Back to Journals » International Journal of Women's Health » Volume 15
Perception and Comfort with Endometriosis Management Among OB/GYN Residents
Authors Sullender RT, Jacobs MB, Sandhu MS ![]() , Lacoursiere DY, Diaz Luevano C, Pickett CM, Agarwal SK
, Lacoursiere DY, Diaz Luevano C, Pickett CM, Agarwal SK ![]()
Received 6 June 2023
Accepted for publication 23 October 2023
Published 20 November 2023 Volume 2023:15 Pages 1801—1809
DOI https://doi.org/10.2147/IJWH.S424554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Renee T Sullender,1 Marni B Jacobs,1 Manpreet S Sandhu,2 D Yvette Lacoursiere,1 Carolina Diaz Luevano,1 Charlotte M Pickett,1 Sanjay K Agarwal1
1Department of Obstetrics, Gynecology and Reproductive Sciences, University of California at San Diego, La Jolla, California, USA; 2University of California at San Diego School of Medicine, La Jolla, California, USA
Correspondence: Sanjay K Agarwal, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of California at San Diego, 9500 Gilman Drive #0633, La Jolla, California, 92093, USA, Tel +1 858 534-8977, Fax +1 858 534-8856, Email [email protected]
Purpose: The diagnosis of endometriosis often takes several years, delaying appropriate care while patients suffer from pelvic pain, dysmenorrhea, and dyspareunia. Understanding whether residents in obstetrics and gynecology (OB/GYN) are being adequately exposed to and trained in the diagnosis and management of the disease is important for improving care.
Methods: We conducted an online cross-sectional survey of OB/GYN residents to investigate their comfort level and familiarity with endometriosis diagnosis and management. Residency program directors and coordinators of 20 OB/GYN residency programs in California, USA were emailed to disseminate the 31-question, anonymous survey in January to February 2023. Responses were collected using Redcap and analysis was conducted using STATA.
Results: 67 residents answered at least one non-demographic question and were included. A resident response rate was not calculated because we were unable to determine how many programs distributed the survey. 84% of residents felt they could recognise symptoms of endometriosis but over 30% of senior residents were not comfortable with sonographic diagnosis of endometrioma. Approximately one third of residents felt comfortable managing hypoestrogenic symptoms, osteoporotic risks, and add-back progestin for certain hormonal therapies. Academic-hospital based residents had significantly more exposure to attendings prescribing long-acting reversible contraception, GnRH antagonists, and GnRH agonists but there were no significant differences in trainee prescribing practices or comfort. More respondents would feel comfortable medically managing endometriosis (52%) than surgically managing the disease (26%) if they were in practice today, with only 39% of PGY3-4 residents feeling comfortable surgically managing endometriosis.
Conclusion: There is considerable room for improvement in the education of residents in the diagnosis and medical and surgical management of endometriosis.
Plain Language Summary: Given the frequent multi-year delay in the diagnosis and proper treatment of endometriosis, we wanted to evaluate whether residents in Obstetrics and Gynecology (OB/GYN) feel adequately trained to manage this disease. Through our survey, we identified that OB/GYN residents are comfortable with diagnosing endometriosis but are less confident with treatment, particularly surgical management. Only 52% of senior residents in their final 2 years of residency training report they would feel comfortable with the medical treatment of endometriosis if they were in practice today, compared to 39% reporting comfort with surgical management. Additional exposure and training during residency are essential for boosting resident comfort with disease management and therefore improving patient care.
Keywords: endometriosis, resident education, GnRH antagonists, surgical training, OB/GYN, pelvic pain
Introduction
Endometriosis is a common disease and a frequent cause of dysmenorrhea, dyspareunia, infertility, and chronic pelvic pain. An estimated 10% of women of reproductive age are predicted to have endometriosis.1 However, due to variable symptomatology, asymptomatic cases, and the lack of non-surgical definitive diagnosis, the true prevalence of endometriosis may be higher.
