Back to Journals » Risk Management and Healthcare Policy » Volume 19
Patient Risk Identification Ability Among Newly Graduated Nurses: A Mixed-Methods Study
Authors He L, Meng L, Tuo C, Tan R ![]() , Li M
, Li M ![]() , Wei X
, Wei X
Received 4 September 2025
Accepted for publication 26 January 2026
Published 5 February 2026 Volume 2026:19 565380
DOI https://doi.org/10.2147/RMHP.S565380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Gulsum Kaya
Lifang He,1 Lingyao Meng,1 Chi Tuo,1 Ruyan Tan,1 Mengyang Li,1 Xiuxia Wei2
1School of Nursing, Xiangnan University, Chenzhou, 423000, People’s Republic of China; 2Department of Nursing, Yancheng Third People’s Hospital, Affiliated Hospital 6 of Nantong University, Yancheng, 224000, People’s Republic of China
Correspondence: Xiuxia Wei, Department of Nursing, Yancheng Third People’s Hospital, Affiliated Hospital 6 of Nantong University, Yancheng, 224000, People’s Republic of China, Tel +86 15861983067, Email [email protected]
Purpose: Risk identification is a primary step in implementing medical risk management. Given the limited research on the patient risk identification ability of newly graduated nurses, this study aims to explore their current capacity for identifying patient risks and the associated influencing factors.
Participants and Methods: A convergent parallel mixed-methods design was employed. Quantitative data were collected via an online cross-sectional survey from 212 newly graduated nurses using the self-assessment questionnaire on patient risk identification ability. Qualitative data were obtained through semi-structured interviews with 11 participants.
Results: Participants scored 73.32 ± 9.20 in patient risk identification. Dimension scores were highest for risk perception (3.96 ± 0.51), followed by risk analysis ability (3.47 ± 0.50) and risk knowledge mastery (3.22 ± 0.54). The regression model revealed that length of employment (β = 7.475, 95% CI [6.551, 8.398]), employment type (permanent: β = 7.487, 95% CI [3.851, 11.123]), having a family member in healthcare (β = 2.409, 95% CI [0.844, 3.973]), received patient-safety training or related coursework (β = 2.700, 95% CI [0.712, 4.688]), marital status (married: β = 3.622, 95% CI [0.858, 6.386]), attitude toward nursing (β = 0.842, 95% CI [0.171, 1.512]), education level (β = 1.729, 95% CI [0.340, 3.118]), and current unit (other units: β = − 3.253, 95% CI [− 5.883, − 0.623]) were significant predictors of risk identification capacity (all p < 0.05). Qualitative analysis identified four themes: heightened risk awareness, limited ability to judge and analyze complex conditions, barriers, and facilitators. Integrated analysis showed high concordance between datasets, except regarding the influence of clinical workload.
Conclusion: The risk identification ability of newly graduated nurses requires considerable improvement, particularly in mastering risk-related knowledge and analyzing risks in complex clinical situations. This ability is influenced by personal knowledge and experience, professional values, clinical workload, patient safety education, and organizational support.
Keywords: patient safety, risk assessment, safety management, clinical competence, nurses
Introduction
Risk identification is an essential prerequisite for implementing risk management; accurately identifying error-prone processes enables the formulation of informed clinical safety management decisions.1 Compared to other healthcare professionals, nurses spend more time with patients and play a critical role in identifying patient safety risks and ensuring high-quality care.2 A nurse’s capacity to identify patient risks encompasses systematic judgment, classification, and analysis of various potential hazards—such as physiological, psychological, procedural, and environmental factors—alongside their causes during a patient’s hospitalization.3 Previous studies have demonstrated that integrating patient safety identification systems can optimize patient safety and treatment outcomes.4,5
Patient risk identification constitutes a critical component of patient safety competence. Currently, research on risk identification capacity is often integrated into broader investigations of patient safety competence. The Canadian Patient Safety Institute has established a Safety Competency Framework for healthcare personnel, encompassing six core competencies: contributing to a safety culture, collaborating within teams, communicating effectively, managing safety risks, optimizing human and environmental factors, and recognizing, responding to, and reporting safety adverse events.6 Within this framework, “managing safety risks” refers specifically to predicting, identifying, and managing patient safety risks. Questionnaires developed based on this framework have been translated into multiple languages and widely used across various countries, demonstrating applicability to diverse healthcare professionals, including physicians, nurses, and pharmacists.7 For instance, a survey conducted by Hwang8 in three Korean hospitals using this questionnaire revealed a moderate level of patient safety competence among nurses; notably, younger, less experienced, and less educated nurses reported lower confidence in safety practices.
