Back to Journals » Patient Preference and Adherence » Volume 17
Patients’ Expectations of Evidence-Based Service at the Pharmacy Regarding Information on Self-Care of the Feet for Persons with Diabetes at Risk of Developing Foot Ulcers – A Cross-Sectional Observational Study in Sweden
Authors Hellstrand Tang U ![]() , Scandurra I, Sundberg L, Annersten Gershater M, Zügner R
, Scandurra I, Sundberg L, Annersten Gershater M, Zügner R
Received 22 August 2023
Accepted for publication 6 December 2023
Published 27 December 2023 Volume 2023:17 Pages 3557—3576
DOI https://doi.org/10.2147/PPA.S435632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ulla Hellstrand Tang,1,2 Isabella Scandurra,3 Leif Sundberg,4 Magdalena Annersten Gershater,5 Roland Zügner2
1Department of Prosthetics and Orthotics, Sahlgrenska University Hospital, Gothenburg, Sweden; 2Department of Orthopaedics, Institute of Clinical Sciences, Sahlgrenska Academy,University of Gothenburg, Sahlgrenska University Hospital, Gothenburg, Sweden; 3Centre of Empirical Research in Information Systems, Örebro University, Örebro, Sweden; 4Gothenburg Diabetes Association, Gothenburg, Sweden; 5Department of Care Science, Faculty of Health and Society, Malmö University, Malmö, Sweden
Correspondence: Ulla Hellstrand Tang, Department of Prosthetics and Orthotics, Sahlgrenska University Hospital, Falkenbergsgatan 3, Gothenburg, SE-412 85, Sweden, Tel +46 70 6397913, Fax +46 31 40 81 62, Email [email protected]
Purpose: Self-care of the feet is one of the cornerstones in the prevention of diabetic foot ulcers (DFU). Often, individuals with diabetes seek help at the pharmacy, but it is still unclear whether the service meets their expectations and needs. The aims were to explore patients’ expectations of support from the pharmacy regarding self-care of their feet and explore how patients with diabetes felt that they managed the self-care of their feet.
Patients and Methods: The included participants (n = 17), aged 70 ± 9 years, answered surveys regarding their expectations of support from the pharmacy related to self-care of the feet and how they felt that they managed the self-care of their feet. By using software, MyFoot Diabetes, they assessed their risk of developing DFU (ranging from 1 = no risk to 4 = DFU). In addition, a healthcare professional assessed the risk grade.
Results: Sixteen patients had not received any information from the pharmacy regarding how to take care of their feet. Several suggestions for ways the pharmacy could help patients with diabetes to take care of their feet were registered. They included having the necessary skills and competence, giving advice regarding self-care, giving information regarding the products they market and have for sale and giving advice on ointments/creams. The participants gave several examples of how they self-managed their feet: by wearing shoes indoors and outdoors, wearing socks and compression stockings as often as possible, being physically active, inspecting their feet, being aware of the fact that their feet have no problems, washing, moisturising their feet, cutting their nails and finally seeking help to prevent DFU.
Conclusion: The participants thought that they should receive competent information from the personnel at the pharmacy to improve the self-care of their feet, eg, being given information about which ointments/creams to use.
Clinical Trial: NCT05692778.
Plain Language Summary: Persons living with diabetes have better opportunities to be physically active, keep on walking and participate in social activity if the feet are in good health. Besides getting support from healthcare, on how to promote good foot health, the pharmacies offer services and products aimed for self-care of the feet. Seventeen persons living with diabetes in the western region of Sweden answered a survey regarding their expectations of support from the pharmacy related to self-care of the feet and how they felt that they managed the self-care of their feet. The study found that persons living with diabetes self-managed their feet in different ways. The services being available from the pharmacies should be improved, promoting good foot health for persons living with diabetes, and in its prolongation prevent the development of diabetic foot ulcers.
Keywords: diabetic foot, prevention, diabetes type 1, diabetes type 2, self-care, self-management, self-monitoring
Introduction
Self-Care
Managing self-care of the foot and obtaining objective and evidence-based information on how to perform the self-care of your feet is one of the cornerstones in the prevention of diabetic foot ulcers (DFU).1 The definition of DFU originates from the International Working Group on the Diabetic Foot (IWGDF) with the expression “diabetes‐related foot disease” meaning a disease of the foot of a person with previously or currently diagnosed diabetes mellitus that includes, eg, peripheral artery disease, peripheral neuropathy, ulcer(s), infection, gangrene, neuro‐osteoarthropathy or amputation.2
The prevention of DFU is important for persons living with diabetes as it has great impact on persons’ quality of life, with limitations in physical capability and worries of further complications such as amputation in the lower extremities.3,4 DFU and amputations are costly for society, and prevention is found to be cost-effective.5,6 Prevention is recommended by the International Working Group on the Diabetic Foot (IWGDF), saying that all people that are diagnosed with diabetes should get an annual foot screening, being risk classified (1 = no risk to 4 = ongoing DFU). Moreover, in accordance with the foot screening, they should get intervention with podiatry and footwear, and they should also get information about self-care, which leads to increased opportunity for the patient to self-care and, in presence of DFU, to rapidly get referral to a specialist team.7,8
The risk of developing DFU is high; 19% to 34% of all persons living with diabetes are estimated to develop a foot ulcer. With a global rise in diabetes, from 537 million in 2021 to 783 million people in 2045,9 the high risk for DFUs prompts for actions according to the IWGDF.10
When strengthening patients’ ability to manage their self-care, their healthcare professionals (HCPs) need to know the patients’ foot status just as the patients need to know their own foot status.11 Are there any risk factors present? Specifically, what are the risk factors and how can these risk factors be limited in a way that promotes good foot health? The main risk factors that the patients’ HCPs need to identify are the presence of peripheral angiopathy and/or neuropathy, foot deformities, skin pathologies, DFUs and amputations and a history of previous DFUs/amputations.1,12 Neuropathy is one of the most important risk factors, being present in 50% or more of the population with symptoms such as sensory loss.5,13 Besides sensory loss, there is a diversity of symptoms, for instance, pain, dry skin and muscular insufficiency. These symptoms can preferably be assessed with a tool kit of measures, such as the 10g monofilament, the Ipswich Touch Test, the C128-Hz tuning fork and questions like “do you have a tingling sensation in your feet” or “do you feel numbness”.5,14,15
To let patients assess their performance of self-caring of their feet, by answering a questionnaire prior to their visit, is one way to improve the dialogue regarding self-care that HCPs and patients have in the care meeting.16 A valid and reliable questionnaire, presented by Navarro-Flores et al, is currently available in Spanish, Italian and Arabic.17,18 The results from the questionnaire form a basis for the dialogue and facilitate the communication, leading to guidance and custom-made advice about self-care. However, patients’ expectations regarding the service from the pharmacy are not included in the questionnaire originating from Navarro-Flores et al.
Pharmacy is an important meeting place for the exchange of information between a person with diabetes and the personnel working at the pharmacy. Recommended self-care includes the following actions: daily inspections of the feet; daily washing the feet, drying the skin especially between the toes; applying emollients to the feet; cutting the nails when needed; wearing the appropriate shoes and avoiding chemical agents to remove calluses.19 Although recommended, the expectations individuals living with diabetes have when it comes to support regarding the self-care of their feet, from the pharmacy, and how to self-care for their feet, are not clear. The optimisation of self-care is only possible if HCPs, including personnel at the pharmacy, are qualified to give objective, evidence-based and individualised advice relating to the self-care of the feet. The question of the role licensed pharmacists play in guiding individuals with diabetes in terms of the personalised self-care of their feet has been investigated by the Swedish Medical Products Agency.20 The report concluded that quality and security should be the focal points when giving objective, expert and individual advice on self-care to their customers.20 An improvement in education and training has been suggested. The strategy pharmacies will formulate to improve evidenced-based education is still unclear.
