Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Patients’ Experiences of a Stress-Management Programme in Primary Care
Authors Köpsén S ![]() , Sjöström R
, Sjöström R ![]()
Received 24 October 2019
Accepted for publication 13 January 2020
Published 21 February 2020 Volume 2020:13 Pages 207—216
DOI https://doi.org/10.2147/JMDH.S235930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sofia Köpsén, 1, 2 Rita Sjöström 2, 3
1Krokom Health Care Center, Region Jämtland Härjedalen, Krokom, Sweden; 2Department of Community Medicine and Rehabilitation, Umeå University, Umeå, Sweden; 3Unit of Research, Education and Development, Region Jämtland Härjedalen, Östersund, Sweden
Correspondence: Sofia Köpsén
Krokom Health Care Center, Genvägen 5, Krokom 834 31, Sweden
Tel +46 730-343099
Email [email protected]
Introduction: Stress and stress-related ill health have a multifactorial impact; both on physical and mental health. To better meet this category of patients a primary care unit started a stress-management programme using cognitive behavioural therapy and basic body awareness therapy.
Purpose: To describe participant´s experiences of a primary care stress-management programme using cognitive behavioural therapy and basic body awareness therapy.
Methods: In a qualitative study, a semi-structured interview guide was used in individual interviews with 9 people, all women aged 41– 57, working or on sick leave, who had enrolled in the stress-management programme. The material was analysed through qualitative content analysis.
Results: The analysis resulted in the theme “Process of change for a sustainable everyday living”. The participants described having gained awareness of the symptoms of their stress, knowledge and tools to manage their stress, ways to relax, awareness of their body, and the means to develop better habits and to change their behaviour. Fundamental in the material was the importance of participants’ identification with the others in the group.
Conclusion: The participants started a process of change with new knowledge and growth, but they encountered difficulties and obstacles. Behavioural change is a time-consuming process.
Keywords: basic body awareness therapy, burnout, cognitive behavioural therapy, exhaustion syndrome, stress rehabilitation, stress-related ill health
Introduction
Psychological ill health is the cause of a large proportion of sick leave in Swedish society, and stress is a leading cause of such illness.1,2 In Sweden, the National Board of Health and Welfare (NBHW) uses the diagnosis “exhaustion syndrome”,3 defined as the result of long-term stress (not necessarily work related), the diagnostic criteria include both physical and psychological symptoms such as pain, cognitive impairment, and sleep disorders.4
Stress and stress-related ill health5 have a multifactorial impact including increased risk of heart- and cardiovascular diseases.6,7 A Finnish study shows that people with stress-related illness are more likely than healthy control subjects to have physical disorders, which appear more often in women as musculoskeletal pain and in men as heart- and cardiovascular diseases.8 The relation of stress to musculoskeletal disorders is also shown in a study by Heiden et al9 which showed sensitization and, a lower pressure/pain -threshold in people with stress-related illness.
Many people with stress-related illness have depressive symptoms.3,4 The NBHW national guidelines10 recommend cognitive behavioural therapy (CBT) as first hand recommendation in treatment for depression and anxiety, and CBT is also a common feature of rehabilitation for stress-related ill health.11,12 The NBHW guidelines also recommends physical activity and basic body awareness therapy as add on treatment, this with a lower priority. BBAT is a method based on Tai Chi and Qigong used by physiotherapists in Scandinavia.13
A study among teaching professionals combining CBT with alternative treatments like Qigong and acupressure showed more positive effects than CBT only, including improvements in physical responses such as handgrip strength and resting heart rate, which are associated with better psychosomatic health.14
A randomized control trial compared treatment as usual, (eg medication or psychotherapy), with combined treatment including BBAT in the rehabilitation of patients in open care psychiatry (including mood disorder, somatoform disorder or personality disorder and complaining about bodily symptoms).15 The group receiving combined treatment showed improved awareness of and attitude towards the body, better sleep, and improved physical coping mechanisms. Long-term follow-up showed lasting effects and less use of healthcare in the group receiving the combined treatment.16 Qualitative studies have shown that BBAT has positive effects not only on body awareness, but also on parameters like social participation and initiative in rehabilitation in psychiatric care with diagnosis including major depression and schizophrenia.17–19
A group of researchers in Umeå, Sweden, has compared the effects of CBT in combination with Qigong and Qigong only in the treatment of exhaustion syndrome.11,20,21 After the 1-year programme, improvements were seen in both groups with no significant difference.11 At the 3-year follow-up in the combined group, however, levels of burnout and use of medications for depression were reduced, and the use of cognitive tools was increased.21 In an interview study, with a sample of the participants, the authors concluded that affirmation and support from health professionals and fellow participants was very important in achieving behavioural change.20
Another type of intervention known as “green rehabilitation”, including therapeutic gardening and visits to forest environments has shown to be beneficial and to facilitate enjoyable activities, which also contribute to occupational balance.22,23 This in a population of clients with stress-related disorders or ill health.