Beyond the physical toll, patients with endometriosis may also experience a significant decline in mental health and overall health-related quality of life. In a survey looking at the disease burden of endometriosis, patients reported increased strain on personal/social relationships, decreased workplace productivity, and a negative impact on educational achievements.2 Costs associated with the management of endometriosis are comparable to other chronic conditions, such as Type 2 Diabetes, and these expenses further exacerbate the burden of the disease on patients.1 In addition, endometriosis may have long-term implications on the health of patients, with associations between the disease and risk of cancer, autoimmune disorders, cardiovascular disease, gastrointestinal disease, and atopic conditions.3
Despite its high prevalence and impact on patients’ quality of life, there is often a significant delay in the diagnosis of endometriosis. Globally, studies estimate a delay ranging from 4–11 years from time of onset of symptoms to diagnosis.4,5 Patients may initially be misdiagnosed by their physicians with confounding conditions such as pelvic inflammatory disease or irritable bowel syndrome, further contributing to the delay in diagnosis. Patients who suffer from endometriosis may experience trivialization and somatization of their symptoms by their providers.6 Thus, adequate training of healthcare professionals on detecting endometriosis is crucial for its early diagnosis and for reducing the burden it has on patients.
Although lack of adequate exposure of healthcare professionals may contribute to the delay in diagnosis, there are limited data on the extent of endometriosis training in residency programs and the preparedness of resident physicians to handle this condition. The objective of this study was to investigate the level of comfort and familiarity with the diagnosis of endometriosis, as well as current medical and surgical management options among Obstetrics and Gynecology (OB/GYN) residents. We hypothesized that senior residents in their last 2 years of training would feel more comfortable with the diagnosis and treatment of endometriosis and that residents would feel more comfortable with medical management than surgical management. We wanted to evaluate if residents felt adequately trained to manage endometriosis as they approach graduation by inquiring about their comfort in various aspects of endometriosis care.
Materials and Methods
Study Population
An online cross-sectional survey of OB/GYN residents in California, USA was conducted. In January and February 2023, the program directors and program coordinators of all 20 civilian OB/GYN residency programs in the state of California were sent emails asking them to disseminate the survey link to their residents. The anonymous survey remained open for 8 weeks. Consent was implied by participation, as outlined in the introduction to the voluntary survey. After survey submission, respondents were eligible to enter their email address to join a lottery for gift cards. To maintain anonymity, email addresses were not linked to survey responses. The study was deemed exempt by the Institutional Review Board at the University of California at San Diego.
Survey Development
There is currently no validated tool for evaluating exposure and comfort level with endometriosis; thus, one was developed by the researchers to assess study objectives (Supplemental Material 1). To assure face validity, 3 faculty familiar with the target audience and topic reviewed the questionnaire. Secondly, focus groups of representatives from each residency year were conducted to ensure the questions were easily understood. The survey consisted of 31 questions including demographic items, educational experiences, comfort with diagnosis, medical treatment, and surgical treatment, and overall confidence level with management after graduation. Questions were either multiple choice, yes/no, or 5-point Likert-scales. There was 1 additional free text question. The survey was estimated to take 5–10 minutes to complete.
Study data were collected and managed using REDCap, a secure, web-based software platform designed to support data capture for research studies.7,8
Analysis
Chi-squared test or Fisher’s exact test were used to carry out statistical comparisons of responses between categorical groups. T-tests were utilized for continuous variables. P values of < 0.05 were considered statistically significant. Data analysis was conducted using STATA/BE 17 software.
Results
Of the 70 initial respondents, 3 answered only demographic questions and were excluded. 67 (95.5%) answered at least one non-demographic question and were included. In order to further maintain anonymity, we did not track how many programs forwarded the survey to their residents and therefore were unable to calculate a response rate.
