")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 15
Perceived Barriers and Facilitators to Breast Cancer Screening Among Women in Saudi Arabia
Authors AlAbdulKader A , Gari D, Al yousif G , Alghamdi A , AlKaltham S , AlDamigh F, AlEisawi Y, AlGhamdi A, Al-Hayek O , AlMudhi A
Received 4 February 2023
Accepted for publication 12 July 2023
Published 25 July 2023 Volume 2023:15 Pages 505—513
DOI https://doi.org/10.2147/BCTT.S406029
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert Clarke
Assim AlAbdulKader,1 Danya Gari,1 Ghada Al yousif,1 Amal Alghamdi,1 Shikha AlKaltham,1 Fahad AlDamigh,2 Yazan AlEisawi,2 Abdulhadi AlGhamdi,2 Omar Al-Hayek,2 Ali AlMudhi2
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, 34224, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, 34224, Saudi Arabia
Correspondence: Shikha AlKaltham, Department of Family and Community Medicine, King Fahad Hospital of the University, Dammam, Saudi Arabia, Email [email protected]
Background: According to the World Health Organization, by the end of 2020, an estimated 7.8 million people was living with breast cancer diagnosed between 2015 and 2020; in Saudi Arabia, more than fifty percent of cancer cases are detected in late stages, which results in increased mortality rates and reduces the chances of remission. Breast cancer screening using mammography in women fifty years and older worldwide and in women forty years and older in Saudi Arabia shows a significant decrease in morbidity and mortality. However, screening rates are not satisfactory and require further investigation.
Methods: This cross-sectional study included women aged 40 years and older. Data was collected through an online survey distributed via social media platforms to all regions of Saudi Arabia. Chi-square and Fisher’s exact tests were used to examine the difference in the distribution of study variables among women who had received breast screening and those who had not. A logistic regression model was used to estimate the risk of not having breast cancer screening.
Results: A total of 973 participants completed the survey. Among respondents, 476 (48.9%) had been screened at least once in their lifetime. The main motivators for screening were: receiving an advice from a physician (41.8%), interest in early detection (39.8%), and receiving free mammography (29.7%). On the other hand, the main barriers to receiving breast cancer screening were: finding screening unnecessary (24.2%), believing screening to be painful (22.1%), and fearing abnormal results (18.6%).
Conclusion: We found that nearly half of the targeted screening group had never received mammography screening. These results warrant urgent attention, as early detection is key to better outcomes. Our study’s results aid in better understanding the public’s points of view and inform interventions to improve breast cancer.
Keywords: breast cancer, barriers, mammography screening, facilitators
Background
According to the World Health Organization, by the end of 2020, an estimated 7.8 million people were living with breast cancer diagnosed between 2015 and 2020. Globally, the confirmed death toll was 685,000 people in 2020.1 In Saudi Arabia, breast cancer cases documented in 2020 accounted for 14.2% of all cancer cases and 29% of all cases in women. Breast cancer consistently ranks as the most common type of cancer in Saudi women, with 3954 patients in 2020 alone. Of those patients, 1095 died, making breast cancer the second most common cause of cancer-related death in Saudi Arabia that year.2
Worldwide, breast-cancer screening guidelines differ, as the United Kingdom National Screening Committee (UK NSC) and the United States Preventative Services Task Force (USPSTF) recommend starting screening at fifty years old, using mammography imaging.3,4 Whereas, in Saudi Arabia, the recommended starting age is 40 years old, as breast cancer is a leading cause of female mortalities and is the most common cancer among Saudi women, accounting for 31.8% of all registered cancers in women in Saudi Arabia.5,6
A leading measure taken by the Ministry of Health in Saudi Arabia to reduce the prevalence of advanced disease is providing free breast cancer screening for all women aged 40 years old and above.5 Screening and early detection reduce morbidity and mortality rates among breast cancer patients.7 Even with such measures, screening rates were still on the lower side, as shown by a study conducted by El Bcheraoui that found that 92% of women had never had mammography screening, and 89% had not had a clinical breast exam in the previous year.8 A 2020 study by S.A. Alsareii showed poor knowledge regarding breast cancer warning signs, especially among women with risk factors.9
Some studies in Saudi Arabia show that many abstain from routine mammography screening, even with the abovementioned measures.8,10,11 These numbers and results need to be examined further to understand the underlying issues behind this abstention and to determine factors that might aid in increasing the number of screened individuals.
