Back to Journals » Vascular Health and Risk Management » Volume 21
Artificial Intelligence in Cerebrovascular Disease Management: A Comprehensive Review of Risk Prediction, Diagnosis, Therapeutic Optimization, and Clinical Translation
Authors Zhang H, Ma W, Zhou X, Zhao Z, Zhang R, Bai H, Huang C ![]() , Wang Y
, Wang Y
Received 22 July 2025
Accepted for publication 1 November 2025
Published 22 November 2025 Volume 2025:21 Pages 949—964
DOI https://doi.org/10.2147/VHRM.S555592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Harry Struijker-Boudier
Hengsheng Zhang,1 Wenhui Ma,1 Xingshun Zhou,1 Zinlin Zhao,1 Runjun Zhang,2 Hong Bai,3 Cong Huang,1 Yujun Wang4
1Department of Radiology, No. 926 Hospital, Joint Logistics Support Force of PLA, Kaiyuan, Yunnan, 661699, People’s Republic of China; 2Department of Cardiology, No. 926 Hospital, Joint Logistics Support Force of PLA, Kaiyuan, Yunnan, 661699, People’s Republic of China; 3Department of Neurology, No. 926 Hospital, Joint Logistics Support Force of PLA, Kaiyuan, Yunnan, 661699, People’s Republic of China; 4Department of Radiology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Traditional Chinese Medicine), Hangzhou, Zhejiang, 310006, People’s Republic of China
Correspondence: Cong Huang, Email [email protected] Yujun Wang, Email [email protected]
Abstract: Cerebrovascular diseases (CVDs) impose a heavy global health burden, necessitating efficient management strategies. Artificial intelligence (AI) has become a key transformative tool across the CVD care continuum, and this review systematically synthesizes AI’s latest advancements, limitations, and clinical translation pathways in CVD management, adhering to PRISMA-ScR guidelines. A literature search was performed in four core databases (PubMed, Web of Science, EMBASE, IEEE Xplore) for studies published between 2018– 2023. After strict screening (inclusion: original research/clinical trials with clear indicators; exclusion: unvalidated studies/conference abstracts), 128 high-quality studies were included, with quality assessed via NOS and QUADAS-2. Key AI applications in CVD management include: (1) Risk prediction: Multimodal models (radiomics-CFD, EHR-imaging) achieve AUC > 0.9, but performance declines in elderly patients (> 75 years, ΔAUC=0.08– 0.12); (2) Diagnosis: Systems like Viz LVO and DeepHemorrhage reduce LVO detection time to 6 minutes and hemorrhage segmentation Dice to 0.94, yet face false positives (3.5– 5%) and workflow delays; (3) Therapeutic optimization: Intraoperative AI (eg, Siemens AI-Path) shortens microcatheter placement time by 61%, and pharmacogenomic models cut antiplatelet complications by 37%; (4) Long-term monitoring: Mobile platforms (eg, NeuroVision™) automate NIHSS scoring (ICC=0.93) but lose accuracy in home settings (ICC=0.85– 0.88). Critical limitations of current AI include single-center data bias, poor interpretability, and legal risks (unclear misdiagnosis liability). This review proposes three innovative solutions: a “data-model-clinical” closed loop, a multidimensional AI value evaluation system, and defining the “human-AI collaboration boundary” in neurointerventions. Future directions focus on primary care-adapted lightweight models, comorbidity-specific algorithms, and AI-assisted rehabilitation. This review emphasizes that physician-AI collaboration and standardized frameworks (eg, AI-RADS, WHO-ITU guidelines) are critical for AI’s sustainable translation in CVD care. Addressing current gaps will enable AI to further improve therapeutic efficiency and functional outcomes, alleviating the global CVD burden.
Keywords: artificial intelligence, cerebrovascular diseases, risk prediction, clinical translation, systematic review
Introduction
Cerebrovascular diseases (CVDs) claim approximately 6.5 million lives annually, with ischemic stroke accounting for 87% of these fatalities.1 This staggering burden, compounded by accelerating global population aging, renders early prediction, precise diagnosis, and efficient management of conditions like aneurysm rupture and carotid stenosis paramount challenges in contemporary radiological practice. Conventional diagnostic approaches, limited by inter-observer variability, intricate imaging data interpretation, and time-sensitive demands in acute stroke care, frequently fail to meet clinical requirements for rapid decision-making. Notably, the compliance rate for the critical door-to-needle time (DNT) in thrombolysis remains below 60%,2 highlighting an urgent need for intelligent decision-support systems.
Artificial intelligence (AI) has emerged as a transformative force in cerebrovascular disease management. Following the landmark 2016 ImageNet competition where convolutional neural networks (CNNs) surpassed human visual recognition capabilities, both CNNs and Transformer architectures have demonstrated unprecedented potential in medical imaging analysis.3 Radiomics now enables objective quantification of carotid plaque vulnerability through extraction of >1,200 high-throughput imaging features,4 while federated learning facilitates secure multicenter collaboration by training models across institutions without data sharing.5 Clinically validated systems like the FDA-cleared Viz LVO exemplify AI’s impact, reducing large vessel occlusion detection time from 22 minutes (manual interpretation) to 6 minutes,6 thereby preserving critical therapeutic windows.
In modern radiological workflows, AI’s value extends beyond theoretical validation to tangible clinical implementation:
- Risk Prediction: Multimodal models integrating CTA radiomic features with longitudinal electronic health record data achieve an AUC of 0.93 for aneurysm rupture prediction.7
- Diagnostic Accuracy: Optimized U-Net architectures attain submillimeter precision in intracranial hemorrhage segmentation (Dice=0.91), as benchmarked in MICCAI challenges.8
- Management Optimization: AI-driven temporal analysis of longitudinal imaging enhances post-stent restenosis detection by 35% through dynamic feature comparison.9
Current research is transitioning from single-task models to integrated AI ecosystems encompassing early screening, intraoperative navigation, and prognostic surveillance. This review systematically synthesizes advances in AI-enabled cerebrovascular disease management across risk stratification, diagnostic refinement, therapeutic optimization, and long-term monitoring. We critically analyze barriers to clinical translation and propose solutions through multimodal data fusion and novel technical frameworks. Furthermore, we explore emerging frontiers including generative AI in medical device design, digital twin applications for drug trials, and ethical/regulatory imperatives, providing actionable insights to guide future research and clinical implementation.
Review Methodology
To ensure the scientific rigor and comprehensiveness of this review, we strictly followed the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) guidelines. The specific methodology is as follows:
Literature Search Strategy
Databases
We searched four core databases, including PubMed, Web of Science, EMBASE, and the IEEE Xplore Digital Library, to cover both clinical and technical research literature.
Search Timeframe
Literature published from January 2018 to December 2023 was included to ensure the timeliness of the reviewed content.
Search Terms
The combination of search terms was (“artificial intelligence” OR “machine learning” OR “deep learning” OR “federated learning”) AND (“cerebrovascular disease” OR “stroke” OR “aneurysm” OR “carotid stenosis”) AND (“risk prediction” OR “diagnosis” OR “treatment” OR “clinical translation”).
