Back to Journals » Journal of Multidisciplinary Healthcare » Volume 11
Patients with heart failure and their partners with chronic illness: interdependence in multiple dimensions of time
Authors Nimmon L, Bates J, Kimel G, Lingard L
Received 21 July 2017
Accepted for publication 9 January 2018
Published 15 March 2018 Volume 2018:11 Pages 175—186
DOI https://doi.org/10.2147/JMDH.S146938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Laura Nimmon,1,2 Joanna Bates,1,3 Gil Kimel,4,5 Lorelei Lingard6
On behalf of the Heart Failure/Palliative Care Teamwork Research Group
1Centre for Health Education Scholarship, 2Department of Occupational Science and Occupational Therapy, 3Department of Family Practice, Faculty of Medicine, University of British Columbia, 4Palliative Care Program, St Paul’s Hospital, 5Department of Medicine, Division of Internal Medicine, University of British Columbia, Vancouver, BC, 6Centre for Education Research and Innovation, Department of Medicine, Schulich School of Medicine and Dentistry, Western University, London, ON, Canada
Background: Informal caregivers play a vital role in supporting patients with heart failure (HF). However, when both the HF patient and their long-term partner suffer from chronic illness, they may equally suffer from diminished quality of life and poor health outcomes. With the focus on this specific couple group as a dimension of the HF health care team, we explored this neglected component of supportive care.
Materials and methods: From a large-scale Canadian multisite study, we analyzed the interview data of 13 HF patient–partner couples (26 participants). The sample consisted of patients with advanced HF and their long-term, live-in partners who also suffer from chronic illness.
Results: The analysis highlighted the profound enmeshment of the couples. The couples’ interdependence was exemplified in the ways they synchronized their experience in shared dimensions of time and adapted their day-to-day routines to accommodate each other’s changing health status. Particularly significant was when both individuals were too ill to perform caregiving tasks, which resulted in the couples being in a highly fragile state.
Conclusion: We conclude that the salience of this couple group’s oscillating health needs and their severe vulnerabilities need to be appreciated when designing and delivering HF team-based care.
Keywords: teamwork, complex adaptive system, palliative care, caregivers, chronic disease, interdependence, dimensions of time
Introduction
Heart failure (HF) is a chronic incurable condition that affects ~600,000 Canadians and 23 million people worldwide.1,2 It is a leading cause of admission to hospital,3–5 and is a major public health concern in Canada and other developed countries whose aging populations have a higher prevalence of HF.4–6 Patients with HF have difficulty carrying out the activities of daily living, due to shortness of breath, extreme tiredness, pain, swelling, and loss of appetite,1,7,8 with symptoms worsening as patients approach death.5
Complex treatment and care for patients with HF is challenging and requires the patient, health professionals, and a range of informal nonprofessional caregivers to coordinate as a team.9 Even with this broad, supportive team system comprising professionals and nonprofessionals, living with HF poses complex demands for the patient, the partner, and the couple as a unit.8,10 Informal caregivers are known to influence HF patients’ health outcomes, self-care, and quality of life.11–18 The health of informal caregivers is itself influenced through their interactions with HF patients, as these caregivers experience burden, depression, isolation, stress, physical exhaustion, anxiety, and reduced quality of life.8,19–23 The burden on caregivers increases with the number of caregiving activities they engage in, which in turn is associated with increasingly poor HF patient prognosis and rehospitalization rates for the very patients being looked after.14–16 This robust research describes the complex interplay of HF patients’ health on informal caregivers’ health and vice versa, and instruments have been developed to measure HF patient caregiver burden.24,25 Although assessment tools have been created, there is little evidence for how HF patients and caregivers negotiate change in their health status.
The existing literature exploring the interaction of HF patients and their informal caregivers is broad, and as such is limited in describing the experiences of specific HF patient–informal caregiver populations. Of significance, very little is known about the experience of HF patients who live with a long-term partner who also suffers from a severe chronic illness. This lack of knowledge may lead to implicit assumptions about the partner of an HF patient and render their own relentless illness invisible. Understanding the fragility of these couples’ dynamics could lead to strengthening of the safety net around the HF patient, a safety net that could lead to positive patient outcomes if robust. Currently, HF patients are the sole focus of the majority of HF interventions, with little consideration for the HF patient’s partner.15,17,26
With the evidence that there is a complex interplay between HF patients’ health and the health of their caregivers, our aim was to explore how HF patients and their caregivers with chronic illness manage day-to-day tasks as they negotiate the phenomenon of change in their health status. Drawing on data from a larger qualitative study of HF care teams, we sought to nuance the current understanding of the HF patient population and their caregivers with chronic illness by investigating this high-risk subgroup. This couple group is particularly vulnerable, because they are at risk of having a sudden health crisis at the same time, which could result in emergency hospitalization for both individuals. With calls to integrate informal caregivers as meaningful members of the health care team,18,26 we need to understand in more detail who HF caregivers are and how the most vulnerable patient–caregiver dyads can best be supported. Bringing understanding to the everyday experience of HF patients and partners who experience chronic illness is particularly timely and urgent, given Canada and other developed countries’ aging populations and subsequent rising prevalence of HF.4–6 This concerning demographic trend is further magnified by the overall wish for elderly people to stay at home and maintain their independence for as long as possible.27,28 With the evidence from this study, we hope to respond to this challenge and incite innovative HF interventions that target the unique needs of HF patients and their partners with chronic illness.
Materials and methods
Research setting
The study presented here is drawn from a large-scale, multisite study of the knowledge, experiences, and needs of the HF team as a complex system seeking to integrate palliative care for patients with HF. The larger constructivist grounded theory study used a novel methodological approach that drew on HF patients’ perspectives of their team to build team sampling units.29 We identified as our recruitment sites five Canadian cities in three provinces (British Columbia, Ontario, and Nova Scotia) with differing health care organization for primary and secondary care and for the care of patients with HF. Using a combination of convenience and purposive sampling, patients with advanced HF — defined as New York Heart Association class III or IV — were recruited primarily from heart function clinics to participate in semistructured interviews. Clinical staff identified eligible patients and provided them with an information sheet about the study. Purposive sampling was used to capture a range of sexes, ages, socioeconomic status, social frailty, and severity of condition to understand how these characteristics influence the HF team’s attitudes toward actions regarding palliative care.29–31 A trained research assistant with no involvement in patients’ health care then followed up with eligible patients to answer any questions about the study and recruit them as participants. If patients were willing to participate, the assistant scheduled an interview at a location convenient for the patients, typically at the patient’s home.