This study aims to understand the barriers and motivators to breast cancer screening as perceived by women in Saudi Arabia. Understanding the population’s perceived barriers and motivators may aid in providing a better clinical approach to women over 40, targeting those barriers in health promotion campaigns, and soliciting the motivators to increase the number of screened individuals.
Methods
This study was undertaken after receiving ethical approval from the Imam Abdulrahman bin Faisal University Institutional Review Board (IRB), Dammam, Saudi Arabia (approval number IRB-2021-01-180). This study complies with the Declaration of Helsinki, and the participants’ written consents were obtained after they were provided with information regarding the study’s objective and assured that their information would be kept anonymous and secure. Participants were not forced to participate; they were not approached individually or offered anything in exchange for participation.
This study was an online survey-based study conducted in Saudi Arabia, Eastern Province. Data collection was done between August 2021 and January 2022. Our study included women aged 40 years and older who were residents of Saudi Arabia, had access to the Internet, and were willing to participate in the study. We excluded responses from women aged 39 and under and women living outside Saudi Arabia.
The bespoke questionnaire we used was in Arabic and distributed online using the QuestionPro platform and was distributed via social media platforms, including Twitter, WhatsApp, and Telegram.
The questionnaire contained 42 questions divided into seven parts. The first part covered pregnancy history (marital status, number of children, age at pregnancy, breastfeeding). The second part aimed to gain information about participants’ menstrual cycle details (use of contraceptives, type of contraceptives used, age of menarche, still menstruating?). The third part asked about participants’ past medical history, surgical history, family history, and prescription medications used regularly. The fourth part was about mammogram screening (previous mammograms, timing of previous mammograms, reasons for obtaining screening, whether fine needle aspiration was done, number of past mammograms, history of radiation therapy, history of chemotherapy). The fifth part aimed to gain details about family history (breast cancer in the family, which generation, maternal or paternal side, colon cancer history in the family, pancreatic cancer history in the family, ovarian cancer history in the family, other types of cancer, having any new complaints, family history of positive BRACA 1 and BRACA 2 genes). The sixth part aimed to understand the barriers to receiving a mammogram screening test (smoking, weight, height, barriers, and motivators). The last part covered participants’ demographics (nationality, place of residency, age, job description, and level of education).
