Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
PD1 and TIM3 Expression is Associated with Very Early Hepatocellular Carcinoma Recurrence After Percutaneous Thermal Ablation
Authors Ghelfi J, Macek Jilkova Z ![]() , Sengel C, Brusset B, Teyssier Y, Costentin C, Mercey-Ressejac M, Dumolard L, Manceau M, Mathieu E, Bricault I, Decaens T
, Sengel C, Brusset B, Teyssier Y, Costentin C, Mercey-Ressejac M, Dumolard L, Manceau M, Mathieu E, Bricault I, Decaens T
Received 4 October 2023
Accepted for publication 16 December 2023
Published 9 January 2024 Volume 2024:11 Pages 39—50
DOI https://doi.org/10.2147/JHC.S443134
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr David Gerber
Julien Ghelfi,1– 3,* Zuzana Macek Jilkova,1,3,4,* Christian Sengel,2 Bleuenn Brusset,4 Yann Teyssier,2 Charlotte Costentin,1,3,4 Marion Mercey-Ressejac,3,4 Lucile Dumolard,1,3 Marc Manceau,5 Eliott Mathieu,2 Ivan Bricault,1,2 Thomas Decaens1,3,4
1University of Grenoble-Alpes, Saint Martin d’Hères, France; 2Department of Radiology, Grenoble-Alpes University Hospital, Grenoble, France; 3Institute for Advanced Biosciences - INSERM U1209/CNRS UMR 5309/University of Grenoble-Alpes, La Tronche, France; 4Department of Hepatology and Gastrointestinal Medical Oncology, Grenoble-Alpes University Hospital, Grenoble, France; 5Clinical Pharmacology Unit, Inserm Clinical Research Center, Grenoble-Alpes University Hospital, Grenoble, France
*These authors contributed equally to this work
Correspondence: Julien Ghelfi, Department of Radiology, Grenoble-Alpes University Hospital, Boulevard de la Chantourne, Grenoble, 38000, France, Tel +33 476768909, Email [email protected] Zuzana Macek Jilkova, Department of Hepato-Gastroenterology, Grenoble-Alpes University Hospital, Boulevard de la Chantourne, Grenoble, 38000, France, Tel +33 669048426, Email [email protected]
Purpose: Percutaneous thermal ablation (PTA) is a cornerstone in the management of early-stage hepatocellular carcinoma (HCC). However, intrahepatic distant recurrence (IDR) occurs in the majority of patients after PTA. The aim of this study was to evaluate the immune signature associated with very early IDR.
Patients and Methods: Thirty-one patients (26 men, 5 women; mean age:72.4 ± 8.6; age range:57– 86 years) who underwent PTA for HCC were included in this study. After PTA for HCC, patients were followed and later divided into two groups: a “very early recurrence” group in case of IDR within 12 months after PTA, and a “prolonged recurrence-free” group in case of no recurrence before 12 months of follow-up. Freshly harvested intratumoral and nontumoral liver tissues and peripheral blood were obtained before PTA and explored by multiparametric flow cytometry.
Results: The frequency of PD1+CD4+ T cells was higher in the early recurrence group than in the prolonged recurrence-free group in the peripheral blood (24.3%, IQR: 22.3– 36.5 vs 14.0%, IQR: 11.5– 16.4, p< 0.0001), in the nontumoral liver (37.9%, IQR: 36.0– 50.0 vs 22.5%, IQR: 18.0– 29.9, p=0.0004), and in the tumor (37.6%, IQR: 32.3– 39.3 vs 24.0%, IQR: 20.0– 30.3, p=0.0137). Similarly, the frequency of TIM+CD8+ T cells was higher in the very early recurrence group in the peripheral blood (p=0.0021), non-tumoral liver (p=0.0012), and tumor (p=0.0239).
Conclusion: The expression of immune checkpoint molecules, such as PD1 and TIM3 on T cells identified HCC patients at risk of very early IDR after PTA who would likely benefit from adjuvant immunotherapy. Thus, our study contributes to a better understanding of the potential association of PTA with adjuvant immunotherapies.
Keywords: immune checkpoint molecules, predictive factors, hepatocellular carcinoma, percutaneous thermal ablation, intrahepatic distant recurrence
Introduction
Percutaneous thermal ablation (PTA), including radiofrequency ablation (RFA)1 and microwave ablation (MWA),2 is a cornerstone of the management of early-stage hepatocellular carcinoma (HCC), together with surgical resection and liver transplantation.3–5 PTA offers several advantages over surgery, such as a lower risk of complications, better tissue preservation, a lower cost, and a shorter hospital stay.1 Despite the benefits, the rate of tumor recurrence after PTA therapy is still high. Intrahepatic distant recurrence (IDR) occurs in 60 to 80% of patients at 5 years after PTA,1,5–7 similar to HCC surgical resection.4,8 A cohort of 412 patients with small HCC who underwent PTA recently showed that IDR occurred in 47.1% of patients, and after a median time of only 8.4 months.9 Alpha-fetoprotein (AFP) >100 ng/mL and tumor size were found to be predictive factors for IDR,9 as well as multifocal lesions.10
During the last decade, immunotherapies, mainly immune checkpoint inhibitors (ICIs), have emerged as promising cancer therapies.11 While targeting the programmed cell death 1 (PD1) pathway in monotherapy failed to achieve statistically significant improvement in HCC patients,12 the combination of atezolizumab (anti-PD-L1) and bevacizumab (anti-VEGF) has shown better overall and progression-free survival outcomes than sorafenib in patients with unresectable HCC.13 One of the main challenges in HCC is the identification and validation of biomarkers that predict response to immunotherapies.14 Immune factors in the tumor microenvironment and circulation are among the predictive biomarkers currently being studied.15,16
To increase the treatment efficacy, combined approaches of immunotherapies with loco-regional treatments are also being explored, including PTA.1,17,18 PTA techniques induce immunomodulation in patients with HCC by releasing cell death components that initiate a local inflammatory response.1,19,20 Tumor-specific antigens become accessible to the whole immune system, triggering an antitumor response.21,22 However, this immunomodulation seems to be insufficient to obtain a prolonged immune response by itself.19 Given the importance of the immune system, different baseline immune patterns could be responsible for different immune responses after PTA and could impact tumor recurrence. Recent translational studies have begun to unravel the crucial contribution of systemic immunity to an antitumor immune response.23
The primary objective of this study was to evaluate the expression of immune checkpoint molecules (ICM) on intrahepatic (tumor and nontumor) and peripheral lymphocytes of HCC patients undergoing PTA and to investigate the possible association with the risk of very early IDR.