The demographic characteristics of the respondents are in Table 1. In the United States, residents can be classified by which level of post-graduate year (PGY) after medical school they are in. Here, 3rd year residents, or PGY3s, were the most frequent respondents. Of respondents, 67% were in an academic or university-based setting and 27% were in a community hospital-based setting. Compared to community hospitals, physicians in academic settings are traditionally more focused on research and the development of new technologies and interventions, and thus may have earlier access to novel therapies.
 |
Table 1 Respondent Demographics |
Exposure and Education
93% of residents (n=62) had encountered at least 1 patient with endometriosis and 72% (n=48) had worked with at least 1 faculty member who specialized in management of endometriosis. Residents accessed a variety of resources to learn about endometriosis, with 75–85% having utilized residency lectures, UptoDate articles, professional consensus bulletins, and discussions with senior residents and attendings. Most respondents had only 1 formal lecture or teaching session on endometriosis in the past year (n=34, 51%) and 30% had none (n=20). 88% of residents (n=59) felt that in general, their attendings were knowledgeable enough about endometriosis diagnosis and management.
Diagnosis
84% of residents (n=56) reported they could reliably recognize the common symptoms of endometriosis. 95% (n=61) stated it was appropriate to treat people for a clinical diagnosis of endometriosis without obtaining a surgical diagnosis. 21% of PGY1-2 (n=6) agreed or strongly agreed to being able to recognize an endometrioma on ultrasound compared to 68% of PGY3-4s (n=26, p< 0.001). Over 30% of senior residents were not comfortable with ultrasonographic diagnosis of endometrioma.
Medical Management
98% and 97% of respondents had seen an attending prescribe or manage endometriosis with non-steroidal anti-inflammatory drugs (NSAIDs) or combined oral contraceptive pills (OCPs), respectively (Figure 1). Exposure to attendings prescribing long-acting reversible contraception (LARC) such as an intrauterine device (IUD) or the implant was more common (70%) than exposure to GnRH antagonists (55%) and agonists (58%), aromatase inhibitors (20%), and androgens (14%).
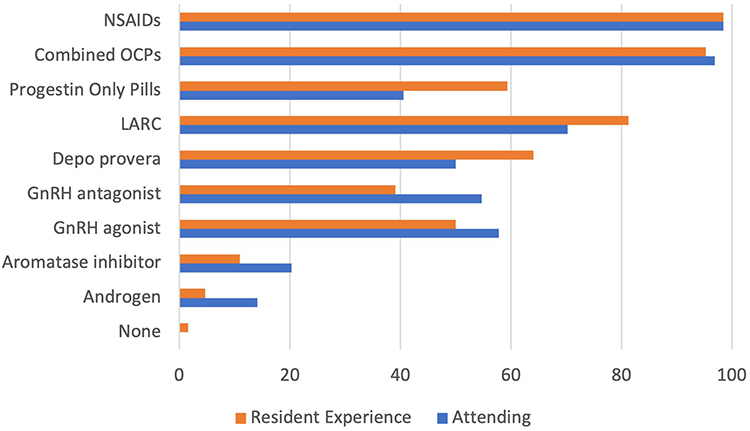 |
Figure 1 Percentage of Residents Reporting Exposure to Attending Prescription versus Personal Experience or Comfort with Prescription. |
Self-reporting of whether a resident had prescribed or would feel comfortable prescribing a medication had similar patterns to their exposure in attendings’ clinics (Figure 1). Smaller percentages of residents reported comfort with prescribing GnRH antagonists (39%) and agonists (50%), aromatase inhibitors (11%), and androgens (5%) but the differences were not statistically significant. Residents were more likely to report that they would or had prescribed progestin only pills for endometriosis compared to what they had seen their attendings prescribe (59% vs 41%, p=0.03).
Residents in academic programs were significantly more likely than residents in community programs to have exposure to attendings prescribing LARC, GnRH antagonists, and GnRH agonistsfor endometriosis (Table 2). There was a trend towards university-based residents being more likely than community-based residents to feel comfortable with LARC for management of endometriosis but this was not significant (p=0.08).
