")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Perceived Social Stigma of Cutaneous Leishmaniasis in Hubuna, Saudi Arabia
Authors Elfaki NK , Alzahrani MJ , Abdalla YHA, Adeh AI, Osman Abdalla AMA , Alkhadher MA , Elrefaey SR , Abdelmagid WHH, Alshameri F , Jarelnape AA , Hakami MS, Alghamdi FAA, Elhaj YHA, Dinar NMAA, Mohamed AAA , Abdulrahman EEH , Mohamed DHM , Sagiron EI, Ali MHM, Ahmed WA
Received 1 January 2024
Accepted for publication 19 February 2024
Published 28 February 2024 Volume 2024:17 Pages 867—876
DOI https://doi.org/10.2147/JMDH.S454135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nahid K Elfaki,1 Mohammed Jamaan Alzahrani,2 Yahya Hussein Ahmed Abdalla,1 Abdullah I Adeh,3 Abdalla Mohammed Ahmed Osman Abdalla,1 Mugahed A Alkhadher,4 Samah R Elrefaey,1 Warga Hashim Hussein Abdelmagid,5 Faroq Alshameri,6 Ahmed Abdalla Jarelnape,7 Manal SA Hakami,7 Fahad Abdullah A Alghamdi,7 Yagoub Hamadt Allah Elhaj,8 Niemat MAA Dinar,7 Amal Abdelgadir Ali Mohamed,9 Elsadig Eltaher Hamed Abdulrahman,4 Duria Hassan Merghani Mohamed,10 Elwaleed Idris Sagiron,1 Maha Hamed Mohamed Ali,1,11 Waled AM Ahmed7
1Department of Community and Mental Health Nursing, College of Nursing, Najran University, Najran, Saudi Arabia; 2Pediatric Department, College of Medicine, Najran University, Najran, Saudi Arabia; 3Internal Medicine Department, College of Medicine, Najran University, Najran, Saudi Arabia; 4Medical- Surgical Nursing Department, College of Nursing, Najran University, Najran, Saudi Arabia; 5Maternity and Child Health Nursing Department, College of Nursing, Najran University, Najran, Saudi Arabia; 6Nursing Department, Faculty of Medical Sciences and Nursing, Alrayan Colleges, Almadina, Saudi Arabia; 7Faculty of Nursing, Al-Baha University, Al-Baha, Saudi Arabia; 8Laboratory Medicine Department, Faculty of Applied Medical Sciences, Al-Baha University, Al-Baha, Saudi Arabia; 9Department of Maternal and Child Nursing Sciences, College of Nursing, Taif University, Taif, Saudi Arabia; 10Faculty of Nursing, King Khalid University, Muhail Aseer, Saudi Arabia; 11Public Health Department, Faculty of Applied Medical Sciences, King Khalid University, Khamis Mushait Aseer, Saudi Arabia
Correspondence: Nahid K Elfaki, Department of Community and Mental Health Nursing, College of Nursing, Najran University, Najran, Saudi Arabia, Email [email protected] Waled AM Ahmed, Community Health Nursing Department, Faculty of Nursing, Al-Baha University, Al-Baha, Saudi Arabia, Tel +966508245369, Email [email protected]
Background: Cutaneous Leishmaniasis (CL) is a vector-borne skin infection that remains prevalent in regions with poor socioeconomic conditions. Stigmatization occurs when individuals with physical or psychological disorders interact with societal stereotypes. The aim of this study was to explore the perceived social stigma surrounding CL among people residing in Hubuna, Saudi Arabia.
Methods: This cross-sectional community-based survey recruited 618 individuals aged 18 years and above using the snowball sampling technique to reach hidden cases within the target population. Data was collected using a self-administered questionnaire and the Explanatory Model Interview Catalogue for Perceived Social Stigma (EMIC-SS-12) was used to assess the level of perceived social stigma. It includes questions on demographic variables, behaviors, and experiences. The analysis was performed using SPSS.
Results: The study included 618 participants, the majority of whom were women and girls (54.2%), with a mean age of 28 ± 12.7 years. The median score for perceived social stigma was 26.0. Only 2.1% (n = 13) of participants had the highest EMIC-SS-12 score of 36, while 7.6% (n = 47) scored zero. The mean score for overall perceived social stigma was 1.89 ± 0.91, while the mean score for experienced stigma was 1.99 ± 1.02. Univariate analysis showed that sex, employment, location of lesions, and number of lesions were insignificantly associated with stigmatization (P-value < 0.05), because these associations were uncertain because the CI includes or very close to 1.
Conclusion: The study reveals insights into stigmatization associated with CL in the Habuna area of Saudi Arabia. It found that the median of perceived social stigma was 26. Factors such as sex, employment status, and location of the lesion are uncertainly associated with stigma. It is crucial to explore negative behaviors and perceptions and develop suitable health education programs.