Data were collected from 2012 to 2015, and the study was approved by research ethics boards at all five study sites. All participants provided informed consent in writing prior to being interviewed. Patients with HF identified 2–19 team members, including health professionals (eg, nurses, family physicians, cardiologists, dentists) and informal caregivers (eg, family, friends, drivers, housekeepers, spiritual advisors).32 With the patients’ written consent, their health-care team members were invited to participate in semistructured interviews that became part of team sampling units.33 A patient-identified team sampling unit included the patient and at least two team members to meet the criteria for inclusion in the study.
Most patients in the larger study identified at least one family or friend caregiver as being on their HF health care team.32 From the larger study’s findings, we concluded that a broadened conceptualization of the HF team – one that includes a range of informal caregivers – was necessary.32 Our findings suggested that a better understanding of each patient’s systems of informal “hidden carers”34 is required to engage these individuals more effectively in HF team-based care.32 Therefore, the foci for the study presented in this paper was informed by one main research question: How can knowledge of the everyday experience of HF patients with their partners who also suffer from chronic illness inform the practice and training of HF care teams?
Theoretical framework
The larger study was framed using complex adaptive system (CAS) theory to attend to the multifactorial, negotiated nature of teamwork in advanced HF care.33,35 Our findings from this research have described the various ways HF teams work together as a dynamically interacting system of care.33,35 When applied to the larger study, this theoretical lens highlighted the interdependence of parts in a whole and the nonlinear, unpredictable nature of human interactions and behaviors.29,36 HF care and health care in general have tended to be approached with a mechanistic mind-set, rendering parts knowable and stable.37,38 CAS theory broadens this understanding to encompass the HF team as an open system that cannot be mechanistically reduced to its parts; rather, the HF health care team consists of individual components that are entangled and dynamically interacting.39–42 Drawing on the CAS theory enables us to examine the emergent behavior and emphasizes how an HF patient’s engagement in activities like self-care is an interdependent, contextually mediated activity that evolves from a dynamic interplay of factors. Some of these factors can be the patient’s social network, support programs, elements of place, and access to financial resources.43,44
Data sample
Interviews
From the larger grounded theory study that focused on the nature of the HF health care team as a CAS, we were interested in exploring the experience of HF patients and informal caregivers as a functioning subsystem on the team. Preexisting interview data from patients with HF and the informal caregivers they cohabitated with (eg, intimate partner, son, daughter, grandchildren) were selected as the data set for analysis.
LN, a social scientist who conducted interviews in the homes of patients with HF and their partners in the British Columbia site, remarked on the vulnerability of couples when both the patients and their partners suffered from chronic illness. With HF affecting mostly older patients,5,6 LN then observed that patients in the preexisting interview data were predominantly aged 60–90 years and that many of their partners also suffered from chronic illness. Deciding to focus on the experiences of these couples, the final selection criteria for an in-depth analysis from the larger study data set included cohabitating intimate partners together >20 years and intimate partners with a chronic illness (eg, arthritis, cancer, chronic pain, cataracts, transverse myelitis, lumbar spinal stenosis). See Table 1 for a description of the range of illnesses experienced by HF patients and their partners.
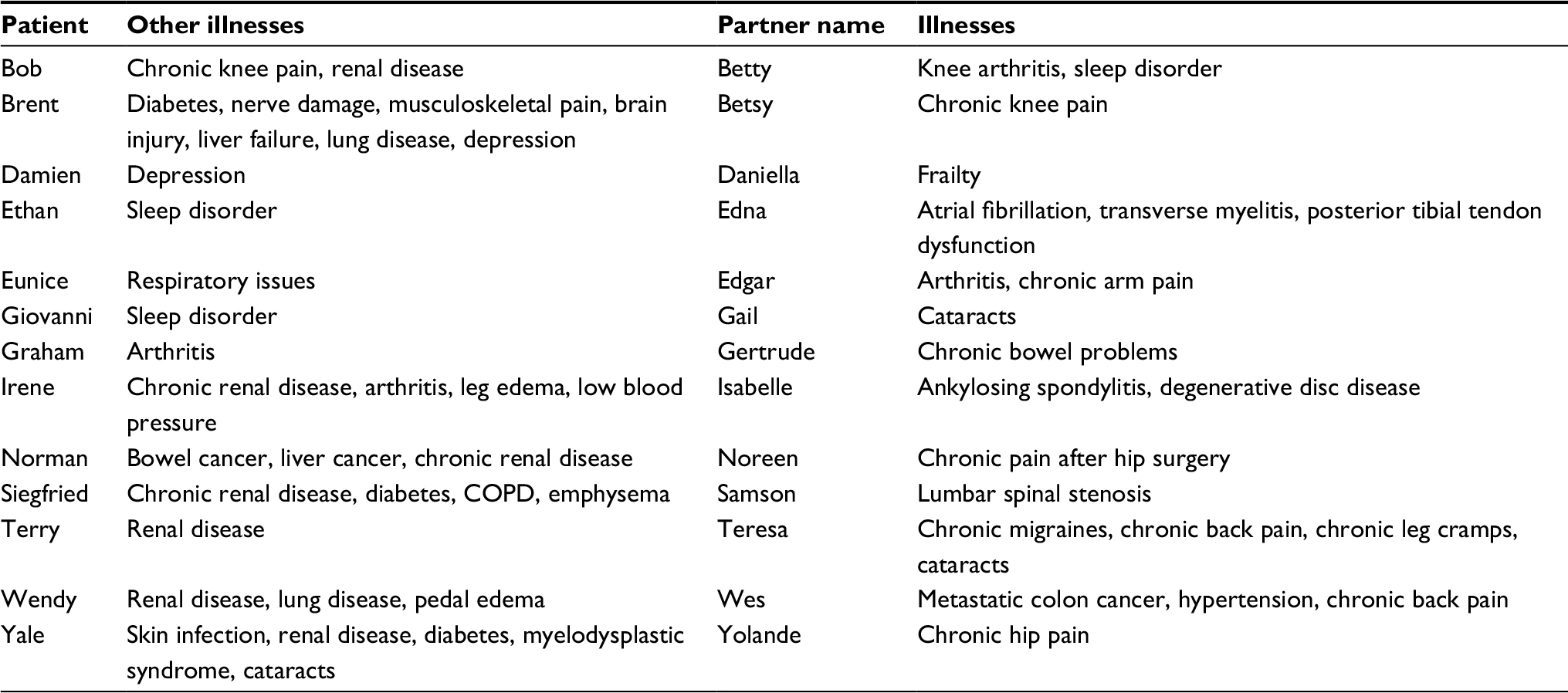 | Table 1 Illnesses of heart failure patients and their partners Note: All names are pseudonyms. |
In this paper, the term “partner” or “couple” is used synonymously to capture the sample, which included married heterosexual couples, common-law same-sex couples, and common-law heterosexual couples. Further, the selection of couples’ interviews did not privilege joint interviews, as each home interview unfolded differently: some couples wished to be interviewed in the room together; in other interviews, one individual would leave the room midway through to rest; still others chose to be interviewed without their partners in the room. Patients were asked to describe their experience of their health care over time, their day-to-day life and care routine, as well as their needs and goals and expectations for the future. They were also asked to describe the composition of their care team, the roles each member played, and how each member interacted with others in the team. Partner caregivers were asked about their perception of the patients’ health care over time, their own role as a team member, and the role of others. They were also asked about their hopes, goals, and priorities for the patients’ future care, as well as about their day-to-day experience managing as a couple.
