Back to Journals » Infection and Drug Resistance » Volume 16
Patterns of Drug Resistance and Bacterial Pathogen Distribution in Patients with Urinary Tract Infections in the Jiaxing Region from 2020 to 2022
Authors Niu X, Hou B, Yang L, Wang W, Yu Q, Mao M, Shen W
Received 9 July 2023
Accepted for publication 31 August 2023
Published 6 September 2023 Volume 2023:16 Pages 5911—5921
DOI https://doi.org/10.2147/IDR.S424158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Xiaoqin Niu, Bolong Hou, Lunyun Yang, Wei Wang, Qinlong Yu, Minjie Mao, Weifeng Shen
Department of Clinical Laboratory, The First Hospital of Jiaxing, The Affiliated Hospital of Jiaxing University, Jiaxing, 314000, People’s Republic of China
Correspondence: Weifeng Shen, Department of Clinical Laboratory, The First Hospital of Jiaxing, The Affiliated Hospital of Jiaxing University, No. 1882, Zhonghuan South Road, Nanhu District, Jiaxing, Zhejiang, 314000, People’s Republic of China, Tel +86-18868345828, Email [email protected]
Background: Urinary tract infections (UTIs) and the antibiotic resistance of pathogenic bacteria pose severe threats to public health in the current healthcare environment.
Objective: The purpose of this study was to assess the frequency distribution of bacterial pathogens causing UTIs as well as the characteristics of antibiotic susceptibility and resistance.
Methods: The retrospective study was conducted on 32,391 samples of midstream urine culture from January 1, 2020, to December 31, 2022, in Jiaxing. Bacteria were cultivated on blood agar and identified using MALDI-TOF, and their susceptibility to different antibiotics was assessed using the Kirby-Bauer disk diffusion method and drug sensitivity reaction cards. The SPSS 22 software was used for data analysis. Bivariate logistic regression was used to analyze the risk factors for multidrug resistance.
Results: The total number of positive growth samples was 5378 (16.6%), including 3206 females (59.6%) and 2172 males (40.4%). The four most common urinary pathogens were Escherichia coli (39.2%), Enterococcus faecalis (12.4%), Klebsiella pneumoniae (7.6%), and Enterococcus faecium (7.6%). As far as antibiotic resistance was concerned, Escherichia coli had a greater than 50% resistance rate to ampicillin (76.1%), ciprofloxacin (58.6%), and levofloxacin (51.2%). The multidrug resistance rate was high (41.8%). Low levels of resistance were seen to ertapenem (0.1%), imipenem (0.7%), meropenem (0.7%), piperacillin/tazobactam (0.7%), and nitrofurantoin (1.8%). Klebsiella pneumoniae was highly sensitive to ertapenem (100%). The resistance rates to nitrofurantoin, ceftriaxone, and ciprofloxacin were 37.4%, 37.1%, and 35.1%, respectively. Up to 41% of Escherichia coli strains and 26% of Klebsiella pneumoniae strains produced extended-spectrum lactamases (ESBL). Two species of enterococci were highly sensitive to tigecycline and linezolid (100%), and a small number of norvancomycin-resistant strains (0.2%/two strains) were found.
Conclusion: Escherichia coli and Enterococcus faecium were the most common urinary pathogens in this study. The isolated pathogens showed different sensitivity patterns. Antibiotics should be selected reasonably according to the sensitivity mode of pathogenic bacteria to effectively treat and prevent urinary tract infections.
Keywords: antibiotic resistance, urinary tract infections, pathogenic bacteria, urine culture
Introduction
Urinary tract infections (UTIs) are one of the most prevalent infections caused by both gram-positive and gram-negative bacteria, as well as certain fungi.1,2 Data shows that more than 150 million individuals worldwide experience UTIs each year,3 and 50% of them will be infected at least once in their lifetimes.4 The morbidity and economic costs, especially in developing countries, are substantial and deplete a lot of human resources.5 Risk factors for UTIs include poor hygiene habits, sexual activity, vaginal infections, diabetes, obesity, catheter use, and genetic susceptibility.2,4,6 According to studies, the most prevalent uropathogens include Escherichia coli (E. coli), Klebsiella pneumoniae (K. pneumoniae), Enterococcus faecium (E. faecium), Enterococcus faecalis (E. faecalis), Streptococcus agalactiae (S. agalactiae), Proteus mirabilis (P. mirabilis), Pseudomonas aeruginosa (P. aeruginosa), Staphylococcus, and other organisms, including Candida spp.6,7 E. coli strains cause 40% of non-community infections and 80% of community-acquired infections.8 Some guidelines allow the treatment of UTIs with empiric antibiotics without the need for urine culture or susceptibility reporting to the causative organism.9 Although this empirical treatment is successful in treating immediate symptoms, it clearly cannot completely eliminate the possibility of recurrence.4 Additionally, due to the increasing prevalence of multidrug-resistant urinary tract pathogens, the current treatment methods are not optimal.4 The rise in antibiotic resistance in UTIs has been attributed to empirical usage, overuse, and the unavailability of innovative medicines, as well as regulatory obstacles.1,8 In recent years, the rapid spread of superbugs and multidrug-resistant bacteria around the world has been one of the biggest problems facing global public health, which seriously threatens human health.1,3,10
International guidelines recommend the use of several antibiotics to treat UTIs, including nitrofurantoin, trimethoprim-sulfamethoxazole, fosfomycin, fluoroquinolones, and beta-lactams.11,12 However, the widespread abuse and overuse of antibiotics led to the rapid development of antibiotic resistance in UTI pathogens, such as the emergence of extended-spectrum beta-lactamases (ESBL) and carbapenemases.11 Recent studies have revealed that the antibiotic resistance of gram-negative urinary tract pathogens varies greatly around the world. A systematic review of drug resistance of urinary tract pathogens in the Asia-Pacific region found that the resistance rate of E. coli to trimethoprim/sulfamethoxazole, ciprofloxacin, and ceftriaxone was 33–90%, the resistance rate to nitrofurantoin was 2.7–31.4%, and the resistance rate to fosfomycin was 1.8%.13 The review from Iran shows that the most effective antibiotics against E. coli were ciprofloxacin, nitrofurantoin, imipenem, and chloramphenicol.14 According to a study from Mexico, K. pneumoniae isolates had poor resistance to amikacin and carbapenems, whereas nitrofurantoin had a median resistance of 52%.9 It has been reported that K. pneumoniae (40.4%) exhibits multidrug resistance more frequently than E. coli (23.3%).15 Unfortunately, some gram-positive cocci (eg, E. faecium and E. faecalis) are resistant to vancomycin, which can lead to a serious and uncontrollable hospital infection.16 These infections could progress into life-threatening diseases if not treated quickly and efficiently, especially in developing countries. Therefore, it is crucial to regularly investigate the microbial pathogens that cause urinary tract infections and assess their susceptibility to antibiotics.
