an inability to take time off work, can further augment disparities in vaccine uptake.14,15 Moreover, language is among the most important factors influencing whether health information is understood and whether individuals, particularly Latinx adults, can access care. Language-concordant care is consistently associated with improved health outcomes; yet amid the COVID-19 pandemic, decreased access to in-person health services and medical interpreters has exacerbated existing challenges.16 Recent surveys suggest that Latinx individuals are approximately 1.5 times more likely than non-Latinx Whites to report vaccine hesitancy.11,12,17 This is of particular concern given that – due to myriad social determinants of health – Latinx individuals are 1.5 times more likely to be infected, 2.2 times more likely to be hospitalized, and 1.8 times more likely to die from COVID-19 compared to non-Latinx White individuals.4
To our knowledge, no published studies have specifically focused on vaccine acceptance and promotion among Latinx older adults, who represent an important group that has been disproportionately affected by the pandemic. Of note, by 2060, nearly 1 in 4 individuals in the US is projected to be 65 years of age or older, and Latinx individuals – already the largest ethnic group in the US – are projected to make up 29% of the population, further underscoring the significance of this group.18 As stated in a recent Lancet Commission publication, sustained, tailored efforts to reach and engage all US communities about COVID-19 vaccination is crucial to disrupt disparities in morbidity and mortality.19 Prior research has demonstrated that public health messaging campaigns can have differential efficacy by race/ethnicity and age group,20,21 and health messages are likely to be more effective when conceptualizing historically marginalized communities as heterogeneous and considering multiple dimensions of social identity at once.19,22–24 Therefore, it is important to engage with local community members in order to guide messaging that is culturally attuned to the unique intersection of their unique, interacting, multiple identities – being of older age and of Latin American decent. Understanding stakeholders’ experiences via in-depth interviews can inform ongoing efforts to promote vaccine uptake by identifying current gaps and integrating real-life, personalized perspectives into the development of materials. Thus, we conducted a qualitative study designed to inform linguistically- and culturally-tailored quality improvement and health communication efforts to enhance COVID-19 vaccine uptake at federally qualified health centers in Chicago. Conclusions and recommendations may be of interest to public health experts responding to the ongoing pandemic and other public health crises, with regards to this important subset of the US population.
Materials and Methods
The current study employed in-depth, semi-structured interviews, guided by the socio-ecological model (SEM).25 The SEM posits that individuals’ behaviors are determined by multiple, interacting levels of influence within a complex set of ecological environments, including individual, interpersonal, organizational, community, and public policy;25 this framework was thus used to inform interview question development and thematic analysis in order to identify multiple levels of influence for individual stakeholders.26 Recruitment and data collection occurred between May and July 2021 in Chicago, Illinois. Participants were eligible if they (a) were 50 years of age or older, (b) self-identified as Latinx/Hispanic, (c) were fluent in Spanish and/or English, and (d) had access to video conferencing technology and/or a phone. Participants were recruited via purposive sampling methods, with potential participants identified through social media posts, flyers and contacting participants from prior studies conducted by the research team.27,28
Data Collection
The study was conducted according to the Declaration of Helsinki and was approved by the Northwestern Institutional Review Board (IRB). For this study, we sought to recruit 15 participants, with 8 English- and 7 Spanish-speaking adults. Prior literature suggests that this number would be sufficient to reach saturation.29,30 Of 20 participants who were recruited and pre-screened, 15 met the eligibility criteria. In concordance with the literature, our own data analysis revealed that this number was sufficient to reach saturation.29–31 During the pre-screening call, eligible participants provided verbal consent to participate in the interviews. Interviews were conducted by two authors (SWL, AZ) trained in qualitative research who followed semi-structured interview guides. Participants were asked a series of open-ended questions about their attitudes, beliefs, and acceptance of the COVID-19 vaccines (see Supplementary Material 1). All interviews were conducted virtually via Zoom videoconference platform’s audio-only function in order to: (a) protect participants’ privacy for the recording, and (b) allow participation of individuals without access to video technology. Interviews were administered in either Spanish or English, depending on each participant’s preference.
Interviews were supplemented with brief demographic questionnaires, which were interviewer-administered and recorded using Research Electronic Data Capture (REDCap).32 In addition to basic demographics, the survey also included assessment of participants’ health literacy and acculturation levels. A single item screener was used to assess health literacy: “How confident are you in filling out medical forms by yourself?” Responses are measured on a scale of 1 (Extremely) to 5 (Not at all), with scores of 3 or greater indicating inadequate health literacy.33,34 The Short Acculturation Scale for Hispanics (SASH) was used to assess language use, media use, and social relations; acculturation scores represent an average of 12 responses, measured on a scale of 1 to 5, with 1 being least acculturated to US culture and 5 being most acculturated.35,36
In total, the research activities lasted approximately 45 minutes. Interviews were audio-recorded and transcribed. Each participant received a $50 gift card for their time and effort.
