Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Patterns and Trends in the Use of Medications for COPD Control in a Cohort of 9476 Colombian Patients, 2017–2019
Authors Machado-Duque ME ![]() , Gaviria-Mendoza A
, Gaviria-Mendoza A ![]() , Valladales-Restrepo LF
, Valladales-Restrepo LF ![]() , González-Rangel A
, González-Rangel A ![]() , Laucho-Contreras ME, Machado-Alba JE
, Laucho-Contreras ME, Machado-Alba JE ![]()
Received 21 February 2023
Accepted for publication 28 May 2023
Published 27 July 2023 Volume 2023:18 Pages 1601—1610
DOI https://doi.org/10.2147/COPD.S391573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
Manuel Enrique Machado-Duque,1,2 Andrés Gaviria-Mendoza,1,2 Luis Fernando Valladales-Restrepo,1,2 Andrés González-Rangel,3 Maria Eugenia Laucho-Contreras,3,4 Jorge Enrique Machado-Alba1
1Grupo de Investigación en Farmacoepidemiología y Farmacovigilancia, Universidad Tecnológica de Pereira – Audifarma S.A, Pereira, Colombia; 2Grupo de Investigación Biomedicina, Fundación Universitaria Autónoma de las Américas, Pereira, Colombia; 3Medical Affairs, GlaxoSmithKline, Bogotá, Colombia; 4Regional Medical Affairs, GlaxoSmithKline, Bogotá, Colombia
Correspondence: Jorge Enrique Machado-Alba, Grupo de Investigación en Farmacoepidemiología y Farmacovigilancia. Universidad Tecnológica de Pereira - Audifarma S.A, Calle 105 No. 14-140, Pereira, Risaralda, 660003, Colombia, Tel +57 3108326970, Fax +57 63137822, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) affects approximately 174 million people worldwide. The objective was to determine the trends of COPD medication use in a group of Colombian patients.
Patients and Methods: This was a retrospective study on prescription patterns of bronchodilators and other medications used in COPD from a population database with follow-up at 12 and 24 months. Patients older than 18 years of age of any sex with a COPD diagnostic code between 2017 and 2019 were included. Sociodemographic variables, medications, treatment schedules for COPD, comorbidities, comedications, and the specialty of the prescriber were considered.
Results: Data from 9476 people with COPD was evaluated. The mean age was 75.9 ± 10.7 years, 50.1% were male, and 86.8% were prescribed by a general practitioner. A total of 57.9% had comorbidities, most often hypertension (44.4%). At the baseline measurement, on average, they received 1.6 medications/patient, mainly short-acting antimuscarinics (3784; 39.9%), followed by short-acting β-agonists (2997, 31.6%) and inhaled corticosteroids (ICS) (2239, 23.6%); more than half (5083, 53.6%) received a long-acting bronchodilator. Prescription of triple therapy (antimuscarinic, β-agonist, and ICS) went from 645 (6.8%) at baseline to 1388 (20.6%) at the 12-month mark.
Conclusion: This group of patients with COPD treated in Colombia frequently received short-acting bronchodilators and ICS, but a growing proportion are undergoing controlled therapy with long-acting bronchodilators, a situation that can improve the indicators of morbidity, exacerbations, and hospitalization.