Keywords: social stigma, cutaneous leishmaniasis, Hubuna, Saudi Arabia, infectious diseases
Background
Cutaneous Leishmaniasis (CL) is considered a vector-borne disease transmitted by the bite of female phlebotomine sand flies. It is considered the most common form of leishmaniasis and causes disease burdens worldwide. The main symptom of CL includes skin ulceration on exposed body parts. Some lesions heal spontaneously, while the majority of lesions are non-healing or chronic conditions with sequels, potentially leading to disfigurement or mutilation and severe economic, psychological, and social consequences.1–5
Late presentation of CL can result in severe undesired complications, such as large ulcerative nodules, damaged noses, scarred lips, and scars. These complications can lead to anxiety, depression, and social stigma. Stigma is associated with misunderstandings and misconceptions about certain illnesses, educational levels, low social class, and/or family income.6,7
The factors that exaggerate stigma are almost the same in different cultures.2,8 In this context, Kippax et al believe that instead of viewing stigma as something individuals impose on others, the focus should be on the widespread social, cultural, political, and economic influences that cause stigma.9 Hu et al examined the effect of CL on the quality of life in Suriname. While they showed that lower limb lesions have more effect on patients’ quality of life, they noted that no stigma was reported among the Suriname patients.10
The stigmatization process refers primarily to social perceptions of negative behaviors towards certain persons or families due to disvalued physical, psychological, or social problems that may lead to discrimination, which adversely affects individuals’ emotional well-being and mental health.11–13 Cutaneous Leishmaniasis Social Stigma (CLSS) refers to negative attitudes and beliefs towards people with CL. Stigma is the main factor that causes negative behavior related to medical, physical, or social disorders.
Several factors play varying roles in CLSS. People may experience stigma during early childhood, adolescence, or even in old age. People with CL often experience internalized stigma, and accordingly, they develop a negative self-image. Women and girls with CL may be considered unacceptable for marriage. CLSS often has a negative impact on all aspects of women and girls’ lives during their marriages, and others may have difficulty getting married at all.14–17 Moreover, a systematic review reported that CLSS often negatively impacts all aspects of a woman’s adult life. Accordingly, it is common for these women and girls to suffer from anxiety, depression, and other mental disorders.18
The situation of CL in Saudi Arabia has previously been reported. Many studies have documented that the rate of CL in the Hubuna area of Najran peaks primarily during the hot and humid season of May to September.3 Another study was conducted in Taif, an area next to Najran, similarly reported high cases of CL, particularly among women. A project conducted in the Hubuna area reported success in treating many of these cases of CL,19 while in the same area, the same project reported many cases reported among women.20,21
Therefore, the study aims to investigate levels of perceived social stigma among CL patients as well as explore the associations between these outcomes and various socio-demographic variables among CL patients in the Hubuna area of Saudi Arabia. The results of this study can help in enhancing the understanding of the effects of CL and may guide the development of effective intervention strategies and services to address the associated stigma. It could also inform policymakers about the needed policies and practices to address CL.
Methods
Study Design
This study utilized a cross-sectional design. In this study, the cross-sectional design was appropriate for assessing the level of perceived social stigma among patients CL.
Study Area and Population
This study was conducted in the Hubuna area, one of the governorates in the Najran region. It has a total population of 20,400 individuals.22 It is known to be vulnerable to CL epidemics due for several reasons, including social, environmental, and climatological factors that directly influence the disease’s epidemiology.1 Among these factors, it was observed that people in Hubuna prefer to live next to or inside farms and breed cattle and/or cows, which increase their vulnerability to the infection. In addition, the high number of job seekers and travelers of all nationalities who regularly come to Saudi Arabia, along with climate and environmental changes, high rates of rainfall and humidity, rapid urbanization, and huge population movements are among the most important risk factors behind the CL problem. It was reported that the incidence of CL in this area peaks primarily during the hot and humid season of May to September.3
Sampling Process
The study employed the Snowball Sampling Technique (SST) to recruit participants. The approach used to target patients with CL was through visiting those patients and through them they guided the team to other patients with CL. Initial participants (seeds) were identified and recruited, and then they helped to refer or recruit additional participants from their social networks who fit the criteria for the study. This process continues iteratively, like a snowball rolling and accumulating more snow, until the desired sample size is achieved. A total of eight hundred individuals were initially contacted and asked to participate. Of these, 68 individuals declined to participate, resulting in a response rate of 91.5% (n = 732). After data cleaning, 114 incomplete or incorrectly completed questionnaires were excluded from the analysis, leaving a final sample size of 618 individuals (as shown in Figure 1).
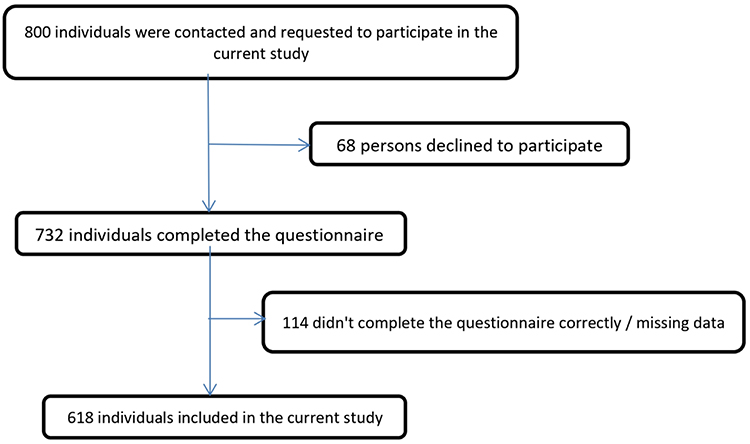 |
Figure 1 Participants’ recruitment flowchart. |
Inclusion Criteria
This study included all individuals aged 18 years or older from all nationalities who are currently living in Hubuna. The study was conducted among individuals from the selected area, including healthy people and those previously diagnosed with CL.
Exclusion Criteria
The study excluded individuals who were less than 18 years old, those who declined to participate in the study, and patients who were severely ill or disoriented to answer the questionnaire correctly. This is because participation may affect their health status, or their participation may deteriorate their health conditions.
