Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Pediatric Pustular Psoriasis in Southern China: A 12-Year Retrospective Analysis of 41 Cases Focusing on Clinical Characteristics and Treatment Outcomes
Authors Tang J, Hou Z, Liao W, Wang Y, Zhang G, Luo Y, Gao X, Wei Z
Received 25 January 2025
Accepted for publication 12 April 2025
Published 12 May 2025 Volume 2025:15 Pages 185—195
DOI https://doi.org/10.2147/PTT.S519385
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Enzo Errichetti
Jinling Tang,1,* Zhaojuan Hou,2,3,* Wei Liao,1 Yuwei Wang,1 Ge Zhang,1 Yangyang Luo,1 Xiaofei Gao,1 Zhu Wei1
1Department of Dermatology, The Affiliated Children’s Hospital of Xiangya School of Medicine, Hunan Children’s Hospital, Central South University, Changsha, Hunan, 410007, People’s Republic of China; 2Center for Reproductive Medicine, Xiangya Hospital of Central South University, Changsha, Hunan, 410008, People’s Republic of China; 3Clinical Research Center for Women’s Reproductive Health in Hunan Province, Changsha, Hunan, 410008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhu Wei; Xiaofei Gao, Department of Dermatology, The Affiliated Children’s Hospital of Xiangya School of Medicine, Hunan Children’s Hospital, Central South University, Changsha, Hunan, 410007, People’s Republic of China, Email [email protected]; [email protected]
Background: Pustular psoriasis (PP) is a systemic inflammatory disease that rarely occurs in children but adversely affects their quality of life.
Objective: This study aimed to evaluate the clinical characteristics, treatment, prognosis, and epidemiology of PP in pediatrics.
Methods: A single center retrospective study on 41 children diagnosed with PP was conducted in a university-affiliated referral hospital between January 2010 and May 2022. The demographics, clinical characteristics, treatment, and prognosis were evaluated in the descriptive analysis. To further investigate the effect of different acitretin-based treatments on the prognosis, 38 patients were included in the subgroup analysis. Patients who received acitretin alone were designated as the Acitretin group, while those who received acitretin combined with intravenous immunoglobulin, ciclosporin, or steroids (or any combination of these agents) were identified as the Combination group.
Results: A total of 41 patients were enrolled in the descriptive analysis. Of these, 65.8% (27/41) were male, and the mean age of onset was 3.2 ± 3.2 years. Among the patients, 63.4% (26/41) presented with pustules, and over half experienced fever and elevated C-reactive protein (CRP) levels. In the subgroup analysis, the CRP level was significantly higher in the Combination group (59.69 ± 43.74 versus 26.35 ± 19.67 mg/dL, P = 0.006), indicating that patients had more severe inflammatory conditions. Nevertheless, there was no significant difference in the remission rate between the Acitretin group and the Combination group.
Conclusion: Pediatric PP is a disease that often occurs in the pre-school period and predominantly affects males. It is characterized by typical skin lesions and systemic inflammatory reactions. Common comorbidities include nutritional disorders such as malnutrition and anemia. Combination treatment based on acitretin is recommended for children with PP and severe inflammation.
Plain Language Summary: Pediatric PP occurs more frequently in boys at pre-school age. Most patients exhibited typical pustules at disease onset, with the trunk and face being the most common sites of skin lesions. Combined treatment based on acitretin benefits patients with systemic inflammation.
Keywords: childhood pustular psoriasis, clinical characteristics, treatment, acitretin, follow-up
Introduction
Psoriasis is a chronic inflammatory immune skin disease that affects approximately 1%~4% of adults and children worldwide, with more than 45% of individuals developing the initial lesions before 20 years of age.1,2 The spectrum of psoriasis includes various forms: psoriasis vulgaris (PV), pustular psoriasis (PP), erythrodermic psoriasis, and psoriatic arthritis (PsA).3
PP is a severe form of psoriasis that rarely develops in children but negatively impacts their quality of life. The incidence of PP in children is about 0.7% to 6.7%.2,4 The age of PP onset in children ranged from 1 month to 11 years.5 The diagnosis of PP was based on morphological and histologic characteristics.6 According to the previous report, PP can be classified into four categories based on morphological characteristics, including generalized (GPP), pustular erythrodermic psoriasis (PEP), annular (APP), and psoriasis vulgaris with pustules (PVP).5
The initial presentations of PP were diverse. PP can develop with or without PV. Some patients can present with a mild and stable form of PV, which may progress into a more severe form of PP. Conversely, patients may initially present with an acute form of PP characterized by widespread pustular eruption, or a subacute variant with an annular phenotype. Both forms can transform into one another following a disease flare episode. However, the most important clue for diagnosing PP is the clinical presentation of widespread, macroscopically visible, sterile pustules and erythema that are not localized to the palmoplantar areas or preexisting psoriatic plaques.6 Symptoms and signs of systemic inflammation may be present in severe subtypes of PP.
Due to the scarcity of pediatric PP cases, knowledge about the clinical features, disease course, therapeutic modalities, and prognosis for children is incomplete. The clinical trials and standard criteria for PP treatment are currently based on adults, making it challenging to achieve the optimal management strategy for pediatric PP. The aim of this study was to evaluate the clinical characteristics, treatment, prognosis, and epidemiology of pediatric PP in a university-affiliated referral hospital between January 2010 and May 2022.
Materials and Methods
Patients
This retrospective single-center study enrolled 41 patients diagnosed with PP between January 2010 and May 2022 at the dermatology department of Hunan Children’s Hospital. The follow-up period ranged from 2 to 11 years. The diagnosis was confirmed by more than 2 dermatologists and was supported by histological examination when necessary. Patients with localized pustular psoriasis, including acrodermatitis continua of Hallopeau (ACH) and palmoplantar pustular psoriasis (PPP), were excluded from the study. This study was performed with approval from the ethical committee of Hunan Children’s Hospital (Approval ID KY2024-35) and in compliance with the Declaration of Helsinki. Written informed consent was obtained from the parent/legal guardian of the patients for their participation in the study.