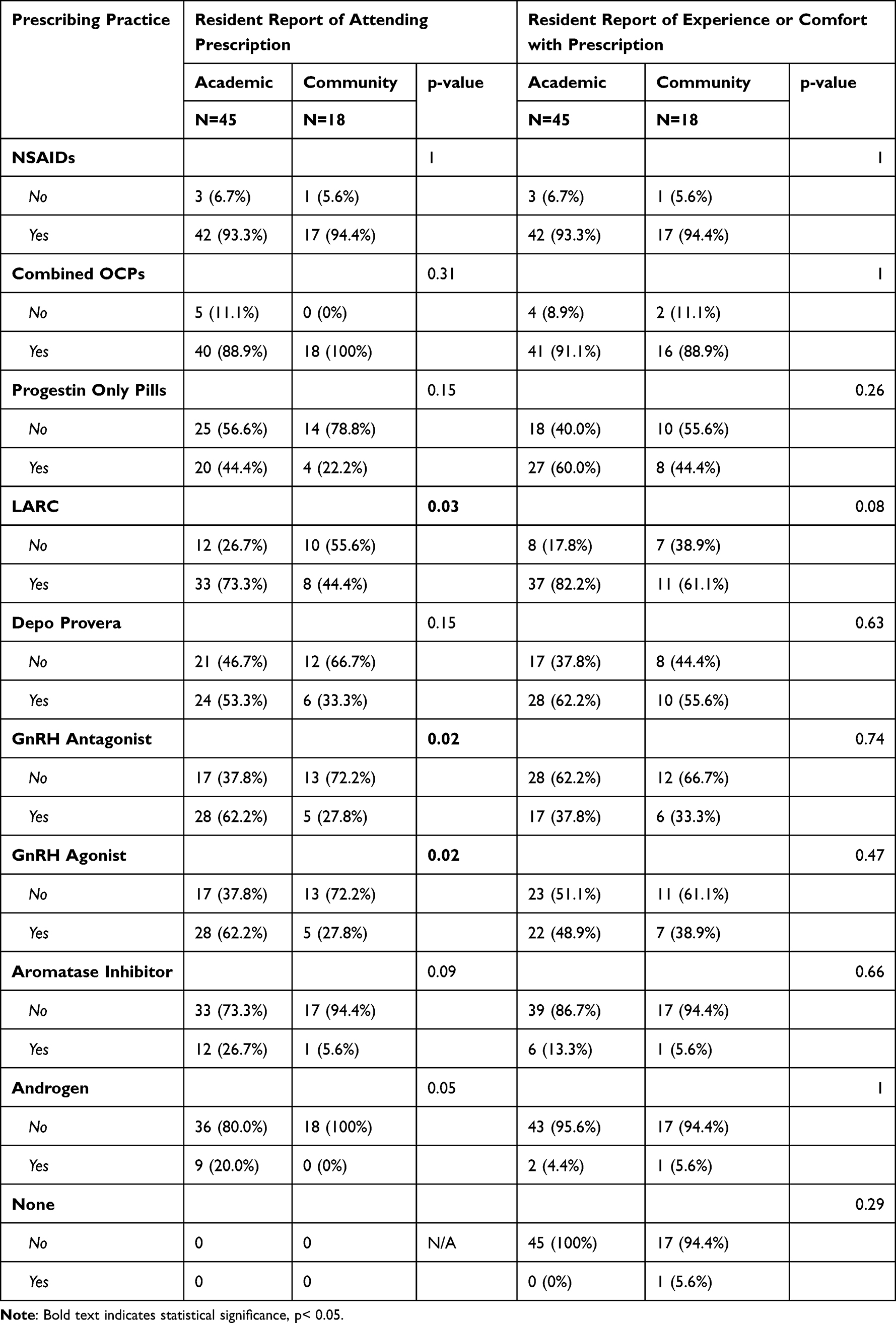 |
Table 2 Attending and Resident Prescribing Practices for Medical Treatment of Endometriosis by Residency Setting |
34% felt comfortable managing the hypoestrogenic effects of GnRH antagonists, agonists, or aromatase inhibitors and 42% did not feel comfortable doing so (Figure 2). 38% of residents felt comfortable counseling about the osteoporotic risk of GnRH antagonists, agonists, and aromatase inhibitors and 31% felt comfortable with the recommendations about adding back progestin for these medications.