Reflective field notes
Reflective field note data that documented contextual issues were also selected, which were collected by LN in the British Columbia site. LN took reflective field notes after every home visit, which included details and interpretations of the contextual setting (eg, pictures of children and grandchildren, fresh roses from a partner, order and cleanliness of the home), any behavior (eg, obvious signs of distress, pain, or fatigue; relational dynamics, such as gestures of affection between the couple or a partner who dominated the interaction), and any discussions that occurred off tape (eg, a partner describing how the patient with HF cries from his/her leg pain). This contextual information gave further insights into how the couple functioned day-to-day.
The first stage of sampling drew on interview and reflective field note data from seven patient–partner couples (14 participants) from the British Columbia site. During this preliminary stage of sampling, LN observed vulnerability (eg, physical frailty) and interdependence (eg, needing to help each other with daily tasks) in the data. LN then looked for similar patient–partner couples in the data from the Nova Scotia and Ontario sites, in order to reach an in-depth understanding of the phenomena of interest.31 This resulted in an additional six couples/12 participants (four couples from Ontario and two couples from Nova Scotia) who met inclusion criteria being added to the sample for analysis, for a total data set of 13 patient–partner couples (26 participants) from three provinces.
Data analysis
All data were organized and managed using NVivo10, a qualitative research software program. A three-stage qualitative analysis approach used in ethnographic research was employed, as this analytic tradition is designed to explore the dimensions of social context.45 This analytic approach was appropriate, as it enabled focusing on contextual patterns that exemplified the couples’ experiences in the individual interviews, in the reflective field notes, and across the patient–partner couple interviews. The couples’ experiences were thus analyzed as a primary unit of interest in three stages: item analysis, pattern analysis, and structural analysis.45 This three-layered inductive strategy involved compiling items together at a specific level, and then creating more conceptual statements about the patterns of relationships in the data to generate overall insights into the topic of interest.
As part of item analysis, LN first went through the data looking for any instances that may have revealed insights into the experiences of the HF patient–partner couples. Groups of similar items of interest became the primary codes for organizing the data.45 During the item analysis process, negative instances, ie, items that were unalike or items that contested the identification of a given item, were sought, in order to avoid making premature judgments about the meaning or identification of an item and accepting early or sometimes favorite interpretations.45 In total, ~70 codes were created. Some examples of these initial codes included “working/coordinating together”, “change in life organization”, and “time”.
During item analysis, LN observed that the temporality of existence permeated many of the original 70 codes. To understand better the various ways the couples appeared to inhabit and experience time, LN captured the permeating influence of various forms of temporality on the couples’ experience of chronic illness and its care. Distinct from the dominant decontextualized conception of bounded clock/machine time – time that is measured in discrete and consistent seconds, minutes, hours, and days – a social analysis of time interrogates local, idiosyncratic, and context-dependent ways of organizing and experiencing time.46 Rooted in the social and organic rhythms of everyday life, this lens emphasizes how people exist in complex multiple dimensions of time that frame human experience.46,47 Working recursively back and forth between the itemized data and Adam’s social analysis of time,46 LN identified that the couples had a complex experience of time outside the prevailing paradigm of linear clock/machine time. Building on this pattern, a process of comparison, contrast, and integration was used to organize and associate items and to identify higher order patterns. This analytical process revealed that many of the initial nontime codes (eg, working/coordinating together) were related to social time. These nontime codes were merged into four broader social time categories, in order to reflect this relationship.
Midway through this stage of analysis, LN met individually with the other members of the analytic team who brought specific expertise to this work: JB (family physician), GK (cardiologist/palliative care specialist), and LL (social scientist). In these meetings, each team member provided feedback about the pattern analysis and integration of a social time perspective, in order to refine the understandings of emerging patterns and concepts. These analytic meetings were recorded in LN’s analytic memos, which included evolving hypotheses and thoughts about the data-analysis process, including interpretations, insights, and questions about the data. As LN pieced together the analytic patterns, an overall structure was created.45 Following pattern analysis, broader themes were developed that involved blending many of the initial codes and higher order patterns into finer-tuned themes that captured similar conceptual dimensions across the data. These fine-tuned themes were generated by LN from Adam’s46 theoretical notions of time: “institutional time”, “biographical time”, “suspended time”, and “relational time”. These themes were then pulled together into a meaningful and coherent interpretation of the data: a story of how the couple assign prominence to their day-to-day experience in a unified way within the temporality of existence. During this final stage of data analysis, LN engaged in peer examination by debriefing the insights with the other three authors to deepen the reflexive analytical process and enhance research credibility.48
Results
In the following sections, we describe the four dominant dimensions of time that the couples appeared to coexist within: institutional time, biographical time, suspended time, and relational time. We also consider how these HF patients–partners are enmeshed and interdependent in each of these time dimensions. For ease of readability, each dimension of time is described sequentially, beginning with the simplest time dimension, institutional time, and ending with the most complex time dimension, relational time. All participants are assigned a pseudonym to maintain confidentiality.