Data Collection
The flow chart of the study is illustrated in Figure 1. Demographic and clinical characteristics of patients, including age at initial visit, age at psoriasis onset, age at PP onset, gender, body mass index (BMI), personal and family history of psoriasis, presentation and localization of initial skin lesions, and comorbidities, were collected. The body surface area (BSA) was used to evaluate the distribution of psoriatic lesions. The following parameters, including fever (> 38 °C), serum albumin level (< 35 g/L), C-reactive protein (CRP) level (> 8.0 mg/dL), and white blood cell (WBC) count (> 15000/mL), were also investigated. The disease location at GPP flare, classification of PP, complications, and systemic treatment were evaluated according to the medical document. The classification of PP was based on previous literature.5,7,8 The concomitant PsA was assessed according to the CASPAR criteria.9 For the follow-up, the course of the disease was assessed, including remission, 1–2 flares per year, 3–5 flares per year, and more than 5 flares per year during follow-up. Hospitalization, predisposing factors of disease flare, current treatment, and clinical status were also evaluated. PV, PVP, and nail lesions were assessed based on medical records obtained during the return visit and self-reported disease conditions from the phone interview.
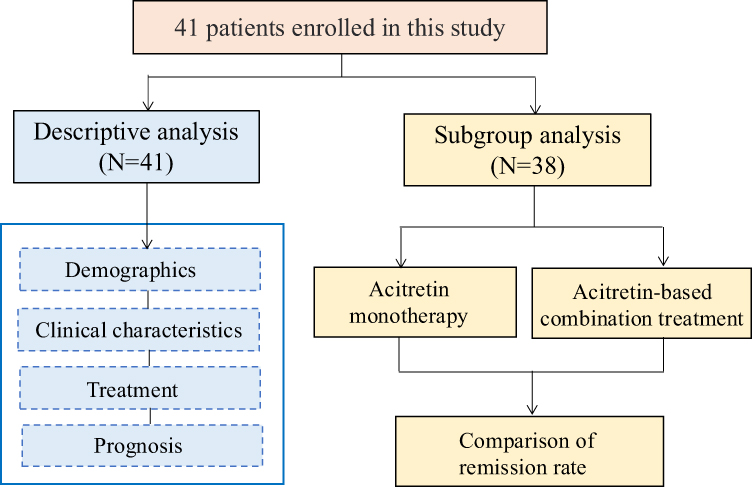 |
Figure 1 Flow chart of the study. |
Definition of Study Groups
Thirty-eight patients who received acitretin during their initial treatment were included in this subgroup analysis, while three patients treated solely with biologic agents or intravenous immunoglobulin (IVIG) were excluded. According to the treatment received, patients were stratified into two groups. Patients who were treated with low-dose acitretin (0.5–1.0 mg/kg/d) exclusively were identified as the Acitretin group. In contrast, patients who received low-dose acitretin (0.5–1.0 mg/kg/d) combined with IVIG, ciclosporin, or steroids, either one or more of these agents, were designated as the Combination group.
Outcomes
The absence of skin lesions and nail lesions at the time of phone interview was deemed to be lesion-free. For the prognosis, remission was defined as the duration of clear skin being equal to or greater than one year, regardless of drug withdrawal. Non-remission was defined as the duration of clear skin being less than one year or the presence of skin lesions at the time of the phone interview.
Statistical Analysis
The statistical analysis was performed using IBM SPSS (version 25.0, IBM, USA). Descriptive statistics were used to describe and summarize the parameters. Normality was examined using the Shapiro–Wilk test. Proportions of patients were presented as percentages of the total population and compared by Fisher’s exact test. For normally distributed continuous variables, means and standard deviations (SDs) were reported, with between-group differences compared using the independent sample t-test. For non-normally distributed continuous variables, medians and interquartile ranges were reported, with differences evaluated using the Mann–Whitney U-test. A two-sided P < 0.05 was considered statistically significant.
A sensitivity analysis was performed to evaluate the effect of lost-to-follow-up cases on prognosis. The remission rate was calculated by using both conservative and optimistic approaches. By applying the conservative approach, lost-to-follow-up patients were deemed to be in remission in the Acitretin group, while they were considered to be in non-remission in the Combination group. Conversely, using the optimistic approach, lost-to-follow-up patients were presumed to be in remission in the Combination group and in non-remission in the Acitretin group.
Results
Descriptive Analysis
The demographic data of the enrolled population is presented in Table 1. A total of 41 patients were included in the study. Of these, 65.8% (27/41) were male, with a male-to-female ratio of 1.5 (27/14). The age at first visit was 5.0 ± 3.9 years, ranging from 0 to 16 years. The average age of psoriasis onset was 3.2 ± 3.2 years, and the age of PP onset was 3.5 ± 3.3 years. The mean BMI was 16.9 ± 3.8 kg/m2 at the initial visit. 7.3% (3/41) of patients reported a positive family history of psoriasis, and 19.5% (8/41) of patients had a history of confirmed psoriasis, including 2 (4.9%) with PV and 6 (14.6%) with PP. In terms of the initial presentation at psoriasis onset, all the enrolled patients had erythema. Additionally, 63.4% (26/41) of patients had pustules, 26.8% (11/41) had papules, and 17.1% (7/41) had scales. The localization of initial skin lesions was distributed as follows: 39.0% (16/41) of patients had lesions in the trunk, 24.4% (10/41) in the face, 19.5% (8/41) in the limbs, 17.1% (7/41) in the neck, 17.1% (7/41) in the folds, 9.8% (4/41) in the scalp, and 4.9% (2/41) in the diaper area. Regarding the comorbidities with PP, 29.3% (12/41) of patients had malnutrition, 29.3% (12/41) had anemia, 12.2% (5/41) had obesity or overweight, 9.7% (4/41) had food allergy, 7.3% (3/41) had vitamin D deficiency, 7.3% (3/41) had otitis media with effusion, 4.8% (2/41) had eczema, 2.4% (1/41) had vitiligo, 2.4% (1/41) had prosopoplegia, and 2.4% (1/41) had PsA.
