")
Back to Journals » International Journal of Women's Health » Volume 12
Perception Determinants of Women and Healthcare Providers on the Effects of Oil Pollution on Maternal and Newborn Outcomes in the Niger Delta, Nigeria
Authors Oghenetega OB, Ojengbede OA, Ana GREE
Received 21 October 2019
Accepted for publication 20 February 2020
Published 25 March 2020 Volume 2020:12 Pages 197—205
DOI https://doi.org/10.2147/IJWH.S235536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Onome B Oghenetega,1 Oladosu A Ojengbede,2 Godson REE Ana3
1Pan African University Life and Earth Sciences Institute, Department of Obstetrics and Gynecology, College of Medicine, University of Ibadan, Ibadan, Oyo State, Nigeria; 2Department of Obstetrics and Gynecology, College of Medicine, University College Hospital, University of Ibadan, Ibadan, Oyo State, Nigeria; 3Department of Environmental Health, Faculty of Public Health, University of Ibadan, Ibadan, Oyo State, Nigeria
Correspondence: Oladosu A Ojengbede
Department of Obstetrics and Gynecology, College of Medicine, University College Hospital, University of Ibadan, Ibadan, Nigeria
Tel +23 480 3442 6047
Email [email protected]
Purpose: This qualitative study examined the perception determinants of women and their local healthcare providers on exposure to oil pollution and its adverse effects on maternal and newborn outcomes in selected communities with history of oil spillage and gas flaring in the Niger Delta region of Nigeria.
Participants and Methods: Thirty-nine participants were used in this study, which included community women leaders (n=2), women of reproductive ages (n=32) and healthcare providers (n= 3 female nurses and 2 male doctors) in the selected communities in the Niger Delta region of Nigeria. The participants were chosen through purposive sampling. Focus group discussions (FGDs) and in-depth interviews (IDIs) were conducted among the participants and recorded in line with research protocols. The recordings of the FGDs and IDIs were transcribed, coded and analysed using Nvivo 10.
Results: Four major themes emerged relating to the perception determinants of women and healthcare workers on the effects of oil pollution on maternal and newborn outcomes. The first theme relates to the fact that personal experiences influence risk perception. The second theme associated perception with cultural norms, values and practices. The third theme shows that perception is influenced by the level of environmental threat or hazard, while the fourth theme borders around the influence of hospital-related factors on risk perception.
Conclusion: The study strongly suggested that both women and local healthcare providers perceived that oil pollution could have adverse effects on maternal and newborn outcomes. However, their perceptions were influenced by the cultural beliefs of the people, individual experiences, environmental and hospital-related factors. We believe that increasing awareness on the importance of attending antenatal care during pregnancy, making hospital charges affordable for pregnant women, and general environment conduciveness will improve maternal and newborn health in communities affected by oil pollution in the Niger Delta region.