There are many reports in the literature describing the distribution and resistance of pathogenic bacteria in UTIs.15 However, regional differences exist in the distribution and resistance of microorganisms.1 Regular monitoring of pathogenic organisms in UTIs and associated resistance patterns in specific areas can promote the rational use of antibiotics and reduce the emergence of resistant strains. At our institution, antibiotic resistance and drug sensitivity trends among uropathogens have not been thoroughly studied. Therefore, the purpose of this study was to investigate the distribution and antibiotic susceptibility characteristics of pathogenic bacteria in midstream urine cultures of patients in our institution from 2020 to 2022, aiming to provide a reference for the prevention and treatment of UTIs and the rational use of antibiotics and guide recommendations for empiric antibiotic regimens based on these data.
Materials and Methods
Sample Collection
This retrospective study examined routine urine culture data from inpatients and outpatients at Jiaxing First Hospital from January 2020 to December 2022, regardless of age or gender. Each patient includes only one non-repetitive isolate. Patients without obvious bacteriuria were used as an exclusion standard.6 Additionally, findings involving more than three pathogens were also disregarded. The urine samples from 32,391 patients included in the study were cultured, and the identified microbes underwent cultural testing. Age, sex, and laboratory information about the patients’ drug susceptibility, antibiotic resistance, and culture outcomes were also noted.
Bacterial Culture
The same standard microbiological techniques were used to cultivate each sample. Midstream urine samples were collected in sterile tubes and sent to the microbiology laboratory for quantitative incubation within two hours. The urine was inoculated onto blood agar (5% defibrinated sheep blood) plates using a sterile inoculation loop (10 µL). The plates were incubated aerobically for 18–24 hours at 35 °C while the size and shape of the colonies were observed. Urinary tract infections were confirmed by a single bacterial species in the urine specimen reaching a concentration of 105 CFU/mL.17,18
Antimicrobial Susceptibility Tests
Bacterial identification and antimicrobial susceptibility testing of isolates were performed with standard microbiological procedures. Specifically, MALDI-TOF was used to identify the microorganisms, and drug sensitivity response cards (VITEK 2 XL® BioMérieux) along with the Kirby-Bauer disk diffusion method were used to assess the antimicrobial susceptibility of the organisms. In this study, the following drugs were tested for susceptibility: ampicillin, amoxicillin-clavulanic acid, piperacillin/tazobactam, cephazolin, ceftazidime, ceftriaxone, cefoxitin, cefepime, aztreonam, meropenem, imipenem, ertapenem, amikacin, tobramycin, gentamicin, trimethoprim/sulfamethoxazole, ciprofloxacin, levofloxacin, nitrofurantoin, erythromycin, linezolid, penicillin G, tetracycline, tigecycline, and vancomycin. Based on the CLSI 2020 criteria (Clinical and Laboratory Standards Institute), these data were interpreted. According to the CLSI criteria, the drug sensitivity reports were divided into three categories: susceptible (S), intermediate (I), and resistant (R). Moreover, the Shanghai Clinical Laboratory Center contributed the quality control strains Escherichia coli ATCC25922, Staphylococcus aureus ATCC25923, Pseudomonas aeruginosa ATCC27853, Enterococcus avium ATCC700327, and Klebsiella pneumoniae ATCC700324 for use.
Statistical Analysis
Patient characteristics (gender and age) are expressed by frequency and proportion. Multidrug resistance (MDR) is defined as resistance to at least one antimicrobial agent in three or more classes of antibiotics. The sensitivity test findings were examined using WHONET 5.6 software (WHO, Geneva, Switzerland). The resistance of different isolates to antibiotics was reported as a percentage. The 95% confidence interval (95% CI) ratio of antibiotics to multidrug resistance was calculated. Binary logistic regression was carried out using MDR positive samples as dependent variables and age and sex as independent factors. To identify the independent and linked causes of UTI in patients due to multi-drug resistant E. coli and K. pneumoniae. The GraphPad Prism 8 software (La Jolla, California, USA) was used for drawing. The culture results were analyzed using SPSS 22 software (Chicago, Illinois, USA). The significance level of all statistical tests was set at a p-value of 0.05.
Results
Patient Characteristics and Proportion of Identified Bacterial Isolates in Urine Samples
In this study, 32,391 urine samples were analyzed between January 2020 and December 2022, of which 17,926 were males and 14,465 were females. Of all these urine samples, 5378 (16.6%) were positive for bacteria in incubators during microbial growth assays with significant bacterial counts (1.0×105 CFU/mL of urine), and these patients were classified as having UTIs (Table 1). The positive rate in male patients was 40.4% (2172/5378), and that in female patients was 59.6% (3206/5378). Comparatively speaking, female patients had a higher positive rate. The majority of culture-positive samples (53.1%) came from patients over the age of 65 (Table 1).