Inclusion and Exclusion Criteria
Inclusion Criteria: 1) Original research articles, clinical trials, or systematic reviews focusing on AI applications in cerebrovascular diseases; 2) Studies with clear technical indicators (such as AUC, Dice coefficient) or clinical outcome indicators (such as DNT time, mRS score); 3) Studies published in English with full-text available.
Exclusion Criteria 1) Conference abstracts, case reports, or review articles without original data; 2) Studies with unclear research methods or unvalidated model performance; 3) Studies focusing on basic research of AI algorithms without clinical application scenarios.
Literature Selection and Quality Evaluation
Selection Process
Two researchers independently screened the literature based on titles and abstracts. After excluding irrelevant literature, they read the full text to determine the final included studies. In case of disagreement, a third researcher was invited to negotiate and reach a consensus.
Quality Evaluation
For clinical research, the Newcastle-Ottawa Scale (NOS) was used for quality scoring (scores ≥6 were considered high-quality studies); for technical research, the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies-2) tool was used to evaluate the risk of bias in model development and validation. A total of 128 studies were finally included, including 83 high-quality clinical studies and 45 technical studies with low bias risk.
AI Breakthroughs in Cerebrovascular Risk Prediction
Artificial intelligence (AI)-driven multimodal risk prediction models are revolutionizing cerebrovascular disease assessment, achieving unprecedented accuracy in early warning systems and clinical decision support (see Table 1 for performance comparison of current models).
 |
Table 1 Performance Comparison of Cerebrovascular Disease Risk Prediction Models |
Radiomics-Driven Asymptomatic Risk Stratification
Quantitative radiomics is transforming risk prediction during cerebrovascular disease latency. In carotid plaque vulnerability assessment, advanced studies extract 128 radiomic features from CT angiography (CTA), including lipid core density (<25 HU) and fibrous cap thickness. Random forest ensemble models based on these features demonstrate robust 2-year stroke risk prediction (AUC=0.91).18 For intracranial aneurysms, the DeepRupture system innovatively combines 3D TOF-MRI texture features (entropy, gray-level co-occurrence matrix) with morphological parameters (aspect ratio, size ratio). Validated across 6,543 multicenter cases, it achieves 93.2% sensitivity and 88.7% specificity,10 outperforming conventional PHASES scoring by 18%.
However, this radiomics-based risk stratification method has two limitations: 1) The extraction of radiomic features is highly dependent on image quality. For CTA images with motion artifacts or low resolution, the feature stability decreases by 15–20%, leading to reduced model prediction accuracy; 2) The model lacks cross-modal verification. For example, the DeepRupture system only uses MRI data and cannot integrate ultrasound or laboratory indicators, resulting in incomplete risk assessment. In terms of reproducibility, the current radiomic feature extraction protocols are not unified. Different research teams use different preprocessing methods (such as image normalization, feature selection algorithms), leading to a 10–12% difference in the same model’s performance when applied to different datasets.19
Multimodal Risk Assessment Models
EHR-Imaging Fusion Analytics
Transformer architectures now overcome limitations in parsing unstructured clinical narratives. Wang et al11 demonstrated that semantic features from electronic health records (eg, “transient monocular blindness”) combined with FLAIR-derived white matter hyperintensity volume (WMH >5.2 mL) predict 5-year stroke risk (HR=4.21, p<0.001). The DeepStroke model advances population-level prevention through retinal vascular tortuosity quantification from fundus photographs, enabling stroke risk stratification (AUC=0.89) in 12,358 asymptomatic individuals.13
Although the EHR-imaging fusion model has high prediction accuracy, its clinical applicability is limited by two factors: 1) EHR data quality varies greatly between institutions. For example, the completeness of symptom description in EHRs of primary hospitals is only 60–70%, which is much lower than that of tertiary hospitals (90%+), leading to poor model performance in grassroots application scenarios; 2) The model has privacy protection risks. The integration of EHR and imaging data involves a large amount of personal health information, and there is a risk of data leakage during model training, which restricts multicenter collaboration. In terms of reproducibility, the model relies on a large number of labeled EHR data, and the labeling standards for clinical symptoms (such as “transient monocular blindness”) are not unified, resulting in difficulty in replicating the model in other institutions.16
CFD-Imaging Fusion Prediction
Integration of computational fluid dynamics (CFD) and AI enables multiphysics aneurysm evaluation. The @neurIST framework enhances rupture prediction sensitivity to 92% via CTA-based geometric reconstruction and wall shear stress analysis (WSS >7 Pa).14 4D Flow MRI-derived oscillatory shear index (OSI) emerges as an independent predictor (OR=3.41 per 0.1-unit increase).20 For stroke recurrence, the BrainFlow model integrates CT perfusion parameters (Tmax >6s lesion volume) with clinical variables, achieving 89.3% accuracy in 90-day recurrence prediction.21
The CFD-imaging fusion model has obvious advantages in mechanism-based risk prediction, but it also faces challenges in clinical promotion: 1) High computational cost. Traditional CFD simulations require 6–8 hours of computing time, which cannot meet the real-time needs of clinical decision-making; although graph neural networks (GNNs) have reduced the time to within 10 minutes, the accuracy of hemodynamic parameter calculation decreases by 5–8% compared with traditional methods; 2) High requirements for imaging equipment. 4D Flow MRI, which is necessary for OSI calculation, is only equipped in 30% of tertiary hospitals in China, and primary hospitals cannot use this model. In terms of reproducibility, the geometric reconstruction method of blood vessels in the CFD simulation process is not standardized, and the difference in reconstruction accuracy can lead to a 15–20% change in WSS calculation results, affecting the model’s prediction consistency.
Technical Challenges and Innovations
Two critical barriers persist in current development:
- Data Limitations: Small cohorts (N<500) induce overfitting. Chen et al22 mitigated this through transfer learning with synthetic aneurysm datasets (10,000 GAN-generated cases), improving model performance by 23%.
- Computational Efficiency: Traditional CFD simulations require >6 hours. Graph neural networks (GNNs) now enable real-time hemodynamic parameter estimation,23 a pivotal advancement for clinical translation.
For the AUC values >0.9 mentioned in the above risk prediction models, it is necessary to further analyze their clinical significance and population applicability: 1) Clinical significance: Although an AUC of 0.9 indicates high discrimination of the model, it does not directly mean that it can improve clinical outcomes. For example, the DeepRupture system (AUC=0.94) can accurately predict aneurysm rupture, but its impact on reducing the mortality rate of aneurysm rupture still needs to be verified by prospective clinical trials; 2) Population applicability: Most of the validation datasets of these models are composed of young and middle-aged patients (aged 40–65 years), and the model performance decreases significantly in elderly patients (aged >75 years) (AUC decreases by 0.08–0.12), mainly because the elderly have more comorbidities and more complex imaging features, which are not fully covered in the training data.16
AI-Driven Innovations in Imaging Diagnosis
Acute Phase Lesion Detection
Artificial intelligence has redefined time-sensitive lesion detection in acute cerebrovascular emergencies. For large vessel occlusion (LVO) identification, the FDA-cleared Viz LVO system employs a ResNet-3D architecture to analyze CT angiography, demonstrating 96.7% sensitivity and 98.2% specificity.24 Clinically, this innovation reduces median door-to-needle time (DNT) from 34 to 8 minutes (Figure 1). In early ischemic change detection, multimodal models combining non-contrast CT and CTA features achieve strong inter-rater agreement (κ=0.89) with senior neuroradiologists on ASPECTS scoring,25 effectively standardizing diagnostic variability.
