")
Back to Journals » International Journal of General Medicine » Volume 15
Perception of Rickets Disease Among Parents in Al-Baha Province, Saudi Arabia
Authors Alzahrani AA
Received 24 February 2022
Accepted for publication 12 May 2022
Published 17 May 2022 Volume 2022:15 Pages 5043—5049
DOI https://doi.org/10.2147/IJGM.S361719
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdulwahab Ahmed Alzahrani
Surgery Department, Faculty of Medicine, Al-Baha University, Albaha, Saudi Arabia
Correspondence: Abdulwahab Ahmed Alzahrani, Surgery Department, Faculty of Medicine, Albaha University, Albaha, 65561, Saudi Arabia, Tel +966505572226, Email [email protected]; [email protected]
Introduction: Rickets involves the softening of bones in children and osteopenia with disordered calcification, leading to a higher proportion of osteoid tissue prior to epiphyseal closure in children. Rickets is common in the Middle East, Africa, and Asia. The peak age of prevalence is 3– 18 months. Signs include bone tenderness, easy fracture, early bone deformity, delayed closure of fontanelles, and softening of skull bones (craniotabes).
Objective: This study assesses knowledge in the AlBaha region about rickets’ clinical presentation, causes, complications, and prevention, as well recommendations to educate the community.
Methods: In this descriptive cross-sectional study, a questionnaire was administered to people in the AlBaha region to assess knowledge related to rickets in children. The sample size was calculated using calculator.net, and the Statistical Package for Social Sciences (SPSS) version 2 was used for analyses with P < 0.05 used for significance.
Results: Of the 692 participants, only 5% reported rickets in their children, but the majority (99%) had heard about rickets. Participants’ knowledge of rickets’ complications was highest for spinal vertebral deformities and lowest for skin deformities. 55% of the participants thought there was no need to stop breast-feeding once rickets is diagnosed, 62% preferred to add fortified milk to the diet, 67% thought that a suitable duration for sunlight exposure is 10 to 15 minutes per day, and 46% thought that sunrise and sunset are suitable times for sun exposure. Preventive measures were believed to depend on having enough exposure to sunlight (77% of participants) and eating vitamin-D rich foods (63%). The majority believed that failure to grow is the most obvious symptom, inadequate milk is the main cause, and exclusive breast-feeding is a major risk factor.
Conclusion: Most people have heard about rickets, but knowledge about complications and prevention varies.
Keywords: rickets, vitamin D, osteopenia, bone growth, prevention
Introduction
Rickets is widespread in developing countries and is common in the Middle East, Africa, and Asia.1 The peak age at which rickets is most prevalent is 3–18 months, especially among exclusively breast-fed infants and infants of dark-skinned immigrants living in temperate climates.2 Rickets is the softening of bones in children and osteopenia with disordered calcification, leading to a higher proportion of osteoid tissue prior to epiphyseal closure.
It involves inadequate calcification of growth plates and is most often caused by vitamin D deficiency due to diet or inadequate sun exposure. Sometimes, it is caused by celiac disease or some genetic conditions.3
Signs include bone tenderness, easy fracture, early bone deformity, delayed closure of fontanelles, and softening of skull bones (craniotabes).4 Pediatricians and other healthcare professionals should try to ensure that children and adolescents receive the daily vitamin D requirements that are appropriate for their risk factors, traditions, and customs.5
It is recommended that all infants, including those who are exclusively breastfed, have a minimum intake of 200 IU of vitamin D per day beginning in the first 2 months of life.
In addition, it is recommended that an intake of 200 IU of vitamin D per day be continued throughout childhood and adolescence because adequate sunlight exposure is not easily determined for a given individual.6
The aim of this study is to assess the awareness and knowledge of people living in the Al-Baha region about the causes, clinical presentation, complications, and prevention of rickets, as well as to identify the recommendations to educate the community.
Methodology
In this descriptive cross-sectional study, a questionnaire was administered to people living in the Al-Baha region through direct interviews and an electronic version. Before starting the questionnaire, vocal consent was required from all of the participants. At any time, the participant had the right to withdraw consent.