Keywords: pulmonary disease, chronic obstructive, bronchodilator agents, muscarinic antagonists, pharmacoepidemiology
Introduction
The worldwide prevalence of chronic obstructive pulmonary disease (COPD) has been estimated at 174 million patients, leading to around 3.1 million deaths each year. Its prevalence and mortality grew by 44.2% and 11.6%, respectively, between 1990 and 2015.1 Low- and very low-income countries have more deaths from this cause due to poor access to current therapies and poor control of complications, which leads to an increase in the burden of disease.1,2
In Colombia, the PREPOCOL study, published in 2008, with a spirometric criterion, enrolled 5539 participants, who had a prevalence of COPD close to 8.9%. It was more frequent in those over 60 years old, smokers and ex-smokers, users of firewood for cooking, and those with low educational levels.3,4
In COPD, there is progressive inflammation and injury of the lungs associated with the use of tobacco or exposure to biomass fuel, which leads to alveolar and microvascular alterations and the destruction of the exchange surface due to loss of elasticity and growth of the lung alveolar space and inflammation of the mucosa and glands by cytokine release.5
The management of COPD depends on its severity, with long-acting bronchodilators such as long-acting antimuscarinics (LAMA) and long-acting β2 agonists (LABA) as the mainstays of treatment, sometimes together with inhaled corticosteroids (ICS), therapies that are considered effective in symptomatic control, slowing the progression of the disease, and decreasing the frequency of exacerbations.2,5 For some patients with a weak response to combined medications, triple therapy is recommended,2,6 and to manage acute symptoms such as dyspnea or cough, short-acting bronchodilators such as short-acting β2 agonists (SABAs) are used.2 Other medications used in patients with poor response are methylxanthine (with an inadequate safety profile),7 phosphodiesterase IV inhibitors such as roflumilast, and short courses of systemic corticosteroids during episodes of exacerbation.6 During the observation period of the study, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines were utilized to stratify patients according to their risk of exacerbations, resulting in stages A through D. Specific therapeutic recommendations were provided for each stage of the disease, with some notable changes for the 2023 GOLD guidelines. Notably, these guidelines emphasize the importance of therapy with LABA/ LAMA combination.7
The prescription patterns of these therapies can vary between countries and even within the same region. In the USA, Petite et al found that patients diagnosed with COPD were most often on short-acting bronchodilators (42.5%), followed by long-acting bronchodilators or ICS (32.3%), where LABA represented 21.3%, followed by LAMA 18.8%, ICS 21.7%, roflumilast 1.6%, and theophylline 2.2%.8 A study on the use of bronchodilators for the management of asthma and COPD in adults in Colombia estimated that 74.3% used short-acting β2-adrenergic agonists (SABAs) and 24.8% used long-acting β2-agonists (LABAs), and 87.1% used short-acting anticholinergics and 16.9% tiotropium.9
The Colombian Health System offers universal coverage through two affiliation regimes, one contributory or paid by the employer and the worker, and another subsidized by the state. Until December 2021, its national formulary included only short-acting bronchodilators such as salbutamol and ipratropium bromide, in addition to a single ICS such as beclomethasone and systemic corticosteroids, excluding other inhaled and all long-acting bronchodilators,10,11 which are the therapies of choice for stable COPD2 due to their effectiveness and safety. Access to long-acting controller therapies was possible but required the completion of special forms or court decisions, which adds a barrier for physicians and patients. On this context, we aimed to determine the trend of use of medications for COPD in a group of Colombian patients between 2017 and 2019.
Materials and Methods
A descriptive retrospective study was conducted on the prescription patterns of bronchodilators and other medications used in the treatment of COPD based on a population drug dispensing database (Audifarma SA, with more than 8.5 million people from six different insurers affiliated within the Colombian health care system), which covers approximately 17.3% of the country’s population. All patients of any sex, older than 18 years, with a diagnosis of COPD according to the codes of the International Classification of Diseases version 10.0 (ICD-10: J440, J441, J448, J449) and dispensations of some control or rescue medication between July 1, 2017, and June 30, 2019, were included. There were no exclusion criteria.
Based on the information on the consumption of medications of the affiliated population that met the inclusion criteria (prevalent cases), a database was constructed that contained the following variables.
- Sociodemographic: sex, age (recorded at the time of first dispensation), city, and region of care.
- Comorbidities: diagnosis identified as comorbidities according to ICD-10 codes during the observation period, extracted from the prescriptions.
- Prescribing physician: identification of the specialty of the prescribing physician.
- Medications used in COPD: drug, pharmaceutical form, and date of dispensation. They were classified as a) SABAs, LABAs, and ultralong-acting agonists (U-LABAs); b) muscarinic antagonists: short-acting (SAMA), long-acting (LAMA), ultralong-acting (U-LAMA); c) inhaled corticosteroids (ICS); d) ICS/LABA combinations; e) LAMA/LABA combinations; f) other medications: theophylline, roflumilast, oral systemic corticosteroids, leukotriene antagonists. Naive patients were defined as those who received the drug for the first time.
- Treatment regimens: whether the medications were used in monotherapy or in combination. The main combinations found are described. Triple therapy was defined as LABA + LAMA + ICS.
- Comedications: medications prescribed concomitantly during COPD therapy.
