Back to Journals » Clinical Ophthalmology » Volume 19
Patterns and Prevention of Occupational Eye Injuries: A Narrative Review
Authors Vought V ![]() , Zarbin F, Vought R, Khouri AS
, Zarbin F, Vought R, Khouri AS
Received 30 August 2025
Accepted for publication 13 November 2025
Published 20 November 2025 Volume 2025:19 Pages 4257—4268
DOI https://doi.org/10.2147/OPTH.S556838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Victoria Vought,1 Francesca Zarbin,2 Rita Vought,1 Albert S Khouri1
1Institute of Ophthalmology and Visual Science, Rutgers New Jersey Medical School, Newark, NJ, USA; 2Dartmouth College, Hanover, NH, USA
Correspondence: Victoria Vought, Rutgers New Jersey Medical School, Institute of Ophthalmology and Visual Science, 90 Bergen St, Suite 6100, Newark, NJ, 07103, USA, Tel +1 973 972-2036, Email [email protected]
Abstract: Occupational eye injuries (OEIs) remain a major public health issue despite regulatory efforts toward increasing protective eyewear use. OEIs encompass a wide spectrum of trauma, from superficial injury to tissue melt and globe rupture. These injuries are associated with substantial medical, economic, and social burden. This narrative review identifies risk factors associated with OEIs, differences based on workplace, and barriers to OEI prevention. Risks for OEI include male sex, low educational attainment, low income, or being a temporary or migrant worker. Certain industries such as metalworking, construction and manufacturing, chemical handling, and agriculture, also carry unique ocular hazards that predispose workers to OEIs. Although many OEIs are minor, those that cause severe injury can result in permanent visual loss and blindness. Industrial and construction workers are frequently exposed to high-velocity foreign bodies (FBs) and blunt trauma, while agricultural workers are at elevated risk for open globe injuries, FBs and the vision-threatening sequalae of infection from organic material. Chemical injuries, although less common, are notable for high rates of bilateral eye involvement, often requiring urgent intervention. Unfortunately, most OEIs occur in the absence of proper protective eyewear. Barriers range from discomfort and poor fit, inadequate access, and lack of perceived need, all of which contribute to low compliance in various occupational settings. Current evaluations of behavioral and regulatory interventions to increase adherence show promise but with mixed results. Advances in protective eyewear technology that optimize comfort and usage tracking may be helpful for employers to ensure compliance. A comprehensive understanding of OEI mechanisms and the obstacles to increased protective eyewear use is critical to mitigate the impact of OEIs on workers.
Keywords: occupational injury, occupational hazards, ocular trauma, eye protection, open globe injury, ocular burns
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Haque has been published for this article.
Introduction
Occupational eye injuries (OEIs) are defined as ocular trauma sustained in the workplace. To mitigate the risk of work-related eye injuries, the Occupational Safety and Health Administration (OSHA) mandates employers to provide ocular protection against chemical, environmental, radiologic, or mechanical hazards.1 Both federal and state level regulations not only require precautions, but also the availability of emergency eyewash and shower facilities in the event of an injury. According to the US Bureau of Labor Statistics (US BLS), the incidence of OEIs has declined in some sectors.2 However, OEIs remain a significant public health concern, with over 38,000 cases recorded by the US BLS in 2021 alone.3 Given the wide variety of mechanisms that can cause an OEI, they can range from corneal abrasions to vision-threatening open-globe injuries (OGIs). The true incidence of OEIs is likely underestimated, since reported cases are likely to comprise more severe injuries. For instance, examinations of OGIs in an agricultural region found over 20% to be attributed to industry or workplace injury,4 and a study of closed globe injuries (CGIs) presenting to a tertiary trauma center also reported over a fifth of cases to have occurred at work.5 The workplace has been previously documented as one of the most common settings where globe injuries occur.6
Vision-threatening OEIs impose significant medical and economic burdens for patients.7,8 In addition to medical cost, individuals face potential loss of vision9,10 and decreased quality of life. Some patients can develop severe psychological distress after a workplace injury.11,12 Eye injuries also result in loss of working days and decreased productivity. In a study of 387 perforating eye injuries presenting to Helsinki University Eye Hospital, 36% were occupational. Among these, 4% of patients had to change profession, and 5% became permanently disabled.13 Punnonen13 also found a mean hospital stay of 20 days both overall and among those suffering from an occupational injury, with an average sick leave of 80 days overall compared to 90 days in OEI. An analysis of cost after work-related eye injuries in Malaysia reported even higher indirect costs (time off from work and value of permanent disability or workers’ compensation) compared to direct medical cost in 884 cases.14 Annually in the US, OEIs have been estimated to cost over 300 million USD in lost productivity, 924 million USD in medical treatment and workers’ compensation, and 4 billion USD in wage and productivity cost.1,15
Given the considerable morbidity and economic impact of OEIs, a greater understanding of the types of eye injuries that occur in various occupational settings is critical. This narrative review aims to characterize the risk factors associated with OEIs and explore worker behaviors surrounding ocular safety in the US and abroad. This study provides an overview of the spectrum of OEIs by epidemiologic factors, job type, differences in injury mechanisms, and visual outcomes. Understanding these topics is critical to analyze existing OEI prevention strategies and identify areas for innovation and improvement.
Methods
A comprehensive literature search was conducted using the PubMed database in July of 2025 to identify relevant recent studies including primary research, meta-analyses, and review articles. The initial search identified 126 articles published between January 2015 to July 2025. A combination of Medical Subject Headings (MeSH) and free-text search terms were used: “occupational”, “occupation”, “employment”, “work”, “work-related”, “workplace injury”, “eye injury”, “eye injuries”, “ocular injury”, “ocular injuries”, “eye trauma”, “ocular trauma”, “industry”, “industrial”, “construction”, “manufacturing”, “utility”, “welding”, “welders”, “electrical”, “electrician”, “plumbing”, “chemical”, “chemical injury”, “ocular burn”, “agriculture”, “agricultural”, “farming”, “agricultural injury”, “harvesting”, and “military”. Boolean operators (AND; OR) were applied to refine the search results. Relevant peer-reviewed, full-text manuscripts authored in English were examined. For topics of interest with a lack of recent published literature, time constraints were removed to identify relevant studies for inclusion.