Data were analyzed using IBM SPSS Statistics for Windows, Version 23.0.0.0 (released 2015; IBM Corp., Armonk, New York, United States). Chi-square and Fisher’s exact tests were used to examine the difference in the distribution of study variables among women who had received breast screening and women who had not. A logistic regression model was used to estimate the risk of not having breast cancer screening. Adjustment of the logistic models involved variables that showed significant statistical results in the univariate analysis. A P-value of less than 0.05 was considered significant during the analysis.
Results
The total number of included participants was 973. The majority of our participants were in their 40s (n=586, 60.2%), unemployed (n=559, 57.5%), having a bachelor’s degree (n=570, 58.6%), married (n=781, 85.1%), and Saudis (n=835, 85.8%) (see Table 1).
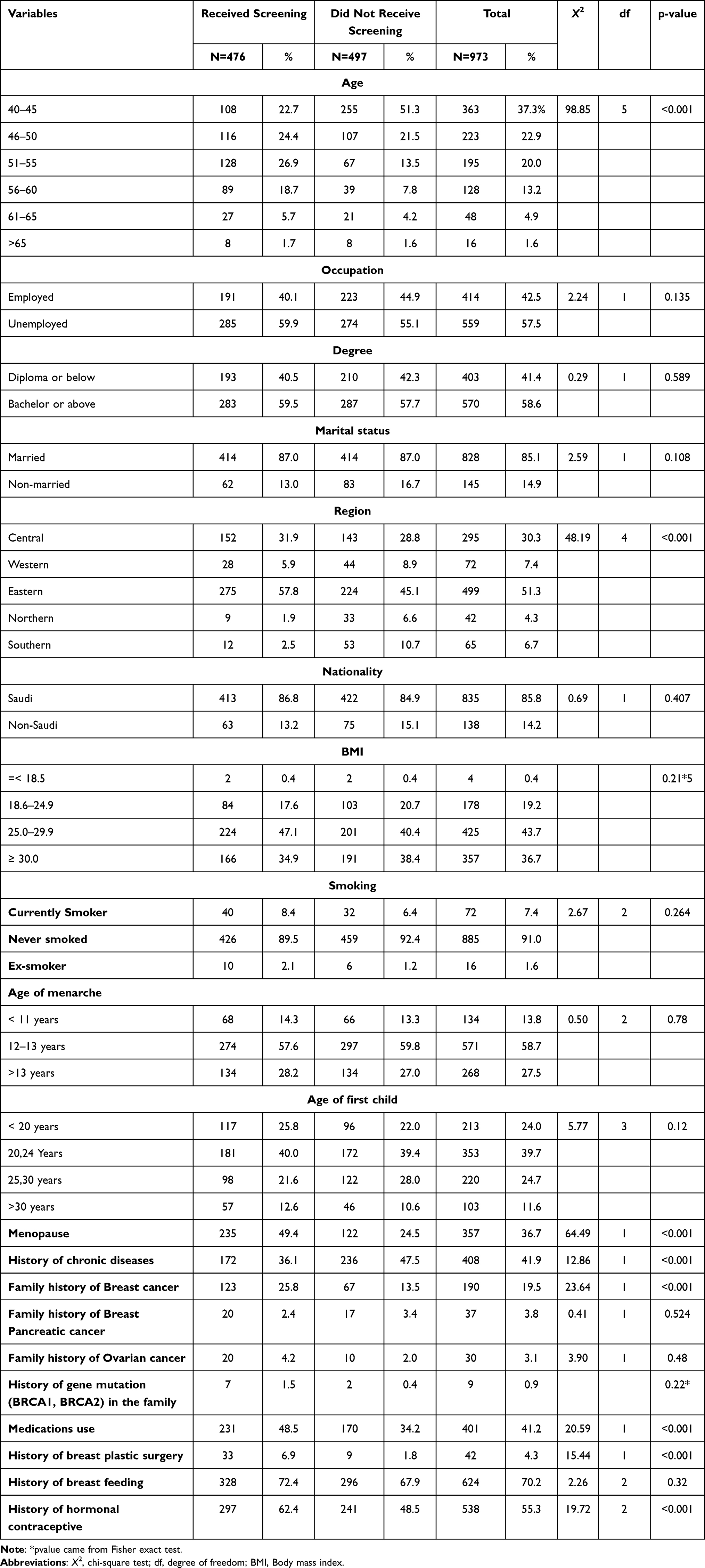 |
Table 1 The Distribution of Participants Individual Characteristics in Relation to Their Breast Screening Status |
Concerning health-related risk factors, most of our participants were overweight or obese (n=782, 80.4%) and had never smoked (n=885, 91%). Moreover, 41.9% suffered from chronic diseases, including diabetes mellitus (n=140, 14.3%), hypertension (n=153, 15.7%), polycystic ovarian syndrome (n=87, 8.9%), peripheral vascular disease (n=13, 1.3%), anemia (n=127, 13.1%), and prolactinoma (n=34, 3.5%) (see Table 1).
Regarding screening, 476 (48.9%) participants had received a screening at least once in their lifetime. The most recent screening was: within the previous year (n=236, 49.6%), from one to two years earlier (n=78, 16.4%), and more than two years earlier (n=162, 34.0%). The main reason for being screened was age (n=289, 60.7%), presence of a complaint (n=106, 22.2%), and having a family history of cancer (n=67, 14.7%). In addition, the majority of screened participants were in their early 50s (n=244, 51.3%, x2(5)=98.85, p<0.001), married (n=396, 87.6%, x2(1)=4.50, p=0.03), or from the Eastern Province (n=275, 57.8%, x2(4)=48.19, p<0.001, Table 1). Furthermore, as seen in Table 1, when comparing the distribution of the screened to the unscreened participants, the screened participants had a higher rate of chronic diseases (n=172, 36.1%, x2(1)=12.86, p<0.000), and a higher rate of family history of breast cancer (n=123, 25.8%, x2(1)=23.64, p<0.001). In addition, (n=45, 4.6%) participants had a history of breast cancer, (n=28, 62.2%) participants had received chemotherapy, and (n=27, 60%) participants had received radiotherapy. Furthermore, participants’ most common breast complaint was breast pain (n=148, 15.2%), followed by breast lump (n=48, 4.9%). However, not all patients presented with breast changes went under screening, as seen in Figure 1.