Keywords: oil spill, gas flaring, perception, maternal and newborn health, Niger Delta
Introduction
Maternal and newborn outcomes are important public health concerns. This is because adverse maternal and newborn events are still the leading cause of maternal and perinatal mortality, and childhood disability in most developing countries. The World Health Organization (WHO), in 2018, reported that 99% of maternal deaths and more than 37% of newborn deaths occur in developing countries among women and children living in poor communities.1,2 Recognizing this challenge, maternal and child mortality reduction remains a priority under Sustainable Development Goal (SDG) 3, which focuses on ensuring healthy lives and promoting wellbeing for all, regardless of age, by reducing the global maternal mortality ratio to less than 70 per 100,000 live births; and reducing neonatal mortality to as low as 12 per 1,000 live births; increasing universal access to quality maternal, newborn, sexual and reproductive healthcare services, amongst other strategic targets.3,4
Although a number of factors have been associated with adverse pregnancy outcomes, there is growing evidence that the environment can play an important role in pregnancy outcomes. Environmental factors have been observed to interact with genetic factors to trigger genetic mutations leading to maternal and newborn complications.5 Pregnant women living in crude oil-polluted communities, both in terms of oil spill and gas flaring, therefore face endemic threats to their health and that of the newborns.5 Exposure to any form of pollutants has been linked to adverse pregnancy and developmental outcomes.5–9 Studies have examined the effects of air pollution on birth outcomes and its implicated negative consequences on foetal growth such as low birth weight or preterm birth, development and duration of pregnancy.5–8 Moreover, slight perturbations caused by chemical exposures during sensitive periods of foetal development can lead to increased risks of disease and disability throughout the life of an individual.9
It is believed that the way people perceive risk and the level of attention given to potential risks go a long way to determine wellbeing. Ferrer and Klein noted that risk perception influences health decision-making, health-seeking behaviour and health outcomes.10 In any given population, country or community, perceptions are formed based on the extent of threat a particular risk portends.10 If a situation is perceived as threatening, risk perception is high; however, if the situation is viewed as less threatening, the perception of risk is low. Hence, perception of risks influences responses to situations. Though people residing in oil spill environments are prone to health problems, pregnant women and the newborns are subgroups that are more vulnerable to these adverse health complications and outcomes. This is because any substance that can cross the placenta can influence the development of the foetus, and has the potential to alter the developmental process.11,12 Studies depicting the risk perception of oil pollution on adverse maternal and newborn outcomes, especially from the perspective of women, are scarce.
This study was, therefore, designed to examine the perception determinants of women and local healthcare providers on the effects of oil pollution on maternal and newborn outcomes in selected oil-polluted communities in the Niger Delta region of Nigeria.
Participants and Methods
Study Area
The Niger Delta region of Nigeria is the major area in the country where crude oil exploration and production takes place. Crude oil accounts for approximately 90% of the country’s revenue, providing more than 90% of the total export.13 The region consists of nine crude oil-producing states which are clearly different from the South-south geopolitical zone in Nigeria. These nine states are Akwa Ibom, Rivers, Delta, Bayelsa, Edo, Cross Rivers, Abia, Imo and Ondo. The region houses many communities and oil facilities with extensive off/on-shore oil production activities and propensities for pollution through oil spills and/or gas flaring.
Research Design
The study employed a descriptive qualitative research design and semi-structured interview guides to obtain data from respondents. Focused group discussions (FGDs) and In-depth Interviews (IDIs) were used to collect data from purposively selected participants in the study area that fall within the study population. FGDs and IDIs were held with women and healthcare providers in five (5) selected communities affected by oil pollution in the Niger Delta region in Nigeria. The data presented in this paper are part of a larger study on oil pollution and pregnancy outcomes in the region.
Study Population and Sample
The population comprised women leaders, women of reproductive age (15–49 years) and healthcare providers living in oil-polluted communities in Niger Delta region of Nigeria. The study employed a qualitative technique and the sample size was purposively selected. Participants were recruited into the study through snowballing and referral methods. Data were collected from women who resided in the affected communities as well as healthcare providers in this communities. Five communities were sampled from Delta and Rivers States in the region. This was due to the presence of crude oil refinery in these States and the high incidence of crude oil spills according to the Nigerian Oil Spill Monitor. Data were collected using Focused Group Discussions (FGDs) and In-depth Interviews (IDIs). Five FGDs were conducted among women of reproductive age (n=32), seven IDIs were conducted among key-informants which include healthcare provider ((n=5); 3 female nurses and 2 male doctors)), as well as community women leaders (n=2) in the affected oil-polluted communities, making a total of 39 participants. In this study, however, no participant below the age of 18 was included.
Data Collection
The FGDs and IDIs were held between August 2018 and October 2018, to capture the perceptions of women and local healthcare workers on the effects of oil pollution on maternal and newborn outcomes. The FGDs and IDIs were facilitated by the researcher using FGD and IDI guidelines.