Epidemiology of Occupational Eye Injuries
The epidemiology of OEIs clarifies which populations are at higher risk for these injuries. The American Optometry Association describes workers employed in construction, manufacturing, mining, carpentry, auto repair, electrical work, plumbing, welding, and maintenance as high risk for occupational injury.16 Several studies have produced data to support this claim;2,15,17,18 however, this list is not exhaustive. Meta-analyses have identified male gender, under-use of eye protection, exposure to hazards, risk taking behavior, and the use of mechanical force to be common features in those who suffer from OEIs.19,20 Male gender has been well established as a risk for OEI, possibly due to higher representation in some professions21 and greater prevalence of high-risk behaviors.22 Lee and Samarawickrama reported almost 90% of CGIs presenting to a tertiary trauma center occurred in males,5 and Syed et al21 found a higher incidence of injuries in male employees compared to their female counterparts, even in industrial sectors with a greater portion of female workers. Other behavioral risk factors, such as cigarette smoking, may also modify the risk of ocular trauma in the workplace.23
The average age of individuals affected by OEIs is consistent with the expected working age. An evaluation of work-related ocular trauma from the National Trauma Databank found a mean age of 40.7 years old,24 with a similar average age reported in other studies conducted in the US8 and abroad.25,26 There is also evidence suggesting a trend toward greater use of eye protection with increased years of job experience.27 Higher levels of educational attainment are also protective against OEIs.26 Conversely, low socioeconomic status has also been linked to increased risk for OEIs, likely owing to an increased exposure to high-risk occupations.18 This association may also be attributed to the possibility that more educated individuals may have better access to and understanding of safety materials.23 When controlling for age, race/ethnicity, health status and insurance, and risk-taking behaviors, men with lower household incomes and high school education or less were at greater risk for an OEI compared to male counterparts.23 Notably, this trend was not observed among female workers.23
Experiencing a previous OEI has been described as a protective factor through increased adherence to eye protection.26 A met-analysis of ocular protection practices among welders in sub-Saharan Africa found pre- and in-service training, previous experience as a welder, and a history of ocular injury to be associated with ocular protection practices.28 Blackburn et al also investigated changes in the use of protective eyewear following OEI in Alabama, where workers were more likely to wear eye protection after having an OEI.27 Those who did not endorse changes in habits attributed this to a lack of perceived need, interference with work, and discomfort.27
Of note, certain populations of workers may be at elevated risk compared to their coworkers. Evidence has been mixed on whether certain racial and ethnic groups are at higher risk for OEI.23 However, Gobba et al highlighted an increased chance of OEIs among foreign workers, who were found to have a 50% higher injury risk.9 Temporary workers may also be more likely to experience an OEI compared to their permanent counterparts.29 Meta-analyses of occupational injuries as a whole have identified migrant workers, commonly employed in agricultural, construction, and manufacturing sectors, as having a high prevalence of workplace injury.30 These data could also reflect that a higher percentage of migrant workers are employed in high-risk industries. It may also suggest disparities in occupational safety training and resource allocation, or differences in the implementation of safety protocols based on worker demographics.
Ocular Injuries by Occupation
Although many studies of occupational injuries evaluate OEIs occurring in the workplace as a single cohort, a more detailed understanding of risk factors present within different sectors can highlight specific hazards present in each environment. Industrial, chemical, and agricultural settings have been heavily reported as common sites of OEIs in the literature. Overall, common OEIs include corneal foreign bodies (FBs), open globe injury, lamellar laceration, anterior chamber hyphema, traumatic cataract, and chemical burns.18
Industry
The term “industrial sector” is broad and often poorly defined in individuals presenting from these settings. A review of the National Trauma Databank found that most work-related trauma occurred in industrial facilities.24 Although sometimes classified separately in OEI studies, industrial jobs can include welding, construction, manufacturing, utility/maintenance, and related fields. Industrial workers have been previously suggested to have the highest rate of workplace ocular trauma compared to other occupations.9,31 For instance, a single-center analysis of OEIs found 47% of presentations attributed to metalworking, 27% to construction, 10% to electricians and carpenters, and 17% to other workers.32 In this study, over 80% of cases with presented with a visual acuity (VA) 20/30 or better and only 5% presented with VA 20/80 or worse.32 This exemplifies an overall pattern observed in OEI severity among industrial workers; although most injuries are minor, OEIs still carry the possibility of severe vision loss. The risk of blindness varies based on the nature of the work.
Metalworking, including welding, is a source of ocular hazard in industrial settings. This broad field encompasses shaping and assembling metals for a wide range of purposes, including construction and manufacturing. Metalworkers frequently utilize lathes, milling machines, grinders, and drills, all of which can generate high-speed debris that can cause OEIs. Similarly, welding involves cutting and fusing metals using heat and pressure sources. Welders can be exposed to sparks, molten metal, and high intensity ultraviolet or infrared radiation. Interviews with welders highlight themes about concerns of fumes and sparks “getting into the eyes” in the setting of mixed reports about eye protection usage.33 As with other OEIs, the majority of injuries observed in metalworking are not vision-threatening. For instance, an evaluation of metalworkers mainly belonging to the unorganized sector in India found that most sustained mechanical injuries that did not require any treatment for recovery.34 CGIs are also commonly observed with metal grinding.35 However, that is not to discount the impact of severe injuries in this setting. A review of patients requiring enucleation or evisceration following ocular trauma over 20 years in a Chinese tertiary care center found the majority of patients to be physical laborers (70.7%), with the most common cause of eye removal attributed to occupational injury (44.1%) and metal- or nail-related wounds (59.7%).36
Interestingly, bilateral and recurrent injuries have also been reported more frequently among metalworkers. A questionnaire study of welders in Ghana found that 47.9% of employees self-reported an eye injury, and most (83.6%) endorsed bilateral injury.37 A higher proportion of OEIs were reported among electric/arc welders compared to gas welders, and most OEIs were chemical in nature.37 Another examination of OEIs that followed workers for a year also found that four percent of individuals analyzed, all of whom were employed in the metalworking sector, had a second OEI from a metal FB within the same year.9 The presence of bilateral and repeat injuries among metalworkers suggests not only a high level of exposure to hazards but gaps in consistent and effective use of protective eyewear. This underscores the need for additional oversight and intervention.