Data Analysis
Data analysis was guided by the Framework Method,37 with transcripts analyzed both deductively and inductively. Once a majority of interviews were completed, two authors (SWL, AP) began reading the transcripts for familiarity and content, and writing memos. A set of a priori codes, developed from the interview guide, was piloted with a subset of transcripts. These transcripts were double coded using NVivo software (release 1.4.1, QRS International), and differences in coding were reconciled for each transcript until full agreement was achieved. Memos were used to identify emergent themes and finalize the codebook. Once the codebook was finalized, two authors (SWL, AP) ensured each transcript was fully coded with a second round of coding. These authors met regularly to review coding and achieve coding consensus.38 Detailed matrices were then created in Microsoft Excel, with rows representing individual participants and columns representing single codes. Content relevant to each code was summarized between and within participants.39 The Consolidated Criteria for Reporting Qualitative Research (COREQ) was followed for reporting findings40 (see Supplementary Material 2).
Results
Sample Characteristics
The sample consisted of 15 Latinx adults between 50 and 79 years of age (m = 56.6 years). Ten were female. Eight participants were US-born, five were born in Mexico, and one each was born in El Salvador, Ecuador, and Canada. Of those who were foreign-born, time living in the US ranged between 8 and 51 years (m = 26.1 years), and nine participants reported low acculturation levels. Six participants were considered to have inadequate health literacy. On the SASH, four participants reported reading and speaking both English and Spanish equally, six reported using more Spanish, four reported using more English, and one reported solely using English. Nearly half (n=7) of the sample reported having government-sponsored health insurance (ie, Medicare, Medicaid), while four each reported being on private insurance or uninsured. Approximately half of the participants (n=8) were fully vaccinated at the time of their interviews, while four had received one of two doses, and three were unvaccinated. (Table 1)
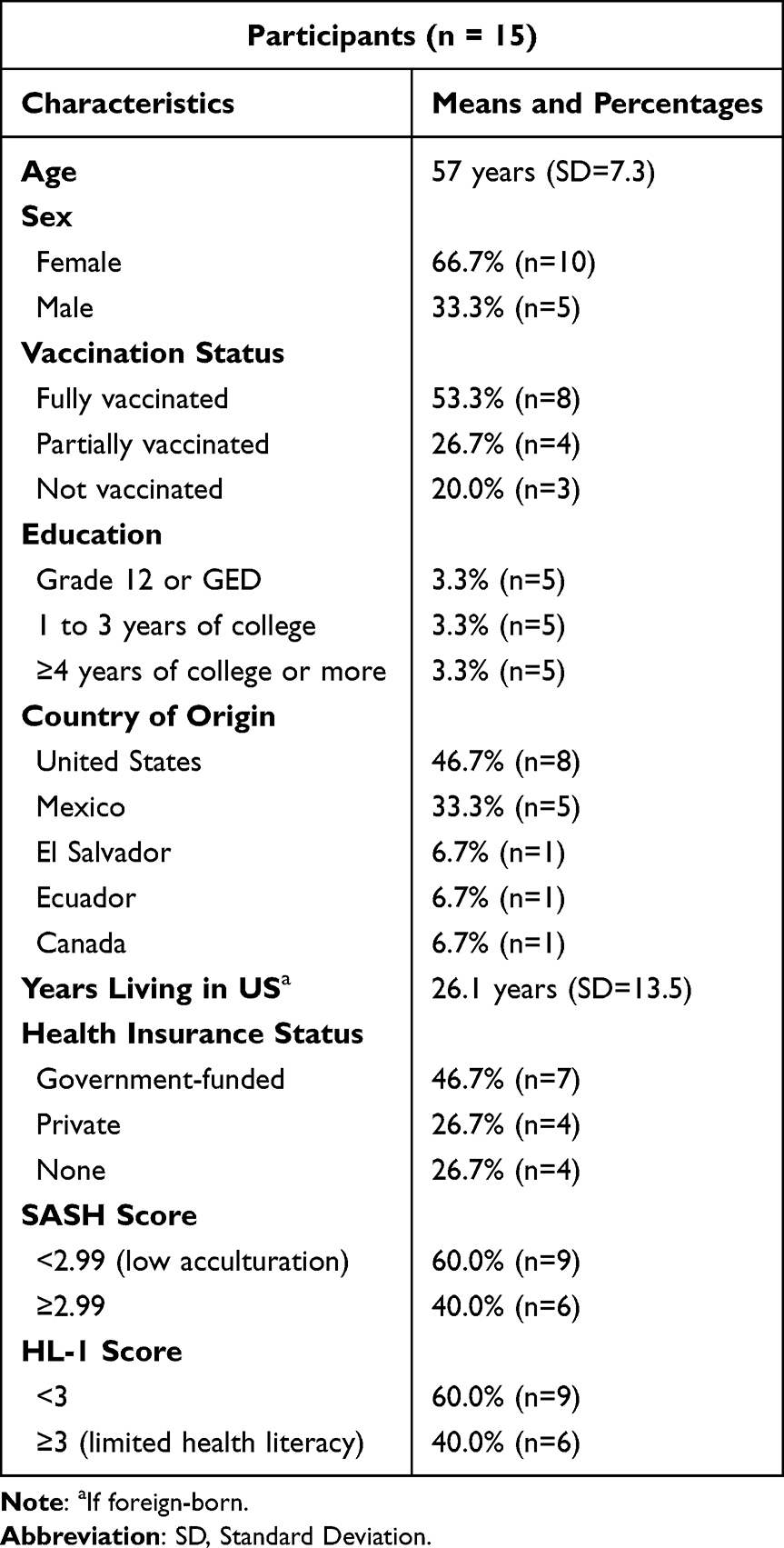 |
Table 1 Participant Demographics |
Themes and Subthemes
Four key factors influencing vaccination decision-making were identified: 1. Protecting oneself and loved ones, 2. Trust in authorities, 3. Access and availability, and 4. Employment and semblance of normalcy. Themes and sub-themes are discussed below, along with representative quotes. (Table 2)
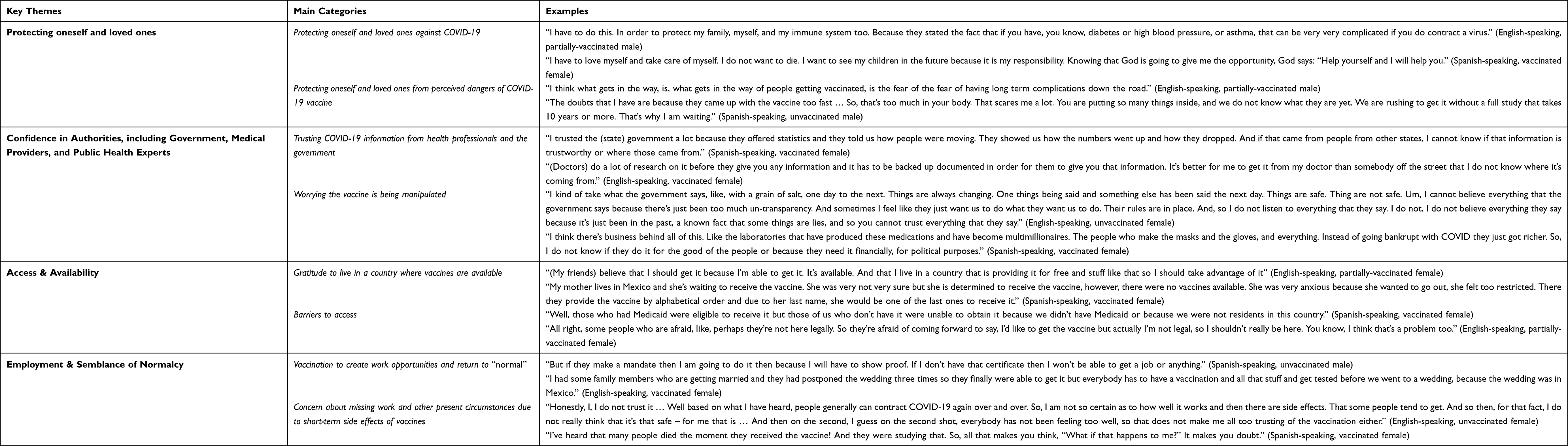 |
Table 2 Key Themes |
Theme 1: Protecting Oneself and Loved Ones
Sub-Theme 1A: Protecting Oneself and Loved Ones Against COVID-19