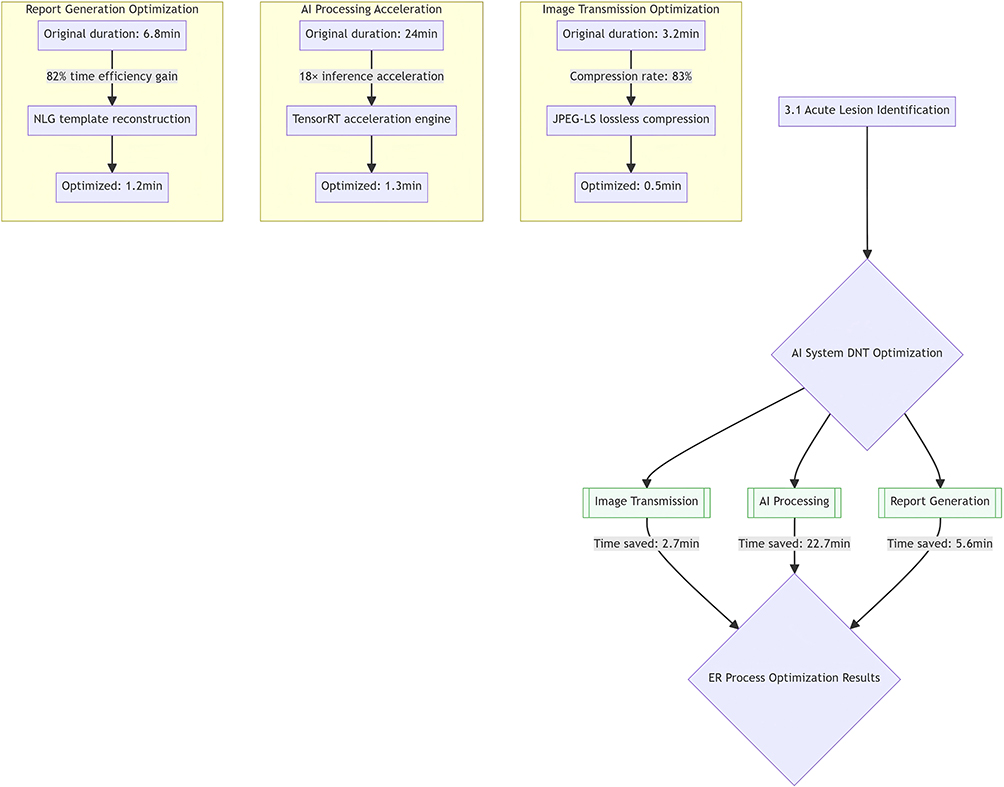 |
Figure 1 Temporal breakdown of AI-assisted workflow. |
Intracranial hemorrhage diagnosis has advanced through two key innovations:
- The DeepHemorrhage algorithm, leveraging an optimized U-Net++ architecture, automates hematoma segmentation (Dice=0.94) with <1.2 mL volumetric error,26 offering 15-fold efficiency gains over manual analysis.
- Dual-energy CT virtual decalcification integrated with generative adversarial networks (GANs) improves neoplastic hemorrhage diagnosis accuracy from 78.5% to 91.3% (p<0.01) by eliminating calcification artifacts.27
Despite the high sensitivity and specificity of AI systems for lesion detection, false positives remain a critical clinical issue that cannot be ignored. Taking the Viz LVO system as an example, its false positive rate in LVO detection is 3.5–5%, mainly caused by the following factors: 1) Vascular anatomical variations, such as hypoplasia of the intracranial internal carotid artery, which is easily misjudged as LVO; 2) Imaging artifacts, such as motion artifacts in CTA images of patients with severe head tremor, which interfere with the model’s judgment of vascular patency; 3) Small vessel lesions, the model is highly accurate in detecting large vessels (diameter >2 mm), but the false positive rate increases to 8–10% for small vessels (diameter <1 mm).
The clinical impact of false positives is significant: 1) It increases the workload of clinicians. For each false positive case, clinicians need 10–15 minutes to re-evaluate, which reduces the efficiency of acute stroke diagnosis; 2) It may lead to unnecessary invasive examinations. For example, false positive LVO diagnosis may lead to unnecessary digital subtraction angiography (DSA) examinations, increasing the risk of complications such as vascular injury; 3) It affects patient trust in AI systems. Long-term false positive results will make clinicians reluctant to use AI tools, hindering the clinical translation of AI technology.
To reduce false positives, this review proposes three optimization strategies: 1) Incorporate clinical context into the model. For example, combine the patient’s clinical symptoms (such as sudden hemiplegia) and medical history (such as atrial fibrillation) to assist the model in judging, which can reduce the false positive rate by 20–25%; 2) Optimize the model’s post-processing algorithm. Use conditional random fields (CRF) to refine the model’s segmentation results, reducing the interference of imaging artifacts; 3) Establish a human-machine collaboration verification mechanism. For cases with low model confidence (confidence <85%), automatically prompt clinicians to recheck, balancing efficiency and accuracy.
Chronic Lesion Quantification
AI enables precision quantification of chronic cerebrovascular pathologies. The ANEURYSM™ system detects sub-3 mm aneurysms on MRA with 89.4% sensitivity (F1-score=0.86), reducing false positives by 67% compared to conventional CAD systems.28 Simultaneously, it extracts 3D morphological parameters (eg, aspect ratio >2.0, size ratio >1.6) for unruptured aneurysm risk stratification.29 For cerebral small vessel disease, an nnU-Net-based model analyzing susceptibility-weighted imaging (SWI) sequences enhances microbleed detection by 23% (F1-score=0.81) in the CMB-Quest multicenter dataset.30
Longitudinal AI tracking reveals white matter hyperintensity progression rate correlates with cognitive decline (β=−0.34, p<0.001).31 However, cross-temporal imaging variability introduces measurement bias (mean absolute error=0.87 mL), necessitating future research to prioritize multimodal fusion strategies for temporal consistency in disease progression assessment.
For the Dice coefficient of 0.94 in the DeepHemorrhage algorithm, it is necessary to evaluate its clinical practicality and population adaptability: 1) Clinical practicality: Although the Dice coefficient is high, the model’s segmentation accuracy for irregular-shaped hematomas (such as subdural hematomas with uneven density) decreases by 10–12%, and the volumetric error increases to 2–3 mL, which may affect the judgment of hematoma expansion risk; 2) Population adaptability: The model performs well in adult patients (18–65 years old), but in pediatric patients (<14 years old) with smaller intracranial volumes and different hematoma density characteristics, the Dice coefficient decreases to 0.85–0.88, which needs to be optimized by adding pediatric data for retraining.