Licensed HCPs are responsible for assessing patients’ risk of developing DFU in an annual foot screening, as described by the IWGDF.7
In Sweden, patient education for individuals living with diabetes is mainly integrated into primary healthcare, where the patients have medical check-ups and individual counselling integrated with annual visits.21 According to the Swedish National Guidelines, education in groups might also be provided, in addition to individual counselling.21 However, Adolfsson et al concluded that improvements were needed in patient education in primary healthcare to facilitate the patients’ potential to realise their overall treatment targets for diabetes.22 One challenge regarding self-care is how to reach people with insufficient health literacy, as they run a higher risk of developing DFUs.5,23
The prevention and care of DFU involve multiple licensed HCPs (registered nurses, doctors, podiatrists, physiotherapists, certified prosthetists and orthotists) and the advice on self-care should optimally be uniform, regardless of which HCP the patient meets, and should be a natural part of the annual check-up.1,24 However, a study by Stolt reported that there are very few options for HCPs to improve their competence and their pedagogic skills regarding how to give advice on self-care of the feet to individuals living with diabetes.25
For persons living with diabetes, several sources of information on self-care are available. In some countries, such as Scotland and Norway, uniform, simple advice on how to prevent DFU is available at national level.26,27 Advice on how to promote good foot health is frequently published by national diabetes organisations.28
Self-Care Supported by the Pharmacy
The pharmacies around the world are organised in various forms, governmental and private, with different professions.29 A professional pharmacy service has been described as an action organised by a pharmacy, delivered by a pharmacist with a patient/client, to optimise the process of care, with the aim of improving health outcomes and the value of healthcare.29
In Sweden, pharmacies are obliged by the Swedish Government to secure good, safe drug use, by 1) ensuring that the consumer obtains access as quickly as possible to prescribed medicines and goods, 2) providing expert and individually tailored information and advice and 3) informing about and exchanging medicines.30
Prior to 2009, the Swedish state was responsible for the service delivered by the professional pharmacies through Apoteksbolaget (National Corporation of Swedish Pharmacies, in English).31 Afterwards, several outpatient pharmacies were set up (n = 1448 in 2022) in Sweden.32 A considerable amount of money is spent on non-prescription drugs used in self-care. In 2021, the cost was SEK 4.2 billion, 8.4% of the total gross turnover of the Swedish pharmacy market.30
In addition to being experts on medication and drugs, the professionals give advice on self-care.33 It is up to the pharmacy organisations to improve the skills and ability to provide evidence-based information to all the staff working at pharmacies and perform the role of giving advice on self-care, as stated in the report from the Swedish Medical Products Agency.20 For a person living with diabetes, it is extremely important that the personnel at the pharmacy, who wear white coats, give evidence-based and objective information about goods sold at the pharmacy.
To our knowledge, there are as yet no national guidelines or indicators in Sweden evaluating the quality of how the pharmacies manage their guidance on self-care, and the management of self-care information has not been clarified.34 Future visions from the pharmacy organisations and new ways to support self-care and self-monitoring using eHealth systems will be introduced continuously and be made available at pharmacies. This will further support both individuals in need and an overloaded healthcare system.33,35
A specific support system, named Symtom Råd Åtgärd (Symptom Advice Action, in English), for personnel working at pharmacies to help them give advice on self-care, was previously available to pharmacies, prior to 2009.36 The support system was made up of questions and self-care advice. It included the questions to ask the customer at the pharmacy, in relation to the symptoms the customer described. Based on the answers, the pharmacist gave advice on when to seek care and decided when it was appropriate to give advice on self-care. For the last few decades, the nationally funded website, 1177.se, has been the site individuals in Sweden frequently visit to obtain advice on health and self-care and information about diseases and what healthcare unit to contact.36,37 However, on 1177, information on how to prevent DFU is sparse.
In addition to www.1177.se, pharmacists in Sweden have other sources of knowledge, including a) Läkemedelshandboken (The Drug Handbook, in English), b) product summaries and c) internally developed guidelines and recommendations.36,38
In some countries (Finland, Denmark, Norway, the United Kingdom and the USA), the pharmacies’ branch associations have developed recommendations and standards relating to self-care advice at the pharmacy.36 Some of the standards are simple, while others include quality indicators. A combination of information sources is often used, as in Sweden, and the vision for most pharmacies focuses on developing a patient-centred approach aimed at supporting customers in terms of self-care. It is unclear whether and how the pharmacies in Sweden manage to offer their customers a high-quality structured service supporting self-care.30
Healthcare, moving toward person-centred, equal and good health, needs to ensure that everyone with diabetes has their feet examined at least once a year. Based on the foot status and the person’s risk of developing DFU (1 = no risk to 4 = ongoing DFU), Figure 1, adequate prevention and self-care can be initiated. If an individual has any risk factors for developing DFU, the HCP should send referrals for podiatry to the Department of Prosthetics and Orthotics (DPO).1,7 At the DPO, based on their foot status, the patients are informed of what footwear to wear and, when needed, the patients are prescribed footwear and insoles.39 In the presence of foot ulcers, the patients are referred to a specialist clinic.7 All HCPs meeting a patient with diabetes with foot complications must assess foot status and the patient’s need for education in self-care including foot care.7 Although recommended, the process of providing individuals with diabetes with advice about self-care to promote good foot health is limited, due to organisational barriers between municipal, primary and secondary care.1
 |
Figure 1 Schedule of the risk stratification as described in Swedish national clinical guidelines.12 |
If a person’s feet are not examined, no information about foot self-care can be discussed between the person and the HCPs. According to the Swedish National Diabetes Register, May 2023, 23% of all adult registered patients with diabetes had not had their feet examined during the last 12 months.40 Moreover, a lack of HCPs and a lack of diabetes-related competence among HCPs contributes to individuals with diabetes not receiving personalised information on self-care of the feet.1,41 Optionally, written and verbal information on how to perform self-care activities to prevent the development of diabetic foot ulcers (DFU) should be customised to meet and fulfil the patient’s demands.19
Healthcare providers, overloaded by long waiting lists, have problems delivering care and advice on self-care of the highest quality to patients with diabetes, as reported by the Diabetes Association in Sweden, based on a survey of 3,500 respondents. One in four respondents experienced that diabetes care, overall, was of poorer quality in 2022 as compared with 2019.42 As a result of poorer quality being reported, 40% of the respondents that experienced poorer quality also perceived that, nowadays, it was difficult to manage self-care.
Self-Care Using mHealth
The rapid implementation of digital solutions has led to a rich selection of applications aimed at the self-monitoring of general health, eg, counting steps per day, checking p-glucose values, counting carbohydrates, measuring blood pressure and/or weight. Globally, the use and spread of mobile wireless technologies for public health (sometimes called mHealth) is recommended by the United Nations to promote equal, good health and “Ensure that no one is left behind” and “Ensure healthy lives and promote well-being at all ages”, which is the Sustainability Development Goal number three.43–45 However, there are few, if any, examples of eHealth tools that are implemented in clinical practice to facilitate communication between patients and HCPs, supporting a smooth care process to prevent the development of DFUs. Some mHealth tools do, however, exist in beta-versions. For example, in a meta-analysis of the use of mHealth and its effectiveness for patients with diabetes, Kitsiou et al showed that mHealth interventions improved glycaemic control by 0.3% on average for patients with type 1 diabetes and by 0.8% for patients with type 2 diabetes compared with standard care or other non-mHealth approaches.46 An intervention with remote self-monitoring blood-glucose tools and coaching was studied by Amante et al.47 The coaching was related to glucose monitoring, being active, healthy eating, taking medication, problem solving, reducing risks and health coping. In a cross-over study by Amante et al, patients (n = 119) with diabetes participated, and it was found that, regardless of being in the intervention group or the group that received standard care, both groups experienced improvements in satisfaction and lowered their blood glucose levels.47 Amante et al concluded that further studies of remote self-monitoring, including coaching and involving family and caregivers, were needed. Overall, there are very few mHealth devices designed to monitor the feet of individuals with diabetes, apart from MyFoot Diabetes, a self-monitoring tool, which is currently being programmed in the Swedish language.48,49 The MyFoot Diabetes software aims to facilitate self-care for persons living with diabetes by generating custom-made advice about self-care of the feet.48,49
With the plethora of pharmacies, with employees with diverse skills and competence, giving advice on self-care, the overarching aim of the present pilot study was to explore patients’ expectations of support from the pharmacy regarding self-care of the feet. The aims were to:
- explore patients’ expectations of support from the pharmacy regarding self-care of their feet, and
- explore how patients with diabetes felt that they managed the self-care of their feet.