Construction workers also face a broad spectrum of hazards in the workplace through building, renovating, and demolishing structures. This sector often includes those working in roofing, painting, plumbing, and electrical installation, among other tasks.38 Individuals in construction often perform jobs that use a variety of equipment, materials, and work in different settings, introducing significant variability in the workplace. This setting exposes construction workers to high-speed debris, chemical agents, falling objects, etc. Incidence reports of occupational injury in West Virginia found that that per 100,000 construction workers, 593.3 suffered from FBs, 490.6 from superficial injury, 61.6 from keratitis, 56.5 from chronic conjunctivitis, and 41.1 from ocular burns.21 CGIs have also been associated with construction workers, frequently manifesting with traumatic cataracts or gross hyphemas.35
In the US, construction has been identified as a common mechanism for OGI.39 The use of nails and nail guns, which occurs frequently in construction, has also been significantly associated with occupational OGIs.35 The Helsinki Ocular Trauma Studies have highlighted high-risk features of OEIs. Although OEIs frequently result in minor trauma, the occupational setting is a major risk factor for serious injury resulting in permanent visual impairment.10,25 Examination of ocular injuries caused by work tools, most commonly occupational and from nails, also found the use of tools to be closely associated with permanent visual impairment compared to other etiologies of ocular trauma.25 Nails and screwdrivers have been previously reported as common causes of OGIs the workplace, which likely contributes to the poor visual prognosis.10 Kolomeyer et al40 reported on nail-gun induced OGIs, the majority of which occurred at work. These eyes mainly suffered Zone I injuries with concurrent vitreous hemorrhage and hyphema with subsequent retinal detachment occurring in 23% of cases. Although most individuals had improvement in final VA, 7% became phthisical or prephthisical, and 2% were enucleated for pain.40
Perforating eye injuries, which confer significant risk for low vision, blindness, and enucleation, have also been observed in construction and industrial work.13 Ilhan et al41 compared OEIs among construction versus manufacturing workers and found higher rates of OGIs and retinal detachments in construction workers. In comparison, the manufacturing setting was more associated with chemical injury and worse final VA (hand motion or worse).41 A greater association between concomitant bone fracture and head trauma with OEIs was also observed among manufacturing employees.41 Similar to construction, manufacturing also is diverse in the nature of work that employees engage in, and their involvement in grinding, cutting, soldering, compressed air use, and drilling can frequently be a source of ocular trauma.9,17 Among manufacturing workers in West Virginia, the reported incidence per 100,000 of most common OEIs was 533.1 for FBs, 402.4 for superficial injuries, 73.5 for ocular burns, 71.0 for keratitis, and 43.6 for chronic conjunctivitis.21
As with other industrial OEIs, while severe trauma in manufacturing can have long-lasting consequences, not all injuries are severe. In other countries, manufacturing has also been a common culprit of OEIs. A survey of sawmill workers in Nigeria documented that almost 80% had suffered an ocular injury, most commonly a superficial FB (68.8%) or blunt trauma (27.6%) from sand/sawdust particles (47.1%) or work tools (31.2%).42 Another review of almost 900 industrial workplace reports involving eye injuries in Malaysia found reports mostly originating from the manufacturing sector.14 The most prevalent mechanism was impact from a fragment/flying particle. In this cohort, most injuries were categorized as mild (45%) compared to moderate (36.8%) or severe (18.2%), and 94.5% of all workers returned to work after being treated.14
Chemical Injuries
Chemical ocular injuries in the workplace predominantly manifest as ocular burns.43 These burns present an urgent workplace hazard because, if not promptly irrigated and treated, they can result in serious long-term complications, including limbal stem cell deficiency, corneal scarring, and glaucoma.44 Epidemiological evaluations of chemical OEIs found demographics consistent with other OEIs, with male predominance in the age 25–50-year range.43–46
Chemical OEIs occur in various settings. One epidemiological study of ocular chemical burns in Spain demonstrated that the service industry accounted for 62.08% of burns, construction 20.86%, agriculture (including farming, fishing, and forestry) 4.96%, and extraction industries 0.33%.43 Since almost half of workplace injuries with chemical products impact the eye, cleaners, workers, and technicians are at particularly high risk of incurring ocular burns.43 Although chemical ocular burns occur more frequently in industrial settings, various studies have demonstrated a higher prevalence of chemical ocular burns in the summer months, which could be attributed to cleaning staff using chemical cleaners in pool or spa settings.43,46
Agents involved in chemical ocular burns can be classified as alkalis and acids.10,44,46 Notable agents include pesticides, lye, toilet cleaner, battery acid, industrial acid, silicone production materials, and glass polishing materials. Various alcohols can also cause OEI.44,47 The occupational setting in which burns occur often correlates with the causative agent; for instance, industrial settings more commonly have burns associated with battery acid or silicone production materials, whereas cleaning industries have a greater incidence of pesticide- or toilet cleaner- related burns. The extent of injury severity depends not only on the chemical type, but also the duration of chemical exposure to the eye.43 For this reason, immediate recognition and access to eyewash stations are imperative to decontaminate the eye and reduce damage inflicted from these agents.
Common clinical diagnoses of patients with occupation-related chemical ocular burns include limbal ischemia, conjunctival ischemia, cornea epithelial damage or loss, corneal stroma haze, eyelid edemas, and obstruction of the pupil by corneal opacities.43,44,48 Limbal and perilimbal ischemia are commonly used as primary indicators of the burn’s damage to the eye,43 and the Roper Hall (RH) and Dua grades provide classification systems to categorize the clinical severity.48 In one five-year study performed in India, the most common severity was Dua grade 1 (73%) and RH grade 1 (75%), but 9% of eyes had Dua grade IV or higher.44 Kate et al also found a close association between visual morbidity and increasing grade of injury. Those with injuries equating to Dua grade III and above required far more surgeries as well, rising from approximately 10% of patients requiring surgery in grades I and II, and up to 80% in grades III and above.44 Furthermore, examination of severe chemical ocular injuries in the UK found high rates of complications at six months, including central corneal scar, persistent epithelial defect, and symblepharon. A significant need for surgical intervention was also observed, most commonly amniotic membrane graft and tarsorrhaphy.48
A unique characteristic of chemical OEIs is the increased frequency of bilateral injuries. Various studies report a significant rate of bilateral burns, ranging from 40% to 60% of patients in a given cohort.44,48,49 This high incidence of bilateral injury may contribute to the psychosocial and economic stress associated with these burns.49 For this reason, an important metric to consider when examining injury severity is the economic impact incurred on the patient. One study performed in Spain found that 75% of patients required up to seven days off from work, 20.86% required 8–30 days, and some had permanent disabilities.43 Although effects on patient incomes may vary, any delay from return-to-work could be devastating for low-income households, particularly if the injured individual is the primary income earner. Another study in China examining the socioeconomic impacts of chemical ocular burns found that the patients’ personal and household incomes had statistically significant decreases after surgery, and the reduction of these incomes increased with injury severity.49 Many patients also reported emotional depression or anxiety following their incidents. Although these economic and personal factors are not often highlighted in the literature, they have significant consequences for affected individuals.