A Cochrane- review from 201524 evaluated if current research could prove any treatment, for preventing occupational stress in health care workers, to be superior. They found low evidence that CBT, physical or mental relaxation, or organisational changes such as different scheduling had effect on perceived stress, but the literature provides no consensus on treatment structure, thus further research is required.
The purpose of the present study was to explore participants’ experiences of a stress-management programme provided through primary care.
Method
Study Design
To fit the purpose of the study, we chose a qualitative method to explore the participants’ experience.25 The material was analysed using qualitative content analysis as described by Graneheim and Lundman.26,27
Stress-Management Programme
In 2016, to better meet the needs of ever more patients with stress-related ill health, a stress-management intervention was initiated in a primary care unit in northern Sweden. The intervention was a collaboration between the physiotherapy unit and the psychological treatment unit at the primary healthcare centre. Inclusion criteria targeted people who had contacted the primary healthcare centre with stress-related ill health or lifestyle issues related to stress. There was no selection for specific diagnoses. The intervention included lectures and homework on CBT (to teach how to identify, understand and handle physical and psychological signs of stress by involving the patient, creating change and maintaining new behavior)28 by staff from the psychological treatment unit (1 h) and BBAT (a method based on Tai Chi and Qigong aiming to increase bodily and mental balance and the ability to be mentally present)13 led by a physiotherapist (1 h). The group met once a week for 10 weeks and the participants were then invited for an individual follow up appointment at the psychological treatment unit 3 months after the programme ended.
Participants
All enrolees (17) in the primary care stress-management programme held in the spring of 2017 were invited by mail to participate in the study. None-responders were followed-up and invited by telephone. To capture as many experiences as possible, all enrolees were invited regardless of how many sessions they had attended. Nine of those invited (all women) agreed to participate in the study. Those who chose to participate did not necessarily have the highest attendance (range = 2–10 sessions; median = 6). The participants were 41 to 57 years old (median = 45), 5 were classified as blue-collar workers and 4 as white-collar. Blue-collar work includes practical work such as nursing and white-collar work is more administrative, such as work in an office. Five of the participants had been on sick leave previously but had returned to work before the programme started (one participant to part-time rather than full-time work), two participants were on sick leave when the programme started but had returned to work at the time of the interview, one participant had not been on sick leave, and one participant had been on sick leave during the programme and still was at the time of the interview.
All participants signed written informed consent before entry into the study. The study was approved by the Regional Ethical Committee in Umeå, Sweden (2017/279-31).
Data Collection
Data were collected through individual interviews using a semi-structured interview guide, with open-ended questions that asked participants to “describe, tell, share” or similar (Appendix). Kvale recommends 5–25, which is consistent with the nine participants in this study, and emphasizes the importance of beginning with an overview of the material before beginning the analysis.29 To test the interview guide, we conducted a pilot interview. No adjustments were made to the guide as a result of this test, so to include as many experiences as possible, the pilot interview was included in the study. All interviews were conducted face-to-face by author S.K., who was familiar with the programme’s organization and content but had not been an active caregiver. The interviews were conducted at the healthcare centre chosen by the participant and lasted from 30 to 60 mins. There was no time restriction and participants were asked at the end whether they had anything to add. The interviews were recorded digitally (Olympus VN-541-PC), transcribed verbatim, de-identified and analysed. The interviewer made short notes after each interview. Data were collected from November 2017 to January 2018, 6 to 9 months after the last group meeting.
Data Analysis
The material was analysed using the qualitative content analysis described by Graneheim and Lundman.26,27 It emphasizes variation thru describing and identifying similarities and differences in the material. The analysis started with repeated readings of the material to get a sense of its entirety and content. Meaning units were identified and condensed to shorten their content, while preserving their core meanings, and then abstracted to codes to capture their essence. The codes were then grouped into categories and sub-categories by their commonalities. Further abstraction resulted a theme that exposes the latent content in the material. The authors coded the material separately, compared their results, then discussed the differences until consensus was reached. Categories and sub-categories were discussed, then adjusted and developed separately, and the final versions were settled through discussion until consensus (Table 1).
 |
Table 1 Example of Analysis; from Meaning Unit to Category |
Results
The analysis revealed six categories, ten sub-categories, and one theme (Table 2).