Statistical Analysis
The data were analyzed with the statistical package SPSS Statistics, version 26.0 for Windows (IBM, USA). A descriptive analysis was performed with frequencies and proportions for the qualitative variables, and measures of central tendency and dispersion for the quantitative variables. For the quantitative variables, normality was tested by the Kolmogorov–Smirnov test; for those variables with normal behavior, means and standard deviations were calculated, and for those without normality, medians and interquartile ranges were calculated. The data, when obtained from the drug dispensing database, has all the sociodemographic information and drug claims, so there were no lost data, if there may be the possibility of information biases regarding data on unregistered comorbidities.
Bioethical Considerations
The protocol was endorsed by the Bioethics Committee of the Universidad Tecnológica de Pereira in the classification of risk-free research (approval code: 01–100220). The principles of confidentiality of information established by the Declaration of Helsinki were respected. According to Resolution 8430 of the Colombian Ministry of Health, risk-free research does not require informed consent and obtaining it was exempted by the Bioethics Committee.
Results
A total of 9476 people diagnosed with COPD were evaluated during the observation period, with an equal proportion of men and women (According to Gil-Rojas et al, in Colombia there were 370,278 cases of COPD in 2015, so the population evaluated in this study would represent approximately 2.56% of the total).12 The regions with the most cases were the Bogotá/capital region, followed by the Valle del Cauca region and the Risaralda, Caldas, and Quindío departments. Table 1 shows the data according to sex, age, and dispensing region.
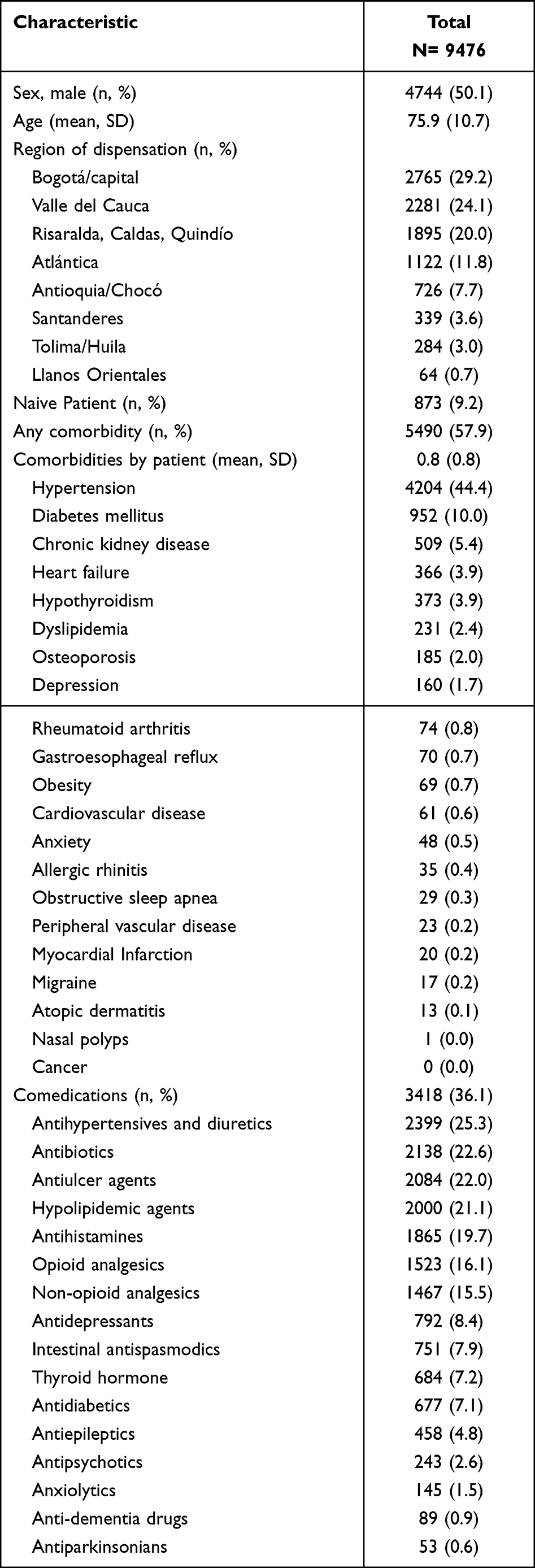 |
Table 1 Sociodemographic Characteristics, Regions of Origin, Comorbidities and Comedications in a Group of Patients with COPD in Colombia |
Some comorbidity was present in 57.9% of the patients, the most frequent being arterial hypertension, diabetes mellitus, chronic kidney disease, heart failure, and hypothyroidism. Prescription of some other medications in addition to those necessary for COPD treatment was seen in 36.1% of patients, most often antihypertensives, diuretics, drugs for acid-related disorders, lipid-lowering drugs, and antihistamines (see Table 1).