Materials and Methods
Study Design and Setting
The study is a quantitative cohort study as part of a larger study in Region Västra Götaland (VGR) in Sweden. In the current study, patients’ expectations of support from the pharmacy regarding the self-care of their feet were explored. Data collection took place in five locations (Falköping, Lidköping, Karlsborg, Hjo and Skövde) located in VGR.
Participants
Patients with diabetes eligible for inclusion (n = 49): a) had, between 1/2/2021 and 30/5/2021, had their feet examined by HCPs (podiatrists or registered nurses) working in primary care in the five locations, b) were aged 18 years or more and c) were able to understand the Swedish language. The setting had been described by Andersson et al.50 The exclusion criterion was being unable to understand the Swedish language. Of 32 dropouts, 18 patients did not respond to the telephone call or letters designed to inform the eligible individuals about the study, Figure 2. Fourteen patients were prevented from attending the study due to sickness, sickness in the family or other reasons. The drop-out group consisted of 10 women and 22 men. Of the included participants, seven were women. The mean age of the included patients was 70 ± 9 years (range 55–83 years). The characteristics of the included patients are presented in Table 1.
 |
Figure 2 Flowchart of the participants in the study. |
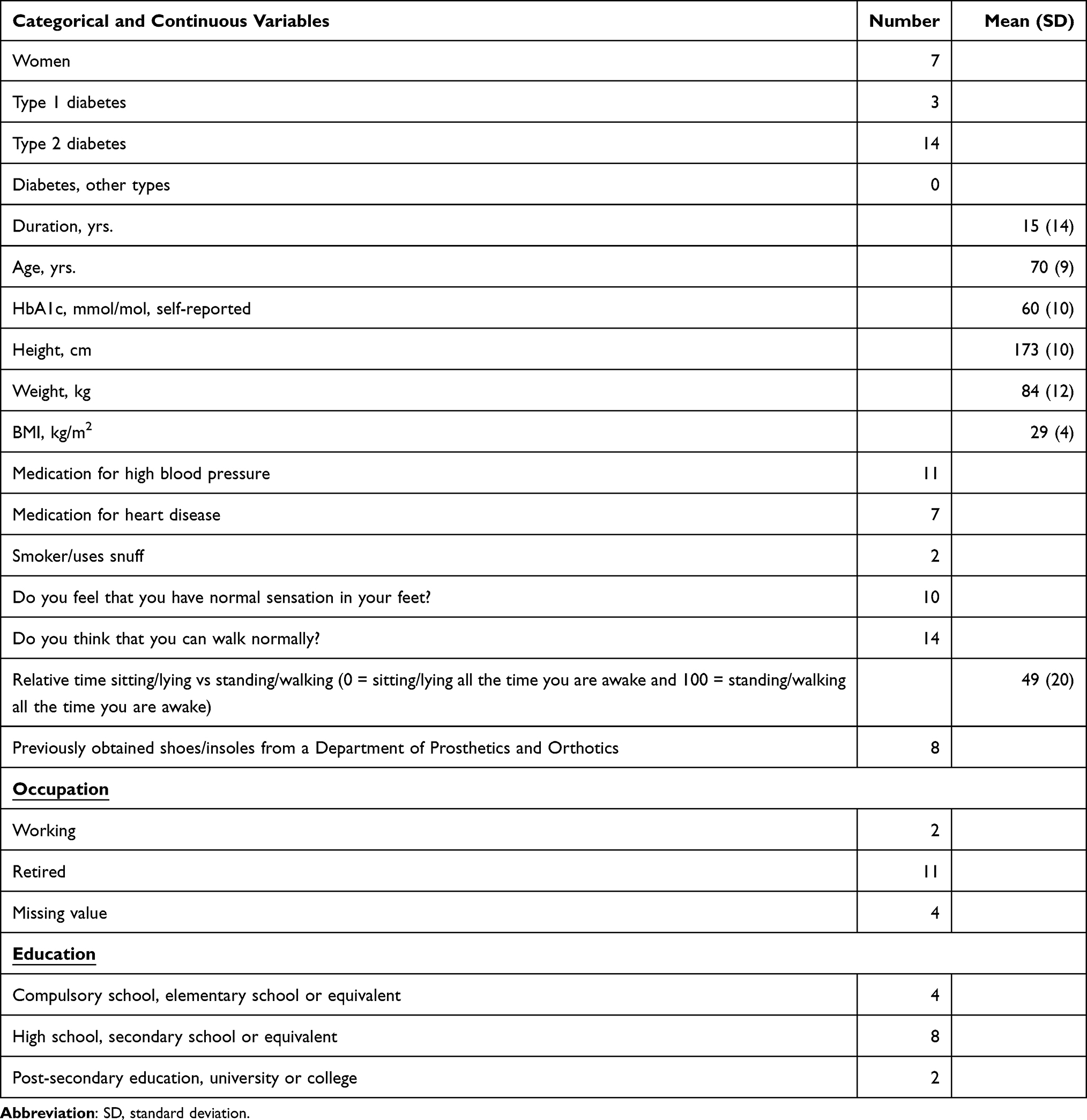 |
Table 1 The Characteristics of the Participants (n = 17) |
Procedure
Prior to recruitment to the current study, all the patients had had their feet examined on a regular visit to an HCP (nurse or podiatrist) in VGR during the last 12 months. During the healthcare visit, the HCP asked the patients if they agreed to be contacted by the principal investigator (UT) with an invitation to participate in the current pilot study.
Those that were interested in participating were then informed and invited to a meeting close to where they lived. The meetings took place in hotels in five locations in VGR, where the participants met the research team, between 1/8/2021 and 31/12/2021. At the study meeting lasting approximately two to three hours, the patients filled in ten surveys and, in the current study, three of the surveys were used, Table 2. The surveys were as follows: 1) MyFoot diabetes, a self-test of the feet programmed in software,51 2) the questionnaires included in the D-Foot software (Appendix 1)52,53 and 3) a paper questionnaire collecting answers on the participants’ foot status, pain in their feet, physical functions related to being able to perform self-care of their feet, how the participants managed the self-care of their feet and if the participants had any, and in that case what, expectations in terms of support from the pharmacy regarding self-managing their feet (Appendix 2). In addition to filling in the surveys, the participants’ feet were examined by an HCP following the procedure in the D-Foot.52,53
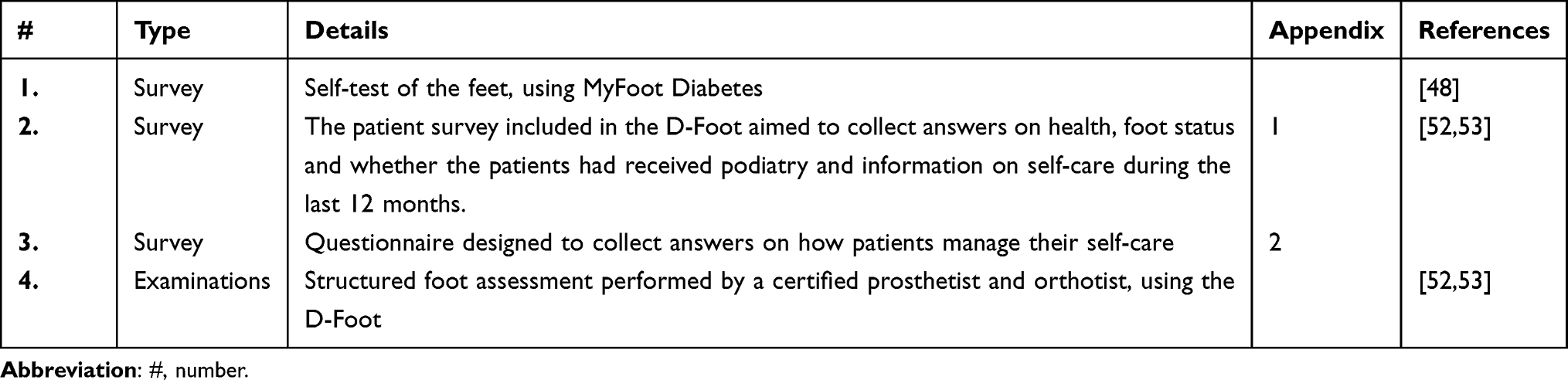 |
Table 2 Surveys and Examinations Used in the Study |
The above-mentioned methods are in various degrees tested for validity and reliability. The content validity of MyFoot Diabetes has, since the release in 2014, continuously been updated by a group consisting of patients’ representatives, diabetes specialist nurses, a podiatrist, a certified prosthetist and orthotist and a medically responsible nurse working within municipal health care.48 The reliability of, and the access to, the software has been secured by the consulting programmers.48 The clinical decision support system, the software D-Foot, has, in an iterative construction process involving a broad spectrum of experts, previously described by Hellstrand Tang et al, been assessed as having a good face and content validity.52 The inter-reliability when using the D-Foot was high, above 0.80 for the risk grade, presence of DFU, amputation, hallux valgus/hallux varus and gait deviations.52 To secure the validity of the first version of the survey, designed to collect answers on how patients manage their self-care and their expectations regarding the services from pharmacy, the construction of the survey followed an iterative process where the team members discussed the formulations and continuously improved the questionnaire, Appendix 2. The team members consisted of a podiatrist, a registered physiotherapist, a certified prosthetist and orthotist and two students in their last year of education at the pharmacy degree programme at the University of Gothenburg. Taken together, the healthcare professionals in the construction team had approximately more than 100 years of clinical experience of care and of giving information regarding self-care of the feet for persons living with diabetes.