Materials and Methods
Study Population
This study was a retrospective analysis of samples from a prospective single-center cohort (biological collection registered AC-2019-3627), including all patients aged >18 years who underwent PTA for histologically-proven HCC between April 2018 and November 2021. This study was conducted according to the guidelines of the Declaration of Helsinki, and protocol was reviewed and approved by the “Comité d’éthique de la recherche en imagerie médicale - CERIM (approval number [CRM-2204-253]”. Written informed consent was obtained from all participants.
The exclusion criteria were as follows: no pathologic evidence of HCC, no immunophenotyping at the time of sampling performed before or at ablation, a diagnosis other than HCC, and no follow-up of less than 12 months. Initial incomplete ablation or local recurrence at the PTA site were also considered as exclusion criteria.
Percutaneous Thermal Ablation
Ablation procedures were performed either by radiofrequency ablation (RFA) using a Leveen™ needle and an RF 3000 ablation generator (Boston Scientific) or by microwave ablation (MWA) using an Amica™ needle and an HS-Amica-Gen generator (Ablatech). The ablation procedures were performed by one of the three participating interventional radiologists with 30, 7, and 5 years of experience. Non-tumoral and tumoral liver samples were taken under ultrasound guidance prior to treatment (during a biopsy procedure to characterize the tumor or just before the ablation procedure). Non-tumoral and tumoral samples between 13 mm and 23 mm, depending on the size of the nodule, were obtained using an 18G needle. At both locations (tumor and non-tumor), two samples were conditioned in formalin for conventional pathological analysis, and one was conditioned in Hypothermosol™ FRS solution for immunophenotyping. Peripheral blood sampling was performed at the same time as biopsy sampling and in all cases before ablation.
Multiparametric Flow Cytometry Analyses
Freshly harvested intratumoral and nontumoral liver tissues, obtained by needle liver biopsy, were transferred to Hypothermosol™ FRS solution, and cells were recovered through mechanical disruption. Samples of whole fresh peripheral blood (100 µL/tube) and intrahepatic cell suspensions were divided into two tubes and immunostained with the following anti-human antibodies for surface markers: anti-CD45-APC/Cy7 (clone HI30, BioLegend), anti-CD3-PerCP-Cy5.5 (clone UCHT1, BioLegend), anti-CD56-BV605 (clone HCD56, BioLegend), anti-CD16-AF700 (clone 3G8, BioLegend), anti-CD8-PE/Cy7 (clone RPA-T8, BD Biosciences), anti-CD69-PE (clone FN50, BioLegend), anti-CTLA4-BV421 (clone BNI3, BioLegend), anti-PD-1-BV711 (clone EH12.2H7, BioLegend), anti-LAG3-PE (clone 3DS223H, eBioscience), anti-OX40-FITC (clone Ber-ACT35, BioLegend), anti-4-1BB-BV421 (clone 4B4-1, BioLegend), and anti-TIM3-BV785 (clone F39-2E2, BioLegend). FluoroFix™ Buffer (BioLegend) was used to fix the cells. The Zombie UV™ Fixable Viability kit was used to exclude dead cells, and fluorescence minus one controls were used to determine the positive immune cell population. Data were acquired with the BD-LSRII flow cytometer (BD Biosciences), collected using BD FACSDiva 6.3.1 software and analyzed using FCS Express 7 Flow software, using the previously described gating strategy,24 Figure S1.
Study Objectives and Endpoints
During follow-up, patients were divided into two groups, a “very early recurrence” group in case of IDR within 12 months after PTA and a “prolonged recurrence-free” group in case of no recurrence before 12 months of follow-up. IDR was defined as the recidivism of HCC in the liver at distance from the ablated area and was considered as the time between the PTA procedure and cross-sectional imaging (CT or MRI) demonstrating recurrence. Recurrence at the ablation site was considered an insufficient PTA responsible for local recurrence and was an exclusion criterion. Follow-up was achieved through a combination of clinical examination and imaging (CT scan or MRI) one month after PTA, every 3 months over 2 years, and subsequently every 6 months over the next 3 years. The primary objective of this study was to compare the expression of PD1 on T cells between the “very early recurrence” and “prolonged recurrence-free” group. The frequency of PD1+ T cells in the CD4+ T cell population and the CD8+ T cell population was compared between the two groups using samples from tumor, nontumoral liver and circulating blood. The secondary objectives evaluated the expression of other ICM-positive cells in T cell populations between the two groups. The frequency of the following ICM-positive cells in CD4+ T cells and CD8+ T cells were compared between the two groups from tumoral, nontumoral liver and circulating blood samples: T cell immunoglobulin and mucin domain-containing protein 3 (TIM3), lymphocyte-activation gene 3 (LAG3), cytotoxic T-lymphocyte antigen 4 (CTLA4), stimulatory inducible T cell co-stimulator (ICOS), OX40 and 4–1BB+.
Statistical Analysis
Standard descriptive statistics were used for continuous quantitative variables, presented as medians and interquartile ranges (or mean and standard deviation when normally distributed), and for qualitative variables, presented as numbers and percentages. Analyses were performed using the statistical software GraphPad Prism 9 (GraphPad Software) as well as the R software (R Core Team). Comparisons between groups of continuous data rely on a Mann–Whitney test, while comparisons between groups of Boolean data relied on the chi-square test; all tests performed were two-sided comparison tests. We report all p-values < 0.05 but caution the reader about the exploratory nature of these tests. Considering a significance threshold of 0.05 allows us on the one hand to identify more interesting variables that will require further investigation in the future. However, it might lead to an overall high number of false positives. Instead, a Bonferroni correction with the total number of tests performed (approximately 100) led to a significance threshold of 5.10–4 to keep the study false positive discovery rate below 0.05.