Current evidence indicates that clinical nurses generally exhibit a moderate level of patient safety competence, collectively influenced by variables such as professional background (eg, years of experience), cognitive capacity (eg, systematic thinking), patient safety education, and organizational culture (eg, teamwork).9 Systematic patient safety education courses and training programs that span from pre-graduation education through to independent clinical practice can shape and enhance nurses’ safety competency.10,11 However, none of these studies specifically addresses nurses’ safety risk management competence. As researchers have noted, despite increasingly complex and dynamic clinical environments, there remains a significant scarcity of data relating to how nurses identify potential and actual safety risks, and how their risk assessments influence patient management decisions and care outcomes.12 Consequently, examining nurses’ abilities in patient safety risk identification and severity judgment is critical, as these competencies directly shape subsequent patient management strategies.
Addressing this gap, Wu3 developed a standardized instrument to assess nurses’ risk identification capacity in China, employing literature reviews, expert interviews, and Delphi consultations. This tool encompasses three dimensions: risk knowledge acquisition, risk perception, and risk analysis, establishing a psychometrically validated instrument for quantitative research. Empirical studies utilizing this instrument indicate that nurses’ risk identification capacity in China is moderately competent overall. Nurses with longer clinical experience, higher professional titles, employment in core clinical departments (eg, surgery, obstetrics and gynecology, Intensive Care Unit), those serving as clinical mentors, and those who have received patient risk-related training or specialized nurse training tend to demonstrate stronger risk identification ability.13–15 Notably, nursing interns demonstrate substantially lower capacity compared to practicing nurses. Interns with ≥7 months of clinical placement, bachelor’s degrees, safety training exposure, and family healthcare backgrounds collectively exhibit enhanced capacity.16 Additionally, a qualitative study from the UK highlighted several organizational-level factors influencing successful risk identification, including inadequate training, the need to balance financial and safety considerations, and the challenge of integrating risk information from different assessment tools and methods.17
Existing research on patient safety competence and risk identification ability predominantly focuses on practicing nurses and nursing interns, with limited investigations into the association between newly graduated nurses and patient safety.18 Prior studies indicate that novice or inexperienced nurses are more likely to miss critical patient signs, particularly within contemporary dynamic clinical environments characterized by increasing patient acuity and rising nurse-to-patient ratios.19,20 Heavy workloads and fixation on specific parameters of a patient may further impede their ability to holistically assess patient condition changes.21 Newly graduated nurses encounter significant transitional challenges, marked by disparities in knowledge application capacity and clinical adaptability compared to experienced nurses. Transitioning from academic settings to clinical practice, they often demonstrate underdeveloped technical skills, limited clinical experience, and deficient anticipatory judgment amid multifaceted pressures. These challenges contribute to unconfident and inaccurate patient risk identification, ultimately compromising patient safety.22,23 Therefore, comprehensive assessment of their risk identification capacity is imperative. This study aims to investigate the current status and influencing factors of patient risk identification capacity among newly graduated nurses. Findings from this study will provide valuable references for nursing administrators to develop targeted training programs and support strategies aimed at enhancing risk identification competency among new nurses, while also offering valuable insights for improving their entry-to-practice education and the quality of clinical nursing care.
Materials and Methods
Study Design
This study employed a convergent parallel mixed-methods design to facilitate a detailed inquiry into the research questions and enhance the validity of the inferences drawn from the results. This approach involved the concurrent but separate collection of quantitative and qualitative data, where both types were given equal priority. Data were then analyzed separately and subsequently integrated for interpretation to compare and validate the findings.24 An overview of the study design is presented in Figure 1.
