Back to Journals » International Journal of General Medicine » Volume 15
Pattern and Sensitivity of Bacterial Colonization on the Tip of Non-Tunneled Temporary Hemodialysis Catheters: Results of a Tertiary Hospital in Somalia
Authors Mohamud Hussein A ![]() , Kizilay M, Ali Nur Adam A, Farah Yusuf Mohamud M
, Kizilay M, Ali Nur Adam A, Farah Yusuf Mohamud M ![]() , Dirie AMH
, Dirie AMH ![]() , Hussein Mohamed A
, Hussein Mohamed A ![]() , UÇaroĞlu E
, UÇaroĞlu E
Received 1 July 2022
Accepted for publication 17 August 2022
Published 24 August 2022 Volume 2022:15 Pages 6775—6781
DOI https://doi.org/10.2147/IJGM.S379642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdinafic Mohamud Hussein,1 Mehmet Kizilay,1 Abdirahim Ali Nur Adam,2 Mohamed Farah Yusuf Mohamud,3 Abdirahman Mohamed Hassan Dirie,4 Abdikarim Hussein Mohamed,5 Erhan UÇaroĞlu1
1Department of Cardiovascular Surgery, Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 2Department of Microbiology and Infectious Diseases, Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 3Department of Emergency Medicine, Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 4Department of Pulmonology, Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia; 5Department of Urology, Mogadishu Somalia Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia
Correspondence: Abdinafic Mohamud Hussein, Email [email protected]
Introduction: Bacterial colonization on the tip of non-tunneled temporary hemodialysis catheters (NTHCs) and associated catheter-related infections (CRI) is a common complication in hemodialysis (HD) patients. In this study, we aimed to investigate the pattern of bacterial colonization formed on the tip of non-tunneled temporary hemodialysis catheters and their antibiotic sensitivity.
Methods: This retrospective analysis was performed in the HD unit of an Education and Research Hospital that follows up a universe of approximately 300 patients, primarily from Mogadishu, Somalia. From September 2020 to September 2021, a total of 137 temporary HD catheters were removed and their tips were sent for culture after there was a suspicion of CRI and other sources of infection were excluded. HD Catheter tips were cultured semi-quantitatively, and the antibiogram of the positive cultures was studied.
Results: Gram-positive cocci were found to be the most predominant bacterial organisms in positive cultures with 27 (31.0%) for Staphylococcus aureus, 9 (10.3%) for Staphylococcus haemolyticus and 5 (5.7%) for Staphylococcus epidermidis. We found Enterococci to be 5.7% of the isolated microorganisms. Gram-negative pathogens isolated included Escherichia coli 13 (14.9%) as the most common, followed by Klebsiella pneumoniae 10 (11.5%) and Acinetobacter baumannii (4.6%). Methicillin-resistant Staphylococcus aureus (MRSA) was found to be 9.4%. Gram-positive isolates showed high sensitivity (100%) to Linezolid, Daptomycin, Vancomycin, and Tigecycline, but a low sensitivity rate to Oxacillin (41.2%). Gram-negative isolates had the highest sensitivity to Tigecycline (100%), Imipenem (88.9%), and Amikacin (87%) but low sensitivity to Ampicillin (4.8%), Trimethoprim/Sulfamethoxazole (TMP-SMX) (23.1%), and Ceftazidime (7.1%).
Conclusion: We conclude that each institution should have its own antibiogram in the management of HD CRIs. According to our findings in this study, we recommend intravenous Vancomycin and Imipenem as empirical therapy in patients with suspected HD CRIs.