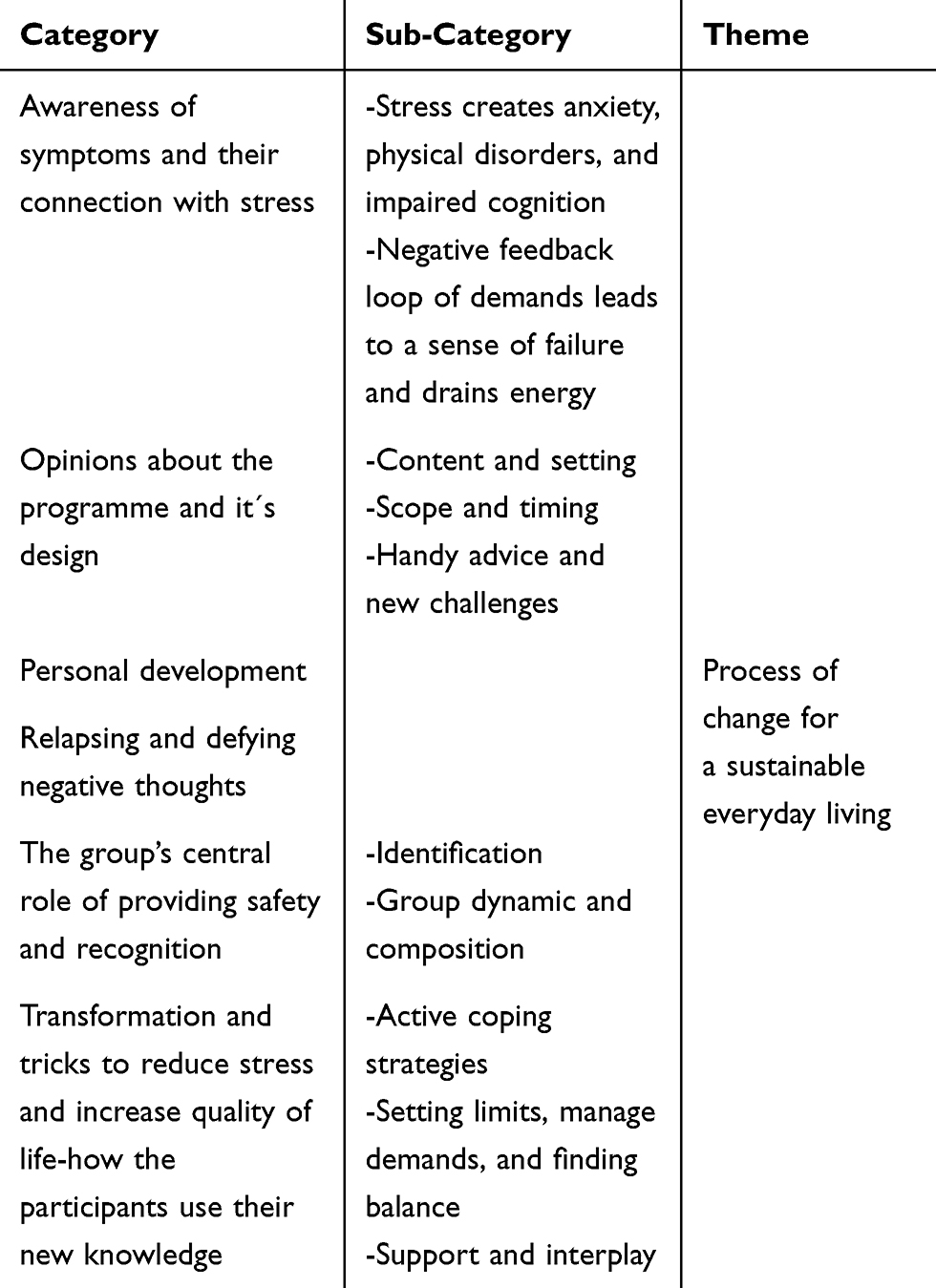 |
Table 2 The Result of the Analysis; Categories, Sub-Categories, and Theme |
From the categories and sub-categories, the theme “Process of change for a sustainable everyday living” was abstracted. The theme originates from the participants’ experiences of increased awareness of their symptoms, how stress has affected their lives in different ways, and their new knowledge and tools for managing or avoiding stress. The results are outlined below with illustrative quotes marked with the participant’s number.
Awareness of Symptoms and Their Connection to Stress
The participants described different warning signs and consequences of stress, some of extent of which continued to varying degrees after the programme had ended. Many talked about their increased awareness and understanding of these symptoms. This knowledge was helpful, but it could also temporarily trigger stress and worsen the illness as participants realized how much the stress had affected them.