Nearly all participants (n=14) vocalized an understanding that the vaccine provides protection against COVID-19 infection, with some specifying the utility of vaccines in preventing serious illness, hospitalization, or death. Some participants highlighted the importance of being vaccinated in the context of preexisting health conditions. Over a quarter of the participants mentioned getting vaccinated as a way of assisting God’s will in allowing them to live as long as possible. These participants saw the vaccine as something that could help prevent death from COVID-19. As such, they saw themselves as working together with God.
Many participants noted that family members played an influential role in their vaccination decisions. For instance, two participants mentioned their desire to protect at-risk family members. Others discussed how witnessing loved ones suffer or die of COVID-19 influenced their decisions. Still others expressed how family members’ decisions to get vaccinated helped assuage their own hesitancy towards the vaccine.
Various participants also spoke about the vaccines on a larger, community-wide level, suggesting the importance of “stopping the spread” of COVID-19.
In addition to protecting yourself, you also protect other people. Sometimes you are asymptomatic, you may have had COVID and you don’t know because you don’t have symptoms, and if you are living with other people, you may infect them. So, out of respect for others as well. (Spanish-speaking, vaccinated male).
In this way, these participants saw the decision to vaccinate as a moral obligation or sign of respect towards others. The potential for the vaccine to protect from severe COVID-19 infections was a key reason that many participants decided to get vaccinated.
Sub-Theme 1B: Protecting Oneself and Loved Ones from Perceived Dangers of the COVID-19 Vaccine
Despite the fact that most participants equated the vaccine with protection against COVID-19, the majority of participants (n=9) also expressed concern over potential long-term side effects from the vaccines. They expressed concern regarding the perceived newness of the vaccine and/or the vaccine technology, as well as the speed with which each of the vaccines was studied. For example,
One of the concerns is that this is a new vaccine, a new technology that is being implemented for this type of vaccine. I’m worried that there will be a side effect over the years, not immediately. (Spanish-speaking, vaccinated male).
Additionally, a couple of participants mentioned their fear of needles or general dislike of shots as a factor contributing to their hesitancy. Some participants mentioned concerns about the possible effects of “unnatural” medical interventions on their bodies:
And they are saying that the vaccines only last six months and you have to get another one. So, that’s too much in your body. That scares me a lot. You’re putting so many things inside, and we don’t know what they are yet. (Spanish-speaking, unvaccinated male).