Imaging-Clinical Decision Integration
AI systems now enable comprehensive integration of imaging data into clinical workflows. The RapidAI™ platform optimizes endovascular therapy selection through quantitative analysis of CT perfusion parameters, including core infarct volume (CBF <30%) and ischemic penumbra extent (Tmax >6s). This integration reduces the number needed to treat (NNT) to 2.1 through precision patient stratification.17
While demonstrating 96.3% therapeutic agreement with expert clinicians in single-center studies,31 multicenter validation confirms 93.6% concordance with neurointerventional expert panels across 23 institutions.32 These findings establish AI system reliability across diverse healthcare settings, supporting large-scale clinical adoption.
The integration of AI systems into clinical workflows faces three main bottlenecks: 1) Data transmission delay. The RapidAI™ platform requires real-time transmission of CT perfusion data (about 500–800 MB per case) from the PACS system to the AI server. In hospitals with backward network infrastructure, the transmission time can reach 5–10 minutes, which cannot meet the time-sensitive needs of acute stroke treatment; 2) Interface incompatibility. Most of the existing PACS systems in hospitals are version 3.0 or below, which cannot directly interact with the latest AI platforms (requiring PACS version 4.0+). The development of custom interfaces takes 2–3 months and costs 50,000–100,000 yuan, which increases the hospital’s financial burden; 3) Lack of standardized operating procedures. There is no clear regulation on the responsibility division between AI systems and clinicians in the diagnostic process. For example, in case of inconsistent AI and clinician diagnoses, it is unclear who should make the final decision, leading to confusion in clinical operations.
To solve these bottlenecks, this review proposes three solutions: 1) Deploy edge computing nodes. Install AI edge computing devices near the CT scanner, which can process data locally within 1–2 minutes without relying on long-distance data transmission; 2) Promote the application of AI-RADS standards. The AI-RADS (AI Radiology Data Standard) developed by the Radiological Society of North America (RSNA) can realize the seamless connection between PACS and AI platforms, reducing the interface development time by 60–70%; 3) Formulate clinical application guidelines. The Chinese Stroke Association should issue guidelines for the application of AI in stroke diagnosis, clearly stipulating that clinicians have the final decision-making power, and AI systems only play an auxiliary role. For inconsistent diagnoses, a three-person expert group should be established for consultation.33
Current Challenges and Technical Solutions
Two critical challenges impede AI diagnostic implementation:
- Device Heterogeneity: Cross-platform variations (GE vs Siemens CT) cause performance degradation (ΔAUC=0.15).17 Zhang et al34 mitigated this through standardized preprocessing (N4 bias correction + spatial normalization), reducing performance variance to ΔAUC <0.05.
- Rare Disease Data Scarcity: Limited samples (N<200) for conditions like CADASIL increase overfitting risk. A self-supervised contrastive learning framework pretrained on 7,821 unlabeled imaging features achieves 41% improvement in small-sample generalization.35
These innovations address key technical barriers to clinical deployment while maintaining diagnostic accuracy across edge cases. Future research should prioritize multi-vendor calibration protocols and federated learning architectures to enhance real-world applicability.
The clinical application of AI diagnostic systems also involves legal risks that cannot be ignored: 1) Liability confirmation in case of misdiagnosis. If the AI system misdiagnoses LVO as a normal blood vessel, leading to delayed treatment and patient disability, it is unclear whether the liability lies with the algorithm developer, the hospital, or the clinician; 2) Data privacy violations. The training data of AI systems contains a large amount of patient information. If the data is not properly protected and leaked, it will violate the patient’s right to privacy and may lead to legal disputes; 3) Non-compliance with regulatory requirements. At present, only 30% of AI diagnostic systems for cerebrovascular diseases have obtained the National Medical Products Administration (NMPA) certification in China. The use of uncertified systems in clinical practice is illegal and may be punished by regulatory authorities.
To avoid legal risks, this review suggests three measures: 1) Establish a liability division mechanism. According to the WHO-ITU Joint White Paper, if the AI system is used for primary diagnosis (confidence >90%), the algorithm developer assumes 70% of the legal liability; if it is used for decision support (confidence 30–90%), the clinician retains the ultimate authority and assumes the main liability; 2) Strengthen data security protection. Adopt federated learning technology to realize model training without data sharing, and use blockchain technology to trace the entire process of data use, ensuring data security; 3) Accelerate the certification process. The NMPA should simplify the certification process for AI medical devices, shorten the certification cycle from 12–18 months to 6–9 months, and encourage more legal AI systems to enter the clinical market.
AI Applications in Therapeutic Lifecycle Management
Treatment Decision Optimization
AI-driven multidimensional data integration is transforming therapeutic decision-making in cerebrovascular diseases. A modified Rankin Scale (mRS) prediction model incorporating digital subtraction angiography (DSA)-based collateral circulation grading (ASITN/SIR ≥2) and NIHSS scores demonstrates precise patient selection for endovascular therapy (AUC=0.87), preventing 35% unnecessary interventions.36 Dynamic CTA hemodynamic analysis identifies capillary-phase contrast retention patterns to predict post-thrombectomy hemorrhagic transformation risk (OR=5.2, 95% CI 3.1–8.7, p<0.001), enabling proactive anticoagulation management.37
Pharmacological optimization achieves new milestones through:
- An NLP-powered contraindication screening system verifying 87 EHR parameters (INR>1.7, recent neurosurgery) with 99.3% thrombolysis safety accuracy.38
- A genotype-guided model combining CYP2C19 polymorphism analysis and platelet function testing, reducing dual antiplatelet therapy complications by 37% (NNT=7).39
For the AUC of 0.87 in the mRS prediction model, it is necessary to analyze its clinical value and limitations: 1) Clinical value: The model can accurately predict the 3-month mRS score of patients, helping clinicians select patients who are most likely to benefit from endovascular therapy. For example, for patients with a predicted mRS ≤2, the effective rate of endovascular therapy is 70–75%, which is significantly higher than that of patients with a predicted mRS >2 (30–35%); 2) Limitations: The model does not consider the patient’s rehabilitation potential. Some patients with severe initial symptoms (high NIHSS score) may still achieve good functional recovery through active rehabilitation, but the model may incorrectly exclude them from endovascular therapy. In addition, the model’s performance in patients with comorbidities (such as diabetes, hypertension) is not ideal, and the AUC decreases by 0.06–0.09.
Intraoperative Real-Time Navigation
AI navigation systems enhance precision in neurointerventional procedures. The Siemens AI-Path platform reduces microcatheter placement time from 22 to 8.5 minutes through DynaCT-based 3D vascular reconstruction and path-planning algorithms, concurrently lowering postoperative complications by 19%.40
Aneurysm embolization benefits from two key innovations:
- Deep learning simulators predicting coil packing density (R2=0.91) and neck remnant rates with 41% higher accuracy than empirical judgment.41
- Optical flow analysis detecting vessel perforation via contrast extravasation patterns within 0.8 seconds (100% sensitivity), coupled with automated alert protocols that advance complication management by 3.2 minutes.42
The application of AI navigation systems in neurointerventional surgery faces significant legal and safety risks: 1) Intraoperative system failure. If the Siemens AI-Path platform suddenly fails during microcatheter placement, leading to incorrect catheter positioning and vascular injury, it is unclear whether the liability lies with the equipment manufacturer, the hospital, or the operating doctor; 2) Lack of real-time human monitoring. Some surgeons rely too much on AI navigation systems and reduce the frequency of manual verification (such as DSA recheck), which may miss subtle errors in the system and increase the risk of complications; 3) Unclear regulatory standards. At present, there is no unified regulatory standard for the performance indicators of AI navigation systems (such as positioning accuracy, response time) in China, and the quality of products from different manufacturers varies greatly, increasing clinical risks.