Each focused group discussions involved 6–8 participants. It was conducted in a conducive environment where the participants were free to express their opinions without fear or intimidation. Although each FGD was conducted in the open air, privacy and avoidance of undue interferences were ensured as shown in Figure 1. The FGD guide designed for women of reproductive age contained 10 questions bordering around their experiences with oil spills and gas flaring; their experiences on maternal and child outcomes in their communities, as well as their perceptions on the effects of oil pollution on maternal and child health and/or outcomes (Supplementary Material).
 |
Figure 1 An FGD with women of reproductive age. Note: Verbal informed consent was obtained from each participant for the image to be published with their faces covered. |
The IDI guide designed for healthcare providers contained 11 questions relating to the perception of the health risk and threat of oil pollution on the health of pregnant women and their unborn children in the area (Supplementary Material). The IDI guide designed for women leaders contained 17 questions relating to their knowledge on oil pollution and their perception of the health risks it portends for pregnant women and their newborns (Supplementary Material). Prior to entry into the study, participants were briefed on the purpose of the study and written informed consent was obtained from each participant. The FGDs and IDIs were conducted in the English Language.
Data Analysis
Data were generated for the study from FGDs and IDIs recordings which were transcribed. The transcripts were imported into NVivo 10 (a qualitative data analysis software), coded based on emerging themes as well as pre-identified themes from the research questions and objectives of the study. Coded results were properly checked, to avoid misrepresentation of data.
Theory
The Risk Perception Theory is used as an explanatory guide in this study. Risk perception is subjective or personal assessment that people make about a threat or hazard in relations to health or the environment. Risk perception involves evaluation of the probability as well as the consequences of a negative outcome.14 In health context, risk perceptions have implications for the overall well-being of a person or a people. Risk perception can either be high or low; optimistic or pessimistic, depending on the level of risk perceived.14 However, perception of risk, sometimes goes beyond the individual. It could be part of social and cultural construct reflecting values, symbols, history, and ideology.14 Similarly, risk perceptions tend to vary between communities and countries depending on the prevailing circumstances; what the people choose to discuss, what cultural norms are viewed as important, as well as what technical and legal opportunities exist for control and regulation of such risks. In other words, risk perception differs as an effect of cultural, environmental, and governmental influences.15 The Risk Perception Theory used in this study is represented by the conceptual framework in Figure 2.
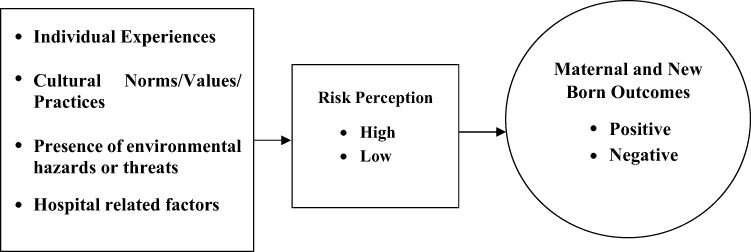 |
Figure 2 The conceptual framework for the study. |
Ethical Approval
Approval for the work was given by the Ethics Review Committee of University of Ibadan, Nigeria. Written informed consent was obtained from each participant and the study was conducted in accordance with the Declaration of Helsinki. In this study, women of reproductive age were 15–45 years. However, no participant was below the age of 18.
Results
The result shows that a total of 39 participants were used for the FGDs and IDIs in this study; 32 (82.1%) of the participants were women of reproductive age with median age of 29.5, 2 (5.1%) were community women leaders with median age of 51, and 5 (12.8%) were healthcare provider with median age of 38.5. The women of reproductive age were used for FGDs, while both the community women leaders and healthcare providers were used for the IDIs. Majority of the participants were artisans/traders who had resided in the oil-polluted communities for over 20 years.
Four main themes emerged from the FGDs and IDIs conducted. These are the influence of individual or personal factors, cultural factors, environmental factors and hospital-related factors on perceived effects of oil pollution on maternal and newborn outcomes.