Participants shared different ideas of how the “chemicals” of the COVID-19 vaccine might affect them, including altering their genetic code or even, as one participant mentioned, summoning the “will of the devil”. The possible risks associated with the vaccines played a critical role in decision-making for sample participants. While this was a main deterrent for those who remained unvaccinated, even those who opted for vaccination endorsed weighing potential vaccine risks as key decision-making considerations.
Theme 2: Confidence in Authorities, Including Government, Medical Providers, and Public Health Experts
Sub-Theme 2A: Trust in COVID-19 Information from Health Professionals and the Government
Nearly two thirds of participants (n=9) mentioned trusting their doctors or healthcare providers with personal health decisions, including those regarding the vaccine. Some connected this to their providers’ training, while others felt their providers have their best interests at heart. Many participants also mentioned that they trust information coming from public health organizations, such as the Center for Disease Control (CDC), the World Health Organization (WHO), or the National Institute on Health (NIH). Similarly, participants frequently mentioned trusting public health experts, particularly those who identify as virologists or other specialists, such as Dr. Anthony Fauci. Some participants described competing views about the quality of information coming from federal versus local officials:
I trusted the (state) government a lot because they offered statistics and they told us how people were moving. They showed us how the numbers went up and how they dropped. And if that came from people from other states, I can’t know if that information is trustworthy or where those came from. (Spanish-speaking, vaccinated female).
Therefore, for some participants, information provided by local officials was considered more relevant and meaningful to them compared to information provided by the federal government.
Sub-Theme 2B: Distrust in Authority
Some participants mentioned distrust of authority, including the government, politicians, healthcare providers, and pharmaceutical companies. A third of participants (n=5) mentioned they had heard of conspiracy theories, including that the government will be able to scan vaccinated people, that the government may be trying to kill people, and that the government could be manipulating the vaccine to contain a microchip to control the population. Four participants stated that the government needs to be more transparent, and five felt that politicians are not trustworthy. Some explained that the rapid and constant change in information provided about the vaccine contributed to their own sense of hesitancy:
I kind of take what the government says, like, with a grain of salt, one day to the next. Things are always changing. One thing’s being said and something else has been said the next day. Things are safe. Things are not safe. Um, I can’t believe everything that the government says because there’s just been too much un-transparency. (English-speaking, unvaccinated female).
Participants also expressed skepticism over entities who may be benefitting financially from the pandemic and/or the vaccines, such as pharmaceutical companies. These beliefs and attitudes reflected a general skepticism and mistrust of the reasons for which officials are promoting the vaccine.
Theme 3: Access and Availability
Sub-Theme 3A: Gratitude to Live in a Country Where Vaccines are Available
A third of participants (n=5) expressed gratitude for having access to the vaccine. A few noted that the pandemic seems more controlled in the United States than in Latin America, where some loved ones have not had the privilege of receiving vaccines. One participant specifically felt she had an obligation to receive the vaccine because, unlike her friends in various Latin American countries, she was fortunate enough to have the opportunity:
(My friends) believe that I should get it because I’m able to get it. It’s available. And that I live in a country that is providing it for free and stuff like that so I should take advantage of it (English-speaking, partially-vaccinated female).
Sub-Theme 3B: Barriers to Access
About a quarter of participants (n=4) mentioned that individuals who are undocumented may feel particularly hesitant to receive the vaccine, either due to a fear of deportation, distrust of the government, or uncertainty about the documentation required to get vaccinated. Some also mentioned uncertainty regarding eligibility when people do not have health insurance or regarding the cost of the vaccine:
Well, those who had Medicaid were eligible to receive it but those of us who don’t have it were unable to obtain it because we didn’t have Medicaid or because we were not residents in this country. (Spanish-speaking, vaccinated female).
This participant, in particular, delayed vaccination until she was assured she did not have to pay for the vaccine. Relatedly, a third of participants expressed concern about a language barrier, highlighting the need for vaccine information to be provided in Spanish or other languages prevalent in given communities. Some participants also suggested that the public vaccination of Latinx celebrities or Spanish-speaking experts might help boost vaccination rates. Approximately half of participants also mentioned the need to inform members of their communities about where to get vaccinated, how to book an appointment, or how to get there. One participant suggested the radio could be an effective mode of communication for community members, while others suggested that setting up vaccination sites in grocery store parking lots or other conveniently located places may help to increase vaccine uptake in their communities.
Theme 4: Employment & Semblance of Normalcy
Sub-Theme 4A: Vaccination to Create Work Opportunities and Return to “Normal”
Some participants spoke about how the vaccine can help people return to normal. Particularly, many participants discussed the vaccine in relationship to employment (n=6), mentioning the economic impact of the pandemic and the need to return to work. One participant suggested he would only get vaccinated if it did become mandatory for work, two mentioned family members who work in healthcare that needed to get vaccinated, and two stated that they personally received the vaccine due to their own employers’ requirements:
Yes, I thought, if I don’t receive the vaccine and I want to work in certain places –many places request that you have the vaccine. I knew that the persons I work with had already received the vaccine, so, if I didn’t get vaccinated they could ask me, “Have you received the vaccine? We have this condition and you won’t be able to come.” (Spanish-speaking, vaccinated female).
Others discussed the vaccine as a means to being able to return to church, go to weddings, travel, spend time with family members, and not have to wear masks indoors. Vaccination, for these participants, facilitated a return to events they enjoyed and missed.