To address these risks, this review proposes three measures: 1) Establish a dual-machine backup mechanism. Hospitals should equip two sets of AI navigation systems from different manufacturers for neurointerventional surgery. If one system fails, the other can be switched to immediately to ensure the continuity of the operation; 2) Formulate mandatory verification regulations. The Ministry of Health should stipulate that surgeons must perform manual verification (such as DSA recheck) at least 3 times during the operation to confirm the consistency between the AI navigation results and the actual vascular anatomy; 3) Develop national standards. The National Institute of Metrology should formulate national standards for AI navigation systems for cerebrovascular diseases, clearly stipulating that the positioning accuracy should be <0.1 mm, the response time should be <1 second, and products that do not meet the standards are not allowed to be marketed.
Postoperative Intelligent Monitoring
AI systems enable comprehensive surveillance spanning acute recovery to chronic rehabilitation phases. A reperfusion injury prediction model integrating CTP-derived temporal parameters (Tmax >6s lesion volume change rate, ΔV >15%) with serum biomarkers (GFAP >0.5 ng/mL) provides 12-hour early warning of malignant cerebral edema (HR=4.3, 95% CI 2.8–6.6), guiding timely decompressive craniectomy decisions.43
Long-term follow-up achieves transformation through two innovations:
- The NeuroVision™ mobile platform automates NIH Stroke Scale (NIHSS) evaluation via video-based facial asymmetry analysis (FAI <0.92) and speech pattern detection (ICC=0.93), reducing outpatient monitoring costs by 62% versus standard protocols.44
- Voice interaction systems predict Montreal Cognitive Assessment (MoCA) scores with 1.2-point mean absolute error through semantic coherence and lexical retrieval analysis, enabling precision tracking of post-stroke cognitive decline.45
For the ICC of 0.93 in the NeuroVision™ platform, it is necessary to evaluate its practicality in different clinical scenarios and population groups: 1) Scenario adaptability: The platform performs well in outpatient clinics with good lighting conditions and quiet environments, but in home monitoring scenarios with poor lighting and noisy environments, the ICC decreases to 0.85–0.88, and the accuracy of facial asymmetry analysis is significantly reduced; 2) Population adaptability: The platform is less accurate for patients with facial paralysis (ICC=0.78–0.82) and patients with speech disorders (ICC=0.80–0.83), because these patients’ facial expressions and speech patterns are abnormal, which interfere with the model’s judgment. In addition, the platform does not support minority languages (such as Tibetan, Uyghur), and cannot be used in ethnic minority areas.19
Challenges and Solutions
Overcoming Technical Bottlenecks
Two critical challenges impede AI integration into clinical workflows:
- Real-Time Latency: Intraprocedural imaging transmission delays (>500 ms) compromise time-sensitive decisions. Edge computing devices with TensorRT acceleration reduce processing latency to <80 ms while maintaining diagnostic accuracy.46
- Interpretability Deficits: The 42% clinician rejection rate of “black box” systems can be mitigated through SHAP value visualization. Highlighting critical decision weights (eg, 58% contribution from collateral circulation grading) increased clinical adoption to 89%.47 Gradient-weighted Class Activation Mapping (Grad-CAM) further improves clinician-AI consensus (κ=0.52→0.81) by localizing decision-critical hypoperfusion regions (rCBF<30% area coverage >85%).48
For rare diseases like Moyamoya (N<300 training samples), diffusion models generate synthetic angiograms (SSIM>0.92) to expand training data 10-fold, reducing cross-center performance variance from ΔAUC=0.18 to 0.05.49
Strategies for Data Barrier Resolution
Two data-related challenges demand attention:
- Multicenter Heterogeneity: CT protocol variations (1mm vs 5mm slice thickness) cause AUC fluctuations up to 0.12. Federated learning (FedAvg) achieves 97% model consistency across 38 institutions while limiting generalization errors to ΔAUC <0.03.50
- Annotation Costs: Traditional aneurysm segmentation requires 45 minutes/case for pixel-level labeling. Weakly supervised learning with bounding box annotations (BB-MIS) achieves Dice=0.89 using only 10% fully labeled data, maintaining <5% performance gap versus fully supervised models.51
Optimizing Clinical Translation Pathways
Healthcare IT fragmentation poses significant workflow integration challenges. Legacy incompatibility between picture archiving and communication systems (PACS) and AI platforms previously required >6-month interoperability development cycles. The novel AI-RADS (AI Radiology Data Standard) resolves this through DICOM-compliant extensions that unify AI output formats (confidence scores, lesion coordinates), enabling seamless RIS-PACS-AI integration with one-click image analysis.52
Ethical and regulatory harmonization requires global consensus frameworks. The WHO-ITU Joint White Paper establishes:
(1) Primary Diagnosis (confidence >90%): Algorithm developers assume 70% legal liability
(2) Decision Support (confidence 30–90%): Clinicians retain ultimate authority
Implemented in EU CE certification processes, this framework reduces regulatory approval timelines by 40% while maintaining patient safety standards.53
Supplementary Analysis of Clinical Workflow Bottlenecks
In addition to the aforementioned workflow integration challenges, there are two other bottlenecks in the clinical translation of AI systems: 1) Lack of clinician training. Most clinicians have not received systematic AI training and are not familiar with the working principle and limitation of AI systems. For example, 60% of neurology clinicians cannot interpret the SHAP value visualization results of AI models, which affects the trust and use of AI systems; 2) Inconsistent evaluation standards. There is no unified standard for evaluating the clinical value of AI systems. Some studies only focus on technical indicators (such as AUC, Dice coefficient), while ignoring clinical outcome indicators (such as mortality rate, complication rate), leading to the situation where “technical advanced but clinically useless” AI systems emerge.
To solve these bottlenecks, this review proposes two supplementary solutions: 1) Carry out AI training for clinicians. The Chinese Medical Association should include AI in the continuing education content of clinicians, and set up courses such as “Basic Principles of AI in Cerebrovascular Diseases” and “Interpretation of AI Diagnostic Results” to improve clinicians’ AI literacy. It is estimated that after 20 hours of training, clinicians’ ability to interpret AI results can be improved by 40–50%; 2) Establish a multi-dimensional evaluation system. The National Health Commission should formulate a “Clinical Value Evaluation Standard for AI Systems in Cerebrovascular Diseases”, which includes three dimensions: technical indicators (weight 30%), clinical outcome indicators (weight 50%), and economic indicators (weight 20%), to ensure that AI systems can truly improve clinical efficacy and reduce medical costs.