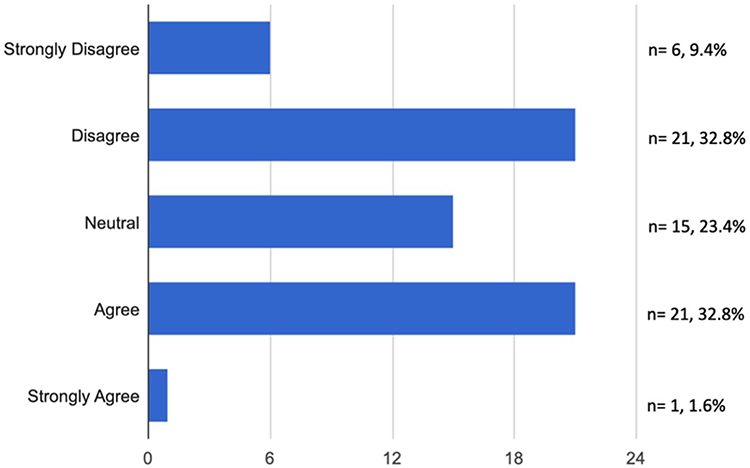 |
Figure 2 Responses to the question “I feel comfortable managing the hypoestrogenic effects of GnRH antagonists, agonists, and aromatase inhibitors”. |
Exposure to referrals to other medical specialties or non-medical management of endometriosis was mixed (Figure 3). The most seen referral was to pelvic floor physical therapy. 28% (n=18) had never seen a patient referred to any other specialties.
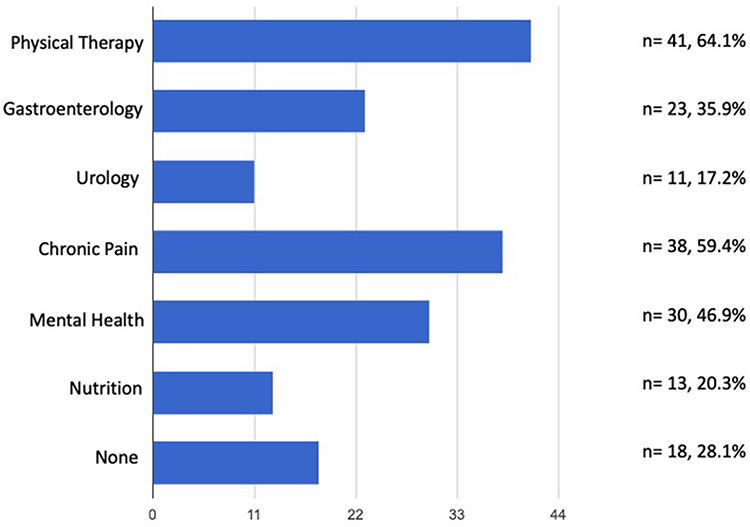 |
Figure 3 Responses to the question “Have you ever had exposure to a patient being referred to the following for alternative management of endometriosis?”. |
Surgical Management
83% of respondents had participated in surgery for endometriosis. Examples of tools seen for surgical management of endometriotic lesions were removal of endometrioma (n=52, 83%) followed by sharp excision of lesions (n=45, 71%), electrosurgical fulguration (n=44, 70%), and laser vaporization (n=20, 32%). Most respondents felt comfortable recognizing a variety of intra-operative findings of endometriosis, including classic powder-burn lesions (n=58, 92%), endometriomas (n=54, 86%), and other non-classic lesions (eg white/fibrotic, blue, clear) (n=34, 54%).