Among the COPD patients at baseline, 57.7% were prescribed a single medication, 29.0% had two medications, and the remaining (13.3%) between three and five medications for the management of COPD. The vast majority were being treated by general practitioners, followed by family medicine physicians and pulmonologists. Table 2 shows the number of medications, the specialty of the prescribing physician, and therapy or main combinations used at the time of initial observation and at 12 and 24 months of follow-up.
 |
Table 2 Prescription Patterns, Frequency of Drug Use and Combinations Used in a Group of COPD Patients in Colombia |
The most frequently used therapy at the beginning of the observation period was SAMAs (n= 3784; 39.9%), ipratropium bromide being the most used of the group, followed by SABAs (n= 2997; 31.6%), with salbutamol as the most used. The combination of SABA + SAMA + ICS was found in 828 patients (8.7%), and 880 (9.3%) patients had initially received LAMA, especially tiotropium. In addition, 184 (1.9%) were on U-LABA monotherapy, and 1348 (14.2%) were on a LABA + LAMA combination, the most frequent being indacaterol + glycopyrronium. Finally, 645 (6.8%) patients were on triple therapy of LABA + LAMA + ICS at baseline. Table 3 shows the most commonly used drugs at the beginning of the follow-up, as well as at 12 and 24 months.
 |
Table 3 Frequencies of Use of Medications for the Treatment by Age Group and During the Different Moments of Observation in a Group of Patients with COPD in Colombia |
Triple Therapy
A total of 2378 (25.1%) patients who received triple therapy (LABA + LAMA + ICS) during the observation period were identified. The most frequently used combination was fluticasone/salmeterol + tiotropium, followed by indacaterol/glycopyrronium + beclomethasone and budesonide/formoterol + tiotropium. Table 4 shows the characteristics according to the age and sex of this group of patients, the specialty of the prescribing physician, the time elapsed from the formulation at the beginning of the observation period to the beginning of triple therapy, and the medications used before it.
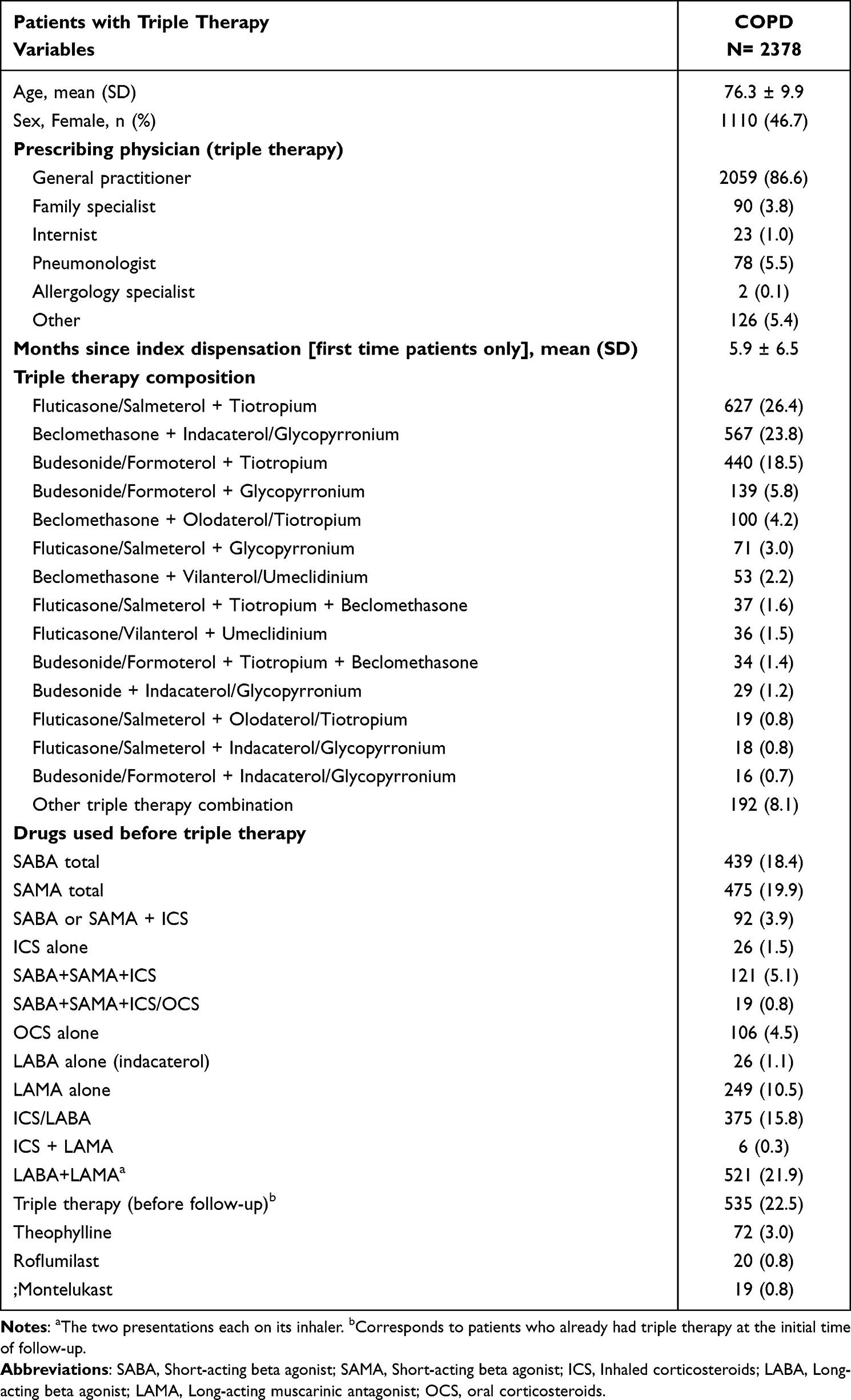 |
Table 4 Sociodemographic Characteristics, Prescription and Frequencies of Triple Therapy Use Patterns (LABA, LAMA, ICS) in a Group of Colombian Patients with COPD |
Discussion
In this analysis, we identified the patterns of use of medications for the treatment of COPD, as well as the most frequent comorbidities, and the drugs used concomitantly. All this information is of interest to prescribe physicians, patients, and decision-makers in the search to optimize the management of COPD by implementing strategies that have greater coverage of symptoms and that appropriately use medications according to each patient’s needs.
The results of this study show that patients with COPD under pharmacological treatment in real-life conditions in Colombia are older adults, with average age close to 75 years and multiple comorbidities, and with a similar male/female ratio as has been described in different observational studies.12–15 More than half of the patients had at least one identified comorbidity (mean: 0.8 per patient), most often hypertension (44.4%), followed by diabetes mellitus (10.0%) and chronic kidney disease (5.4%), with a prevalence slightly lower than those reported by Ding et al for the United States in 2020, who reported rates of arterial hypertension of 64%, diabetes mellitus of 28%, and dyslipidemia of 45%. These discrepancies may be evidence of a lower diagnosis rate of the different comorbidities of the patients evaluated, at least in the records from the prescription of medications.13