The questionnaire contained 13 questions. The questions were divided into two sections: one for demographic characteristics comprising the first 4 questions and one for knowledge and prevention comprising the remaining 9 questions. The assessment of participants’ knowledge was performed using those 9 questions, and 1 point was assigned for each correctly answered question, while those answered incorrectly received 0 points. The total score of knowledge was calculated for each participant. The minimum possible score was 0, and the maximum possible score was 17 due to more than one correct answer being possible (Table 1).
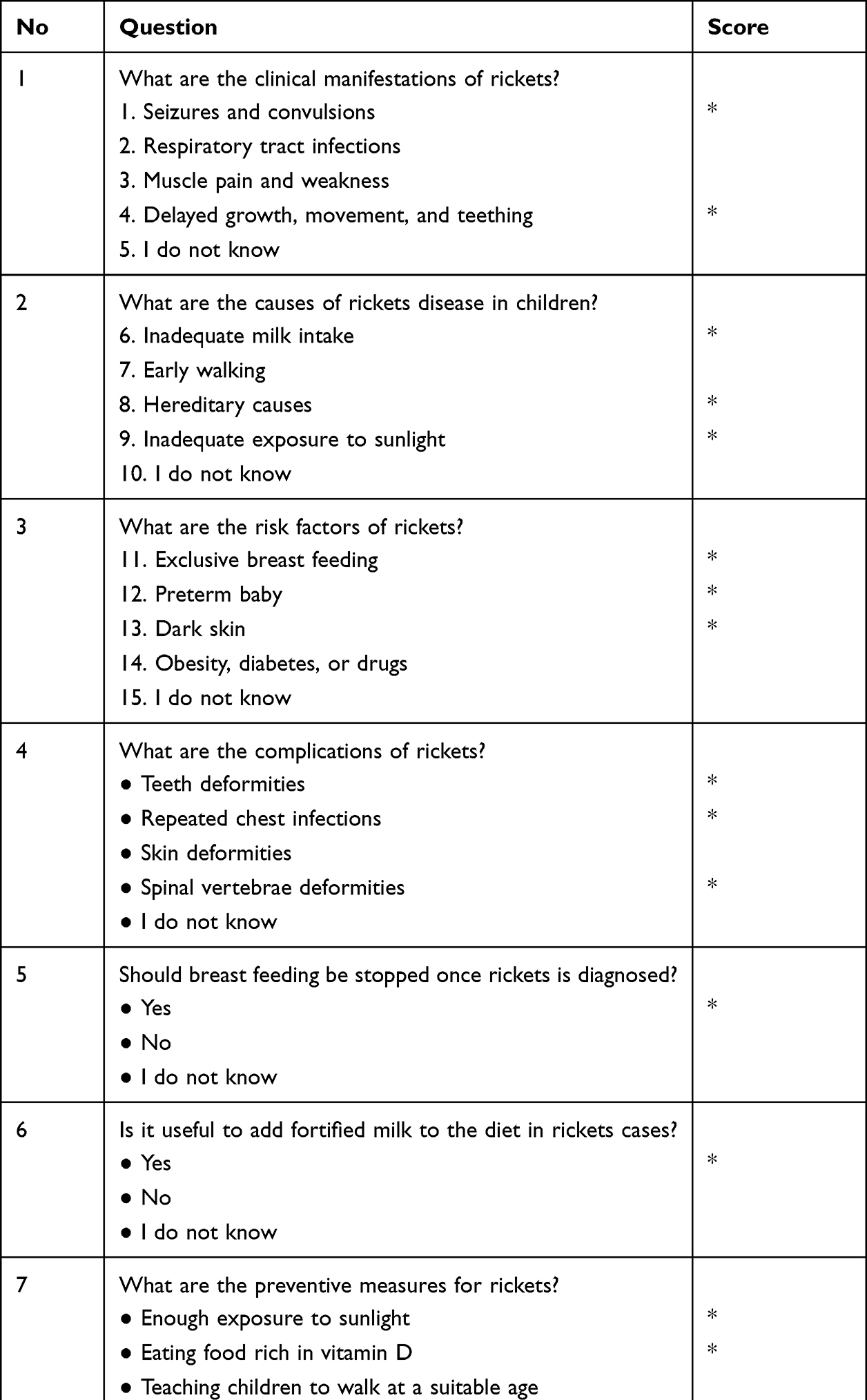 |
Table 1 Rickets Knowledge Score |
The data were collected during the period from February 27 to May 27, 2019. All collected data were statistically analyzed. Only people living in Al Baha in the last two years were included in the study. People who fit the inclusion criteria and agreed to participate voluntarily were enrolled in the study.