Results
Patient Inclusion
During the study period, 142 HCC patients were treated with PTA, among whom 40 (28.2%) did not have a biopsy and 52 (36.6%) did not have samples for immunophenotyping and were thus excluded. Five patients (3.5%) had incomplete PTA or local recurrence, 12 patients (8.5%) had different storage of immune samples (paraffin), and 2 patients (1.4%) had follow-up of less than 12 months without recurrence (shown in Figure 1). Finally, 31 patients were included, of whom 26 patients were male (83.9%) and 5 (16.1%) were female. The mean age was 72.4 ± 8.6 (age range: 57–86 years).
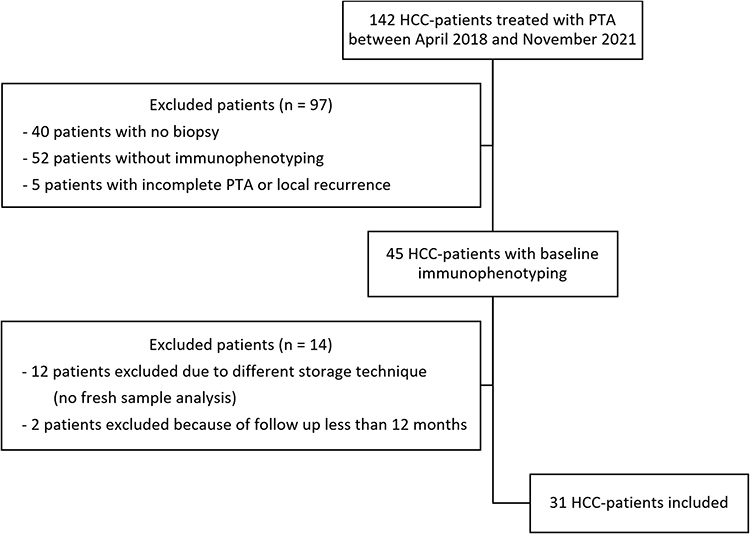 |
Figure 1 Flowchart of the study. |
Patients’ Characteristics
Table 1 shows the characteristics of the study population. Among the 31 patients included in the study, 9 patients (29%) were later categorized into the very early recurrence group and 22 patients (71%) into the prolonged recurrence-free group. Patients were treated with RFA (12 patients (38.7%)) and with MWA (19 patients (61.3%)). The mean tumor diameter was 22.8 mm ± 7.5, and 2 patients (6.5%) had bifocal HCC. The median follow-up time after PTA was 23.5 months [IQR:17.9–29.5] in the prolonged recurrence-free group and 19.0 months [IQR:14.3–32.5] in the very early recurrence group (p=0.28). In the very early recurrence group, the median time between PTA and IDR was 4.5 months [IQR: 3.1–9] (shown in Figure 2A), and 2 patients (22%) died during the follow-up period. In the prolonged recurrence-free group, three patients (13.6%) experienced IDR 35 months, 47 months, and 48 months respectively after PTA, and one patient (4.5%) died 20.9 months after PTA of acute kidney failure, without any HCC recurrence.
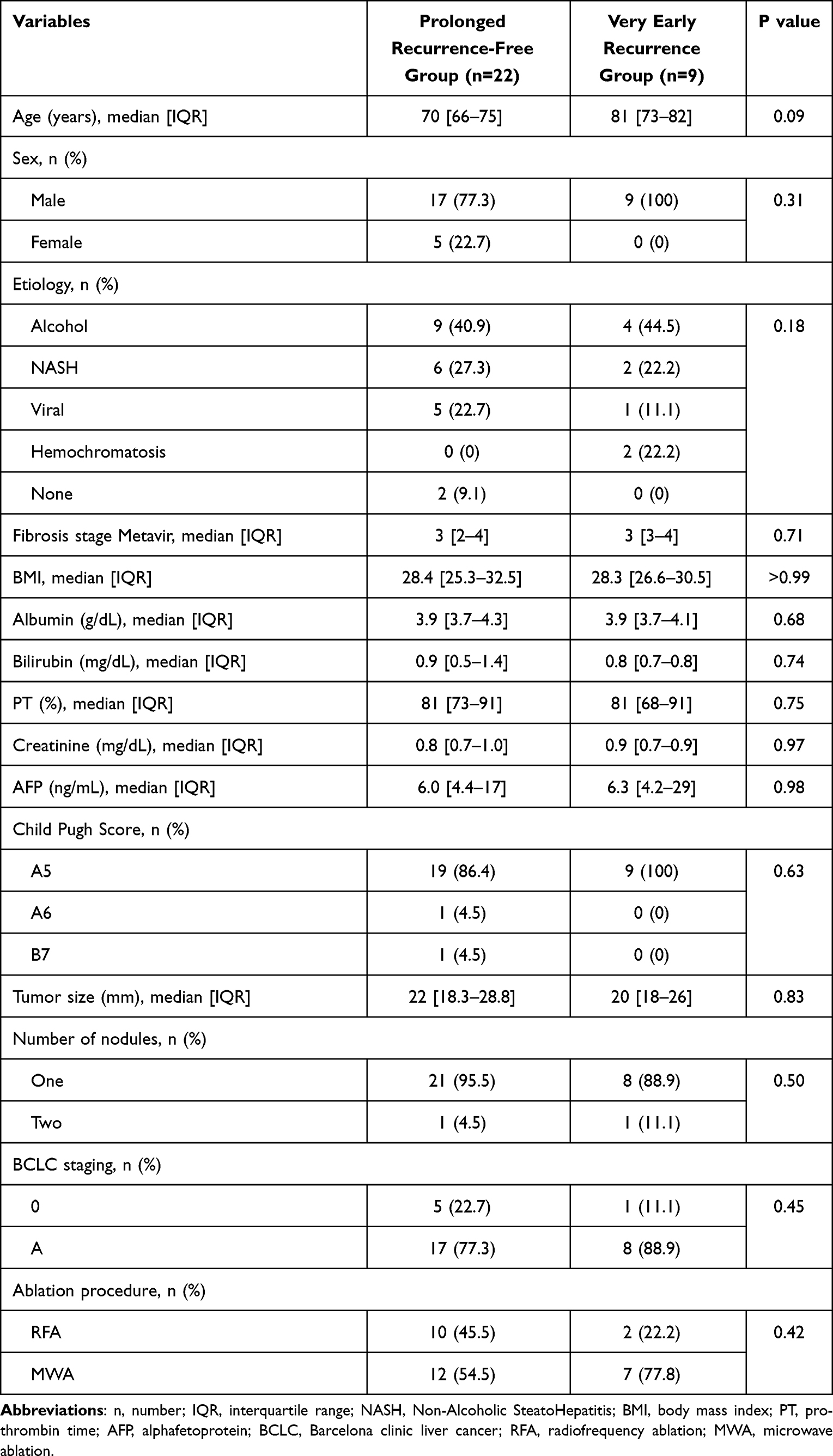 |
Table 1 Patients’ Characteristics |
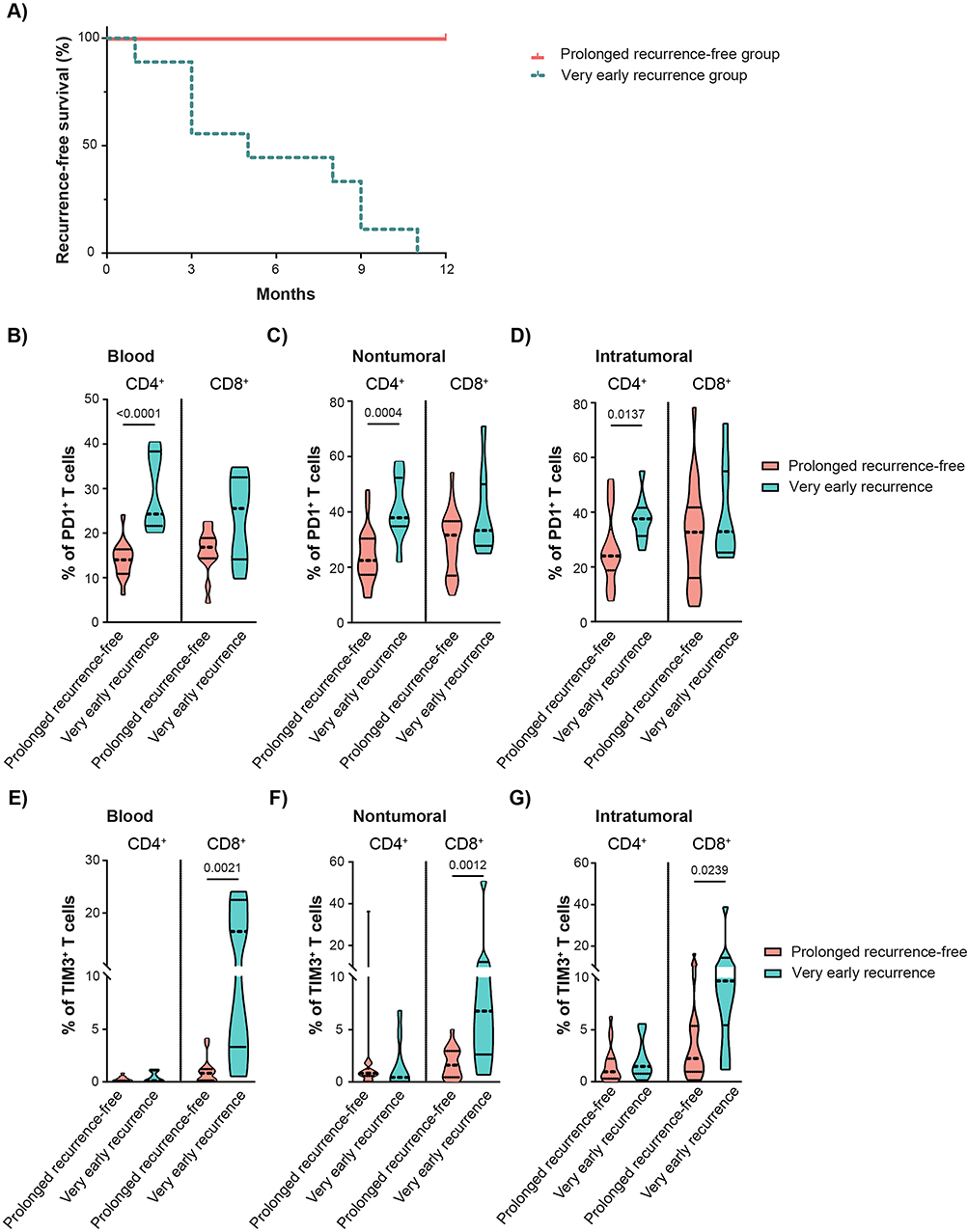 |