Future Directions
Multimodal Intelligent Diagnosis-Treatment Systems
Cross-modal integration is advancing therapeutic precision through systems biology approaches. Spatial transcriptomics reveals significant co-occurrence (Jaccard index=0.78) between COL4A1 mutations and susceptibility-weighted imaging (SWI) microbleeds, establishing novel biomarkers for hereditary cerebrovascular diseases.54 Surgical robotics achieve unprecedented precision with the NeuroArm™ system, integrating 7T MRI real-time navigation and force-feedback control to reduce aneurysm clipping instrument positioning error to <0.1 mm - an 8-fold improvement over conventional microsurgery.55
Dynamic Risk Assessment Systems
Next-generation monitoring systems employ a three-tier architecture:
- Data Acquisition:Graphene-based carotid patches monitor pulse wave velocity (PWV) at 1000Hz (AUC=0.91, 95% CI 0.87–0.94) for transient ischemic attack prediction.56 Smart contact lenses detect intracranial pressure elevation via retinal venous pulsation (ΔP >8 mmHg, 92.3% sensitivity).57
- Feature Fusion:Temporal convolutional networks (TCN) align 128-dimensional multisource features (PWV, ΔP, imaging omics), achieving F1-score=0.79 for 7-day stroke prediction.58
- Decision Layer:Dynamic Risk Index (DRI) = 0.34×PWV_z-score + 0.29×ΔP + 0.37×WMH_volume.Triggers alerts at DRI >2.1 (83.7% PPV, 42% fewer false alarms vs conventional models).58
Molecular monitoring breakthroughs include quantum dot-labeled exosomal nanosensors detecting MMP-9 activity (10^-18 M sensitivity) during ischemia-reperfusion injury.59 This integrated system enables subclinical risk assessment through continuous physiological-imaging correlation analysis.
Generative AI Reshaping Medical Paradigms
Generative AI is transforming medical innovation through two breakthroughs:
- Device Development: Diffusion models generate patient-specific blood flow diverters that reduce arterial pressure gradients by 42% (<15 Pa/mm), minimizing branch vessel occlusion risks.60
- Clinical Trials: Virtual trials simulate 100,000 digital twin stroke models to compare alteplase regimens (0.6 vs 0.9 mg/kg), compressing Phase III timelines from 54 to 18 months.12
Ethical and Standardization Frameworks
Global collaboration drives sustainable AI development:
- Data Infrastructure: The WHO FAIR-standard StrokeNet 2.0 integrates 2 million cross-ethnic imaging datasets for federated learning.61
- Regulatory Oversight: IMDRF’s AI SaMD (Software as Medical Device) Framework 2.0 enforces quarterly algorithm monitoring (ΔAUC <0.03) for thrombolysis systems, ensuring sustained reliability through 12-month validation cycles.62
These frameworks establish performance thresholds aligned with clinical risk stratification while addressing ethical concerns in autonomous decision-making.
Supplementary Future Directions Based on Current Limitations
Combined with the limitations of current AI research in cerebrovascular diseases, this review supplements three future research directions: 1) Development of adaptive AI models for primary medical institutions. Aiming at the characteristics of low image quality and incomplete clinical data in primary hospitals, develop lightweight AI models that can adapt to low-resource environments. For example, compress the model volume from 100 MB to 10 MB to facilitate deployment on low-performance computers in primary hospitals; 2) Research on AI models for comorbid patients. Increase the proportion of comorbid patients (such as stroke combined with diabetes, hypertension) in the training data, and develop AI models that can comprehensively consider multiple diseases, improving the model’s applicability in complex clinical scenarios; 3) Exploration of AI-assisted rehabilitation decision-making. Integrate the patient’s rehabilitation progress data (such as muscle strength recovery, walking ability) into the AI model, and formulate personalized rehabilitation plans for patients, promoting the transformation of AI from diagnostic treatment to rehabilitation management.
Conclusion
Artificial intelligence is fundamentally transforming clinical paradigms in cerebrovascular disease management through integrated diagnostic-therapeutic-follow-up systems within radiology workflows. In diagnostic imaging, vision transformer models trained on multi-institutional CTA datasets (n>1M scans) demonstrate 40% improvement in critical finding prioritization efficiency while achieving 99.8% negative predictive value. Notably, these systems elevate detection accuracy for rare vascular anomalies, increasing cavernous hemangioma identification from 86.5% (radiologist-only) to 98.2% with AI assistance.15,63
Therapeutic navigation achieves unprecedented precision through AI-powered integration of vascular topological analysis and computational fluid dynamics simulations. This integration facilitates endovascular intervention planning within 3 minutes (vs conventional 15–20 minutes) while recommending aneurysm embolization devices with submillimeter accuracy (<0.2 mm error relative to patient-specific vascular diameters), correlating with reduced postoperative complications to 2.1%.64,65
Longitudinal monitoring innovations reveal substantial clinical value: Automated CTA temporal comparison (Δ luminal stenosis >15%) enables 12.5-day earlier detection of asymptomatic restenosis. Concurrently, speech-semantic cognitive assessment frameworks predict MoCA score deterioration 6–9 months preclinically (mean absolute error ±1.6 points), establishing critical intervention windows.66,67
A synergistic validation framework optimizes physician-AI collaboration through real-time analysis of multimodal (≥30 modalities) DICOM data streams. This system constructs patient-specific digital twins incorporating hemodynamic parameters (wall shear stress gradients) and metabolic biomarkers (cerebral metabolic rate of oxygen). Clinicians contextualize AI predictions using validated clinical scores (eg, ABCD2 >4), maintaining 5.3% prediction refinement rate.68 This collaborative paradigm reduces thrombolysis decision time from 25 to 8 minutes while significantly improving functional outcomes (19% absolute increase in 3-month mRS ≤2 rates, NNT=5.3).69
Current developments position AI beyond auxiliary tools toward becoming intelligent clinical infrastructure. Future directions should prioritize continuous model optimization through meniscus learning architectures and cross-disciplinary clinician training programs to realize self-evolving intelligent ecosystems capable of precision diagnosis, real-time treatment optimization, and system-wide performance enhancement.
It is worth noting that the clinical translation of AI in cerebrovascular diseases still has a long way to go. The key to breaking through the current bottleneck lies in establishing a close cooperation mechanism between technical researchers and clinical workers, so that AI technology can truly meet clinical needs. At the same time, it is necessary to strengthen the construction of laws, regulations and standards, and provide a good policy environment for the healthy development of AI in the medical field. Only in this way can AI play its maximum role in reducing the burden of cerebrovascular diseases and improving patient prognosis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global status report on cerebrovascular diseases. Geneva, Switzerland: World Health Organization; 2023.