According to the sample size equation, we targeted about 384 participants (n = 384), but the actual sample size was about 692. All statistical analyses were performed using the Statistical Package for Software Sciences (SPSS). P < 0.05 was used for significance.
Results
Table 2 shows information about the 692 participants, of which 38% were males and 62% were females. Most of them were married and were above the age of 24 years. Most had a high-school education and above. As shown in Table 3, the 692 participants were asked about their experience and knowledge of rickets disease. Only 5% of the participants’ children had rickets, and the majority (99%) had heard about rickets. The sources of information about rickets for most participants were mass media (43%), social media (27%), and health-education programs (25%).
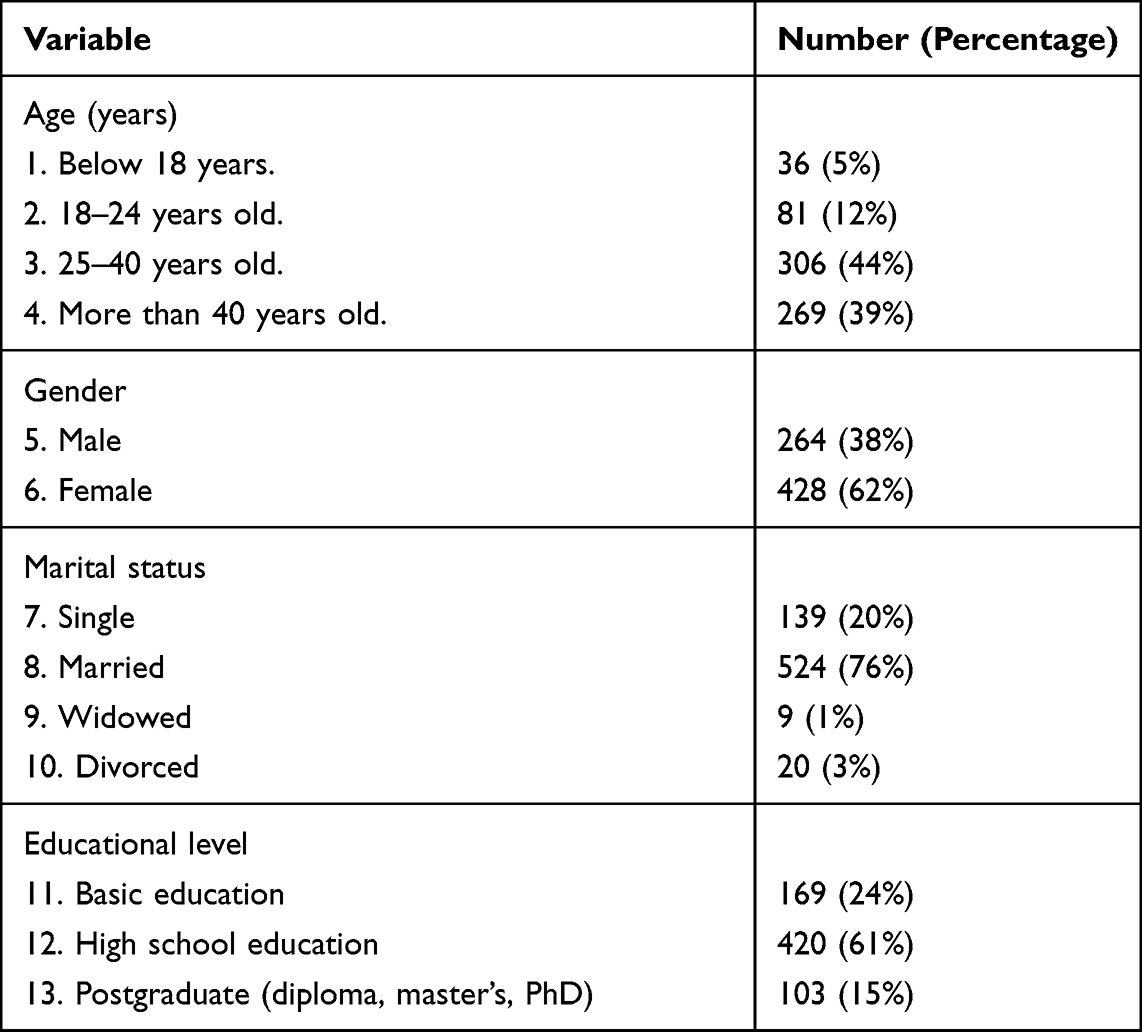 |
Table 2 Socio-Demographic Data of the Study Group (Number = 692) |
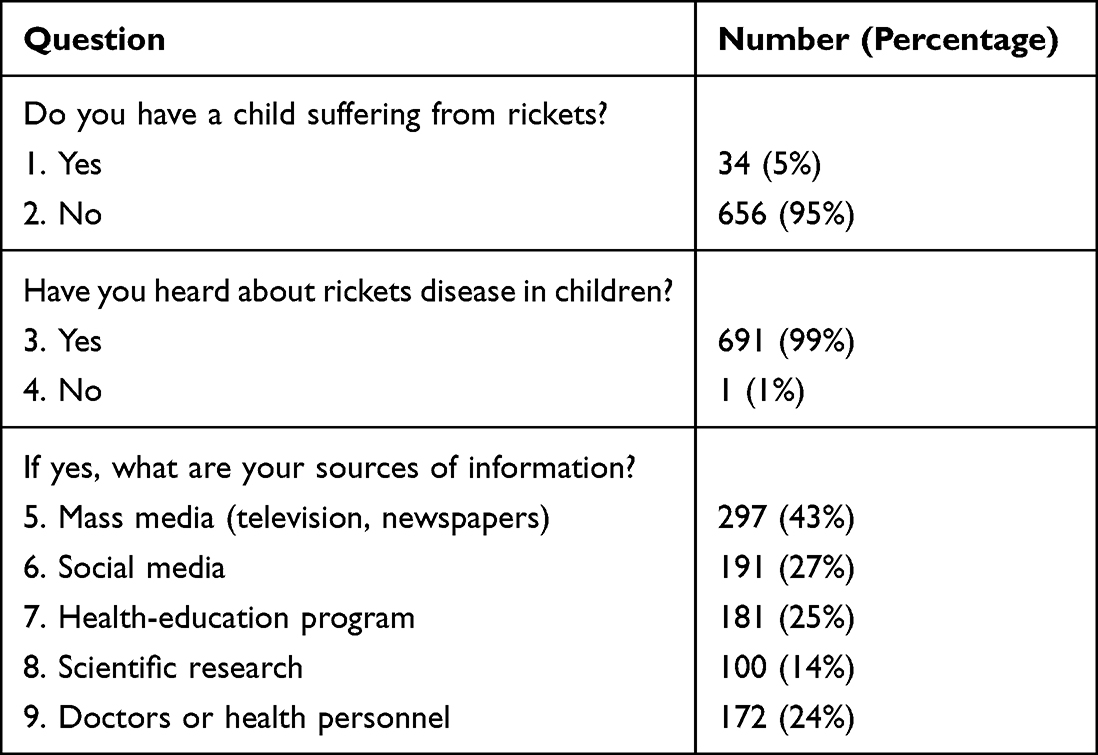 |
Table 3 Experience and Awareness of the Studied Group with Rickets (Number = 692) |
Table 4 shows that the majority of participants had good knowledge about the clinical manifestations, causes, and risk factors of rickets, but lower percentages had wrong ideas in this regard, and even lower percentages had no ideas. Table 5 shows that most participants 70% perceived those spinal vertebrae deformities are some of the complications of rickets, while 24% also considered teeth deformities as a complication, and 28% had no idea. For the prevention of rickets, the majority indicated that breast-feeding should not be stopped (55%) and that it is useful to add fortified milk to the diet (62%). Table 6 shows that there was a good knowledge of preventive measures in that 77% perceived that enough exposure to sunlight is a preventive measure at sunrise and sunset (46%) and that 10–15 minutes is enough time (67%). Furthermore, 63% of participants perceived that eating food rich in vitamin D is a preventive measure. A low percentage had no idea about preventive measures. The mean knowledge score of participant’s perception of rickets was 11.6 ± 2.4 out of 17. Knowledge score showed a significantly negative correlation with age below 18 years old (P = 0.03) and basic education (P = 0.02).