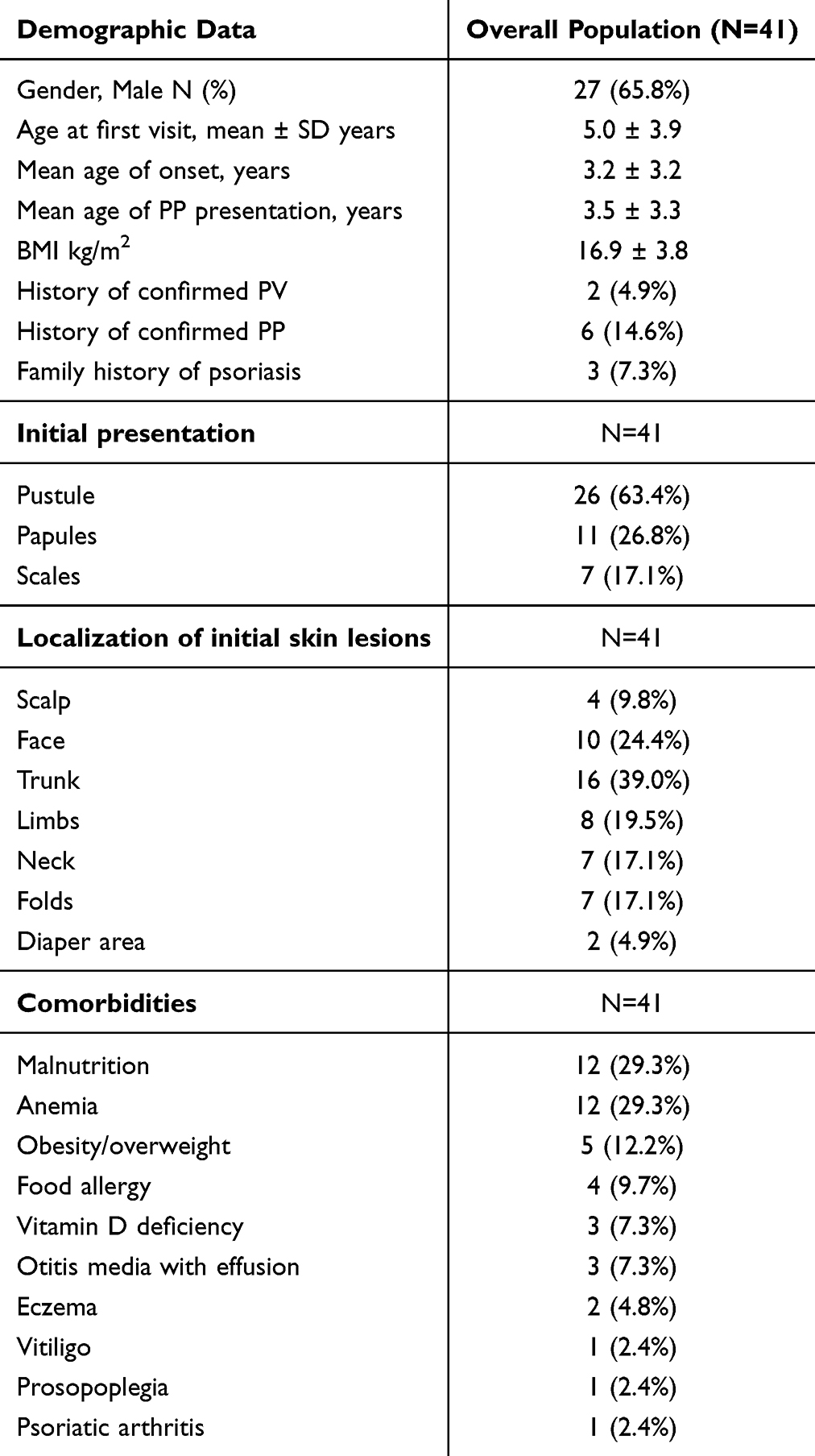 |
Table 1 Demographic and Clinical Characteristics of the Children with Pustular Psoriasis |
The location, presentation, and treatment of PP at the initial visit are summarized in Table 2. The mean BSA was 53.73 ± 19.27%. A total of 23 patients (56.1%) had fever, 10 patients (24.4%) had low levels of serum albumin, 35 patients (85.4%) had increased levels of CRP, and 20 patients (48.8%) had leukocytosis. All patients had skin lesions on the trunk. Other disease localizations included: head-neck involvement in 35 patients (85.4%), limb involvement in 29 patients (70.7%), palmoplantar involvement in 10 patients (24.4%), nail involvement in 3 patients (7.3%), skin fold involvement in 3 patients (7.3%), and oral mucosa involvement in 1 patient (2.4%). As for the subtypes of PP, 27 patients (65.9%) had GPP, 8 patients (19.5%) had PEP, 4 patients (9.8%) had APP, and 2 patients (4.9%) had PVP. The epidemiologic data and subtypes for each case are listed in Supplemental Table 1. Regarding the systemic treatments at the initial visit, 38 patients (92.7%) were treated with oral acitretin, and 16 patients (39.0%) received IVIG infusion. Among these, 2 infants (patients 18 and 31) received IVIG as monotherapy. Additionally, 6 patients (14.6%) were given ciclosporin treatment, 7 patients (17.1%) were treated with short-term systemic steroids (within 4 weeks), including 6 with methylprednisolone and 1 with prednisone. One patient (patient 7) received biological treatment as monotherapy. The details of treatment for individuals are detailed in Supplemental Table 2.