Individual Factors and Perception of the Effects of Oil Pollution on Maternal and Newborn Outcomes
Majority of the study participants in the present study agreed that oil pollution may have adverse effects on maternal and newborn outcomes. This attribution is based on what some of them have experienced as well as the seeming prevalence of oil pollution in the area. Some of the women said:
Some of the women give birth wrongly (presentation of the foetus during delivery). Some of the children had birth defects when they were given birth to … some of them, the defect is in their eyes, some their legs, some the defects in their mouths. But in the olden days, it was not like that. FGD,
Women (15–49 years), Uviamughe Community, Delta State
Most women in this community have experienced miscarriages. Even my mummy has had two miscarriages in this community because she drinks the river water in this community. FGD,
Women (15–49 years), Kurugbene Community, Delta State
It has happened in this community; my sister has experienced it, she gave birth to her baby in the seventh month, the baby could not survive, so the baby died. FGD,
Women (15–49 years), Kurugbene Community, Delta State
Findings in this present study showed that majority of pregnant women in the oil-polluted communities appear to prefer patronizing Traditional Birth Attendants (TBAs). Their perception is that TBAs counselling and prayers including the use of herbs and traditional practices can mitigate the effect of oil pollution on adverse maternal and newborn outcomes. There are two types of TBAs in this area; church-based and non-church-based TBAs. Church-based TBAs are owned by local churches where prayers and pastoral counselling are offered. They also recruit non-skilled midwives who are deemed experienced due to long-time practice in aiding mothers during childbirth. The non-church-based TBAs are owned and run by these same non-skilled midwives, who make use of herbs and native practices. Inability to pay hospital bills seems to play a major role in the patronage of these TBAs who are perceived to be relatively cheaper. The practice is encouraged and sustained by women who have patronized the TBAs before and make referrals to others based on their experience. Despite the fact the TBAs cannot handle complications arising during delivery, most pregnant women still prefer to patronize them than rather than go to healthcare centres where potential emergencies can be properly handled. One of the FGD participants said:
They (pregnant women) often go to church that has midwives that attend to them and also pray for pregnant women … most times, they go for traditional check-up. We do take care of our pregnant women traditionally … FGD,
Women (15–49 years), Bodo Community, Rivers State
When asked why some of the women in the study area prefer to use traditional birth attendants during delivery, it was gathered that the services of the traditional birth attendants are cheaper than the government established health centres. Some of the respondents explain this succinctly:
… their fee (at the hospital) is just too much even drugs are quite expensive … lack of money to pay hospital bills make pregnant women go to local birth attendants … FGD,
Women (15–49 years), Bodo Community, Rivers State
Some of the pregnant women who register in churches (TBA), suffer more complications. After birth, they come to the hospital with complications like low birth weight, defects, anaemia and abnormalities … Most of the pregnant women prefer registering with TBAs … some of the pregnant women do complain about not having enough money for the registration (antenatal registration) … IDI,
Chief Nursing Officer, General Hospital, Bodo, Rivers States
The Chief Antenatal Nursing Officer, General Hospital, Bodo said:
Some of the pregnant women do complain about not having enough money for the registration. Most of the pregnant women prefer registering in TBA’s. IDI,
Chief Antenatal Nursing Officer, General Hospital, Bodo, Rivers States
Finance is a key influence on perception. When poverty prevails in an area, there is a tendency to not pay the required attention to threatening health symptoms.
Cultural Factors and Perception on the Effects of Oil Pollution on Maternal and Newborn Outcomes
Findings in this study suggested that though oil spill and gas flaring have been found to contribute negatively to pregnancy outcomes, the people still hold on to traditions and cultural values that forbid them from disclosing any issues relating to their pregnancy and the outcomes to non-family members. Culture also dictates that some actions or practices are adhered to. For example, women who had experienced stillbirths were forbidden from going to the farm until they have undergone certain traditional rites.