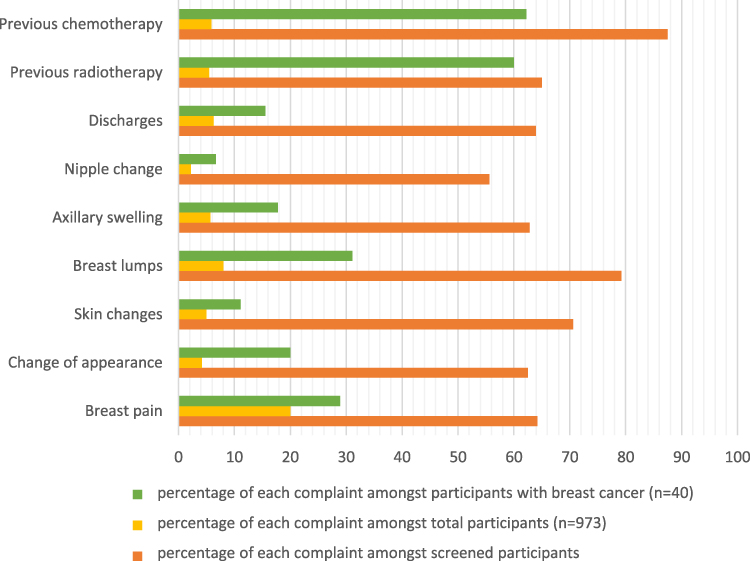 |
Figure 1 Bar graph showing the distribution of different breast complaints amongst the total participants of the study, participants with breast cancer, and screened participants. |
The screening was most common among participants who had received cancer chemotherapy (n=28,87.5%), had a breast lump (n=38, 79.2%), or showed skin changes (n=24, 70.6%). At the same time, it was least common among participants who complained of nipple discharge (n=10, 55.6%) (see Figure 1). The most commonly believed barrier regarding screening was that participants believed it was unnecessary (n=235, 24.2%), followed by the belief that screening would be painful (n=215, 22.1%) (see Table 2). The prevalence of breast screening was less among participants who believed that screening was embarrassing (n=60, 61.86%, x2(1)=5.01, p=0.025), feared the results (n=108, 59.7%, x2(1)=6.57, p=0.01), thought it was unnecessary (n=185, 78.7%, x2(1)=94.75, p<0.001), was not interested in early detection (n=22, 81, x2(1)=10.27, p<0.001), did not know where to obtain a screening (n=73, 82.9%, x2(1)=39.34, p<0.001), or had an unsupportive family (n=9, 81.8%, x2(1)=4.21, p=0.04) (see Table 2).
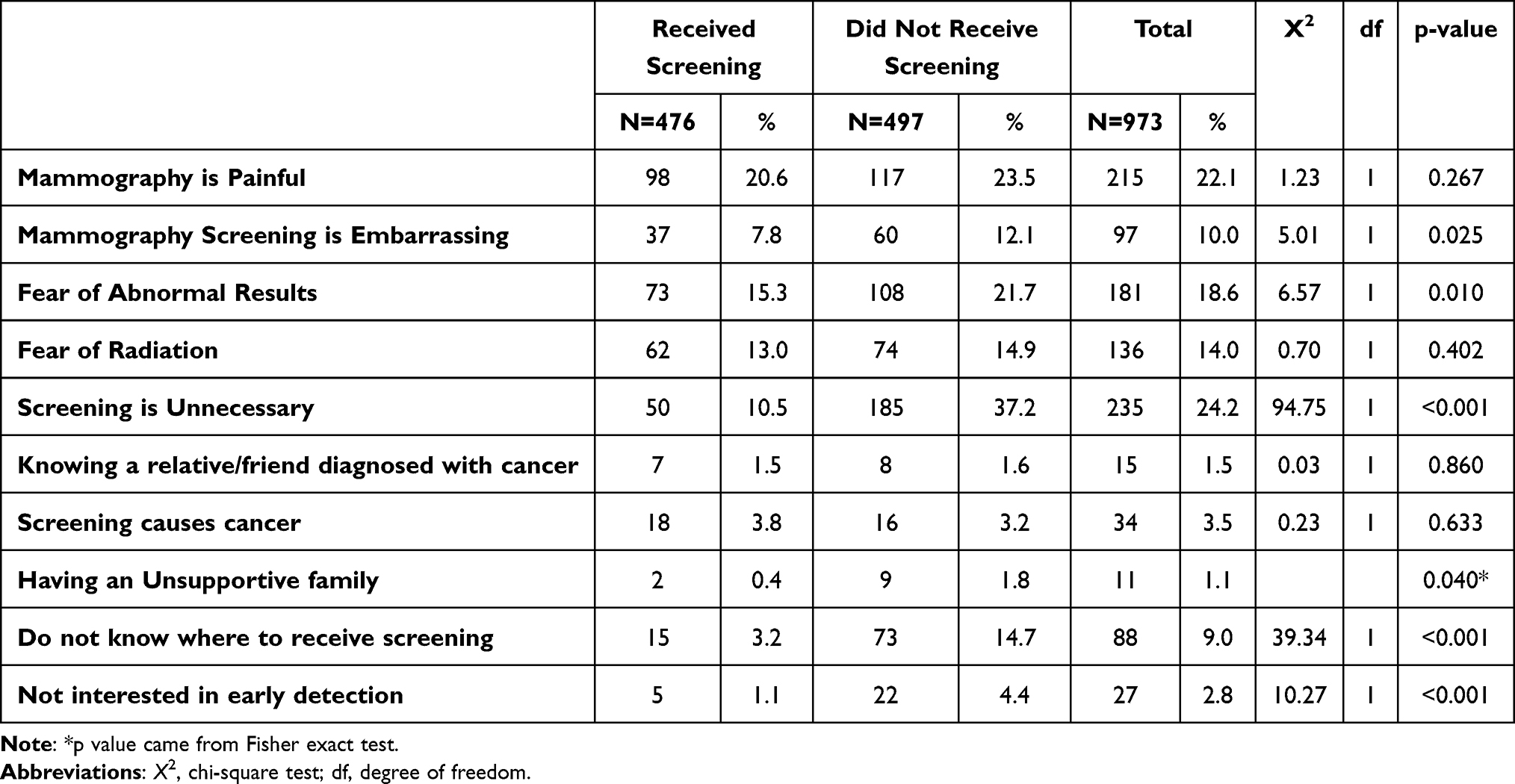 |
Table 2 The Frequency and Percentages of the Distribution of Suggested Barriers of Breast Cancer Screening in Relation to the Participants Screening Status |
On the other hand, the most common motivator for screening was receiving a physician’s advice to do so (n=407, 41.8%). However, among screened participants, the most common motivator was the interest in early detection (n=250, 52.5%). More than half (n=43, 68.3%, x2(1)=7.95, p=0.005) of participants with a relative/friend who had received mammography screening had not themselves received screenings while having a personal experience of mammography screening aligned with a higher rate of screening (n=49, 87.5%, x2(1)=35.39, p<0.001). In addition, interest in the early detection of cancer influenced the rate of screening among participants (n=250, 64.6%, x2(1)=63.21, p<0.001) (see Table 3).
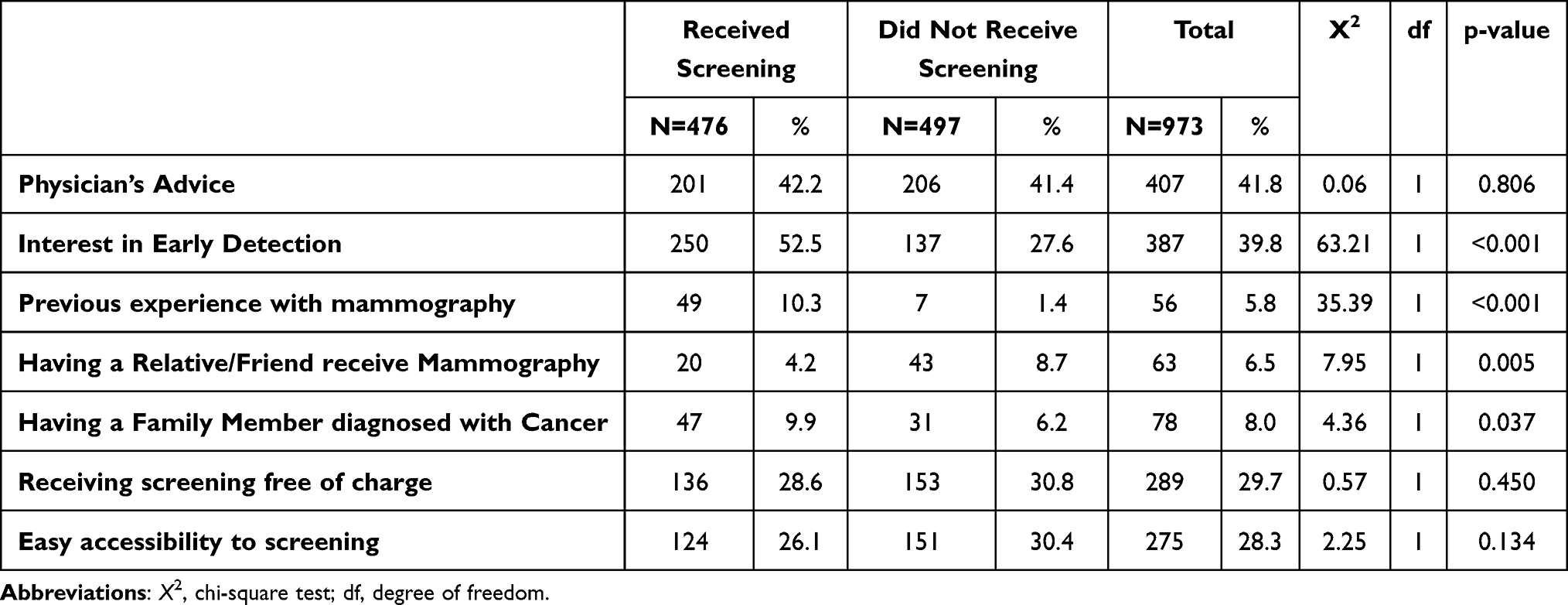 |
Table 3 The Frequency and Percentages of the Distribution of Suggested Breast Cancer Screening Motivators in Relation to Our Participants Screening Status |