Data Collection Process
A validated online questionnaire was used, which consisted of two sections. Section one was for demographic characteristics, and section two was for the level of PS and ESS. An Explanatory Model Interview Catalogue for Social Stigma (EMIC-SS), a validated assessment tool, was used.23 This tool consists of 12 items (questions), and individuals were asked to indicate the number that best represents their perception (ranging from 3, which indicates “yes”, 2 represents “possibly”, while 1 means “uncertain”, and “no” = 0 points). People who answered “yes” were considered to have a strong indication of social or perceived stigma and, therefore, received three points, while those with no response received zero scores and were considered without any stigma feelings. The level of stigmatization was indicated by summing the total scores. A higher score implies a higher level of perceived stigma experienced by the respondent. “Yes” is scored as three points, indicating a strong social or perceived stigma, “possibly” is scored as two points, “uncertain” is scored as one point, and “no” is scored as zero points, indicating no stigma feelings.
The questionnaire was translated into Arabic and evaluated for content validity by a jury of five medical experts, while Cronbach’s evaluated the internal consistency. The translated version of the questionnaire was validated by the pilot test and revised by Arabic speakers to ensure its comprehensiveness, clarity, and appropriateness.
Statistical Analysis
Data cleaning and coding were performed prior to the analysis using IBM SPSS Statistics version 24 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the demographic characteristics. The Chi-square test was used to examine the association between variables, and linear regression was applied to explore the relationship between the stigma and various demographic variables.
Results
Out of eight hundred invited individuals, 618 participants completed the questionnaire. The response rate was 77.25%.
Socio-Demographic Characteristics of the Sample (n=618)
A total of 618 participants were included in this study, with a majority of female respondents (54.2%). The mean age of the participants was 28 ± 12.7 years, ranging from 19 to 64 years. In terms of educational level, 44.8% of participants had completed secondary education. It is worth noting that a high proportion of participants (82.2%) were currently residing in or near farming areas, which are considered one of the most high-risk environments for CL transmission. They were either previously diagnosed with CL or have current condition of CL.