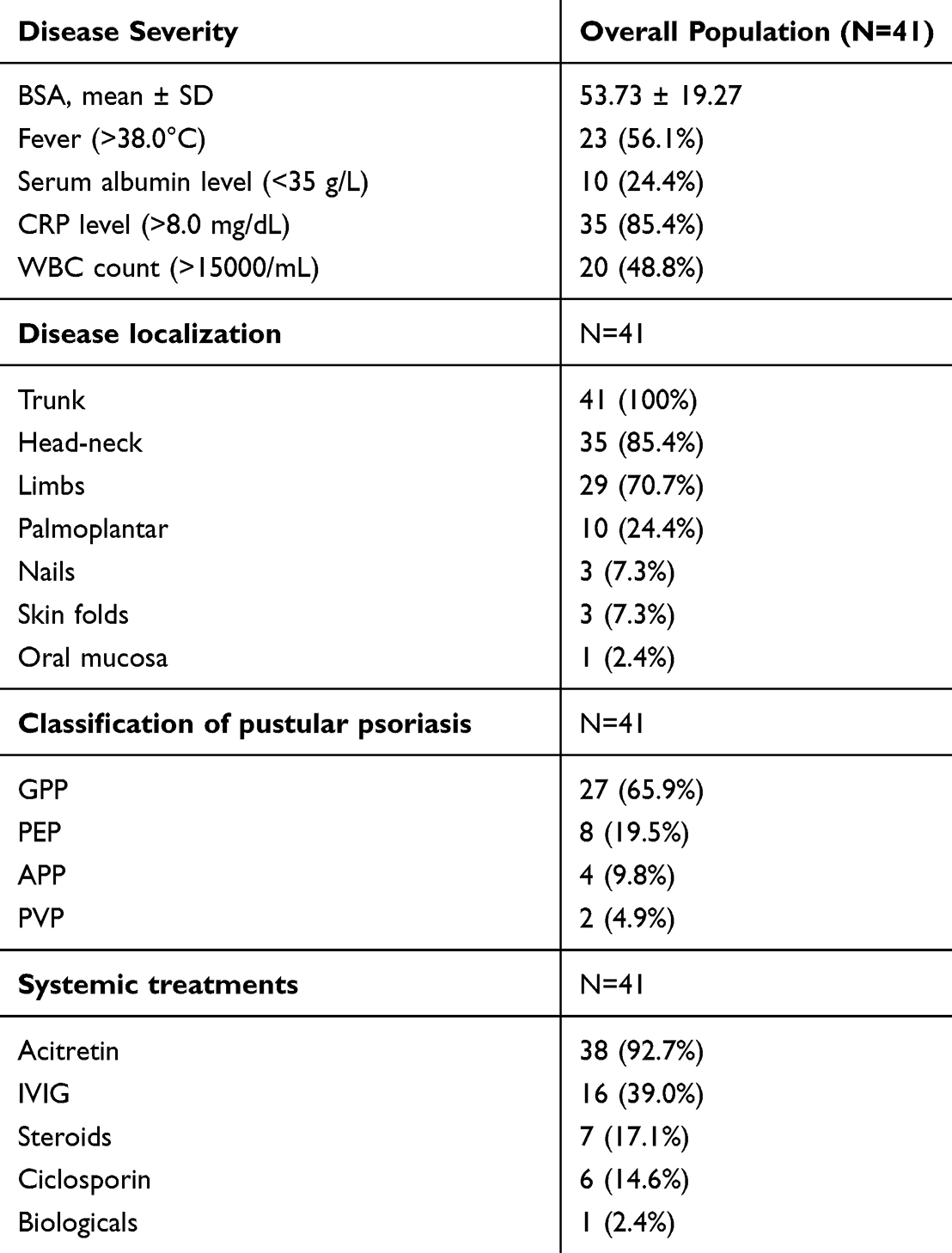 |
Table 2 Clinical Features and Systemic Treatment of the Children with Pustular Psoriasis at Initial Visit |
The number of flares, triggers, the course of the disease, and follow-up are listed in Table 3. The duration of follow-up ranged from 2 to 11 years, with a mean follow-up of 5.0 ± 2.1 years. In the latest phone interviews, 7 (17.1%) patients were lost to follow-up (Supplemental Table 1). According to the medical records and feedback from telephone interviews, 19 (46.3%) patients had potential predisposing factors associated with PP flare, including infection in 14 (34.1%), medications in 3 (7.3%), seasonal change in 3 (7.3%), and trauma in 1 (2.4%). In terms of healthcare utilization, 2.4% (1/41) of patients had no hospital admissions, 29.3% (12/41) had one hospitalization, 26.8% (11/41) had two hospitalizations, 31.7% (13/41) had 3 to 5 hospitalizations, and 9.8% (4/41) had more than 6 hospitalizations during the follow-up. Regarding the number of disease flares, 61.8% (21/34) of patients entered long-term remission, 17.6% (6/34) had 1–2 flares per year, 8.8% (3/34) had 3–5 flares per year, and 11.8% (4/34) still had frequent relapses with more than 5 flares per year. For current treatment (Supplemental Table 2), 52.9% (18/34) of patients have been weaned off medications, including 3 patients with mild PV or nail lesions. Additionally, 26.5% (9/34) are receiving topical treatment, 5.9% (2/34) are taking acitretin orally, and 26.5% (9/34) are receiving biological treatment. For current clinical status (Supplemental Table 1), 8.8% (3/34) of patients have developed PV, 8.8% (3/34) of patients (2 with GPP and 1 with APP) have converted into PVP, 20.6% (7/34) have nail lesions, 11.8% (4/34) have joint pain, 58.8% (20/34) are lesion-free, and 14 of these patients have successfully withdrawn from medication.
