Back to Journals » Drug Design, Development and Therapy » Volume 20
Peptide-Based Therapeutics for Alzheimer’s Disease: Medicinal Chemistry, AI-Guided Computational Design, and Blood–Brain Barrier Delivery
Authors Al Khzem AH ![]() , Gomaa MS
, Gomaa MS ![]()
Received 18 January 2026
Accepted for publication 2 April 2026
Published 13 April 2026 Volume 2026:20 597087
DOI https://doi.org/10.2147/DDDT.S597087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Abdulaziz H Al Khzem, Mohamed S Gomaa
Department of Pharmaceutical Chemistry, College of Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Eastern Province, 31441, Kingdom of Saudi Arabia
Correspondence: Abdulaziz H Al Khzem, Mohamed S Gomaa, Email [email protected]; [email protected]
Abstract: Alzheimer’s disease (AD) represents a pressing challenge in modern medicine, with current therapeutics offering only symptomatic relief. Peptide-based therapeutics have emerged as promising candidates owing to their target specificity, favorable safety profiles, and ability to modulate protein–protein interactions inaccessible to small molecules. This narrative review evaluates medicinal chemistry and artificial intelligence (AI)-driven approaches that are reshaping peptide drug discovery for AD, spanning target selection, sequence design, synthesis optimization, and central nervous system (CNS) delivery. Peptides targeting key AD pathological mechanisms-including amyloid-β (Aβ) aggregation inhibition, tau hyperphosphorylation disruption, and neurotrophic signaling enhancement-are discussed alongside strategies such as cyclization, D-amino acid incorporation, PEGylation, and peptidomimetic design to improve metabolic stability and blood–brain barrier (BBB) penetration. We review automated fast-flow peptide synthesis with inline UV-vis monitoring as a platform for rapid, high-fidelity preparation of complex sequences suitable for translational development. Delivery platforms-including cell-penetrating peptides, intranasal formulations, and nanocarrier systems-which primarily increase systemic exposure or fundamentally alter CNS distribution mechanisms are presented. AI and machine-learning (ML) technologies, molecular simulations, and structure-prediction systems are examined as an integrated pipeline that supports end-to-end design, validation, and optimization, with emphasis on rigorous QSAR and docking/MD validation practices. Clinical translation is analyzed through peptide repurposing (e.g. GLP‑1 receptor agonists, intranasal insulin, oxytocin), dedicated peptide candidates, and evolving regulatory expectations. Finally, we outline concrete design checklists for CNS ready peptides, discuss key translational bottlenecks, and propose priorities for the next 5– 10 years of peptide-based AD therapy development.
Keywords: Alzheimer’s disease, blood–brain barrier, peptide drugs, artificial intelligence, drug discovery, pharmaceutical medicinal chemistry, clinical translation
Introduction
Background
Neurodegenerative disorders are among the most challenging and complex issues in modern medicine. They are characterized by progressive neuronal function and structural loss and include conditions such as Alzheimer’s disease (AD), Parkinson’s disease (PD), amyotrophic lateral sclerosis, and Huntington’s disease, which affect millions of individuals worldwide and impose a significant burden on healthcare systems.1,2 Alzheimer’s disease is the most common, accounting for approximately 60–80% of dementia cases worldwide.3,4 The decision to concentrate on Alzheimer’s disease in this review is based on its high prevalence, devastating effect on cognitive function and quality of life, and the absence of effective disease-modifying therapies. After decades of investigation, current treatments for AD remain mostly symptomatic, providing only modest gains in memory and function without affecting the disease course.
Peptide medications have also become an up-and-coming therapeutic option for the treatment of Alzheimer’s disease because they can selectively target the molecular mechanisms involved in disease pathology.5 For example, peptides that interfere with the aggregation of amyloid-β (Aβ) or tau proteins, which are key features of AD, may be able to stop or reverse neurodegeneration. Other peptides, including neurotrophic mimetics, have been designed to promote neuronal survival, synaptic plasticity, and cognition by activating selected growth factor signaling pathways.6–8 Although more specific than small molecules with fewer off-target effects, peptide therapeutics are an attractive option for addressing the multifaceted and progressive aspects of AD. Achieving their full potential requires overcoming significant hurdles, including delivery and stability in the central nervous system (CNS). However, the translation of peptide drugs into effective CNS therapies is fraught with challenges, primarily because of the protective nature of the blood–brain barrier (BBB). The BBB, formed by tightly connected endothelial cells, acts as a selective gatekeeper that restricts the entry of large hydrophilic molecules, including most peptides, into the brain. This physiological barrier presents a significant obstacle for peptide delivery, compounded by the inherent instability of peptides in the systemic circulation due to enzymatic degradation and rapid renal clearance. Despite their therapeutic potential, peptide drugs face substantial limitations in reaching their intended targets within the CNS.1,9
Recent advancements in medicinal chemistry have introduced numerous innovative methods to enhance the pharmacokinetic and pharmacodynamic characteristics of peptide medicines. Cyclization of the peptide structure, N-methylation, and replacement of the native L-amino acids with D-amino acids can lead to increased stability toward enzymes and extension of half-life.10 Linkage with lipid groups or cell-penetrating peptides increases BBB penetration, whereas delivery of nanoparticles or liposomes permits site-specific and slow release.11 Moreover, the discovery of peptidomimetic molecules that emulate the activity of peptides, but not their precise structures, has further extended the therapeutic use of this drug class. Such chemical advances are critical for making peptide drugs more feasible under CNS conditions.12
Complementing these advances, artificial intelligence (AI) and machine learning (ML) are increasingly being used in modern medicinal chemistry and peptide drug discovery. AI-powered platforms can generate novel peptide sequences with optimized binding affinities, predict peptide–protein interactions, and model BBB permeability profiles. ML algorithms also assist in the early prediction of absorption, distribution, metabolism, excretion, and toxicity (ADMET) properties, thereby accelerating the lead optimization process. AI-driven retrosynthetic planning and automation tools facilitate efficient synthesis of complex peptide candidates. Together, these technologies reduce the time and cost traditionally associated with peptide drug development while enhancing design precision and accuracy.13,14
Scope and Conceptual Framework
This review is structured around a translational pipeline that links computational and AI‑guided discovery to medicinal chemistry optimization, scalable synthesis, BBB‑competent delivery, and clinical testing of peptide therapeutics in Alzheimer’s disease. Rather than cataloging approaches in isolation, we emphasize how these components interact in a stepwise “AI → Design → Synthesis → Delivery → Clinical Translation” framework. Sections 4 and 5 focus on sequence‑level and structural design, including stability and target engagement; Section 4.2.5 addresses synthesis platforms; Sections 4.2.1, 4.2.2 and the BBB‑focused portions of Sections 4 and 7 discuss delivery; and Sections 6 and 7 examine clinical translation, regulatory considerations, and future directions. Our goal is to provide peptide chemists and translational scientists with a roadmap that connects technological advances to practical decision‑making across this continuum (Figure 1).
 |
Figure 1 The proposed translational pipeline for peptide‑based AD therapeutics, beginning with AI‑enabled target identification and de novo sequence generation, followed by medicinal chemistry optimization and stability engineering, scalable synthesis (including fast‑flow platforms), BBB‑competent delivery strategies, and finally clinical trial design and regulatory evaluation. Feedback arrows indicate that data from in vitro assays, in vivo models, and early‑phase trials iteratively refine upstream AI models and design criteria. |
Search Strategy
This review aimed to evaluate the current evidence on the therapeutic potential of peptide-based drugs for central nervous system (CNS) disorders, with a particular focus on Alzheimer’s disease (AD). We sought to identify peptide candidates that demonstrate structural and pharmacological properties supporting disease modifying potential, target engagement, and central bioavailability in preclinical and clinical studies.
To ensure a comprehensive and reproducible assessment, we designed a search strategy across multiple electronic databases. The literature search covered publications from January 2010 to January 2026 across PubMed, Scopus, Web of Science, and Embase, using combinations of controlled vocabulary and free‑text terms related to “Alzheimer’s disease”, “peptide therapeutics”, “Aβ aggregation”, “tau”, “GLP‑1 receptor agonists”, “blood–brain barrier”, “nanoparticles”, “intranasal delivery”, and “artificial intelligence” or “machine learning” in drug discovery. We restricted inclusion to peer‑reviewed articles and registered clinical trials in humans or in vivo/in vitro models relevant to AD or closely related neurodegenerative phenotypes; reviews, commentaries, editorials, and purely theoretical pieces were used only for background context. Non‑English publications and studies focusing exclusively on non‑peptidic modalities were excluded. Titles and abstracts were screened independently by both authors, followed by full‑text evaluation of potentially eligible articles. Duplicates were identified and removed using reference‑management software and manual checking. We also included studies investigating peptide-based therapeutics for CNS diseases, focusing on AD, across in vivo animal models, human clinical trials, and advanced in vitro systems. Studies employing strategies to enhance CNS delivery including rational drug design, peptide conjugation, and nanocarrier systems were also considered. When evidence from different sources was inconsistent, we prioritized larger, randomized and controlled clinical trials over smaller or open‑label studies, and clinical data over preclinical findings, while also considering convergence across independent mechanistic and pharmacokinetic studies.
Disease Context and Pathophysiology
Alzheimer’s Pathology
AD is pathologically characterized by two hallmark lesions: extracellular Aβ plaques and intracellular neurofibrillary tangles composed of hyperphosphorylated tau protein.15,16 The aggregation of Aβ into oligomers and fibrils leads to synaptic dysfunction and neuronal toxicity, forming a central hypothesis known as the amyloid cascade model.15–18 In parallel, the accumulation of hyperphosphorylated tau disrupts microtubule stability, impairs axonal transport, and ultimately leads to neuronal death.19,20 These pathological events are further exacerbated by a chronic inflammatory response involving microglial activation, cytokine release, and blood–brain barrier disruption, contributing to a toxic neural environment.21–24 Initiating factors, such as post-translational modifications, oxidative stress, and mutations in APP, PSEN1, and PSEN2 promote the misfolding of Aβ peptides and tau proteins.25 This pathological cascade underlies the key features of AD and highlights the mechanistic link between molecular insults and neurodegeneration.
The failure of monotherapies targeting only one pathological component has led to a growing consensus that multitarget strategies are essential. Peptide-based interventions are desirable in this context, as they can be designed to inhibit Aβ aggregation, block tau hyperphosphorylation, or modulate neuroinflammatory pathways simultaneously.21
Aβ, Tau, BACE1, and Design Implications
Three primary molecular targets control the therapeutic landscape of AD: Aβ, tau protein, and β-site amyloid precursor protein cleaving enzyme 1 (BACE1). Aβ targeting is achieved by inhibiting Aβ production (eg., BACE1 inhibitors), inhibiting Aβ aggregation (eg., Aβ-binding peptides), or facilitating Aβ clearance through immunotherapy or enzymatic breakdown.13,19,20 BACE1 is a challenging but inviting target, considering its function in the initial cleavage of amyloid precursor protein (APP) to generate Aβ peptides. However, complete inhibition of BACE1 results in tremendous off-target effects because of its involvement in synaptic function and myelination.26
Tau protein is a key therapeutic target. Disease-causing forms propagate in a prion-like manner throughout the brain. Peptides that target tau can interfere with oligomer formation or inhibit its hyperphosphorylation by targeting kinases like GSK-3β or CDK5. Unlike small molecules, peptide therapeutics can be engineered to target specific pathological conformations of tau or aggregation-prone motifs, thereby providing greater specificity and lower toxicity.13,21
Their intracellular and extracellular localization is an important design consideration when targeting these molecules. Aβ aggregation begins extracellularly, favoring peptide drugs with cell-penetrating capabilities or those that can persist in the interstitial fluid.27 Conversely, tau and BACE1 are predominantly intracellular, necessitating the design of peptides that are capable of efficient cellular uptake and endosomal escape. These factors have driven the development of conjugated peptides, lapidated constructs, and nanoparticle delivery systems to improve CNS permeability and target engagement.28–30
Peptide Therapeutics in CNS Diseases
Peptides, by their modular amino acid composition and secondary structures, possess a unique set of physicochemical characteristics that directly influence their drug-like behavior. They are typically highly hydrophilic, rendering them generally soluble in aqueous environments, which is advantageous for their systemic administration and formulation. However, the same hydrophilicity limits their membrane permeability, posing a significant challenge for crossing lipid-rich barriers, such as the BBB.31 Peptides are also subjected to enzymatic degradation by exopeptidases and endopeptidases, particularly in the gastrointestinal tract and bloodstream. Their metabolic instability and short half-lives often necessitate chemical modifications or the use of protective delivery systems. Peptides can adopt alpha-helical, beta-sheet, or random coil structures, and their conformational plasticity plays a crucial role in target recognition. Owing to the restricted conformational entropy, constrained or cyclic peptides often show enhanced protease resistance and target selectivity, making them attractive scaffolds for CNS-targeted therapeutics.32
Developmental Challenges
Despite their promise as therapeutic agents, peptide drugs face considerable developmental challenges that impede their clinical translation to neurodegenerative diseases, particularly AD. These obstacles include molecular instability, delivery limitations (particularly across the BBB), immunogenicity, and issues related to scalable manufacturing. Understanding and overcoming these hurdles is crucial for advancing peptide-based therapeutics from the bench to the bedside.
Challenges to CNS Delivery
The pharmacokinetics (PK) of peptide drugs are substantially affected by their tendency to swift renal clearance and poor oral bioavailability, which are mainly based on their size, polarity, and enzymatic lability. Formidable physiological and PK challenges hinder effective therapeutic interventions for AD using peptide-based drugs.33,34 The majority of peptide drugs are required to be administered through parenteral routes (eg., intravenous, subcutaneous) to prevent first-pass metabolism. Additionally, peptides have a limited capacity to pass through the blood–brain barrier, which is a significant obstacle in CNS drug development.30
Stability Issues: Degradation and Short Half-Life
A primary limitation of therapeutic peptides is their intrinsic instability. Linear peptides are highly susceptible to enzymatic degradation by exopeptidases and endopeptidases, particularly in the gastrointestinal tract and systemic circulation. This leads to rapid proteolytic cleavage, significantly reducing their half-life, and often necessitating frequent dosing or parenteral administration, which can diminish patient compliance. For example, the therapeutic peptide NAP (NAPVSIPQ), derived from activity-dependent neuroprotective protein, showed potent neuroprotective activity in vitro but exhibited limited in vivo stability, curtailing its therapeutic potential.35,36 In AD, where chronic administration is often required, poor stability represents a significant roadblock for the sustained bioavailability of therapeutic peptides, highlighting the necessity for structural optimization and delivery innovations.