At the beginning of the observation period, ICS and SABA or SAMA were the most used drugs in patients with COPD. This combination is not recommended by any guideline, since the use of ICS always must be combined with one or two long-acting bronchodilators (LABA, LAMA, or LABA+LAMA). One possible explanation is that some severe patients (based on low lung function, exacerbation rate, dyspnea) are being treated with short-acting drugs. This situation could be considered inadequate according to clinical practice guidelines or systematic reviews,16 that recommend therapy based on the knowledge that the use of long-acting bronchodilators compared with short-acting bronchodilators was associated with improved lung function, fewer hospital admissions (including those for exacerbations of COPD), fewer exacerbations of COPD and improved quality of life, with a good safety profile.2,17–19
Almost one in four patients took an ICS, a higher proportion than expected. ICS monotherapy did not reduce the accelerated rate of decline in pulmonary function that is characteristic of COPD, and thus ICS monotherapy is not disease-modifying, and it is not recommended as a treatment, irrespectively of the severity.20 The combined therapy of ICS with short-acting bronchodilators has been associated with an increased risk of pneumonia in patients older than 65 years with COPD, especially at higher doses and for prolonged periods of time.19,21 Treating physicians and decision-makers need to establish the role of ICS in stable COPD, knowing the potential risks as well as the benefits, including a lesser decrease in quality of life and improvement of symptoms.21
At the beginning of the observation period, almost 10% of the patients were on LAMA in monotherapy, which suggests that they have moderate disease. In line with other studies, by the 24 months timepoint, the proportion was reduced to nearly 5%, probably because studies showed that around 50% of the patients persist with symptoms, exacerbations and poor quality of life when they are treated with monotherapy with LAMA.2,7,17,22 At the baseline time of observation, 27.5% of the cohort was being managed with either ICS/LABA or LAMA/LABA, which are recommended moderate to severe COPD patients,2,7 This proportion is lower than that reported by Xu et al in New Zealand, where 59.1% received LABA/ICS in combination for the management of COPD,23 The proportion of patients taking LAMA + LABA increased to approximately 22% at 12 and 24 months, while the use of ICS + LABA remained stable, where in New Zealand they also report an increase in the proportions of use of bronchodilators over time to 24 months.23 This can be explained mainly by the findings in which the combined therapy with bronchodilators long-acting can achieve adequate control of symptoms and reduce exacerbations, without being associated with an increase in the incidence of pneumonia, which has been described in ICS/LABA, although these different trends over time can also be due to the preferences of the treating physicians, typical in pharmacoepidemiological studies.19,24