Figure 2 Immune signature associated with very early HCC recurrence after PTA. (A) Recurrence-free survival of thirty-one patients included in the study: 9 patients (29%) were later categorized into the very early recurrence group and 22 patients (71%) into the prolonged recurrence-free group. The median time between ablation procedure and intrahepatic distant recurrence was 4.5 months [IQR:3.1–9] in the very early recurrence group. (B) The frequencies of circulating PD1+ T cells compared between “prolonged free recurrence group” and “very early recurrence group”. The frequencies of PD1+ T cells, (C) in nontumoral and (D) in tumoral biopsies. (E) The frequencies of circulating TIM3+ T cells. The frequencies of TIM3+ T cells, (F) in nontumoral and (G) in tumoral biopsies. The violin plots show the distribution of the data, with median and quartiles. |
The Frequencies of Immune Cells
The median frequency of peripheral blood T cells per CD45+ cell was 62.5% [IQR: 56.8–71.3] in the very early recurrence group versus 63.2% [IQR: 56.8–69] in the prolonged recurrence-free group (p=0.84), Table S1. The frequency of T cells was also similar between the two groups in nontumoral liver (38.4%, IQR: 31.0–50.0 vs 44.3% IQR: 36.0–49.0, p=0.56) and in intratumoral tissue (53.9%, IQR: 47.6–56.5 vs 52.0%, IQR: 44.9–65.5, p=0.92). The frequency of CD4+ or CD8+ T cell subpopulations did not differ between the two groups in peripheral blood, non-tumoral liver, or intratumoral tissue (Table S1). As expected, CD8+ T cells were reduced in intratumoral tissue compared to those in non-tumoral liver.24,25 More precisely, CD8+ T cells represented approximately 35% of the T cell population in the tumor tissue and 46% in the non-tumoral part of the liver. Interestingly, we observed significant correlations between intra-tumoral and non-tumoral immune profile as well as between non-tumoral and blood immune profile. On contrary, the correlation between intra-tumoral profile and blood profile was lower (Figure S2). The frequencies of NK and NKT did not differ between the two groups (Table S1).