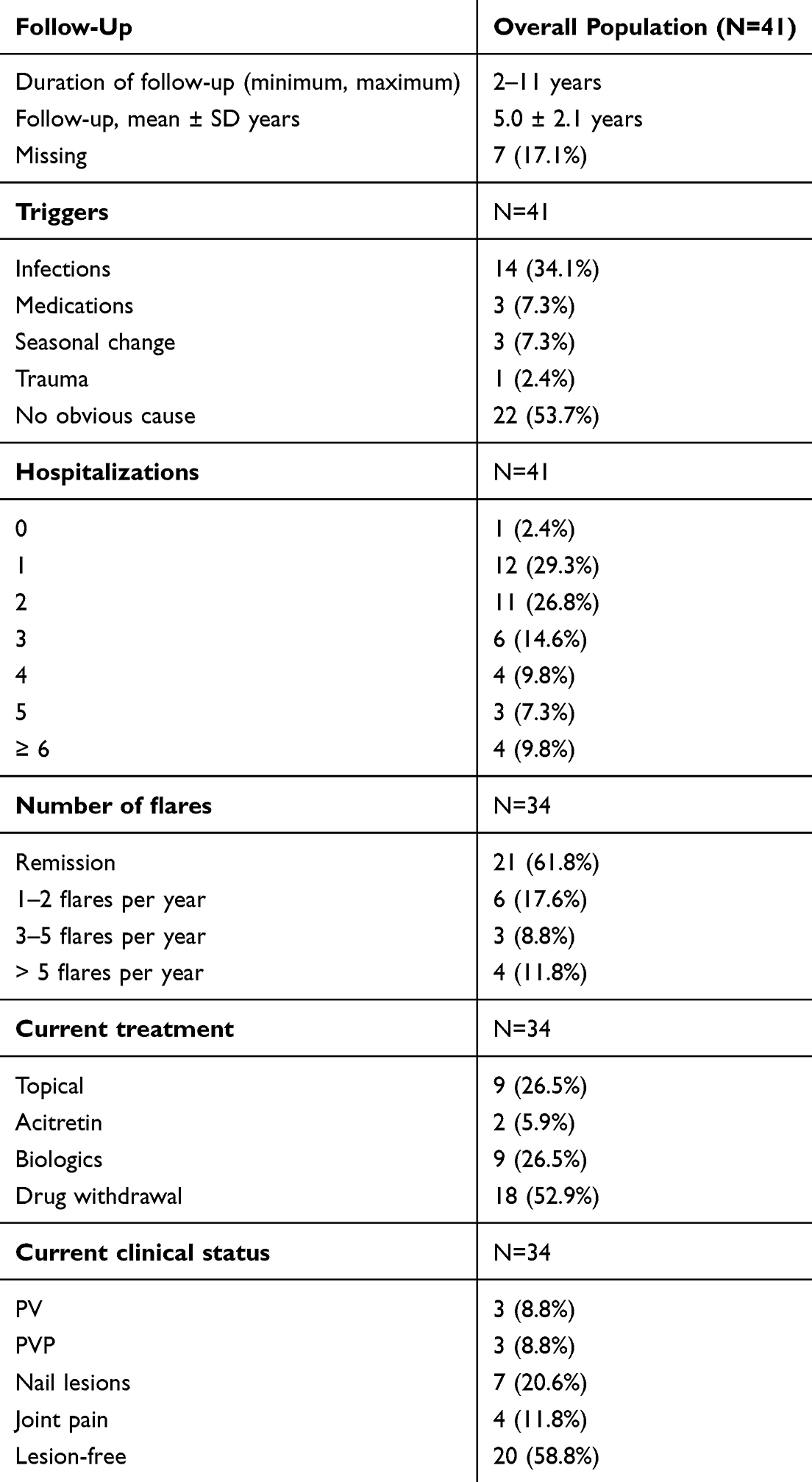 |
Table 3 Course of the Disease and Follow-Up |
Subgroup Analysis
A total of 38 patients were included, with 19 in each group (Table 4). There were no significant differences in the baseline characteristics, including age at first visit, mean age of onset, mean age of PP presentation, BMI, and gender. Regarding the severity evaluation of PP, the serum albumin level (37.05 ± 4.46 versus 38.20 ± 3.27 g/L, P = 0.374), the presentation of fever, WBC count [(16.89 ± 5.87) versus (14.07 ± 5.79) × 109/L, P = 0.150], neutrophil count [(10.24 ± 5.57) versus (8.93 ± 5.32) × 109/L, P = 0.471], the percentage of neutrophil [0.66 (0.62, 0.72) versus 0.71 (0.61, 0.78), P = 0.295], number of hospitalization [2.00 (1.00, 4.00) versus 2.00 (2.00, 5.00), P = 0.603], BSA [59.00 (45.00, 64.00) % versus 63.00 (52.00, 69.00) %, P = 0.402], and initial presentation of pustules (68.4% versus 57.9%, P = 0.737) were not significantly different between the Acitretin group and the Combination group. However, the CRP level was significantly higher in the Combination group compared to the Acitretin group (59.69 ±43.74 versus 26.35 ± 19.67 mg/dL, P = 0.006), indicating that these patients had more severe inflammatory conditions.