Stress Creates Anxiety, Physical Disorders, and Impaired Cognition
The informants talked about physical symptoms like vertigo, palpitation, and pain. The initial symptoms were often interpreted as physical illnesses unrelated to stress. Despite their new awareness of the stress-related cause of these symptoms, participants could remain concerned about having a physical disease. Sleep disturbance was described as a major problem both in the early stage of the illness and as a residual problem. Some had trouble falling asleep, and others slept through large parts of the day without feeling thoroughly rested. Other symptoms were cognitive dysfunction; such as reduced memory, which could affect their rehabilitation.
At first, I didn’t understand that I was stressed, but sought help thinking I had some strange disease, Alzheimer’s or something. #2
Negative Feedback Loop of Demands Leads to a Sense of Failure and Drains Energy
The participants discussed feeling pressured by high performance demands, both professional and private, and a great sense of responsibility. The impression of too many demands and requirements runs through the interviews and is connected to feelings of shame, participants felt ashamed of not being able to cope with all the tasks they or others expect them, and this shame contributed to their not speaking up or getting help earlier.
The way society seems, you should work, you should handle everything, and when you don’t, it was a huge failure in my world. #6
Reduced capacity for initiative and feeling a lack or drainage of energy came at a later stage in the illness but remained at the time of interviews. Participants described how quickly their energy ran out, and they said that they no longer had the capacities they had before.
Opinions About the Programme and It´s Design
There were different opinions about the arrangement and design of the programme and, which parts were more rewarding or easier to grasp. The follow-up, for example, was felt to be unnecessary.
Content and Setting
The content was described as a palette where you sample different techniques, which in turn raised different thoughts and insights. Some found the practical exercises easier and others found the theoretical parts more rewarding. The content was described as informative and interesting, but also as too theoretical and lacking in individual focus. The staff’s dedication and reception affected the atmosphere and participants’ experiences of the meetings. It was important to create a safe atmosphere in the group, making it comfortable for everyone to share their thoughts and experiences. Some participants, however, did not feel that the safe atmosphere had been achieved.
Scope and Timing
Scope and timing were discussed in all interviews. Suggestions for changes ranged from offering the programme on a full-time basis, several times a week, or over a longer period to providing a “light” -version of the intervention, with fewer sessions. The importance of early, preferably preventative, intervention was mentioned frequently. Many participants felt the 3-month follow-up session was unnecessary or too time-consuming, while for others, the follow-up was barely noticeable amongst ongoing meetings with their therapist. Some suggested a group follow-up, rather than individual sessions.
Handy Advice and New Challenges
The two parts of the programme were described as a positive combination. Difficulties understanding and using BBAT were mentioned; some participants found it difficult to shift their attention from the mind to the body, others said that BBAT did not take effect very quickly, and opinions varied about whether more theory would make BBAT more helpful. Participants did, however, describe BBAT as a tool in their daily stress management, and they frequently reported having used BBAT in everyday life and described how it gave them both energy and focus.
…. this simple exercise to ground yourself, or that rotation, or when waiting in line somewhere, or at work, or anywhere, to be able to ground [myself] and feel that relaxation. #1
Participants responded positively to CBT lectures and conversations and picked up on different parts of it. Some felt it was easier to grasp than BBAT, although others found it more difficult to implement in their daily life and behaviour. All participants said that the meetings provided useful advice. Discussions about CBT techniques for sleep management were experienced as very central and important.
Personal Development
The informants mentioned different ways in which they had evolved and changed during and after the programme, especially their increased awareness about their own behaviours. The programme provided knowledge that could be difficult to handle, since it made them aware, for example, of how stress could harm their bodies and affect their relationships. Learning to be more present in the moment and in what they were doing right now was described as something new. Many described how they had learned to prioritize themselves.
Now I’ ve got a totally different way of thinking …. that I’ m the most important, because then it will be good for the rest of the family as well. #8
Relapsing and Defying Negative Thoughts
All the participants talked about different difficulties with participating, changing their thoughts and habits, and avoiding relapse. In the interviews, participants frequently reported having difficulty making time for the meetings, this difficulty, however, provoked thoughts about how they prioritized their time and how that influenced their stress and daily living. They found it very challenging to leave work on time and prioritize this time for themselves.
We all were a bit goofy, thinking it was stressful finding the time, which is ridiculous thinking about it afterwards. It was for our own sake. #7
Another central motif in the interviews was how difficult they found it to maintain the changes they had made and avoid a relapse into old patterns. New routines were easily lost when everyday life sped up and the new routines and knowledge had not been fully incorporated. It was difficult for participants to maintain their new practice and continue with home assignments, new knowledge was therefore easily forgotten, not only because behavioural change is demanding, but also because their memory and cognition could have been affected by their stress.