As seen in Table 4, the odds of not receiving screening increased in women who did not know where to receive screening (adjusted OR=5.34, 95% CI = 2.93, 9.72), women who were not interested in early detection (adjusted OR=4.77, 95% CI=1.71, 13.26), in women who believed screening was unnecessary (adjusted OR=5.52, 95% CI=3.81, 7.99), and women who feared having an abnormal result (adjusted OR=1.62, 95% CI=1.14, 2.30).
 |
Table 4 Odd Ratios of Unadjusted and Adjusted Logistic Regression Models That Measures the Association Between Breast Cancer Screening Barriers and Not Receiving Screening |
Discussion
This study aimed to understand the motivators and barriers perceived by women regarding breast cancer screening and the factors associated with abstaining from routine screening, as well as to explore factors associated with receiving mammography screening. We hope to provide insight into the concepts physicians and stakeholders should focus on in future patient encounters and health promotion campaigns to increase the willingness to undergo routine mammography screening.
Breast cancer screening with mammography is one of the essential components of preventive care, as it has been proven to decrease breast cancer mortality across a broad age group of 39 to 70 years old.7,12,13 In this study, approximately half of the participants had received breast cancer screening at least once in their life. On the other hand, in the United States of America (USA), the Department of Health and Human Services reports that more than three-quarters of women within the screening window had received mammography screening in 2019.14 However, a local study done in 2014 showed that 92% of women within the screening population did not receive mammography.8 Moreover, a recent local study done in 2018 showed a slight increase, as 12.4% of the participants had received mammography screening.10 The increase since then in the local percentage noted in this study may indicate a gradual and promising increase in the public’s awareness, as the Saudi MOH has only started its yearly breast cancer awareness campaigns in 2006. The studies mentioned above were only done six and 12 years after the campaign’s start.