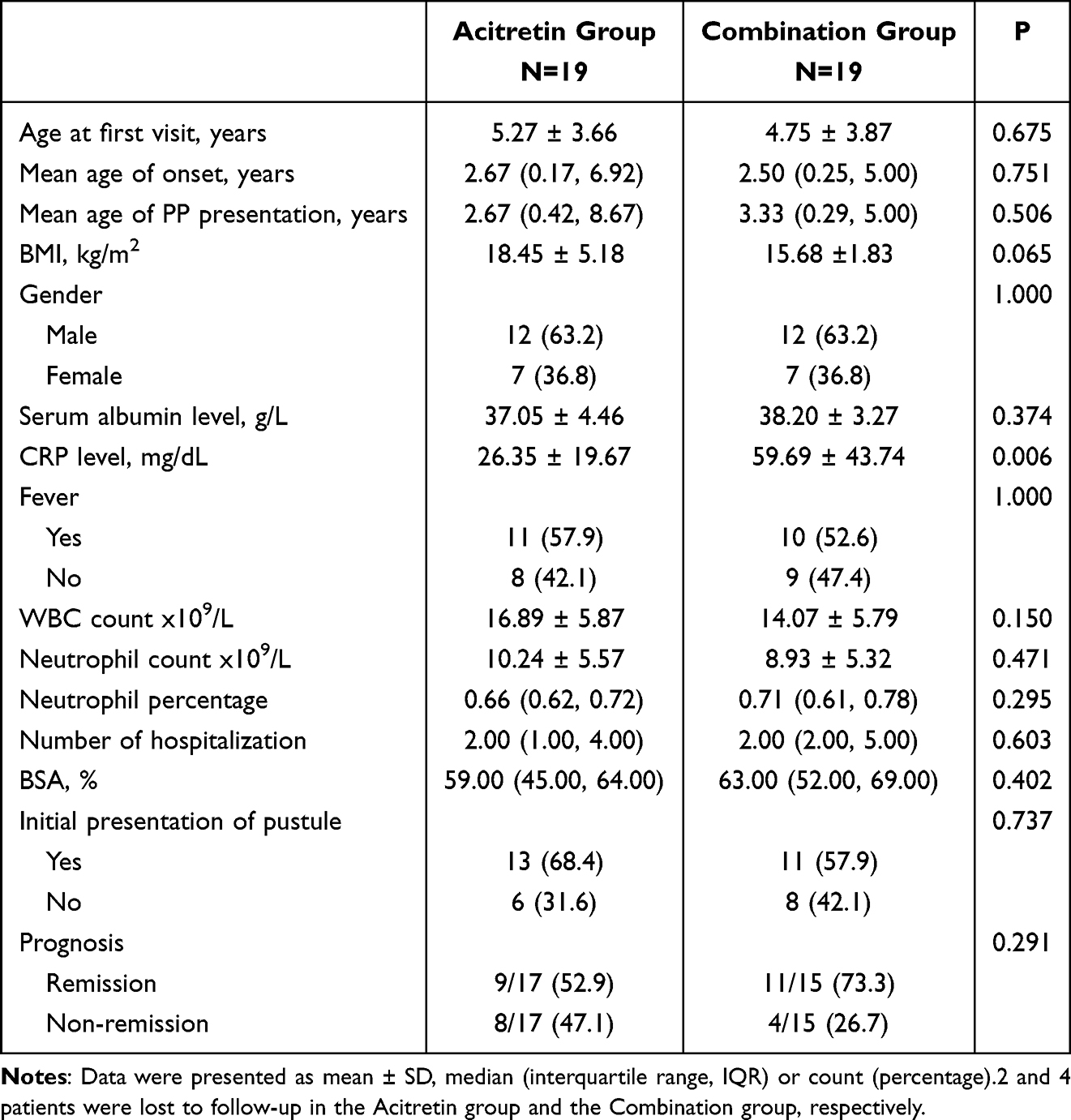 |
Table 4 Comparison of Baseline Characteristics, Disease Severity and Prognosis Between the Acitretin Group and the Combination Group |
With respect to prognosis, there was no significant difference between the Acitretin group and the Combination group (52.9% versus 73.3%, P = 0.291). A sensitivity analysis (Supplemental Table 3) yielded similar results to those obtained by excluding all patients lost to follow-up.
Discussion
In this study, we described the clinical characteristics, treatment, prognosis, and epidemiology of children with PP during follow-up. Our data indicated that pediatric PP primarily affects preschool-aged males, presenting with characteristic skin lesions and systemic inflammatory response. Notably, children with PP who exhibited a more severe inflammatory response achieved comparable remission rates through combination therapy as compared to those with milder inflammation treated with acitretin monotherapy.
In our series, PP predominately affected male patients. Although the prevalence of PP is generally higher in females than in males globally, a higher prevalence in males has been reported in the Chinese population.7,10–13 PP can develop with or without PV. Onset at < 18 years was more common in the PP without PV group than in the PP with PV group.14 In our sample, approximately 20% of patients had a history of psoriasis, including 2 with PV and 6 with PP. Due to the high incidence of psoriasis in adults, the prevalence of psoriasis in grownups ranges from 70% to 85%, which is significantly higher than that in children, according to published literature.12,13,15
In our study, 36 patients (87.8%) were first diagnosed with PP in our hospital. The initial presentations of the disease were diverse: 63.4% (26/41) of patients had pustules at disease onset, and only 17.1% (7/41) had obvious scales in their cutaneous lesions. Although the latest international consensus statement points out that PP can be diagnosed with or without scales,6 topical treatment with steroidal medications at the onset of disease may also mask the original presentation of skin lesions. This is especially relevant given that 17 (41.5%) patients had previously been diagnosed with eczema at other hospitals and received topical steroid treatment.
The previous study showed that APP was the most common type of PP.8 In our series, the presentations of PP at the first visit were as follows: GPP in 65.9%, PEP in 19.5%, APP in 9.8%, and PVP in 4.9%. Patients with APP and PVP tend to have milder symptoms and may not be referred to our hospital. Most patients had involvement of over half of the BSA. Additionally, 56% of patients had a fever (>38.0°C), 24.4% had low serum albumin levels, 85.4% had increased CRP levels, and 48.8% had leukocytosis. These systemic symptoms and laboratory indices, which indicated disease flare at the initial visit, are not only useful for confirming the diagnosis of PP but are also positively associated with disease severity.6,16,17 Regarding comorbidities, adult patients with PP had higher rates of cardiovascular and cerebrovascular diseases as well as hypertension.13,18 Torres et al reported that more than 80% of adult patients with PP presented with at least one comorbidity in their multicenter retrospective cohort study, with hypertension, obesity, and dyslipidemia being the most common comorbidities.15 Moreover, lifestyle habits such as smoking and alcohol use were prevalent in adult patients.15 However, nutritional issues such as malnutrition and anemia were common in our series. In pediatric patients with PP, the pain associated with skin lesions and systemic inflammatory responses may impair appetite and elevate nutritional consumption, potentially leading to malnutrition and anemia. Our findings indicated a lower comorbidity burden in pediatric PP compared with that in adults, and the distinct comorbidity patterns in adult versus childhood-onset PP could be attributed to divergences in lifestyle-related risk factors inherent to different developmental stages.