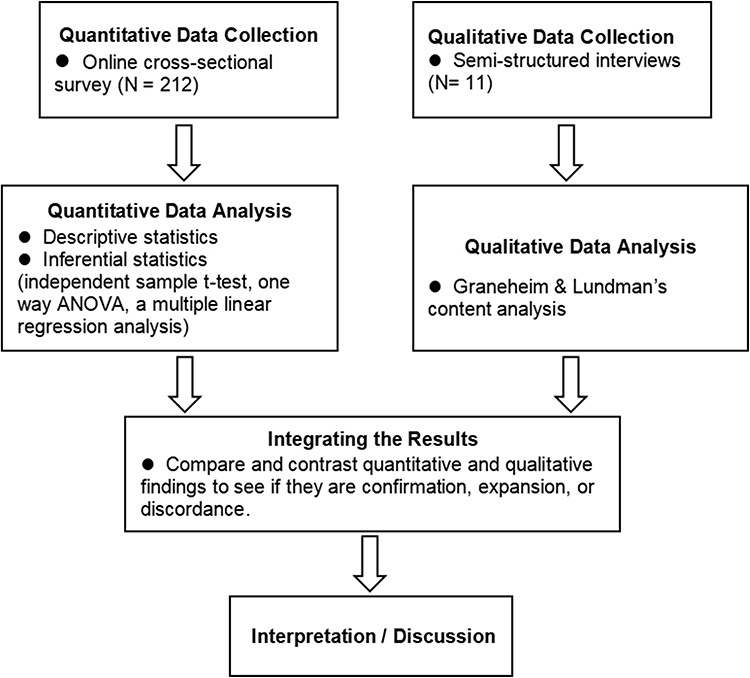 |
Figure 1 Convergent parallel mixed methods design used for study. |
Study Setting and Sampling
This study recruited newly graduated nurses from two higher education institutions in Hunan Province, China, as research participants. Inclusion criteria were: (1) New nursing graduates; (2) holding a valid national nurse practice license; and (3) having ≤1 year of clinical work experience. Exclusion criteria comprised: (1) any prior formal clinical work experience and (2) non-frontline clinical practitioners. Informed consent was obtained from all participants. Participants for the quantitative component were recruited via convenience sampling. The sample size was estimated a priori using G*Power 3.1. Based on a linear multiple regression model with 17 predictors, a significance level of.05, a statistical power (1-β) of.90, and an effect size f2 of 0.15, the required sample size was 179. Ultimately, 212 valid questionnaires were collected, satisfying the predetermined sample size criteria. Purposive sampling was used for qualitative methods, considering nurses who completed the questionnaire for the interviews. Sample size was determined based on the principle of data saturation, achieved when no new information emerged from subsequent data collection.25
Quantitative Data Collection and Analysis
An online cross-sectional survey was administered via the online survey platform “Wenjuanxing” (www.wjx.cn) from September 2024 to November 2024. The online questionnaire consisted of two parts: general information and the self-assessment questionnaire on patient risk identification ability. The first part included 17 questions regarding participants’ socio-demographic characteristics (eg, gender, age, etc)., professional background (eg, education levels, length of employment, etc)., and professional attitude. The self-assessment questionnaire on patient risk identification ability developed by Wu et al4 comprises three dimensions: risk knowledge mastery, risk perception, and risk analysis ability. The questionnaire consists of 21 items rated on a 5-point Likert scale from 1 (very poor) to 5 (excellent), yielding a total score ranging from 21 to 105, with higher scores indicating better risk identification ability. It has demonstrated good reliability and validity, with a Cronbach’s α of 0.956.13 In the current study, its Cronbach’s α was 0.882. Prior to completing the online questionnaire, participants were required to review the informed consent form and click the “Agree” button to proceed. The questionnaire ensured anonymity, and participants could withdraw at any time. Technical restrictions prevented multiple submissions from the same device to avoid duplicate responses. Data cleaning was performed to exclude invalid questionnaires with uniform responses or logical inconsistencies, ensuring data accuracy.
Statistical analyses were conducted using SPSS 27.0. Categorical data were presented as frequencies (percentages), and continuous data (age and patient risk identification scores) were expressed as means (standard deviation). Independent-samples t-tests or one-way analysis of variance were employed to compare differences in patient risk identification ability across the demographic characteristics of new graduate nurses. Variables showing statistical significance in preliminary analyses were further examined using stepwise multiple regression to identify determinants of risk identification ability. The Variance Inflation Factor (VIF) was used to detect multicollinearity issues among independent variables, excluding those with VIF > 10 to mitigate bias from collinear predictors. A threshold of p < 0.05 were considered statistically significant.