Clinical Characteristics of CL Lesions Among People with CL
The duration between the onset of symptoms and the first medical consultation (case-delay) was found to range from 2 to 20 weeks, with a mean duration of 8.6 ± 5.5 weeks, as presented in Table 1. The majority of cases, about 36.4% (n = 76), reported experiencing CL lesions on their upper parts, followed by 26.3% (n = 55) reporting lesions on their upper extremities. The number of lesions varied, with 44.5% of people with CL (n = 93) reporting having 3–4 lesions. It was found that 40.2% (n = 84) of cases had lesions for ≥12 months, while more than half of the cases had lesions with less than one year of duration. The mean duration of disease chronicity was 6.8 ± 3.5 months. Delayed diagnosis, along with poor treatment adherence, was reported in 22% (n = 46) of cases.
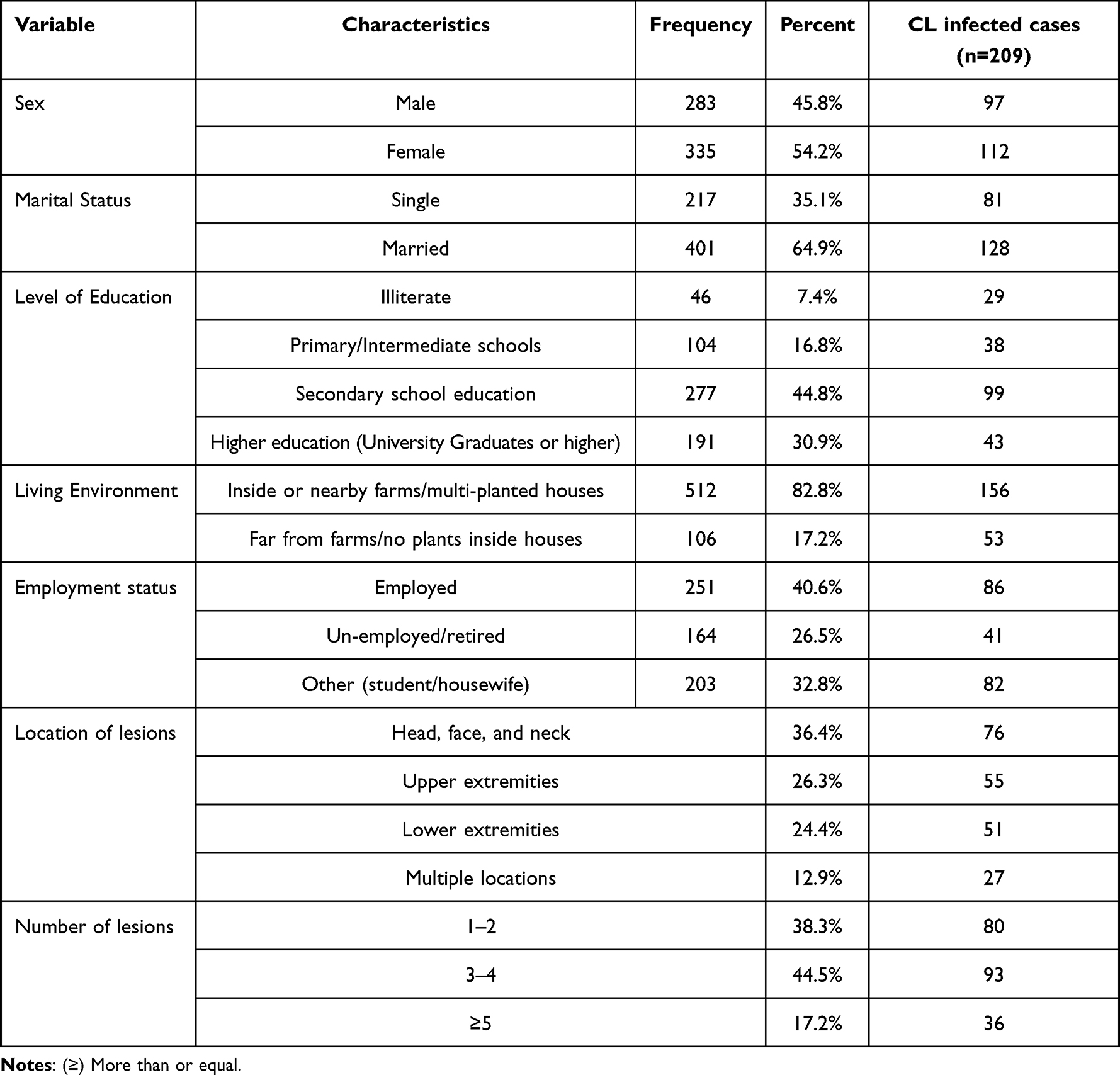 |
Table 1 Socio-Demographic Characteristics of the Participants (n = 618) |
Table 2 represents EMIC-SS-12 stigma mean scores among participants. The questions asked in this scale include questions about feeling less of self, feeling ashamed, less respect from neighbors, and deciding to stay away from society. The median score for the perceived stigma was 26.0. It had been noticed that only 2.1% (n = 13) of the participants had the highest EMIC-SS score of 36.0, while, on the other hand, 7.6% (n = 47) of participants scored zero. The range is 0 for no stigma, >0–<1 for uncertain stigma, 1–<2 for uncertain stigma, and 2–3 for strong stigma level. Regarding the overall perceived stigma, the mean score was 1.89 ± 0.91, while for experienced stigma the overall mean score was 1.99±1.02, respectively, indicating the uncertainty of presence of stigma related to CL.
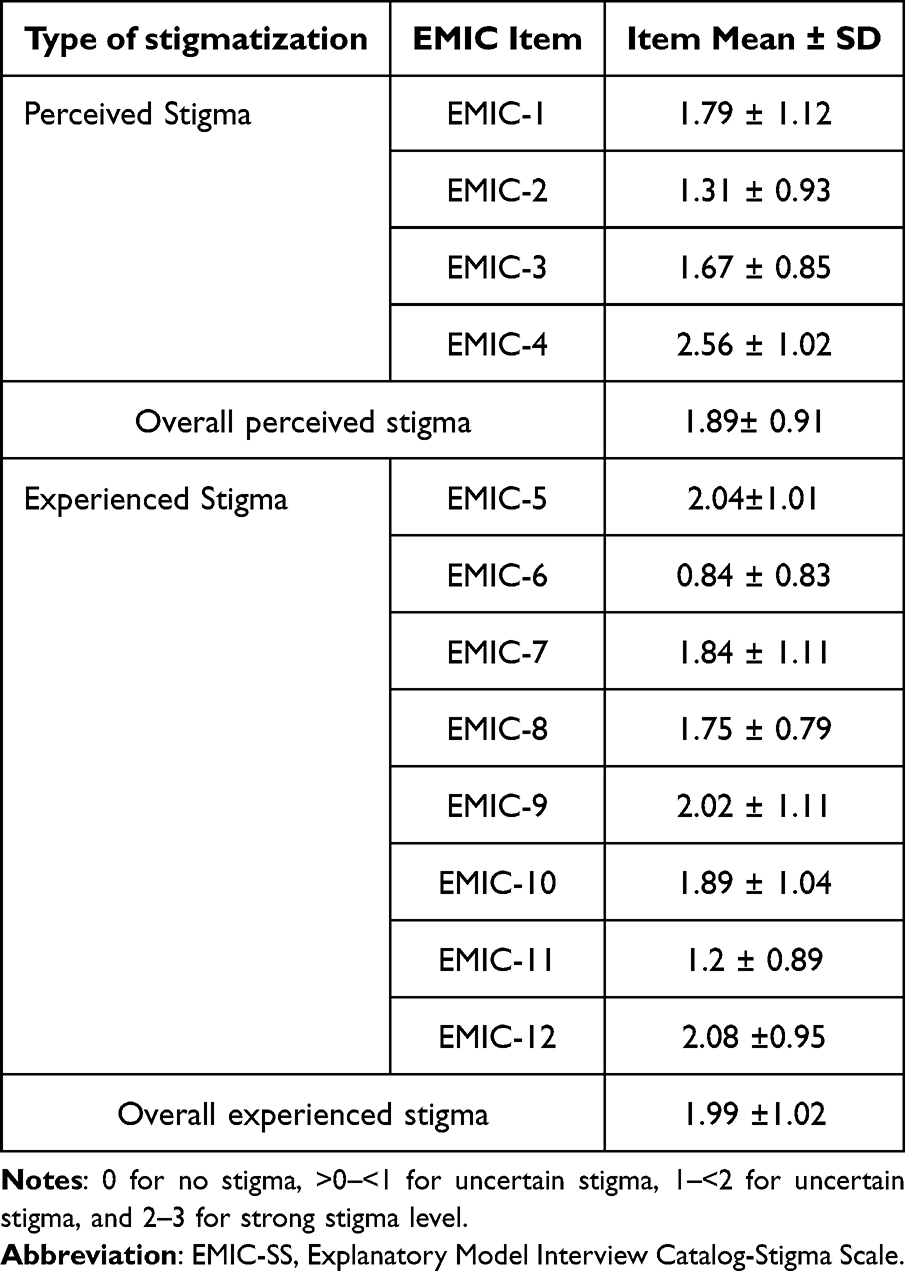 |
Table 2 Mean Scores of EMIC-SS-12 Items Among Participants (n = 209) |
Based on the univariate analysis presented in Table 3, the following factors were found to be insignificantly associated with stigmatization: sex (OR 0.964; 95% CI 0.801–1.137), employment status (OR 0.70; 95% CI 0.771–1.097), location of lesions (OR 1.352; 95% CI 0.63–2.4), this is because it included CI among these factors including 1, which limit certainty of their significance. The number of lesions (OR 0.921; 95% CI 0.633–0.731) has negligible association with stigmatization, because the CI is near to 1. On the other hand, age, educational level, and living environment were not found to be significantly associated with stigmatization, with a P-value >0.05.