Treatment of PP in children remains challenging due to the lack of randomized controlled trials and standard guidelines. Current therapy recommendations are based on limited case reports and insufficient evidence. The first-line therapies for PP in children include acitretin, ciclosporin, methotrexate, glucocorticoid, and biologicals.16 To manage disease flares, different systemic treatments were prescribed, with patients generally receiving acitretin (92.7%) and IVIG (39.0%). Short-term steroids (17.1%) and ciclosporin (14.6%) were prescribed to patients experiencing flares of GPP or PEP. One patient (Patient 7) with severe GPP received adalimumab as initial therapy to rapidly control the disease flare. Although the focus of this study did not include an evaluation of adverse effects of anti-psoriatic medications, no severe side effects were documented according to the medical records. Previous studies have demonstrated that acitretin, a conventional PP treatment, exhibits satisfactory therapeutic efficacy and safety in children at relatively low doses (0.2–1.0 mg/kg/day),19,20 regardless of treatment duration (short-term or long-term therapeutic regimens). The role of IVIG has not been widely established; however, IVIG therapy has been successful in individual cases.21–23 This method utilizes immunomodulation to remove active granulocytes and monocytes from the peripheral blood, and these immune cells are considered pathogenic in GPP.16,24 Among the patients receiving IVIG treatment, most had high fever or were children younger than 1 year old at the initial visit. It is worth noting that 2 infants (Patients 18 and 31) were given IVIG as monotherapy due to their parents’ concerns about the side effects of other systemic medications, and significant improvements were observed in both at the time of discharge. The results of our study indicated that, for children with systemic symptoms or those younger than 1 year old, IVIG is a good and safe treatment option to effectively control systemic inflammation.
It is well-known that PP has a relapsing nature that can be triggered by several precipitating factors. In our study, triggers were identified in 46.3% (19/41) of cases, including infection in 34.1% (14/41), medications in 7.3% (3/41), seasonal change in 7.3% (3/41), and trauma in 2.4% (1/41). The most common infection associated with PP flare was upper respiratory infections, consistent with a previous study.13 For medication, the use of antibiotics and acitretin withdrawal were described in our series. Other drugs, such as terbinafine, TNF-alpha inhibitors, and corticosteroid withdrawal, have also been reported previously.25,26 One patient had a PP flare after trauma, which may be associated with the isomorphic response in psoriasis.27 In our series, over 95% of patients had more than one hospitalization. GPP and PEP, which are the more severe types of PP, predominate in these cases. Most cases require systemic treatment, leading to higher hospitalization requirements.
Regarding the current treatment, 18 patients (52.9%, 18/34) have been weaned off treatment. Of these, 14 are lesion-free, and 4 have mild PV or nail lesions. Topical ointment is applied to 9 patients (26.5%, 9/34) for maintenance treatment. Additionally, 9 patients (26.5%, 9/34) who have more than one flare per year are receiving biological treatment, including 8 with secukinumab and one with adalimumab. Oral acitretin is still administered to 2 patients (Patients 15 and 32). Patient 32 has achieved good disease control and is in remission, while Patient 15, who experiences more than 5 flares per year, concurrently receives biological treatment. Concerning the current clinical status, 20 patients (58.8%, 20/34) are lesion-free, and 14 of them have withdrawn from medication. In addition, 3 patients (8.8%, 3/34) have developed PV, and another 3 patients (8.8%, 3/34) have converted into PVP. Although the clinical features and pathological mechanisms of PP are distinct from those of PV, the conversion between PV and PP has been documented previously.7,28 The factors and pathogenic mechanisms associated with the conversion from PP to PV remain to be further investigated.
The study has some limitations and strengths. First, the single-center retrospective design may introduce recall bias and limit generalizability. Second, the sample size is relatively small, which restricts the ability to establish causality between subtypes, treatment, and disease course. Finally, genetic mutations associated with PP were not detected in most cases. However, due to the rare occurrence of PP in children, knowledge about the disease course of pediatric PP is very limited. Additionally, randomized controlled trials and standard criteria for the treatment of pediatric PP are still lacking. This study depicted the epidemiology and clinical features of pediatric PP and emphasized the treatment and prognosis of pediatric PP, which may contribute to a better understanding of the disease and facilitate the development of an optimal management strategy for young children with PP.
Conclusion
Pediatric PP is a disease that often occurs in pre-school-aged children and is more prevalent in males. It is characterized by typical skin lesions and is often accompanied by systemic inflammatory reactions. Common comorbidities include nutritional disorders such as malnutrition and anemia. PP has a significant negative impact on children’s quality of life and is associated with limitations in treatment options. Acitretin has demonstrated an effective and safe profile at low doses in children. It is recommended that children with PP who have severe inflammation receive combination treatment based on acitretin.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
This study was performed with the approval of the ethical committee of Hunan Children’s Hospital (Approval ID KY2024-35). Written informed consent was obtained from the parent/legal guardian of the patients to participate in the study.