Qualitative Data Collection and Analysis
Semi-structured interviews were conducted using an interview outline based on literature and practical experience to elicit rich and insightful responses from October 2024 to November 2024. To ensure broad geographic participation and accommodate daily communication preferences, WeChat was selected as the platform for conducting online interviews. Research confirms that web-based interviews yield results of accuracy comparable to face-to-face interviews.26 Before the interview, the researcher sent the informed consent form to participants via WeChat and confirmed their availability. Participants were instructed to read the informed consent form thoroughly, sign it electronically, and return the signed file before the formal interview commenced. Audio recording software was used to record all interviews, along with non-verbal information such as intonation and pauses. The interview outline included core questions: (1) In your current unit or during clinical rotations, which patient-safety risks do you consider most critical to remain vigilant for? (2) Reflecting on your experience since you began working as a registered nurse: a) Which specific aspects of identifying patient risks do you feel confident about? b) In which areas do you require further development? (3) What perceived barriers or difficulties have you encountered in identifying patient risks? (4) What factors do you believe contribute to the enhancement of your ability to identify patient risks? Probes such as “Can you give an example?” and “Could you tell me a bit more about that?” were used to elicit rich and insightful responses. Interviews continued until data saturation was reached; that is, subsequent data collection yielded no new information.25 All interview recordings were transcribed verbatim within 24 hours and meticulously verified by the research team. Following participant verification, qualitative data analysis was conducted using NVivo 12 software, employing the Graneheim & Lundman content analysis method.27 The analytical process entailed (1) iterative close reading to establish a holistic understanding; (2) segmentation of text into research-aligned meaning units, with semantic condensation yielding condensed units assigned initial codes; (3) integration of semantically cognate codes into subcategories and categories, culminating in the abstraction of profound themes. Two researchers independently analyzed the data, resolving any discrepancies through discussion with the broader research team.
The trustworthiness of the qualitative component was ensured by adhering to the four criteria proposed by Lincoln and Guba28—credibility, dependability, confirmability, and transferability. Credibility: The researchers received training in qualitative research theory and methods, demonstrating proficiency in qualitative approaches and interview techniques. After data analysis, the findings were returned to the participants for verification to ensure alignment with their original intent. Dependability: Two researchers familiar with content analysis independently performed the data analysis, and any discrepancies were resolved through group discussions to reach consensus. Confirmability: To ensure the reliability of the study, all research materials (such as the interview guide, raw data, and analytical results) were properly archived for potential future verification. Transferability: Detailed demographic descriptions of the participants are provided to allow others to assess the applicability of the findings in different contexts.
Mixed Methods Analysis
Quantitative and qualitative data were integrated at the interpretation and reporting levels via a joint display table This approach facilitates direct data integration and enhances the meta-inference of mixed-methods findings.29 Assessment of fit of integration allows for three possible outcomes: Confirmation, where the findings from both sources support each other; Expansion, where divergence addresses different aspects of the phenomenon; and Discordance, where qualitative and quantitative findings conflict.
Results
Characteristics of Participants
A total of 235 newly graduated nurses responded to the survey, with 212 valid questionnaires collected. Among the 212 participants, 16 (7.55%) were male, with a mean age of 22.98 ± 1.87 years. Further general data are presented in Table 1. Eleven participants were recruited for the semi-structured interviews, with interviewee ages ranging from 22 to 27 years, including one male, and work experience spanning 1 to 10 months. They worked across 10 different clinical units, including internal medicine, surgery, the operating room, and the intensive care unit (see Table S1).