Institutional time
Participants received care primarily outside the home. In some cases, when health care providers deemed participants too unwell to travel, providers made house calls. Regardless of the setting for care, as the couples structured their days around each other’s health care appointments, they described living in a shared temporal dimension of institutional time. This dimension of time appeared to be a collective experience of time driven by interactions with health systems and institutions. For example, the couples described how their day-to-day existence was entangled within institutionally driven appointment waiting times and test results, and institutionally paced interactions with health care providers. One patient with HF, Brent, expressed how waiting times for appointments were institutionally decided and frequently dictated his and his wife’s day-to-day life: “Yeah, there’s that wait time [to see specialists]. Got a wait time now to bring in your [his] equipment. It’s going to be quite a wait”. By contrast, others experienced institutional time in a more enabling way, describing a sense of ease due to the promptness and accommodation of certain health care providers. For example, Gertrude, the partner of Giovanni (HF patient), was pleased that she and Giovanni did not have to wait for his appointments: “The appointments are always good, like if you’re supposed to be there at 9:00, they see you at 9:00. You might wait 5 minutes, but that’s it: you don’t sit for hours.” The dimension of institutional time that the couples lived in was also documented in their material context, as lists of their appointment times were posted on the fridge, noted on loose paper throughout the house, or written in calendars on the wall. Institutional time shaped the couples’ day-to-day experience in restrictive or empowering ways, and was thus a nuanced and idiosyncratic shared time dimension.
Biographical time
The couples also appeared to live in biographical time as they narrated their life history together. This dimension of time appeared to be how time experienced in the present is interwoven with a series of memories and experiences from the past. For example, the couple explained how significant events of the past – marriage, birth of children, and major life decisions – shaped their experience of the present. One partner of an HF patient, Teresa, recalled how a hard life of partying and substance abuse was radically altered when the couple attended a church service and suddenly decided to take a more spiritual direction:
When Terry [HF Patient] and I first got married, we had a rough life. We had a hard life and we used to drink and smoke and all that stuff, but we didn’t know any better . . . we gave our life to the Lord . . . it has had a profound impact on our life, our health.
Biographical time and shared memories that interweave into the present shaped the couples’ actions and behavior. This theme was reinforced in the field notes, which detailed the numerous artifacts (eg, wedding pictures), trinkets (eg, souvenirs from travel together), and other memorabilia (eg, shared books on spirituality) dispersed throughout the couples’ homes that were interwoven into the fabric of their relational meaning-making system. These shared multifaceted memories coalesced with their sense of identity as a couple, including existential dimensions of their experience, such as the deeper meaning they brought to constructions of life, health, illness, and death. For example, Teresa (wife) and Terry (HF patient), whose life history and choices led them to embrace spirituality, described how their long-term relationship with God allowed them peacefully to accept the prospect of Terry’s inevitable death together in a unified way. The biographical time dimension interwove with other temporal dimensions of experience to bring a holistic understanding of the ways the couple coped day-to-day and engaged in making sense.
Suspended time
Participants seemed to have an understanding of the prognosis of HF: “You look at life a little differently, because you don’t know how you’re going to go, but you don’t know when and that’s all right … I’m not afraid to die. I have no qualms about that” (Norman, HF patient). As one or both partners approached death, the couple described living interdependently in suspended time. Time had an existential dimension for the couples as they configured their experience within a proximity to death. The couples’ very existence appeared to be situated in suspended time: an experience of time living within an indefinite future, driven by an unknown but recognized pending prospect of death. Participants explained how they lived together in the now, without much planning for the future, given the erratic and oscillating nature of HF: “Well, we will just take it as it comes. Don’t know what is going to happen, so we really can’t make plans” (Terry, HF patient). As one or both partners lived with a severe life-limiting illness, the couple appeared to relate to time in an unquantifiable way. Together, they surrendered to the possibility of finality, choosing to live moment to moment: “We take every day as it comes, and try to make the most of our time” (Gail, partner of HF patient Giovanni). Reflective field notes corroborated this finding. In particular, LN described one home visit in the British Columbia site where a couple purposefully put out of sight a Do Not Resuscitate form provided by an HF patient’s cardiologist. It was documented in the reflective field notes how the couple described that they would prefer to live in a shared temporal space where they could focus on being together in the present.
Relational time
A final, more complex, dimension of shared time was observed in relational time. As both patients with HF and their partners managed complex chronic illnesses together at home, they organized their day-to-day activity in an adaptive way over time. Their day-to-day activity was never static or predictable: rather, they described their activities as negotiated and coordinated daily. For example, when both individuals were feeling well and able, the division of tasks was described as being organized in a fairly stable way: “Usually, I help her [wife] clean. I vacuum for her and clean the sinks and toilets. She does everything else in the house” (Ethan, HF patient); or “I mostly do the cooking, but my wife always helps me and tries to do the most she can, and she does” (Giovanni, HF patient). However, these set activities were often destabilized as the health of one partner deteriorated. Participants thus adapted day-to-day activities based on each other’s level of physical function, such as moving, breathing, and digesting. Further, as one partner’s health deteriorated, the other partner responded by taking on the majority of caregiving activities (eg, preparing and providing medications, lifting, bathing, driving, dressing, shopping, cooking, cleaning). The couples appeared to synchronize their activities in a cycle of dependence and interdependence that appeared to unfold in relational time:
We just basically take it one day at a time. We support each other. If I’m having a bad day, usually it works out when I’m having a bad day, she’s not, so we back each other up and keep getting each other through it. And we are honest with each other about how we’re feeling most of the time (Isabelle, partner of HF patient).
The couples who seemed to have a temporal synchronized system for managing everyday tasks were catapulted into a state of vulnerability when both individuals were too ill to perform such tasks. In these unpredictable circumstances, their flexible, adaptive system broke down, as described by Wes, the partner of HF patient Wendy:
My health has gone downhill relatively rapidly over the last year, including the back thing, and all the other stuff [cancer]. My ability to be a caregiver, as opposed to a supporter, has decreased . . . I can only do stuff in the kitchen that does not take too long . . . I’ve gone from being someone who could at least take care of themselves, without draining Wendy’s energy, to being dependent on her fairly chronically over the last . . . well, since, probably March. It’s close to 3 months now. It’s become the new normal.
In such scenarios, health care providers and other informal caregivers sometimes modified their provision of care to accommodate the vulnerable state of the couple. For instance, a daughter or son would step in and help with cooking or driving when their parents were not able to manage, or a family physician would make a house call when it was judged that both partners were in a highly vulnerable state.