Most screened individuals were in their early 50s, which might be attributed to known other countries’ guidelines recommending mammograms for all women aged 50 and above.3,4 However, Saudi Arabia’s Ministry of Health recommends starting regular screening at the age of 40, as the average age of diagnosis is 52 years old.5 Moreover, screening was significantly higher in individuals living in Eastern Province. A possible explanation might be related to the Saudi Cancer Registry (SCR) published results, which showed that the Eastern Province has the highest age-standardized rate of breast cancer—37.1/100,000 in 2015 and 52.2/100,000 in 2017.6
This study found a significant association between having a family history of breast cancer and receiving mammography screening. This finding is in adherence with the results of Seiffert et al, who found that individuals with a family history of breast cancer had significantly more mammography screenings throughout their lives than those with no family history of breast cancer. Interestingly, the screening rate was not different whether the person was a first-degree or a second-degree family member.13
An expected finding was that having a chronic disease is associated with receiving mammography screening. This result might be explained by the fact that individuals with chronic diseases frequently encounter their physicians, who are likely to recommend undergoing routine screenings. This study showed that a physician’s advice was the top factor in considering mammography screening. This theory was proven by a recent study done by Elewonibi and Nkwonta, who found that women with frequent primary care encounters were more likely to undergo routine screenings.15
As for the motivators encouraging women to undergo mammography screening, this study found that the most common influencer was “physician’s advice”, reported by nearly half of the participants. In an explicit acknowledgment of the importance of this motivator, another study conducted by Jovicevic et al found that “physician advice” was the most influential factor that caused a significant increase in breast cancer screening rates.16 This result emphasizes the importance of physicians advising patients to undergo routine screenings during every visit.