Keywords: antibiogram, antibiotics, bacterial colonization, catheter-related infection, hemodialysis, temporary catheters
Introduction
HD is essential for patients with acute or chronic kidney disease. Its use is a frequent and growing practice worldwide. Every year, millions of intravascular catheters are used in healthcare centers to establish vascular access sites through the insertion of a catheter into a femoral, subclavian or internal jugular vein if a fistula is not present.1,2 NTHCs are usually used when there is an urgent need for vascular access in patients who require immediate HD.3 Unfortunately, the discouraging fact is that the use of these catheters is associated with bacterial colonization that produces a biofilm (a slimy mucopolysaccharide matrix) on the catheter surface. The biofilm forms a shield for the microorganisms protecting them from innate immune defenses. Bacterial biofilm is associated with catheter-related bloodstream infections (CRBSI) followed by serious complications that may lead into patient morbidity and mortality.4,5 CRBSI and related complications requiring hospitalization account for nearly one-third of the cost of chronic kidney disease management with reported mortality rates of 12–25.9%.6 Timely diagnosis and management of the responsible microorganism with appropriate antibiotics are crucial to prevent infectious complications. Therefore, a better understanding of the pathogenesis of these infections is important in developing management strategies to reduce the occurrences of catheter-related sepsis.
In Somalia, NTHCs are commonly used as a source of temporary vascular access for the initiation of HD in both acute and chronic kidney disease patients, and to our knowledge, there are no previous studies on the pattern and sensitivity of bacterial colonization at the tip of hemodialysis catheters. This present study aimed to investigate the pattern of bacterial colonization formed on the tip of non-tunneled temporary hemodialysis catheters and their antimicrobial susceptibility.
Methods
We conducted this retrospective analysis in the HD unit of Education and Research Hospital that follows up a universe of approximately 300 patients, primarily from Mogadishu, Somalia.
We carried out the study from September 2020 to September 2021. A total of 137 temporary hemodialysis catheters were removed and their tips were sent for culture. Catheters were removed and sent for culture when there was a suspicion of CRI and other sources of infection were excluded. All catheters which were removed due to other reasons were excluded from the study. Catheter-related infection was suspected when the patients present with fever, chills, rigors and pus at the catheter site. Peripheral blood cultures were also recorded. Catheter colonization was defined as a significant growth of a microorganism of >15 Colony Forming Units (CFUs) in the semiquantitative culture of the catheter tips.7 CRBSI was diagnosed if the same microorganism was grown from peripheral blood culture and catheter tip culture at least once.8
The catheters were removed under aseptic precautions by one investigator after obtaining informed consent from the patient. A 5-cm segment of the tips was cultured semi-quantitatively, by rolling them back and forth across the surface at least four times, on a blood agar plate. Colonies were counted after 24 hours of incubation at 37°C. The criteria of positivity were based on when more than 15 CFUs were isolated.7
Not all positive cultures were tested for the same list of antibiotics, as some bacteria were tested according to the availability of that antibiotic at the center or antibiotics upon special request. Cultures and antibiotic sensitivity to the bacteria were performed by the Infectious and Microbiology department of the Hospital following the standard laboratory protocols. The findings of bacterial microorganisms were achieved by using a BD BBL crystal identification system, as well as biochemical tests, including oxidase, coagulase, citrate, and catalase tests. Finally, antibiogram was performed using the standard Kirby–Bauer disk diffusion method and commercial disks (Oxoid discs). Cefoxitin-resistant Staphylococcus aureus was considered methicillin-resistant Staphylococcus aureus (MRSA), and the extended-spectrum beta-lactamase (ESBL) was identified using Cephalosporins (cefuroxime + ceftriaxone) and Amoxicillin-Clavulanic acid combination discs. Enterococcus antimicrobial susceptibility was assessed using blood agar.
Antibiotic susceptibility of the pathogens was studied by using Ciprofloxacin 5 mcg, Levofloxacin 5 mcg, piperacillin/tazobactam 100/10 mcg, Imipenem 10 µg, Amikacin 30 mcg, Tigecycline 15 ug, Penicillin G 1 U, Ampicillin 10 µg, Amoxicillin + Clavulanic Acid 20 + 10 µg, Ceftazidime 30 ug, Linezolid 30 mcg, Clindamycin 2 mcg, Gentamicin 120 µg, Daptomycin 30 mcg, TMX-SMX 1.25/23.75 mcg, Vancomycin 30 mcg, Tetracycline 30 mcg, Cefoxitin 30 mcg, Cefuroxime 30 µg, and Ceftriaxone 30 µg.