Respondents have this to say:
It (oil pollution) affects the pregnant women and their children, it makes them have miscarriages … we have many cases of stillbirth in this community and the community also forbids stillbirths. A woman who has had stillbirth is usually restricted from going to the farm until she performs some traditional rites … and this sometimes affects the woman’s livelihood. FGD,
Women (15–49 years), Uviamughe Community, Delta States
… we don’t disclose issues of pregnancy to outsiders, myself (I) can never disclose any issue about my current pregnancy even if I am being diagnosed of a critical sickness, that will affect the health of my baby and me; still, I will tell nobody. That is how it is here in Bodo. FGD,
Women (18–49 years), Bodo Community, Rivers States
I have a sister, who lost two of her babies immediately after she delivered each of them, before visiting the hospital to give birth to the third child who is alive. She is currently pregnant; I asked her about what the doctors said was responsible for the death of her babies, she said nothing, even if she was diagnosed of any health complications … she won’t tell me. FGD,
Women (18–49 years), Bodo Community, Rivers States
This finding in the present study seems to suggest that, even when pregnant women are experiencing challenging health symptoms, they are expected to keep it to themselves because that is the norm in the community. Community members believed that pregnancy is a family and private issue and should, therefore, not be discussed with outsiders, even neighbors. With such cultural norms, and since they are reluctant to go to the hospital for antenatal care, it becomes difficult to identify women who may require referral to appropriate health centres for appropriate medical attention. Cultural beliefs and norms have key influence on perception. When there is lack of awareness on the threatening health effects of a hazard in a community, there is a tendency to explain everything away as having spiritual or cultural undertone and treating threatening health risk with inappropriacy.
Environmental Factors and Perception on the Effects of Oil Pollution on Maternal and Newborn Outcomes
Respondents in this study agreed that water in the study area was highly polluted and residents had no alternative sources of clean water. This suggests that residents including the pregnant women had no choice but to consume such water, and this has the potential to impact negatively on their health. Community members believe that increased incidences of miscarriage, birth defects, and stillbirths among others, is directly due to the consumption of unsafe water and other polluted items. Some of the respondents said:
… The water is not clean; it is not filtered. So, it affects them (pregnant women) … pregnancy defect is … as a result of the oil spillage … majority of the problem we are having is as a result of the oil spillage. FGD,
Women (18–49 years), Bodo Community, Rivers States
Findings in the present study showed that healthcare providers working in the oil spill affected communities are also of the firm opinion that oil spills and gas flaring is detrimental to the health of pregnant women and their newborns. The medical professionals explained that pregnant women living in the area, seem to have a higher possibility of experiencing miscarriages, preterm births, congenital malformation, pre-eclampsia and eclampsia. The excerpts explain this further:
… pregnant women living in areas where there is oil spills or recurrent gas flaring, face the possibility of miscarriage, preterm delivery, congenital malformations …. Some women present with miscarriage, preterm delivery; some come with hypertensive disorders of pregnancy such as preeclampsia and eclampsia, as well as postpartum haemorrhage from various causes. The foetuses come with intrauterine death. Congenital malformation is quite common in this environment … IDI,
Consultant (Obstetrics and Gynaecology), Central Hospital, Ughelli
… at the first trimester, it is more of miscarriage, low birth weight; at the second trimester and at the third trimester, it is pregnancy-induced hypertension. IDI,
Resident Doctor, Central Hospital, Warri
The crude oil contains chemical components that if ingested at the first trimester can cause miscarriage, low birth weight and intrauterine growth restriction … IDI,
Resident Doctor, Central Hospital, Warri
However, the healthcare practitioners made it clear that though these health outcomes seem to be common in the area, they cannot exclusively be linked to oil pollution. They could also be as a result of other reasons such as failure to attend antenatal care in order to detect any complications early. Some of the respondents said:
… some women present with miscarriage, preterm delivery; some come with hypertension disorders of pregnancy such as preeclampsia and eclampsia. Some come with obstructed labour, ruptured uterus and some come with postpartum haemorrhage from various causes. The foetuses come with intrauterine death; the congenital malformation is quite common in this environment but I won’t boldly link it all to oil pollution. IDI,
Consultant (Obstetrics and Gynaecology), Central Hospital, Ughelli
Pregnant women and their newborns face potentially adverse health complications in these oil-polluted communities. Sources of drinking water and food appear to be contaminated; majority of these women appear unable to afford medical bills, hence patronize local birth attendants that may not be able to handle complications when they occur, thereby jeopardizing the health and life of mother and child.