Sub-Theme 4B: Concern About Missing Work and Other Present Circumstances Due to Short-Term Side Effects of Vaccines
While the fear of missing work due to side effects from the vaccine was mentioned as a potential deterrent, for the majority this did not come up organically. That said, a majority of participants (n=9) did express concern over the potential short-term side effects of the vaccines. Some mentioned concern about feeling sick after getting vaccinated.
Honestly, I, I don’t trust it … Well based on what I’ve heard, people generally can contract COVID-19 again over and over. So, I’m not so certain as to how well it works and then there are side effects. That some people tend to get. And so then, for that fact, I don’t really think that it’s that safe – for me that is … And then on the second, I guess on the second shot, everybody has not been feeling too well, so that doesn’t make me all too trusting of the vaccination either. (English-speaking, unvaccinated female).
Two participants expressed concern after hearing that some had died from the vaccine. These participants considered the possibility of short-term and immediate consequences of the vaccine interrupting their current functioning.
Discussion
The present study explored Chicago-based Latinx older adults’ perceptions, attitudes, and decision-making factors related to the COVID-19 vaccines, with the purpose of informing the development of vaccine messaging for this population. Latinx older adults represent a sector of the US that has been disproportionately impacted by the pandemic.7 Nevertheless, to our knowledge, this is the first study to engage stakeholders from this community in an exploration of themes related to COVID-19 vaccine acceptance and uptake, in order to inform material development. Findings revealed several factors that contribute to the vaccination decision-making process of sample participants: their desire to protect themselves and their loved ones, trust in authorities, concerns about access and employment, and desire for some semblance of normalcy. These themes suggested that, in designing vaccine messaging strategies for Latinx older adults in Chicago, general messaging strategies would benefit from key culturally-appropriate adjustments.
General Messaging
Numerous findings from the present study were similar to results found among the general population. Specifically, many participants in our study shared a “wait and see” attitude towards the vaccine – preferring to defer receiving the vaccine until more long-term consequences are clarified – or a preference for natural immunity, which has previously been associated with a lower likelihood of getting the influenza vaccine.41–43 Similar to results of other vaccine studies,36,44 the weighing of perceived risks and benefits of vaccination was central to decision-making among sample participants. These findings highlighted the need for increasing awareness and knowledge of the serious risks of coronavirus, the direct prevention benefits of the vaccines, and the safety of the ingredients in the vaccines. Also consistent with recent work from the United Kingdom,13 many respondents discussed the vaccines as a way to return to “normal” faster, including socializing with friends and family, hugging loved ones, attending weddings and religious events, and traveling and working. Consistent with Lancet Commission recommendations,19 various participants mentioned the potential of mandates from employers as an important facilitator in getting vaccinated. These findings suggested that messaging could benefit from highlighting that vaccines are a key aspect of expediting a return to a pre-COVID-19 way of life – particularly in terms of socializing and sustaining employment.
Cultural Tailoring
On the other hand, by engaging with the target population, our study revealed key areas where messaging should be adapted to the target population, including leveraging collective pronouns, spirituality, language, technology, trust, insurance, and immigration. Tailoring of health messages has been shown to be effective for changing behavior.45 In our study, the concept of vaccination as a moral responsibility in “stopping the spread” of COVID-19 is consistent with previous research that demonstrated that a lower sense of collective responsibility independently predicted lack of uptake of influenza, pneumococcal, and shingles vaccines in older adults.42 As Latinx culture is commonly more collectivist,46 it might be particularly useful to utilize collective pronouns such as “we” in messaging efforts, which has previously been associated with increased health intentions, including social distancing and mask wearing.47 Personal spiritual beliefs also surfaced as a common factor in decision-making. Similar to prior research on vaccine acceptance in Latinx communities,36 our findings suggested the importance of taking spiritual beliefs into account when designing and disseminating materials to promote COVID-19 vaccine uptake, for instance by seeking partnerships with religious organizations in communities targeted by vaccine promotion efforts.
Logistical barriers, such as limited language-concordant information, transportation, and technology, were mentioned by various participants. In the context of the Latinx community, the perceived language barrier is particularly relevant, as inequity in access to health services is often compounded by language and communication challenges.16 Efforts to enhance vaccination uptake among older Latinx individuals should focus on ensuring that information is conveyed in Spanish through a variety of mediums, including low-tech options. For example, language-specific advice could be disseminated in texts, emails, letters, the radio, and posters in local community sites.48 Vaccination sites should also ensure the availability of language-concordant providers and/or interpreters, and translated, culturally-appropriate vaccine information.
Participants’ perceptions of healthcare providers and governmental officials consistently influenced decision-making. Discrimination, racialized processes, prior injustices, and unethical research have led to mistrust of the government and pharmaceutical companies among many historically marginalized racial and ethnic groups throughout history, and this has recently been shown to be associated with COVID-19 vaccine hesitancy and refusal.13,49 Addressing this mistrust will require drastic systemic change.13 Our findings suggested that a first step could be embedding within informational materials the explicit acknowledgement of historical and contemporary abuses of power in the context of vaccine acceptance, and the clear articulation of roles and responsibilities of the various entities that will contribute to COVID-19 vaccination efforts.13,19 In terms of future directions, governmental bodies and public health agencies may benefit from partnering with trusted community-based organizations and respected individuals to help spread accurate, research-based information and dispel the myths and conspiracies that have been circulated.49,50
Poor treatment of immigrants in the US may also be negatively influencing uptake behaviors among the Latinx population, as some participants discussed the fear of deportation or the uncertainty regarding vaccine access for those without citizenship. Relatedly, doubts were raised regarding access to the vaccines for those without health insurance, highlighting deep institutional problems with the healthcare system in the US, which is largely based on employment benefits or the ability to pay, and thus inherently discriminatory.51,52 Therefore, these findings indicated the importance of messaging that directly states that COVID-19 vaccinations are available at no cost and that citizenship and health insurance are not required for vaccination.