Delivery Barriers: Oral Bioavailability and Blood–Brain Barrier (BBB) Penetration
Oral administration remains the preferred route for chronic therapy, owing to its convenience and patient adherence. However, peptides generally suffer from poor oral bioavailability (<1%) owing to enzymatic digestion of the gastrointestinal tract and low permeability across epithelial membranes.37 Consequently, most peptide drugs require invasive routes of administration, such as intravenous or intranasal delivery, which limits their practical utility in neurodegenerative disorders. A more formidable barrier is the BBB, which restricts the entry of over 98% of small-molecule drugs and nearly 100% of macromolecules, including therapeutic peptides.38
Although generally lower than that of protein biologics, the immunogenic potential of peptide therapeutics remains a concern, particularly with repeated administrations. Immunogenicity may arise from non-native sequences, aggregation, or impurities introduced during synthesis and formulation.39 The development of neutralizing antibodies could compromise therapeutic efficacy and safety in neurodegenerative conditions that require long-term therapy. Another critical bottleneck is in the manufacturing process. The large-scale synthesis of therapeutic peptides with high purity and batch-to-batch consistency remains a challenge. Solid-phase peptide synthesis (SPPS) has revolutionized peptide production; however, longer sequences (>30 amino acids) often suffer from low yields and purification difficulties owing to incomplete coupling or side reactions.32 Furthermore, peptides containing modified residues, disulfide bonds, or specific folding motifs require complex downstream processing, which increases the production costs.
Overcoming Challenges
Fortunately, recent advances in drug delivery, design strategies, and interdisciplinary collaboration have helped address these challenges and make peptide therapies more viable. This section will examine the reported strategies and techniques that have shown promise in addressing the aforementioned challenges.
The BBB presents a significant obstacle to central nervous system delivery, contributing to the poor permeability and rapid enzymatic degradation of peptide therapeutics. To address these limitations, current peptide drug design strategies aim to enhance stability and enable CNS penetration while targeting key pathological processes. These include stabilizing tau protein to preserve microtubule integrity, inhibiting Aβ aggregation by blocking the oligomerization and fibrillization cascade, and mimicking molecular chaperones, such as TRIM11, to disaggregate tau polymers and facilitate their proteostatic clearance. These approaches collectively reflect the multifaceted objectives of rational peptide design in combating neurodegenerative proteinopathies. For example, the fusion of neuroprotective peptides with rabies virus glycoprotein (RVG29) has shown promise in delivering active molecules into the CNS via nicotinic acetylcholine receptor-mediated transcytosis.40
BBB Delivery Approaches
Conceptually, BBB‑related strategies can be divided into two groups. First, approaches that primarily increase systemic exposure, such as PEGylation, albumin‑binding motifs, depot formulations, or oral absorption enhancers, extend circulation time and overall exposure but do not fundamentally alter how the peptide crosses the BBB. Second, approaches that change the mechanism of CNS distribution, including receptor‑mediated transcytosis (eg., transferrin or insulin receptor ligands), cell‑penetrating peptides, exosome or nanoparticle shuttles, and intranasal administration, directly target or bypass the BBB. In practice, smaller (≤2–3 kDa), moderately lipophilic or cyclic peptides with low polar surface area may benefit from prodrug or lipidation strategies combined with half‑life extension, whereas larger, highly charged, or hydrophilic constructs generally require an active transport or carrier‑based solution. Matching peptide physicochemical properties to the most appropriate BBB strategy early in design can avoid late‑stage failures driven by inadequate brain exposure.41–43
Delivery Systems: Nanoparticles and Exosome Mimetics
Peptides quickly break down in the body and struggle to cross the BBB. Efforts to enhance BBB penetration have focused on several strategies, including chemical modification (eg., lipidation or use of cell-penetrating peptides), nanocarrier encapsulation (eg., liposomes, exosomes, and polymeric nanoparticles), and receptor-mediated transcytosis (eg., using ligands for transferrin or insulin receptors).44,45 Sophisticated formulations, including liposomes, cell-penetrating peptides, nanoparticle carriers, and intranasal delivery systems, have emerged as valuable tools for evading BBB limitations without sacrificing effectiveness.46 Another promising tool is exosome mimetics, which are engineered particles that mimic the natural cellular messengers. These vesicles can naturally cross the BBB and deliver their cargo directly to neurons.47 By loading therapeutic peptides into exosome-like structures, these built-in transport systems can be used to safely and efficiently deliver drugs.
Peptide‑only and nanoparticle‑assisted BBB strategies offer complementary trade‑offs. Direct engineering of small, cyclic, or lipidated peptides can yield relatively simple products with predictable PK, lower manufacturing complexity, and reduced long‑term accumulation in off‑target tissues, but is constrained by strict physicochemical limits on size, charge, and polarity. In contrast, encapsulation of peptides within polymeric nanoparticles, liposomes, or exosome mimetics can dramatically enhance brain delivery and protect unstable sequences without heavily modifying the peptide itself; however, these systems introduce additional layers of complexity in formulation, scalability, and regulatory characterization (eg., heterogeneity of particle size, surface composition, and long‑term biodistribution). For AD, lean “peptide‑only” solutions may be preferable for chronic administration when suitable scaffolds exist, whereas nanoparticle‑assisted strategies are particularly attractive for larger or highly polar peptides that cannot realistically meet BBB constraints through medicinal chemistry alone.48
Rational Design via SAR
The structure–activity relationship (SAR) of peptide-based CNS therapeutics is critical for rational drug design. Key activity determinants include the amino acid sequence, side-chain composition, hydrophobic/hydrophilic balance, and molecular conformation. For example, Aβ-targeting peptides often incorporate hydrophobic residues that complement the aggregation-prone regions of Aβ, enabling high-affinity binding and aggregation inhibition.49 SAR studies have revealed that backbone cyclization, the introduction of β-amino acids, and stapling techniques can enhance receptor affinity, proteolytic stability, and BBB penetration without significantly compromising solubility. Additionally, peptide–drug conjugates (PDCs) and multivalent constructs have emerged as strategies to boost efficacy by combining targeting moieties with effector functions in a single molecular framework. Computational tools, including molecular dynamics simulations and quantitative SAR (QSAR) modelling, increasingly support peptide optimization by predicting favorable conformations and identifying binding hotspots, thereby accelerating the discovery of lead candidates with CNS penetration potential.50
Improving the stability and activity of peptide drugs has begun with better design. Traditional drug discovery involves many trial-and-error processes. However, researchers are now using SAR studies and computer modelling to predict how small changes in a peptide’s structure affect its behavior in the body.51 This includes the stability of the peptide, how well it binds to its target, and how likely it is to be broken down by enzymes. For example, modifying the peptide backbone using non-natural amino acids or cyclizing the peptide can increase its resistance to degradation. These design tweaks, informed by predictive models and ML tools, have already led to more stable peptide candidates that retain their ability to block toxic protein interactions in AD.52
Peptide drug development is no longer just a domain of chemists. Tackling complex diseases such as Alzheimer’s requires input from multiple fields. Medicinal chemists work to improve peptide structure and stability. Computational scientists utilize AI to model the behavior of peptides in the body, whereas pharmacologists investigate how drugs interact with the brain and how the body processes them.52,53 By combining the expertise from these areas, researchers can design peptides more efficiently, predict side effects earlier, and streamline the path from laboratory discovery to clinical testing. For example, collaborations between chemists, imaging specialists, and pharmacologists have led to the development of peptide-based tracers for brain imaging in Alzheimer’s patients, aiding both diagnosis and treatment monitoring.54
Stability & Efficacy Enhancement for CNS Targeting
Medicinal chemistry approaches to enhance peptide stability and efficacy include structural alterations, such as cyclization, terminal protection, and non-natural amino acids, each designed to enhance metabolic stability, binding affinity, and pharmacokinetic properties.55–57
Cyclization
Cyclization is perhaps one of the most effective methods to increase the stability and activity of peptide therapeutics, especially for neurological diseases.32,58 Head-to-tail cyclization stabilizes the conformation of the peptide by covalently connecting the N- and C-termini, increasing protease resistance, and decreasing susceptibility to enzymatic degradation. Stapling is an example of a cyclic constraint whereby incorporating artificial cross-links (most achieved via side-chain interactions) holds the peptide in a target bioactive structure.59–61 Such processes increase metabolic stability and can further increase receptor binding affinity and selectivity towards a target, which is critical to manifest therapeutic activity within the CNS. Additionally, such cyclic peptides are generally more effective at penetrating biological barriers such as the BBB because of their rigid and compact structures, which facilitate better membrane penetration and receptor binding.59,60
In a recent example, researchers have explored cyclic cell-penetrating peptides (CPPs) in which hydroxy- or amino-prolines in β-turns are replaced by hydrophobic residues to improve uptake. Screening 17 linear and cyclic peptides showed that one cyclic peptide, cCPP 15, had particularly high permeability and efficiently delivered a fluorophore (ATOTA) and EGFP into MCF-7 and HeLa cells. Structurally, cCPP 15 contains two endocyclic and two exocyclic D-arginines plus a trans amino-L-proline bearing a 2‑naphthylmethylene group in a type II β‑turn, which markedly enhances cell penetration and may support delivery of macromolecules, potentially even across the blood–brain barrier (Figure 2a).62
 |
Figure 2 Chemical structures of cyclic peptide (a), PEGylated peptide (b), β-Peptides (c and d). |
PEGylation, Acetylation, and Amidation
Terminal modifications are key for enhancing peptide pharmacokinetics and pharmacodynamics. PEGylation, the attachment of polyethylene glycol chains to the peptide, is a proven method for extending peptide half-life within the bloodstream, improving solubility, and decreasing immunogenicity.63,64 This alteration efficiently protects the peptide from enzymatic proteolytic digestion. This enhances a more desirable PK profile, which is beneficial for drugs entering the CNS, where therapeutic efficacy requires sustained drug concentrations over time. For example, Leuprolide, a GnRH agonist for advanced prostate cancer, with a short plasma half-life was optimized through the synthesis of two N‑terminally PEGylated leuprolide analogs with different PEG sizes via NHS chemistry, yielding highly pure 1:1 conjugates selectively modified on the histidine imidazole and stable at physiological pH. These PEGylated peptides retained in vitro suppression of androgen- and EGF-driven proliferation and reproduced the in vivo pharmacodynamic profile of native leuprolide, while exhibiting prolonged half-life, increased AUC, and reduced clearance after both I.V. and S.C. administration (Figure 2b).65 Acetylation and amidation of the termini of a peptide can also help stabilize and resist enzymatic breakdown. These structural changes enhance the peptide’s metabolic half-life and potency to traverse the BBB, which is the most important condition for CNS delivery therapies.66,67 These terminal alterations fine-tune the drug-like pharmacology of the peptide, thereby enabling more efficient and persistent therapeutic effects.
Non-Natural Amino Acids: D-Amino Acids, β-Peptides, and Methylation
Incorporating non-natural amino acids is an advanced strategy for enhancing the structural stability and biological activity of peptide-based drugs. D-amino acids, the mirror image of L-amino acids typically found in peptides, can improve resistance to enzymatic degradation without compromising the biological activity of the peptide. This modification is particularly useful in stabilizing peptides against proteases, thereby increasing their bioavailability and potency. β-peptides, which are composed of β-amino acids instead of α-amino acids, offer further stability improvements by providing a more rigid, nonproteinogenic backbone.68 This rigidity reduces the peptide’s conformational flexibility, enhancing its resistance to proteolysis and improving its interaction with biological targets. Additionally, methylation of peptide side chains or backbones can fine-tune the peptide’s binding affinity and stability, offering increased selectivity for its target, while further protecting against metabolic breakdown. These modifications enhance the therapeutic potential of the peptide, particularly for challenging targets in the CNS.69
These foundational concepts were effectively utilized in the groundbreaking research conducted by DeGrado et al, who investigated peptides comprising the β3-hVal/hLeu-β3-hLys-β3-hLeu motif (Figure 2c).70 Initial antibacterial β-peptide design used the β3-hVal/hLeu–β3-hLys–β3-hLeu motif and showed micromolar antibacterial activity but also comparable hemolysis. Refining the sequence to less lipophilic β3-hAla–β3-hLys–β3-hLeu repeats improved specificity by reducing hemolytic activity. In contrast, related β3-hAla–β3-hLys–β3-hPhe peptides displayed only moderate antibacterial effects combined with high hemolytic activity, indicating an unfavorable selectivity profile. Subsequent work expanded β‑antimicrobial peptide libraries with diverse β‑amino acid building blocks, confirming that activity and selectivity depend on a fine balance of lipophilicity, charge distribution, and conformational flexibility. Overall, positive charge proved critical: introducing a negatively charged C‑terminal carboxylate markedly reduced antimicrobial potency relative to the corresponding C‑terminal amide analogs (Figure 2d).71
Experimental & Synthesis Platforms
Fast-Flow Synthesis: Inline Monitoring with UV–Vis
Peptide-based therapeutics for neurodegenerative diseases, particularly AD, require precise, reproducible, and scalable synthetic methods to ensure batch-to-batch consistency, bioactivity, and manufacturability.72,73 Traditional SPPS have revolutionized the development of peptide drugs. However, inherent limitations such as long cycle times, inefficient reagent usage, and poor scalability have driven the adoption of flow-based synthesis technologies.
Fast-flow synthesis has emerged as a transformative platform for rapid, efficient, and automated peptide preparation. Unlike batch synthesis, fast-flow techniques enable continuous reagent delivery through packed resin beds under controlled conditions, dramatically accelerating reaction kinetics. The key advantages of fast-flow peptide synthesis include shortened reaction times, improved coupling efficiency, reduced side reactions, and potential to integrate real-time quality control strategies.72,74
A critical advancement within fast-flow platforms is the implementation of inline monitoring using ultraviolet–visible (UV–vis) spectroscopy. This technique allows real-time monitoring of the deprotection and coupling steps by detecting changes in chromophores associated with Fmoc groups or other UV-active species released during synthesis.74–76 Inline UV–vis detection offers several advantages.
- Immediate feedback on reaction completion, facilitating dynamic adjustment of reaction parameters if necessary.
- Reduction of synthesis failures by enabling the early detection of incomplete reactions or resin fouling.
- Data-rich synthesis runs provide quantitative metrics such as coupling yields and deprotection efficiencies for each step.
- Decision-making automation allows real-time optimization through feedback control loops.