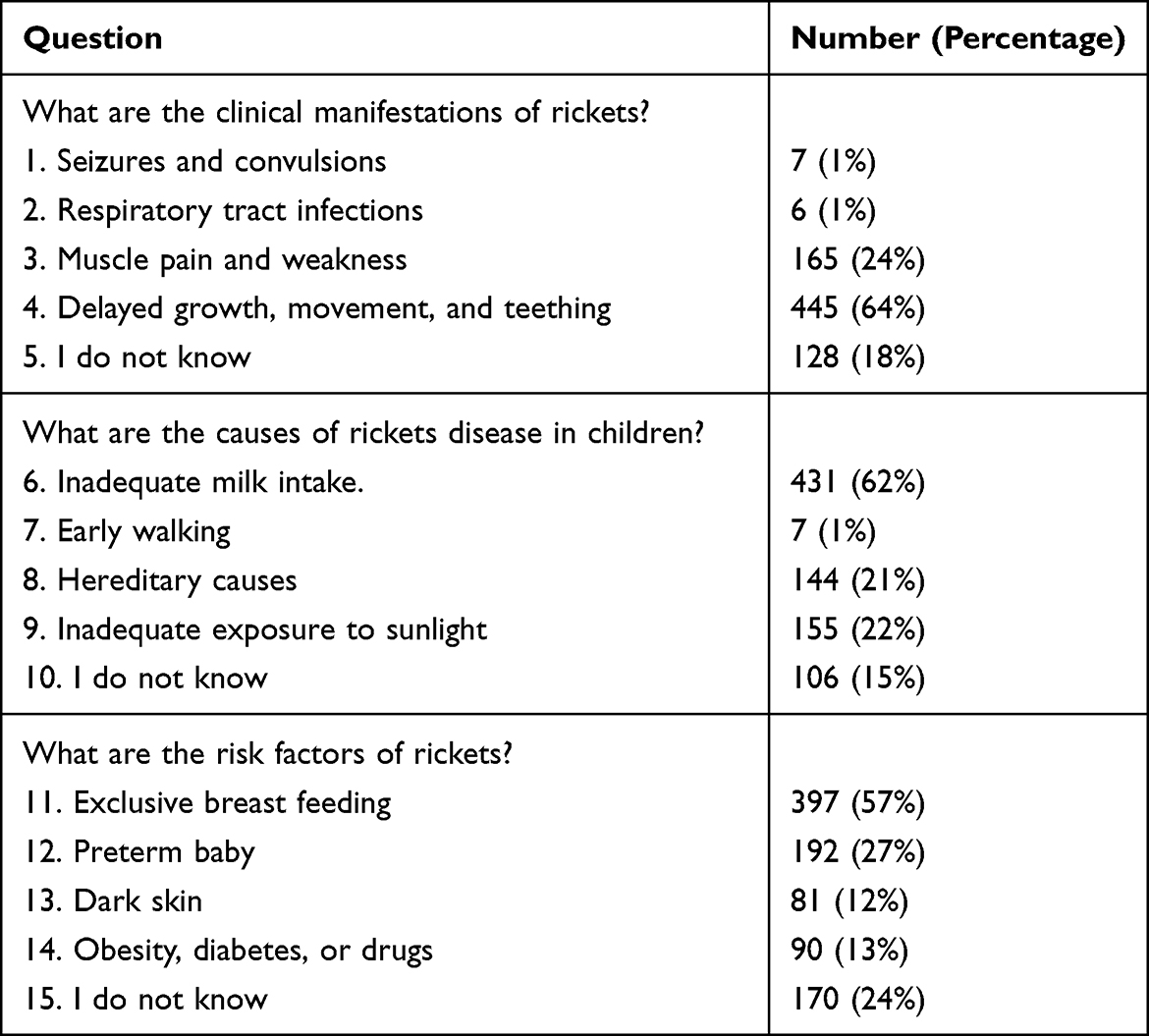 |
Table 4 Participants’ Responses to Clinical Picture, Cause, and Risk Factor Questions (Number = 692) |
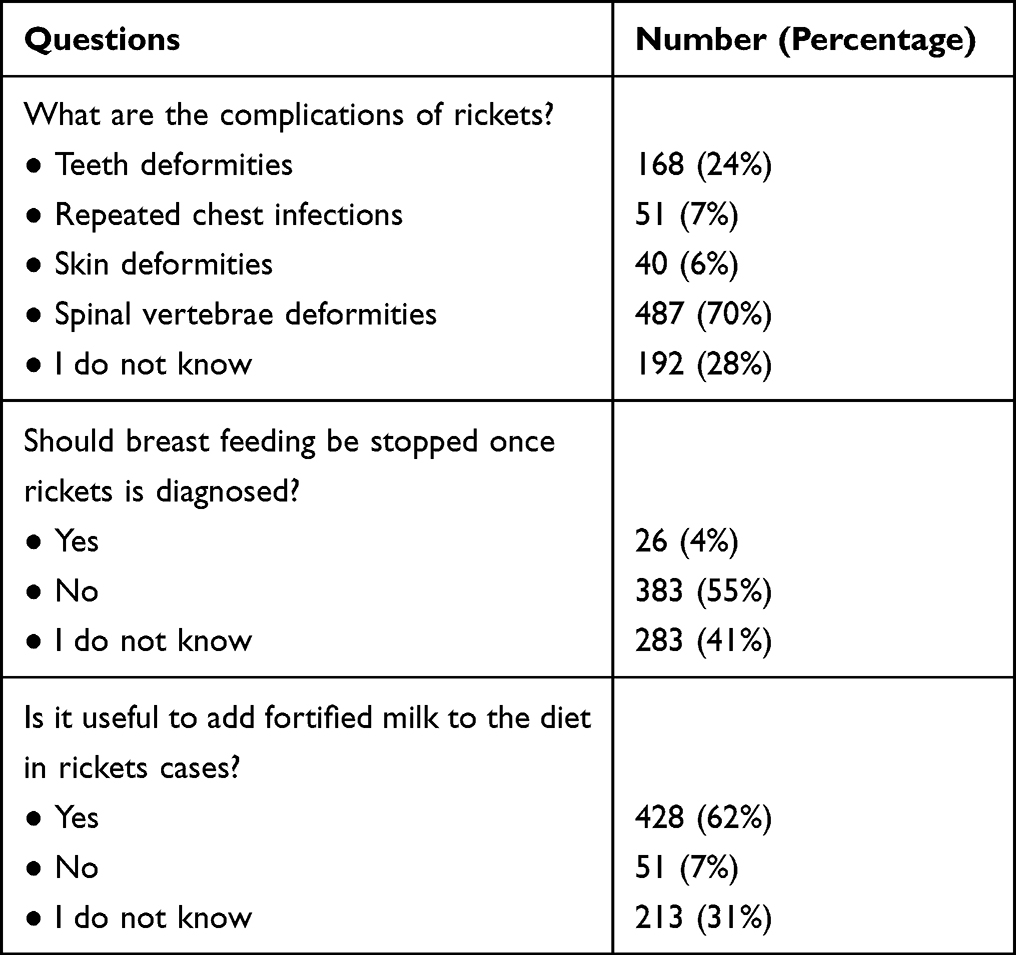 |
Table 5 Participants’ Responses to Complications and Breast-Feeding Questions (Number = 692) |
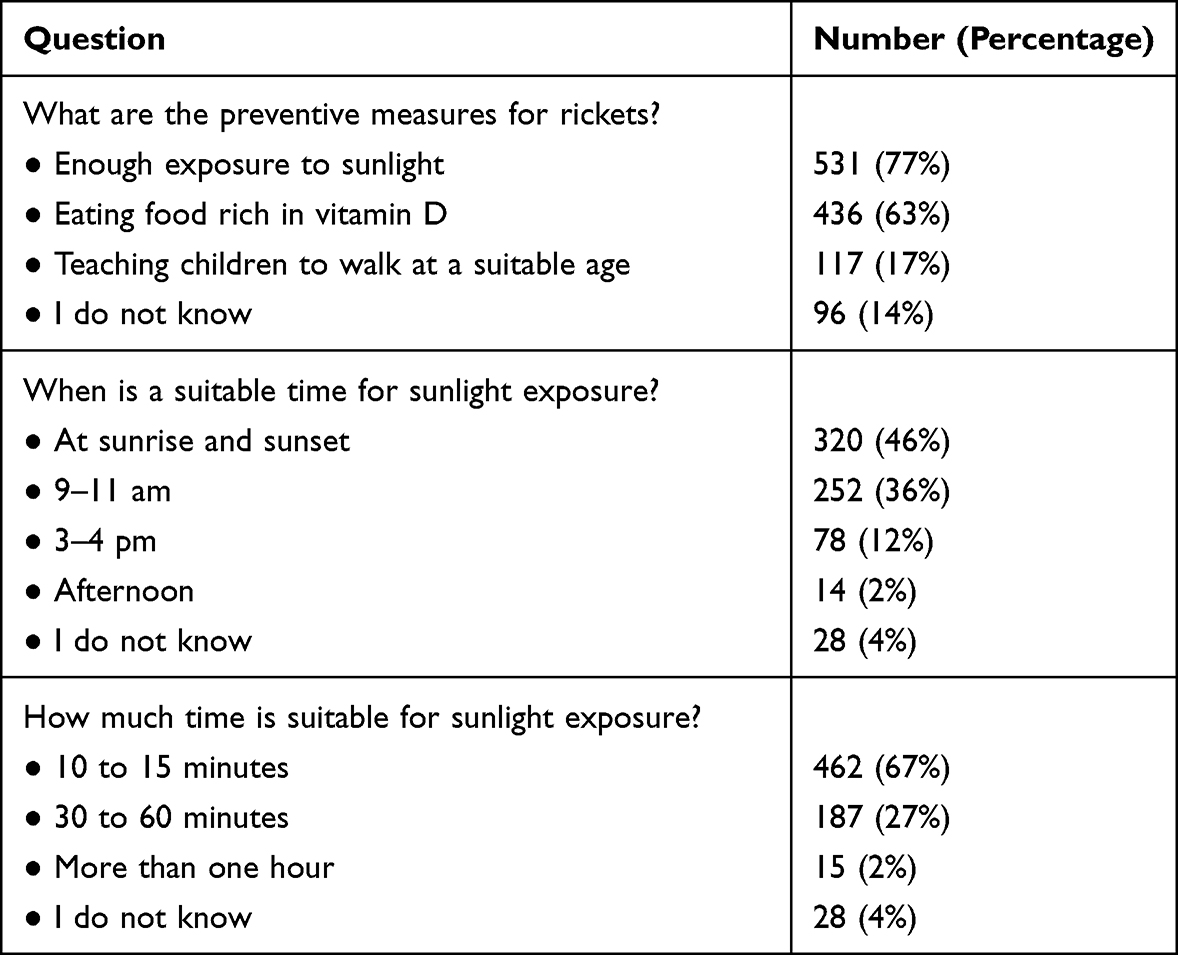 |
Table 6 Participants’ Responses to Rickets Prevention Questions (Number = 692) |
Discussion
In a similar study, Khalifa et al had measured awareness, knowledge, perception, and sources of information about rickets and its related risk factors in the Eastern Region of KSA through a self-administered electronic questionnaire. A total of 422 had participated in the study, among them 62.8% had low level of knowledge about rickets and the commonest source of their information was the internet (44.1%)7 compared to (99%) heard about rickets in our study with the main sources of information were mass-media, television, and newspapers (43%).
The overall knowledge score of participants for rickets was in our study was 11.6 ±2.4 out of 17, and the score had a negative correlation with age below 18 years and low education (basic education). So, from all these results, we concluded the need to spread awareness and knowledge among the people in Al-Baha region, and a similar conclusion was obtained by Fahad et al in their hospital-based study that performed in 150 mothers with their children attending Maternal Child Health Hospital in Taif city, KSA. Their study aimed to investigate the knowledge and awareness of mothers about rickets and to correlate this with vitamin D level of their children. The results showed that there were 146 (97.3%) of children with vitamin D deficiency. So, they had reached the same conclusion, as in our study, that there was a need for campaigns that spread awareness among mothers and young adult females about the nutritional prevention of rickets.8
Also, in a similar study conducted by Abdulmoein Eid Al-Agha (2016) in Jeddah city, KSA, they assessed awareness, perception and understanding of vitamin D deficiency among families living in Jeddah. Determining the resources of information about vitamin D deficiency in the society. The study was conducted on 1752 parents of children aged from 2 to 18, and dividing them into 746 highly educated, 491 low educated.