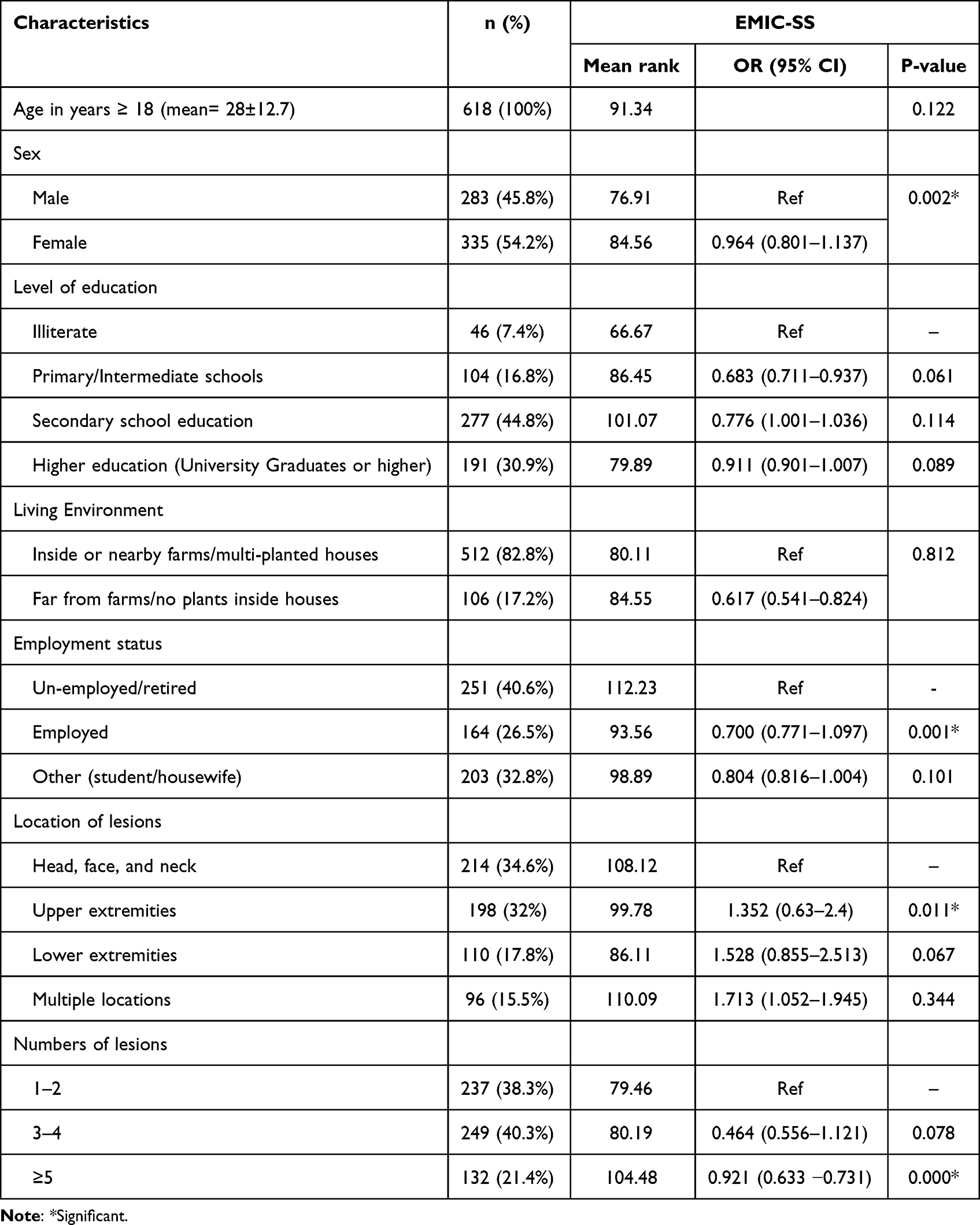 |
Table 3 Association Between EMIC-SS Score and Participants’ Socio-Demographic Characteristics (n = 618) |
Discussion
The burden of CL goes beyond physical symptoms and can have significant psychological impacts on affected individuals. This is a commonly observed phenomenon, and several studies have highlighted the potential psychological burden associated with CL and its scarring.24–26 Stigmatization is a major psychological burden that individuals with CL often experience. It is a common phenomenon and can lead to negative psychosocial consequences such as social isolation, discrimination, and depression. In our study, we found that 33.8% of participants reported experiencing stigmatization due to CL, which highlights the need to address this issue in affected populations. Furthermore, our study identified sex, employment status, location, and number of lesions as factors associated with stigmatization because the CI includes or very close to 1. In the same line, one qualitative study reported that people suffered self-stigmatization due to CL and further isolation or rejection is common in the case of severe infection.27 Similar findings were also reported from a study in Uganda in 2020 where 47% of people with CL reported stigma.28 In a previous study by Gomez using an explanatory model interview catalogue, it was reported that mental distress and stigma were prevalent among patients with CL.29
This study yielded numerous findings; the most significant one was the perceived stigma. The median score for the perceived stigma among participants in the current study was 26.0 which is much lower than what had been documented by Ramdas et al in Tunisia, which was 73% among women and girls.30 They used short interviews with people with CL to find out the stigma and mental distress. On the other hand, in a study conducted by Hu et al (2020), they investigated the impact of CL on patients’ quality of life. Their findings indicated that there was no significant stigma associated with lower limb CL lesions among patients in Suriname.10
Based on the findings in the current study, stigmatization was observed to occur for all ages, although younger individuals were more affected. The same findings had been observed by Yap et al in Australia, Frota et al in Brazil, Garapati et al in India, and Voorend and Van Brakel in the Netherlands.8,31,32 Many people in this survey reported that it is embarrassing for them to seek medical help; this would explain why people delay or present late for medical help with severe undesired complications. These observations are inconsistent with what had been reported by Al-Kamel, Ramdas et al, and Karimkhani et al.16,30,33 The delay in seeking medical advice for diagnosis could increase the burden of CL and complicate the emotional and social distress experienced by people with CL.
Additionally, it appears from this study that Hubuna people’s experiences of stigma are influenced by certain general fear and anticipation of rejection rather than any rejection they may really experience from their community. The same idea was reported by Chahed et al in Tunisia,11 and also these results were found to correspond to Leventhal’s theory of illness perception.34
Moreover, and based on our results, a significant correlation was noticed between stigma and the location of lesions, especially those on faces and/or upper extremities, which had also been reported by the WHO and Nilforoushzadeh.35,36
It is believed that the best way for people to prevent CL infection is to protect themselves from sand fly bites as there are no drugs or vaccines to prevent CL infection. Therefore, the vector and parasite abundance is strongly affected by human interventions. In this line, the most cited method of prevention, as stated in the current study, was using insecticide-treated bed-nets followed by the use of wood smoke for repelling mosquitoes, which is supported by Alzahrani et al.20