Despite these advantages, fast‑flow peptide synthesis also has important limitations. The initial capital cost and technical expertise required to implement high‑pressure flow systems remain barriers for many academic and early‑stage industrial laboratories. Very long or aggregation‑prone sequences can still suffer from incomplete couplings, aspartimide formation, or on‑resin aggregation even under flow, necessitating extensive optimization of temperature, solvent composition, and residence time. Moreover, the accelerated cycle times increase the importance of inline and offline analytics to ensure that truncated or modified by‑products are detected and controlled; comprehensive impurity profiling and scale‑up under GMP conditions are still less mature than for classical batch SPPS. As a result, fast‑flow platforms are currently best suited to rapid lead optimization and library generation, with final process development often transitioning to more established production formats.77,78
For instance, Pentelute et al developed an automated fast-flow peptide synthesizer that integrates inline UV–vis detectors to monitor Fmoc deprotection kinetics at 310 nm, achieving synthesis times of less than one hour for complex peptides such as a 40-mer β-amyloid peptide implicated in AD pathogenesis.79 By recording UV–vis traces during synthesis, aberrant steps can be rapidly identified and corrected, ensuring high fidelity and reducing synthesis artifacts that compromise therapeutic efficacy. Fast-flow synthesis with inline UV–vis monitoring is highly compatible with the stringent quality control requirements necessary for good manufacturing practices (GMP) and is intended for clinical-grade peptide drugs used in neurodegenerative disease applications.79
In the context of AD research, where therapeutic peptides such as β-sheet breakers, Aβ aggregation inhibitors, and tau-targeting peptides demand high structural purity and conformational integrity, fast-flow synthesis with inline UV–vis monitoring represents a crucial technological advance. This ensures that lead candidates can be produced swiftly, reproducibly, and at scales suitable for pre-clinical and clinical evaluations. Overall, the synergy between fast-flow synthesis platforms and real-time UV–vis monitoring paves the way for the next generation of peptide therapeutics for AD, promising enhanced control over molecular quality, accelerated development timelines, and better translation from bench to bedside.80
Drug Repurposing and Clinical Translation
In the context of AD, peptide drug repurposing offers several advantages, including high target specificity, favorable safety profiles, and potential for multimodal actions affecting neuroinflammation, oxidative stress, and synaptic plasticity (Table 1).81
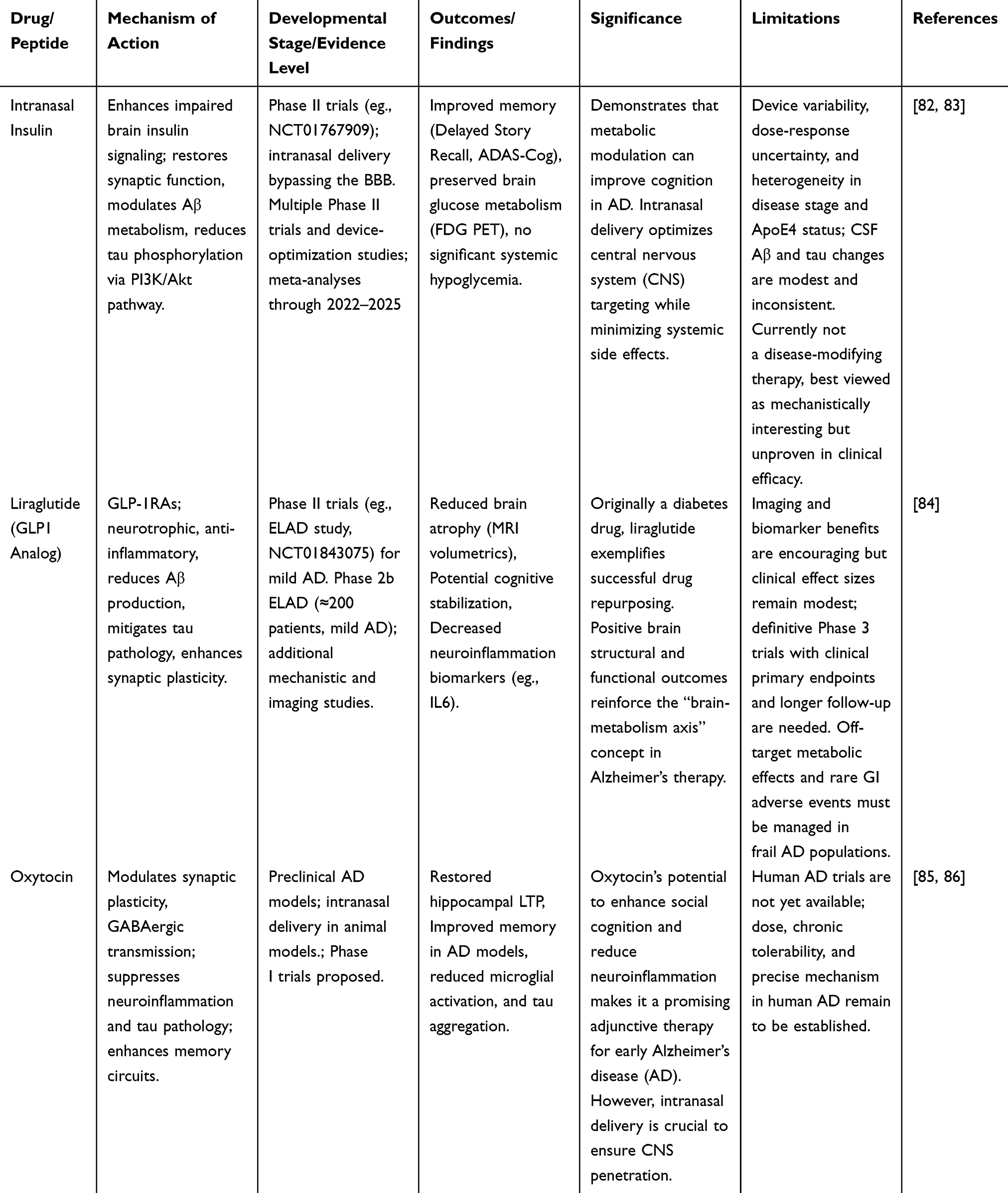 |
Table 1 Clinical Profiles and Mechanistic Insights of Repurposed Peptide Therapeutics in Alzheimer’s Disease |
One of the earliest examples was intranasal insulin. Disruption of insulin signaling has been implicated in AD pathogenesis, with the brain exhibiting features akin to those of insulin resistance. Intranasal delivery bypasses the BBB and ensures direct transport to the CNS via olfactory and trigeminal pathways, minimizing peripheral side effects, such as hypoglycemia.82,83 Randomized phase II studies of intranasal insulin in participants with mild cognitive impairment or early Alzheimer’s disease (sample sizes typically 60–300) have reported improvements in memory composites (eg., Delayed Story Recall, ADAS‑Cog) and preservation of regional brain glucose metabolism on FDG‑PET over 4–12 months, without significant systemic hypoglycemia. These data suggest target engagement and potential symptomatic benefit but are not yet sufficient to establish durable disease modification.82,83
Similarly, glucagon-like peptide-1 (GLP-1) receptor agonists such as liraglutide and exenatide, initially developed for type 2 diabetes mellitus, have been repurposed for AD owing to their neurotrophic and anti-inflammatory properties. Preclinical studies have consistently reported that GLP-1 analogs reduce amyloid plaque burden, diminish tau hyperphosphorylation, attenuate microglial activation, and enhance synaptic plasticity. In transgenic AD mouse models, GLP‑1 receptor agonists (GLP-1RAs) such as liraglutide improve memory performance and normalize long‑term potentiation, supporting a neurotrophic and anti‑inflammatory mechanism. In humans, the Phase 2b ELAD trial (NCT01843075) enrolled patients with mild AD and evaluated liraglutide versus placebo over 12 months; interim analyses have reported preserved brain volume and a numerically smaller decline on cognitive scales, but the magnitude and durability of clinical benefit remain uncertain and require confirmation in larger, longer‑term trials.84
In addition to metabolic peptides, oxytocin, implicated in social cognition, is gaining attention for its therapeutic potential in AD. Recent work has demonstrated that intranasal oxytocin restores hippocampal synaptic plasticity and memory deficits in an AD mouse model, primarily by suppressing tau pathology and neuroinflammation.85,86 Mechanistically, oxytocin modulates GABAergic transmission and neuroimmune responses, suggesting a novel neuromodulator approach distinct from Aβ- or tau-targeted therapies. Collectively, these examples highlight the repositioning of approved peptide drugs as innovative strategies to address the multifactorial pathogenesis of AD and potentially alter its natural course.85,86
Practical Design Checklist for CNS Peptide Candidates
A practical design checklist to aid early-stage programs in defining minimal data packages before strong claims of “CNS readiness” would involve:
– Biological target and mechanism: Define the primary target (eg., Aβ, tau, neuroinflammatory pathway) and whether the peptide acts as an inhibitor, agonist, or decoy.
– Intended route of administration: Select route (intravenous, subcutaneous, intranasal, oral) consistent with chronic use in older adults and with the peptide’s stability profile.
– Stabilization strategy: Plan backbone and side‑chain modifications (cyclization, D‑amino acids, N‑terminal capping, PEGylation, or β‑residues) required to achieve a therapeutically relevant half‑life and protease resistance in plasma and CSF.
– Brain‑exposure strategy: Match peptide size, polarity, and charge to an appropriate BBB approach (eg., lipidation or small cyclic scaffolds for passive diffusion, receptor‑mediated transcytosis tags, CPP motifs, nanoparticle or exosome encapsulation, or intranasal delivery).
– Safety and immunogenicity: Have sequence and modifications been screened in silico for immunogenic epitopes and off-target liabilities.
– Early experimental package: At minimum, establish (i) in vitro target engagement and mechanism, (ii) serum and CSF stability and basic DMPK, (iii) in vitro BBB permeability or endothelial transport assays, (iv) in vivo PK with brain:plasma ratios, and (v) proof‑of‑concept efficacy on cognitive or pathological readouts in at least one AD‑relevant model before making strong claims about clinical potential.
Computational and AI Design in Peptide Therapeutics
Computational and AI Approaches to Improve Peptide Therapeutics
The emergence of AI and computational design technologies has opened a revolutionary age for peptide therapeutics. Previously, the evolution of bioactive peptides relied on empirical screening and medicinal chemistry processes, which are labor-intensive, time-consuming, and have limitations.87
Computational methods have become pivotal for accelerating peptide discovery for AD therapeutics. These approaches integrate bioinformatics, molecular modeling, and machine learning to predict peptide structure, binding affinity, and biological activity. The current workflow follows a “funnel” approach, starting with high-throughput virtual screening (VS) and culminating in computationally intensive molecular dynamics (MD) simulations.88 Molecular docking and dynamics simulations enable the exploration of peptide interactions with Aβ aggregates and tau proteins, which are key pathological hallmarks of AD.89 Molecular docking provides detailed insights into binding conformations and affinities, allowing researchers to identify key interaction sites and predict the strength and specificity of peptide-target binding. Critically, for flexible targets such as Aβ oligomers, which are intrinsically disordered proteins, recent protocols employ “flexible-flexible” docking to account for backbone conformational movements in both the ligand and the receptor.89,90 Docking is often used in an ML-docking cascade to confirm that computationally predicted peptide hits can physically fit and interact strongly with the enzyme active site.91 MD simulations complement docking by offering dynamic perspectives on peptide-target stability and conformational changes over time, which are essential for understanding the mechanistic basis of peptide efficacy and potential off-target effects. MD is instrumental in elucidating the mechanisms of aggregation inhibition, such as stabilizing Aβ in an unfolded state or blocking aggregation-prone regions through specific interactions such as π-π stacking.92 Binding stability was rigorously assessed by calculating the binding free energy (ΔG bind) using methods, such as MM/GBSA.93,94 Furthermore, Quantum Biochemistry methods, coupled with MD, offer detailed molecular insights, confirming, for example, that three Complementarity Determining Regions contributed approximately 77% of Aducanumab’s total affinity to the Aβ(2–7) epitope.95
Docking and MD‑based workflows should be interpreted as hypothesis‑generating tools rather than definitive predictors of efficacy. In practice, we consider docking results more credible when the protocol can (i) accurately re‑dock co‑crystallized ligands within a low RMSD, (ii) reproduce key interactions observed experimentally, (iii) distinguish active from inactive analogues in retrospective benchmarking, and (iv) yield consistent binding poses across different starting conformations or docking programs. MD simulations add confidence when independent replicas converge to similar interfacial contact patterns and when peptide-target complexes remain stable over tens to hundreds of nanoseconds. Free‑energy estimates from MM(GB/PB)SA are useful for ranking closely related analogues but should not be treated as absolute binding energies; they neglect important entropic and solvent contributions and are highly protocol‑dependent. Recent docking‑driven analyses of peptide-protein interactions exemplify how such methods can guide interaction mapping and sequence optimization while explicitly acknowledging these limitations.96 Reported peptide–target interaction studies commonly cite MM/GBSA-derived binding energies in the range of −20 to −60 kcal/mol for high-affinity interactions, but inter-laboratory variability is substantial and absolute values depend strongly on force field, solvent model, and trajectory length. As a practical guideline:
• Energies within ≈5–10 kcal/mol of each other should generally be treated as comparable without overinterpreting rank order.
• Stability over MD trajectories (eg., persistent hydrogen bonds, stable contact networks, and low RMSD fluctuations) is often more informative than a single aggregate ΔG value.
Validation should, whenever possible, link computed rankings to experimental measures such as IC50 or Kd value. This principle is well illustrated in docking‑driven optimization of isosteviol-based FXa inhibitors, where docking scores and MM/GBSA energies were used to prioritize analogs that subsequently validated in biochemical assays,96 serving as a methodological benchmark for peptide and peptidomimetic projects.
Quantitative structure–activity relationship (QSAR) modeling is increasingly applied to peptide datasets to prioritize sequences based on predicted potency, selectivity, or BBB permeability. However, robust performance requires careful control of information leakage, appropriate training/validation splits, and clear applicability domains. A recent structured QSAR pipeline for 2‑aminothiazol-4(5H)-one derivatives as 11β‑HSD1 inhibitors illustrates several best practices: (i) internal validation with cross-validation; (ii) external test sets that are structurally distinct from training compounds; (iii) mechanistically interpretable descriptors; and (iv) explicit definition of chemical space boundaries beyond which predictions should be treated as exploratory rather than confirmatory. For peptide‑focused QSAR and ML models, stringent validation is essential to avoid over‑fitting and misleading performance estimates. Recent QSAR workflows in neuroactive peptide and small‑molecule design illustrate how such structured pipelines, combined with interpretable feature analysis, can provide robust guidance for medicinal chemistry optimization.97
ML algorithms analyze large datasets, including peptide sequences, physicochemical properties, and biological assay results, to identify peptide candidates with optimal characteristics such as BBB permeability, metabolic stability, and target specificity.98 These algorithms employ diverse techniques, including support vector machines, random forests, and deep neural networks, to capture complex relationships between sequence features and functional outcomes. By leveraging sequence-based features, structural motifs, and physicochemical parameters, ML models enable the rapid screening and prioritization of vast peptide libraries, dramatically reducing the time and cost associated with traditional experimental screening. ML algorithms are adept at learning cross-domain features to overcome the challenges of sparse peptide data, leading to the discovery of novel actives.14,99,100
AI-driven de novo peptide design platforms generate novel peptide candidates by learning from existing peptide libraries and structural databases.101 These generative models, such as variational autoencoders and generative adversarial networks, facilitate the creation of peptide sequences with tailored properties by simultaneously optimizing multiple parameters, including the binding affinity, solubility, and PK profiles.13 The integration of multi-omics datasets, including genomics, proteomics, transcriptomics, and metabolomics, with AI models further refines target identification and peptide optimization, enabling a systems biology approach to AD therapeutics. This holistic strategy allows the identification of novel peptide targets linked to disease pathways, thereby improving the likelihood of therapeutic success.102
Generative AI techniques (eg., GANs, VAEs, Reinforcement Learning) are essential for de novo peptide design, enabling the simultaneous creation of entirely new sequences optimized for multiple characteristics.103 These algorithms can design peptides to “tile” the surface of amyloid fibrils, acting as molecular caps to halt elongation.104 DL models such as DeepB3P have been specifically developed to predict and generate BBB-penetrating peptides with high accuracy.105
Generative models such as VAEs and GANs have shown strong performance in producing diverse, high‑affinity peptides for antimicrobial and hormone‑like targets, but most applications in AD remain preclinical, with only a few examples progressing to animal efficacy studies. In contrast, specialized models such as DeepB3P are explicitly trained to identify BBB‑penetrant sequences and therefore directly address CNS exposure; however, their outputs still require extensive experimental validation, and no DeepB3P‑derived peptide has yet reached advanced clinical testing.105 At present, the most mature AI‑enabled pipelines for AD combine conventional docking/MD and QSAR with structure prediction, while purely generative and BBB‑specific models should be viewed as powerful hypothesis generators that must be integrated carefully into experimental workflows.