Comfort After Residency
Among all residency levels, 64% (n=39) would feel comfortable with the diagnosis of endometriosis if they were in practice today, as opposed to 52% (n=32) feeling comfortable with medical management and 26% (n=16) with surgical management. There were significant differences in comfort level between PGY1-2 and PGY3-4 (Table 3). Senior residents were comfortable diagnosing endometriosis (91%) but their comfort in medical and surgical management declined to 75% and 39% respectively. There were no statistically significant differences in comfort with diagnosis, medical management, or surgical management between academic and community-based residents.
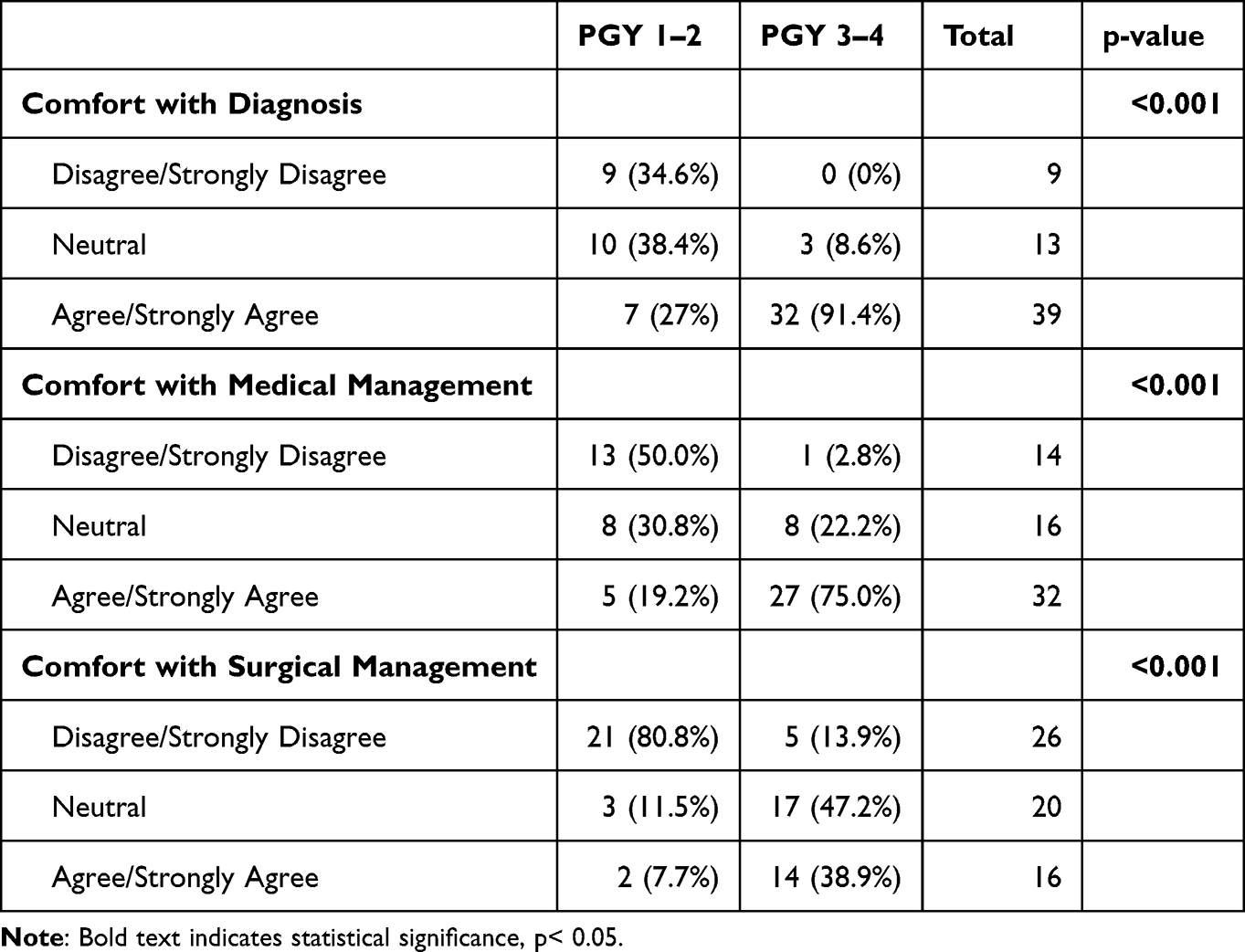 |
Table 3 Responses to the Question “If I Were to Be in Practice on My Own Today, I Would Feel Comfortable” with the Diagnosis of or Medical or Surgical Treatment of Endometriosis |
Respondents overall would like to learn about endometriosis through a variety of methods, with the most popular options being hands on learning (n=52, 85%), residency lectures or didactics (n=50, 82%), and surgical videos (n=47, 77%). Reading on one’s own was the least popular option (n=28, 46%). Residents further reported in the free text response that they would want to learn in the following ways:
- Journal clubs to discuss the evidence.