The Group’s Central Role of Providing Safety and Recognition
The central role of the group itself in the programme featured largely in the interviews. All participants found it extremely important and fruitful to recognize themselves in the others, and to be able to share and listen in a group of people who had similar experiences.
Identification
Recognizing and identifying with the other participants was very important, since many otherwise felt alone in their situation and different to others. Hear about the others’ similar feelings and experiences confirmed their own. Not feeling involved in the group or having a sense of not fitting in affected participants’ whole experience.
Thinking it’s probably only me and I’m just strange. To be able to recognize yourself, that you are so alike. It’s so incredibly good to hear. These thoughts you have and the problems you get … they´re just the same. #5
Group Dynamic and Composition
Participants described the group dynamic in terms of the inclusive feeling in the group and how the conversations proceeded. They talked about the importance of good cohesion and respect in providing safety and a positive dynamic. Some, however, did not share this view and felt that neither the group nor the discussions were very inclusive. The participants all described that group members took up different amounts of space in the discussions, but that all had an opportunity to talk and be seen. The mix of ages and professions in the group was experienced as positive. Most of the people in the groups were women and the study participants would have liked to have more male participants to hear their ways of thinking and handling things. The participants felt that they were in different stages of stress and problems, and they found it very positive to be able to share their different experiences. The number of participants in the programme had varied from session to session, but this was not seen as negative in fact, some thought it was positive, since if there were always a few people miss, the group would never be too big.
Transformation and Tricks to Reduce Stress and Increase Quality of Life – How the Participants Use Their New Knowledge
The participants gave different examples of how they were currently acting to reduce and prevent stress in everyday life, including finding different enjoyable activities for recovery, adopting preventive strategies, and planning how to avoid stress. They also talked about the importance of having support.
Active Coping Strategies
Active coping strategies to prevent or manage stress was a recurrent topic in the interviews, strategies included physical activity, outdoor life, and breathing exercises. Listening to and being more present in one’s own body was another positive change that contributed to better health, since the participants were used to living in their head and focusing on ruminative and repetitive thoughts that increased their stress. Another strategy was improving communications and conflict management, which helped them save energy and prevent stress. Their new knowledge of tools and strategies they could use by themselves was considered a measure of safety.
I wrote a note saying this day I’m going to do that and that day I’m going to do this so that each day I had some recovery. #1
Setting Limits, Managing Demands, and Finding Balance
Setting limits, for example, making an active choice about which assignments and responsibilities to undertake, was an important aspect of finding a balance between commitment and recovery. This requires the ability to say no and to prioritize rest when in need of recovery. “More brake and less gas” were a helpful thought for some participants, however, it remained difficult for participants to take opportunities for rest and recovery without feeling stressed and uncomfortable.
Support and Interplay
Pervasive in the interviews was the importance of having the support of family, friends, and colleagues. Participants talked about daring to communicate about their health and mood with their boss and colleagues. Support from healthcare, rehabilitation services, and insurance was another factor in gaining successful results.
I showed my family (the home-assignments) …. Then they also got some insight into things. #3
Discussion
The theme is based on the participants’ experiences becoming aware of the symptoms induced by their stress, gaining knowledge and tools to manage their stress, finding opportunities to relax, and starting to listen to their body. Those factors allowed them to develop and, to a greater or lesser extent, change their behaviour. During this process participant encountered various obstacles and occasional relapses, which illustrate the difficulties of making sustained behavioural changes: it is a process that takes time.
The participants talked about several difficulties and setbacks during and after the programme. The paradox of not having time for their own rehabilitation and, relapsing to old patterns and, knowing the tools to convert their habits into healthier behaviours, but feeling unable to use them, was frustrating and for a time added to their stress rather than relieving it. Difficulty prioritizing the time to go to the rehabilitation was a recurrent topic in the interviews. Linton and Flink28 describe a process of three steps in CBT, (1) involving the patient, (2) creating change, and (3) maintaining new behaviour. The informants’ experienced difficulties in all three steps, but mostly in the maintenance phase, which seems to be a difficult and crucial factor in the success of the intervention. These processes and difficulties are important to consider when planning and developing similar rehabilitation programmes to be effective. The stress-management programme we studied had individual follow-up sessions after 3 months intended to support participants’ in maintaining their new behaviours, but the participants did not find this rewarding. One reason for this could be that some had ongoing individual therapeutic contact and the follow-up became a part of that instead. An important factor in the implementation and maintenance of therapeutic change is home assignments. This was included in both the CBT and BBAT parts, but if home assignments are to be effective, continuity is key. The participants had different difficulties in managing this; for example, it was found difficult to take the initiative to practise at home, some could not find the time, for some it felt like yet another demand, and others did not understand why they should do it. Finding a balance between doing home assignments and not increasing feelings of demands and failure is difficult but essential.