However, in other instances, the couple never received the help they needed, which was particularly challenging:
If it was an ideal situation, I’d like the nursing care to come in four times a day and change Irene’s dressings, I’d like someone to come in and bathe her and help her get dressed in the morning, I would like . . . [sighing] . . . someone to come in once a week and clean my house, you know, if it was an ideal situation. You know, I could keep it up the rest of the week if I had all of the other stuff done for me, and you know, they just come in and do the big stuff once a week. If it was ideal, and it isn’t. And I don’t see it ever getting back to that. I mean, I know there used to be a time when you got what you needed and you just don’t anymore (Isabella, partner of HF patient Irene).
When both partners were able to share tasks or one partner was able to care for the other, their coping system appeared to function. In these situations, they coordinated and adapted to accommodate each other’s health status in a dimension of relational time. A critical aspect of this finding was that when both partners were too fragile to support each other, team members played an important role in terms of how, when, and if they adjusted care to care for the couple. When no support was provided, the couple was particularly vulnerable or in crisis, as their temporal–relational system for coping deteriorated.
Discussion
The analysis highlighted how the couples co-constructed meaning with regard to their experience of life and death in dimensions of institutional time, biographical time, suspended time, and relational time. The way the couples synchronize their experience in multiple dimensions of time brings an in-depth appreciation of the HF patient’s context by highlighting the profound enmeshment of these couples as they comanage chronic illness and live day-to-day.
These insights illuminate the unique and complex challenges faced by these couples as they comanage chronic illness together at home. In particular, the salience of these couples’ interdependence challenges current assumptions about HF partner caregivers. Informal caregiving plays an important role for patients with HF and is considered a significant contextual factor influencing a patient with HF’s self-care.17 However, built into the narrative of the support HF caregivers provide is an implicit assumption that — while caregivers experience some negative health outcomes related to caregiving — they do not suffer from their own debilitating illness. It was significant how the HF patients, who are typically the focus of the HF team,44 sometimes shifted the roles to become caregivers to their partners. The changing of caregiver roles was illustrated by Wes, who suffered from cancer and went from being a caregiver to his wife, Wendy (HF patient), to being “chronically” dependent on her as his cancer progressed.
Attention must be paid to the acute vulnerability of the couple when the partner becomes dependent on the HF patient for caregiving. The results further alert us to the crisis situation that can occur when neither partner can perform self-care or caregiving activities, as they are surviving on a thin line. To reduce the impact on the HF patient and his/her partner, sustained support must be adaptive to this couple’s needs and responsive to what is happening at any given moment in time. In other words, providers need to be aware of what is going on with this group of HF patient–partner couples, being particularly attentive to when the couple is frail, and then intervening with appropriate support and resources.
Living together in multiple dimensions of time
This subset of HF patients–partners described day-to-day life as a unified “we” situated within shared dimensions of time, which needs to be appreciated in future HF program and care delivery initiatives. Employing social time theory brings valuable insights in to the experience of patients with HF and their partners with a chronic illness, as it highlights the way these couples co-construct time, meaning, health, life, and death together. The couples did not appear to experience day-to-day life through binaries of “self” and “other”, or even “patient” and “partner”, but framed their existence in dimensions of time in a unified, interdependent way. In fact, their collective nature was noted in analytic notes describing that the couples unified their experience in discursive ways, which was evident in how they used the plural pronoun “we” throughout their interviews. The critical findings add to the recent call for HF training and care delivery initiatives to account for informal caregivers as part of the team,18,26,49 by illuminating the symbiotic nature of this specific couple groups’ partnership.
Integrating a social analysis of time enhanced the explanatory power of the analysis, as this lens appreciates the nature of time as it is experienced in social interactions, structures, practices, artifacts, the mind and body, and the environment.46 Employing a social time conceptual tool, we were able to frame how the couples described living together in time, which seemed to be experienced as temporal, multifaceted, and nonlinear.46,47 This is a valuable insight, given that end-of-life (EOL) conversations tend to focus on advanced directive paperwork and choices for resuscitation.50–52 We suspect that the nature of the team sampling-unit data collection method29 offered new insights into how the couples oriented themselves together in multiple dimensions of time. The way the couples coexist and embody shared time dimensions builds on findings from metasynthesis of qualitative literature on patients’ perception of time in palliative care.53 This metasynthesis of research similarly revealed how terminally ill patients move toward perceptions of time that are less clock-based and more internalized and embodied as they make sense of living with a terminal illness.53 This resonates also with literature that describes how individuals relate to time in new ways when they are chronically ill, a phenomenon that links to the ways they create meaning of their illness and experience self.54
Our analysis, however, suggests that not only the individual with HF but the couple actually move toward living in multiple dimensions of time, including living in a suspended, embodied time with an emphasis on the present. The way the couples situated themselves in multiple dimensions of time without projection to the future may have implications for the foci of EOL conversations. This insight challenges assumptions that we should singularly frame all EOL conversations to be future-based.55 It also brings a layer of insight to the finding that some HF patients do not wish to have EOL conversations, which has been attributed to a lack of information about the severity of the disease or the patient’s fears of losing of hope.56,57 The participants in this study were aware of the prognosis of HF and appeared to have accepted the trajectory toward death. The couples’ preference to situate their experience in a time dimension that is concentrated on the now, despite their acknowledgment of the severity of HF, is intriguing. Future research could build on these findings and explore in more depth these couples’ preferences for EOL conversations.
A complex adaptive system
CAS theory assisted with understanding how the couples coexisted in shared time dimensions as a unified subsystem within a broader CAS of care. Our previous findings suggested that informal caregivers may function in adaptive ways that are responsive to patients’ needs.33 CAS theory is compatible with Adam’s46 multidimensional theory of time that recognizes nonlinearity and complexity. In particular, CAS theory helps us understand further the way the couples were adaptive to each other, particularly in how they negotiated day-to-day routines in relational time. This theory emphasizes that a change in a CAS often occurs unpredictably through the process of self-organization in which local interactions between agents affect the broader system, often in unintended ways.58 Further, these local patterns of interaction and self-organization in shared caregiving tasks between the couples sometimes precipitated the emergent adaptive behavior on the team. This emergence was most evident when both partners were too ill to self-care or take on the role of caregiver. Certainly, this adaptive behavior is not always a given. Nonetheless, in many situations, some members of the team (health professionals and informal caregivers) were responsive to the severity of couples’ situations.