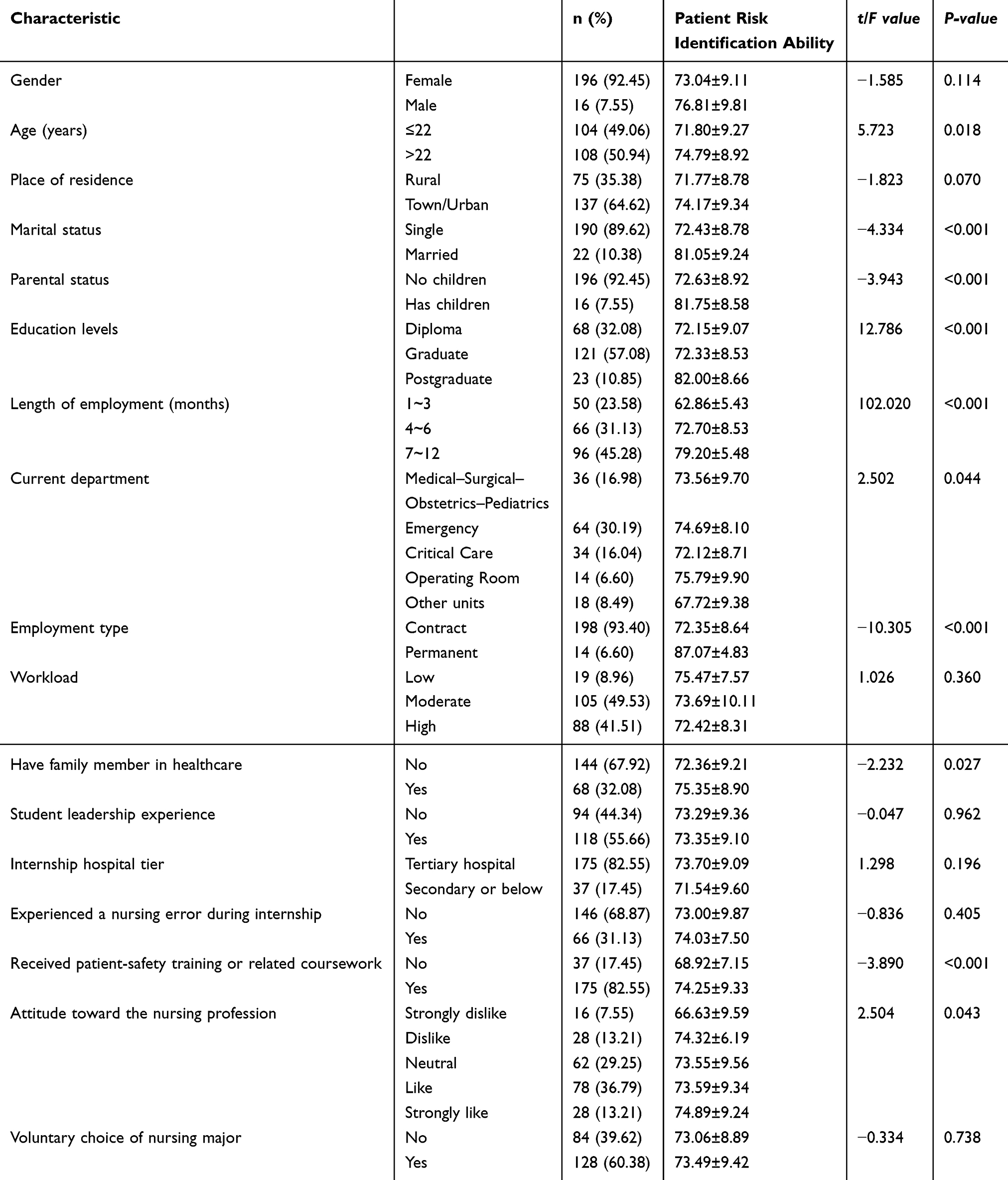 |
Table 1 General Information About the Participants and the Candidate Factors Influencing Their Patient Risk Identification Ability |
Quantitative results
Scores of Patient Risk Identification Ability
Newly graduated nurses self-reported a patient risk identification ability score of 73.32 ± 9.20, with an average item score of 3.49 ± 0.44. The scores across dimensions, ranked from highest to lowest, were as follows: 3.96 ± 0.51 for risk perception, 3.47 ± 0.50 for risk analysis ability, and 3.22 ± 0.54 for risk knowledge mastery.
Factors Influencing Patient Risk Identification Ability
Univariate analysis revealed statistically significant differences in patient risk identification ability scores across the following variables: age, marital status, parental status, education levels, length of employment, current unit, employment type, have family member in healthcare, received patient-safety training or related coursework, and attitude toward the nursing profession (all p < 0.05). Detailed results are presented in Table 1.
The total score of patient risk identification ability was used as the dependent variable, while the variables exhibiting statistically significant differences in univariate analysis were incorporated into the multiple linear regression model as independent variables (variable assignments are detailed in Table 2). The regression analysis identified the following significant predictors of risk identification ability: length of employment (β = 7.475, p < 0.01), employment type (permanent: β = 7.487, p < 0.01), having a family member in healthcare (β = 2.409, p = 0.003), received patient-safety training or related coursework (β = 2.700, p = 0.008), marital status (married: β = 3.622, p = 0.010), attitude toward nursing (β = 0.842, p = 0.014), education level (β = 1.729, p = 0.015), and current unit (other units: β = −3.253, p = 0.016) were significant predictors of risk identification capacity. The regression model demonstrated an R2 of 0.674 and an adjusted R2 of 0.661, indicating that these factors collectively account for 66.1% of the variance in patient risk identification ability scores (see Table 3).