The team consisting of two pharmacy students, the principal investigator and a research assistant constructed and followed a structured study protocol, which can be found below. At each of the locations in VGR, three to five participants were scheduled to meet the research team. The study flow for the participants, according to the study protocol, was as follows.
The participants visited each of the stations and the aim was for them to perform the task at each station individually. All the examinations and tests are briefly described in Table 2.
 |
Figure 3 The participants answered a questionnaire in a separate room during the study. |
 |
Figure 4 In a separate room “a fictitious Pharmacy room” the participants answered questionnaires. Notes: In a separate room, “a fictitious pharmacy room”, the participants met two pharmacy students and the participants filled in a survey regarding how they performed self-care of their feet, their foot status, pain in their feet and physical functions related to being able to perform self-care of their feet. |
 |
Figure 5 The participants performed the self-test of their feet using the MyFoot Diabetes software. Notes: In a separate room, “a fictitious pharmacy room”, the participants met two pharmacy students. The participants performed the MyFoot Diabetes self-test using a tablet. |
Survey – Self-Care of the Feet
A survey was constructed by the research team together with a registered physiotherapist, Appendix 2. The purpose of the survey was to collect answers relating to the way patients performed self-care of their feet, their foot status, pain in their feet and physical functions related to being able to perform self-care of the feet. The participants’ expectations of support from the pharmacy relating to self-care of the feet were also captured in the survey. In the survey, the participants answered whether self-management actions were included in their daily life, such as wearing appropriate shoes both outdoors and indoors; wearing socks made of skin-friendly material; moisturising the feet; taking walks; wearing compression stockings (in Swedish “stödstrumpor”) and inspecting the feet. Moreover, questions relating to worries, awareness of the condition of the feet, awareness of risk factors to note on the feet and where to find help if signs of skin lesions appear were included in the survey, Appendix 2.
Ethics
There is always a risk of intrusion of integrity when personal experiences of health and self-care are shared with others. However, the study was carried out following the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.54 The participants received oral and written information about the study, including information on their right to withdraw from the study at any moment without explanation. Participants were included after they signed written informed consent and all the participants agreed to be photographed.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. The study was approved by the Swedish Ethical Review Authority, 2020-08-03, Reg. No. 2020-02175. The advantages of the study were judged to outweigh the eventual inconvenience that participants might experience, eg, the time they spent on the study and travelling. To facilitate participation, the study took place in hotels close to where the participants lived. To respect the participants’ integrity, separate rooms or separate areas in a large room were allocated to the task.
Statistics
Descriptive statistics were used for the age, gender and foot status of the participating patients. Dichotomous variables, such as the presence of risk factors to develop DFU, interventions to prevent DFU and self-reported physical function, foot status, pain and activities of self-care, were presented as numbers, and relevant percentages and continuous values were reported as the mean, standard deviation (SD) and, when relevant, with minimum and maximum values.
Comments, in free text, were reported in the same way as the participants had written their comments in the survey.
In a sub-analysis, the presence of neuropathy was compared from three sources. The self-reported presence of neuropathy was collected 1) when the participant checked their foot status by using MyFoot Diabetes, 2) when the participant filled in the patient survey that was included in the D-Foot and was assessed and 3) when the certified prosthetist and orthotist performed the tests included in the D-Foot.
Results
In Table 3, the foot status is presented with categories of risk factors, eg, the presence of neuropathy, angiopathy, foot deformities, skin pathologies and previous ulcers. The distribution of the patients in risk groups 1–4, respectively, is presented.
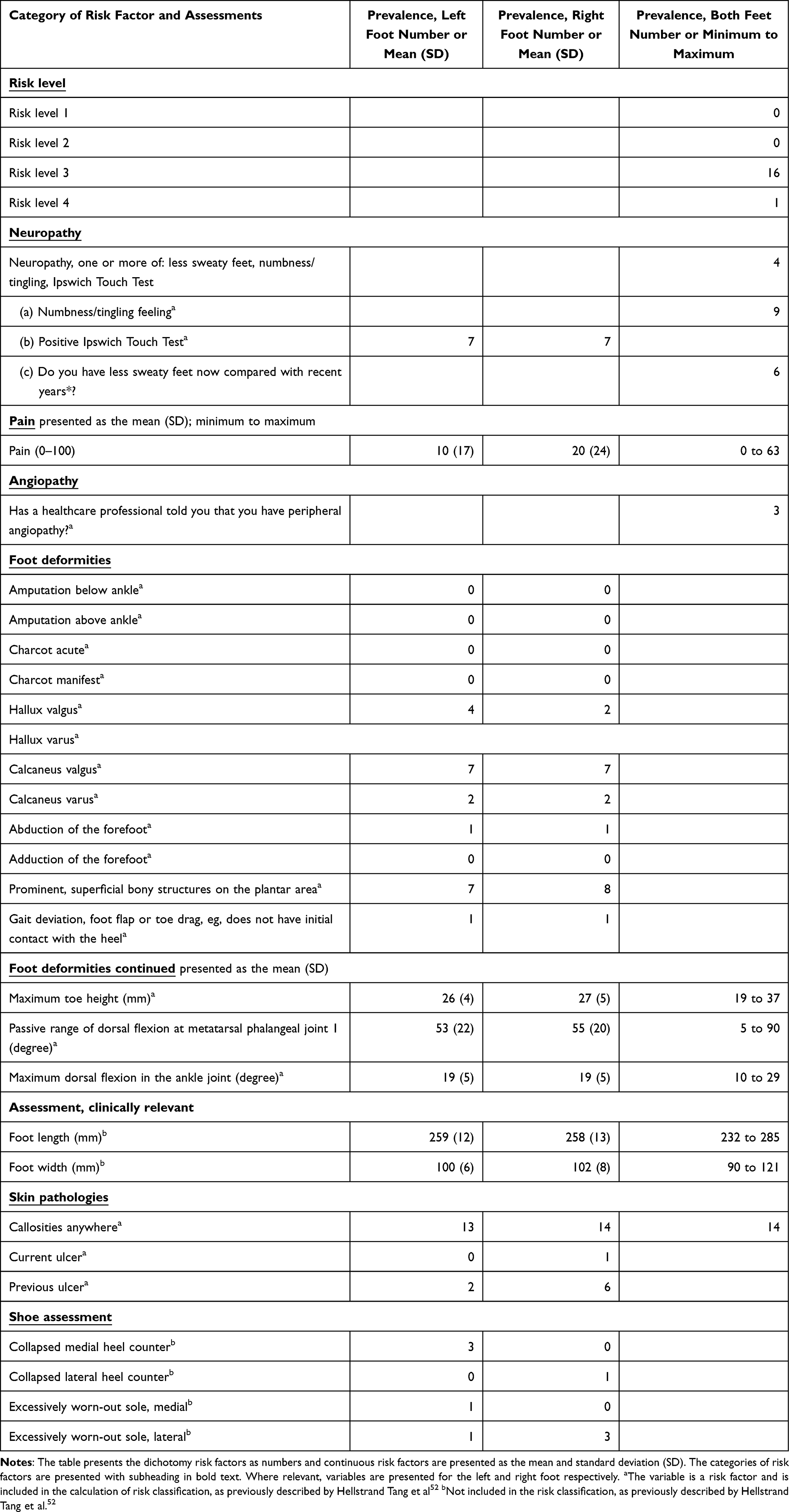 |
Table 3 Risk Factors for Developing DFU Identified with D-Foot |
Differences according to the presence of neuropathy, self-reported and measured with the D-Foot, are presented in Table 4.