This study was carried out according to the Helsinki Declaration, and Ethical approval of this research was obtained from the research ethics committee of Mogadishu Somali Turkey Recep Tayyip Erdogan Training and Research Hospital with a reference number of MSTH/3784. The study’s objective was explained to the participants and all patients provided informed consent to participate in this study.
Patient demographics, including gender, age, and presence of concurrent disease states and cause of catheter removal were collected. Results of catheter tip cultures and antibiotic sensitivity were also recorded. Data were analyzed by using Statistical Package for Social Sciences (SPSS) version 23. Tables and figures were presented with Microsoft Word.
Results
This retrospective study included a total of 137 patients in which their temporary HD catheters were removed after catheter infection was suspected between September 1, 2020, and August 31, 2021. Eighty-one (59.1%) of the patients were male and 56 (40.9%) female. The average age was 51 years (range: 10–87 years).
The most significant comorbid diseases included anemia (94%), hypertension (47.4), diabetes mellitus (40.1%), and congestive heart failure (5.1%) (Table 1).
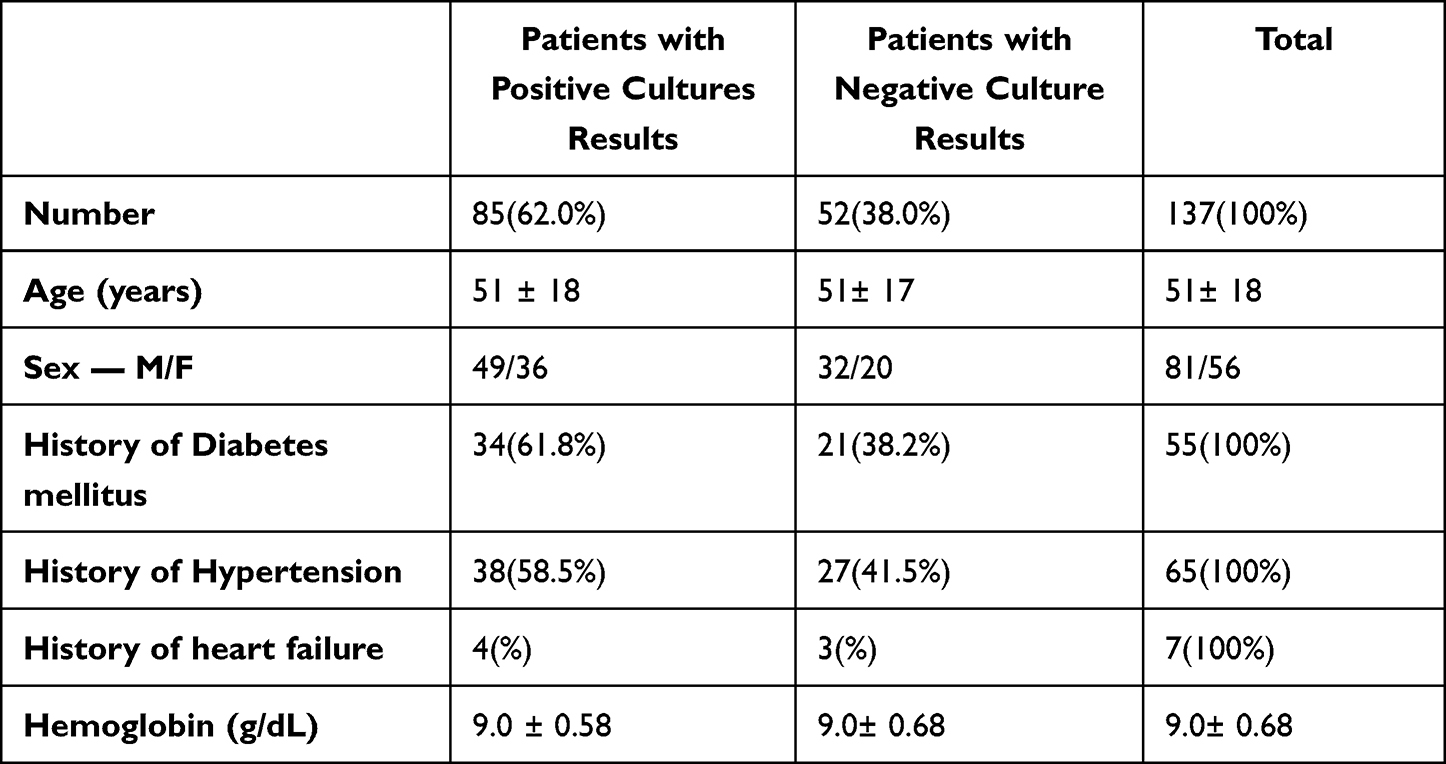 |
Table 1 Patient Characteristics |
The presenting signs and symptoms are seen to be fever most commonly (72%), pus at the catheter site (64%), chills (56.1%), and rigors (51.8%) (Figure 1).