The Frequency of PD1+ T Cells
The frequency of circulating PD1+ T cells in the CD4+ T cell population was significantly higher in the very early recurrence group than in the prolonged recurrence-free group in the peripheral blood (24.3%, IQR: 22.3–36.5 vs 14.0%, IQR: 11.5–16.4, p<0.0001), in the nontumoral liver (37.9%, IQR: 36.0–50.0 vs 22.5%, IQR: 18.0–29.9, p=0.0004), and in the tumor (37.6%, IQR: 32.3–39.3 vs 24.0%, IQR: 20.0–30.3, p=0.0137), (shown in Figure 2B-D).
There was no difference in the median frequency of PD1+ T cells in the CD8+ T cell population between the two groups in the peripheral blood (25.6%, IQR: 16.1–30.4 vs 16.9%, IQR: 14.5–18.9, p=0.12), in the nontumoral liver (33.3%, IQR: 27.9–45.6 vs 31.6%, IQR: 18.8–36.2, p=0.18), and in the tumors (32.9%, IQR: 26.5–50.7 vs 32.7%, IQR: 18.3–40.3, p=0.38), Figure 2B-D, Table 2.
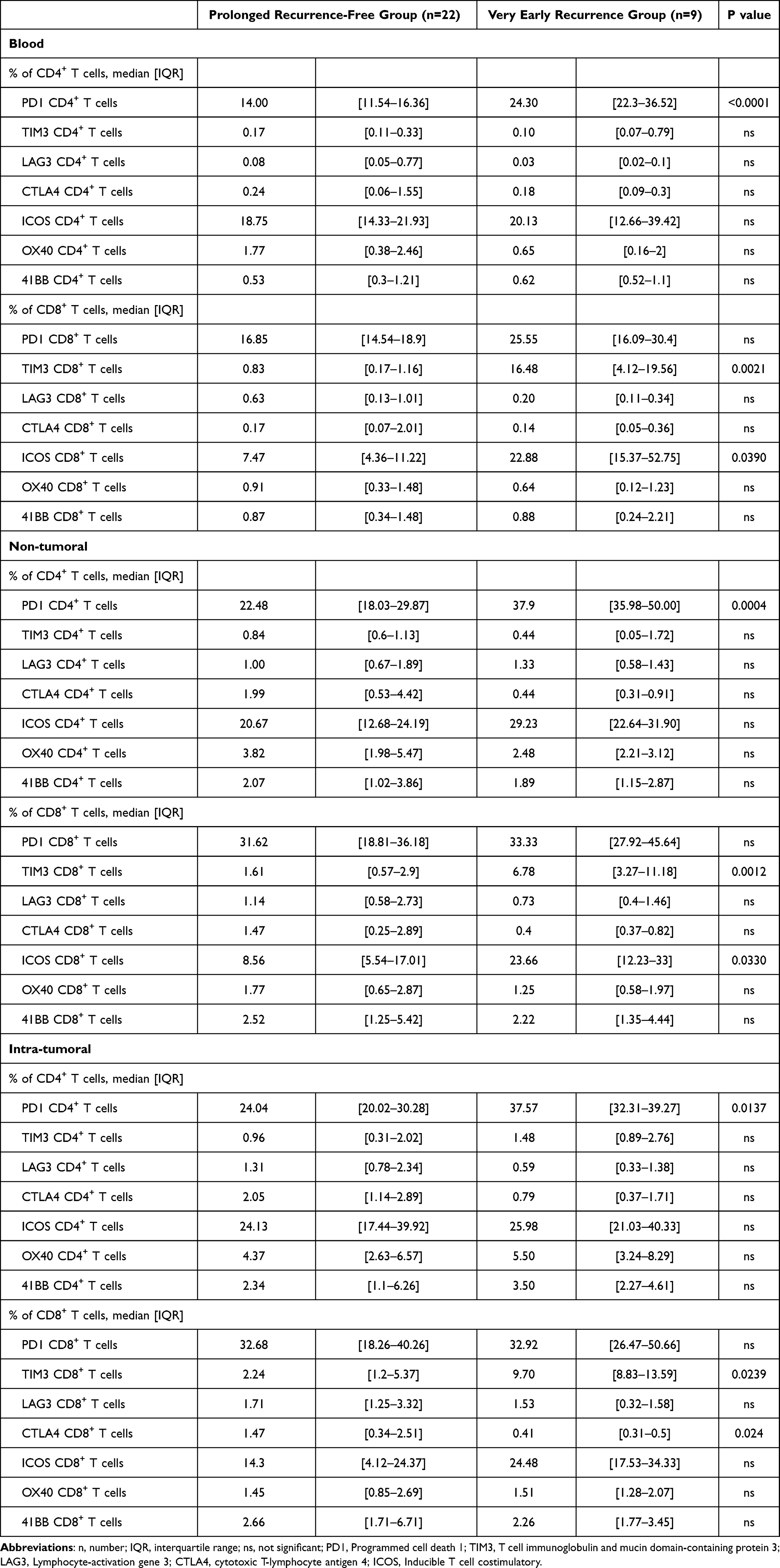 |
Table 2 The Baseline Frequency of T Cells Expressing Immune Checkpoint Molecules in Peripheral Blood, Nontumoral and Intratumoral Liver Tissue |
The Frequency of Others ICM Positive T Cells
The frequency of TIM3+ cells in the CD8+ T cell population was also higher in the very early recurrence group in the peripheral blood (16.5%, IQR: 4.1–19.6 vs 0.8%, IQR: 0.2–1.2, p=0.0021), in nontumoral liver (6.8%, IQR: 3.3–11.2 vs 1.6%, IQR: 0.6–2.9, p=0.001) and in the tumor (9.7%, IQR: 8.8–13.6 vs 2.2%, IQR: 1.2–5.4, p=0.0239) (shown in Figure 2E-G).