Based on the information from this study, employment status was insignificantly associated with stigma especially among employed women and girls. Research has reported that women with CL are more likely to experience psychiatric morbidity if they report, for instance, social stigmatization or discrimination.11,37 Most women and girls in Hubuna pointed at the negative psychological consequences due to scars, which resulted from CL, especially those located on their faces. The same findings had been reported in other countries.11,14,38–40 Additionally, the number of lesions among people with CL has minimal impact on stigmatization.
The study also indicated that sex, employment status, and location of lesions were insignificantly associated with stigmatization, because these factors include a CI of 1, which indicates a lack of statistical significance. While these factors were associated with stigmatization with uncertainty about its significance, additionally the number of lesions was statistically associated with stigmatization with CI very close to 1 indicating negligible impact. These findings underscore the need for further studies to investigate the factors associated with CL’s perceived social stigma.
The findings highlight the importance of developing interventions to urgently address the psychological and social consequences of CL. These interventions are not limited to managing physical symptoms of infected case, but they could also include emotional and social aspects. It is also necessary to address stigmatization by raising awareness and education campaigns about the disease and its consequences, educating the population about the causes, prevention, transmission, and management. These interventions could also improve access to care and treatment and develop support groups for CL patients to help them cope with the psychological and social burdens of the disease. This study could contribute to the existing body of knowledge on the psychosocial aspects of CL and provides constructive insights for conducting clinical practice and public health interventions. Further research is needed to better understand the complex nature of stigmatization and its impact on the health and well-being of CL patients and to gain a deeper understanding of the condition.
Limitations
Some limitations were identified in this study. Firstly, this study used self-administered questionnaires, which are less detailed than in-depth individual interviews in terms of generated information. Secondly, it relates to the non-probability sampling method (Snowball) which may limit the chance of generalizing the results.
Conclusion
Based on the findings of this study it had been concluded that the median of PSS was 26. While our findings indicated sex, employment status, and location of the lesions are insignificantly associated with PSS, these associations should be taken with caution due to the wide confidence intervals that encompass 1. Interestingly, a significant association was reported between the number of lesions with PSS, with minimal impact due to its CI being very close to 1. Thus, acknowledging that the significance association is very close to 1 indicates minimal or no effect. These findings highlighted the multifaceted nature of stigmatization, underscoring the need for further research addressing the associated factors with stigmatization among individuals with CL. The findings highlight the urgent need for interventions focusing on psychological and social aspects of CL, which could also contribute to guiding the clinical practices and health policies related to the disease.
Data Sharing Statement
Data are available upon request from the corresponding author (Nahid K. Elfaki).
Ethical Approval
The ethical approval was obtained from the Institutional Review Board of Najran University (NU/RG/MRC/11/1). Informed consent was obtained from all study participants, indicating their right to decline participation or withdraw from the study at any time. Confidentiality and anonymity of the participants were ensured throughout the study. This study complies with the Declaration of Helsinki.