Limitations
The current study has several limitations. This small sample is from one geographic region and is not generalizable to older Latinx adults living in other diverse regions of the US. Latinx individuals living in the US represent diverse backgrounds and experiences, shaped by myriad social, environmental, and structural factors and must be viewed as heterogeneous. As all coding was completed on English transcripts, it is possible that the translation process obscured certain nuances present in the original Spanish recordings. Despite bilingualism and professional and personal experience with Latinx communities, neither coder identifies as Latinx. Additionally, there was researcher overlap in collection and analysis of the data, which may introduce some bias. However, this study was novel in its inclusion of both English- and Spanish-speaking Latinx older adults, as well as its utilization of qualitative methodologies, which allowed for the exploration of the complexities and nuances involved in vaccination decision-making during the ongoing pandemic.
Conclusion
Semi-structured interviews with Latinx older adults revealed several key factors involved in COVID-19 vaccine decision-making. Culturally-tailored messaging may benefit from leveraging collective pronouns and spirituality, addressing insurance and immigration doubts, and considering language concordance, low-tech options, and trusted community partners. Next steps are to develop educational materials based on these themes, followed by dissemination and evaluation of their effectiveness. Lessons learned from this local engagement with stakeholders may provide insights to support future health behavior messaging that is culturally-based and catered to unique, intersectional communities that are disproportionately impacted by various public health crises.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval & Informed Consent
This study was conducted according to the Declaration of Helsinki and approved by the Northwestern University Institutional Review Board (IRB). Informed consent was obtained from all individual participants included in the study, including publication of anonymized responses. Due to the risks involved with COVID-19 at the time, the Northwestern University IRB approved verbal consent. This was deemed a minimal risk study, and the barriers to meeting in-person would have been substantial. Research team members reviewed verbal consent forms in depth with all participants over the phone. Verbal consent was informed, witnessed, and recorded by research team members.
Funding
Research reported in this publication was supported by the RRF Foundation for Aging and by the National Institute on Aging, Grant Number P30AG059988. Research reported in this publication was additionally supported, in part, by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422. The content is solely the responsibility of the authors and does not necessarily represent the official views of either RRF or the National Institutes of Health.
Disclosure
Dr. Pack reports grants via her University from NIH, RRF Foundation for Aging, Pfizer, Merck, Gordon and Betty Moore Foundation, Lundbeck and Eli Lilly during the conduct of the study.
Dr. Bailey reports grants from the NIH, Retirement Research Foundation, during the conduct of the study; grants from Pfizer, Gordon and Betty Moore Foundation, Merck, Lundbeck, and Eli Lilly and personal fees from Sanofi, Pfizer, University of Westminster, Lundbeck and Luto outside the submitted work.
Dr. Wolf reports grants from RRF Foundation for Aging, during the conduct of the study; grants from the NIH (NIA, NIDDK, NINR, NHLBI, NINDS), Gordon and Betty Moore Foundation, Pfizer, Merck and Eli Lilly, and personal fees from Pfizer, Sanofi, Luto UK, University of Westminster, Lundbeck and GlaxoSmithKline, outside the submitted work.
References
1. Center for Disease Control. COVID data tracker. centers for disease control and prevention; 2020. Available from: https://covid.cdc.gov/covid-data-tracker.
2. Clark A, Jit M, Warren-Gash C, et al. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health. 2020;8(8):e1003–e1017. doi:10.1016/S2214-109X(20)30264-3
3. World Health Organization. COVID-19 and NCDs. Information note on COVID-19 and noncommunicable diseases. World Health Organization; 2020. Available from: https://www.who.int/who-documents-detail/covid-19-and-ncds.
4. Center for Disease Control and Prevention (CDC). Cases, data, and surveillance. Centers for disease control and prevention; 2022. Available from: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html.
5. Peteet B, Belliard JC, Abdul-Mutakabbir J, Casey S, Simmons K. Community-academic partnerships to reduce COVID-19 vaccine hesitancy in minoritized communities. EClinicalMedicine. 2021;34:100834. doi:10.1016/j.eclinm.2021.100834
6. Tai DBG, Shah A, Doubeni CA, Sia IG, Wieland ML. The disproportionate impact of COVID-19 on racial and ethnic minorities in the United States. Clin Infect Dis. 2021;72(4):703–706. doi:10.1093/cid/ciaa815
7. Garcia MA, Homan PA, García C, Brown TH. The color of COVID-19: structural racism and the disproportionate impact of the pandemic on older black and latinx adults. J Gerontol Ser B. 2021;76(3):e75–e80. doi:10.1093/geronb/gbaa114
8. Center for Disease Control. Benefits of getting a COVID-19 vaccine. centers for disease control and prevention; 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/vaccine-benefits.html.