Hospital Services Related Factors and Perception on the Effects of Oil Pollution on Maternal and Newborn Outcomes
In this study, findings showed that the way hospital services are rendered by healthcare providers seem to affect the view of women about presenting themselves for antenatal care, thereby making them more vulnerable to the adverse effects of oil pollution on pregnancy and its outcomes. Excerpt from one of the FGD explains this further:
… most times, whenever you go to the hospital, you won’t meet the doctors in the hospital, so no need going to the hospital. FGD,
Women (18–49 years), Bodo Community, Rivers States
However, healthcare providers think otherwise:
Some of the pregnant women register in churches (TBAs) … they prefer TBAs where families and friends will have unlimited access to them …. … because of the hospital settings … they opt for lesser time not knowing the consequences involved. … After birth, they come to the hospital with complications like low birth weight, defects, anaemia and abnormalities. IDI,
Chief Antenatal Nursing Officer, General Hospital, Bodo, Rivers States
Discussion
This study was designed to examine the perception determinants of women and local healthcare providers on the effects of oil pollution on maternal and newborn outcomes in selected oil-polluted communities in the Niger Delta region of Nigeria. The findings revealed that a number of factors influence the perception of women and local healthcare providers on the effects of oil pollution on maternal and newborn outcomes. The cultural beliefs of the people, individual experiences, environmental issues as well as hospital-related issues, all influence how women and the local healthcare providers perceive health risks emanating from oil pollution.
The perception of women on the effects of oil pollution on maternal and newborn outcomes is influenced by the cultural practices, norms and values of the communities. In some of the communities in the oil-polluted areas, their culture does not permit disclosure on issues or complications resulting from pregnancy. Therefore, these particular women were unwilling to disclose their pregnancy-related issues and this made it difficult to ascertain the personal experiences of these women on the perceived adverse effects of oil pollution on maternal and newborn health. However, this only impeded getting information from one particular community. Furthermore, there are certain traditional practices such as restraining women who had experienced stillbirths from going to the farm until they performed some traditional rites. These practices are perceived to affect their livelihood and the psychosocial health of the women. This is in contrast to the study of Ajiboye and Adebayo who reported that majority of the pregnant women and their spouses do not believe that cultural practices have negative correlates with pregnancy outcomes.16 However, the findings of the present study are in agreement with the study of John et al on indigenous childcare beliefs and practices in Niger Delta, which revealed that there are several beliefs and customs regarding the care of the newborn that are held in high regard by residents, some of which are actually injurious to the health of the newborn.17
Cost of seeking healthcare emerged as one of the major influences on the perceived risk of oil pollution on maternal and newborn outcomes. Due to financial limitations and alleged poor healthcare services, most pregnant women seemed to prefer Traditional Birth Attendants which they perceive to be relatively cheaper disregarding the fact that these TBAs may not have the professional training necessary to manage possible adverse pregnancy outcomes during gestation and childbirth. This is in tandem with the study of Igboanugo and Martins, which showed that lack of finances deterred childbearing women in the Niger Delta region of Nigeria from accessing essential medical care.18 However, the local healthcare providers opine that hospital charges are moderate and the services provided are adequate. They indicated that pregnant women preferred patronizing the TBAs because they seemed cheaper and they gave unrestricted access to family members to visit the mother and her newborn, which is part of their social norms. Giving credence to the above proposition, Ugboaja et al postulated that TBAs enjoy high patronage due to the respect they accord the culture and social norms of the people.19 Moreover, prayers been organized including the use of herbs and traditional practices in the TBAs is perceived by the pregnant women to mitigate the effect of oil pollution on maternal and newborn health in this study. This is consistent with the study of Ayede which reported that organizing prayers is one of the attractive roles of the TBAs that encourage the persistent use of TBAs by expectant mothers.20 However, the local healthcare providers insisted that in cases when complications occur at the TBA centres, the hospital becomes their last hope to avert a crisis. Thus, they recommended that early registration for antenatal services would help to ameliorate the possible adverse effects of oil pollutions on pregnancy outcomes.