AlphaFold and related structure‑prediction tools are the most mature in terms of broad adoption and benchmarking; they are particularly useful for L‑peptide and protein scaffolds involved in Aβ and tau binding, but they are less reliable for disordered segments and D‑rich or cyclic peptides. However, a key limitation persists while AlphaFold and AlphaFold 3 have been transformative for protein structure prediction, AlphaFold 3 performs poorly in predicting the structure of D-amino acid peptides, a critical therapeutic class, owing to its high chiral violation rate (~51%).106,107
The poor performance of current structure‑prediction tools for D‑amino‑acid and retro‑inverso peptides has practical consequences for design workflows: in many cases, reliable 3D models are not available a priori, which constrains purely structure‑based optimization. In practice, designers often start from experimentally supported L‑peptide structures, then generate retro‑inverso or D‑rich analogues and refine them by targeted MD simulations or energy minimization, treating the predicted conformations as qualitative hypotheses rather than ground truth. Where possible, low‑resolution experimental data (eg., CD spectra, NMR distance restraints) or coarse‑grained models are used to validate and calibrate these in silico structures before committing to large design cycles. From a translational perspective, limited reliability of structure prediction for D‑peptides and β‑peptides means that medicinal chemists cannot yet rely on a “design‑once, model‑driven” workflow. Instead, D‑enrichment is typically introduced after initial L‑peptide leads have been validated, with iterative cycles of synthesis, biophysical characterization, and MD‑supported conformational analysis to ensure that stability gains do not compromise target engagement.55,108,109
Moreover, computational approaches have increasingly incorporated predictive toxicology and immunogenicity assessments to evaluate peptide safety profiles early in the development process and mitigate downstream risks. In silico toxicity prediction models assess potential off-target interactions, immunogenic epitopes, and adverse pharmacodynamic effects, thereby guiding the selection of safer candidates. The synergy of these computational strategies reduces the experimental burden by prioritizing candidates with the highest likelihood of efficacy and safety, thereby streamlining the drug development pipeline and shortening the timelines from discovery to clinical evaluation. The continuous evolution of computational power and algorithmic sophistication promises further enhancements in peptide design accuracy and predictive capabilities, enabling a more reliable translation from in silico predictions to in vivo efficacy. A summary of AI driven platforms and computational workflows is presented in Table 2.
 |
Table 2 Selected AI/ML Platforms Relevant to Peptide Therapeutics in AD |
Examples of Successful AI/Computational Guided Peptide Discovery
Several studies have demonstrated the success of AI and computational tools in identifying peptides that modulate AD pathology.
AI algorithms have designed peptides that inhibit Aβ aggregation by targeting specific amyloidogenic regions, effectively reducing plaque formation in in vitro and in vivo models.114,115 These peptides act by binding to aggregation-prone sequences within Aβ, thereby preventing the nucleation and elongation phases of fibril formation that are critical for plaque development. Prosome Therapeutics® exemplifies this approach by leveraging proprietary AI to develop decoy peptides that neutralize Aβ peptides and protect neurotransmission. Their platform utilizes deep learning to predict peptide-Aβ interactions and optimize sequences for enhanced stability, brain penetration, and therapeutic efficacy. DL models led to the identification of AI-Pep-1, which potently inhibits Aβ oligomerization and protects neurons in vitro. Structure-based design algorithms have been used to create mini-protein inhibitors (35–48 residues) designed to bind and cap the tips of Aβ and tau fibrils, successfully blocking toxicity in C. elegans models.116 VS techniques identified small peptides (tri- and hexapeptides such as WWW and CILFWG) capable of destroying Aβ fibrils, emphasizing the role of tryptophan and proline residues.92,117
Beyond Aβ targeting, DL models have been employed to optimize peptide sequences for enhanced binding to the tau protein, another key pathological hallmark of AD, resulting in peptides that prevent tau aggregation and neurofibrillary tangle formation.116,118 These tau-targeting peptides are designed to interfere with the pathological phosphorylation and aggregation processes, thereby mitigating tau-mediated neurotoxicity. Structure-based design led to the cyclic peptide cTau-binder, optimized to sterically hinder the lateral association of tau protofilaments, reducing aggregation and improving cognition in transgenic mice.119 A significant computational success is the retro-inverso peptide RI-AG03, designed to “dual-cap” the two key tau aggregation hotspots (306VQIVYK311 and 275VQIINK280), showing high potency and extended survival in Drosophila tauopathy models. Computational mutagenesis also identified the bovine milk peptide p136 as a binder for the tau PHF core, which was predicted to disrupt further aggregation.120 Computational screening has also identified multifunctional peptides with antioxidant and anti-inflammatory properties that simultaneously address multiple AD pathological pathways.121 Such multifunctional peptides demonstrate the ability to scavenge reactive oxygen species, inhibit pro-inflammatory cytokine release, and modulate microglial activation, offering a holistic therapeutic approach.122 A hybrid ML–molecular docking cascade successfully discovered six novel anti-acetylcholinesterase (AChE) hexapeptides, with the most potent achieving an IC50 in the low nanomolar range.91 ML models have also guided the discovery of peptides that inhibit RAGE receptor with anti-inflammatory effects.123 The ApoE-mimetic peptide CS-6253 was rationally designed to promote cholesterol efflux by stabilizing the ABCA1 transporter, successfully reducing Aβ pathology, and improving memory in AD model mice.124
Furthermore, AI-guided discovery has enabled the identification of peptides with enhanced PK properties such as improved BBB permeability and resistance to proteolytic degradation, which are critical for effective CNS delivery. Computational modeling has enabled the design of Brazilian Copper-Chelating Peptides capable of crossing the BBB to reverse memory deficits by addressing metal dyshomeostasis.125
These advances have facilitated the development of peptides with an optimized balance between efficacy and safety profiles, thereby accelerating their progression toward clinical evaluation. Collectively, these successes underscore the transformative potential of AI-guided peptide discovery in AD drug development, enabling the design of highly specific multifunctional therapeutic agents with optimized pharmacological profiles and reduced development timelines.
Case Studies of Recent Research and Clinical Trials of Peptides in AD
This section will report on individual cases with measurable outcomes in AD therapeutics at both preclinical and clinical stages, with a dedicated subsection focusing on recent research in peptide therapeutics for AD.
Overview of Recent Research in AD Therapeutics
Recent research on AD therapeutics reflects a diverse array of strategies focusing on metabolic regulation, Aβ targeting, neurovascular unit (NVU) integrity, and novel drug delivery systems, each with promising findings and notable limitations. Studies have emphasized the therapeutic potential of GLP-1RAs and DPP-IV inhibitors, which enhance glucose metabolism and reduce neuroinflammation, demonstrating preclinical success in AD and PD models.126 However, challenges remain in improving BBB penetration and expanding the clinical trials to confirm its efficacy in humans. Similarly, a triad of antidiabetic agents was explored to improve insulin sensitivity and lower Aβ accumulation, showing neuroprotective effects in AD models, but underscoring the need for clinical validation.127 Another study reviewed Aβ-targeting therapies, including monoclonal antibodies such as aducanumab and donanemab, which have shown the capacity to reduce amyloid plaques with potential benefits from combination therapies.127 However, their long-term clinical efficacy and impact on disease progression remain unclear. A review combining metformin, GLP-1RAs, and herbal compounds to improve glucose and mitochondrial function reported enhanced cognition and Aβ reduction in preclinical studies, although robust clinical trials are still needed. In parallel, NVU-targeting approaches focus on maintaining BBB integrity, a crucial factor in AD pathogenesis, but these strategies are still largely confined to basic research.128 Diagnostic advancements and monoclonal antibody therapies targeting Aβ biomarkers hold promise for early detection and intervention, although studies on their efficacy and long-term outcomes continue.129 Innovations in peptide-loaded delivery systems, Poly(lactide-co-glycolide) (PLGA) nanocarriers, show improved bioavailability and controlled release, which make them effective for neurological and regenerative applications; however, challenges in scalability, cost, and regulatory approval limit their broader application.130 Peptidomimetics of tropomyosin receptor kinase (Trk) ligands demonstrate preclinical benefits in promoting neuronal survival and plasticity in AD and PD; however, optimizing BBB delivery remains a significant hurdle.131 System-level GLP-1 receptor therapies modulate insulin signaling and neuronal pathways, presenting a multi-targeted neurotherapeutic approach still under mechanistic investigation.132 Focused studies on metformin revealed modulation of Aβ, mitochondrial function, and neuroinflammation with cognitive benefits in models, but human trials are required.133 Indole-based drugs are promising scaffolds for neurodegenerative therapy through diverse pathway targeting, although translational hurdles persist.134 Finally, mitochondrial-targeting drugs aim to reverse AD-associated energy deficits by enhancing mitochondrial function, underscoring the need for clinical validation to confirm their therapeutic potential.135 These studies illustrate a multifaceted and evolving landscape in AD research (Table 3).
 |
Table 3 Comparative Analysis of Different Treatment Research Approaches of Alzheimer’s Disease |
Discussion of Ongoing Clinical Trials and Their Outcomes
The clinical landscape reflects diversification, with approximately 164–182 active AD clinical trials as of 2025.136,137 Several peptide-based therapeutics for AD are currently under clinical evaluation, reflecting the translational progress of the preclinical findings. Clinical trials have included peptides designed to inhibit Aβ aggregation, promote amyloid clearance, or modulate neuroinflammatory responses.138 Early phase trials have reported favorable safety profiles and biomarker improvements, such as reduction in cerebrospinal fluid Aβ levels and modulation of inflammatory markers, indicating target engagement and biological activity. The peptide vaccine ALZ-101 (NCT05184335), designed computationally to target soluble Aβ oligomers, showed a favorable safety profile and dose-dependent reduction in CSF oligomer levels during Phase II interim analysis.139 ND-001 (NCT05267535), an APOE receptor-binding domain mimic, was well tolerated and achieved therapeutic CNS concentrations, showing a trend toward reduced phospho-tau levels in the CSF during Phase I/IIa.140 The most advanced peptide candidate is the repurposed metabolic GLP1-RA. Liraglutide (Phase 2b ELAD) demonstrated a statistically significant 18% reduction in cognitive decline and preserved brain volume in patients with mild AD.84 For GLP‑1 receptor agonists, it is important to distinguish biomarker and imaging signals from clinically meaningful outcomes. Most AD‑focused trials to date have been modest in size and duration and have primarily demonstrated changes in neuroimaging measures (eg., regional brain atrophy) and metabolic or inflammatory biomarkers, whereas effects on global cognitive and functional endpoints have been small or inconsistent. Consequently, GLP‑1RAs should currently be considered promising metabolic and neurotrophic modulators under evaluation rather than established disease‑modifying therapies in AD.141 Cerebrolysin, a peptide mixture with neurotrophic properties, is in phase 3/4 trials and is effective in improving global clinical function scores.142
However, efficacy outcomes in cognitive endpoints have been variable, with some phase II/III trials demonstrating limited or no significant cognitive benefits despite biochemical improvements. The octapeptide NAP (davunetide) failed to meet the primary endpoints in a Phase III trial, despite earlier preclinical promise.143 The Phase III trial for the tau-targeting peptide Pept-AD-03 was halted for futility owing to a lack of clinical slowing. This translational gap highlights the complexity of AD pathophysiology and the challenges in achieving clinical efficacy. Factors influencing trial outcomes include peptide stability in vivo, efficient CNS delivery, and patient heterogeneity, encompassing disease stage, genetic background, and comorbidities.144
The mixed track record of peptide‑based AD candidates in clinical trials reflects several recurring issues. First, many programs advanced into phase II or III with limited quantitative evidence of sustained brain exposure or target engagement in humans; peptides that were potent in vitro or in animal models often failed to achieve sufficient free concentrations in the human CNS. Second, strong effects on surrogate biomarkers or pathology (eg., plaque or tangle load) have not always translated into meaningful improvements on cognitive or functional scales, underscoring an incomplete understanding of the timing and causal relevance of these targets. Third, trial designs have sometimes been underpowered or inadequately enriched for patients most likely to benefit (eg., by pathology status, stage, or genetic background), diluting potential signals. Finally, long‑term safety, particularly immunogenicity and off‑target effects in frail, multimorbid populations, remains a critical challenge for chronic peptide therapy. Recognizing and addressing these failure modes is essential for the next generation of CNS‑directed peptides.145
To address these challenges, peptide engineering efforts have focused on enhancing stability through chemical modifications and advanced drug delivery technologies, aim to improve the bioavailability in the CNS.146 Adaptive clinical trial designs incorporating biomarker-driven patient stratification and AI-assisted data analysis are increasingly being employed to improve the detection of therapeutic effects and optimize dosing regimens.147
Ongoing clinical efforts underscore the translational potential of peptide therapeutics in AD while emphasizing the need for continued innovation in peptide design, delivery, and trial methodology to overcome current limitations and achieve meaningful clinical outcomes.
Future Directions and Challenges
Opportunities for Further Research and Development in Peptide-Based Treatments
BBB penetration remains the “greatest challenge” for peptide therapeutics. Future research should prioritize enhancing peptide stability, specificity, and brain penetration to maximize the therapeutic efficacy.121 Implementing advanced chemical modifications to enhance proteolytic stability and half-life is crucial.148–150 Advances in delivery systems, including exosomes, liposomes, polymeric nanoparticles, and other nanocarriers, can improve peptide bioavailability, enhance brain targeting, and minimize off-target effects.151 These platforms enable controlled release and protection from enzymatic degradation, which are critical for effective CNS delivery. Developing “Trojan horse” strategies, such as Receptor-Mediated Transcytosis using functionalized nanoparticles. Nanocarriers protect peptide payloads from enzymatic degradation and significantly increase brain uptake.152 Intranasal administration offers a noninvasive direct route to the CNS.153
The synergistic integration of simulations, ML, and experimental validation offers “integrated design platforms” for end-to-end computational prediction of novel sequences, activities, stability, and ADMET profiles.111,149 Integrating multi-omics data with AI platforms can also facilitate the identification of novel peptide targets and optimize sequence design tailored to individual pathological profiles, thus enabling precision therapeutics.102 The development of multifunctional peptides capable of simultaneously targeting the Aβ, tau, and neuroinflammation pathways offers a promising strategy to address the multifactorial nature of AD pathology.154 Such peptides may combine aggregation inhibition with anti-inflammatory and neuroprotective activities within a single molecule.
Developing agents that modulate multiple pathways (polypharmacology) is essential, given AD’s complexity of AD.155 Novel targets constitute 70% of current pipelines.156 Peptides are ideal candidates for this purpose, capable of combining functions such as Aβ aggregation inhibition, metal chelation, and neuroinflammatory modulation.157 Research should target non-canonical mechanisms, including neuroimmune modulation, mitochondrial function158 and the gut-brain axis.159
Collaborative efforts combining computational modeling, experimental validation, and clinical expertise are essential to overcome the current limitations and accelerate peptide drug development.