It was found that the highly educated parents got the right answers in most of the questions, however both high and low education parents had the media as their source of information. The majority have heard about vitamin D.9 Almost similar results were obtained in our study that educated got the higher knowledge score and the mass media was the main source for information.
Alamoudi et al had conducted a similar study in Jeddah city, KSA, to assess the knowledge about rickets in general population. Their knowledge mean score was 5.9 ± 1.2 (39.3%)10 compared to ours of 11.6 ± 2.4 out of 17. Both studies had confirmed the strong association between the high knowledge score and the high level of education.
Conclusion
Most of the people in the Al-Baha area had heard about rickets disease (99%), but the average knowledge score was 11.6 ± 2.4 out of 17 for clinical features, causes, risk factors, complications, and prevention measures. The knowledge score was negatively correlated with maternal age below 18 years (5.2 ± 2.4) and basic education (4.7 ± 2.4).
Recommendations
There should be coordination between health-education programs for rickets disease and mass media. Rickets health-education programs should make the best use of social media. Programs should also focus on rural communities where maternal age and educational levels are low.
Health-education campaigns should consider educating mothers to take calcium and vitamin D supplements during pregnancy and all throughout lactation.
Informed Consent Statement
We confirm that informed consent was obtained from all subjects involved in the study prior to study commencement.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by an Education, Training Center & Academic Affairs Scientific and Research Committee at King Fahad Hospital, Al Baha, Saudi Arabia, Ref Number KFH/IRB/21122021/5.
Data Sharing Statement
The datasets are available from the corresponding authors upon reasonable request and IRB approval.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. This research received no external funding.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Creo AL, Thacher TD, Pettifor JM, et al. Nutritional rickets around the world: an update. Paediatr Int Child Health. 2017;37(2):84–98. doi:10.1080/20469047.2016.1248170
2. Pettifor JM. Nutritional rickets: deficiency of vitamin D, calcium, or both? Am J Clin Nutr. 2004;80(6):1725S–9S. doi:10.1093/ajcn/80.6.1725S
3. Florin TM, Ludwig S, Aronson PL, Werner HC. Netter’s pediatrics. E H Sci. 2011;2011:430.
4. Prentice A. Nutritional rickets around the world. J Steroid Biochem Mol Biol. 2013;136:201–206. doi:10.1016/j.jsbmb.2012.11.018
5. Fiscaletti M, Stewart P, Munns CF. The importance of vitamin D in maternal and child health: a global perspective. Public Health Rev. 2017;38(1):19. doi:10.1186/s40985-017-0066-3
6. Gartner LM, Greer FR. Prevention of rickets and vitamin D deficiency: new guidelines for vitamin D intake. Pediatrics. 2003;111(4 Pt 1):908–910. doi:10.1542/peds.111.4.908
7. Khalifa M. Knowledge and awareness about rickets disease in Eastern Region of Saudi Arabia. Int J Med Develop Countries. 2021;5(4):1051–1059.
8. Fahad AS, Nouf AZ, Mohammed AS, et al. Knowledge and attitude practice of rickets disease among mothers in KSA. Egypt J Hosp Med. 2018;72(6):482–485.
9. Eid Al-Agha A, Alorabi SH, Saeed SM, Shalabi NM. Awareness of vitamin D and its deficiency in Jeddah Population, Saudi Arabia. J Comm Pub Health Nurs. 2016;2(2):2. doi:10.4172/2471-9846.1000120
10. Alamoudi LH, Almuteeri RZ, Al-Otaibi ME, et al. Awareness of vitamin D deficiency among the general population in Jeddah, Saudi Arabia. J Nutr Metab. 2019;4138187:7.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.