9. Corey L, Mascola JR, Fauci AS, Collins FS. A strategic approach to COVID-19 vaccine R&D. Science. 2020;368(6494):948–950. doi:10.1126/science.abc5312
10. Jarrett C, Wilson R, O’Leary M, Eckersberger E, Larson HJ. Strategies for addressing vaccine hesitancy – a systematic review. Vaccine. 2014;33(34):4180–4190. doi:10.1016/j.vaccine.2015.04.040
11. Kociolek LK, Elhadary J, Jhaveri R, Patel AB, Stahulak B, Cartland J. Coronavirus disease 2019 vaccine hesitancy among children’s hospital staff: a single-center survey. Infect Control Hosp Epidemiol. 2021;42(6):775–777. doi:10.1017/ice.2021.58
12. Ndugga N, Hill L, Artiga S, Parker N. Latest data on COVID-19 vaccinations race/ethnicity. KFF; 2021. Available from: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-april-2021/.
13. Woodhead C, Onwumere J, Rhead R, et al. Race, ethnicity and COVID-19 vaccination: a qualitative study of UK healthcare staff. Ethn Health. 2021:1–20. doi:10.1080/13557858.2021.1936464
14. Bogart LM, Dong L, Gandhi P, et al. What Contributes to COVID-19 Vaccine Hesitancy in Black Communities, and How Can It Be Addressed? RAND Corporation; 2021. doi:10.7249/RRA1110-1
15. Karpman M, Zuckerman S, Gonzalez D, Kenney GM. Confronting COVID-19 vaccine hesitancy among nonelderly adults; 2021:21.
16. Ortega P, Shin TM, Pérez-Cordón C, Martínez GA. Virtual medical Spanish education at the Corazón of Hispanic/Latinx health during COVID-19. Med Sci Educ. 2020;30(4):1661–1666. doi:10.1007/s40670-020-01058-0
17. Nguyen LH, Joshi AD, Drew DA, et al. Racial and ethnic differences in COVID-19 vaccine hesitancy and uptake. medRxiv. 2021. doi:10.1101/2021.02.25.21252402
18. Colby SL, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. US Dep Commer Econ Stat Adm US Census Bur. 2015;13:45.
19. Omer SB, Benjamin RM, Brewer NT, et al. Promoting COVID-19 vaccine acceptance: recommendations from the lancet commission on vaccine refusal, acceptance, and demand in the USA. Lancet. 2021;398(10317):2186–2192. doi:10.1016/S0140-6736(21)02507-1
20. Cowell AJ, Farrelly MC, Chou R, Vallone DM. Assessing the impact of the national “truth” antismoking campaign on beliefs, attitudes, and intent to smoke by race/ethnicity. Ethn Health. 2009;14(1):75–91. doi:10.1080/13557850802257715
21. Najib Balbale S, Schwingel A, Chodzko-Zajko W, Huhman M. Visual and participatory research methods for the development of health messages for underserved populations. Health Commun. 2014;29(7):728–740. doi:10.1080/10410236.2013.800442
22. Heard E, Fitzgerald L, Wigginton B, Mutch A. Applying intersectionality theory in health promotion research and practice. Health Promot Int. 2020;35(4):866–876. doi:10.1093/heapro/daz080
23. Samra R, Hankivsky O. Adopting an intersectionality framework to address power and equity in medicine. Lancet. 2021;397(10277):857–859. doi:10.1016/S0140-6736(20)32513-7
24. Hotez E, Hudson S, Cho A, et al. Addressing disparities for intersectional Bipoc communities: the hood medicine initiative case study. eClinicalMedicine. 2021;42:101199. doi:10.1016/j.eclinm.2021.101199
25. Bronfenbrenner U. The Ecology of Human Development: Experiments by Nature and Design. Harvard university press; 1979. Available from: https://books.google.com/books?hl=es&id=OCmbzWka6xUC&oi=fnd&pg=PA3&dq=Bronfenbrenner+U.+The+ecology+of+human+development:+Experiments+by+nature+and+design.+Cambridge,+MA:+Harvard+University+Press%3B+1979.&ots=yzMYI1STgf&sig=BKqdxE8_pF1N8J9EdbbRmlMFkhY#v=onepage&q=Bronfenbrenner%20U.%20The%20ecology%20of%20human%20development%3A%20Experiments%20by%20nature%20and%20design.%20Cambridge%2C%20MA%3A%20Harvard%20University%20Press%3B%201979.&f=false.
26. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi:10.1177/109019818801500401
27. Gioia CJ, Sobell LC, Sobell MB, Agrawal S. Craigslist versus print newspaper advertising for recruiting research participants for alcohol studies: cost and participant characteristics. Addict Behav. 2016;54:24–32. doi:10.1016/j.addbeh.2015.11.008
28. Topolovec-Vranic J, Natarajan K. The use of social media in recruitment for medical research studies: a scoping review. J Med Internet Res. 2016;18(11):e286. doi:10.2196/jmir.5698
29. Guest G, Bunce A, Johnson L. How many interviews are enough?: An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
30. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
31. Dubé E, Gagnon D, MacDonald N, Bocquier A, Peretti-Watel P, Verger P. Underlying factors impacting vaccine hesitancy in high income countries: a review of qualitative studies. Expert Rev Vaccines. 2018;17(11):989–1004. doi:10.1080/14760584.2018.1541406
32. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) - A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inf. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
33. Chew LD, Griffin JM, Partin MR, et al. Validation of screening questions for limited health literacy in a large VA outpatient population. J Gen Intern Med. 2008;23(5):561–566. doi:10.1007/s11606-008-0520-5
34. Sarkar U, Karter AJ, Liu JY, Moffet HH, Adler NE, Schillinger D. Hypoglycemia is more common among type 2 diabetes patients with limited health literacy: the diabetes study of Northern California (DISTANCE). J Gen Intern Med. 2010;25(9):962–968. doi:10.1007/s11606-010-1389-7
35. Marin G, Sabogal F, Marin BV, Otero-Sabogal R, Perez-Stable EJ. Development of a short acculturation scale for hispanics. Hisp J Behav Sci. 1987;9(2):183–205. doi:10.1177/07399863870092005
36. Lindsay AC, Valdez MJ, Delgado D, Restrepo E, Guzmán YM, Granberry P. Acceptance of the HPV vaccine in a multiethnic sample of Latinx mothers. Qual Health Res. 2021;31(3):472–483. doi:10.1177/1049732320980697
37. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
38. Cohen D, Crabtree BF, Damschroder L, et al. Qualitative methods in implementation science; 2018:31.
39. Tolley EE, Ulin PR, Mack N, Robinson ET, Succop SM. Qualitative Methods in Public Health: A Field Guide for Applied Research. John Wiley & Sons; 2016.
40. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
41. Zein S, Abdallah SB, Al-Smadi A, Gammoh O, Al-Awaida WJ, Al-Zein HJ. Factors associated with the unwillingness of Jordanians, Palestinians and Syrians to be vaccinated against COVID-19. PLoS Negl Trop Dis. 2021;15(12):e0009957. doi:10.1371/journal.pntd.0009957
42. Nicholls LAB, Gallant AJ, Cogan N, Rasmussen S, Young D, Williams L. Older adults’ vaccine hesitancy: psychosocial factors associated with influenza, pneumococcal, and shingles vaccine uptake. Vaccine. 2021;39(26):3520–3527. doi:10.1016/j.vaccine.2021.04.062
43. Martin LR, Petrie KJ. Understanding the dimensions of anti-vaccination attitudes: the Vaccination Attitudes Examination (VAX) scale. Ann Behav Med. 2017;51(5):652–660. doi:10.1007/s12160-017-9888-y
44. Betsch C, Schmid P, Heinemeier D, Korn L, Holtmann C, Böhm R. Beyond confidence: development of a measure assessing the 5C psychological antecedents of vaccination. PLoS One. 2018;13(12):e0208601. doi:10.1371/journal.pone.0208601
45. Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol Bull. 2007;133(4):673–693. doi:10.1037/0033-2909.133.4.673
46. Rinderle S, Montoya D. Hispanic/Latino identity labels: an examination of cultural values and personal experiences. Howard J Commun. 2008;19(2):144–164. doi:10.1080/10646170801990953
47. Courtney EP, Felig RN, Goldenberg JL. Together we can slow the spread of COVID-19: the interactive effects of priming collectivism and mortality salience on virus-related health behaviour intentions. Br J Soc Psychol. 2022;61(1):410–431. doi:10.1111/bjso.12487
48. Knights F, Carter J, Deal A, et al. Impact of COVID-19 on migrants’ access to primary care and implications for vaccine roll-out: a national qualitative study. Br J Gen Pract. 2021;71(709):e583–e595. doi:10.3399/BJGP.2021.0028
49. Ateghang-Awankem B, Anchang KY. Engaging African Diaspora in the fight against vaccine hesitancy. Am J Public Health Res. 2020;9(1):28–37.
50. Thomas CM, Osterholm MT, Stauffer WM. Critical considerations for COVID-19 vaccination of refugees, immigrants, and migrants. Am J Trop Med Hyg. 2021;104(2):433–435. doi:10.4269/ajtmh.20-1614
51. Lanesskog D, Schneider S, Barragán A. Bureaucratic incorporation or abdication? Public health with Latinx immigrants in new destinations. Hum Serv Organ Manag Leadersh Gov. 2021;45(4):307–325. doi:10.1080/23303131.2021.1901816
52. Portes A, Light D, Fernández-Kelly P. The U.S. health system and immigration: an institutional interpretation1. Sociol Forum. 2009;24(3):487–514. doi:10.1111/j.1573-7861.2009.01117.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Factors Associated with Depression Among Older Adults During the COVID-19 Pandemic: A Cross-Sectional Study in Urban Areas in Thailand
Tangthong A, Manomaipiboon B
Clinical Interventions in Aging 2023, 18:1055-1065
Published Date: 10 July 2023
Exploring Varied Experiences of Three Stakeholders of the COVID-19 Pandemic
Nandonik AJ, Anik AI, Kabir ZN
Risk Management and Healthcare Policy 2024, 17:1827-1833
Published Date: 15 July 2024
Real-World Effectiveness of Nirmatrelvir/Ritonavir in Hospitalized Older Adults with Severe Omicron COVID-19: A Retrospective Cohort Study from China
Chen Y, Liu L, Liu Y, Huang F, Guo L, Wan W, Jiang H
Infection and Drug Resistance 2025, 18:2901-2909
Published Date: 7 June 2025