Moreover, interest in early detection was the second most common motivator among this study’s participants, as it was reported by more than one-third of the participants. Furthermore, it is the leading motivator among participants who have received mammography screening. When coupled with timely treatment access, early detection will form a critical prerequisite, as the more clinical downstaging achieved, the lower the mortality rate will be.7
Our study showed that having a personal mammography experience influenced the screening rate, as most of our participants who had undergone mammography tended to continue to have screenings. On the other hand, most participants with a family experience of mammography had not had screenings. This comparison raised a statistically significant difference in the screening rate between these two groups.
It is puzzling that personal mammography experience positively impacts the screening rates while family experience does not. This observation signifies the importance of practical intervention to increase the community’s awareness that family history is an important predisposing risk factor for breast cancer. A study in Serbia showed that the most common motivators among participants are gynecologist advice, health maintenance, and family history of cancer, respectively.16 It is not surprising that most community motivators are consistent.
Regarding barriers that keep participants from obtaining screenings, our study revealed that the most common barrier to screening was the misconception that mammograms were unnecessary. A quarter of participants indicated they were not interested in undergoing mammograms. This seems consistent with another cross-sectional survey conducted in Saudi Arabia in 2017; the study raised the fact that one-third of participants believe that screening is unnecessary. Another 22% of participants believed that screening would be painful. When comparing this to a collateral study in Saudi Arabia, the second most common barrier was that women were worried about possible abnormal results.17
Our study determined that the third most common barrier that keeps people away from screening is the fear of abnormal results. Similarly, a group of Greek women described “Fear of pain, fear of a serious diagnosis, embarrassment, and stress while anticipating the results” as the main factors in avoiding mammograms in a study by Trigoni et al.18
Moving to a global point of view, a systematic review conducted in 2020 revealed that lack of awareness is one of the most prominent barriers worldwide.19 Lack of awareness encompasses multiple aspects, such as the importance of screening, the benefits of early detection of breast cancer, the consequence of late diagnosis, the time of screening, and the accessibility of screening. Furthermore, fear is the most prominent psychological barrier considered in multiple studies.20–22
Conclusion
The findings of this study showed a marked increase in the rate of mammography screening in Saudi Arabia, reflecting the rising awareness of women in the area and showing that there is room for improvement as, despite the rise in numbers, the percentage is still not satisfactory.
A thorough understanding of the perceived barriers and motivators is warranted to encourage women to undergo routine screening. This study found that the primary motivators were physicians’ advice and interest in early detection. These findings encourage physicians to discuss routine screenings and their benefits, as physician advice may increase the number of screened individuals.
This study found that the main barriers to screening are a person’s belief that screening is unnecessary, lack of interest in early detection, fear of abnormal results, embarrassment, fear of pain, and not knowing where to receive screening. All of the mentioned barriers could be tackled by increasing public awareness and explaining the procedure thoroughly. Another critical barrier was the lack of family support. One way to overcome this is by raising awareness among the population in general, men and women, as breast cancer can affect both sexes and having educated families encourage their family members to undergo regular screening.
The standing strength of this study is that it provides a comprehensive understanding of the general public’s insights and beliefs. As mentioned previously, this directs the attention of physicians and stakeholders toward tackling these specific fears and barriers to have a tangible outcome at the individual level in physician-patient encounters and the community level through health promotion campaigns.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Who.int. Breast cancer; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer.
2. World Health Organization. Saudi Arabia fact sheet. International Agency for Research on Cancer; 2022. Available from: https://gco.iarc.fr/today/data/factsheets/populations/682-saudi-arabia-fact-sheets.pdf.
3. Gov.uk. Breast cancer; 2023. Available from: https://view-health-screening-recommendations.service.gov.uk/breast-cancer/.
4. Uspreventiveservicestaskforce.org. US Preventive Services Taskforce. Breast cancer: screening; 2016. Available from: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/breast-cancer-screening.
5. Ministry of Health. National campaign for breast cancer awareness. Saudi Arabia: Ministry of Health; 2022. Available from: https://www.moh.gov.sa/en/HealthAwareness/Campaigns/Breastcancer/Pages/stat.aspx.