Agriculture
The International Labor Organization categorizes agricultural activity as hazardous work,50 and various studies demonstrate a high incidence of agriculture-related OEIs compared to other workplace environments.9,51 Common environments that predispose workers to agricultural OEIs include rural areas, developing nations, and low- and middle-income countries, where there is typically less mechanization of farm work and lower usage of personal protective equipment.51–53 Agricultural OEIs are most frequently observed in traditionally rural and agrarian regions, particularly across South and East Asia, rather than in more commercial farming sectors found in the United States, although US migrant workers face similar risks as rural workers elsewhere.50,53 Janani et al found that agricultural OEIs occurred primarily during general farming tasks, such as operating machinery or harvesting crops (59.7%); followed by basic farming tasks, such as planting seeds or weeding (18.4%); gardening (12.3%); and farming and animal husbandry (9.4%).54 Additional factors, such as fatigue, poorly-designed tools, exposure to extreme weather, and prevalence of poor health in agrarian areas, significantly augment the risk of accidents and contribute to the high incidence of agricultural OEIs.50
While the agents causing OEIs can vary between agricultural settings, the most common sources are FBs such as branches, thorns, or flying particles while cutting or harvesting, and other debris from grass trimmers.54,55 For example, a study examining grape shelf eye injuries in Japan found that 36.7% were caused by wires, 36.7% by flying objects while handling grass trimmers, 16.7% by branches, and 6.7% by pipes.55 Similarly, a nine-year study in Bosnia found that 25% of work-related ocular injuries were due to plant or lawn materials.51 Investigations of other agricultural fields, such as rice harvesting, report similar findings.53 Another significant agent is UV radiation, as prolonged sun exposure can result in multiple vision-impairing injuries.54,55 Chemical and biological hazards are not as common in agricultural OEIs, but still play a role, potentially through exposure to pesticides/insecticides, or via fungal or parasitic infections following penetrating injuries.52,54 Although it is rare, infectious keratitis is a sight-threatening disease that can follow these penetrating injuries, and it is associated with significant economic and societal burdens, in addition to ocular morbidity.56
Clinically, severe agricultural OEIs often present as OGIs. A study of OEIs in Northern Thailand, where agricultural workers were found to have a high rate of OGIs, reported that these OGIs often manifested with IOFBs, endophthalmitis, and retinal detachment.35 Kikushima et al also reported high rates of IOFBs, but they noted lower rates of retinal detachment (only 10.0% of their cohort). Instead, full- and partial-thickness corneal penetrations were most common (56.7%).55 In West Virginia, superficial injuries, FBs, and atopic conjunctivitis had the highest incidence among OEIs of agricultural workers.21 Other prevalent injuries include contusions, lacerations, and corneal ulcerations, as well as severe cataracts, pterygium, or corneal erosions caused by ultraviolet (UV) radiation.54,55,57 UV radiation constitutes a significant occupational exposure for agricultural workers that manifests outside of acute injury. For instance, a study of occupational ocular morbidities performed in India found that pterygium in 16.6% of patients working in agriculture, pinguecula in 11.6%, and conjunctival pigmentation in 23.3%. Cataract lens changes were observed in 78% of workers as well.54 Although the presence of cataract or pterygium does not constitute an acute OEI, these conditions may impact vision and increase the risk of incurring another non-ocular injury in the workplace.54
Agricultural OEIs are typically severe injuries and often cause complications that may necessitate further surgical intervention or lead to permanent vision loss. Common interventions include corneal suturing, lensectomy, pars plana vitrectomy, lacrimal canaliculi reconstruction, or a combination of these.55 Kikushima et al reported that 83% of patients with an OEI required emergency ophthalmic surgery, and some required follow-up procedures.55 The study of OEIs in Thailand found that after treatment, although vision did improve, 42% of those that suffered from OGIs had a final BCVA of 20/400 or worse.35 This finding is supported by other evaluations that also found the highest severity of injury among agricultural OEIs.9 For instance, a study in Northern Italy examining work-related eye injuries found that the longest recovery times occurred in agriculture (3.4 days) compared to industry (2.3 days) and services (2.1 days). Even though the absolute number of agricultural OEIs was lower compared to industry, the frequency of injury was quite similar.9 The same study found that residual vision loss (RVL) was observed more frequently in agricultural injury claims compared to non-agricultural claims, and a third of RVL cases resulted in bilateral vision loss greater than 4/20.9 This can often translate to a disproportionate economic impact of agricultural OEIs for agrarian communities, as their livelihoods depend on their ability to farm, which is compromised by visual impairment.53 In communities lacking agricultural mechanization, the value and necessity of each worker is heightened,53 making the prevention of agricultural OEI a critical objective.
Other Occupational Eye Trauma
OEIs occur in a number of workplace settings beyond those commonly studied. For instance, the incidence of OEIs in deployed military personnel is estimated around 10–16%58 with varied mechanism. The use of mustard gas, an alkylating agent, can cause ocular surface complications and severe vision loss.59 In contrast, blast injuries can result in blunt trauma or penetrating injury from IOFBs. Even with the use of eye protection, high rates of ocular trauma have been reported among military personnel, with one study reporting 37% of ocular trauma to be bilateral.60 Delays in clinical care for injuries that occur on the battlefield may also contribute to worse visual outcomes among military personnel.60 Travor et al quantified the disability associated life years of ocular injuries among deployed US service members and found significant burden associated with these OEIs.58
OEIs have also been reported in service jobs and other industries.20,21 An examination of OEIs in 2019 by the US BLS identified 24.8% occurred in the service industry, 17.0% in transportation, and 16.6% in production.2 Within the healthcare sector, regular use of protective eyewear can also reduce rates of injury and infection. Ekmekcioglu and Ulnur reported on a range of ocular injuries that can occur within dentistry, affecting both healthcare practitioners and patients during treatments, including from laser devices and high-speed drills that can create high-velocity FBs.61 Increased exposure to radiation among healthcare workers can also increase risk of posterior subcapsular cataracts, underscoring the need to promote adherence to protective eyewear in these settings.62 More broadly, an observational study of healthcare workers found an incidence of 8 per 1000 in six months, with an even distribution of infectious and noninfectious eye hazards.63 Among affected individuals, awareness of personal protective equipment and adequate usage was relatively low (45% and 28%, respectively).63
OEIs described in other occupations include within the food preparation,64 textile/garment,65 and transportation66 industries. A survey of 300 restaurant workers found 29% reported symptoms of eye disorders, possibly attributed to high temperatures and smoke as well as the use of different ingredients, chemicals, and detergents.64 In this cohort, only one individual endorsed the use of protective eyewear.64 Ocular FBs have also been reported as sources of OEIs in food preparation and textile/leather workers.67 Qualitative interviews with female garment workers highlighted frequent ocular complaints among this population.65 Similarly, ocular symptoms are commonly reported among transportation workers.66 Occupational transportation and traffic accidents occur outside of transport workers as well, and these injuries may also carry significant extra-ocular morbidity.67 A study of 109 auto-workers in Nigeria found a high rate (73.3%) of OEIs, most commonly from metal particles and petroleum or hydraulic oil.68 Although only eight eyes had VA 20/60 or worse, the majority (87.2%) of these autoworkers did not endorse using any eye protection at work.68
Unfortunately, there is a paucity of data available on OEIs in many of these sectors. A limitation of the literature on OEIs is the varied reporting and classification of OEIs. Although the use of survey studies, chart reviews, and large-scale database studies all provide unique insights, these different study designs can contribute to varied results. In addition, stratification using different trauma scoring systems such as the Birmingham Eye Trauma Terminology or the Ocular Trauma Score can also affect generalizability of studies. Standardization of reporting across different settings may provide insights that can be better compared and analyzed. Similarly, greater investigation into occupational risks and visual outcomes among these workers can elucidate how to best protect against these injuries.