 |
Figure 1 Presenting signs and symptoms of patients with confirmed catheter-related infections. |
HD catheter tip bacterial colonization was positive (>15 CFUs) in 85 (62.0%) patients and 52 (38.0%) were negative (no growth or <15 CFUs). According to the positive cultures, 46 (54.1%) were gram-positive and 39 (45.9%) were gram-negative. In our study 59 (69.4%) of the catheters with bacterial colonization at the tip of the catheter showed same organism growth at the peripheral blood culture confirming the presence of HD CRBSIs based on our study criteria.
Gram-positive cocci were the most predominant bacterial biofilm in positive cultures with a 27 (31.2%) for Staphylococcus aureus, 9 (10.6%) for Staphylococcus haemolyticus, and 5 (5.9%) for Staphylococcus epidermidis. Enterococci were found to be 5 (5.9%) of the isolated microorganisms (Table 2).
 |
Table 2 Pattern of Microorganisms Responsible for Hemodialysis Catheter Tip Bacterial Colonization |
Gram-negative pathogens isolated included Escherichia coli 13 (15.3%), Klebsiella pneumoniae 10 (11.8%), and Acinetobacter baumannii 4 (4.7%).
Antibiotic sensitivities tested against staphylococcal species indicated that they were completely sensitive (100%) to antibiotics like Linezolid, Daptomycin, Vancomycin, and tigecycline. Other antibiotics sensitivity to staphylococcus were as following Clindamycin 80.6%, Gentamicin 66.7%, Cefoxitin 63.9%, Tetracycline 55.6%, and Ciprofloxacin 51.4%. Gram-positive pathogens revealed the lowest sensitivity rate to Oxacillin (41.2%) (Table 3).
 |
Table 3 Staphylococcus aureus and Staphylococcus haemolyticus Catheter Tip Culture Susceptibilities |
The prevalence of Methicillin-resistant Staphylococcus aureus (MRSA) was found to be 9.4% (8 patients), and Vancomycin-Resistant Enterococci (VRE) was not found in our study.
Regarding Gram-negative pathogens, they displayed complete sensitivity (100%) to Tigecycline, 88.9% to Imipenem, 87% to Amikacin, 73.3% to cefoxitin, 70.4% to Gentamicin and Ciprofloxacin.
Gram-negative pathogens revealed the lowest sensitivity to Ampicillin (4.8%), Trimethoprim/Sulfamethoxazole (TMP-SMX) (23.1%), and Ceftazidime (7.1%). The prevalence of extended ESBLs among gram-negative cultures was found to be 20.5% (8 patients) (Table 4).
 |
Table 4 E. coli, Klebsiella pneumoniae and Acinetobacter baumannii Catheter Tip Culture Susceptibilities |
Discussion
Uncuffed, NTHCs are considered as the preferred way to gain immediate access for dialysis, although bacteremia is the primary complication that limits their use.3,9
This study aimed to reveal the bacterial colonization on the tip of NTHCs and their antibiotic sensitivity. Bacterial colonization on HD catheters is associated with a high rate of HD CRI. De Freitas et al reported a high correlation of 93.3%, between the catheter tip cultures and the peripheral blood cultures.2 To the authors’ knowledge, this is the first study to obtain data on HD catheter bacterial colonization and antibiotic sensitivity in Somalia.