To synthesize these translational issues, Table 4 summarizes major bottlenecks for peptide-based AD therapeutics across manufacturing, stability, immunogenicity, CNS exposure, and regulatory/reimbursement domains, together with representative mitigation strategies and a qualitative assessment of their current priority in the development pipeline.
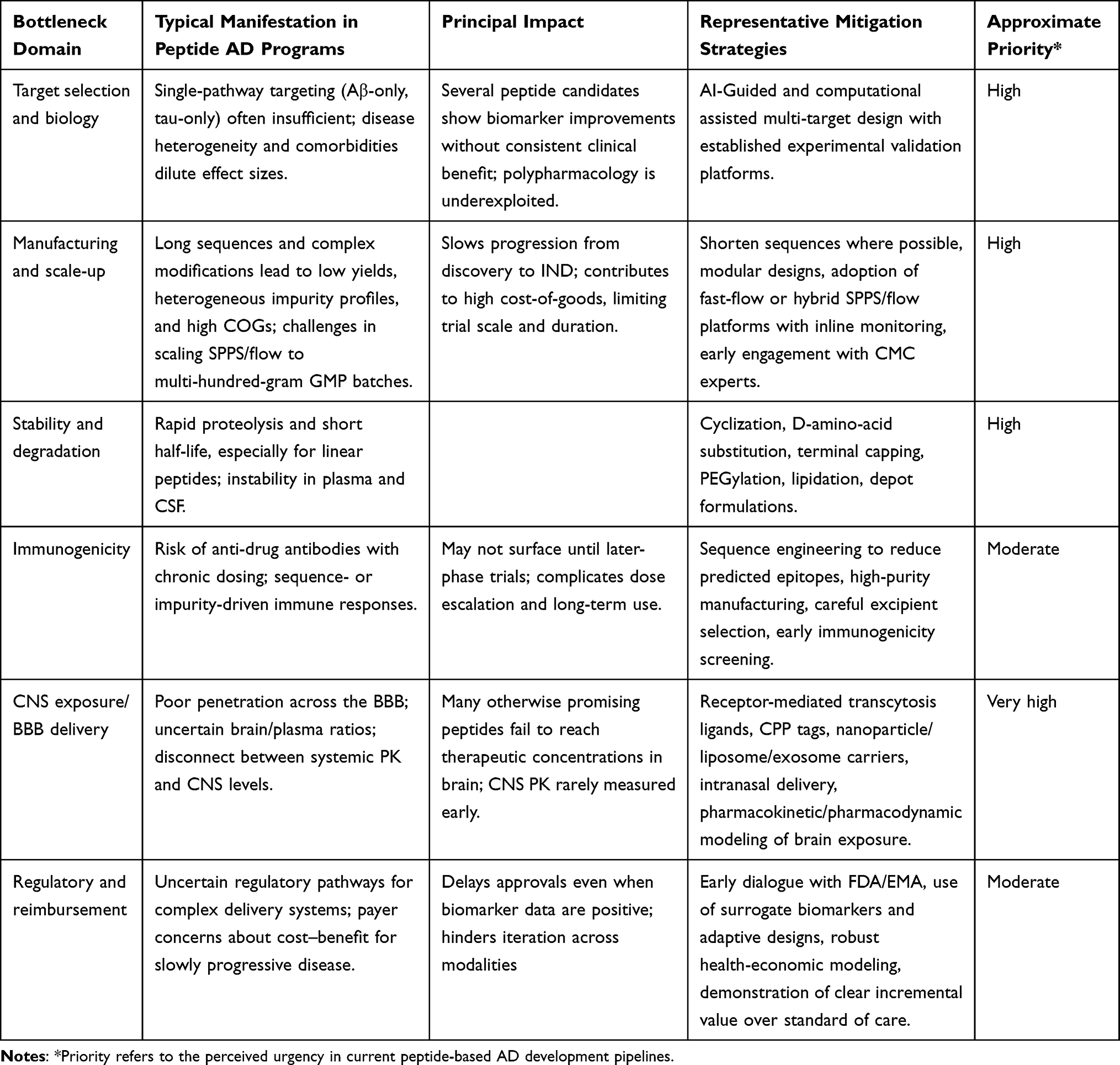 |
Table 4 Major Translational Bottlenecks for Peptide-Based Therapeutics in Alzheimer’s Disease and Potential Mitigation Strategies |
Ethical Considerations and Regulatory Challenges in Peptide Drug Development
The accelerated pace of AI-driven peptide discovery introduces novel ethical and regulatory complexities.111 Peptide-based therapeutics for AD have significant ethical and regulatory considerations, including patient safety, informed consent, and equitable access. A primary concern is the risk of algorithmic bias.160 If AI models are trained on non-representative datasets, the resulting peptides may show differential efficacy or safety in underrepresented genetic ancestries, exacerbating health disparities.161 The complexity of AI-guided design necessitates transparency in algorithmic decision-making to ensure reproducibility, accountability, and avoidance of bias, addressing concerns about the “black-box” nature of AI models. Regulatory agencies require rigorous validation of peptide efficacy, safety, and manufacturing consistency, which can be challenging given the novelty of AI-derived candidates and the inherent complexity of peptide synthesis and characterization.162
The U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA) have established robust pathways yet unique challenges concerning peptide-based molecules. For peptides intended to treat AD, the regulatory journey typically commences with an Investigational New Drug (IND) application in the U.S. or scientific advice procedures in Europe. Subsequently, Phase I trials have focused on systemic safety and CNS penetration, pharmacodynamics at neural targets, and early biomarker changes (eg., cerebrospinal fluid Aβ42, total tau, phosphorylated tau). Phase II and III trials must demonstrate statistically significant improvements in validated cognitive and functional endpoints, such as the AD Assessment Scale-Cognitive Subscale (ADAS-Cog), Clinical Dementia Rating Sum of Boxes (CDR-SB), and global scales such as the AD Cooperative Study–Activities of Daily Living (ADCS-ADL).82,83,163,164 Importantly, regulatory agencies have increasingly recognized surrogate biomarkers as acceptable endpoints for accelerated approval. For instance, the FDA’s accelerated approval of aducanumab was based on amyloid plaque reduction rather than clinical benefits. This evolving landscape may facilitate earlier access to peptide therapeutics, resulting in compelling biomarker modulation. Nevertheless, peptides face regulatory hurdles unique to their biophysical nature, including susceptibility to enzymatic degradation, immunogenicity risk, and limitations in CNS bioavailability, necessitating rigorous formulation innovations to meet regulatory expectations of durability, consistency, and CNS exposure. Furthermore, before considering full marketing authorization, the FDA and EMA emphasize the need for extensive longitudinal safety data, particularly regarding immunogenicity (eg., anti-drug antibody formation) and off-target effects in sensitive CNS environments.
Compared with monoclonal antibodies, therapeutic peptides generally present a simpler regulatory and CMC profile: they are chemically synthesized, structurally well‑defined, and often fall under small‑molecule‑like quality frameworks, with less extensive requirements for glycosylation profiling, higher‑order structure characterization, and comparability after manufacturing changes. Immunogenicity risk is typically lower but still requires systematic assessment, particularly for highly modified or conjugated constructs. Nevertheless, for Alzheimer’s disease, the evidentiary bar for demonstrating cognitive and functional benefit is similar for peptides and antibodies; both must show robust, reproducible effects on validated clinical endpoints, even if surrogate biomarker responses can support accelerated approval in selected cases.165,166
The high cost associated with novel AD therapies raises concerns about equitable access and financial burden on healthcare systems.95 Intellectual property issues surrounding AI-generated sequences present legal complexities, including questions on ownership, patentability, and licensing.167 Ethical dilemmas also include psychological distress caused by disclosing sensitive diagnostic information (eg., amyloid status) to asymptomatic participants and the imperative to avoid overstating evidence for unvalidated treatments.168 Ethical frameworks must, therefore, address data privacy concerns in AI training datasets, especially when incorporating patient-derived information, to protect confidentiality and comply with data protection regulations such as GDPR and HIPAA.169
Proactive engagement with regulatory bodies and ethical oversight committees is critical to navigating these challenges, ensuring responsible clinical translation, and fostering public trust. Equitable access to peptide therapeutics should be considered to prevent disparities in treatment availability across different populations and healthcare systems. Transparent communication with patients and stakeholders regarding AI involvement in drug development is essential for maintaining ethical standards and societal acceptance.
Potential Impact of AI-Guided Design on the Future of Alzheimer’s Therapeutics
The integration of AI into peptide drug discovery is the most transformative force in AD therapeutics, offering pathways to address the complexity of the disease.170 AI-guided peptide design holds transformative potential for AD therapeutics by enabling the rapid, cost-effective discovery of highly specific and multifunctional peptides.114 AI-guided design promises to drastically reduce the time and cost of the discovery phase by compressing the “Design-Make-Test-Analyze” cycle.171 Generative biology models allow researchers to move beyond screening existing libraries to “hallucinating” entirely new chemical entities with atomic precision.172 This capability enables the design of peptides against historically “undruggable” targets (eg., flat interfaces of protein aggregates) by simultaneously optimizing their stability, permeability, and target specificity.103 AI can explore a chemical space approximately 10 times larger than that accessible via traditional methods. This approach can uncover novel molecular targets and optimize peptide properties beyond the capabilities of traditional methods, potentially leading to breakthroughs in disease modification and symptom management. AI enables the precise design of intricate Multi-Target Directed ligands or peptide cocktails that target different nodes in the AD network. AI is uniquely suited to perform multi-objective optimization, balancing potency across several targets.111 AI integration with high-throughput screening and patient data analytics may be useful in precision medicine paradigms tailored to individual disease profiles, improving therapeutic efficacy, while minimizing adverse effects. By integrating AI analysis of multi-omics and genetic data (eg., APOE genotype), it may be feasible to design peptides or peptide sets dynamically tailored to an individual patient’s specific disease subtype.173
Furthermore, AI can streamline clinical trial design by predicting responder populations, optimizing dosing regimens, and identifying potential safety concerns early in development, thereby increasing trial success rates and reducing costs. AI can profoundly enhance clinical trials by enabling patient stratification, identifying specific subgroups who benefit most from a drug (as demonstrated by the re-analysis of the “Amaranth” trial).104 This precision minimizes trial risks and accelerates the success rate of rationally designed compounds.
As AI-guided peptide therapeutics mature, they are poised to become a cornerstone in the next generation of AD treatment strategies, accelerating the translation from bench to bedside and ultimately improving patient outcomes and quality of life.101 The integration of AI with multidisciplinary research promises to reshape the landscape of neurodegenerative disease therapeutics, fostering innovation and precision in drug discovery.
Conclusions and Perspectives
Peptide-based therapeutics have emerged as promising candidates for Alzheimer’s disease (AD) because of their exceptional target specificity, favorable safety profiles, and ability to engage in protein–protein interactions that small molecules cannot readily access. In particular, peptides are being designed to address core AD pathologies, including the inhibition of amyloid β (Aβ) aggregation, disruption of tau hyperphosphorylation, and enhancement of neurotrophic signaling. Unlike conventional small molecules, peptides can be engineered to recognize specific pathological protein conformations or aggregation-prone motifs. For example, tau-targeting peptides can bind aberrant tau assemblies with high selectivity and low toxicity. This versatility makes peptides uniquely suited for modulating the multifactorial mechanisms of AD.
Medicinal chemistry strategies are critical for optimizing the drug-like properties of peptides. Techniques such as backbone cyclization, N methylation, and the incorporation of D amino acids or PEG chains have been shown to significantly improve metabolic stability and CNS exposure. Structure–activity relationship (SAR) studies guide the placement of hydrophobic and charged residues to enhance target binding and blood–brain barrier (BBB) penetration. For instance, the introduction of cyclized or stapled motifs can increase receptor affinity and protease resistance without sacrificing solubility. Multivalent designs and peptide–drug conjugates have also been explored to combine targeting and effector functions within single molecules. In each case, the choice of modification is determined by computational modelling to predict how sequence changes affect stability, permeability, and binding.
Computational and AI-driven methods play central roles in peptide discovery. High-throughput in silico screening, molecular docking, and molecular dynamics simulations are routinely used to predict peptide–target interactions with Aβ and tau and to identify key binding conformations and affinities. Machine learning and generative models enable rapid design of novel peptide sequences optimized for multiple criteria (eg., affinity, solubility, and BBB permeability). Recent AI platforms have generated peptides that cap amyloid fibrils or predict sequences capable of crossing the BBB with a high probability. At the same time, the limitations of current tools are recognized (for example, AlphaFold’s structures for D-amino acid peptides remain unreliable), underscoring the need for specialized algorithms and iterative validation.
The effective delivery of peptides to the brain remains a significant challenge. The BBB excludes over 98% of small molecules and virtually all peptide drugs. Therefore, advanced delivery vehicles are under development. Lipid-based nanoparticles, receptor-targeting conjugates, cell-penetrating peptide tags, and intranasal formulations have been investigated for their ability to enhance CNS uptake. Concurrently, innovations in peptide synthesis, such as automated continuous-flow platforms with inline monitoring, now allow the rapid generation and optimization of large peptide libraries. These technologies facilitate systematic testing of sequence variants and formulations to identify candidates with improved permeability and stability.
On the translational front, multiple peptide candidates have demonstrated efficacy in AD models and early phase studies. Some FDA-approved peptides (for example, metabolic peptides such as GLP-1 analogs) are being repurposed in AD trials, and novel peptide vaccines and neuroprotective peptides are under clinical evaluation. Several candidates have shown a reduction in amyloid or tau pathology and cognitive benefit in preclinical models, and ongoing trials are assessing the safety and biomarker effects in patients. These advances indicate a growing momentum in the field, although to date, no peptide has yet reached late-stage approval for AD.
Notwithstanding these advances, several notable challenges remain. The chief among them is the impermeability of the BBB: most therapeutic peptides are excluded from the brain unless they are chemically modified or delivered via specialized carriers. Peptides are intrinsically susceptible to enzymatic degradation, resulting in a short in vivo half-life that complicates chronic treatment. Immunogenicity is a concern for long-term administration, and manufacturing large or highly modified peptides at a scale remains technically and economically difficult. Furthermore, AI and data-driven pipelines require careful curation to avoid biases, and the lack of human-relevant BBB models limits their predictive power. Finally, regulatory considerations and the need for cost-effective manufacturing affect the path toward clinical use.
In summary, the field of peptide therapeutics for AD has matured substantially; integrated advances in medicinal chemistry, computational design, and delivery are yielding lead candidates with improved stability and CNS activity. Current strategies blend rational design with high-throughput AI approaches to explore expanded peptide chemical spaces. Addressing the remaining translational gaps, particularly BBB penetration, long-term stability, and scalable production, will be essential. Meeting these challenges will require sustained interdisciplinary efforts, but the convergence of computational and experimental innovation provides a robust foundation for developing disease-modifying peptide therapies for AD.