The stress-management programme consisted of a combination treatment using both CBT and BBAT, which the informants felt was positive. Previous studies have shown the benefits of combined treatments including treatment as usual with the addition of BBAT;15,16 CBT with green rehabilitation;22 and CBT with another alternative treatment.14 Melamed et al6 define “burnout” in terms of three dimensions (physical fatigue, emotional exhaustion, and cognitive weariness), which must all be considered in rehabilitation. This strengthens the concept of effective combined treatment, which can be seen to address all those parts. Another factor in successful rehabilitation is timing (when it is initiated), and the interviewee’s in our study expressed opinions that early, and preferably preventive help is most desirable. Perski30 writes about the phases of exhaustion syndrome. In the first phase, the person is very sensitive to stress and, needs a great amount of sleep and care. In the second phase, the patient benefits from help in balancing their body and mind, for example, through participating in a stress-management group. The third phase should include vocational rehabilitation in cooperation with the workplace. These three phases can be helpful in planning a rehabilitative intervention. According to Perski,30 modern healthcare spends a vast amount of money on patients in phase one, who are unready and unable to gain from rehabilitation. Our study seems to support this idea, since participants whose interview placed them in the first phase, experienced the stress-management programme as yet another unmanageable set of demands and requirements or were unable to learn or use the rehabilitative tools because of cognitive impairment. Rather than considering phase one too early for intervention, however, it would be desirable to provide a preventive intervention before exhaustion syndrome begins to develop.
In the interviews, the participants described how they had developed and changed to feel better and manage life. They related the different strategies they used to avoid stressful situations and how they learned to handle stressful situations that occurred. In reviewing the results, we noticed that most participants had improved body awareness and were more likely listen to their body and rest when they needed to, instead of just going on. This concurs with previous research in patients treated with BBAT.17–19 Being present and focused on the body rather than the stressed head was a useful strategy for managing stress. Many also participated in outdoor activities, similar to green rehabilitation, which also has positive effects.22,23
An essential point in the participants’ stories was the importance of group cohesion and identification with the other participants. The group’s central role has been identified in previous studies as significant in successful rehabilitation.20 Affirmation and support have also been shown to be important factors in inducing behavioural change, as confirmed in this study.20 Although identification with other members was a central factor in the positive opinions about group treatment, patients with stress-related ill health are heterogeneous, with many different symptoms as the definition of exhaustion syndrome includes a complex mix of symptoms.4 This makes rehabilitation difficult to choose and plan. From the interviews, we believe that it may be necessary to provide both individual and group treatments to achieve the best result, providing both individual attention and peer support. Multiple professions may be required to treat all the different symptoms in multimodal form of rehabilitation. An important preliminary factor seems to be to address patients’ speculations about their various physical symptoms to relive their worries about serious disease, which could otherwise impair their rehabilitation. Patients who are focused on a possible disease have difficulty attending to and assimilating seemingly unrelated information such as lectures about how to handle stress. Health care has an important task to observe stress-related symptoms and it is a pedagogical challenge to attain consensus about its causes and connections. The participants reported several symptoms that they later understood were related to stress, but which had previously caused them a great deal of worry and speculation. Because stress is a risk factor for developing cardiovascular diseases,6,7 it is important to distinguish between stress-induced psychosomatic symptoms and early symptoms of purely physical disease before the stress is expressed in more serious morbidity.
Only women participated in this study, which reflects the majority in the group of patients who underwent the programme, but in future research it would also be interesting to study men’s experience and to investigate gender differences and/or similarities in responses to stress and stress-management techniques. Further studies are needed to investigate how often and for how long rehabilitation should continue to provide the most optimal chance of achieving and maintaining behavioural change.
The use of individual interviews is considered adequate for this type of study since participants may experience them as sensitive and intimate, and they may be more willing to discuss subject that might be difficult to share in a focus group, even with others from their own therapeutic group.25,29 The use of a semi-structured interview guide ensured the informants were asked identical questions. The questions were not distributed before the interview, so participants did not have a chance to prepare specifically, but knowing the purpose of the interview, they could prepare a general response or consider what they wanted to share. Not having access to the questions beforehand meant they had to give spontaneous answers, which are considered preferable to prepared answers.