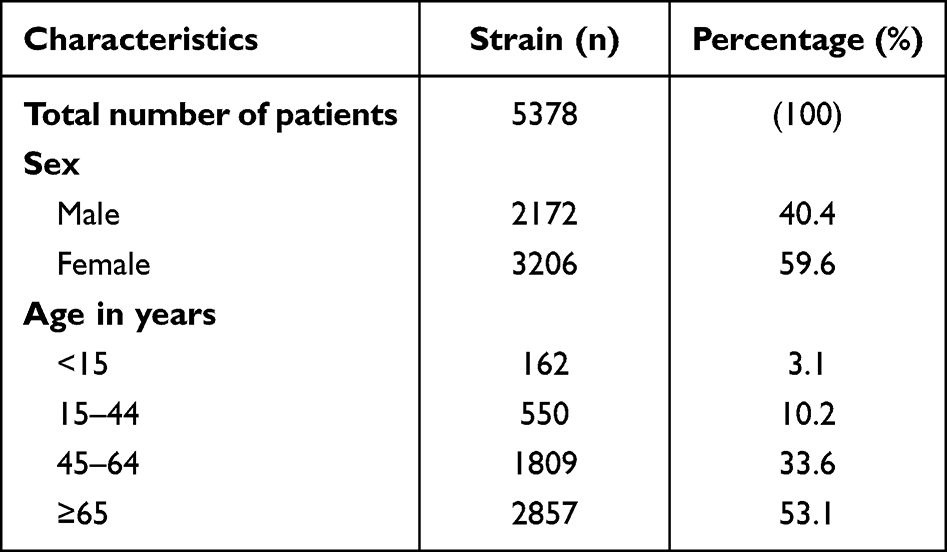 |
Table 1 Determine the Characteristics of Patients According to Their Age and Gender |
Pathogen Characteristics
A total of 5378 bacterial strains were isolated, including 3690 gram-negative (68.6%) and 1688 gram-positive (31.4%). The distribution and proportion of pathogenic microorganisms isolated from urine cultures in the midstream region were depicted in Figure 1. The most common pathogen was Escherichia coli, with 2110 strains (39.2%) detected (Figure 1). This was followed by Enterococcus faecalis, Klebsiella pneumoniae, Enterococcus faecium, Proteus mirabilis, Streptococcus agalactiae, Pseudomonas aeruginosa, Staphylococcus epidermidis, Enterobacter cloacae, and Acinetobacter baumannii with 668 (12.4%), 408 (7.6%), 407 (7.6%), 300 (5.6%), 200 (3.7%), 175 (3.3%), 112 (2.2%), 92 (1.7%), and 87 (1.6%), respectively (Figure 1). Meanwhile, as shown in Figure 2, we examined the annual quantitative variations of the top four pathogens isolated from 2020 to 2022. The results showed that E. coli and E. faecalis were most prevalent in 2021, whereas K. pneumoniae and E. faecium numbers were largely steady over the course of three years.
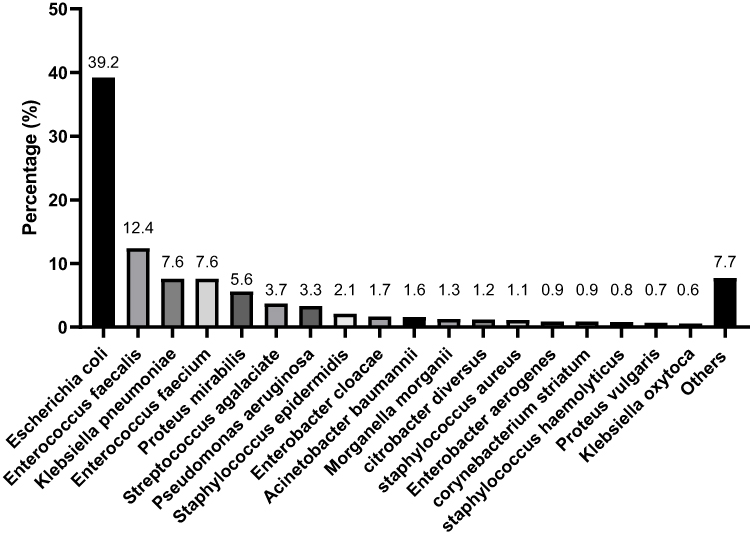 |
Figure 1 Distribution of main bacterial pathogens causing UTIs among patients from 2020 to 2022. The number above the histogram represents the percentage of the corresponding strain. |
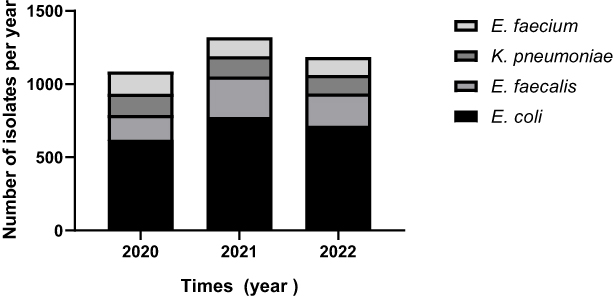 |
Figure 2 Annual change trends of the number of the top four bacterial pathogens in urine samples of patients with urinary tract infection from 2020 to 2022. The annual quantity is the total number of each isolate in a specific year. |
Antibiotic Resistance Patterns of Pathogens
The resistance rate of E. coli to ampicillin (76.2%) was the highest, followed by ciprofloxacin (58.9%), levofloxacin (51.4%), cefazolin (44.9%), bactrim (44.3%), and ceftriaxone (41.4%) (Table 2). Additionally, tobramycin (9.5%), cefoxitin (8.8%), amoxicillin-clavulanic acid (7.2%), amikacin (2.1%), nitrofurantoin (1.7%), piperacillin/tazobactam (0.8%), imipenem (0.8%), meropenem (0.7%), and ertapenem (0.07%) were the antibiotics with resistance rates less than 10% (Table 2). For K. pneumoniae isolates, high resistance rates were found to ceftriaxone (37.7%), aztreonam (37.2%), and nitrofurantoin (35.4%). However, K. pneumoniae was highly sensitive to ertapenem (100%) (Table 2).