Based on current knowledge, a peptide can reasonably be considered “CNS‑ready” when it fulfills at least the following minimal criteria: (a) reproducible demonstration of target engagement and disease‑relevant efficacy in at least two independent AD‑relevant models; (b) documented brain exposure with free brain concentrations at or above estimated efficacious levels, supported by appropriate PK/PD modeling; (c) adequate stability and safety in vivo, including a favorable immunogenicity profile over repeated dosing; and (d) a clearly defined and scalable synthetic route compatible with GMP requirements. Candidates that do not yet meet these benchmarks should be regarded as promising tool compounds or early leads rather than near‑term clinical contenders.
Looking ahead, a realistic 5–10‑year roadmap for peptide therapeutics in AD might include the following milestones: (i) integrating robust BBB‑relevant pharmacokinetics and brain exposure measurements into early lead optimization rather than treating them as late‑stage “gating” criteria; (ii) combining AI‑guided sequence design with experimentally validated BBB models and multi‑target pharmacology to generate peptides that address Aβ, tau, and neuroinflammation simultaneously; and (iii) embedding adaptive, biomarker‑rich designs into clinical trials to de‑risk translation and identify responder subgroups more efficiently. Achieving these milestones will require coordinated progress across computation, medicinal chemistry, delivery science, and clinical methodology.
Abbreviations
AD, Alzheimer’s disease; AI, artificial intelligence; Aβ, amyloid-β; BBB, blood–brain barrier; ML, machine learning; PD, Parkinson’s disease; CNS, central nervous system; ADMET, absorption, distribution, metabolism, excretion, and toxicity; BACE-1, β-site amyloid precursor protein cleaving enzyme 1; APP, amyloid precursor protein; PK, pharmacokinetics; SPPS, Solid-phase peptide synthesis; SAR structure–activity relationship; PDCs, peptide–drug conjugates; UV–vis, ultraviolet–visible; GLP-1, glucagon-like peptide-1; DL, deep learning; VS, virtual screening; MD, molecular dynamics; NVU, neurovascular unit; GLP-1RAs, GLP-1 receptor agonists; Trk, tropomyosin receptor kinase; BDNF, brain-derived neurotrophic factor; FDA, U.S. Food and Drug Administration; EMA, European Medicines Agency; CPPs, Cell-penetrating peptides.
Data Sharing Statement
No new data were created or analyzed in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Ahmad MA, Kareem O, Khushtar M, et al. Neuroinflammation: a Potential Risk for Dementia. Int J Mol Sci. 2022;23(2):616. doi:10.3390/ijms23020616
2. Gadhave DG, Sugandhi VV, Jha SK, et al. Neurodegenerative disorders: mechanisms of degeneration and therapeutic approaches with their clinical relevance. Ageing Res Rev. 2024;99:102357. doi:10.1016/j.arr.2024.102357
3. Alzheimer’s Association. Alzheimer’s disease facts and figures. Alzheimer’s Dementia. 2019;15(3):321–28. doi:10.1016/j.jalz.2019.01.010.
4. Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimer’s Dementia. 2025;21(4):70235. doi:10.1002/alz.70235.
5. Wang C, Shao S, Li N, Zhang Z, Zhang H, Liu B. Advances in Alzheimer’s Disease-Associated Aβ Therapy Based on Peptide. Int J Mol Sci. 2023;24(17):13110. doi:10.3390/ijms241713110
6. Lukiw WJ. Amyloid beta (Aβ) peptide modulators and other current treatment strategies for Alzheimer’s disease (AD). Expert Opin Emerg Drugs. 2012;17(1):43–60. doi:10.1517/14728214.2012.672559
7. Jeremic D, Jiménez-Díaz L, Navarro-López JD. Past, present and future of therapeutic strategies against amyloid-β peptides in Alzheimer’s disease: a systematic review. Ageing Res Rev. 2021;72:101496. doi:10.1016/j.arr.2021.101496
8. Hussain R, Zubair H, Pursell S, Shahab M. Neurodegenerative Diseases: regenerative Mechanisms and Novel Therapeutic Approaches. Brain Sci. 2018;8(9):177. doi:10.3390/brainsci8090177
9. Arvanitis CD, Ferraro GB, Jain RK. The blood–brain barrier and blood–tumour barrier in brain tumours and metastases. Nat Rev Cancer. 2020;20(1):26–41. doi:10.1038/s41568-019-0205-x
10. Lucana MC, Arruga Y, Petrachi E, Roig A, Lucchi R, Oller-Salvia B. Protease-Resistant Peptides for Targeting and Intracellular Delivery of Therapeutics. Pharmaceutics. 2021;13(12):2065. doi:10.3390/pharmaceutics13122065
11. Wang Y, Zhang L, Liu C, Luo Y, Chen D. Peptide-Mediated Nanocarriers for Targeted Drug Delivery: developments and Strategies. Pharmaceutics. 2024;16(2):240. doi:10.3390/pharmaceutics16020240
12. Hamada Y, Ziora ZM. Peptidomimetic Synthesis: drug Discovery for Alzheimer’s Disease. Methods in Molecular Biology (Clifton, N.J.). 2020;2103:215–223. doi:10.1007/978-1-0716-0227-0_14
13. Ekambaram S, Dokholyan NV. Peptide-based drug design using generative AI. Chem Commun. 2026;62(3):672–691. doi:10.1039/D5CC04998A
14. Ye J, Li A, Zheng H, Yang B, Lu Y. Machine Learning Advances in Predicting Peptide/Protein‐Protein Interactions Based on Sequence Information for Lead Peptides Discovery. Adv Biol. 2023;7(6). doi:10.1002/adbi.202200232
15. Selkoe DJ, Hardy J. The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO Mol Med. EMBO Molecular Medicine. 2016;8(6):595–608. doi:10.15252/emmm.201606210
16. De-Paula VJ, Radanovic M, Diniz BS, Forlenza OV. Alzheimer’s Disease. Sub-Cellular Biochemistry. 2012;65:329–352. doi:10.1007/978-94-007-5416-4_14
17. Kim M, Bezprozvanny I. Analysis of Non-Amyloidogenic Mutations in APP Supports Loss of Function Hypothesis of Alzheimer’s Disease. Int J Mol Sci. 2023;24(3):2092. doi:10.3390/ijms24032092
18. Hardy JA, Higgins GA. Alzheimer’s Disease: the Amyloid Cascade Hypothesis. Science. 1992;256(5054):184–185. doi:10.1126/science.1566067
19. Wang Y, Mandelkow E. Tau in physiology and pathology. Nat Rev Neurosci. 2016;17(1):22–35. doi:10.1038/nrn.2015.1
20. Venkatramani A, Panda D. Regulation of neuronal microtubule dynamics by tau: implications for tauopathies. Int J Biol Macromol. 2019;133:473–483. doi:10.1016/j.ijbiomac.2019.04.120
21. Heneka MT, Carson MJ, Khoury J, et al. Neuroinflammation in Alzheimer’s disease. Lancet Neurol. 2015;14(4):388–405. doi:10.1016/S1474-4422(15)70016-5
22. Uddin M, Kabir M, Jalouli M, et al. Neuroinflammatory Signaling in the Pathogenesis of Alzheimer’s Disease. Curr Neuropharmacol. 2022;20(1):126–146. doi:10.2174/1570159X19666210826130210
23. Shadfar S, Hwang CJ, Lim MS, Choi DY, Hong JT. Involvement of inflammation in Alzheimer’s disease pathogenesis and therapeutic potential of anti-inflammatory agents. Arch Pharm Res. 2015;38(12):2106–2119. doi:10.1007/s12272-015-0648-x
24. Kwon HS, Koh SH. Neuroinflammation in neurodegenerative disorders: the roles of microglia and astrocytes. Transl Neurodegener. 2020;9(1):42. doi:10.1186/s40035-020-00221-2
25. Muronets VI, Kudryavtseva SS, Kurochkina LP, Leisi EV, Stroylova Y, Schmalhausen EV. Factors Affecting Pathological Amyloid Protein Transformation: from Post-Translational Modifications to Chaperones. Biochem Moscow. 2025;90(S1):S164–S192. doi:10.1134/S0006297924604003
26. Barão S, Moechars D, Lichtenthaler SF, De Strooper B. BACE1 Physiological Functions May Limit Its Use as Therapeutic Target for Alzheimer’s Disease. Trends Neurosci. 2016;39(3):158–169. doi:10.1016/j.tins.2016.01.003
27. Cerrato CP, Langel Ü. An update on cell-penetrating peptides with intracellular organelle targeting. Expert Opin Drug Deliv. 2022;19(2):133–146. doi:10.1080/17425247.2022.2034784
28. Daneman R, Prat A. The Blood–Brain Barrier. Cold Spring Harb Perspect Biol. 2015;7(1):a020412. doi:10.1101/cshperspect.a020412
29. René CA, Parks RJ. Delivery of Therapeutic Agents to the Central Nervous System and the Promise of Extracellular Vesicles. Pharmaceutics. 2021;13(4):492. doi:10.3390/pharmaceutics13040492
30. Banks WA. From blood–brain barrier to blood–brain interface: new opportunities for CNS drug delivery. Nat Rev Drug Discov. 2016;15(4):275–292. doi:10.1038/nrd.2015.21
31. Fosgerau K, Hoffmann T. Peptide therapeutics: current status and future directions. Drug Discov Today. 2015;20(1):122–128. doi:10.1016/j.drudis.2014.10.003
32. Henninot A, Collins JC, Nuss JM. The Current State of Peptide Drug Discovery: back to the Future? J Med Chem. 2018;61(4):1382–1414. doi:10.1021/acs.jmedchem.7b00318
33. Saleh SR, Abd-Elmegied A, Aly Madhy S, et al. Brain-targeted Tet-1 peptide-PLGA nanoparticles for berberine delivery against STZ-induced Alzheimer’s disease in a rat model: alleviation of hippocampal synaptic dysfunction, Tau pathology, and amyloidogenesis. Int J Pharm. 2024;658:124218. doi:10.1016/j.ijpharm.2024.124218
34. Saleh SR, Khamiss SE, Aly Madhy S, et al. Biochemical investigation and in silico analysis of the therapeutic efficacy of Ipriflavone through Tet-1 Surface-Modified-PLGA nanoparticles in Streptozotocin-Induced Alzheimer’s like Disease: reduced oxidative damage and etiological Descriptors. Int J Pharm. 2025;669:125021. doi:10.1016/j.ijpharm.2024.125021
35. Gozes I. NAP (Davunetide) Provides Functional and Structural Neuroprotection. Curr Pharm Des. 2011;17(10):1040–1044. doi:10.2174/138161211795589373
36. Gozes I. Microtubules (tau) as an Emerging Therapeutic Target: NAP (Davunetide). Curr Pharm Des. 2011;17(31):3413–3417. doi:10.2174/138161211798072553
37. Baral KC, Choi KY. Barriers and Strategies for Oral Peptide and Protein Therapeutics Delivery: update on Clinical Advances. Pharmaceutics. 2025;17(4):397. doi:10.3390/pharmaceutics17040397
38. Renukuntla J, Vadlapudi AD, Patel A, Boddu SHS, Mitra AK. Approaches for enhancing oral bioavailability of peptides and proteins. Int J Pharm. 2013;447(1–2):75–93. doi:10.1016/j.ijpharm.2013.02.030
39. Sahu D, Gupta C, Yennamalli RM, et al. Novel peptide inhibitor of human tumor necrosis factor-α has antiarthritic activity. Sci Rep. 2024;14(1):12935. doi:10.1038/s41598-024-63790-6
40. Mhaske A, Shukla S, Ahirwar K, Singh KK, Shukla R. Receptor-Assisted Nanotherapeutics for Overcoming the Blood–Brain Barrier. Mol Neurobiol. 2024;61(11):8702–8738. doi:10.1007/s12035-024-04015-9
41. Sánchez-Navarro M, Giralt E. Peptide Shuttles for Blood–Brain Barrier Drug Delivery. Pharmaceutics. 2022;14(9):1874. doi:10.3390/pharmaceutics14091874
42. Cavaco M, Fraga P, Valle J, et al. Molecular determinants for brain targeting by peptides: a meta-analysis approach with experimental validation. Fluids Barriers CNS. 2024;21(1):45. doi:10.1186/s12987-024-00545-5
43. Blades R, Ittner LM, Tietz O. Peptides for trans‐blood–brain barrier delivery. J Labelled Comp Radiopharm. 2023;66(9):237–248. doi:10.1002/jlcr.4023
44. Ding S, Khan AI, Cai X, et al. Overcoming blood–brain barrier transport: advances in nanoparticle-based drug delivery strategies. Mater Today. 2020;37:112–125. doi:10.1016/j.mattod.2020.02.001
45. Cogill SA, Lee JH, Jeon MT, Kim DG, Chang Y. Hopping the Hurdle: strategies to Enhance the Molecular Delivery to the Brain through the Blood–Brain Barrier. Cells. 2024;13(10):789. doi:10.3390/cells13100789
46. Pauletti G. Improvement of oral peptide bioavailability: peptidomimetics and prodrug strategies. Adv Drug Deliv Rev. 1997;27(2–3):235–256. doi:10.1016/S0169-409X(97)00045-8
47. Chavda VP, Pandya A, Kumar L, et al. Exosome nanovesicles: a potential carrier for therapeutic delivery. Nano Today. 2023;49:101771. doi:10.1016/j.nantod.2023.101771
48. Wu D, Chen Q, Chen X, Han F, Chen Z, Wang Y. The blood–brain barrier: structure, regulation and drug delivery. Signal Transduct Target Ther. 2023;8(1):217. doi:10.1038/s41392-023-01481-w
49. Goyal D, Shuaib S, Mann S, Goyal B. Rationally Designed Peptides and Peptidomimetics as Inhibitors of Amyloid-β (Aβ) Aggregation: potential Therapeutics of Alzheimer’s Disease. ACS Comb Sci. 2017;19(2):55–80. doi:10.1021/acscombsci.6b00116
50. Sliwoski G, Kothiwale S, Meiler J, Lowe EW. Computational Methods in Drug Discovery. Pharmacol Rev. 2014;66(1):334–395. doi:10.1124/pr.112.007336
51. Torchilin V. Intracellular delivery of protein and peptide therapeutics. Drug Discov Today Technol. 2008;5(2–3):e95–e103. doi:10.1016/j.ddtec.2009.01.002
52. Ding Y, Ting JP, Liu J, Al-Azzam S, Pandya P, Afshar S. Impact of non-proteinogenic amino acids in the discovery and development of peptide therapeutics. Amino Acids. 2020;52(9):1207–1226. doi:10.1007/s00726-020-02890-9
53. Visan AI, Negut I. Integrating Artificial Intelligence for Drug Discovery in the Context of Revolutionizing Drug Delivery. Life (Basel, Switzerland). 2024;14(2):233. doi:10.3390/life14020233