Attitudes Towards the Use of Eye Protection
It has been well-documented that OEIs frequently occur in the absence of eye protection,19 and that the use of protective eyewear is effective in reducing OEIs.27 For instance, no eye protection was worn in 89.1%,5 78.6%,69 and 98%35 of individuals who suffered from OEIs in some studies. Several barriers to the use of eye protection have been previously identified and are summarized in Table 1. Punnonen13 described reasons workers were not using eye protection, including the perception that the task was quick, user discomfort, and dislike of safety googles due reduced visual field. Poor fit and goggle fogging have been raised as compliance barriers as well.70 In the United States, OSHA regulations mandate precautions at the federal level, and state plans must be equally strict or stricter than the federal guideline.1 However, even with these regulations, lack of perceived need for eye protection is still a major factor contributing to low compliance.27 Industry-specific education that enables workers to identify hazards and understand the potential consequences of working without protective gear may help promote compliance.70
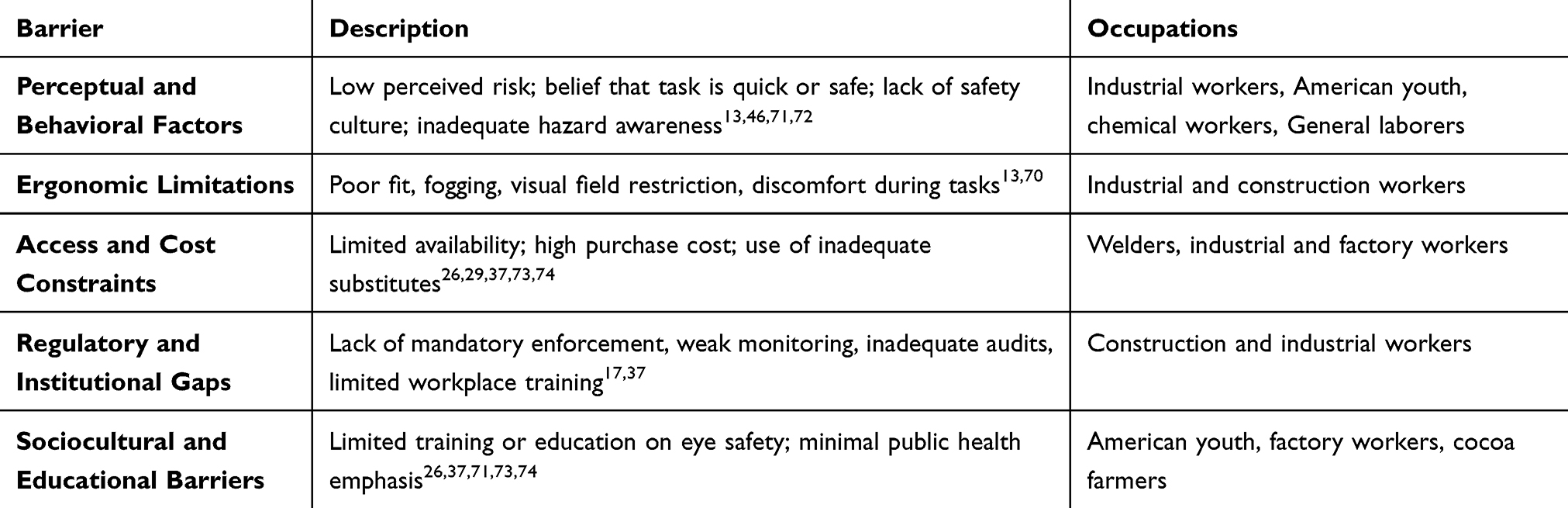 |
Table 1 Categorization of Major Reported Barriers to Protective Eyewear Use |
In populations of workers that have access to eye protection, other obstacles can preclude their use. A US-based survey study of youth (ages 14–24 years old) highlighted possible gaps in public health education, where individuals had generalized eye safety concerns around screen time and UV light, but little concern towards and eye protection use for sport or work activities.71 Outside of the US, significant variation in both safety regulations and access to eye protection impacts OEI rates. A survey of welders in Ghana found that the majority of workers did not use eye protection because it was not mandatory and they had never received safety training, even though they had access to the equipment.37 In contrast, a 2019 survey of industrial workers in Ethiopia found eye protection access to be a significant problem, with almost 70% of employees using sunglasses as their sole eye protection. In the same survey, the majority of individuals reported lack of access in the workplace and agreed that that purchase was too expensive.29 Similarly, a survey of factory workers in Nepal found that almost three-quarters of employees denied ever wearing eye protection while working, although 38% reported having experienced at least one ocular injury at work.26 Of these individuals, not all (86%) sought medical treatment.26 In addition, despite the existence of labor laws in India, a review of OEIs among construction workers has found low compliance in the setting of the lack of safety norms, audits, and monitoring by regulatory bodies.17 Limited data on some cohorts, such as the manufacturing sector, can also limit efforts to increase accessibility and change the culture around eye protection use.17
Kyriakaki also examined barriers to protective eye equipment among individuals of different lines of work and nationalities and found varying obstacles.18 For instance, lack of funds was highlighted among cocoa farm workers in Ghana,73,74 while lack of risk awareness was observed among chemical workers in China.46 Among foreign employees working in industrial roles, inadequate and incorrectly fitted protective eyewear was present in the workplace.75,76 A general review of occupational accidents in Nordic countries also emphasized that poor safety culture often contributes to workers feeling rushed and with minimal control over the working pace.72 This may exacerbate the lack of safety culture in some settings.
Interventions to Increase Eye Protection Use
Different interventions have been tested to increase adherence to protective eyewear, although large-scale results with statistically significant differences have not yet been demonstrated, especially in recent years.77,78 Such programs often incorporate multiple components, including education on safety practice, free protective eyewear, periodic vision screening, and the institution of safety guidelines. Although increases in adherence were often observed at the start of each study, compliance generally wanes over time. Some behavioral interventions, such as disciplinary actions for noncompliance, may increase the use of eye protection; however, because various studies measure different endpoints at different times, the long-term effects of these interventions may be difficult to determine.77
Other efforts, such as those focused on standardizing protective eye gear and simplifying regulations, may improve compliance and reduce rates of OEIs.70 As lens material technology improves and more data has become available on the mechanisms by which OEIs occur, eye protection design has shifted to a more comprehensive approach. Rather than a focus on specifying individual materials or components, current standards prioritize overall performance, including such as impact resistance, UV protection, and coverage of the ocular adnexa.70 This promotes better eye protection design and helps employers select gear that meets safety requirements without sacrificing comfort or usability.
Emerging technologies may also be used to enhance compliance with safety regulations. Several new innovations have allowed employers to track utilization of safety equipment. For instance, the DBI-SALA Smart Lock Connected SRL technology, produced by 3M Technologies (Minnesota, USA), uses integrated sensors and Bluetooth to assist with tracking compliance and incident reporting.79 This not only allows employers to identify areas with low usage of safety equipment but also streamlines the monitoring process. However, updated data piloting these new interventions is necessary to assess their efficacy. In addition, evaluation of other factors affecting eye protection availability and use may also provide insights into worker behaviors. For instance, although OEIs decreased during the COVID era,80 investigation into the cause of this change (decreased work or greater use of personal protective equipment), can be beneficial to continue to reduce OEIs in the post-COVID era.
Conclusion
Despite ongoing regulatory and educational efforts, OEIs continue to pose a significant source of ocular morbidity across a wide range of industries. Although most common in young males, the spectrum of OEIs occurring in these settings is broad, and their etiologies are variable. High risk sectors, including construction, manufacturing, metalworking, agriculture, and occupations requiring chemical-handling, each present with unique hazards that require tailored prevention strategies. For instance, while industrial, construction, and agricultural settings expose employees to OGI risk, those with a chemical etiology are more likely to have a bilateral injury and worse subsequent morbidity. Although many OEIs are preventable, barriers to eye protection use persist, ranging from access to ergonomic challenges. Even with variations in reported injury rates and protective eyewear use in different occupations, the literature uniformly highlights persistent occupational hazards causing OEIs. Regulatory mandates, education, and new technological innovations may have a role in improving adherence to protective eyewear, but sustained impact remains a challenge. Industry-specific safety training may further reduce the incidence and severity of OEIs. However, there remains a gap in the literature regarding the epidemiological and outcomes of OEIs in some fields. Future studies may investigate long-term outcomes and disparities in access to safety resources, which can inform more effective prevention strategies. Greater investment into improving safety culture and awareness may improve worker health and ultimately reduce the burden of OEIs.