- Learning from other disciplines such as dietitians and mental health providers.
- Seeing more patients in clinic with endometriosis.
- More surgical exposure to endometriosis.
- Podcasts.
- Learning about specific patients from discussions with knowledgeable attendings.
Discussion
OB/GYN residents value learning about endometriosis but many report their current confidence with disease management is lacking. Our findings support our hypothesis that senior residents are more comfortable managing endometriosis than junior residents as well as that residents are more comfortable with medical treatment than surgical treatment. However, even senior residents may not always feel comfortable with surgical treatment. Only 39% of PGY 3–4 residents felt comfortable about surgically managing endometriosis if they were to be in practice today. These numbers may reflect not just limited endometriosis exposure in the operating room but also limited overall gynecologic surgery experience in residency.
With regards to medical therapy, only approximately a third of all residents felt comfortable with managing hypoestrogenic effects, osteoporotic risks, and add-back progestin for certain hormonal therapies, indicating a need for further training on the nuances of these medications. Residents are most comfortable with first line medical therapies including contraception but are less comfortable with other medication options, including those that are US Food and Drug Administration (FDA) approved for endometriosis such as GnRH antagonists.9 Formal teaching about these medications including how to manage the hypoestrogenic effects of GnRH antagonists, agonists, and aromatase inhibitors may be beneficial as this was an area of discomfort for many residents, in addition to reviewing bone impact and when to use add-back progestin.10–13
80% of surveyed residents received no or one formal lecture on endometriosis within the past year. As many residency programs rotate didactic curriculum every two years, junior residents may have not yet encountered a lecture on this topic. Given the prevalence of endometriosis, more frequent lectures on the topic should be considered by residency program leadership. Incorporating endometriosis teaching sessions while on a general gynecology or subspeciality rotation, such as Reproductive Endocrinology and Infertility or Minimally Invasive Gynecology Surgery, is another strategy to strengthen the education of residents in this topic.
Community-based residents were significantly less likely to be exposed to attendings prescribing LARC, GnRH antagonists, and GnRH agonists for endometriosis than university residents. There were no statistically significant differences in comfort or experience with endometriosis diagnosis, medical management, or surgical management between trainees in academic and community programs.
Strengths of the study include that the survey questionnaire was internally validated by review with residents from each year to assess for understandability. Respondents included a diverse sample of OB/GYN residents in a large state from all residency years. However, it is possible that these results are not generalizable to residency programs outside of California, although there is no reason to suspect there would be substantially different practices elsewhere. Since we were not able to track which programs forwarded the survey to their residents, we are unable to calculate a response rate. There may be bias in terms of who received the survey, for instance a program director with more interest in the topic matter may have been more likely to forward the link to their residents. The survey was sent halfway through the academic year and interns would not have had the opportunity for as much as exposure as more senior residents. This study utilized an unvalidated survey as one does not exist.