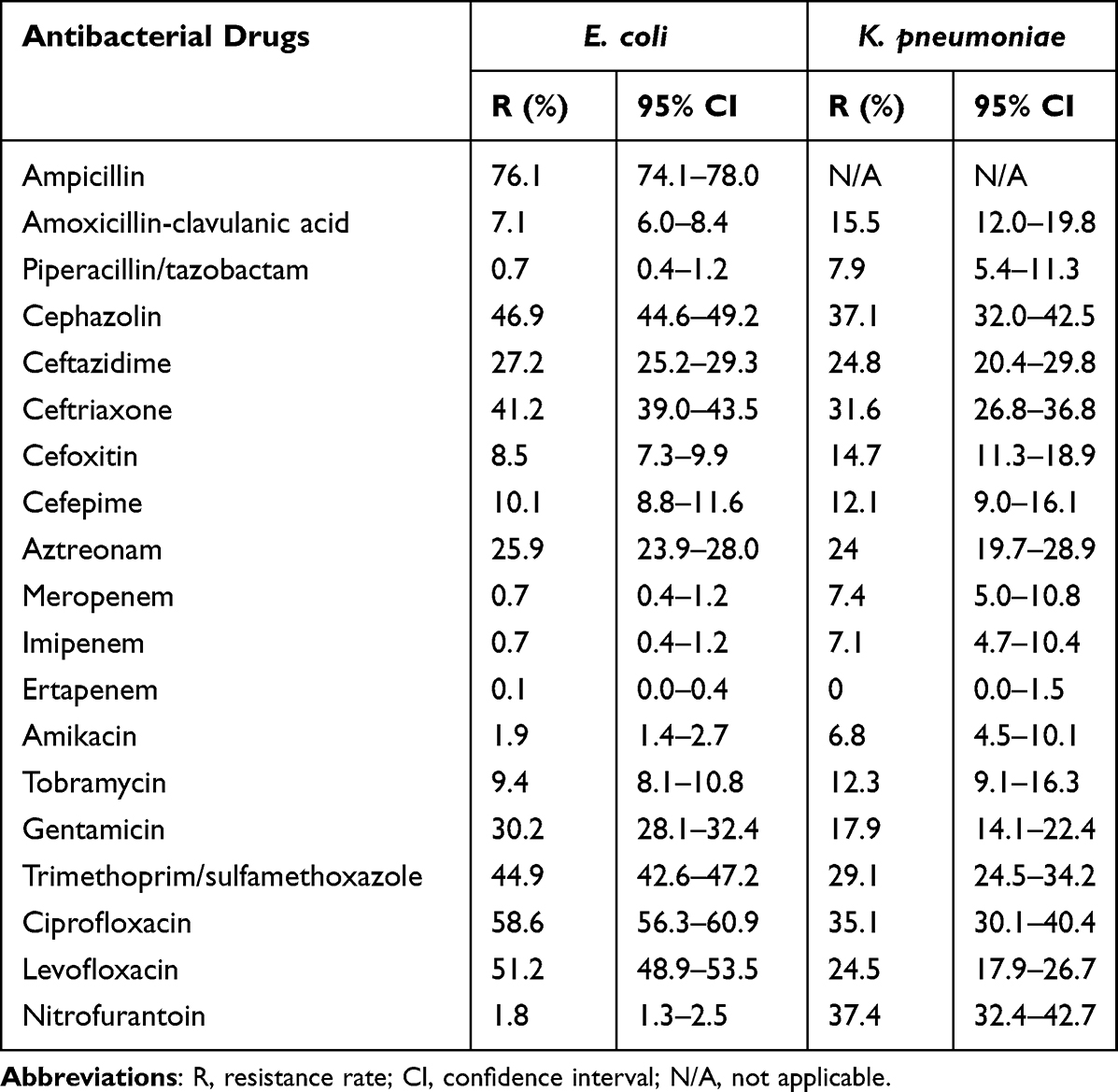 |
Table 2 Antibiotic Resistance Rates of E. coli (n = 2110) and K. pneumoniae (n = 408) Isolated from Urine Cultures |
Only a few gram-positive enterococci strains were found to be resistant to vancomycin, but two strains were not found to be resistant to linezolid, tigecycline, high-concentration streptomycin, or gentamicin (Table 3). The two antibiotics that E. faecalis was most resistant to were tetracycline (83.7%) and erythromycin (58.3%), followed by ciprofloxacin (28.3%), levofloxacin (28%), penicillin G (1.8%), nitrofurantoin (0.9%), and ampicillin (0.3%) (Table 3). E. faecium has a high resistance rate to ciprofloxacin, ampicillin, levofloxacin, and erythromycin, and the resistance rate was over 90%. The resistance rates to nitrofurantoin and tetracycline were 68.7% and 20.6%, respectively (Table 3).
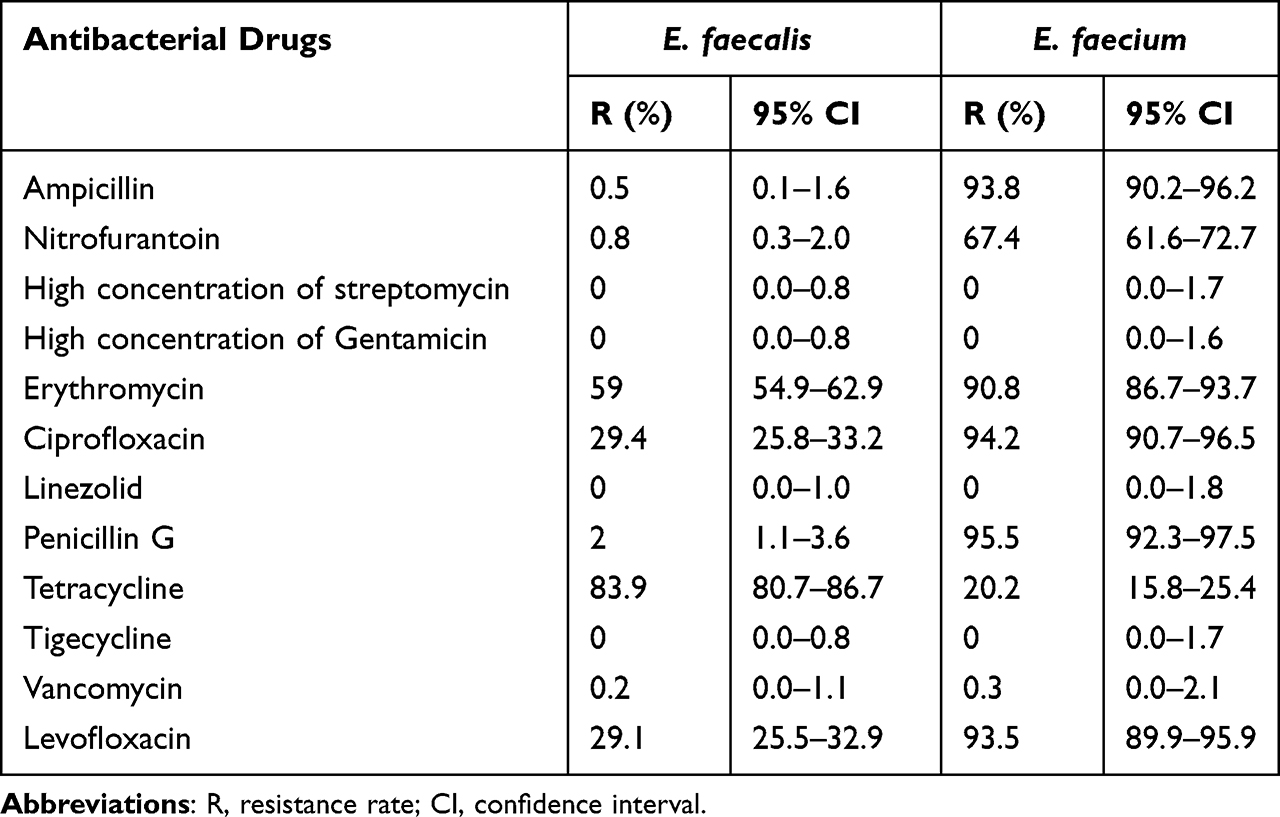 |
Table 3 Antibiotic Resistance Rates of E. faecalis (n = 668) and E. faecium (n = 407) Isolated from Urine Cultures |
Multi-Drug Resistance and ESBL Positivity
The details of MDR and the results of ESBL positivity were listed in Table 4. The proportion of strains showing MDR in E. coli reached 41.8%, and there was a downward trend (Table 4). The positive rate of ESBL in E. coli also showed a similar trend, with a positive rate of 40.8%, and the positive rate decreased with time (Table 4). However, the proportion of strains showing MDR in K. pneumoniae was 35.5%, with an increasing trend reaching 43.8% in 2022 (Table 4). The positive rate of ESBL in K. pneumoniae was 26.2% (Table 4). During the whole study period, only two drug-resistant isolates of gram-positive bacteria were found, or less than 1%. In addition, the proportion of ESBL remained stable throughout the study period.
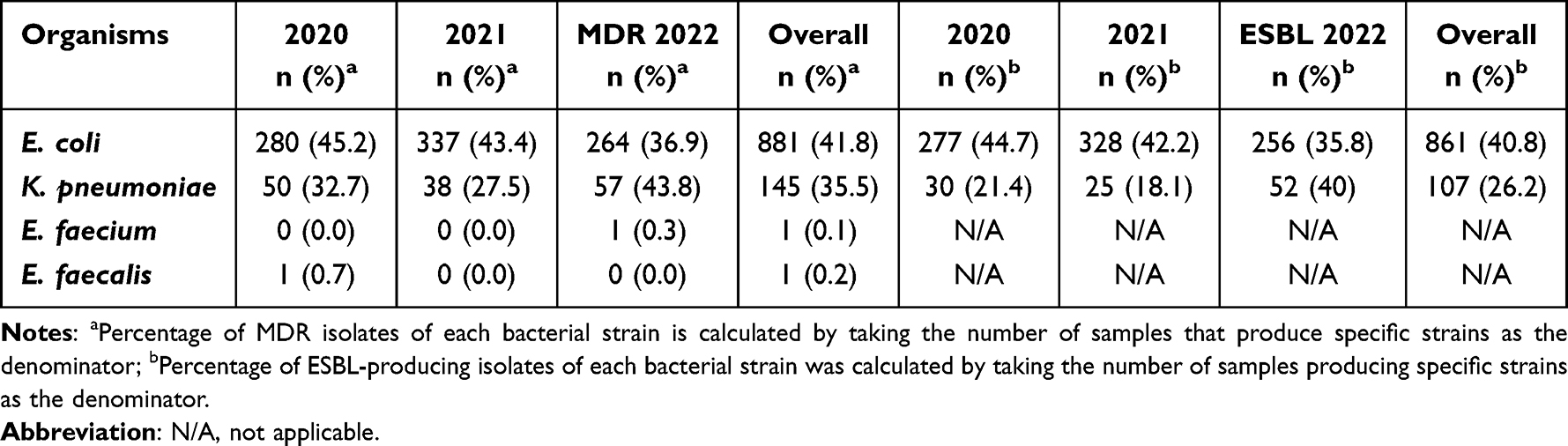 |