The adverse effects of the oil spill and gas flaring have led to several devastating environmental consequences in Nigeria’s Niger Delta with the attendant repercussions on human health. Participants in the study seem to suggest that consumption of crude oil-contaminated food and water has played a role in increased incidences of miscarriages, stillbirths and infant deaths among women living in the oil-polluted communities. This is consistent with the study of San Sebastian who reported a strong association between oil pollution and miscarriage and the study of Bruederle and Hodler who reported that pregnant women exposed to oil pollution are more likely to have infant death.21,22 Moreover, the WHO 2018 report on air pollution and child health, suggested that both prenatal and postnatal exposure to pollutants can have adverse effects on newborn outcomes.11 Participants in this study seemed to have a unanimous perception that oil-polluted environment had adversely affected maternal and newborn health outcomes in the study area and this agreed with the findings of Al-Hadithi, et al, Al-Sabbak et al and Khader et al.5,9,23
Limitations
Data collection and analysis process was solely dependent on the researcher’s skills which could affect the quality of the data. To an extent, this bias was reduced by engaging two skilled researchers and a moderator in the interviews and FGDs. More so, we were unable to recruit participants from very volatile and hard to reach communities among the oil-polluted communities because of the volatility and terrain of the Niger Delta region. As such, the perspectives of such group of women were not well captured in the study. The participants in this study were mainly from the rural areas and were purposively selected, which could have caused selection bias. In spite of these limitations, the study still suggests useful insights into the perception determinants of women and local healthcare provider on the adverse effects of oil pollution.
Conclusion
This paper examined the perception determinants of women and local healthcare providers regarding the effects of oil pollution on maternal and newborn outcomes. The study strongly suggested that both women and local healthcare providers agreed that oil spills and gas flaring could have adverse effects on maternal and newborn outcomes. However, their perceptions were influenced by a number of factors such as their cultural beliefs, individual experiences, environmental and hospital-related factors.
It is recommended that safe and clean water be made available to the people, especially the pregnant women and children that are more vulnerable to the adverse effects of oil pollution in the oil-polluted communities. Also, crucial is the need for more awareness amongst pregnant women on the importance of receiving antenatal care and the use of healthcare facilities during delivery, instead of home delivery with traditional birth attendants who may not be able to handle potential emergencies.
Acknowledgments
The authors acknowledge the sponsorship of this study by Pan African University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Newborns: reducing mortality. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality.
2. WHO. Maternal mortality. Available from: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality.
3. Aminu M Sustainable development goals: what is in it for maternal and newborn health? Centre for maternal and newborn health. Liverpool School of Tropical Medicine. Available from: https://cmnh.lstmed.ac.uk/sustainable-development-goals-what-is-in-it-for-maternal-and-newborn-health-0.
4. Kalipeni E, Iwelunmor J, Grigsby-Toussaint D. Maternal and child health in Africa for sustainable development goals beyond 2015. Glob Public Health. 2017;12(6):643–647. doi:10.1080/17441692.2017.1304622
5. Al-Hadithi TS, Al-Diwan JK, Saleh AM, Shabila NP. Birth defects in Iraq and the plausibility of environmental exposure: a review. Confl Health. 2012;6:3. doi:10.1186/1752-1505-6-3
6. Dugandzic R, Dodds L, Stieb D, Smith-Doiron M. The association between low level exposures to ambient air pollution and term low birth weight: a retrospective cohort study. Environ Health. 2006;5:3. doi:10.1186/1476-069X-5-3
7. Ballester F, Estarlich M, Iñiguez C, et al. Air pollution exposure during pregnancy and reduced birth size: a prospective birth cohort study in Valencia, Spain. Environ Health. 2010;9:6.