Trustworthiness in qualitative research is evaluated in terms describing its validity and reliability; credibility, dependability, confirmability, and transferability.26,27 The authors conducted the first part of the analysis separately and then compared and discussed their initial impressions and suggestions until reaching consensus. To further strengthen credibility leaders of the programme read and commented on the codes, categories, and results to provide expert validation.31 The authors have strived to be objective. Lincoln and Guba31 write that an interview is co-created between the researcher and the interviewee. Furthermore, the process of selecting participants and the analysis are both thoroughly described in the Method and Results sections, the latter of which is supported by representative quotes. The ability of the reader to follow the process of analysis is important for trustworthiness and authenticity. Quotations from all informants clarified and confirmed the findings, which strengthens their authenticity. Transferability is accounted for through the description of the whole process, from recruiting the sample to completing and writing up the analysis, including the context. From this information the reader should be able to judge the study`s transferability.
The participants represented the full range of age and professions in the intervention group and corresponded with the groups mostly female composition. Participants were also in different phases of their rehabilitation, which provided a wide range of opinions and experiences. There was also variation in the number of sessions they had participated in, which contributes to a truer picture of the experience. Otherwise, it could be suspected that low attenders, who might be presumed to be discontented with the programme, would choose not to participate in this study, which could be interpreted as selection bias. A larger group of interviewees would have been needed to analyse differences between participation rates. These factors of the interview sample and the interview group strengthen the study’s credibility.
Conclusion
In the results, we found that the participants began a process of change during the stress-management programme, gained new knowledge and tools from both CBT and BBAT, which have enabled their personal development, but there were difficulties and obstacles along the way. Behavioural change is a time-consuming process. Furthermore, we found that it is important to start rehabilitation at the right time for the best effect. In general, and as found in previous studies, the combination of CBT and BBAT was a positive experience for the participants.
Implications for Rehabilitation
- Rehabilitation for stress-related ill health should target behavioural change, which is time consuming.
- Participants found the group dynamics and sense of identification with other group members essential to the success of the intervention.
- The timing of beginning rehabilitation is important for a successful intervention.
- Participants felt strengthened by acquiring new tools to manage their problems and situations actively.
Data Sharing Statement
The data used in this research was collected subject to the informed consent of the participants. Access to the data will only be granted in line with that consent, subject to approval by the project ethics board.
Acknowledgments
We gratefully acknowledge financial support of this study from the Unit of Research, Education and Development, Region Jämtland Härjedalen and Jämtland County Cancer and Care Fund.
The authors thank Krokom Health Care Centre, Sweden, especially Tomas Karlsson, Elisabeth Landegren-Eriksson and Monika Fredriksson for their support with making this study possible.
We express our gratitude to the informants who participated in this study.
Disclosure
The authors report no conflicts of interest.
References
1. Swedish Social Insurance Agency. [Internet] Korta analyser 2017:1. Lång väg tillbaka till arbete vid sjukskrivning. [Short analyzes 2017:1. Long way back to work from sick leave]. Stockholm: Försäkringskassan: 6. Available from: https://www.forsakringskassan.se/wps/wcm/connect/d57be02c-46dc-4079-b68d-760739441f11/korta-analyser-2017-1.pdf?MOD=AJPERES&CVID=.
2. Swedish Social Insurance Agency. [Internet] Sjukfrånvarons utveckling 2017, Socialförsäkringsrapport 2017:13. [Development of sick leave 2017, Social Insurance Report 2017:13]. Stockholm: Försäkringskassan: 88. Available from: https://www.forsakringskassan.se/wps/wcm/connect/1596d32b-7ff7-4811-8215-d90cb9c2f38d/socialforsakringsrapport-2017-13.pdf?MOD=AJPERES&CVID=.
3. National Board of Health and Welfare. [Internet] Diagnoskoder ICD-10. [International Statistical Classification of Diseases and Related Health Problems, Swedish version] Stockholm: Socialstyrelsen. [
4. National Board of Health and Welfare. [Internet] Utmattningssyndrom. Stressrelaterad psykisk ohälsa 2003 [Exhaustion syndrome. Stress-related psychological ill health 2003] Stockholm: Socialstyrelsen: 90. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2003-123-18.pdf.
5. Åsberg M, Grape T, Krakau I, et al. Stress som orsak till psykisk ohälsa. [Stress as the cause of mental illness]. Lakartidningen. 2010;19–20(107):1307–1310.
6. Melamed S, Kushnir T, Shirom A. Burnout and risk factors for cardiovascular diseases. Behav Med. 1992;18(2):53–60. doi:10.1080/08964289.1992.9935172
7. Melamed S, Shirom A, Toker S, Berliner S, Shapira I. Burnout and risk of cardiovascular disease: evidence, possible causal paths, and promising research directions. Psychol Bull. 2006;132(3):327–353. doi:10.1037/0033-2909.132.3.327
8. Honkonen T, Ahola K, Pertovaara M, et al. The association between burnout and physical illness in the general population—results from the Finnish Health 2000 Study. J Psychosom Re. 2006;61(1):59–66. doi:10.1016/j.jpsychores.2005.10.002
9. Heiden M, Barnekow-Bergkvist M, Nakata M, Lyskov E. Autonomic activity, pain, and perceived health in patients on sick leave due to stress-related illnesses. Integr Physiol Behav Sci. 2005;40(1):3–16. doi:10.1007/BF02734184
10. National Board of Health and Welfare. [Internet] Nationella riktlinjer för vård vid depression och ångestsyndrom 2017. [National guidelines for the care of depression and anxiety] Stockholm: Socialstyrelsen: 136. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2017-12-4.pdf.