Table 4 Multidrug Resistance (MDR) and Extended-Spectrum Beta-Lactamase (ESBL) Prevalence in Common Bacteria Isolated from Urine Cultures |
Distribution of MDR Uropathogens by Age and Sex
There is no significant difference in the prevalence of multidrug-resistant (E. coli and K. pneumoniae) UTIs among different age groups. However, compared with male patients (10.0%), the proportion of MDR-positive E. coli in female patients (20.7%) was significantly higher (p < 0.001). In terms of MDR of K. pneumoniae, on the contrary, the positive rate of female patients was lower than that of male patients (Table 5).
 |
Table 5 Examination of MDR Bacterial (E. coli and K. pneumoniae) Urinary Tract Infections by Binary Logistic Regression Analysis According to Age, and Sex |
Discussion
UTIs are the most common bacterial infections in the human urinary system. In recent years, UTI-related pathogens and sensitivity patterns have changed significantly around the world.4,6 Despite the continuous updating of antibacterial drug types, pathogen resistance is increasing.8 Antibiotic resistance is also very prevalent as a result of antibiotic overuse. The incidence, pathogens, and drug resistance of UTIs vary by geographic location.1 Understanding the epidemiological information of the local pathogens is necessary for the empirical therapy of UTI. In order to guarantee the responsible use of antibiotics and prevent the emergence of drug-resistant strains, it is crucial to comprehend the pathogen distribution and drug resistance characteristics of bacterial infections in this region.8 In this research, the pathogens and sensitivity of 32,391 urine samples collected in our hospital between 2020 and 2022 were examined. The distribution of pathogenic bacteria displayed some striking drug resistance traits over the course of the three years of this research.