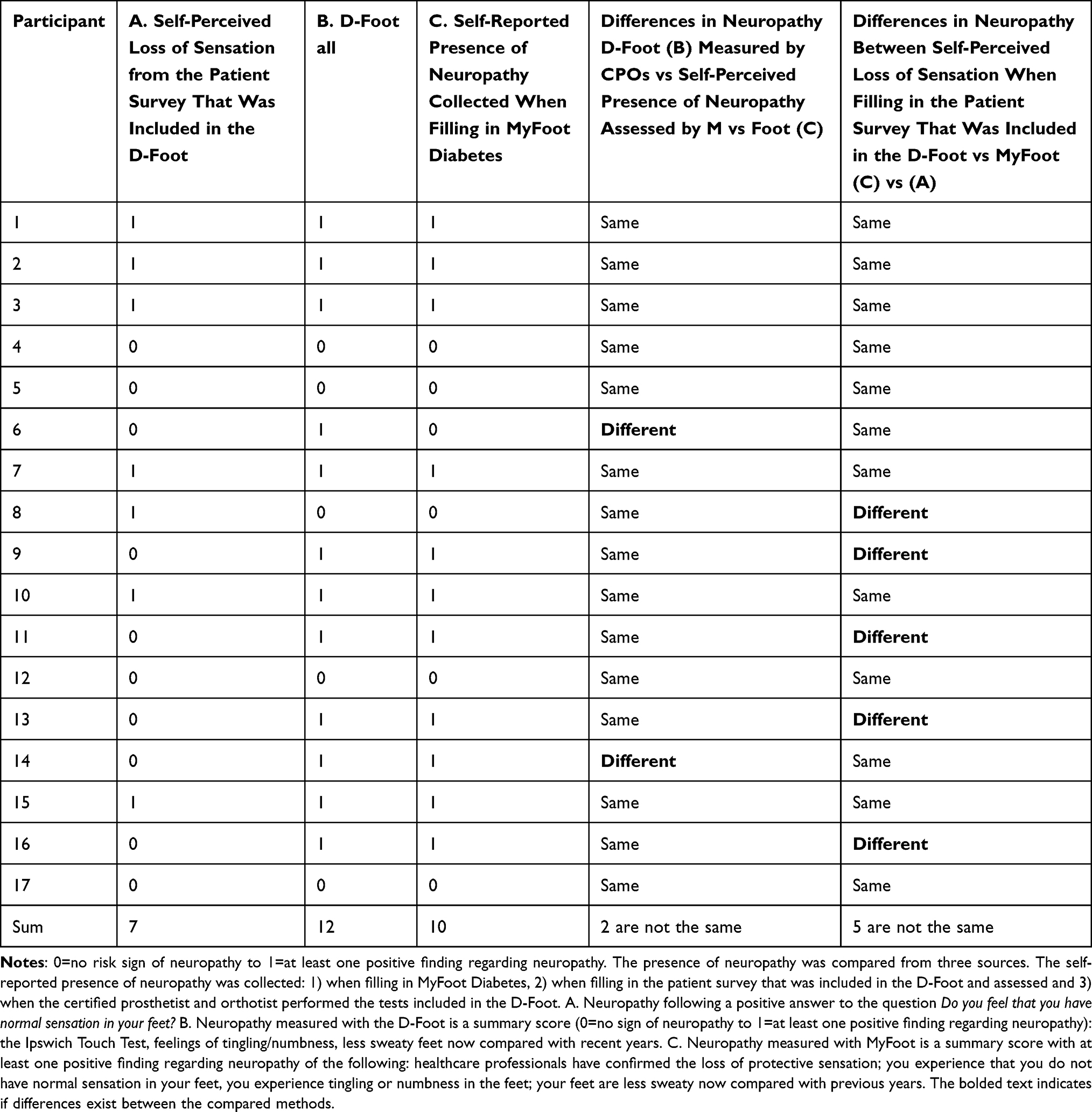 |
Table 4 Presence of Neuropathy, Self-Assessed and Examined (Measured with the D-Foot and MyFoot) |
Self-reported access to podiatry during the last 12 months, having feet examined during the last 12 months and receiving information about self-care of the feet, are presented in Table 5.
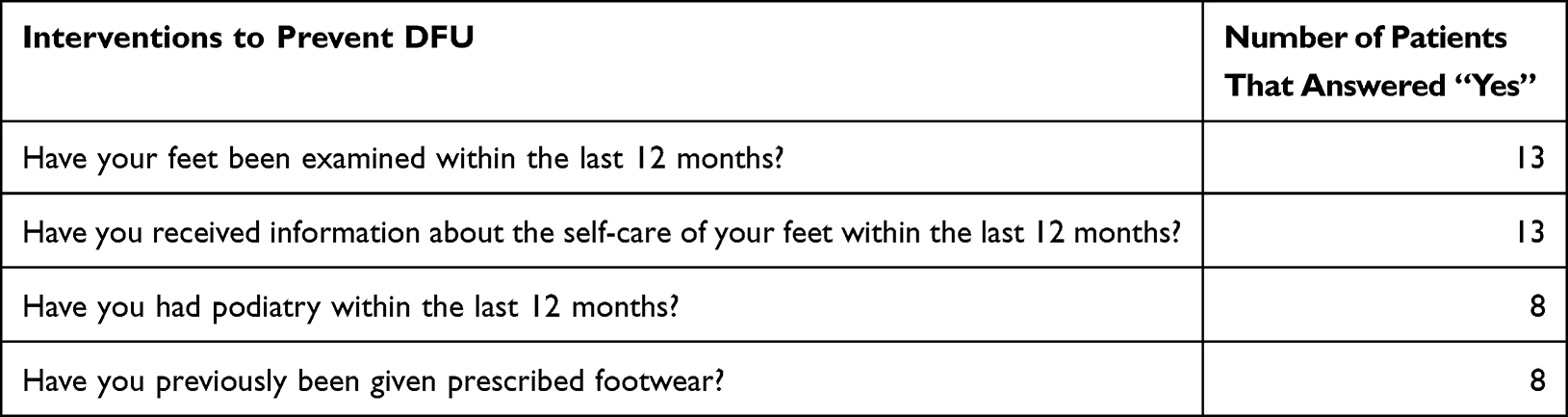 |
Table 5 Patients’ (n = 17) Access to the Interventions Designed to Prevent the Development of DFU Measured with the D-Foot |
In Table 6, the activity of self-management is reported. Eight of the participants reported having made a daily inspection of their feet; nine washed their feet every day and thirteen participants dried the skin between their toes after washing. All the patients (n = 13) who reported that they had dry skin on their feet also answered that they used ointment/creams. Seven patients used ointments/creams between the toes. Nine of the participants walked barefoot indoors and three walked barefoot outdoors. Fourteen always wore socks when wearing shoes. Nine wore socks made of more than 60% cotton, six did not know what material their socks were made of, and the majority (n = 13) were able to cut their toenails themselves.