Responsiveness to the couple was demonstrated in adaptive behaviors from team members. An instance was a community home-care coordinator organizing a spiritual counselor to visit the home of a distressed couple following prognosis of end-stage disease. Another example was a neighbor stopping by frequently to help the couple with day-to-day tasks, such as lifting one of the partners into a vehicle for him/her to make appointments. Such occasions are salient examples of how microlevel interactions between HF patient and his/her partner can influence team dynamics in a cyclic way, affecting the behavior of the health care team and producing unpredictable consequences.
Alternatively, a powerful example of non-adaptive care was illustrated in the team sampling unit of a patient with HF who lost his partner during the course of the study. Although his family physician was aware of his emotional vulnerability, the patient received only minimal and temporary psychological support. Overwhelmed with grief and turning to alcohol as a coping mechanism, the patient was readmitted to the hospital regularly as he lapsed into a state of being unable to manage his HF. The health care system designed to focus only on the patient with HF was non-adaptive to the patient’s domestic circumstance, resulting in serious health consequences for the patient and subsequently overburdening the health care system.
The insights that a CAS lens affords are akin to a shifting-perspective model of chronic illness, where living with chronic illness is understood as an ongoing and continually shifting process within which perspectives about the disease are nonlinear and predictable.59 The importance of focusing on the state and illness perspectives of the couple also resonates with the current discussion in the HF literature that suggests how relevant and effective coordination of care should consider adapting care to the couple as a family unit.60,61 A CAS lens has been a suggested framework to use when designing HF programs.33,43,44 Our findings support the value of placing a CAS lens on HF programming and delivery initiatives, as this lens attends to contextual dimensions and incites readiness to reorganize care when unpredictable disturbances in couples’ health occur.
Implications
The majority of chronic illness care is enacted by informal caregivers in the confines of the home, away from the supervision or support of health professionals.27,28,44,62,63 When both partners who live together at home suffer from chronic illness, diminished quality of life and poor health outcomes may result. Useful tools exist that initiate EOL conversations among seriously ill patients, partners, and health care providers.64,65 However, careful attention to these couples’ changing needs through the development of specific screening tools is recommended. Screening tools that provide information about the state of the couple will minimize waiting for a crisis that may lead to acute hospitalizations, medical interventions, and couple separation. Health professionals should also regularly ask HF patients and their partners how they are coping day-to-day, and be prepared to intervene with appropriate support when necessary. In addition, future research should explore HF patient outcomes — specifically quality of life — as a function of spousal health.
This study builds on the broader HF literature that underscores the importance of a family-centered approach for educating and supporting patients with HF and their partner.60,61 Policy-makers and practitioners must include family caregivers as members of the health care team to improve HF patients’ outcomes.18,26,32,49 Partners play a significant role in the day-to-day care of HF patients and in supporting HF patients’ self-care. However, they have historically been excluded from the majority of HF interventions.15,17,26,66 In addition, HF patients and their partners have reported that health professionals do not spend enough time with them or address their concerns adequately.21 Undervaluing patients’ and/or their partners’ knowledge and opinions about care is a hegemonic practice that represents top-down institutional power.67 Health care professionals should coordinate appropriate physiological and psychosocial care for the couple as their needs change, in order best to support this high-risk couple group.
Limitations
The data were collected from the larger study using a constructivist grounded theory approach.35 To answer our research question, however, we used an analytic approach for analyzing data that derived from ethnography, which is epistemologically commensurable with grounded theory. These two methodological traditions are compatible in that they share the same constant comparative technique and inductive process for analyzing data. We strategically employed the three-stage analytic process derived from ethnography to greater foreground issues of context.45
This sample is not fully representative of all HF patient–partner couples, as both individuals lived with a chronic illness and were in a loving and supportive relationship sustained for at least 20 years. Future work could include other selection criteria – eg, together <20 years, in an unsupportive relationship, partners who are both ill and do not live together, earlier stage of HF – to enhance our understanding of the contextual significance of specific types of couples and the implications for HF team-based care delivery. Although life partners were of particular interest to us, we are aware that patients with HF interact with a diversity of informal caregivers, such as drivers, friends, neighbors, and spiritual advisors.32 More research into particular subsets of the HF patient–informal caregiver population is required to find patterns of generalizability across contexts. For example, future research could explore if other HF couple groups live in similar or divergent dimensions of time found in this study.
Our decision to use CAS and a social theory of time to frame the interpretation draws our attention to certain aspects of the dimensions of the couples’ relationship and forgoes others. Other conceptual tools and other research approaches may generate more insights we did not capture with respect to the nature of this specific HF patient–partner relationship. For example, more time in the field could build trust with the participants and illuminate in more depth the mental health challenges of these couples. We also recognize that joint interviews may emphasize insights into couples’ world of shared experience and meaning.68 Given that each interview setting was idiosyncratic, it reinforces, rather than minimizes, how the couples held a deeply intimate shared meaning-making system.
Conclusion
There has been a recent call for research to examine in more depth the influence of contextual factors, such as the presence and influence of caregivers, on HF patients’ self-care.44 The scenario of HF patients living with their partners with chronic illness is a critical dimension of context that requires attention when designing HF team-based disease management and home-care support programs. Our findings suggest that policy-makers and practitioners must design integrated health and social services that are responsive to these couples’ needs, as their health and coping system oscillates unpredictably. The vulnerability of patients with HF and their partners as they manage chronic illness at home is paramount. Health professional education initiatives could train novices to be perceptually aware of each patient with HF as an individual inextricably linked to their unique familial system. However, the health care system will remain ill equipped to incorporate these approaches if the influence of context (physical, social, financial factors) in HF intervention research, clinical recommendations, and guidelines continue primarily to attend to the individual, dismissing contextual factors.44 Our results demonstrate how important the context of coupledom is for HF team-based education and delivery. We hope this work contributes to a departure from the commonly used personalized framework in HF care,44 which focuses on the individual HF patient and implies separation.