No difference was observed in other ICM explored on CD4+ T cells or CD8+ T cells, apart from a slightly higher frequency of circulating ICOS+ cells in the CD8+ T cell population in the very early recurrence group compared with the prolonged recurrence-free group in the circulating blood (22.9%, IQR: 15.4–52.8 vs 7.5%, IQR: 4.4–11.2, p=0.0390) and in nontumoral liver (23.7%, IQR: 12.2–33.0 vs 8.6%, IQR: 5.5–17.0, p=0.0330) but not in the tumor (Table 2).
Association of ICM Expression in the Circulating Blood with IDR
In our cohort of patients, the frequencies of PD1 expression on CD4+ T cells and TIM3 expression on CD8+ T cells on circulating blood before PTA were associated with the clinical outcomes. Contrary to patients with prolonged recurrence free survival (Figure 3A and B), patients with high frequency of CD4+ PD1+ T cells and CD8+ TIM3+ T cells were frequently associated with very early recurrence at distance from the site of PTA on cross-sectional imaging (Figure 3C-G). Importantly, the most discriminative variable was the frequency of PD1 expression on CD4+ T cells, with a clear threshold at 20%. All individuals in the very early recurrence group were found to have a frequency above this threshold, while only one individual from the prolonged recurrence-free group was found above this threshold.
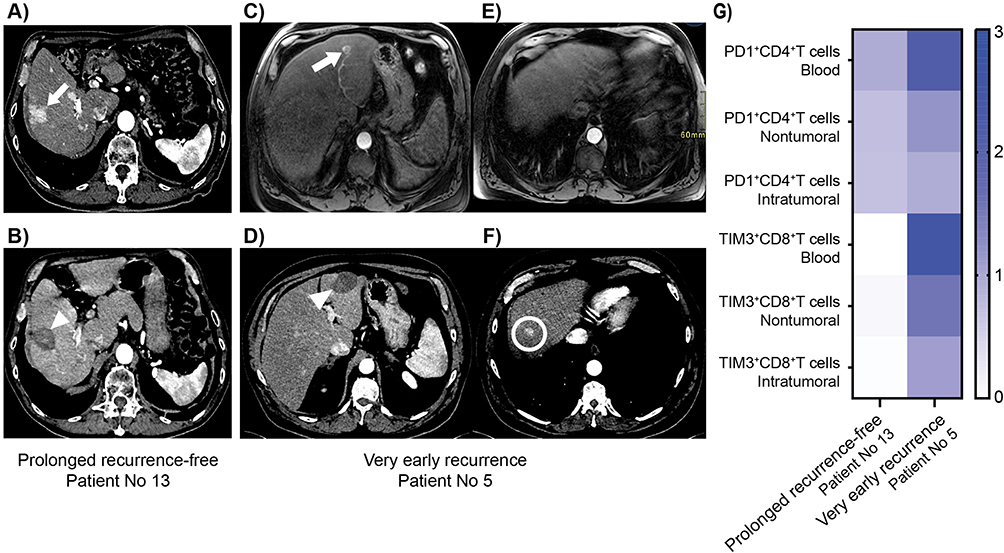 |
Figure 3 Imaging and immunological profiles of representative patients. (A) Arterial phase axial abdominal CT scan in a 73-year-old man (patient No 13) shows a single 28-mm right liver HCC (white arrow) with peripheral perfusional disturbances at baseline. (B) Arterial phase axial abdominal CT scan of the same patient 45 months after percutaneous thermal ablation shows the ablated area (white arrowhead) without any recurrence. (C) and (E) Arterial phase axial abdominal MRI in a 66-year-old man (patient No 5) shows a single 18-mm left liver HCC (white arrow) at baseline. (D and F) Arterial phase axial abdominal CT scan in the same patient 9 months after percutaneous thermal ablation shows no recurrence at the ablated area (white arrowhead) but a very early intrahepatic distant recurrence in segment VIII (white circle). (G) Immunological profiles of patients No 13 and 5 at baseline. Results are expressed as a heat map-based frequency of positive cells compared with the mean frequency of a corresponding subpopulation of cells of the entire cohort; higher than the mean in dark blue. |
Discussion
This study showed that the frequency of PD1+ CD4+ T cells and TIM3+ CD8+ T cells at baseline was significantly higher in patients with very early IDR than in patients with prolonged recurrence-free survival after PTA for HCC in peripheral blood, nontumoral liver, and in the tumor. Overall, our data revealed an immunological profile associated with early IDR. This profile is characterized by the immunosuppressive status of T cells in circulation and in the liver; however, the most important differences were observed in the circulating blood and in the non-tumoral tissue, demonstrating the relevance of systemic and non-tumoral liver immunity for tumor recurrence. Moreover, in circulating blood, the frequency of PD1+ CD4+ T cells was found to be the most discriminative parameter for predicting very early recurrence. Frequency thresholds of PD1+ CD4+ T cells > 20% in peripheral blood were associated with an increased risk of very early recurrence. We hypothesized that an even better diagnostic test could be designed by logistic regression considering the frequencies of PD1+ CD4+ and TIM3+ CD8+. Further work on future larger cohorts is required to confirm the findings observed here and further characterize the sensitivity and specificity of such a test.