6. Saudi Health Council. Saudi Cancer Registry [Internet]; 2018. Available from: https://shc.gov.sa/Arabic/NCC/Activities/Pages/AnnualReports.aspx.
7. Christiansen SR, Autier P, Støvring H. Change ineffectiveness of mammography screening with decreasing breast cancer mortality: a population-based study. Eur J Public Health. 2022;32(4):630–635. doi:10.1093/eurpub/ckac047
8. El Bcheraoui C, Basulaiman M, Wilson S, et al. Breast cancer screening in Saudi Arabia: free but almost no takers. PLoS One. 2015;10(3):e0119051. doi:10.1371/journal.pone.0119051
9. Alsareii SA, Alqahtani SM, Alamri AM, et al. Awareness of breast cancer among female students and faculty from Najran University, Najran, Saudi Arabia. Asian Pac J Cancer Prev. 2020;21(5):1415–1422. doi:10.31557/APJCP.2020.21.5.1415
10. Bakr R, AL-Mulhim F, Almedallah D, Alkaltham N, Alotaibi A, Alnoaim S. Screening mammography and breast self-examination: attitudes and practices of women in the Eastern Province of Saudi Arabia. Saudi J Health Sci. 2018;7(2):89. doi:10.4103/sjhs.sjhs_4_18
11. Alshahrani M, Alhammam SYM, Al Munyif HAS, et al. Knowledge, attitudes, and practices of breast cancer screening methods among female patients in primary healthcare centers in Najran, Saudi Arabia. J Cancer Educ. 2019;34(6):1167–1172. doi:10.1007/s13187-018-1423-8
12. Magnus MC, Ping M, Shen MM, Bourgeois J, Magnus JH. Effectiveness of mammography screening in reducing breast cancer mortality in women aged 39–49 years: a meta-analysis. J Womens Health. 2011;20(6):845–852. doi:10.1089/jwh.2010.2098
13. Seiffert K, Thoene K, Eulenburg CZ, et al. The effect of family history on screening procedures and prognosis in breast cancer patients - results of a large population-based case-control study. Breast. 2021;55:98–104. doi:10.1016/j.breast.2020.12.008
14. Health.gov. Increase the proportion of females who get screened for breast cancer — c-05 - Healthy People 2030; 2023. Available from: https://health.gov/healthypeople/objectives-and-data/browse-objectives/cancer/increase-proportion-females-who-get-screened-breast-cancer-c-05.
15. Elewonibi B, Nkwonta C. The association of chronic diseases and mammography among Medicare beneficiaries living in Appalachia. Womens Health. 2020;16:1745506520933020. doi:10.1177/1745506520933020
16. Jovicevic A, Ristic S, Mandic V, et al. Factors influencing participation in breast cancer opportunistic screening in Belgrade, Serbia. J BUON. 2018;23(3):706–712.
17. Al-Wassia RK, Farsi NJ, Merdad LA, Hagi SK. Patterns, knowledge, and barriers of mammography use among women in Saudi Arabia. Saudi Med J. 2017;38(9):913–921. doi:10.15537/smj.2017.9.20842
18. Trigoni M, Griffiths F, Tsiftsis D, Koumantakis E, Green E, Lionis C. Mammography screening: views from women and primary care physicians in Crete. BMC Womens Health. 2008;8(1):20. doi:10.1186/1472-6874-8-20
19. Wu Z, Liu Y, Li X, Song B, Ni C, Lin F. Factors associated with breast cancer screening participation among women in mainland China: a systematic review. BMJ Open. 2019;9(8):e028705. doi:10.1136/bmjopen-2018-028705
20. Marzouq Muhanna A, Floyd MJ. A qualitative study to determine Kuwaiti Women’s knowledge of breast cancer and barriers deterring attendance at mammography screening. Radiography. 2019;25(1):65–71. doi:10.1016/j.radi.2018.10.003
21. Kim J-H, Kim O. Predictors of perceived barriers to mammography in Korean women. Asian Nurs Res. 2008;2(2):74–81. doi:10.1016/S1976-1317(08)60031-6
22. Abdel-Aziz SB, Amin TT, Al-Gadeeb MB, et al. Perceived barriers to breast cancer screening among Saudi women in primary care setting. J Prev Med Hyg. 2018;59(1):E20–9. doi:10.15167/2421-4248/jpmh2018.59.1.689
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.