Acknowledgments
The authors would like to acknowledge the patients, family members, and health professionals who shared their experiences with them. The authors received peer-reviewed funding to support this research from the Canadian Institutes of Health Research and the Academic Medical Organization of Southwestern Ontario. The authors acknowledge the support from the Heart Failure/Palliative Care Teamwork Research group: Malcolm Arnold, Fred Burge, Samuel Burnett, Sheri Burns, Karen Harkness, Kori LaDonna, Donna Lowery, Denise Marshall, Allan McDougall, Robert McKelvie, Joshua Shadd, Stuart Smith, Valerie Schulz, Patricia Strachan, Glendon Tait, and Donna Ward. The authors acknowledge some coding assistance from Wendy Hartford and a final proofreading of this paper from Dr Letitia Henville.
Disclosure
The authors report no conflicts of interest in this work.
References
Heart and Stroke Foundation of Canada. Heart failure. Available from: https://www.heartandstroke.ca/heart/conditions/heart-failure. Accessed July 19, 2017. | ||
Dunlay SM, Roger VL. Understanding the epidemic of heart failure: past, present, and future. Curr Heart Fail Rep. 2014;11(4):404–415. | ||
Yeung DF, Boom NK, Guo H, Lee DS, Schultz SE, Tu JV. Trends in the incidence and outcomes of heart failure in Ontario, Canada: 1997 to 2007. CMAJ. 2012;184(14):E765–E773. | ||
Hayes SM, Peloquin S, Howlett JG, et al. A qualitative study of the current state of heart failure community care in Canada: what can we learn for the future? BMC Health Serv Res. 2015;15:290. | ||
Levenson JW, McCarthy EP, Lynn J, Davis RB, Phillips RS. The last six months of life for patients with congestive heart failure. J Am Geriatr Soc. 2000;48(Suppl 1):S101–S109. | ||
Stewart S, MacIntyre K, Capewell S, McMurray JJV. Heart failure and the aging population: an increasing burden in the 21st century? Heart. 2003;89(1):49–53. | ||
Howlett J, Morrin L, Fortin M, et al. End-of-life planning in heart failure: it should be the end of the beginning. Can J Cardiol. 2010;26(3):135–141. | ||
Pattenden JF, Roberts H, Lewin RJ. Living with heart failure; patient and carer perspectives. Eur J Cardiovasc Nurs. 2007;6(4):273–279. | ||
Dracup K. It takes a village: interprofessional collaboration in cardiology. J Card Fail. 2017;23(7):570–573. | ||
Luttik ML, Jaarsma T, Veeger N, Tijssen J, Sanderman R, Veldhuisen DJ. Caregiver burden in partners of heart failure patients: limited influence of disease severity. Eur J Heart Fail. 2007;9(6–7):695–701. | ||
Zhang KM, Dindoff K, Arnold JM, Lane J, Swartzman LC. What matters to patients with heart failure? The influence of non-health-related goals on patient adherence to self-care management. Patient Educ Couns. 2015;98(8):927–934. | ||
Heo S, Lennie TA, Moser DK, Kennedy RL. Types of social support and their relationships to physical and depressive symptoms and health-related quality of life in patients with heart failure. Heart Lung. 2014;43(4):299–305. | ||
Kang X, Li Z, Nolan MT. Informal caregivers’ experiences of caring for patients with chronic heart failure: systematic review and metasynthesis of qualitative studies. J Cardiovasc Nurs. 2011;26(5):386–394. | ||
Hooley PJ, Butler G, Howlett JG. The relationship of quality of life, depression, and caregiver burden in outpatients with congestive heart failure. Congest Heart Fail. 2005;11(6):303–310. | ||
Molloy GJ, Johnston DW, Witham MD. Family caregiving and congestive heart failure: review and analysis. Eur J Heart Fail. 2005;7(4):592–603. | ||
Schwarz KA, Elman CS. Identification of factors predictive of hospital readmissions for patients with heart failure. Heart Lung. 2003;32(2):88–99. | ||
Clark AM, Reid ME, Morrison CE, et al. The complex nature of informal care in home-based heart failure management. J Adv Nurs. 2008;61(4):373–383. | ||
Clark AM, Spaling M, Harkness K, et al. Determinants of effective heart failure self-care: a systematic review of patients’ and caregivers’ perceptions. Heart. 2014;100(9):716–721. | ||
Strömberg A, Luttik ML. Burden of caring: risks and consequences imposed on caregivers of those living and dying with advanced heart failure. Curr Opin Support Palliat Care. 2015;9(1):26–30. | ||
Kaholokula JK, Saito E, Mau M, Latimer R, Seto TB. Pacific Islanders’ perspectives on heart failure management. Patient Educ Couns. 2008:70(2):281–291. | ||
Aldred H, Gott M, Gariballa S. Advanced heart failure: impact on older patients and informal carers. J Adv Nurs. 2005;49(2):116–124. | ||
Thorton N, Hopp FP. “So I just took over”: African American daughters’ caregiving for parents with heart failure. Fam Soc. 2011:92(2):211–217. | ||
Scott LD. The Effect of Inotropic Infusions on Health-Related Quality of Life for Heart Failure Patients and their Caregivers [doctoral thesis]. Ann Arbor, MI: University of Michigan; 1999. | ||
Nauser JA, Bakas T, Welch JL. A new instrument to measure quality of life of heart failure family caregivers. J Cardiovasc Nurs. 2011;26(1):53–64. | ||
Strömberg A, Bonner N, Grant L, et al. Psychometric validation of the Heart Failure Caregiver Questionnaire (HF-CQ). Patient. 2017;10(5):579–592. | ||
Harkness K, Spaling MA, Currie K, Strachan PH, Clark AM. A systematic review of patient heart failure self-care strategies. J Cardiovasc Nurs. 2015;30(2):121–135. | ||
Sinha M. Portrait of Caregivers. Ottawa, ON: Statistics Canada; 2012. | ||
Canadian Institute for Health Information. Supporting informal caregivers: the heart of home care. 2010. Available from: https://secure.cihi.ca/free_products/Caregiver_Distress_AIB_2010_EN.pdf. Accessed July 19, 2017. | ||
Lingard LA, McDougall A, Schulz V, et al. Understanding palliative care on the heart failure care team: an innovative research methodology. J Pain Symptom Manage. 2013;45(5):901–911. | ||
Luborsky MR, Rubinstein RL. Sampling in qualitative research: rationale, issues, and methods. Res Aging. 1995;17(1):89–113. | ||