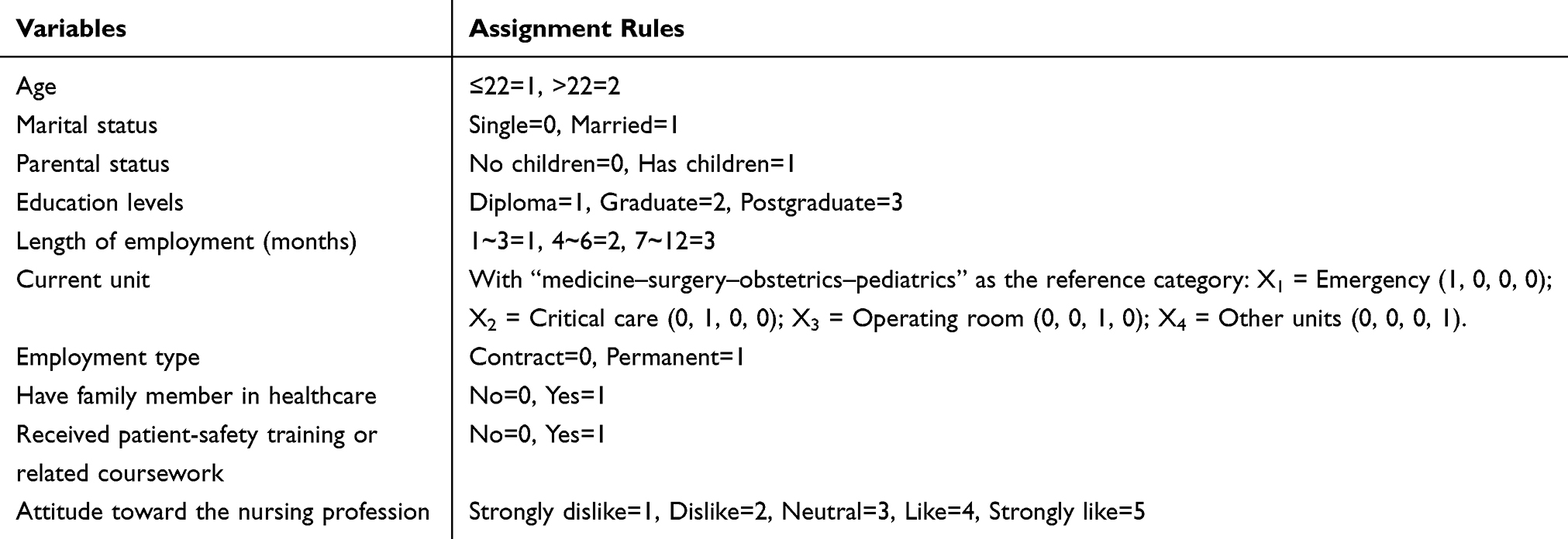 |
Table 2 Assignment Rules of the Variables |
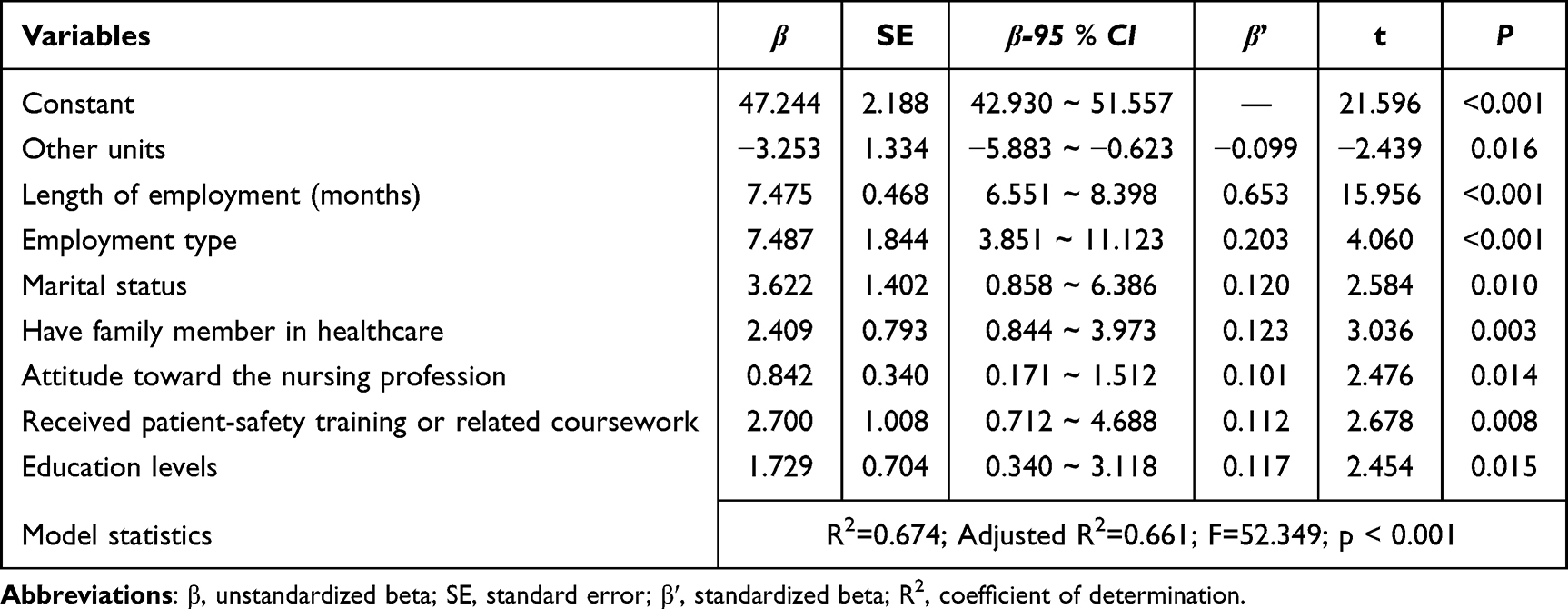 |
Table 3 Multiple Linear Regression Analysis of Variables Affecting the Patient Risk Identification Ability of Newly Graduated Nurses |
Qualitative Results
Content analysis identified four themes regarding the current status and influencing factors of patient risk identification capacity among newly graduated nurses: heightened risk awareness, limited ability to judge and analyze complex conditions, barriers, and facilitators. The barrier theme comprised three categories: inadequate clinical experience, insufficient specialty-specific knowledge, and heavy clinical workload. The facilitator theme included four categories: patient-risk-related training, guidance from senior colleagues, accessible professional resources, and a sense of responsibility.
Heightened Risk Awareness
Interviewees fully recognized the pivotal role of patient risk identification in their daily practice. They considered potential safety hazards from multiple perspectives—environmental conditions, patient-related factors, and procedural actions taken by healthcare personnel—and consistently demonstrated self-discipline by adhering to standard operating procedures to regulate their behavior.
For example, in our unit the most common risk is falls. First, many elderly patients have poor balance… some simply cannot accurately assess their own abilities. Second, environmental factors play a role—cleaning staff frequently mop the floors, and at night the ward is dim when patients get up to use the bathroom. Finally, if healthcare staff do not adequately educate the patient and family, the risk is heightened because they fail to take it seriously. (P3)