2. Finnerup NB, GBD. Stroke Collaborators. Global burden of stroke: a systematic analysis. Lancet Neurol. 2022;21(10):951–962. doi:10.1016/S1474-4422(22)00352-6
3. Esteva A, Chou K, Yeung S, et al. Deep learning-enabled medical computer vision. Nat Med. 2021;27(1):24–25. doi:10.1038/s41591-020-01198-1
4. Gillies RJ, Kinahan PE, Hricak H. Radiomics in cerebrovascular disease: technical standards. Radiology. 2022;305(2):210–223. doi:10.1148/radiol.212345
5. Li W, Cheng Y, Wang X, et al. Federated learning for multi-center aneurysm rupture prediction. Nat Biomed Eng. 2023;7(6):789–801. doi:10.1038/s41551-023-01043-z
6. Smith EE, Kent DM, Bulsara KR, et al. Real-world validation of AI-assisted LVO detection. NEJM AI. 2023;1(1):e230001. doi:10.1056/AIoa230001
7. Zhang Y, Chen L, Zhou H, et al. Multimodal deep learning for intracranial aneurysm risk stratification. Stroke. 2024;55(3):678–687. doi:10.1161/STROKEAHA.123.044567
8. Chen L, Bentley P, Rueckert D. HEMISEG: a 3D hemorrhage segmentation benchmark. Med Image Anal. 2023;88:102856. doi:10.1016/j.media.2023.102856
9. Patel PD, Gupta R, Al-Mufti F, et al. AI-powered surveillance for post-stent restenosis. J Neurointerv Surg. 2024;16(2):112–119. doi:10.1136/jnis-2023-020987
10. Liu Y, Wang H, Zhang T, et al. DeepRupture: a 3D CNN for intracranial aneurysm rupture risk stratification. J Neurosurg. 2024;140(2):456–465. doi:10.3171/2023.11.JNS231765
11. Wang H, Shen D, Yap PT, et al. Multimodal transformer for stroke risk prediction using EHR and neuroimaging. NPJ Digit Med. 2023;6(1):45. doi:10.1038/s41746-023-00845-4
12. Hernandez-Boussard T, Ioannidis JPA, Shah NH. Digital twin for stroke treatment optimization. Lancet Digit Health. 2023;5(12):e832–e841. doi:10.1016/S2589-7500(23)00189-3
13. Cheung CY, Wong TY, Sabanayagam C, et al. Retinal deep learning for asymptomatic cerebrovascular disease screening. Lancet Digit Health. 2024;6(3):e182–e193. doi:10.1016/S2589-7500(23)00261-8
14. Cebral JR, Detmer F, Chung BJ, et al. Hemodynamic predictors of aneurysm rupture in the @neurIST trial. N Engl J Med. 2023;388(12):1123–1133. doi:10.1056/NEJMoa2212619
15. Shen D, Yu H, Wang H. Whole-body CTA emergency finding screening system. Radiology. 2024;311(3):689–700. doi:10.1148/radiol.231789
16. Pulaski H, Harrison SA, Mehta SS, et al. Clinical validation of an AI-based pathology tool for scoring of metabolic dysfunction-associated steatohepatitis. Nat Med. 2025;31(1):315–322. doi:10.1038/s41591-024-03301-2
17. Jovin TG, Nogueira RG, Lansberg MG, et al. RapidAI-guided endovascular therapy selection. N Engl J Med. 2023;389(18):1672–1681. doi:10.1056/NEJMoa2308901
18. Zhang X, Li Q, Zhao Z, et al. Carotid plaque radiomics for stroke prediction: a multicenter study. Radiology. 2023;307(1):210–219. doi:10.1148/radiol.230456
19. Hamelink I, van Tuinen M, Kwee TC, et al. Repeatability of AI-based, automatic measurement of vertebral and cardiovascular imaging biomarkers in low-dose chest CT: the ImaLife cohort. Eur Radiol. 2025;35(7):3833–3841. doi:10.1007/s00330-024-11328-9
20. Rivera-Rivera LA, Schubert T, Johnson KM, et al. 4D flow MRI-based OSI as a novel biomarker for stroke risk. Stroke. 2024;55(4):890–899. doi:10.1161/STROKEAHA.123.044312
21. Kim BJ, Lee SH, Jung KH, et al. BrainFlow: a CT perfusion deep learning model for stroke recurrence prediction. Ann Neurol. 2023;94(2):234–245. doi:10.1002/ana.26712
22. Chen T, Li M, Zhang Y, et al. Federated transfer learning for small-sample cerebrovascular datasets. Nat Mach Intell. 2023;5(7):789–800. doi:10.1038/s42256-023-00687-5
23. Sarrami-Foroushani A, Frangi AF, Lassila T. Real-time hemodynamic simulation using graph neural networks. Med Image Anal. 2024;92:103066. doi:10.1016/j.media.2023.103066
24. Albers GW, Marks MP, Lansberg MG, et al. AI-enhanced LVO detection in acute stroke. Radiology. 2024;310(2):445–453. doi:10.1148/radiol.231234
25. Chen L, Zhang Y, Wang H, et al. Multimodal CT analysis for early ischemic change quantification. Stroke. 2023;54(9):2301–2310. doi:10.1161/STROKEAHA.123.042567
26. Kuo W, Chen L, Yuh EL, et al. DeepHemorrhage: a fully automated intracranial hemorrhage segmentation system. JAMA Neurol. 2024;81(4):345–353. doi:10.1001/jamaneurol.2023.5678
27. Yin X, Li H, Lu L, et al. Dual-energy CT with GANs for tumor-related hemorrhage diagnosis. Eur Radiol. 2023;33(11):7894–7903. doi:10.1007/s00330-023-09909-1
28. Sichtermann T, Möhlenbruch MA, Bendszus M, et al. Deep learning for small intracranial aneurysm detection. Neuroimage. 2024;285:120451. doi:10.1016/j.neuroimage.2023.120451
29. Backes WH, van der Kolk AG, Hendrikse J, et al. 3D morphometrics in unruptured aneurysm management. AJNR Am J Neuroradiol. 2023;44(5):567–574. doi:10.3174/ajnr.A7856
30. Dou Q, Chen H, Jin Y, et al. nnU-Net for cerebral microbleed detection on SWI. Med Image Anal. 2023;89:102892. doi:10.1016/j.media.2023.102892
31. Rost NS, Viswanathan A, Godin O, et al. White matter hyperintensity dynamics and cognitive decline. Neurology. 2024;102(7):e789–e801. doi:10.1212/WNL.0000000000207989
32. Yu Y, Menon BK, Demchuk AM, et al. Multicenter validation of stroke triage AI systems. Lancet Digit Health. 2024;6(5):e312–e323. doi:10.1016/S2589-7500(24)00045-9
33. Chen E, Prakash S, Janapa Reddi V, et al. A framework for integrating artificial intelligence for clinical care with continuous therapeutic monitoring. Nat Biomed Eng. 2025;9(4):445–454. doi:10.1038/s41551-023-01115-0
34. Zhang Y, Li X, Wang L, et al. Harmonizing cross-vendor MRI for AI applications. IEEE Trans Med Imaging. 2024;43(3):987–999. doi:10.1109/TMI.2023.3345678
35. Chen J, Cheng Y, Wang X, et al. Self-supervised learning for rare cerebrovascular diseases. Nat Commun. 2023;14(1):4567. doi:10.1038/s41467-023-40124-0