Abbreviations
CGI, Closed globe injury; FB, Foreign body; MeSH, Medical Subject Headings; OEI, Occupational eye injury; OGI, Open globe injury; OSHA, Occupational Safety and Health Administration; RH, Roper Hall; RVL, Residual vision loss; US BLS, United States Bureau of Labor Statistics; UV, Ultraviolet; VA, Visual acuity.
Funding
There is no funding to report.
Disclosure
Dr Albert Khouri is speaker/consultant for Bausch and Lomb, Glaukos, and Alcon, outside the submitted work; also reports grants from NJ Health Foundation and NJ Fund for the Blind. The authors declare no other conflicts of interest regarding this manuscript.
References
1. Eye and face protection (US department of labor). 2016.
2. Patel A, Berkowitz S, Sridhar J, Durrani A, Patel S. Trends in workplace-related eye injuries in the United States from 2011 through 2020. J Vitreoretin Dis. 2023;7(1):49–56. doi:10.1177/24741264221117418
3. Survey of occupational injuries and illnesses data (US bureau of labor statistics). 2021.
4. Aryasit O, Tassanasunthornwong C, Rattanalert N, Tengtrisorn S, Singha P. Risk factors for globe removal after open-globe injury in agricultural regions. Sci Rep. 2022;12(1):17122. doi:10.1038/s41598-022-21666-7
5. Lee BWH, Samarawickrama C. Closed globe and adnexal eye injuries: epidemiology, clinical and surgical outcomes, and an economic cost analysis. Clin Exp Ophthalmol. 2023;51(5):425–436. doi:10.1111/ceo.14232
6. Kousiouris P, Klavdianou O, Douglas KAA, et al. Role of socioeconomic status (SES) in globe injuries: a review. Clin Ophthalmol. 2022;16(null):25–31. doi:10.2147/OPTH.S317017
7. Lee BWH, Hunter D, Robaei DS, Samarawickrama C. Open globe injuries: epidemiology, visual and surgical predictive variables, prognostic models, and economic cost analysis. Clin Exp Ophthalmol. 2021;49(4):336–346. doi:10.1111/ceo.13944
8. McCall BP, Horwitz IB. Assessment of occupational eye injury risk and severity: an analysis of Rhode Island workers’ compensation data 1998–2002. Am J Ind Med. 2006;49(1):45–53. doi:10.1002/ajim.20234
9. Gobba F, Dall’Olio E, Modenese A, De Maria M, Campi L, Cavallini GM. Work-related eye injuries: a relevant health problem. Main epidemiological data from a highly-industrialized area of Northern Italy. Int J Environ Res Public Health. 2017;14(6):604. doi:10.3390/ijerph14060604
10. Sahraravand A, Haavisto AK, Holopainen JM, Leivo T. Ocular traumas in working age adults in Finland - Helsinki ocular trauma study. Acta Ophthalmol. 2017;95(3):288–294. doi:10.1111/aos.13313
11. Kumar P. Vishweshwaraiah Iron Steel Limited (VISL) fire disasters following steel converter blast, 30 July 2003. Burns. 2010;36(1):135–138. doi:10.1016/j.burns.2009.04.029
12. Aggarwal S, Maitz P, Kennedy P. Electrical flash burns due to switchboard explosions in New South Wales—A 9-year experience. Burns. 2011;37(6):1038–1043. doi:10.1016/j.burns.2011.01.017
13. Punnonen E. Epidemiological and social aspects of perforating eye injuries. Acta Ophthalmol. 1989;67(5):492–498. doi:10.1111/j.1755-3768.1989.tb04098.x
14. Omar R, Anan NS, Azri IA, Majumder C, Knight VF. Characteristics of eye injuries, medical cost and return-to-work status among industrial workers: a retrospective study. BMJ open. 2022;12(1):e048965. doi:10.1136/bmjopen-2021-048965
15. Almoosa A, Asal A, Atif M, Ayachit S, Doms P. Occupational Eye Injury: the neglected role of eye protection. Bahrain Med Bulletin. 2017;39(2):82–84. doi:10.12816/0047525
16. Protecting your eyes at work. protecting your vision. American optometric association. Available from: https://www.aoa.org/healthy-eyes/caring-for-your-eyes/protecting-your-vision.
17. Jha KN. Ocular trauma has fallen on our blind spot. J Clin Ophthalmol Res. 2016;4(2):65. doi:10.4103/2320-3897.183656
18. Kyriakaki ED, Symvoulakis EK, Chlouverakis G, Detorakis ET. Causes, occupational risk and socio-economic determinants of eye injuries: a literature review. Med Pharm Rep. 2021;94(2):131–144. doi:10.15386/mpr-1761
19. Nowrouzi-Kia B, Nadesar N, Sun Y, Gohar B, Casole J, Nowrouzi-Kia B. Types of ocular injury and their antecedent factors: a systematic review and meta-analysis. Am J Ind Med. 2020;63(7):589–599. doi:10.1002/ajim.23117
20. Li Q, Drinkwater JJ, Hoskin A, Turner AW. Eye injury epidemiology in Australia: a 25-year systematic review and public health perspective. Clin Exp Ophthalmol. 2025. doi:10.1111/ceo.14596
21. Islam SS, Doyle EJ, Velilla A, Martin CJ, Ducatman AM. Epidemiology of compensable work-related ocular injuries and illnesses: incidence and risk factors. J Occup Environ Med. 2000;42(6):575–581. doi:10.1097/00043764-200006000-00004
22. Patil SB, Biala A, Khanna A, Meena A. Prevalence of ocular trauma in KLES Hospital: a 1-year cross-sectional study. Indian J Health Sci Biomed Res Kleu. 2016;9(2):175. doi:10.4103/2349-5006.191262
23. Luo H, Beckles GL, Fang X, Crews JE, Saaddine JB, Zhang X. Socioeconomic status and lifetime risk for workplace eye injury reported by a us population aged 50 years and over. Ophthalmic Epidemiol. 2012;19(2):103–110. doi:10.3109/09286586.2011.639977
24. Zhou B, Uppuluri A, Zarbin MA, Bhagat N. Work-related ocular trauma in the United States: a national trauma databank study. Graefes Arch Clin Exp Ophthalmol. 2023;261(7):2081–2088. doi:10.1007/s00417-023-05983-9