It is worrisome that almost 4% of patients with COPD received theophylline, with increasing proportions in the follow-up, as xanthine has a modest bronchodilator effect in stable forms of the disease,25 and has contradictory evidence regarding the frequency of exacerbations, with associated neurological and cardiovascular toxicity, so it is suggested to avoid its use.26 However, this finding, added to many patients receiving combined short-acting bronchodilators without long-acting bronchodilators, should generate reflections on the existing therapeutic gap for many patients with COPD in Colombia.2,7
Twenty-five percent of patients were prescribed triple therapy (LABA + LAMA + ICS) at some point during the observation period in any of the different possible combinations, which is recommended for patients with severe disease in those with an exacerbator profile or in patients with frequent or persistent symptoms that cannot achieve control with long-acting dual therapy.2,7 The study by Monteagudo et al in Spain showed similar proportions of use of the same bronchodilators before initiation of triple therapy, the most common being the use of ICS + LABA and LAMA + LABA. However, there were greater differences when comparing this analysis in terms of the prescription of previous short-acting bronchodilators (SABA 18.4% vs 15.7% and SAMA 19.9% vs 11.8%), which was lower in Spanish patients.6 The IMPACT study published in 2018 also showed that triple therapy in COPD patients with at least one exacerbation is highly effective, improving lung function and symptoms and reducing exacerbation rates compared to dual therapy, with either ICS/LABA or LAMA/LABA,27 Another study focused on patients from Canada who reach triple therapy is the one published by Jiang et al, where only 41.2% had an exacerbation in the previous year and even so, 32.5% of patients reach triple therapy without the use of other previous bronchodilators, 29.8% from LAMA and 15.4% from ICS/LABA, Being something different from what was found in Colombia where the most frequent is that before they were with LABA/LAMA followed by ICS/LABA and LAMA monotherapy.28
An important limitation of this study was the absence of clinical data, such as confirmatory spirometry that could quantify lung function, information on the control of symptoms or exacerbations in patients, classification of the stage of the disease, disease progression, and history of past or current smoking. Given that the information was from patients affiliated with the health system, our findings have limited generalizability to populations with different types of service provision. Some strengths are the large sample size, the follow-up for 12 and 24 months, and the identification of different variables about the use of these therapies for COPD, which have not been described in Colombia.
Conclusions
This group of COPD patients treated in Colombia frequently receive short-acting bronchodilators and ICS, but a growing proportion of them are being given therapy with long-acting bronchodilators such as LABAs or LAMAs, a trend that is likely to increase with the recent inclusion of these drugs in the benefit plan of the Colombian Health System. This development can improve the indicators of morbidity, exacerbations, and hospitalization and requires close monitoring of its results, which can be an input for treating physicians, especially decision-makers and those who formulate health policies.