8. Santos V, Medeiros AP, Lima TA, Nascimento LF. The effect of air pollutants on birth weight in medium-sized towns in the state of São Paulo. Rev Paul Pediatr. 2014;32(4):306–312. doi:10.1016/j.rpped.2014.06.003
9. Al-Sabbak M, Ali SS, Savabi O, Savabi G, Dastgiri S, Savabieasfahani M. Metal contamination and the epidemic of congenital birth defects in Iraqi Cities. Bull Environ Contam Toxicol. 2012;89:937–944. doi:10.1007/s00128-012-0817-2
10. Ferrer R, Klein WM. Risk perceptions and health behaviour. Curr Opin Psychol. 2015;1(5):85–89.
11. WHO. Air pollution and child health: prescribing clean air (Advance copy). Available from: https://www.who.int/ceh/publications/Advance-copy-Oct24_18150_Air-Pollution-and-Child-Health-merged-compressed.pdf.
12. Zheng T, Zhang J, Sommer K, et al. Effects of environmental exposures on fetal and childhood growth trajectories. Ann Glob Health. 2016;82(1):41–99. doi:10.1016/j.aogh.2016.01.008
13. Akpan NS, Akpabio EM. Oil and conflicts in the Niger Delta region, Nigeria: facing the facts. J Soc Dev Afr. 2009;24(1).
14. Sjöberg L, Moen BE, Rundmo T. Explaining Risk Perception. An Evaluation of the Psychometric Paradigm in Risk Perception Research. Rotunde Publikasjoner Rotunde. Vol. 84. 2004;55–76.
15. Keown CF. Risk perceptions of Hong Kongese vs. Americans. Risk Anal. 1989;Sep(3):401–405. doi:10.1111/j.1539-6924.1989.tb01005.x
16. Ajiboye OE, Adebayo KA. Socio-cultural factors affecting pregnancy outcome among the ogu speaking people of badagry area of Lagos State, Nigeria. Int J Humanit Soc Sci. 2012;2:133–144.
17. John ME, Nsemo AD, John EE, et al. Indigenous child care beliefs and practices in the Niger Delta region of Nigeria: implications for health care. Int J Health Sci Res. 2015;5(11):235–247.
18. Igboanugo GM, Martins CH. What are pregnant women in a rural Niger delta community’s perceptions of conventional maternity service provision? An exploratory qualitative study. Afr J Reprod Health. 2011;15(3):59.
19. Ugboaja JO, Oguejiofor CB, Oranu EO, Igwegbe AO. Factors associated with the use of traditional birth attendants in Nigeria: a secondary analysis of 2013 Nigeria national demography and health survey. Niger J Gen Pract. 2018;16:45–52. doi:10.4103/NJGP.NJGP_27_17
20. Ayede AI. Persistent mission home delivery in Ibadan: attractive role of traditional birth attendants. Ann Ib Postgrad Med. 2012;10(2):22–27.
21. San Sebastian M, Armstrong B, Stephens C. Outcomes of pregnancy among women living in the proximity of oil fields in the Amazon basin of Ecuador. Int J Occup Environ Health. 2002;8:312–319. doi:10.1179/oeh.2002.8.4.312
22. Bruederle A, Hodler R The effects of oil spills on infant mortality: evidence from Nigeria. Munich society for the promotion of economics research. CESifo working paper No 6653; 2017. ISSN 2364-1428
23. Khader Y, Abdelrahman M, Abdo N, et al. Exposure to air pollution and pregnancy outcomes in the east mediterranean region: a systematic review. Int J Pediatr. 2016;4(1):1255–1271.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.