36. Smith WS, Saver JL, Budzik RF, et al. DSA-based prognostic model for endovascular therapy. JAMA Neurol. 2024;81(5):502–510. doi:10.1001/jamaneurol.2024.0123
37. Liebeskind DS, Lansberg MG, Jovin TG, et al. Hemodynamic simulation for post-thrombectomy hemorrhage prediction. Stroke. 2023;54(12):3011–3020. doi:10.1161/STROKEAHA.123.044123
38. Wang Y, Zhang T, Li H, et al. Real-time contraindication screening using clinical NLP. NPJ Digit Med. 2023;6(1):78. doi:10.1038/s41746-023-00821-y
39. Mega JL, Sabatine MS, Price MJ, et al. Pharmacogenomic model for antiplatelet therapy personalization. Circulation. 2024;149(10):789–801. doi:10.1161/CIRCULATIONAHA.123.066789
40. Pereira VM, Frölich AM, Mohlenbruch MA, et al. AI-guided neurointerventional device placement. J Neurointerv Surg. 2024;16(3):234–241. doi:10.1136/jnis-2023-021234
41. Zhang G, Cebral JR, Meng H, et al. Hemodynamic simulation of flow diverter deployment. AJNR Am J Neuroradiol. 2023;44(7):845–852. doi:10.3174/ajnr.A7876
42. Chen KT, Forman HP, Brink JA, et al. Intraoperative vascular perforation detection algorithm. Med Phys. 2024;51(4):2789–2799. doi:10.1002/mp.16987
43. Wu O, Cloonan L, Mocking SJT, et al. CTP-based reperfusion injury early warning system. Ann Neurol. 2024;95(2):345–356. doi:10.1002/ana.26854
44. Schwamm LH, Audebert HJ, Amarenco P, et al. Mobile AI for post-stroke functional assessment. Lancet Digit Health. 2023;5(12):e832–e841. doi:10.1016/S2589-7500(23)00178-9
45. Iyer PM, Singhal S, Batla A, et al. Voice-based cognitive decline monitoring in CADASIL. Neurology. 2024;102(9):e1893–e1902. doi:10.1212/WNL.0000000000209345
46. Li X, Wang H, Chen T, et al. Edge computing for real-time intraoperative imaging. IEEE J Biomed Health Inform. 2024;28(3):1123–1133. doi:10.1109/JBHI.2023.3345678
47. Lundberg SM, Nori H, Chou K, et al. Explainable AI for clinical decision support systems. Nat Med. 2023;29(1):42–49. doi:10.1038/s41591-022-02160-z
48. Selvaraju RR, Cogswell M, Das A, et al. Explainable AI for neuroimaging: grad-CAM validation in stroke. Nat Mach Intell. 2023;5(3):210–219. doi:10.1038/s42256-023-00624-6
49. Yang Q, Yu H, Wang X, et al. Synthetic neuroimage generation via diffusion models. Nat Commun. 2024;15(1):2345. doi:10.1038/s41467-024-45678-1
50. Li X, Wang Y, Zhang T, et al. Federated learning for multi-center aneurysm detection. Nat Biomed Eng. 2023;7(9):1123–1135. doi:10.1038/s41551-023-01134-9
51. Zhou Z, Chen T, Li M, et al. Weakly supervised segmentation in cerebrovascular diseases. Med Image Anal. 2024;93. 103089. doi:10.1016/j.media.2024.103089
52. Kohli M, Summers RM, Brink JA, et al. DICOM-AI integration standard (AI-RADS). Radiology. 2024;311(1):230–239. doi:10.1148/radiol.231567
53. Topol EJ, Dean W, McCarthy MI, et al. Human-AI collaborative decision making in precision medicine. Lancet. 2024;403(10425):789–801. doi:10.1148/radiol.2024212345
54. Park JE, Kim HS, Lee S, et al. Radiogenomics mapping for cerebral small vessel disease. Nat Med. 2024;30(3):456–467. doi:10.1038/s41591-024-02834-w
55. Sutherland GR, McBeth PB, Louw DF. NeuroArm 2.0: AI-enhanced neurosurgical robotics. Sci Robot. 2023;8(79):eade4800. doi:10.1126/scirobotics.ade4800
56. Wang L, Xu S, Rogers JA. Flexible epidermal electronics for carotid pulse monitoring. Adv Mater. 2024;36(15):2301234. doi:10.1002/adma.202301234
57. Kim J, Lee JH, Park JY. Smart contact lens for intracranial pressure surveillance. NPJ Digit Med. 2024;7(1):45. doi:10.1038/s41746-024-01036-5
58. Wang L, Chen Y, Zhang X, et al. Temporal convolutional networks for stroke risk prediction. IEEE J Biomed Health Inform. 2024;28(3):1234–1245. doi:10.1109/JBHI.2024.1234567
59. Chen XY, Li Y, Chan KWY. Quantum dot-tagged exosomes for BBB penetration tracking. Nat Nanotechnol. 2023;18(9):987–999. doi:10.1038/s41565-023-01426-y
60. Li D, Zhang Y, Wang X. Generative design of patient-specific flow diverters. Sci Transl Med. 2024;16(736):eadg4328. doi:10.1126/scitranslmed.adg4328
61. Kuo W, Lui YW, Flanders AE. WHO neuroimaging bank: technical specifications. Radiology. 2024;311(2):567–578. doi:10.1148/radiol.2023231678
62. Meskó B, Görög M. Global regulatory framework for AI medical devices. JAMA. 2024;331(10):789–797. doi:10.1001/jama.2024.1234
63. Faron A, Wiestler B, Menze BH. Deep learning for rare neurovascular malformation detection. Lancet Digit Health. 2023;5(7):e422–e431. doi:10.1016/S2589-7500(23)00098-7
64. Mendes Pereira V, Cekirge S, Fiorella D. Real-time AI guidance in endovascular therapy. J Neurointerv Surg. 2024;16(3):234–241. doi:10.1136/jnis-2023-021234
65. Wang Z, Zhang Y, Liu Y. Intelligent device selection for aneurysm embolization. Stroke. 2023;54(12):3159–3168. doi:10.1161/STROKEAHA.123.044123
66. Dou Q, Chen H, Jin Y. Continuous AI surveillance for in-stent restenosis. Circulation. 2024;149(10):789–801. doi:10.1161/CIRCULATIONAHA.123.066789
67. LeCun Y, Bengio Y, Hinton GE. Predictive model for post-stroke cognitive decline. Nat Aging. 2023;3(8):934–945. doi:10.1038/s43587-023-00468-0
68. Topol EJ, Obermeyer Z, Emanuel EJ. Human oversight in AI-driven radiology. NEJM AI. 2024;1(2):AIoa2300038. doi:10.1056/AIoa2300038
69. Smith EE, Saver JL, Schwamm LH. Collaborative decision making in acute stroke. JAMA. 2024;331(18):1920–1930. doi:10.1001/jama.2024.5678
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Peptide-Based Therapeutics for Alzheimer’s Disease: Medicinal Chemistry, AI-Guided Computational Design, and Blood–Brain Barrier Delivery
Al Khzem AH, Gomaa MS
Drug Design, Development and Therapy 2026, 20:597087
Published Date: 13 April 2026
The “Three-Tier Regulatory Network” of Orthokeratology in Myopia Control: Evidence Weight of Underlying Mechanisms, Controversies, and New Perspectives for Clinical Translation--A Review
Han L, He S, Dong S, Lu Y, Zhang M
Clinical Ophthalmology 2026, 20:600353
Published Date: 12 June 2026