25. Sahraravand A, Haavisto AK, Puska P, Leivo T. Work tool-related eye injuries: helsinki ocular trauma study. Int Ophthalmol. 2020;40(3):753–761. doi:10.1007/s10792-019-01237-y
26. Limbu B, Moore G, Marvasti AH, Poole ME, Saiju R. Work related ocular injury: Nepal. Nepal J Ophthalmol. 2018;10(19):47–56. doi:10.3126/nepjoph.v10i1.21689
27. Blackburn JL, Levitan EB, MacLennan PA, Owsley C, McGwin G. Changes in eye protection behavior following an occupational eye injury. Workplace Health Safety. 2012;60(9):393–400. doi:10.1177/216507991206000904
28. Atalay YA, Gebeyehu NA, Gelaw KA. Systematic review and meta-analysis on prevalence, pattern, and factors associated with ocular protection practices among welders in sub-Saharan Africa. Front Public Health. 2024;12:1397578. doi:10.3389/fpubh.2024.1397578
29. Mengistu HG, Alemu DS, Alimaw YA, Yibekal BT. Prevalence of occupational ocular injury and associated factors among small-scale industry workers in Gondar Town, Northwest Ethiopia, 2019. Clin Optom. 2021;Volume 13:167–174. doi:10.2147/OPTO.S290257
30. Hargreaves S, Rustage K, Nellums LB, et al. Occupational health outcomes among international migrant workers: a systematic review and meta-analysis. Lancet Glob Health. 2019;7(7):e872–e882. doi:10.1016/S2214-109X(19)30204-9
31. Martin-Prieto S, Álvarez-Peregrina C, Thuissard-Vasallo I, et al. Description of the epidemiological characteristics of work-related eye injuries in Spain: a retrospective study. BMJ Open. 2020;10(10):e035696. doi:10.1136/bmjopen-2019-035696
32. Agrawal C, Girgis S, Sethi A, et al. Etiological causes and epidemiological characteristics of patients with occupational corneal foreign bodies: a prospective study in a hospital-based setting in India. Indian J Ophthalmol. 2020;68(1):54–57. doi:10.4103/ijo.IJO_623_19
33. Mashimbyi M, Seisa KJ, Ramathuthu M, Sepadi MM. Assessing occupational safety risks and challenges among informal welders in Pretoria West, South Africa. Int J Environ Res Public Health. 2025;22(7):1132. doi:10.3390/ijerph22071132
34. Adak P, Ghoshal R, Kumar N. Effectiveness of a multifaceted intervention on ocular health and ophthalmic safety among metal workers of Moradabad, Uttar Pradesh. Indian J Occup Environ Med. 2025;29(2):102–109. doi:10.4103/ijoem.ijoem_291_24
35. Chaikitmongkol V, Leeungurasatien T, Sengupta S. Work-related eye injuries: important occupational health problem in Northern Thailand. Asia-Pac J Ophthalmol. 2015;4(3):155–160. doi:10.1097/APO.0000000000000046
36. Wu H, Wang JY, Zhong XC, Shi X, Wu YH, Ye J. Ocular injury resulting in eye removal at a large tertiary care center in China. Int J Ophthalmol. 2020;13(8):1312–1317. doi:10.18240/ijo.2020.08.19
37. Kwaku Tetteh KK, Owusu R, Axame WK. Prevalence and factors influencing eye injuries among welders in Accra, Ghana. Adv Prev Med. 2020;2020:2170247. doi:10.1155/2020/2170247
38. Berglund L, Johansson M, Nygren M, Samuelson B, Stenberg M, Johansson J. Occupational accidents in Swedish construction trades. Int J Occup Saf Ergon. 2021;27(2):552–561. doi:10.1080/10803548.2019.1598123
39. Guzmán-Almagro E, Fernandez-Sanz G, Herrero-Escudero D, Contreras I, González Martín-Moro J. Open-globe-injury: a single center Spanish retrospective 5-year cohort study. European J Ophthalmol. 2021;31(5):2710–2716. doi:10.1177/1120672120962039
40. Kolomeyer AM, Shah A, Bauza AM, Langer PD, Zarbin MA, Bhagat N. Nail gun-induced open-globe injuries: a 10-year retrospective review. Retina. 2014;34(2):254–261. doi:10.1097/IAE.0b013e3182979e0b
41. Ilhan C, Citirik M, Uzel MM, Bagli S. Characteristics of work-related eye trauma in construction and manufacturing industries. Clin Exp Optom. 2022;105(5):546–551. doi:10.1080/08164622.2021.1952842
42. Ezinne NE, Ekemiri KK, Nwanali Daniel MA. Occupational ocular injuries and utilization of eye protective devices among sawmill workers in the ojo local government area of Lagos State, Nigeria. Vision. 2021;5(4). doi:10.3390/vision5040060
43. Quesada JM-A, Lloves JM, Delgado DV. Ocular chemical burns in the workplace: epidemiological characteristics. Burns. 2020;46(5):1212–1218. doi:10.1016/j.burns.2019.11.007
44. Kate A, Sharma S, Yathish S, et al. Demographic profile and clinical characteristics of patients presenting with acute ocular burns. Indian J Ophthalmol. 2023;71(7):2694–2703. doi:10.4103/ijo.Ijo_3330_22
45. Hom GL, Kalur A, Iyer A, Singh RP. Ocular occupational injuries in the United States between 2011–2018. Occup Med. 2022;72(4):255–259. doi:10.1093/occmed/kqab189
46. Ye C, Wang X, Zhang Y, et al. Ten-year epidemiology of chemical burns in western Zhejiang Province, China. Burns. 2016;42(3):668–674. doi:10.1016/j.burns.2015.12.004
47. Novak JF. Ocular trauma in industry. J Occup Environ Med. 1970;12(8):287–290.
48. Cronbach N, Foot B, Scawn R. Severe ocular chemical injury in the UK: a British ophthalmological surveillance unit study. Eye. 2024;38(13):2552–2556. doi:10.1038/s41433-024-03073-6
49. Le Q, Chen Y, Wang X, Hong J, Sun X, Xu J. Analysis of medical expenditure and socio-economic status in patients with ocular chemical burns in East China: a retrospective study. BMC Public Health. 2012;12(1):409. doi:10.1186/1471-2458-12-409