Our results suggest that presenting signs and symptoms of chills, fever, rigors, and redness at the catheter site could be a good indicator of bacterial infection and bacterial colonization at the tip of the catheter in approximately 50% of cases.
The bacterial organisms isolated from catheter tip cultures were consistent with that associated with CRIs, indicating that gram-positive organisms including Staphylococcus aureus (S. aureus) and Staphylococcus coagulase-negative remain the most common organisms isolated. Similar results were found by Dopairak et al, Sathish et al, Blakestijin et al and Kairaitis et al.10–13
We identified Escherichia coli as the most common gram-negative organism followed by Klebsiella pneumoniae and Acinetobacter baumannii. This is comparable with the results found by Eleanor et al.14
Antibiogram is a list of laboratory testing used to examine the susceptibility of bacterial isolates to different types of antibiotics. To avoid bacterial resistance, a careful selection of antibiotics is crucial. Since trends of bacterial resistance change over time, bacterial susceptibility has to be reviewed regularly, and this is particularly important in developing countries.15,16
Based on this study, the pattern of antimicrobial sensitivity differed in the different classes of antibiotics and the pathogens isolated from the culture. We noted that all gram-positive bacteria were sensitive to Linezolid, Vancomycin, Daptomycin, and Tigecycline, including methicillin-resistant staphylococcus aureus. These were followed by Clindamycin, Gentamicin, and Cefoxitin, which showed 80.6%, 66.7%, and 63.9% sensitivity, respectively. In our study, Ceftazidime showed high resistance rates to gram-negative isolates contrary to the finding of Abdul Gafor et al, and this could be due to the widespread use of ceftazidime in our center as empirical therapy.15
Due to the occurrence of MRSA isolates in our study, we recommend Vancomycin as empirical therapy as recommended by the guidelines of Infectious Diseases Society of America (IDSA).7 Interestingly, oxacillin showed lower rates of sensitivity (41.2%) to staphylococcal isolates, contrary to the IDSA recommendation of its use to methicillin-sensitive staphylococcal species. We found that 29.6% of S. aureus were characterized as methicillin-resistant; this is nearly the occurrence of MRSA associated with hemodialysis catheter-related bacteremia reported by Elisabeth et al.5
As recommended by IDSA, empirical coverage of gram-negative bacilli is usually based on the local antimicrobial susceptibility data and the severity of the disease.7 Our current study shows the sensitivity of all gram-negative bacteria to Imipenem, except Acinetobacter baumannii. Tigecycline showed sensitivity to all gram-negative bacteria, while Amikacin had low resistance rates. The high multidrug resistance rate of Acinetobacter baumannii in hemodialysis catheter culture was also reported by Sahli et al.17
Before this study, the empirical antibiotics for HD CRBSIs in our Hospital were intravenous Ceftazidime and Vancomycin, but after this study, we noted that most of the gram-negative bacteria were resistant to Ceftazidime but sensitive to Imipenem and Amikacin. Thus, following these results, empirical antibiotics for HD CRBSIs in our center were switched to intravenous Imipenem and Vancomycin.
The limitation of this study is that it is a retrospective study that is conducted in a single-center, which limits its generalizability to other centers, although this is the largest hemodialysis center in Somalia at the time of this study. We also could not correlate catheter vascular insertion site and infection rates since there were no recorded data about the insertion sites.
Conclusion
Our study revealed that the staphylococcal bacteria are the most common organisms responsible for non-tunneled temporary hemodialysis catheter tip bacterial colonization. We highly recommend that each institution should have their own antibiogram in the management of HD CRBSIs. Based on our findings in this study, we also recommend intravenous Vancomycin and Imipenem as the empirical therapy in patients with suspected HD CRIs.
Data Sharing Statement
Datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Consent for publication was obtained from the patients. Ethical approval of this research was obtained from the research ethics committee of the Hospital with reference number MSTH-3784.