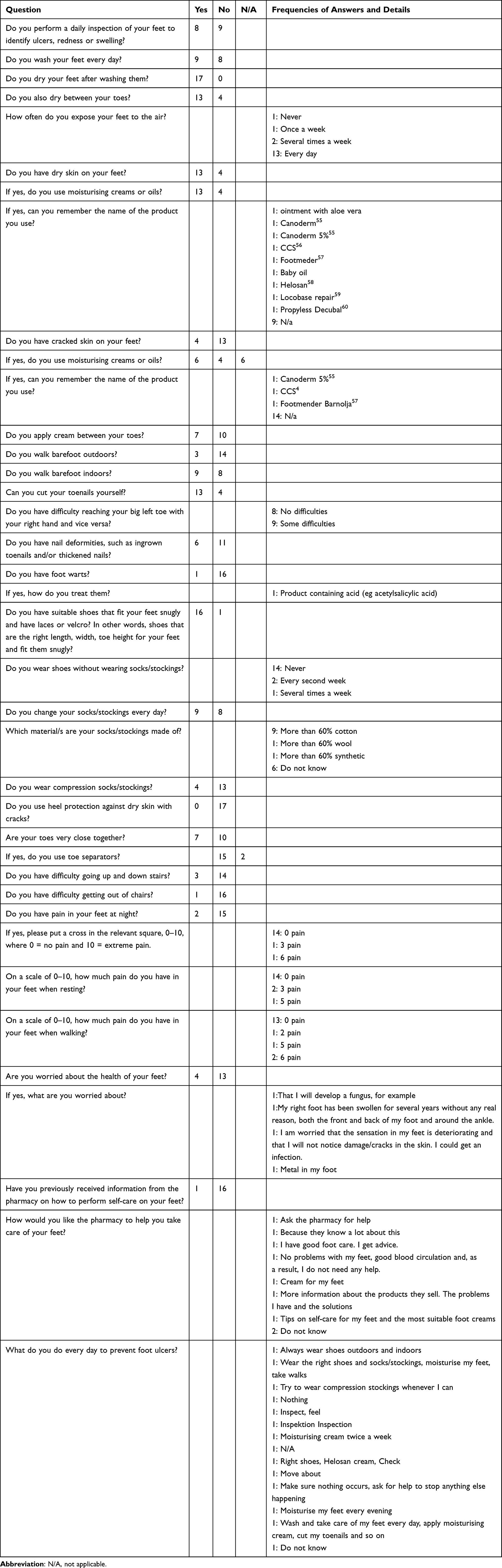 |
Table 6 Self-Reported Physical Function, Foot Status, Pain and Activities of Self-Care from 17 Participants |
Nine patients had some difficulty reaching their toes. Difficulty going up and down stairs and rising from sitting in a chair to standing was present in three of the participants and one of the participants, respectively. Four patients answered that they had pain in their feet while walking (minimum 2 to maximum 6 [0–10 scale]). Two patients had pain during the night and three while resting. Four patients were worried about their foot health in terms of developing mycosis on the feet, the presence of long-term swelling in the foot and sensory loss leading to trauma/fissures going unnoticed.
Sixteen patients had not previously been given information by the pharmacy regarding how to take care of their feet. Several suggestions on how the pharmacy could help them to take care of their feet were registered, for example: giving advice on self-care, having the right skills, giving information about the products they sell, giving advice on ointments/creams.
Discussion
Self-Management of Risk Factors for Developing Diabetic Foot Ulcers
In the current study, 17 patients with diabetes participated in a study describing their expectations regarding support from the pharmacy to improve the self-care of their feet. The participants also reported how they managed the self-care of their feet. Surveys were filled in and the participants assessed their foot status by using the MyFoot Diabetes software. In addition, their foot status was examined by an HCP.
The participants gave several examples of how they self-managed their feet – by wearing shoes indoors and outdoors; wearing socks; moisturising their feet; walking; wearing compression stockings as often as possible; inspecting their feet; checking their feet; being physically active; being aware that their feet are OK; seeking help to prevent DFU; washing their feet; cutting their nails. One participant did not report any action and one did not know. Worries regarding foot health were reported by four of the 17 participants. Supporting findings, from Al Sayah et al, regarding how patients with diabetes manage the care of their feet, show that the self-care varies, and that on average 14% of respondents performed foot self-care behaviours 6 days/week or more.61 The authors of the present study found that some groups were less likely to perform the recommended self-care, eg, men, patients with duration less than 10 years and patients at a younger age.
Expectations of Support from the Pharmacy to Improve Self-Care of the Feet
The participants expected that they would be given competent information from the personnel at the pharmacy to improve the self-care of their feet, eg, information about which ointments/creams to use. Only one of the 17 participants had been given information by the pharmacy on how to perform self-care on his/her feet. Obviously, there is a gap between the expectations of individuals living with diabetes when it comes to whether and how the personnel at the pharmacy support the self-care of the feet. The participants wanted the staff at the pharmacy to be competent and to give relevant, customised information on care of the feet and what ointment/cream to use to moisturise the feet, Table 6. Some participants requested more information about their products.
The study reveals that individuals with diabetes have expectations of support and help from the pharmacy. The gap between the participants’ expectations and reality is also described in the report from the Swedish Medical Products Agency, which concluded that the quality and security of customers should be the focal point when giving objective, expert and individual advice on self-care to their customers.20 A long-awaited improvement in education was suggested. In the report, the reality is described; the staff at the pharmacy have different professions and educations regarding self-care. Bearing this in mind, it is not surprising that there is a lack of quality indicators in Sweden to evaluate whether the service at the pharmacies is of a good standard.36 The Swedish National Board of Health and Welfare concluded in a report that the pharmacies do not have a national assignment regarding advice on self-care and that the staff needed more skills and competence.36
Improvements in competence, regarding advice on the self-care of the feet, among the staff working at the pharmacy, are hopefully being developed in parallel with new evidence-based advice being available on the internet from FASS or 1177, for example.36,62
Risk Factors for Developing DFU and the Responsibility of the Staff at the Pharmacy
Questions arise regarding the responsibility of the staff working at the pharmacy. How should the staff at the pharmacy be able to give individual advice on self-care of the feet that correspond to the customers’ risk factors, eg, the presence of dry skin on the heel or the presence of neuropathy? This question needs to be discussed in the community of HCPs and staff at the pharmacy to clarify when the advice given at the pharmacy is about self-care and when the customer/patient should be referred to healthcare for treatment. Another question is whether it is appropriate that pharmacies develop/use self-tests of the feet, eg, MyFoot Diabetes, as a basis for giving personalised advice on self-care of the feet. Table 3 reveals that the participants had several risk factors; one of them had an ongoing foot ulcer (risk classification 4) and the other 16 patients ran a high risk of developing DFU (risk classification 3). Twelve of the 17 participants had neuropathy, according to the foot examination following the D-Foot routine. Differences according to the presence of neuropathy, self-reported and measured with the D-Foot, are presented in Table 4. The differences are not surprising, as there are many symptoms of neuropathy and several measurements are used.7 Table 4 shows that, of 17 assessments of neuropathy, two differed when comparing the presence of neuropathy examined with the D-Foot as compared with the self-test performed using MyFoot Diabetes. As mentioned above, it is important to know whether and how staff at the pharmacy should act and how the advice on self-care of the feet should be formulated if an individual says that the self-test with MyFoot Diabetes reveals that he/she has neuropathy. The role of self-care activities led by pharmacists needs to be further investigated. Previous studies have shown, in a meta-analysis, an increase in self-care activities following interventions led by pharmacists on foot care (1.20 95% CI [0.49, 1.90] = 95.0% <0.001) and the self-monitoring of glucose levels (1.62 95% CI [0.92, 2.32] = 70.5% = 0.005), according to Bukhsh et al.63 Moreover, a new method presented by Gerber et al includes pharmacists, physicians, case managers, nurses and community-based peer health promoters designed to test and evaluate team-based care to realise therapeutic goals (levels of haemoglobin A1c, LDL-cholesterol levels and blood pressure) in the treatment of diabetes.64
To summarise, the self-care of the feet varied, Table 6, but all the 13 participants, with dry skin on their feet, used emollients. Nine participants had problems reaching their toes, but they all dried their feet after washing. Eight of 17 had not accessed podiatry during the last 12 months, nor had they been prescribed footwear. However, the majority, 13 of 17, had been given information regarding the self-care of their feet from an HCP and had had their feet examined, Table 5.
Method – Discussion
The population in the current study included relatively more patients with diabetes type 2, as compared with the national percentage, 90% of a total of 500,000 persons living with diabetes.65 The reason for this was that the study population was mainly recruited from primary care, where most of the patients with type 2 receive their treatment. According to age and the percentage of women, the study population did not deviate from the larger population of individuals living with diabetes in Sweden. Of the participants aged 70 years, 14 had diabetes type 2 and seven were women.
With few exceptions, all the surveys were filled in at the time the workshop was run. Two people, who did not have time to fill in all the surveys at the workshops, were given a second opportunity to fill in the surveys, as the surveys were sent to them by post and included a stamped, addressed envelope to return their answer in. In addition, one participant gave the answers to a survey by phone to the principal investigator.