Data Sharing Statement
protocols.io; dx.doi.org/10.17504/protocols.io.bzyfp7tn
Acknowledgments
The authors gratefully acknowledge Soffy López and Carlos Tovar for their support in obtaining the initial database of patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by GlaxoSmithKline Colombia (ID 213332).
Disclosure
This work was funded by GSK. GSK did not participate in the management or data analysis of the study information. MEMD, JEMA, AGM and LFVR have developed studies funded by GSK, Pfizer, Biotoscana, Sanofi, Sanofi-Pasteur, Abbot, Tecnoquímicas, Bayer, and Novartis. MELC and AGR are GSK employees. MELC has received speaker’s fees for: GSK, Astra Zeneca, Novartis. AGM reports grants from GSK, during the conduct of the study; and has developed studies funded by GSK, Pfizer, Biotoscana, Sanofi, Sanofi-Pasteur, Abbot, Tecnoquímicas, Bayer, and Novartis. The authors report no other conflicts of interest in this work.
References
1. GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir med. 2017;5(9):691–706. doi:10.1016/s2213-2600(17)30293-x
2. GOLD. Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2019. Available from: https://goldcoped.org/.
3. Caballero A, Torres-Duque CA, Jaramillo C, et al. Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest. 2008;133(2):343–349. doi:10.1378/chest.07-1361
4. Kuzmar I, Giraldo CO, Acevedo GO, Rua GS. Morbilidad de la enfermedad pulmonar obstructiva crónica en Colombia. Resultados del estudio SANEPOC-2. Revista de la Facultad de Ciencias Médicas. 2017;75(1):19–24.
5. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/s0140-6736(17)31222-9
6. Monteagudo M, Nuñez A, Solntseva I, et al. Treatment Pathways Before and After Triple Therapy in COPD: a Population-based Study in Primary Care in Spain. Arch Bronconeumol. 2021;57(3):205–213. doi:10.1016/j.arbres.2020.07.032
7. Agustí A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am J Respir Crit Care Med. 2023;207(7):819–837. doi:10.1164/rccm.202301-0106PP
8. Petite SE. Characterization of chronic obstructive pulmonary disease prescribing patterns in the United States. Pulmonary Pharmacol Therapeutics. 2018;49:119–122. doi:10.1016/j.pupt.2018.02.003
9. Machado-Alba JE, Moreno Gutiérrez PA, Bañol Giraldo AM. Patrones de prescripción de broncodilatadores y corticoides inhalados en pacientes adultos de Colombia. Acta Medica Colombiana. 2015;40:218–226.
10. Ministerio de Salud y Protección Social. República de Colombia. Resolución 5857 de 2018. Available from: https://www.minsalud.gov.co/Normatividad_Nuevo/Resoluci%C3%B3n%205857%20de%202018.pdf.
11. Ministerio de Salud y Protección Social. República de Colombia. Resolución 1885 de 2018. Available from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/resolucion-1885-de-2018.pdf.
12. Gil-Rojas Y, Duque-Torres CAT, Del Carmen Figueredo M, et al. Estimación de la prevalencia de EPOC en Colombia a partir del Registro Individual de Prestaciones de Servicios de Salud (RIPS). Revista Colombiana de Neumología. 2019;31(1):564.