In this study, the prevalence of UTIs was found to be 16.6%, which was comparable to the findings of other investigations.19,20 Ours found that females (59.6%) had a greater infection rate than males (40.4%). The results of this study were consistent with another study by Mays et al where they observed that the incidence of UTIs in females (61.7%) was higher than that in males (39.3%).15 In Portugal, the number of females suffering from UTIs was 12,351 (79.6%), which was much higher than the males (3088, 20.4%).11 Numerous factors, including the shorter length of the female urethra and its proximity to the rectum, sexual contact that allows bacteria from the vaginal area to enter the urethra, vaginal irritation brought on by contraceptive diaphragms, menopause, and pregnancy, contribute to the high prevalence of UTIs in females.11 According to previous records, UTIs will increase with the age of patients.15,21 This study found that more than half of the infections (53.1%) were caused by the elderly population, which was consistent with Andreia et al15 This may be because older people are more likely to experience repeated hospitalization, which exposes them to hospital infections, continuous use of antimicrobials, frequent use of urogenital conductors, and diminished adaptability and innate immunity.22 In the current research, E. coli was discovered to be the most prevalent urinary pathogen in urine culture, which is also the result that researchers from other parts of the world have reached at various times.19 Followed by E. faecalis, K. pneumoniae, and E. faecium. Similar results were found in the study by Li et al1 E. faecalis was the second most common isolated pathogen in the urinary tract, followed by K. pneumoniae and E. faecium.1 Some studies also listed K. pneumoniae as the second most common urinary pathogen. For instance, E. coli accounted for 77.9% of the isolates in an Indian investigation, with K. pneumoniae accounting for 22.1%.23 In any case, the most common pathogens causing urinary tract infections remain the same, and the ranking varies slightly from region to region.
This study discovered that pathogens isolated from urine samples showed a high proportion of drug resistance. The high resistance of E. coli isolates to antibiotics commonly used in clinics, such as ampicillin, ciprofloxacin, levofloxacin, cefazolin, trimethoprim, and ceftriaxone, reached 40%–76%. Similar findings were made by Li et al who noted that E. coli had a resistance rate of more than 55% to ceftriaxone, ampicillin, and quinolones.1 This high level of drug resistance reduces the effectiveness of antibiotics that are frequently employed in our clinical work and may also be the reason why empirical treatment often fails.1 According to studies, E. coli strains with extended-spectrum β-lactamases are responsible for one-third of urinary tract infections.17 These germs are highly resistant to common antibiotics, which limits the efficacy of empirical treatment.8 β-lactamase inhibitors are regarded as a good control for strains that produce ESBL. The resistance rates of E. coli to piperacillin/tazobactam and amoxicillin-clavulanic acid were 0.7% and 7.1%, respectively, which showed an upward trend in the past three years. This rising tendency might be connected to the increase of β-lactamases in recent years.24 In addition, ertapenem, meropenem, imipenem, piperacillin/tazobactam, nitrofurantoin, and amikacin had strong antibacterial action against E. coli, which was similar to a study in Poland.25 However, a study in India reported that the resistance rate of E. coli to nitrofurantoin was 81.82%,26 demonstrating that there are considerable regional and national variations in antibiotic resistance patterns. This can be attributed to many factors, including variations in the research population and geographical location.11 Patients who misuse antibiotics without any medical advice are one of the factors contributing to the development of antibiotic-resistant bacteria. Due to the formation of mutant strains, they are now better able to shield themselves against medications.11
In this investigation, the resistance rate of K. pneumoniae isolates to nitrofurantoin, cephazolin, ciprofloxacin, and ceftriaxone was greater than 30%. The drug resistance to ertapenem, imipenem, meropenem, and piperacillin/tazobactam was lower than 8%. And K. pneumoniae was highly sensitive to ertapenem. A study conducted in Iraq showed that K. pneumoniae was resistant to piperacillin (81.6%), levofloxacin (78.9%), cefotaxime (73.7%), trimethoprim-sulfamethoxazole (71.1%), ceftazidime (65.8%), and gentamicin (63.2%).11 Another study in China showed that the resistance rate of K. pneumoniae to imipenem and cefotetan was about 45%, and the resistance rate to ceftazidime, cefepime, piperacillin, tazobactam, and ampicillin sulbactam was more than 55%.1 There are differences in the drug resistance rate of bacteria causing UTIs in all studies, which can be attributed to many factors, such as differences in the research population and geographical location.11 This study found that the MDR of K. pneumoniae was 21%. Multi-drug resistance in K. pneumoniae reduces the available antibiotic options and poses a serious threat to human life.27 K. pneumoniae can produce carbapenemase and produce resistance to carbapenems,27 and strains with this characteristic are resistant to penicillin and cephalosporin.27,28 According to the research report, such drug-resistant bacteria are conveniently disseminated. Drug sensitivity testing and molecular biological testing should be carried out as soon as possible to guide the use of antibiotics for UTIs caused by suspected multi-drug-resistant infections, especially carbapenemase-resistant K. pneumoniae.27
Previous studies have shown that E. coli accounts for the majority of UTIs,29 but Enterococcus has also become a widespread pathogen. The findings of this investigation revealed that 1075 strains (20%) of enterococcus, including E. faecalis (668 strains) and E. faecium (407 strains), were detected in 5168 individuals with UTIs. This is similar to a straightforward UTI pathogen investigation done in Shanghai, China, where Enterococci account for 30.4% of the pathogen population. Risk factors for UTIs include advanced age, diabetes, and catheter implantation.8,30 The majority of samples in this study were taken from inpatients, and the elderly patients and catheter-related infections may be to blame for the high percentage of gram-positive bacteria found there.
The drug resistance mechanism of enterococci is intricate. Several antibiotics, including cephalosporins and aminoglycosides, are naturally resistant due to their cell wall structure, and transposons and plasmids can be used to acquire resistance to common antibiotics.31,32 The results of the drug sensitivity test revealed that E. faecalis was extremely resistant to tetracycline, erythromycin, ciprofloxacin, and levofloxacin. E. faecium was highly resistant to ciprofloxacin, penicillin G, levofloxacin, ampicillin, erythromycin, and nitrofurantoin, which was essentially consistent with the findings of the previous research.1 Studies have shown that the antibiotic resistance of various enterococci varies greatly. The resistance rate of E. faecium to most antibiotics is higher than that of E. faecalis. However, E. faecalis carries more virulence genes and forms biofilms more easily to obtain stronger pathogenicity.33 According to reports, vancomycin-resistant Enterococci infections are gradually increasing in hospitals.33 It is important to note that a few vancomycin-resistant strains of E. faecalis and E. faecium were grown in this study, indicating the requirement for adequate monitoring and control measures to be implemented going forward to prevent the spread of multidrug-resistant Enterococci in hospitals.