The method chosen, an observational descriptive study, is relevant when a new area of research is explored, with the rationale to better formulate further research questions.66 To improve coming measurements regarding patients’ expectations of evidence-based service at the pharmacy with information on self-care of the feet for persons with diabetes at risk of developing foot ulcers, the questionnaire, Appendix 2, needs to be further developed, validated and, when used in other contexts, transculturally adapted. Experiences from Navarro-Flores et al have demonstrated how to improve measurements quality in the development, psychometric analysis and validation of a foot self-care questionnaire.66 Similar methods are recommended when working with research aimed to improve the pharmacies’ services, with the long-term goal to improve how patients self-manage their feet.
Additional improvements, suggested for future studies, are as follows: Firstly, having several separate rooms available so that people’s integrity is secured when the participants fill in the surveys and have their feet examined. Secondly, validating the survey that asked questions about expectations of support from the pharmacy regarding the self-care of their feet, with questions such as the following: What are your expectations of support from the pharmacy? How do you feel that the pharmacy meets your expectations of support? To differentiate the answers, five options are suggested, including very high expectations, high expectations, moderate expectations and low to very low expectations. Thirdly, investigating how the staff at the pharmacy think they manage to give evidence-based, personalised advice on self-care of the feet and how individuals living with diabetes prefer to receive advice (orally, in writing or by digital links).
Conclusion
Patients with diabetes who risk developing foot ulcers expect the staff at the pharmacy to be competent and give them evidence-based, personalised advice so that they can manage the self-care of their feet.
Abbreviations
DFU/s, diabetic foot ulcer/s; DPO, department of prosthetics and orthotics; HCP/s, healthcare professional/s; IWGDF, International Working Group on the Diabetic Foot; mHealth, mobile wireless technologies for public health; PI, principal investigator.
Definitions
Diabetes‐related foot disease: Disease of the foot of a person with current or previously diagnosed diabetes mellitus that includes one or more of the following: peripheral neuropathy, peripheral artery disease, infection, ulcer(s), neuro‐osteoarthropathy, gangrene or amputation.
Acknowledgments
The study was supported by the Innovation Platform in Västra Götaland Region and the Diabetes Organisation in Gothenburg. The authors would like to thank everyone that participated in the study, and we are most grateful to Susanna Danial and Erika Bolin for their contribution to the study during the collection and analysis of the data as a part of their studies at Gothenburg University at the Programme in Pharmacy. We would also like to thank statistician Christer Johansson for the statistical analyses. Finally, we would like to express our appreciation to our graphic designer Pontus Andersson for the illustrations in the MyFoot Diabetes and D-Foot software.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sveriges Kommuner och Regioner. Personcentrerat och sammanhållet vårdförlopp Diabetes med hög risk för fotsår [Person-centered clinical guidelines for persons with diabetes and a high risk of developing foot ulcers]; 2022. Swedish.
2. International Working Group on Diabetic Foot. Definitions & criteria (2023 update); 2023.
3. Khunkaew S, Fernandez R, Sim J. Health-related quality of life among adults living with diabetic foot ulcers: a meta-analysis. Qual Life Res. 2019;28(6):1413–1427. doi:10.1007/s11136-018-2082-2
4. Wukich DK, Raspovic KM, Jupiter DC, et al. Amputation and infection are the greatest fears in patients with diabetes foot complications. J Diabetes Complications. 2022;36(7):108222. doi:10.1016/j.jdiacomp.2022.108222
5. McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, epidemiology, and disparities in the burden of diabetic foot ulcers. Diabetes Care. 2023;46(1):209–221. doi:10.2337/dci22-0043
6. Ragnarson Tennvall G, Apelqvist J. Prevention of diabetes-related foot ulcers and amputations: a cost-utility analysis based on Markov model simulations. Diabetologia. 2001;44(11):2077–2087. doi:10.1007/s001250100013
7. International Working Group on the Diabetic Foot. IWGDF guidelines; 2023. Available from: https://iwgdfguidelines.org/guidelines-2023/.
8. Bus SA, Armstrong DG, Crews RT, et al. Guidelines on offloading foot ulcers in persons with diabetes - IWGDF 2023 update; 2023. Available from: https://iwgdfguidelines.org/wp-content/uploads/2023/07/IWGDF-2023-06-Offloading-Guideline.pdf.
9. International Diabetes Federation. IDF diabetes atlas 2021; 2022.
10. Schaper NC, van Netten JJ, Apelqvist J, et al. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2023:e3657. doi:10.1002/dmrr.3657
11. Socialdepartementet [The patient law]. Patientlagen (SFS 2014:821) [The patient law]. Socialdepartementet; 2014.
12. Sveriges Kommuner och Regioner. Fotundersökning vid diabetes - Nationellt vårdprogram för prevention av fotkomplikationer vid diabetes [Foot examination in diabetes - National clinical guidelines for the prevention of foot complications in diabetes]. 2018.
13. Karvestedt L, Martensson E, Grill V, et al. The prevalence of peripheral neuropathy in a population-based study of patients with type 2 diabetes in Sweden. J Diabetes Complications. 2011;25(2):97–106. doi:10.1016/j.jdiacomp.2010.04.001
14. Chicharro-Luna E, Pomares-Gómez FJ, Ortega-ávila AB, Marchena-Rodríguez A, Blanquer-Gregori JFJ, Navarro-Flores E. Predictive model to identify the risk of losing protective sensibility of the foot in patients with diabetes mellitus. Int Wound J. 2020;17(1):220–227.
15. Rayman G, Vas PR, Baker N, et al. The Ipswich Touch Test: a simple and novel method to identify inpatients with diabetes at risk of foot ulceration. Diabetes Care. 2011;34(7):1517–1518. doi:10.2337/dc11-0156
16. Navarro-Flores E, Morales-Asencio JM, Cervera-Marín JA, Labajos-Manzanares MT, Gijon-Nogueron G. Development, validation and psychometric analysis of the diabetic foot self-care questionnaire of the University of Malaga, Spain (DFSQ-UMA). J Tissue Viability. 2015;24(1):24–34. doi:10.1016/j.jtv.2014.11.001
17. Navarro-Flores E, Romero-Morales C, Villafañe JH, et al. Transcultural adaptation and validation of Italian Selfcare diabetic foot questionnaire. Int Wound J. 2021;18(4):543–551. doi:10.1111/iwj.13554
18. Navarro-Flores E, Losa-Iglesias ME, Becerro-de-bengoa-vallejo R, et al. Repeatability and reliability of the diabetic foot self-care questionnaire in Arabic patients: a transcultural adaptation. J Tissue Viability. 2022;31(1):62–68. doi:10.1016/j.jtv.2021.06.007
19. Bus SA, Armstrong DG, Crews RT, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev. 2023;e3647. doi:10.1002/dmrr.3647
20. Läkemedelsverket. Förslag till reglering av kompetenskrav vid egenvårdsrådgivning [Proposal for regulation of competence requirements for self-care advice]; 2023. Swedish.
21. Socialstyrelsen. Nationella Riktlinjer för Diabetesvård [National clinical guidelines for diabetes care]; 2018. Swedish.
22. Adolfsson ET, Smide B, Rosenblad A, Wikblad K. Does patient education facilitate diabetic patients’ possibilities to reach national treatment targets?: a national survey in Swedish primary healthcare. Scand J Prim Health Care. 2009;27(2):91–96. doi:10.1080/02813430902759671
23. Chen P, Callisaya M, Wills K, Greenaway T, Winzenberg T. Health literacy predicts incident foot ulcers after 4 years – the SHELLED cohort study. J Foot Ankle Res. 2023;16(1):45. doi:10.1186/s13047-023-00644-w
24. Socialstyrelsen. Förskrivning av hjälpmedel [Prescription of assistive devices]; 2016. Swedish.
25. Stolt M, Suhonen R, Puukka P, Viitanen M, Voutilainen P, Leino-Kilpi H. Nurses’ knowledge of foot care in the context of home care: a cross-sectional correlational survey study. J Clin Nurs. 2015;24(19–20):2916–2925. doi:10.1111/jocn.12922
26. Helsenorge. Fotsår og pleie av føtter ved diabetes [Foot ulcers and care of the feet for persons with diabetes]; 2023. Available from: https://www.helsenorge.no/sykdom/diabetes/fotsar-og-pleie-av-fotter-ved-diabetes/.