11. Stenlund T, Ahlgren C, Lindahl B, et al. Cognitively oriented behavioral rehabilitation in combination with Qigong for patients on long-term sick leave because of burnout: REST a randomized clinical trial. J Behav Med. 2009;16(3):294–303. doi:10.1007/s12529-008-9011-7
12. Heiden M, Lyskov E, Nakata M, et al. Evaluation of cognitive behavioural training and physical activity for patients with stress-related illnesses: a randomized controlled study. J Rehabil Med. 2007;39(5):366–373. doi:10.2340/16501977-0053
13. Lundvik Gyllensten A, Skoglund K, Wulf I. Basal Kroppskännedom: Den Levda Kroppen. [Basic Body Awareness Therapy: The Living Body].
14. Au DW, Tsang HW, Lee JL, et al. Psychosomatic and physical responses to a multi-component stress management program among teaching professionals: a randomized study of cognitive behavioral intervention (CB) with complementary and alternative medicine (CAM) approach. Behav Res Ther. 2016;80:10–16. doi:10.1016/j.brat.2016.02.004
15. Gyllensten AL, Hansson L, Ekdahl C. Outcome of basic body awareness therapy. A randomized controlled study of patients in psychiatric outpatient care. Adv Physiother. 2003;5(4):179–190. doi:10.1080/14038109310012061
16. Gyllensten AL, Ekdahl C, Hansson L. Long-term effectiveness of basic body awareness therapy in psychiatric outpatient care. A randomized controlled study. Adv Physiother. 2009;11(1):2–12. doi:10.1080/14038190802242061
17. Danielsson L, Rosberg S. Opening toward life: experiences of basic body awareness therapy in persons with major depression. Int J Qual Stud Health Well-Being. 2015;10:27069. doi:10.3402/qhw.v10.27069
18. Hedlund L, Gyllensten AL. The experiences of basic body awareness therapy in patients with schizophrenia. J Bodyw Mov Ther. 2010;14(3):245–254. doi:10.1016/j.jbmt.2009.03.002
19. Johnsen RW, Råheim M. Feeling more in balance and grounded in one’s own body and life. Focus group interviews on experiences with basic body awareness therapy in psychiatric healthcare. Adv Physiother. 2010;12(3):166–174. doi:10.3109/14038196.2010.501383
20. Fjellman-Wiklund A, Stenlund T, Steinholtz K, Ahlgren C. Take charge: patients’ experiences during participation in a rehabilitation programme for burnout. J Rehabil Med. 2010;42(5):475–481. doi:10.2340/16501977-0534
21. Stenlund T, Nordin M, Jarvholm LS. Effects of rehabilitation programmes for patients on long-term sick leave for burnout: a 3-year follow-up of the REST study. J Rehabil Med. 2012;44(8):684–690. doi:10.2340/16501977-1003
22. Eriksson T, Karlstrom E, Jonsson H, Tham K. An exploratory study of the rehabilitation process of people with stress-related disorders. Scand J Occup Ther. 2010;17(1):29–39. doi:10.3109/11038120902956878
23. Eriksson T, Westerberg Y, Jonsson H. Experiences of women with stress-related ill health in a therapeutic gardening program. Can J Occup Ther. 2011;78(5):273–281. doi:10.2182/cjot.2011.78.5.2
24. Ruotsalainen JH, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev. 2015;4:Cd002892.
25. Bryman A. Social Research Methods. Oxford: Oxford University Press; 2016.
26. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
27. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
28. Linton SJ, Flink I 12 verktyg i KBT: från teori till färdighet. [12 tools in CBT: from theory to proficiency] Stockholm: Natur & kultur; 2011. Swedish.
29. Kvale S, Brinkmann S. InterViews: Learning the Craft of Qualitative Research Interviewing.
30. Perski A. Rehabilitering av stressjukdomar sker i olika faser och blir ofta lång. [Rehabilitation of stress diseases occurs in different phases and often become long]. Lakartidningen. 2004;14(101):1292–1294.
31. Lincoln YS, Guba EG. Naturalistic Inquiry. Beverly Hills, CA: Sage; 1985.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.