Despite these limitations, this study provides a foundation for understanding the strengths and weaknesses of resident training and highlights realistic areas for improvement. OB/GYN trainees should be provided with a comprehensive education regarding the medical and surgical management of endometriosis and should be able to graduate confident to treat this disease.
Conclusions
This survey suggests that OB/GYN residents understand the value of a comprehensive training about endometriosis but recognize that there are several gaps in both their formal and hands-on education. More formal didactic education should be built into the residency curriculum, especially to review some of the more complex medical therapies. Given trainees feel the least comfortable with surgical management, actively seeking out opportunities for residents to have surgical exposure to endometriosis should be a goal for programs. We hope that by highlighting deficits in training we can improve the teaching on this disease and reduce the multi-year delay in diagnosis of endometriosis. Future research should evaluate for evidence-based educational materials on this topic.
Acknowledgments
Thank you to the residents who participated in this study.
Funding
This project was partially supported by the National Institutes of Health, Grant UL1TR001442 of CTSA funding through our use of REDCap. The content is solely the responsibility of the authors and does not necessarily represent the views of the NIH.
Disclosure
Dr D Yvette Lacoursiere is a SASGOG Board Member. The authors have no other disclosures or conflicts of interest to report for this work.
References
1. Shafrir AL, Farland LV, Shah DK, et al. Risk for and consequences of endometriosis: a critical epidemiologic review. Best Pract Res Clin Obstet Gynaecol. 2018;51:1–15. doi:10.1016/j.bpobgyn.2018.06.001
2. Missmer SA, Tu F, Soliman AM, et al. Impact of endometriosis on women’s life decisions and goal attainment: a cross-sectional survey of members of an online patient community. BMJ Open. 2022;12(4):e052765. doi:10.1136/bmjopen-2021-052765
3. Parazzini F, Esposito G, Tozzi L, Noli S, Bianchi S. Epidemiology of endometriosis and its comorbidities. Eur J Obstet Gynecol Reprod Biol. 2017;209:3–7. doi:10.1016/j.ejogrb.2016.04.021
4. Soliman AM, Fuldeore M, Snabes MC. Factors Associated with Time to Endometriosis Diagnosis in the United States. J Women's Health. 2017;26(7):788–797. doi:10.1089/jwh.2016.6003
5. Hadfield R, Mardon H, Barlow D, Kennedy S. Delay in the diagnosis of endometriosis: a survey of women from the USA and the UK. Hum Reprod. 1996;11(4):878–880. doi:10.1093/oxfordjournals.humrep.a019270
6. Roullier C, Sanguin S, Parent C, Lombart M, Sergent F, Foulon A. General practitioners and endometriosis: level of knowledge and the impact of training. J Gynecol Obstet Hum Reprod. 2021;50(10):102227. doi:10.1016/j.jogoh.2021.102227
7. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
8. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
9. National Institutes of Health. Elagolix- The First FDA-Approved Treatment for Endometriosis and Uterine Fibroids. Available from: https://www.nichd.nih.gov/grants-contracts/SBIR_STTR/showcase/Elagolix.
10. Leyland N, Estes SJ, Lessey BA, Advincula AP, Taylor HS. A clinician’s guide to the treatment of endometriosis with elagolix. J Women's Health. 2021;30(4):569–578. doi:10.1089/jwh.2019.8096
11. Ferrero S, Evangelisti G, Barra F. Current and emerging treatment options for endometriosis. Expert Opin Pharmacother. 2018;19(10):1109–1125. doi:10.1080/14656566.2018.1494154
12. Selak V, Farquhar C, Prentice A, Singla A. Danazol for pelvic pain associated with endometriosis. Cochrane Database Syst Rev. 2007;4:CD000068. doi:10.1002/14651858.CD000068.pub2
13. Donnez J, Dolmans MM. GnRH Antagonists with or without Add-Back Therapy: a New Alternative in the Management of Endometriosis? Int J Mol Sci. 2021;22(21). doi:10.3390/ijms222111342
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.