27. Diabetes in Scotland. Leaflets; 2023. Available from: https://www.diabetesinscotland.org.uk/publications/#leaflet-docs.
28. American Diabetes Association. Diabetes foot complications; 2023. Available from: https://diabetes.org/diabetes/foot-complications.
29. Moullin JC, Sabater-Hernández D, Fernandez-Llimos F, Benrimoj SI. Defining professional pharmacy services in community pharmacy. Res Social Administrative Pharm. 2013;9(6):989–995. doi:10.1016/j.sapharm.2013.02.005
30. Sveriges Apotekarförening. Branschrapport 2022 [Industry report 2022]; 2022. Swedish.
31. Socialdepartementet. Omreglering av apoteksmarknaden Prop. 2008/09:145 [Reregulation of the pharmacy market Prop. 2008/09:145]; 2008. Swedish.
32. Regelrådet. Yttrande över Begränsningar i möjligheterna för vissa aktörer att få tillstånd att bedriva öppenvårdsapotek [Statement on limitations in the possibilities for certain actors to obtain permission to operate outpatient pharmacies] (SOU 2022:27); 2022. Swedish.
33. Sveriges Apotekarförening. Vitbok - Apotekens roll i samhället [White paper - The role of pharmacies in society]. 2013.
34. Sveriges Apoteksförening. Vad är en farmaceutisk tjänst? [What is a pharmaceutical service?] 2023. Available from: http://www.sverigesapoteksforening.se/vad-ar-en-farmaceutisk-tjanst/.
35. Ubeid Z. Hur framtidens apoteksverksamhet kan komma att se ut år 2030 [How the future pharmacy business may look like in year 2030]. Malmö universitet/Hälsa och samhälle; 2019.
36. Socialstyrelsen. Apotekens egenvårdsrådgivning av receptfria läkemedel och andra handelsvaror [The pharmacies service regarding self-care on over-the-counter medicines and other commercial goods]; 2018. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2018-4-24.pdf.
37. 1177.se. 1177; 2022. Available from: www.1177.se.
38. Läkemedelsverket. Läkemedelsboken [The drug book]. Available from: https://beta.lakemedelsboken.se/.
39. Bus SA, Armstrong DG, Crews RT, et al. Guidelines on offloading foot ulcers in persons with diabetes - IWGDF 2023 update. Diabetes Metab Res Rev. 2023;():e3647. doi:10.1002/dmrr.3647
40. Nationella Diabetes Registret. Andel fotundersökta senaste året [Percentage of persons with diabetes being foot examined last year]; 2023. Available from: https://www.ndr.nu/#/statistik.
41. Arbetsgrupp-regional kunskapsstyrning diabetes Västragötalandsregionen [GAP analysis of the clinical person-centered guidelines for persons with diabetes and a high risk of developing foot ulcers]. GAP-analys personcentrerat och sammanhållet vårdförlopp. Diabetes med hög risk för fotsår; 2023. Swedish.
42. Svenska Diabetesförbundet. Diabetesbarometern 2022 [The diabetes barometer 2022]; 2022. Swedish.
43. World Health Organization. mHealth: use of mobile wireless technologies for public health; 2018. Available from: https://apps.who.int/gb/ebwha/pdf_files/EB139/B139_8-en.pdf.
44. United Nation. International Telecommunication Union (ITU). 2022. Available from: https://sustainabledevelopment.un.org/index.php?page=view&type=30022&nr=231&menu=3170.
45. United Nation. SDG 3; 2021. Available from: https://www.un.org/sustainabledevelopment/health/.
46. Kitsiou S, Paré G, Jaana M, Gerber B. Effectiveness of mHealth interventions for patients with diabetes: an overview of systematic reviews. PLoS One. 2017;12(3):e0173160. doi:10.1371/journal.pone.0173160
47. Amante DJ, Harlan DM, Lemon SC, et al. Evaluation of a diabetes remote monitoring program facilitated by connected glucose meters for patients with poorly controlled type 2 diabetes: randomized crossover trial. JMIR Diabetes. 2021;6(1):e25574. doi:10.2196/25574
48. Alnemo J, Hellstrand Tang U. MyFoot, diabetes: an eHealth tool for the diabetic foot.
49. MyFoot diabetes; 2022. Available from: http://www.myfootdiabetes.se/.
50. Andersson S, Scandurra I, Nyström U, Varemo M, Hellstrad Tang U. Experiences of a novel structured foot examination form for patients with diabetes from a healthcare professional’s perspective: a qualitative study. JMIR nursing. 2023;2023. doi:10.2196/45501
51. MyFoot Diabetes. 2023. Available from: www.myfootdiabetes.se.
52. Hellstrand Tang U, Tranberg R, Zügner R, et al. The D-Foot, for prosthetists and orthotists, a new eHealth tool useful in useful in risk classification and foot assessment in diabetes. Foot Ankle Online J. 2017;10(2):4. doi:10.3827/faoj.2017.1002.0004
53. Zügner R, Jarl G, Sundberg L, Hellstrand Tang U. Experiences of using a digital tool, the D-foot, in the screening of risk factors for diabetic foot ulcers. J Foot Ankle Res. 2022;15(1):90. doi:10.1186/s13047-022-00594-9
54. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
55. FASS. Canoderm®; 2023. Available from: https://www.fass.se/LIF/product?userType=2&nplId=19971219000113.
56. Ccs® CCS. 2023. Available from: https://ccshudvard.se/produkter/.
57. FOOTMENDER. Footmender®; 2023. Available from: https://footmender.se/.
58. HELOSAN. HELOSAN®; 2023. Available from: https://helosan.se/.
59. Locobase. Locobase®; 2023. Available from: https://locobase.com/se/.
60. Decubal. Decubal® repair cream; 2023. Available from: https://decubal.com/se/produkt/decubal-repair-cream/.
61. Al Sayah F, Soprovich A, Qiu W, Edwards AL, Johnson JA. Diabetic foot disease, self-care and clinical monitoring in adults with type 2 diabetes: the Alberta’s Caring for Diabetes (ABCD) Cohort Study. Can J Diabetes. 2015;39 Suppl 3:S120–6. doi:10.1016/j.jcjd.2015.05.006
62. Läkemedelsindustriföreningens Service AB [Pharmaceutical specialties in Sweden]. FASS; 2023. Available from: https://www.fass.se/LIF/startpage.
63. Bukhsh A, Tan XY, Chan KG, Lee L-H, Goh B-H, Khan TM. Effectiveness of pharmacist-led educational interventions on self-care activities and glycemic control of type 2 diabetes patients: a systematic review and meta-analysis. Patient Preference Adherence. 2018;12:2457–2474. doi:10.2147/PPA.S180256
64. Gerber BS, Rapacki L, Castillo A, et al. Design of a trial to evaluate the impact of clinical pharmacists and community health promoters working with African-Americans and Latinos with diabetes. BMC Public Health. 2012;12(1):891. doi:10.1186/1471-2458-12-891
65. Nationella Diabetes Registret. Årsrapport 2022 [Annual Report 2022]; 2023. Swedish.
66. Rezigalla AA. Observational study designs: synopsis for selecting an appropriate study design. Cureus. 2020;12(1):e6692. doi:10.7759/cureus.6692
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Educational Interventions in Immigrants for Asthma and COPD: A Systematic Review
Al-Juhaishi M, Lim CX, Chan V, Stupans I, Thrimawithana TR
Patient Preference and Adherence 2023, 17:3245-3257
Published Date: 11 December 2023
The Existing Interventions to Promote Self-Care and Self-Monitoring Preventing Hypertension Among Thai Risk People: A Scoping Review
Banharak S, Potempa K, Limpawattana P, Pamungkas RA, Mahikul W, Jeamjitvibool T, Karaket A, Siriprathum S, Ransinyo K
Vascular Health and Risk Management 2025, 21:519-544
Published Date: 9 July 2025
Anticipations and Requirements of Individuals with Long-Term Health Conditions Regarding Self-Management and Digital Health Support Tools
Alessa T
Patient Preference and Adherence 2025, 19:2901-2918
Published Date: 13 September 2025