13. Ding B, Kallenbach L, Slipski L, Wilk A, O’Brien D, Guranlioglu D. Patient Characteristics and Healthcare Resource Utilization Among Patients with COPD New to LAMA/LABA Fixed-Dose Combination Treatment in US-Based Real-World Practice. Int J Chron Obstruct Pulmon Dis. 2020;15:775–786. doi:10.2147/copd.S238408
14. Lopez-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
15. Sá-Sousa A, Amaral R, Almeida R, Freitas A, Almeida Fonseca J. Prescribing patterns of medication for respiratory diseases - cluster analysis of the Portuguese electronic prescription database. Eur Ann Allergy Clin Immunol. 2021. doi:10.23822/EurAnnACI.1764-1489.186
16. Cheyne L, Irvin-Sellers MJ, White J. Tiotropium versus ipratropium bromide for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2015(9):Cd009552. doi:10.1002/14651858.CD009552.pub3
17. Mirza S, Clay RD, Koslow MA, Scanlon PD. COPD Guidelines: a Review of the 2018 GOLD Report. Mayo Clinic Proceedings. 2018;93(10):1488–1502. doi:10.1016/j.mayocp.2018.05.026
18. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol–Glycopyrronium versus Salmeterol–Fluticasone for COPD. N Eng J Med. 2016;374(23):2222–2234. doi:10.1056/NEJMoa1516385
19. Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009;169(3):219–229. doi:10.1001/archinternmed.2008.550
20. Tashkin DP, Strange C. Inhaled corticosteroids for chronic obstructive pulmonary disease: what is their role in therapy? Int J Chron Obstruct Pulmon Dis. 2018;13:2587–2601. doi:10.2147/copd.S172240
21. Drummond MB, Dasenbrook EC, Pitz MW, Murphy DJ, Fan E. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300(20):2407–2416. doi:10.1001/jama.2008.717
22. Dransfield MT, Bailey W, Crater G, Emmett A, O’Dell DM, Yawn B. Disease severity and symptoms among patients receiving monotherapy for COPD. Prim Care Respir J. 2011;20(1):46–53. doi:10.4104/pcrj.2010.00059
23. Xu X, Milea D, Navarro Rojas AA, et al. A Real-World Analysis of Treatment Patterns and Clinical Characteristics Among Patients with COPD Who Initiated Multiple-Inhaler Triple Therapy in New Zealand. Int J Chron Obstruct Pulmon Dis. 2021;16:1835–1850. doi:10.2147/copd.S295183
24. Wedzicha JA, Banerji D, Chapman KR, et al. Indacaterol-Glycopyrronium versus Salmeterol-Fluticasone for COPD. N Engl J Med. 2016;374(23):2222–2234. doi:10.1056/NEJMoa1516385
25. Ram FS, Jones PW, Castro AA, et al. Oral theophylline for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2002;2002(4):Cd003902. doi:10.1002/14651858.Cd003902
26. Devereux G, Cotton S, Fielding S, et al. Effect of Theophylline as Adjunct to Inhaled Corticosteroids on Exacerbations in Patients With COPD: a Randomized Clinical Trial. JAMA. 2018;320(15):1548–1559. doi:10.1001/jama.2018.14432
27. Lipson DA, Barnhart F, Brealey N, et al. Once-Daily Single-Inhaler Triple versus Dual Therapy in Patients with COPD. N Eng J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
28. Jiang L, Kendzerska T, Aaron SD, et al. Prescription Pathways from Initial Medication Use to Triple Therapy in Older COPD Patients: a Real-World Population Study. Copd. 2022;19(1):315–323. doi:10.1080/15412555.2022.2087616
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
U-Shaped Relationship Between Serum Lactate Dehydrogenase with All-Cause Mortality in Patients with Chronic Obstructive Pulmonary Disease
Huang L, Lu Z, Zhou X, He L, You X, Chen C, Zou C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:305-316
Published Date: 15 March 2023
Characteristics of Inhaler Technique in COPD Patients in a Specialized Center in Armenia, Colombia: A Cross-Sectional Study
Montes Cardona JA, Hincapié Erira DA, Nati-Castillo HA, Sánchez-Vallejo J, Izquierdo-Condoy JS
Patient Preference and Adherence 2023, 17:2025-2038
Published Date: 16 August 2023
Adherence to Inhalation Devices in Patients with Chronic Obstructive Pulmonary Disease
Valladales-Restrepo LF, Oyuela-Gutiérrez MC, Delgado-Araujo AC, Calvo-Salazar J, Osorio-Bustamante D, Lerma-Barco CE, Machado-Alba JE
Patient Preference and Adherence 2023, 17:3233-3244
Published Date: 8 December 2023
Predictive Role of White Blood Cell Differential Count for the Development of Acute Exacerbation in Korean Chronic Obstructive Pulmonary Disease
Yoon EC, Koo SM, Park HY, Kim HC, Kim WJ, Kim KU, Jung KS, Yoo KH, Yoon HK, Yoon HY
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:17-31
Published Date: 4 January 2024
The Dosing Strategy to Improve Adherence to Roflumilast in Treatment for Chronic Obstructive Lung Disease: A Systemic Review and Meta-Analysis
Lee J, Song JU
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:655-663
Published Date: 5 March 2024