MDR bacteria frequently cause UTIs.34 Most studies showed that men were an independent risk factor for UTIs with MDR bacteria.19,34 Although females have a higher incidence of UTIs, males are much more at risk of developing MDR infections.19 Other studies found that the risk of MDR infection in different age groups was correlated with that of older patients (≥ 65 years old).34 However, this study found no significant differences in the incidence of multi-resistant microbial UTIs in various age groups, and females were the main risk factors for MDR infection. Unlike previous findings, this may be relevant to different study populations or geographical locations. However, it should be carefully explained that, although there is evidence that different regions and populations are sensitive to different pathogens, our data do not provide information about the health status of patients or the types of health care providers.19
This study has several limitations, including the fact that it is retrospective, has limited clinical data, lacks knowledge of risk factors, the characteristics of the infection, concomitant conditions, recent hospitalizations, past antibiotic use, treatment response, etc. Urine samples were only inoculated on blood agar plates, and selective culture media (eg, MacConkey plates) and fungal chromogenic plates were not inoculated, which may have led to the missed detection of pathogens. This study was based only on laboratory-reported data and did not conduct a genomic analysis of different resistant strains. Furthermore, this study only analyzed the susceptibility and resistance patterns of the first four pathogens of the urinary tract. The remaining microorganisms were not analyzed in this study. The research has indicated that potential clinical conditions as well as information regarding prior use of antibiotics may be used to better identify the risk factors of antimicrobial resistance and create prospects for obtaining extremely trustworthy therapeutic recommendations. Hence, a multicenter prospective design study is required to fill the existing evidence gap in UTI.
Conclusion
Our results will be helpful for clinicians to better understand the microbiological characteristics of UTI pathogens and the situation of antibiotic resistance in this region. The results of this study revealed that female urinary tract infections were more numerous than male cases (59.6% vs 40.4%). The pathogens most frequently discovered in the urine isolates were E. coli, E. faecalis, K. pneumoniae, and E. faecium. Meanwhile, we noticed that some pathogens were becoming more and more resistant to antibiotics. We advocate performing drug sensitivity testing and bacterial cultures before administering antibiotics to ensure prudent antibiotic use. To better understand the molecular epidemiology of the gathered isolates, molecular research on the genes encoding these antibiotic resistance markers is strongly advised.
Abbreviations
UTIs, Urinary tract infections; ESBL, Extended-spectrum beta-lactamases; MDR, Multidrug resistance.
Ethics Approval
The study was approved by the ethics committee of the First Hospital of Jiaxing (No. 2023-LY-297). The ethics committee abandoned the requirement for participants to give formal informed permission because of the retrospective nature of this study. Patients’ anonymous information was provided from the microbiology hospital laboratory, which isolated the strains. The study completely followed the guiding principles in the Declaration of Helsinki.
Acknowledgments
We thank anonymous reviewers whose comments and suggestions helped improve this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Science and Technology Plan Project of Jiaxing of Zhejiang Province of China under Grant 2022AD30056, the “Venus” Talent Training of the First Hospital of Jiaxing of Zhejiang Province of China under Grant 2021-QXM-21, and Clinical Laboratory Medical Diagnostics Fund of the First Hospital of Jiaxing of Zhejiang Province of China under Grant 2023-ZC-002.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Li J, Jiang F, Xie A, et al. Analysis of the distribution and drug resistance of pathogens in patients with urinary tract infection in the Eastern Chongming area of Shanghai from 2018 to 2020. Infect Drug Resist. 2022;15:6413–6422. doi:10.2147/IDR.S384515
2. Choi H, Shin K, Kim Y, et al. Characteristics of Escherichia coli urine isolates and risk factors for secondary bloodstream infections in patients with urinary tract infections. Microbiol Spectr. 2022;10(4):e0166022. doi:10.1128/spectrum.01660-22
3. Rozwadowski M, Gawel D. Molecular factors and mechanisms driving multidrug resistance in uropathogenic Escherichia coli—an update. Genes. 2022;13(8):1397. doi:10.3390/genes13081397
4. Mclellan L, Hunstad D. Urinary tract infection: pathogenesis and outlook. Trends Mol Med. 2016;22(11):946–957. doi:10.1016/j.molmed.2016.09.003
5. Rao C, Vennila T, Kosanam S, et al. Assessment of bacterial isolates from the urine specimens of urinary tract infected patient. Biomed Res Int. 2022;4088187. doi:10.1155/2022/4088187
6. Islam M, Islam M, Khan R, et al. Prevalence, etiology and antibiotic resistance patterns of community-acquired urinary tract infections in Dhaka, Bangladesh. PLoS One. 2022;17:e0274423. doi:10.1371/journal.pone.0274423
7. Sokhn ES, Salami A, Roz AE, et al. Antimicrobial susceptibilities and laboratory profiles of Escherichia coli, Klebsiella pneumoniae, and Proteus mirabilis isolates as agents of urinary tract infection in Lebanon: paving the way for better diagnostics. Med Sci. 2020;8(3):32. doi:10.3390/medsci8030032
8. Lee D, Lee S-J, Choe H-S. Community-acquired urinary tract infection by Escherichia coli in the era of antibiotic resistance. Biomed Res Int. 2018;7656752. doi:10.1155/2018/7656752