Acknowledgments
We acknowledge the technical assistance provided by our Hospital managers Aşir Eraslan and Ahmed Ibrahim Nageye.
Disclosure
The authors declare that they have no conflicts of interest regarding the publication of this article.
References
1. Vercaigne LM, Gosnell T, Gin A. A retrospective analysis of catheter-related infections in a hemodialysis population. Can J Hosp Pharm. 1999;52(2):77–82.
2. De Freitas LWC, Neto MM, Nascimento MMP, Figueiredo JF. Bacterial colonization in hemodialysis temporary dual lumen catheters: a prospective study. Ren Fail. 2008;30(1):31–35. doi:10.1080/08860220701741940
3. Nabi Z, Anwar S, Barhamein M, Al Mukdad H, El Nassri A. Renal data from the Arab world catheter related infection in hemodialysis patients. Saudi J Kidney Dis Transpl. 2009;20(6):1091–1095.
4. Ramanathan V, Riosa S, Al-Sharif AH, et al. Characteristics of biofilm on tunneled cuffed hemodialysis catheters in the presence and absence of clinical infection. Am J Kidney Dis. 2012;60(6):976–982. doi:10.1053/j.ajkd.2012.06.003
5. Aoki EE, Pizzolitto AC, Garcia LB, Pizzolitto EL. Staphylococcus aureus biofilms on central venous haemodialysis catheters. Braz J Microbiol. 2005;36(4):342–346. doi:10.1590/S1517-83822005000400007
6. Saxena AK, Panbotra BR. Haemodialysis catheter-related bloodstream infections: current treatment options and strategies for prevention. Swiss Med Wkly. 2005;135(9–10):127–138.
7. Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the infectious diseases society of America. Clin Infect Dis. 2009;49(1):1–45. doi:10.1086/599376
8. Wang K, Wang P, Liang X, Lu X, Liu Z. Epidemiology of haemodialysis catheter complications: a survey of 865 dialysis patients from 14 haemodialysis centres in Henan province in China. BMJ Open. 2015;5(11):e007136. doi:10.1136/bmjopen-2014-007136
9. Oliver MJ, Callery SM, Thorpe KE, Schwab SJ, Churchill DN. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: a prospective study. Kidney Int. 2000;58(6):2543–2545. doi:10.1046/j.1523-1755.2000.00439.x
10. Dopirak M, Hill CDD, Oleksiw M. Surveillance of HD associated primary blood stream infections. Infect Control Hosp Epidemiol. 2002;23:713–715. doi:10.1086/502000
11. Sathish JV, Pavan M. Characteristics of biofilms formed on non-tunneled hemodialysis catheters. Diálisis y Trasplante. 2014;35(2):47–51. doi:10.1016/j.dialis.2014.02.005
12. Blankestijn PJ. Treatment and prevention of catheter related infections in hemodialysis patients. Nephrol Dial Transpl. 2001;16:1975–1978. doi:10.1093/ndt/16.10.1975
13. Kairaitis LK, Gottlieb T. Outcome and complications of temporary haemodialysis catheters. Nephrol Dial Transplant. 1999;14(7):1710–1714. doi:10.1093/ndt/14.7.1710
14. Murray EC, Marek A, Thomson PC, Coia JE. Gram-negative bacteraemia in haemodialysis. Nephrol Dial Transplant. 2015;30(7):1202–1208. doi:10.1093/ndt/gfv205
15. Gafor AHA, Ping PC, Abidin AFZ, et al. Antibiogram for haemodialysis catheter-related bloodstream infections. Int J Nephrol. 2014;2014. doi:10.1155/2014/629459
16. Lacy MK, Klutman NE, Horvat RT, et al. “Antibiograms: new NCCLS guidelines, development, and clinical application. Hosp Pharm. 2004;39(6):542–553. doi:10.1177/001857870403900608
17. Sahli F, Feidjel R, Laalaoui R. Hemodialysis catheter-related infection: rates, risk factors and pathogens. J Infect Public Health. 2017;10(4):403–408. doi:10.1016/j.jiph.2016.06.008
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.