The specific expression of ICM in this study was consistent with previous observations. While PD-1 expression is expected on both CD4+ and CD8+ T cells, TIM3 is known to be preferentially expressed on CD8+ T cells.26 Although the majority of studies have focused on intratumoral PD1+ CD8+ T cells, our results highlight the importance of the PD-1 expressing CD4+ T cell population for early IDR, suggesting that functional systemic immunity is largely dependent on CD4+ T cells.27
Studies to evaluate the safety and efficacy of thermal ablation with immunotherapy for HCC are currently ongoing.1,28,29 Recently, the IMbrave050 trial reported a significantly improved recurrence-free survival in HCC patients treated with local therapy (surgery or PTA) and adjuvant atezolizumab plus bevacizumab compared with local therapy alone.30 In this study, the majority of patients underwent surgery as local therapy, but about 12% of patients underwent PTA, indicating interest in this combined approach. Patients included in the IMBrave050 trial had a high risk of recurrence such as size >2 cm for PTA with a median diameter of 25 mm, not so different from the mean diameter of 22.8 mm in our study. Tumor heterogeneity is a major challenge in this context,31 and the selection of patients treated with PTA who would benefit from combined immunotherapy is paramount. A pilot study of 39 patients combining anti-CTLA4 therapy and ablation confirmed the feasibility of this association and showed that the frequency of CD4+ PD1+ cells among peripheral blood mononuclear cells at baseline was higher in patients responding to therapy than in non-responding patients.32 Higher levels of PD1+ CD4+ T cells were also associated with a better response to immune checkpoint inhibitors in lung cancer.33 As suggested by our data, if the same category of patients is at risk of early IDR after ablation, the combination of PTA with immune checkpoint blockade targeting PD1 and TIM3 should be explored in this specific population.
One limitation of this study was the small cohort size. The difference in the distribution of ablation techniques and sex between the two groups may also be discussed, although the difference was not statistically significant. Similar to other HCC studies, the current study was performed on a relatively small sample of tissue obtained via needle biopsy, which could limit the accuracy of the description of the heterogeneous landscape of the liver immune microenvironment. However, our data revealed that the main immunological differences between patients with very early IDR and patients with prolonged recurrence-free survival after PTA for HCC can be observed at the peripheral blood level. Additionally, immunomonitoring of peripheral blood after PTA would also have provided interesting information, as systemic modulation was reported after PTA34,35 and should be explored in the future.
Conclusion
This study highlights the importance of the baseline systemic immunosuppressive status, mainly PD1 expression on CD4+ T cells and TIM3 expression on CD8+ T cells, as a predictive factor for very early intrahepatic distant recurrence after PTA. These results may be of interest to better understand the future association of PTA with adjuvant immunotherapies to prevent very early tumor recurrence. Further studies are needed to confirm this pilot study.
Acknowledgments
We thank Dr M. Pezet for supervising the Flow-Cytometry MicroCell platform. This study has received funding by grants from “Fonds Agir pour les Maladies Chroniques” (France) and “Association Française pour l’Etude du Foie – AFEF” (France).
Disclosure
Prof. Dr. Charlotte Costentin reports grants, personal fees, non-financial support from Gilead, non-financial support from Ipsen, personal fees, non-financial support from AbbVie, RNPC, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Wang H, Wu Z, Cui D, Shi Y, Zhai B. Radiofrequency ablation of hepatocellular carcinoma: current status, challenges, and prospects. Liver Res. 2023;7(2):108–115. doi:10.1016/j.livres.2023.05.002
2. Dong TT, Wang L, Li M, Yin C, Li YY, Nie F. Clinical Results, Risk Factors, and Future Directions of Ultrasound-Guided Percutaneous Microwave Ablation for Hepatocellular Carcinoma. J Hepatocell Carcinoma. 2023;10:733–743. doi:10.2147/jhc.S409011
3. Huber TC, Bochnakova T, Koethe Y, Park B, Farsad K. Percutaneous Therapies for Hepatocellular Carcinoma: evolution of Liver Directed Therapies. J Hepatocell Carcinoma. 2021;8:1181–1193. doi:10.2147/jhc.S268300
4. Galle PR. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
5. Nault JC, Sutter O, Nahon P, Ganne-Carrie N, Seror O. Percutaneous treatment of hepatocellular carcinoma: state of the art and innovations. J Hepatol. 2018;68(4):783–797. doi:10.1016/j.jhep.2017.10.004
6. Livraghi T, Meloni F, Di Stasi M, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice? Hepatology. 2008;47(1):82–89. doi:10.1002/hep.21933
7. N’Kontchou G, Mahamoudi A, Aout M, et al. Radiofrequency ablation of hepatocellular carcinoma: long-term results and prognostic factors in 235 Western patients with cirrhosis. Hepatology. 2009;50(5):1475–1483. doi:10.1002/hep.23181
8. Imamura H, Matsuyama Y, Tanaka E, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. 2003;38(2):200–207. doi:10.1016/s0168-8278(02)00360-4
9. Hermida M, Cassinotto C, Piron L, et al. Multimodal Percutaneous Thermal Ablation of Small Hepatocellular Carcinoma: predictive Factors of Recurrence and Survival in Western Patients. Cancers. 2020;12(2):313. doi:10.3390/cancers12020313