50. Agriculture: a hazardous work. 2015. Available from: https://www.ilo.org/resource/agriculture-hazardous-work-0.
51. Jovanovic N, Peek-Asa C, Swanton A, et al. Prevalence and risk factors associated with work-related eye injuries in Bosnia and Herzegovina. Int J Occup Environ Health. 2016;22(4):325–332. doi:10.1080/10773525.2016.1243081
52. Ghafari M, Cheraghi Z, Doosti-Irani A. Occupational risk factors among Iranian farmworkers: a review of the available evidence. Epidemiol Health. 2017;39:e2017027. doi:10.4178/epih.e2017027
53. Chatterjee S, Agrawal D. Primary prevention of ocular injury in agricultural workers with safety eyewear. Indian J Ophthalmol. 2017;65(9):859–864. doi:10.4103/ijo.IJO_334_17
54. Janani S, Krithica S, Saranya SB, et al. Occupational hazards, associated ocular morbidities and impact of refractive safety eyewear among agriculture workers in India - a two state study. Indian J Occup Environ Med. 2024;28(3):182–188. doi:10.4103/ijoem.ijoem_254_23
55. Kikushima W, Sakurada Y, Kashiwagi K. Characteristics of grape shelf eye injuries at vineyards in Japan. J Clin Med. 2022;11(23):7079. doi:10.3390/jcm11237079
56. Stapleton F. The epidemiology of infectious keratitis. Ocul Surf. 2023;28:351–363. doi:10.1016/j.jtos.2021.08.007
57. Riccò M, Vezzosi L, Mezzoiuso AG. Occupational eye injuries in the agricultural settings: a retrospective study from North-Eastern Italy. Acta Biomed. 2020;90(4):457–467. doi:10.23750/abm.v90i4.7602
58. Travor MD, Levine ES, Catomeris AJ, et al. Disability-adjusted life years resulting from ocular injury among deployed service members, 2001–2020. Ophthalmology. 2024;131(5):534–544. doi:10.1016/j.ophtha.2023.11.023
59. Soleimani M, Momenaei B, Baradaran-Rafii A, et al. Mustard gas-induced ocular surface disorders: an update on the pathogenesis, clinical manifestations, and management. Cornea. 2023;42(6):776–786. doi:10.1097/ico.0000000000003182
60. Kempuraj D, Mohan RR. Blast injury: impact to the cornea. Exp Eye Res. 2024;244:109915. doi:10.1016/j.exer.2024.109915
61. Ekmekcioglu H, Unur M. Eye-related trauma and infection in dentistry. Journal of Istanbul University Faculty of Dentistry. 2017;51(3):55–63. doi:10.17096/jiufd.60117
62. Alhasan AS, Aalam WA. Eye lens opacities and cataracts among physicians and healthcare workers occupationally exposed to radiation: a systematic review and meta-analysis. Saudi Med J. 2022;43(7):665–677. doi:10.15537/smj.2022.43.7.20220022
63. Obed P, Amritanand A, Antipas OJH, et al. Acute work-related hazardous eye exposures in a health care environment – an observational study from a tertiary care hospital in South India. Indian J Ophthalmol. 2021;69(12):3532–3537. doi:10.4103/ijo.IJO_912_21
64. Jahangiri M, Eskandari F, Karimi N, Hasanipour S, Shakerian M, Zare A. Self-reported, work-related injuries and illnesses among restaurant workers in Shiraz City, South of Iran. Ann Glob Health. 2019;85(1). doi:10.5334/aogh.2440
65. Akhter S, Rutherford S, Chu C. Sewing shirts with injured fingers and tears: exploring the experience of female garment workers health problems in Bangladesh. BMC Int Health Human Rights. 2019;19(1):2. doi:10.1186/s12914-019-0188-4
66. Shetty K, Prabhu S, D’Cunha D, D’Souza O, Suvarna A, Jacob B. Morbidity profile of transport sector workers and its correlation with social and work factors. Int J Med Sci Public Health. 2016;5(10):2030. doi:10.5455/ijmsph.2016.12022016407
67. Hösükler E, Turan T, Erkol ZZ. Analysis of injuries and deaths by trauma scores due to occupational accidents [İş kazasına bağlı yaralanma ve ölümlerin travma skorları ile analizi]. Ulus Travma Acil Cerrahi Derg. 2022;28(9):1258–1269. doi:10.14744/tjtes.2022.22796
68. Abraham EG, Megbelayin EO, Akpan SI. Awareness and use of protective eye devices among auto mechanic technicians and auto spare parts traders in Uyo, Nigeria. Int J Med Sci Public Health. 2015;4(9):1227. doi:10.5455/ijmsph.2015.05052015254
69. Voon LW, See J, Wong TY. The epidemiology of ocular trauma in Singapore: perspective from the emergency service of a large tertiary hospital. Eye. 2001;15(Pt 1):75–81. doi:10.1038/eye.2001.18
70. Hoskin AK, Mackey DA, Keay L, Agrawal R, Watson S. Eye Injuries across history and the evolution of eye protection. Acta Ophthalmologica. 2019;97(6):637–643. doi:10.1111/aos.14086
71. Killeen OJ, Waselewski E, Vorias T, et al. US youth perspectives on eye trauma and eye protection. J Aapos. 2024;28(4):103949. doi:10.1016/j.jaapos.2024.103949
72. Hanvold TN, Kines P, Nykänen M, et al. Occupational safety and health among young workers in the Nordic countries: a systematic literature review. Safety Health Work. 2019;10(1):3–20. doi:10.1016/j.shaw.2018.12.003
73. Boadi-Kusi SB, Hansraj R, Mashige KP, Ilechie AA. Factors associated with protective eyewear use among cocoa farmers in Ghana. Inj Prev. 2016;22(5):365–369. doi:10.1136/injuryprev-2014-041531
74. Boadi-Kusi SB, Hansraj R, Kumi-Kyereme A, et al. Ocular health assessment of cocoa farmers in a rural community in Ghana. J Agromed. 2014;19(2):171–180. doi:10.1080/1059924X.2014.886537
75. Shepherd M, Barker R, Scott D, Hockey R, Spinks D, Pott R. Occupational eye injuries. Injury Bulletin Queensland Injury Surveillance Unit. 2006.
76. Ngo C, Leo S. Industrial accident-related ocular emergencies in a tertiary hospital in Singapore. Singapore Med J. 2008;49(4):280.
77. Lipscomb HJ. Effectiveness of interventions to prevent work-related eye injuries. Am J Preventive Med. 2000;18(4, Supplement 1):27–32. doi:10.1016/S0749-3797(00)00138-0
78. Dyreborg J, Lipscomb HJ, Nielsen K, et al. Safety interventions for the prevention of accidents at work: a systematic review. Campbell Syst Rev. 2022;18(2):e1234. doi:10.1002/cl2.1234
79. Patel V, Chesmore A, Legner CM, Pandey S. Trends in workplace wearable technologies and connected-worker solutions for next-generation occupational safety, health, and productivity. Adv Intell Sys. 2022;4(1):2100099. doi:10.1002/aisy.202100099
80. Liang H, Zhang M, Chen M, Lin TPH, Lai M, Chen H. Ocular trauma during COVID-19 pandemic: a systematic review and meta-analysis. Asia-Pac J Ophthalmol. 2022;11(5):481–487. doi:10.1097/APO.0000000000000539
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Open Globe Injuries: Review of Evaluation, Management, and Surgical Pearls
Zhou Y, DiSclafani M, Jeang L, Shah AA
Clinical Ophthalmology 2022, 16:2545-2559
Published Date: 10 August 2022
Comparison of Time-to-Surgery and Outcomes in Transferred Vs Non-Transferred Open Globe Injuries

Fernandez EO, Miller HM, Pham VQ, Fleischman D
Clinical Ophthalmology 2022, 16:2733-2742
Published Date: 22 August 2022
Vitreoretinal Injury Associated with Sports Ball Ocular Trauma
Rohowetz LJ, Fan J, Flynn HW Jr
Clinical Ophthalmology 2025, 19:1931-1943
Published Date: 23 June 2025