9. Miranda-Novales M, Flores-Moreno K, López-Vidal Y, et al. Limited therapeutic options in Mexico for the treatment of urinary tract infections. Antibiotics. 2022;11:1656. doi:10.3390/antibiotics11111656
10. Ezzeddine Z, Ghssein G. Towards new antibiotics classes targeting bacterial metallophores. Microb Pathog. 2023;182:106221. doi:10.1016/j.micpath.2023.106221
11. Jalil M, Naji Al Atbee M. The prevalence of multiple drug resistance Escherichia coli and Klebsiella pneumoniae isolated from patients with urinary tract infections. J Clin Lab Anal. 2022;36(9):e24619. doi:10.1002/jcla.24619
12. Adamus-Bialek W, AnnaWawszczak M, StanislawGad B, KlaudiaBator P, MartaParniewski P. The genetic background of antibiotic resistance among clinical uropathogenic Escherichia coli strains. Mol Biol Rep. 2018;45(5):1055–1065. doi:10.1007/s11033-018-4254-0
13. Sugianli AK, Ginting F, Parwati I, et al. Antimicrobial resistance among uropathogens in the Asia-Pacific region: a systematic review. JAC Antimicrob Resist. 2021;3(1):dlab003. doi:10.1093/jacamr/dlab003
14. Mortazavi-Tabatabaei S, Ghaderkhani J, Nazari A, et al. Pattern of antibacterial resistance in urinary tract infections: a systematic review and meta-analysis. Int J Prev Med. 2019;10(1):169. doi:10.4103/ijpvm.IJPVM_419_17
15. Silva A, Costa E, Freitas A, et al. Revisiting the frequency and antimicrobial resistance patterns of bacteria implicated in community urinary tract infections. Antibiotics. 2022;11(6):768. doi:10.3390/antibiotics11060768
16. Lu X, Wang Y, Guo W, et al. Antibacterial activity of an FtsZ inhibitor celastrol and its synergistic effect with vancomycin against enterococci in vitro and in vivo. Microbiol Spectr. 2023;11:e0369922. doi:10.1128/spectrum.03699-22
17. Joya M, Aalemi AK, Baryali T. Prevalence and antibiotic susceptibility of the common bacterial uropathogen among UTI patients in French medical institute for children. Infect Drug Resist. 2022;15:4959–4960. doi:10.2147/IDR.S387390
18. Vallo S, Wirth P, Kukic A, et al. Decreasing susceptibility of bacteria to ampicillin/ sulbactam and third generation cephalosporins in urinary tract infections. Curr Urol. 2022;16(2):94–98. doi:10.1097/CU9.0000000000000079
19. Salm J, Salm F, Arendarski P, et al. High antimicrobial resistance in urinary tract infections in male outpatients in routine laboratory data, Germany, 2015 to 2020. Eurosurveillance. 2022;27(30):2101012. doi:10.2807/1560-7917.ES.2022.27.30.2101012
20. Wojno K, Baunoch D, Luke N, et al. Multiplex PCR based Urinary Tract Infection (UTI) analysis compared to traditional urine culture in identifying significant pathogens in symptomatic patients. Urology. 2019;136:119–126. doi:10.1016/j.urology.2019.10.018
21. Costa T, Linhares I, Ferreira R, et al. Frequency and antibiotic resistance of bacteria implicated in community urinary tract infections in North Aveiro between 2011 and 2014. Microb Drug Resist. 2018;24:493–504. doi:10.1089/mdr.2016.0318
22. Rowe TA, Juthani-Mehta M. Diagnosis and management of urinary tract infection in older adults. Infect Dis Clin North Am. 2014;28(1):75–89. doi:10.1016/j.idc.2013.10.004
23. Mohd R, Akhtar M, Najmi A, Singh K. Escherichia coli and Klebsiella pneumoniae sensitivity/resistance pattern towards antimicrobial agents in primary and simple urinary tract infection patients visiting university hospital of Jamia Hamdard New Delhi. Drug Res. 2018;68(7):415–420. doi:10.1055/a-0576-0079
24. Ríos E, Diaz M, Culebras E, et al. Resistance to fosfomycin is increasing and is significantly associated with extended-spectrum β-lactamase-production in urinary isolates of Escherichia coli. Med Microbiol Immunol. 2022;211(5–6):269–272. doi:10.1007/s00430-022-00749-2
25. Barbara K, Wicha J, Grużewska A, et al. Virulence factors, biofilm-forming ability, and antimicrobial resistance of urinary Escherichia coli strains isolated from hospitalized patients. Turk J Med Sci. 2016;46:1908–1914. doi:10.3906/sag-1508-105
26. Prakash D, Saxena RS. Distribution and antimicrobial susceptibility pattern of bacterial pathogens causing urinary tract infection in urban community of Meerut City, India. ISRN Microbiol. 2013;2013:749629. doi:10.1155/2013/749629
27. Shrief R, El-Ashry A, Mahmoud R, et al. Effect of colistin, fosfomycin and meropenem/vaborbactam on carbapenem-resistant Enterobacterales in Egypt: a cross-sectional study. Infect Drug Resist. 2022;15:6203–6214. doi:10.2147/IDR.S385411
28. Carvalhaes CG, Shortridge D, Sader HS, et al. Activity of meropenem-vaborbactam against bacterial isolates causing pneumonia in hospitalized patients from U.S. Hospitals during 2014 to 2018. Antimicrob Agents Chemother. 2020;64(3). doi:10.1128/AAC.02177-19
29. Ballash G, Mollenkopf D, Diaz-Campos D, et al. Pathogenomics and clinical recurrence influence biofilm capacity of Escherichia coli isolated from canine urinary tract infections. PLoS One. 2022;17:e0270461. doi:10.1371/journal.pone.0270461
30. Ch’ng JH, Chong K, Ling NL, et al. Biofilm-associated infection by enterococci. Nat Rev Microbiol. 2018;17(2):82–94. doi:10.1038/s41579-018-0107-z
31. Rao C, Dhawan B, Vishnubhatla S, et al. Emergence of high-risk multidrug-resistant Enterococcus faecalis CC2 (ST181) and CC87 (ST28) causing healthcare-associated infections in India. Infect Genet Evol. 2020;85(6890):104519. doi:10.1016/j.meegid.2020.104519
32. Gajdács M, Brók M, Lázár A, et al. Increasing relevance of Gram-positive cocci in urinary tract infections: a 10-year analysis of their prevalence and resistance trends. Sci Rep. 2020;10(1):17658. doi:10.1038/s41598-020-74834-y
33. Asfaw T. Biofilm formation by Enterococcus Faecalis and Enterococcus Faecium: review. ARC J. 2019;2019:2349–2365. doi:10.20431/2349-0365.0704002
34. Guclu E, Halis F, Kose E, et al. Risk factors of multidrug-resistant bacteria in community-acquired urinary tract infections. Afr J Online. 2021;1:214–219. doi:10.4314/ahs.v21i1.28
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.