Morse JM. Sampling in qualitative research. In: Lewis-Beck MS, Bryman A, Liao TF, editors. The Sage Encyclopedia of Social Science Research Methods. Thousand Oaks, CA: Sage; 2004:993–996. | ||
LaDonna K, Bates J, Tait G, McDougall A, Schulz V, Lingard L. “Who is on your health-care team?” Asking individuals with heart failure about care team membership and roles. Health Expect. 2016;20,(2):198–210. | ||
Tait GR, Bates J, LaDonna KA, et al. Adaptive practices in heart failure care teams: implications for patient-centered care in the context of complexity. J Multidiscip Healthc. 2015;8:365–376. | ||
Knowles S, Combs R, Kirk S, Griffiths M, Patel N, Sanders C. Hidden caring, hidden carers? Exploring the experience of carers for people with long-term conditions. Health Soc Care Community. 2015;24(2):203–213. | ||
Lingard L, Sue-Chue-Lam C, Tait GR, et al. Pulling together and pulling apart: influences of convergence and divergence on distributed healthcare teams. Adv Health Sci Educ Theory Pract. 2017;22(5):1085–1099. | ||
Rouse WB. Health care as a complex adaptive system: implications for design and management. Bridge (Kans City). 2008;38(1):17–25. | ||
Lanham HJ, McDaniel RR, Crabtree BF, et al. How improving practice relationships among clinicians and nonclinicians can improve quality in primary care. Jt Comm J Qual Patient Saf. 2009;35(9):457–466. | ||
Capra F. The Web of Life: A New Scientific Understanding of Living Systems. New York: Anchor Books; 1995. | ||
Eoyang GH, Berkas TH. Evaluating Performance in a Complex, Adaptive System. Westport, CT: Quorum Books; 1999. | ||
Marion R, Bacon J. Organizational extinction and complex systems. Emergence Complex Organ. 2000;1(4):71–96. | ||
Plesk P. Redesiging Health Care with Insights from the Science of Complex Adaptive Systems. Washington, DC: National Academy Press; 2001. | ||
Waldrop MM. Complexity: The Emerging Science at the Edge of Order and Chaos. New York: Simon & Schuster; 1992. | ||
Clark AM. What are the components of complex interventions in healthcare? Theorizing approaches to parts, powers and the whole intervention. Soc Sci Med. 2013;93:185–193. | ||
Strachan PH, Currie K, Harkness K, Spaling M, Clark AM. Context matters in heart failure self-care: a qualitative systematic review. J Card Fail. 2014;20(6):448–455. | ||
LeCompte MD, Schensul JJ. Designing and Conducting Ethnographic Research. Walnut Creek, CA: AltaMira Press; 1999. | ||
Adam B. Timewatch: The Social Analysis of Time. Cambridge, MA: Polity Press; 1995. | ||
Heidegger M. Being and Time. Oxford: Blackwell; 1927. | ||
Lincoln YS, Guba EG. Naturalistic Inquiry. Vol. 75. Thousand Oaks, CA: Sage; 1985. | ||
Sebern M, Riegel B. Contributions of supportive relationships to heart failure self-care. Eur J Cardiovasc Nurs. 2009;8(2):97–104. | ||
Tierney WM, Dexter PR, Gramelspacher GP, Perkins AJ, Zhou XH, Wolinsky FD. The effect of discussions about advance directives on patients’ satisfaction with primary care. J Gen Intern Med. 2001;16(1):32–40. | ||
Golin, CE, Wenger NS, Liu H, et al. A prospective study of patient-physician communication about resuscitation. J Am Geriatr Soc. 2000;48(Suppl 1):S52–S60. | ||
Hofmann JC, Wenger NS, Davis RB, et al. Patient preferences for communication with physicians about end-of-life decisions. Ann Intern Med. 1997;127(1):1–12. | ||
Giuliani L, Piredda M, Ghilardi G, Marinis MG. Patients’ perception of time in palliative care: a metasynthesis of qualitative studies. J Hosp Palliat Nurs. 2015;17(5):413–426. | ||
Charmaz K. Good Days, Bad Days: The Self in Chronic Illness and Time. New Brunswick, NJ) Rutgers University Press; 1991. | ||
Low J, Pattenden J, Candy B, Beattie JM, Jones L. Palliative care in advanced heart failure: an international review of the perspectives of recipients and health professionals on care provision. J Card Fail. 2011;17(3):231–252. | ||
Barclay S, Momen N, Case-Upton S, Kuhn I, Smith E. End-of-life care conversations with heart failure patients: a systematic literature review and narrative synthesis. Br J Gen Pract. 2011;61(582):e49–e62. | ||
Ågård A, Hermerén G, Herlitz J. When is a patient with heart failure adequately informed? A study of patients’ knowledge of and attitudes toward medical information. Heart Lung. 2004;33(4):219–226. | ||
Kauffman S. At Home in the Universe: The Search for Laws of Self-Organization and Complexity. New York: Oxford University Press; 1995. | ||
Paterson B. The shifting perspectives model of chronic illness. J Nurs Scholarsh. 2001;33(1):21–26. | ||
Dunbar SB, Clark PC, Quinn C, Gary RA, Kaslow NJ. Family influences on heart failure self-care and outcomes. J Cardiovasc Nurs. 2008;23(3):258–265. | ||
Agren S, Evangelista L, Strömberg A. Do patients with chronic heart failure experience caregiver burden? Eur J Cardiovasc Nurs. 2010;9(4):254–262. | ||
Evangelista LS, Schinnick MA. What do we know about adherence and self care? J Cardiovasc Nurs. 2008;23(3):250–257. | ||
Riegel B. Self-care of heart failure: what is the state of science? J Cardiovasc Nurs. 2008;23(3):187–189. | ||
Ariadne Labs. Serious illness care. Available from: https://www.ariadnelabs.org/areas-of-work/serious-illness-care/research. Accessed December 18, 2017. | ||
Government of British Columbia. Advance care planning. 2017. Available from: https://www2.gov.bc.ca/gov/content/family-social-supports/seniors/health-safety/advance-care-planning. Accessed December 18, 2017. | ||
Clark AM, Thompson DR. The future of management programmes for heart failure. Lancet. 2008:372(9641):784–786. | ||
Lindahl B, Lidén E, Lindblad BM. A meta-synthesis describing the relationships between patients, informal caregivers and health professionals in home-care settings. J Clin Nurs. 2011;20(3–4):454–463. | ||
Taylor B, de Vocht H. Interviewing separately or as couples? Considerations of authenticity of method. Qual Health Res. 2011;21(11):1576–1587. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.