Acknowledgment
The authors acknowledge the Ministry of Education and Deanship of Scientific Research at Najran University, Saudi Arabia, for financial support (project no. NU/RG/MRC/11/1).
Funding
This project was funded by the Ministry of Education, Saudi Arabia, and the Deanship of Scientific Research at Najran University, Saudi Arabia, under Project No. (NU/RG/MRC/11/1).
Disclosure
The authors declared that there was no potential conflict of interest.
References
1. Tzani M, Barrasa A, Vakali A, Georgakopoulou T, Mellou K, Pervanidou D. Surveillance data for human leishmaniasis indicate the need for a sustainable action plan for its management and control, Greece, 2004 to 2018. Euro Surveill; 2021;26(18):2000159 doi:10.2807/1560-7917.ES.2021.26.18.2000159
2. Kassi M, Kassi M, Afghan AK, Rehman R, Kasi PM. Marring leishmaniasis: the stigmatization and the impact of cutaneous leishmaniasis in Pakistan and Afghanistan. PLoS Negl Trop Dis. 2008;2(10):e259. doi:10.1371/journal.pntd.0000259
3. Abuzaid AA, Abdoon AM, Aldahan MA, et al. Cutaneous leishmaniasis in Saudi Arabia: a comprehensive overview. Vector-Borne Zoonotic Dis. 2017;17(10):673–684. doi:10.1089/vbz.2017.2119
4. Basra MKA, Fenech R, Gatt RM, Salek MS, Finlay AY. The dermatology life quality index 1994–2007: a comprehensive review of validation data and clinical results. Br J Dermatol. 2008;159(5):997–1035. doi:10.1111/j.1365-2133.2008.08832.x
5. Okwor I, Uzonna J. Social and economic burden of human leishmaniasis. American JTrop Med Hyg. 2016;94(3):489. doi:10.4269/ajtmh.15-0408
6. Akilov OE, Khachemoune A, Hasan T. Clinical manifestations and classification of old world cutaneous leishmaniasis. Int J Dermatol. 2007;46(2):132–142. doi:10.1111/j.1365-4632.2007.03154.x
7. Afghan AK, Kassi M, Kasi PM, Ayub A, Kakar N, Marri SM. Clinical manifestations and distribution of cutaneous leishmaniasis in Pakistan. J Trop Med. 2011;2011. doi:10.1155/2011/359145
8. Voorend CGN, Van Brakel WH, Cross H, Augustine V, Ebenso B. Report of the stigma research workshop for the development of scientific consensus papers and field guidelines on health-related stigma, held in Amsterdam, the Netherlands from 11–14 October 2010. Leprosy Rev. 2011;82(2):188–201. doi:10.47276/lr.82.2.188
9. Kippax S, Stephenson N, Parker RG, Aggleton P. Between individual agency and structure in HIV prevention: understanding the middle ground of social practice. Am J Public Health. 2013;103(8):1367–1375. doi:10.2105/AJPH.2013.301301
10. Hu RV, Ramdas S, Nieuwkerk P, et al. Body location of “New World” cutaneous leishmaniasis lesions and its impact on the quality of life of patients in Suriname. PLoS Negl Trop Dis. 2020;14(10):e0008759. doi:10.1371/journal.pntd.0008759
11. Chahed MK, Bellali H, Ben Jemaa S, Bellaj T. Psychological and psychosocial consequences of zoonotic cutaneous leishmaniasis among women in Tunisia: preliminary findings from an exploratory study. PLoS Negl Trop Dis. 2016;10(10):e0005090. doi:10.1371/journal.pntd.0005090
12. Rafael F, Houinato D, Nubukpo P, et al. Sociocultural and psychological features of perceived stigma reported by people with epilepsy in Benin. Epilepsia. 2010;51(6):1061–1068. doi:10.1111/j.1528-1167.2009.02511.x
13. Galvão EL, Pedras MJ, Cota GF, Rabello A, Simões TC. How cutaneous leishmaniasis and treatment impacts in the patients’ lives: a cross-sectional study. PLoS One. 2019;14(1):e0211374. doi:10.1371/journal.pone.0211374
14. Bennis I, De Brouwere V, Belrhiti Z, Sahibi H, Boelaert M. Psychosocial burden of localised cutaneous Leishmaniasis: a scoping review. BMC Public Health. 2018;18:1–12. doi:10.1186/s12889-018-5260-9
15. Al‐Kamel MA. Leishmaniasis in Yemen: a clinicoepidemiological study of leishmaniasis in central Yemen. Int J Dermatol. 2016;55(8):849–855. doi:10.1111/ijd.13041
16. Al-Kamel MA. Stigmata in cutaneous leishmaniasis: historical and new evidence-based concepts. Our Dermatol. 2017;8(1):81. doi:10.7241/ourd.20171.21
17. Fischer LS, Mansergh G, Lynch J, Santibanez S. Addressing disease-related stigma during infectious disease outbreaks. Disast Med Public Health Prepared. 2019;13(5–6):989–994. doi:10.1017/dmp.2018.157
18. Wenning B, Price H, Nuwangi H, et al. Exploring the cultural effects of gender on perceptions of cutaneous leishmaniasis: a systematic literature review. Global Health Res Poli. 2022;7(1):34. doi:10.1186/s41256-022-00266-y
19. Wajihullah K, Zakai HA. Epidemiology, pathology and treatment of cutaneous leishmaniasis in Taif region of Saudi Arabia. Iran J Parasitol. 2014;9(3):365. doi:10.1186/1756-3305-5-51
20. Alzahrani MJ, Elfaki N, Abdalla YHA, Alkhadher MA, Ali MHM, Ahmed WAM. Cutaneous leishmaniasis: associated risk factors and prevention in Hubuna, Najran, Saudi Arabia. Int J Gene Med. 2023;723–731. doi:10.2147/IJGM.S401618
21. Elfaki N, Alzahrani M, Abdalla YHA, et al. Self-reported depression and anxiety rates among females with cutaneous leishmaniasis in Hubuna, Saudi Arabia. PeerJ. 2023;11:e15582. doi:10.7717/peerj.15582