Acknowledgments
Jinling Tang and Zhaojuan Hou are co-first authors for this study. We are grateful to the participants and their parent/legal guardian to participate in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (project 82304031), and Natural Science Foundation of Hunan Province (projects 2023JJ40344, 2023JJ60278).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Parisi R, Symmons DP, Griffiths CE. et al. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. doi:10.1038/jid.2012.339
2. Chiam LY, de Jager ME, Giam YC, et al. Juvenile psoriasis in European and Asian children: similarities and differences. Br J Dermatol. 2011;164(5):1101–1103. doi:10.1111/j.1365-2133.2010.10196.x
3. Griffiths CEM, Armstrong AW, Gudjonsson JE, et al. Psoriasis. Psoriasis Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
4. Morris A, Rogers M, Fischer G, et al. Childhood psoriasis: a clinical review of 1262 cases. Pediatr Dermatol. 2001;18(3):188–198. doi:10.1046/j.1525-1470.2001.018003188.x
5. de Oliveira ST, Maragno L, Arnone M, et al. Generalized pustular psoriasis in childhood. Pediatr Dermatol. 2010;27(4):349–354. doi:10.1111/j.1525-1470.2010.01084.x
6. Choon SE, van de Kerkhof P, Gudjonsson JE, et al. international consensus definition and diagnostic criteria for generalized pustular psoriasis from the international psoriasis council. JAMA Dermatol. 2024;160(7):758–768. doi:10.1001/jamadermatol.2024.0915
7. Popadic S, Nikolic M. Pustular psoriasis in childhood and adolescence: a 20-year single-center experience. Pediatr Dermatol. 2014;31(5):575–579. doi:10.1111/pde.12296
8. Liao PB, Rubinson R, Howard R, et al. Annular pustular psoriasis--most common form of pustular psoriasis in children: report of three cases and review of the literature. Pediatr Dermatol. 2002;19(1):19–25. doi:10.1046/j.1525-1470.2002.00026.x
9. Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006;54(8):2665–2673. doi:10.1002/art.21972
10. Fanghui FU, S.z. YANGQ, Guangjin WANG, et al. Clinical analysis of 61 childhood pustular psoriasis. China J Lepr Skin Dis. 2019;35(3):136–139.
11. Zhang Q, Shi P, Wang Z, et al. Identification of the BTN3A3 gene as a molecule implicated in generalized pustular psoriasis in a Chinese Population. J Invest Dermatol. 2023;143(8):1439–1448.e21. doi:10.1016/j.jid.2023.01.023
12. Zheng J, Chen W, Gao Y, et al. Clinical analysis of generalized pustular psoriasis in Chinese patients: a retrospective study of 110 patients. J Dermatol. 2021;48(9):1336–1342. doi:10.1111/1346-8138.15958
13. Bellinato F, Gisondi P, Marzano AV, et al. Characteristics of patients experiencing a flare of generalized pustular psoriasis: a multicenter observational study. Vaccines. 2023;11(4):740. doi:10.3390/vaccines11040740
14. Li X-N, Peng B, Geng S-M. Characterization of generalized pustular psoriasis in Northwest China: a single-center retrospective study. Int. J Dermatol Venereol. 2022;5(4):191–198. doi:10.1097/JD9.0000000000000275
15. Torres T, Antunes J, Brasileiro A, et al. Clinical course and disease burden of patients with generalized pustular psoriasis in Portugal: a multicenter retrospective cohort study. J DermatolTreat. 2024;35(1):2345728. doi:10.1080/09546634.2024.2345728
16. Fujita H, Terui T, Hayama K, et al. Japanese guidelines for the management and treatment of generalized pustular psoriasis: the new pathogenesis and treatment of GPP. J Dermatol. 2018;45(11):1235–1270. doi:10.1111/1346-8138.14523
17. Burden AD, Choon SE, Gottlieb AB, et al. Clinical disease measures in generalized pustular psoriasis. Am J Clin Dermatol. 2022;23(Suppl 1):39–50. doi:10.1007/s40257-021-00653-0
18. Kołt-Kamińska M, Marek-Józefowicz L, Krajewski P, et al. Characteristics of patients with generalized pustular psoriasis: a report of the polish generalized pustular psoriasis group. Dermatol Ther. 2024;14(12):3379–3393. doi:10.1007/s13555-024-01306-w
19. Di Lernia V, Bonamonte D, Lasagni C, et al. Effectiveness and safety of acitretin in children with plaque psoriasis: a multicenter retrospective analysis. Pediatr Dermatol. 2016;33(5):530–535. doi:10.1111/pde.12940
20. Chen P, Li C, Xue R, et al. Efficacy and safety of Acitretin monotherapy in children with pustular psoriasis: results from 15 cases and a literature review. J DermatolTreat. 2018;29(4):353–363. doi:10.1080/09546634.2017.1395798
21. Jolles S, Hughes J. Use of IGIV in the treatment of atopic dermatitis, urticaria, scleromyxedema, pyoderma gangrenosum, psoriasis, and pretibial myxedema. Int Immunopharmacol. 2006;6(4):579–591. doi:10.1016/j.intimp.2005.11.017
22. Taguchi Y, Takashima S, Yoshida S, et al. Psoriasis improved by intravenous immunoglobulin therapy. Intern Med. 2006;45(14):879–880. doi:10.2169/internalmedicine.45.1704
23. Gurmin V, Mediwake R, Fernando M, et al. Psoriasis: response to high-dose intravenous immunoglobulin in three patients. Br J Dermatol. 2002;147(3):554–557. doi:10.1046/j.1365-2133.2002.04753.x
24. Varman KM, Namias N, Schulman CI, et al. Acute generalized pustular psoriasis, von Zumbusch type, treated in the burn unit. A review of clinical features and new therapeutics. Burns. 2014;40(4):e35–9. doi:10.1016/j.burns.2014.01.003
25. Kara Polat A, Alpsoy E, Kalkan G, et al. Sociodemographic, clinical, laboratory, treatment and prognostic characteristics of 156 generalized pustular psoriasis patients in Turkey: a multicentre case series. J Eur Acad Dermatol Venereol. 2022;36(8):1256–1265. doi:10.1111/jdv.18103
26. Brenner M, Molin S, Ruebsam K, et al. Generalized pustular psoriasis induced by systemic glucocorticosteroids: four cases and recommendations for treatment. Br J Dermatol. 2009;161(4):964–966. doi:10.1111/j.1365-2133.2009.09348.x
27. Karampinis E, Georgopoulou KE, Goudouras G, et al. Laser-induced koebner-related skin reactions: a clinical overview. Medicina. 2024;60(7):1177. doi:10.3390/medicina60071177
28. Hayama K, Iwasaki R, Tian Y, et al. Factors associated with generalized pustular psoriasis progression among patients with psoriasis vulgaris in Japan: results from a claims database study. J Dermatol. 2023;50(12):1531–1538. doi:10.1111/1346-8138.16949
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.