54. Fu C, Chen Q. The future of pharmaceuticals: artificial intelligence in drug discovery and development. J Pharm Anal. 2025;15(8):101248. doi:10.1016/j.jpha.2025.101248
55. Bruno BJ, Miller GD, Lim CS. Basics and Recent Advances in Peptide and Protein Drug Delivery. Ther Deliv. 2013;4(11):1443–1467. doi:10.4155/tde.13.104
56. Kaspar AA, Reichert JM. Future directions for peptide therapeutics development. Drug Discov Today. 2013;18(17–18):807–817. doi:10.1016/j.drudis.2013.05.011
57. Lau JL, Dunn MK. Therapeutic peptides: historical perspectives, current development trends, and future directions. Bioorg Med Chem. 2018;26(10):2700–2707. doi:10.1016/j.bmc.2017.06.052
58. Craik DJ, Fairlie DP, Liras S, Price D. The Future of Peptide‐based Drugs. Chem Biol Drug Des. 2013;81(1):136–147. doi:10.1111/cbdd.12055
59. Hayes HC, Luk LYP, Tsai YH. Approaches for peptide and protein cyclisation. Org Biomol Chem. 2021;19(18):3983–4001. doi:10.1039/D1OB00411E
60. Fang P, Pang WK, Xuan S, Chan WL, Leung KCF. Recent advances in peptide macrocyclization strategies. Chem Soc Rev. 2024;53(24):11725–11771. doi:10.1039/D3CS01066J
61. Al Musaimi O, Lombardi L, Williams DR, Albericio F. Strategies for Improving Peptide Stability and Delivery. Pharmaceuticals. 2022;15(10):1283. doi:10.3390/ph15101283
62. Zhang Y, Kæstel‐Hansen J, Teze D, et al. Click‐Cyclized Cell Penetrating Peptides Containing Hydrophobic Proline Derivatives for Efficient Intracellular Delivery. Angew Chem Int Ed. 2025;64(50):4862. doi:10.1002/anie.202504862
63. Santhanakrishnan KR, Koilpillai J, Narayanasamy D. PEGylation in Pharmaceutical Development: current Status and Emerging Trends in Macromolecular and Immunotherapeutic Drugs. Cureus. 2024. doi:10.7759/cureus.66669
64. Hussain Z, Khan S, Imran M, Sohail M, Shah SWA, de Matas M. PEGylation: a promising strategy to overcome challenges to cancer-targeted nanomedicines: a review of challenges to clinical transition and promising resolution. Drug Deliv Transl Res. 2019;9(3):721–734. doi:10.1007/s13346-019-00631-4
65. Fu M, Zhuang X, Zhang T, Guan Y, Meng Q, Zhang Y. PEGylated leuprolide with improved pharmacokinetic properties. Bioorg Med Chem. 2020;28(4):115306. doi:10.1016/j.bmc.2020.115306
66. Wilczewska AZ, Niemirowicz K, Markiewicz KH, Car H. Nanoparticles as drug delivery systems. Pharmacol Rep. 2012;64(5):1020–1037. doi:10.1016/S1734-1140(12)70901-5
67. McTiernan N, Kjosås I, Arnesen T. Illuminating the impact of N-terminal acetylation: from protein to physiology. Nat Commun. 2025;16(1):703. doi:10.1038/s41467-025-55960-5
68. Cabrele C, Martinek TA, Reiser O, Berlicki Ł. Peptides Containing β-Amino Acid Patterns: challenges and Successes in Medicinal Chemistry. J Med Chem. 2014;57(23):9718–9739. doi:10.1021/jm5010896
69. Manzari MT, Shamay Y, Kiguchi H, Rosen N, Scaltriti M, Heller DA. Targeted drug delivery strategies for precision medicines. Nat Rev Mater. 2021;6(4):351–370. doi:10.1038/s41578-020-00269-6
70. Liu D, DeGrado WF. De Novo Design, Synthesis, and Characterization of Antimicrobial β-Peptides. J Am Chem Soc. 2001;123(31):7553–7559. doi:10.1021/ja0107475
71. Raguse TL, Porter EA, Weisblum B, Gellman SH. Structure−Activity Studies of 14-Helical Antimicrobial β-Peptides:Probing the Relationship between Conformational Stability and Antimicrobial Potency. J Am Chem Soc. 2002;124(43):12774–12785. doi:10.1021/ja0270423
72. Liu L, He H, Du B, He Y. Nanoscale drug formulations for the treatment of Alzheimer’s disease progression. RSC Adv. 2025;15(6):4031–4078. doi:10.1039/D4RA08128E
73. Legutki JB, Zhao ZG, Greving M, Woodbury N, Johnston SA, Stafford P. Scalable high-density peptide arrays for comprehensive health monitoring. Nat Commun. 2014;5(1):4785. doi:10.1038/ncomms5785
74. Hartrampf N, Saebi A, Poskus M, et al. Synthesis of proteins by automated flow chemistry. Science. 2020;368(6494):980–987. doi:10.1126/science.abb2491
75. Sletten ET, Nuño M, Guthrie D, Seeberger PH. Real-time monitoring of solid-phase peptide synthesis using a variable bed flow reactor. Chem Commun. 2019;55(97):14598–14601. doi:10.1039/C9CC08421E
76. Mohapatra S, Hartrampf N, Poskus M, Loas A, Gómez-Bombarelli R, Pentelute BL. Deep Learning for Prediction and Optimization of Fast-Flow Peptide Synthesis. ACS Cent Sci. 2020;6(12):2277–2286. doi:10.1021/acscentsci.0c00979
77. Overby C, Abraham B, Adjei‐Sowah E, et al. A Rapid Manual Solid Phase Peptide Synthesis Method for High‐Throughput Peptide Production. J Biomed Mater Res A. 2025;113(5). doi:10.1002/jbm.a.37922
78. Mándity IM, Olasz B, Ötvös SB, Fülöp F. Continuous‐Flow Solid‐Phase Peptide Synthesis: a Revolutionary Reduction of the Amino Acid Excess. ChemSusChem. 2014;7(11):3172–3176. doi:10.1002/cssc.201402436
79. Mijalis AJ, Thomas DA, Simon MD, et al. A fully automated flow-based approach for accelerated peptide synthesis. Nat Chem Biol. 2017;13(5):464–466. doi:10.1038/nchembio.2318
80. Saebi A, Brown JS, Marando VM, et al. Rapid Single-Shot Synthesis of the 214 Amino Acid-Long N-Terminal Domain of Pyocin S2. ACS Chem Biol. 2023;18(3):518–527. doi:10.1021/acschembio.2c00862
81. Wang L, Wang N, Zhang W, et al. Therapeutic peptides: current applications and future directions. Signal Transduct Target Ther. 2022;7(1):48. doi:10.1038/s41392-022-00904-4
82. Freiherr J, Hallschmid M, Frey WH, et al. Intranasal Insulin as a Treatment for Alzheimer’s Disease: a Review of Basic Research and Clinical Evidence. CNS Drugs. 2013;27(7):505–514. doi:10.1007/s40263-013-0076-8
83. Craft S, Raman R, Chow TW, et al. Safety, Efficacy, and Feasibility of Intranasal Insulin for the Treatment of Mild Cognitive Impairment and Alzheimer Disease Dementia. JAMA Neurol. 2020;77(9):1099. doi:10.1001/jamaneurol.2020.1840
84. Femminella GD, Frangou E, Love SB, et al. Evaluating the effects of the novel GLP-1 analogue liraglutide in Alzheimer’s disease: study protocol for a randomised controlled trial (ELAD study). Trials. 2019;20(1):191. doi:10.1186/s13063-019-3259-x
85. El-Ganainy SO, Soliman OA, Ghazy AA, et al. Intranasal Oxytocin Attenuates Cognitive Impairment, β-Amyloid Burden and Tau Deposition in Female Rats with Alzheimer’s Disease: interplay of ERK1/2/GSK3β/Caspase-3. Neurochem Res. 2022;47(8):2345–2356. doi:10.1007/s11064-022-03624-x
86. Keech B, Crowe S, Hocking DR. Intranasal oxytocin, social cognition and neurodevelopmental disorders: a meta-analysis. Psychoneuroendocrinology. 2018;87:9–19. doi:10.1016/j.psyneuen.2017.09.022
87. Purohit K, Reddy N, Sunna A. Exploring the Potential of Bioactive Peptides: from Natural Sources to Therapeutics. Int J Mol Sci. 2024;25(3):1391. doi:10.3390/ijms25031391
88. Vicidomini C, Fontanella F, D’Alessandro T, Roviello GN. A Survey on Computational Methods in Drug Discovery for Neurodegenerative Diseases. Biomolecules. 2024;14(10):1330. doi:10.3390/biom14101330
89. Job N, Thimmakondu VS, Thirumoorthy K. In Silico Drug Design and Analysis of Dual Amyloid-Beta and Tau Protein-Aggregation Inhibitors for Alzheimer’s Disease Treatment. Molecules. 2023;28(3):1388. doi:10.3390/molecules28031388
90. Vugmeyster L, Clark MA, Falconer IB, et al. Flexibility and Solvation of Amyloid-β Hydrophobic Core. J Biol Chem. 2016;291(35):18484–18495. doi:10.1074/jbc.M116.740530
91. Xiao W, Chen LZ, Chang J, Xiao YW. Discovery of Novel Anti-Acetylcholinesterase Peptides Using a Machine Learning and Molecular Docking Approach. Drug Des Devel Ther. 2025;19:5085–5098. doi:10.2147/DDDT.S523769
92. Lemkul JA, Bevan DR. The Role of Molecular Simulations in the Development of Inhibitors of Amyloid β-Peptide Aggregation for the Treatment of Alzheimer’s Disease. ACS Chem Neurosci. 2012;3(11):845–856. doi:10.1021/cn300091a
93. Llorach-Pares L, Nonell-Canals A, Sanchez-Martinez M, Avila C. Computer-Aided Drug Design Applied to Marine Drug Discovery: meridianins as Alzheimer’s Disease Therapeutic Agents. Mar Drugs. 2017;15(12):366. doi:10.3390/md15120366
94. Nguyen PH, Tufféry P, Derreumaux P. Dynamics of Amyloid Formation from Simplified Representation to Atomistic Simulations. Methods in Molecular Biology (Clifton, N.J.). 2022;2405:95–113. doi:10.1007/978-1-0716-1855-4_5
95. França VLB, Bezerra EM, da Costa RF, Carvalho HF, Freire VN, Matos G. Alzheimer’s Disease Immunotherapy and Mimetic Peptide Design for Drug Development: mutation Screening, Molecular Dynamics, and a Quantum Biochemistry Approach Focusing on Aducanumab::Aβ2–7 Binding Affinity. ACS Chem Neurosci. 2024;15(19):3543–3562. doi:10.1021/acschemneuro.4c00453
96. Gackowski M, Madriwala B, Studzińska R, Koba M. Novel Isosteviol-Based FXa Inhibitors: molecular Modeling, In Silico Design and Docking Simulation. Molecules. 2023;28(13):4977. doi:10.3390/molecules28134977
97. Mądra-Gackowska K, Baumgart S, Jędrzejewski M, Studzińska R, Szeleszczuk Ł, Gackowski M. Computational QSAR study of novel 2-aminothiazol-4(5H)-one derivatives as 11β‐HSD1 inhibitors. J Comput Aided Mol Des. 2025;39(1):67. doi:10.1007/s10822-025-00648-7
98. Goles M, Daza A, Cabas-Mora G, et al. Peptide-based drug discovery through artificial intelligence: towards an autonomous design of therapeutic peptides. Brief Bioinform. 2024;25(4). doi:10.1093/bib/bbae275
99. Lavecchia A. Machine-learning approaches in drug discovery: methods and applications. Drug Discov Today. 2015;20(3):318–331. doi:10.1016/j.drudis.2014.10.012
100. Vamathevan J, Clark D, Czodrowski P, et al. Applications of machine learning in drug discovery and development. Nat Rev Drug Discov. 2019;18(6):463–477. doi:10.1038/s41573-019-0024-5
101. Zhang G, Liu C, Lu J, Zhang S, Zhu L. The Role of AI-Driven De Novo Protein Design in the Exploration of the Protein Functional Universe. Biology. 2025;14(9):1268. doi:10.3390/biology14091268
102. Vacher M, Canovas R, Laws SM, Doecke JD. A comprehensive multi-omics analysis reveals unique signatures to predict Alzheimer’s disease. Front Bioinform. 2024;4:1390607. doi:10.3389/fbinf.2024.1390607
103. Chen S, Lin T, Basu R, et al. Design of target specific peptide inhibitors using generative deep learning and molecular dynamics simulations. Nat Commun. 2024;15(1):1611. doi:10.1038/s41467-024-45766-2
104. Wallace HM, Yang H, Tan S, et al. De novo design of peptides that bind specific conformers of α-synuclein. Chem Sci. 2024;15(22):8414–8421. doi:10.1039/D3SC06245G
105. Tang Q, Chen W. DeepB3P: a transformer-based model for identifying blood-brain barrier penetrating peptides with data augmentation using feedback GAN. J Adv Res. 2025;73:459–468. doi:10.1016/j.jare.2024.08.002
106. Krokidis MG, Koumadorakis DE, Lazaros K, et al. AlphaFold3: an Overview of Applications and Performance Insights. Int J Mol Sci. 2025;26(8):3671. doi:10.3390/ijms26083671
107. Abramson J, Adler J, Dunger J, et al. Accurate structure prediction of biomolecular interactions with AlphaFold 3. Nature. 2024;630(8016):
108. Li C, Pazgier M, Li J, et al. Limitations of Peptide Retro-inverso Isomerization in Molecular Mimicry. J Biol Chem. 2010;285(25):19572–19581. doi:10.1074/jbc.M110.116814
109. Garton M, Nim S, Stone TA, Wang KE, Deber CM, Kim PM. Method to generate highly stable D-amino acid analogs of bioactive helical peptides using a mirror image of the entire PDB. Proc Natl Acad Sci. 2018;115(7):1505–1510. doi:10.1073/pnas.1711837115
110. Geylan G, Janet JP, Tibo A, et al. PepINVENT: generative peptide design beyond natural amino acids. Chem Sci. 2025;16(20):8682–8696. doi:10.1039/D4SC07642G
111. Nissan N, Allen MC, Sabatino D, Biggar KK. Future Perspective: harnessing the Power of Artificial Intelligence in the Generation of New Peptide Drugs. Biomolecules. 2024;14(10):1303. doi:10.3390/biom14101303
112. Forli S, Huey R, Pique ME, Sanner MF, Goodsell DS, Olson AJ. Computational protein–ligand docking and virtual drug screening with the AutoDock suite. Nat Protoc. 2016;11(5):905–919. doi:10.1038/nprot.2016.051
113. Jumper J, Evans R, Pritzel A, et al. Highly accurate protein structure prediction with AlphaFold. Nature. 2021;596(7873):583–589. doi:10.1038/s41586-021-03819-2
114. Zhang Y, Chen H, Li R, Sterling K, Song W. Amyloid β-based therapy for Alzheimer’s disease: challenges, successes and future. Signal Transduct Target Ther. 2023;8(1):248. doi:10.1038/s41392-023-01484-7
115. Lu J, Cao Q, Wang C, et al. Structure-Based Peptide Inhibitor Design of Amyloid-β Aggregation. Front Mol Neurosci. 2019;12:12. doi:10.3389/fnmol.2019.00054
116. Murray KA, Hu CJ, Griner SL, et al. De novo designed protein inhibitors of amyloid aggregation and seeding. Proc Natl Acad Sci. 2022;119(34). doi:10.1073/pnas.2206240119