22. General Authority for Statistics. Demographic Survey. Kingdom of Saudi Arabia. Riyadh 2022.
23. Nik Jaafar N, Leong Bin Abdullah M, Talib N, et al. Validation of the Malay version of the explanatory model interview catalogue stigma scale among COVID-19 Survivors in Malaysia. J Health Translat Med. 2022;2022:112–120.
24. Hatzenbuehler ML, Phelan JC, Link BG. Stigma as a fundamental cause of population health inequalities. Am J Public Health. 2013;103(5):813–821. doi:10.2105/AJPH.2012.301069
25. Ranawaka RR, Weerakoon HS, de Silva SH. The quality of life of Sri Lankan patients with cutaneous leishmaniasis. Mymensingh Med J. 2014;23(2):345–351.
26. Reithinger R, Aadil K, Kolaczinski J, Mohsen M, Hami S. Social impact of leishmaniasis. Afghanistan. 2005;2005:1.
27. Hagos B, Zerihun Z. Self-stigma’of people with cutaneous leishmaniasis the unrecognized one: what do we think; what do we know; what can we prove? Internat J Equ Health. 2023;22(1):180. doi:10.1186/s12939-023-01998-0
28. Ssewanyana IMB, Tibakabikoba H, Nakabugo J, Lule SA, Mugisha JFS. Physical and social burden of cutaneous leishmaniasis on the quality of life of patients in endemic communities of Uganda. BMC Public Health. 2020;20(1):1373. doi:10.1186/s12889-020-09376-z
29. Gómez LJ, van Wijk R, van Selm L, et al. Stigma, participation restriction and mental distress in patients affected by leprosy, cutaneous leishmaniasis and Chagas disease: a pilot study in two co-endemic regions of eastern Colombia. Transact Roy Soc Trop Med Hyg. 2020;114(7):476–482. doi:10.1093/trstmh/trz132
30. Ramdas S, van der Geest S, Schallig HD. Nuancing stigma through ethnography: the case of cutaneous leishmaniasis in Suriname. Soc sci med. 2016;151:139–146. doi:10.1016/j.socscimed.2015.12.044
31. Frota da Rocha Morgado F, Kopp Xavier da Silveira EM, Pinheiro Rodrigues Do Nascimento L, et al. Psychometric assessment of the EMIC Stigma Scale for Brazilians affected by leprosy. PLoS One. 2020;15(9):e0239186. doi:10.1371/journal.pone.0239186
32. Garapati P, Pal B, Siddiqui NA, et al. Knowledge, stigma, health seeking behaviour and its determinants among patients with post kalaazar dermal leishmaniasis, Bihar, India. PLoS One. 2018;13(9):e0203407. doi:10.1371/journal.pone.0203407
33. Karimkhani C, Wanga V, Naghavi P, Dellavalle RP, Naghavi M. Global burden of cutaneous leishmaniasis. Lancet Infect Dis. 2017;17(3):264. doi:10.1016/S1473-3099(16)30217-1
34. Leventhal H, Nerenz DR, Steele DJ. Illness representations and coping with health threats. In: Handbook of Psychology and Health. Routledge; 2020:219–252.
35. Nilforoushzadeh MA, Roohafza H, Jaffary F, Khatuni M. Comparison of quality of life in women suffering from cutaneous leishmaniasis treated with topical and systemic glucantime along with psychiatric consultation compared with the group without psychiatric consultation. J Skin Leishman. 2010;1:1.
36. World Health Organization. Investing to Overcome the Global Impact of Neglected Tropical Diseases: Third WHO Report on Neglected Tropical Diseases 2015. World Health Organization; 2015.
37. Pires M, Wright B, Kaye PM, da Conceição V, Churchill RC. The impact of leishmaniasis on mental health and psychosocial well-being: a systematic review. PLoS One. 2019;14(10):e0223313. doi:10.1371/journal.pone.0223313
38. Bennis I, Thys S, Filali H, De Brouwere V, Sahibi H, Boelaert M. Psychosocial impact of scars due to cutaneous leishmaniasis on high school students in Errachidia Province, Morocco. Infect Diseases Poverty. 2017;6:1–8. doi:10.1186/s40249-017-0267-5
39. Fikre H, van Henten S, van Griensven J, et al. Psychosocial effects of cutaneous leishmaniasis on patients in Northwestern Ethiopia: a qualitative study. medRxiv. 2023;2023:23297130.
40. Nuwangi H, Agampodi TC, Price HP, Shepherd T, Weerakoon KG, Agampodi SB. Stigma associated with cutaneous and mucocutaneous leishmaniasis: a systematic review. PLoS Negl Trop Dis. 2023;17(12):e0011818. doi:10.1371/journal.pntd.0011818
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.