10. Preel A, Hermida M, Allimant C, et al. Uni-, Bi- or Trifocal Hepatocellular Carcinoma in Western Patients: recurrence and Survival after Percutaneous Thermal Ablation. Cancers. 2021;13(11):2700. doi:10.3390/cancers13112700
11. Versluis JM, Long GV, Blank CU. Learning from clinical trials of neoadjuvant checkpoint blockade. Nature Med. 2020;26(4):475–484. doi:10.1038/s41591-020-0829-0
12. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, Phase 3 trial. Lancet Oncol. 2021;23(1):77–90. doi:10.1016/s1470-2045(21)00604-5
13. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
14. Macek Jilkova Z, Ghelfi J, Decaens T. Immunomodulation for hepatocellular carcinoma therapy: current challenges. Current Opinion Oncol. 2022;34(2):155–160. doi:10.1097/cco.0000000000000812
15. Ji JH, Ha SY, Lee D, et al. Predictive Biomarkers for Immune-Checkpoint Inhibitor Treatment Response in Patients with Hepatocellular Carcinoma. Int J Mol Sci. 2023;24(8):7640. doi:10.3390/ijms24087640
16. Macek Jilkova Z, Aspord C, Decaens T. Predictive Factors for Response to PD-1/PD-L1 Checkpoint Inhibition in the Field of Hepatocellular Carcinoma: current Status and Challenges. Cancers. 2019;11(10):1554. doi:10.3390/cancers11101554
17. Tischfield DJ, Gurevich A, Johnson O, et al. Transarterial Embolization Modulates the Immune Response within Target and Nontarget Hepatocellular Carcinomas in a Rat Model. Radiology. 2022:211028. doi:10.1148/radiol.211028
18. Zhu J, Yu M, Chen L, et al. Enhanced antitumor efficacy through microwave ablation in combination with immune checkpoints blockade in breast cancer: a pre-clinical study in a murine model. Diagn Interventional Imaging. 2018;99(3):135–142. doi:10.1016/j.diii.2017.12.011
19. Dumolard L, Ghelfi J, Roth G, Decaens T, Macek Jilkova Z. Percutaneous Ablation-Induced Immunomodulation in Hepatocellular Carcinoma. Int J Mol Sci. 2020;21(12):4398. doi:10.3390/ijms21124398
20. Takaki H, Cornelis F, Kako Y, Kobayashi K, Kamikonya N, Yamakado K. Thermal ablation and immunomodulation: from preclinical experiments to clinical trials. Diagn Interventional Imaging. 2017;98(9):651–659. doi:10.1016/j.diii.2017.04.008
21. Li L, Wang W, Pan H, et al. Microwave ablation combined with OK-432 induces Th1-type response and specific antitumor immunity in a murine model of breast cancer. J Transl Med. 2017;15(1):23. doi:10.1186/s12967-017-1124-9
22. Huang KW, Jayant K, Lee PH, et al. Positive Immuno-Modulation Following Radiofrequency Assisted Liver Resection in Hepatocellular Carcinoma. J Clin Med. 2019;8(3):385. doi:10.3390/jcm8030385
23. Hiam-Galvez KJ, Allen BM, Spitzer MH. Systemic immunity in cancer. Nat Rev Cancer. 2021;21(6):345–359. doi:10.1038/s41568-021-00347-z
24. Macek Jilkova Z, Aspord C, Kurma K, et al. Immunologic Features of Patients With Advanced Hepatocellular Carcinoma Before and During Sorafenib or Anti-programmed Death-1/Programmed Death-L1 Treatment. Clin Transl Gastroenterol. 2019;10(7):e00058. doi:10.14309/ctg.0000000000000058
25. Li Z, Zheng B, Qiu X, et al. The identification and functional analysis of CD8+PD-1+CD161+ T cells in hepatocellular carcinoma. Npj Precision Oncology. 2020;4(1):28. doi:10.1038/s41698-020-00133-4
26. Liu F, Liu Y, Chen Z. Tim-3 expression and its role in hepatocellular carcinoma. J Hematol Oncol. 2018;11(1):126. doi:10.1186/s13045-018-0667-4
27. Tay RE, Richardson EK, Toh HC. Revisiting the role of CD4(+) T cells in cancer immunotherapy-new insights into old paradigms. Cancer Genet Ther. 2021;28(1–2):5–17. doi:10.1038/s41417-020-0183-x
28. Erinjeri JP, Fine GC, Adema GJ, et al. Immunotherapy and the Interventional Oncologist: challenges and Opportunities-A Society of Interventional Oncology White Paper. Radiology. 2019;292(1):25–34. doi:10.1148/radiol.2019182326
29. Wang K, Wang C, Jiang H, et al. Combination of Ablation and Immunotherapy for Hepatocellular Carcinoma: where We Are and Where to Go. Front Immunol. 2021;12:792781. doi:10.3389/fimmu.2021.792781
30. Qin S, Chen M, Cheng AL, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;402(10415):1835–1847. doi:10.1016/s0140-6736(23)01796-8
31. Kurebayashi Y, Ojima H, Tsujikawa H, et al. Landscape of immune microenvironment in hepatocellular carcinoma and its additional impact on histological and molecular classification. Hepatology. 2018;68(3):1025–1041. doi:10.1002/hep.29904
32. Agdashian D, ElGindi M, Xie C, et al. The effect of anti-CTLA4 treatment on peripheral and intra-tumoral T cells in patients with hepatocellular carcinoma. Cancer Immunol Immunother. 2019;68(4):599–608. doi:10.1007/s00262-019-02299-8
33. Inomata M, Kado T, Okazawa S, et al. Peripheral PD1-positive CD4 T-Lymphocyte Count Can Predict Progression-free Survival in Patients With Non-small Cell Lung Cancer Receiving Immune Checkpoint Inhibitor. Anticancer Res. 2019;39(12):6887–6893. doi:10.21873/anticanres.13908
34. Leuchte K, Staib E, Thelen M, et al. Microwave ablation enhances tumor-specific immune response in patients with hepatocellular carcinoma. Cancer Immunol Immunother. 2021;70(4):893–907. doi:10.1007/s00262-020-02734-1
35. Rochigneux P, Nault JC, Mallet F, et al. Dynamic of systemic immunity and its impact on tumor recurrence after radiofrequency ablation of hepatocellular carcinoma. Oncoimmunology. 2019;8(8):1615818. doi:10.1080/2162402x.2019.1615818
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.