117. Vincenzi M, Mercurio FA, Leone M. Virtual Screening of Peptide Libraries: the Search for Peptide-Based Therapeutics Using Computational Tools. Int J Mol Sci. 2024;25(3):1798. doi:10.3390/ijms25031798
118. Santambrogio A, Horne RI, Metrick MA, et al. Design of Tau Aggregation Inhibitors Using Iterative Machine Learning and a Polymorph-Specific Brain-Seeded Fibril Amplification Assay. J Am Chem Soc. 2025;147(39):35942–35952. doi:10.1021/jacs.5c12812
119. Lippens G, Gigant B. Elucidating Tau function and dysfunction in the era of cryo-EM. J Biol Chem. 2019;294(24):9316–9325. doi:10.1074/jbc.REV119.008031
120. Pourmand S, Zareei S, Jozi M, Massahi S. Computational disruption of paired helical filaments (PHFs) assembly using Milk Lactalbumin-derived peptides against Alzheimer’s disease. J Funct Foods. 2025;130:106853. doi:10.1016/j.jff.2025.106853
121. Mesias A, Borges S, Pintado M, Baptista-Silva S. Bioactive peptides as multipotent molecules bespoke and designed for Alzheimer’s disease. Neuropeptides. 2025;111:102515. doi:10.1016/j.npep.2025.102515
122. Jegani KT, Balde A, Nazeer RA. A review on anti-inflammatory and antioxidant peptides derived from marine organisms: mechanism of action and therapeutic applications. Food Biosci. 2025;63:105745. doi:10.1016/j.fbio.2024.105745
123. Cai Y, Liu J, Wang B, Sun M, Yang H. Microglia in the Neuroinflammatory Pathogenesis of Alzheimer’s Disease and Related Therapeutic Targets. Front Immunol. 2022;13:856376. doi:10.3389/fimmu.2022.856376
124. Valencia-Olvera AC, Balu D, Bellur S, et al. A novel apoE-mimetic increases brain apoE levels, reduces Aβ pathology and improves memory when treated before onset of pathology in male mice that express APOE3. Alzheimers Res Ther. 2023;15(1):216. doi:10.1186/s13195-023-01353-z
125. Camargo MLM, Farias AB, Bertazzo GB, et al. Novel Copper Chelators Enhance Spatial Memory and Biochemical Outcomes in Alzheimer’s Disease Model. ACS Chem Neurosci. 2025;16(17):3267–3281. doi:10.1021/acschemneuro.5c00291
126. Złotek M, Kurowska A, Herbet M, Piątkowska-Chmiel I. GLP-1 Analogs, SGLT-2, and DPP-4 Inhibitors: a Triad of Hope for Alzheimer’s Disease Therapy. Biomedicines. 2023;11(11):3035. doi:10.3390/biomedicines11113035
127. Decourt B, Noorda K, Noorda K, Shi J, Sabbagh MN. Review of Advanced Drug Trials Focusing on the Reduction of Brain Beta-Amyloid to Prevent and Treat Dementia. J Exp Pharmacol. 2022;14:331–352. doi:10.2147/JEP.S265626
128. Soto-Rojas LO, Pacheco-Herrero M, Martínez-Gómez PA, et al. The Neurovascular Unit Dysfunction in Alzheimer’s Disease. Int J Mol Sci. 2021;22(4):2022. doi:10.3390/ijms22042022
129. Pokrzyk J, Kulczyńska-Przybik A, Guzik-Makaruk E, Winkel I, Mroczko B. Clinical Importance of Amyloid Beta Implication in the Detection and Treatment of Alzheimer’s Disease. Int J Mol Sci. 2025;26(5):1935. doi:10.3390/ijms26051935
130. Omidian H, Wilson RL, Castejon AM. Recent Advances in Peptide-Loaded PLGA Nanocarriers for Drug Delivery and Regenerative Medicine. Pharmaceuticals. 2025;18(1):127. doi:10.3390/ph18010127
131. Thompson TS, Sefiani A, Burgess K. Small-Molecule Trk Agonists: where Do We Go from Here? J Med Chem. 2025;68(15):15233–15259. doi:10.1021/acs.jmedchem.4c02365
132. Janssens J, Etienne H, Idriss S, Azmi A, Martin B, Maudsley S. Systems-Level G Protein-Coupled Receptor Therapy Across a Neurodegenerative Continuum by the GLP-1 Receptor System. Front Endocrinol. 2014;5:5. doi:10.3389/fendo.2014.00142
133. Ríos JA, Bórquez JC, Godoy JA, Zolezzi JM, Furrianca MC, Inestrosa NC. Emerging role of Metformin in Alzheimer’s disease: a translational view. Ageing Res Rev. 2024;100:102439. doi:10.1016/j.arr.2024.102439
134. Mo X, Rao DP, Kaur K, et al. Indole Derivatives: a Versatile Scaffold in Modern Drug Discovery—An Updated Review on Their Multifaceted Therapeutic Applications (2020–2024). Molecules. 2024;29(19):4770. doi:10.3390/molecules29194770
135. Sousa T, Moreira PI, Cardoso S. Current Advances in Mitochondrial Targeted Interventions in Alzheimer’s Disease. Biomedicines. 2023;11(9):2331. doi:10.3390/biomedicines11092331
136. Cummings JL, Zhou Y, Lee G, et al. Alzheimer’s disease drug development pipeline: 2025. Alzheimers Dementia. 2025;11(2):70098. doi:10.1002/trc2.70098
137. Cummings J, Zhou Y, Lee G, Zhong K, Fonseca J, Cheng F. Alzheimer’s disease drug development pipeline: 2024. Alzheimers Dementia. 2024;10(2):12465. doi:10.1002/trc2.12465
138. Feldman HH, Cummings JL, Boxer AL, et al. A framework for translating tauopathy therapeutics: drug discovery to clinical trials. Alzheimer’s Dementia. 2024;20(11):8129–8152. doi:10.1002/alz.14250
139. Zetterberg H, Rinne JO, Sandberg A, et al. Phase 1b trial on the safety, tolerability and immunogenicity of anti‐amyloid vaccine ALZ‐101 in subjects with MCI or mild AD. Alzheimer’s Dementia. 2024;20(S8). doi:10.1002/alz.095440
140. ClinicalTrialsgov. A Study of ND-001 in Patients with Early Alzheimer’s Disease. 2024. Available from: https://clinicaltrials.gov/ct2/show/NCT05267535.
141. O’Mara A, Mody BP, Mammi M, et al. The effect of GLP-1 receptor agonists on cognition in nondiabetic patients with mild cognitive impairment or Alzheimer’s disease: a meta-analysis of randomized controlled trials. Neurol Sci. 2026;47(1):149. doi:10.1007/s10072-025-08602-z
142. ClinicalTrialsgov. Study of Cerebrolysin in Dementia. 2025. Available from: https://clinicaltrials.gov/study/NCT06677502.
143. Cummings J, Lee G, Nahed P, et al. Alzheimer’s disease drug development pipeline: 2022. Alzheimers Dementia. 2022;8(1):12295. doi:10.1002/trc2.12295
144. Antonioni A, Di Lorenzo F. Topic Issue: “Translational Advances in Neurodegenerative Dementias. Neurol Int. 2025;17(2):31. doi:10.3390/neurolint17020031
145. Salameh TS, Banks WA. Delivery of Therapeutic Peptides and Proteins to the CNS. Advances in Pharmacology (San Diego, Calif.). 2014;71:277–299. doi:10.1016/bs.apha.2014.06.004
146. Martian PC, Tertis M, Leonte D, Hadade N, Cristea C, Crisan O. Cyclic peptides: a powerful instrument for advancing biomedical nanotechnologies and drug development. J Pharm Biomed Anal. 2025;252:116488. doi:10.1016/j.jpba.2024.116488
147. Hashemi S, Vosough P, Taghizadeh S, Savardashtaki A. Therapeutic peptide development revolutionized: harnessing the power of artificial intelligence for drug discovery. Heliyon. 2024;10(22):e40265. doi:10.1016/j.heliyon.2024.e40265
148. Otero-Losada M, Capani F, Pérez-Lloret S. Neuroprotection - New Approaches and Prospects. Otero-Losada M, Capani F, Perez Lloret S, eds.. IntechOpen;2020. doi:10.5772/intechopen.77918
149. de Raffele D, Ilie IM. Unlocking novel therapies: cyclic peptide design for amyloidogenic targets through synergies of experiments, simulations, and machine learning. Chem Commun. 2024;60(6):632–645. doi:10.1039/D3CC04630C
150. Aileen Funke S, Willbold D. Peptides for Therapy and Diagnosis of Alzheimer’s Disease. Curr Pharm Des. 2012;18(6):755–767. doi:10.2174/138161212799277752
151. Ruderisch N, Schlatter D, Kuglstatter A, et al. Potent and Selective BACE-1 Peptide Inhibitors Lower Brain Aβ Levels Mediated by Brain Shuttle Transport. EBioMedicine. 2017;24:76–92. doi:10.1016/j.ebiom.2017.09.004
152. Mojarad-Jabali S, Roh KH. Peptide-based inhibitors and nanoparticles: emerging therapeutics for Alzheimer’s disease. Int J Pharm. 2025;669:125055. doi:10.1016/j.ijpharm.2024.125055
153. Meredith ME, Salameh TS, Banks WA. Intranasal Delivery of Proteins and Peptides in the Treatment of Neurodegenerative Diseases. AAPS J. 2015;17(4):780–787. doi:10.1208/s12248-015-9719-7
154. Nam Y, Shin SJ, Kumar V, Won J, Kim S, Moon M. Dual modulation of amyloid beta and tau aggregation and dissociation in Alzheimer’s disease: a comprehensive review of the characteristics and therapeutic strategies. Transl Neurodegener. 2025;14(1):15. doi:10.1186/s40035-025-00479-4
155. Cummings J, Lee G, Ritter A, Sabbagh M, Zhong K. Alzheimer’s disease drug development pipeline: 2020. Alzheimers Dementia. 2020;6(1):12050. doi:10.1002/trc2.12050
156. Cummings JL, Osse AML, Kinney JW. Alzheimer’s Disease: novel Targets and Investigational Drugs for Disease Modification. Drugs. 2023;83(15):1387–1408. doi:10.1007/s40265-023-01938-w
157. Spinelli R, Sanchís I, Siano A. Fighting Alzheimer’s naturally: peptides as multitarget drug leads. Bioorg Med Chem Lett. 2025;127:130305. doi:10.1016/j.bmcl.2025.130305
158. Wang S, Liao Z, Zhang Q, Han X, Liu C, Wang J. Mitochondrial dysfunction in Alzheimer’s disease: a key frontier for future targeted therapies. Front Immunol. 2025;15:1484373. doi:10.3389/fimmu.2024.1484373
159. Wang M, Amakye WK, Gong C, Ren Z, Yuan E, Ren J. Effect of oral and intraperitoneal administration of walnut-derived pentapeptide PW5 on cognitive impairments in APPSWE/PS1ΔE9mice. Free Radic Biol Med. 2022;180:191–197. doi:10.1016/j.freeradbiomed.2022.01.003
160. McCradden MD, Joshi S, Mazwi M, Anderson JA. Ethical limitations of algorithmic fairness solutions in health care machine learning. Lancet Digit Health. 2020;2(5):e221–e223. doi:10.1016/S2589-7500(20)30065-0
161. F.D.A. Considerations for the Use of Artificial Intelligence to Support Regulatory Decision-Making for Drug and Biological Products. 2025. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considerations-use-artificial-intelligence-support-regulatory-decision-making-drug-and-biological.
162. Röösli E, Bozkurt S, Hernandez-Boussard T. Peeking into a black box, the fairness and generalizability of a MIMIC-III benchmarking model. Sci Data. 2022;9(1):24. doi:10.1038/s41597-021-01110-7
163. H Johnson, F Kim, J Kim, et al. 16th Clinical Trials on Alzheimer’s Disease (CTAD) Boston, MA (USA) October 24–27, 2023: symposia. J Prev Alzheimers Dis. 2023;10:4–55. doi:10.14283/jpad.2022.129
164. Pascoal TA, Aguzzoli CS, Lussier FZ, et al. Insights into the use of biomarkers in clinical trials in Alzheimer’s disease. EBioMedicine. 2024;108:105322. doi:10.1016/j.ebiom.2024.105322
165. Puig M, Shubow S. Immunogenicity of therapeutic peptide products: bridging the gaps regarding the role of product-related risk factors. Front Immunol. 2025;16. doi:10.3389/fimmu.2025.1608401.
166. Achilleos K, Petrou C, Nicolaidou V, Sarigiannis Y. Beyond Efficacy: ensuring Safety in Peptide Therapeutics through Immunogenicity Assessment. J Pept Sci. 2025;31(6). doi:10.1002/psc.70016
167. Mamoudou H, Mune MAM. AI-driven bioactive peptide discovery of next-generation metabolic biotherapeutics. Applied Food Research. 2025;5(2):101291. doi:10.1016/j.afres.2025.101291
168. Gustavsson E, Raaschou P, Lärfars G, Sandman L, Juth N. Novel drug candidates targeting Alzheimer’s disease: ethical challenges with identifying the relevant patient population. J Med Ethics. 2021;47(9):608–614. doi:10.1136/medethics-2021-107304
169. Gold ER, Cook-Deegan R. AI drug development’s data problem. Science. 2025;388(6743):131. doi:10.1126/science.adx0339
170. Alghamdi MA. From Molecules to Medicines: the Role of AI-Driven Drug Discovery Against Alzheimer’s Disease and Other Neurological Disorders. Pharmaceuticals. 2025;18(7):1041. doi:10.3390/ph18071041
171. Dermawan D, Alotaiq N. From Lab to Clinic: how Artificial Intelligence (AI) Is Reshaping Drug Discovery Timelines and Industry Outcomes. Pharmaceuticals. 2025;18(7):981. doi:10.3390/ph18070981
172. Ai R, Xiao X, Deng S, et al. Artificial intelligence in drug development for delirium and Alzheimer’s disease. Acta Pharm Sin B. 2025;15(9):4386–4410. doi:10.1016/j.apsb.2025.04.026
173. Qiu Y, Cheng F. Artificial intelligence for drug discovery and development in Alzheimer’s disease. Curr Opin Struct Biol. 2024;85:102776. doi:10.1016/j.sbi.2024.102776
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Artificial Intelligence in Cerebrovascular Disease Management: A Comprehensive Review of Risk Prediction, Diagnosis, Therapeutic Optimization, and Clinical Translation
Zhang H, Ma W, Zhou X, Zhao Z, Zhang R, Bai H, Huang C, Wang Y
Vascular Health and Risk Management 2025, 21:949-964
Published Date: 22 November 2025
Evaluating the Role of AI Assistants in Accelerating Neurodegenerative Disease Research: Opportunities and Translational Limitations
Yu X, Yao Q
Neuropsychiatric Disease and Treatment 2026, 22:614952
Published Date: 30 May 2026
The “Three-Tier Regulatory Network” of Orthokeratology in Myopia Control: Evidence Weight of Underlying Mechanisms, Controversies, and New Perspectives for Clinical Translation--A Review
Han L, He S, Dong S, Lu Y, Zhang M
Clinical Ophthalmology 2026, 20:600353
Published Date: 12 June 2026