As a newly hired nurse, I’m actually very alert to the principle of professional integrity, because my career has just begun and I’m especially conscientious. (P5)
Participants emphasized the importance of continuously expanding their theoretical knowledge to internalize risk awareness and enhance risk-identification competence. As one interviewee noted:
I realize that one of the most important things is to keep supplementing my knowledge, because all practice is built on theory. Before facing a situation—or even before it arises—we have at least studied relevant theories and literature to understand potential patient scenarios and necessary interventions. (P4)
Limited Ability to Judge and Analyze Complex Conditions
Newly graduated nurses reported deficits in clinical judgment and analytical capacity for complex cases, primarily manifested as: (1) a compromised ability to holistically analyze patients with multiple comorbidities and intertwined symptoms/signs, hindering precise determination of pathophysiological linkages; and (2) insufficient predictive capacity and detection sensitivity for rapidly evolving complications in clinically deteriorating patients.
I’m still quite weak at synthesizing complex cases. I often struggle to pinpoint how multiple illnesses and overlapping symptoms relate to one another, and I worry that overlooking a single detail could stall a patient’s treatment. (P5)
Some patients deteriorate rapidly, and I know I need to sharpen my ability to anticipate their potential complications before they surface. (P7)
Barriers
Insufficient Clinical Experience
All participants identified a lack of hands-on experience as the key barrier to recognizing patient risk. On one hand, the textbook knowledge they acquired as students has not yet been fully translated into practical clinical skills, causing them to mechanically apply this knowledge during patient evaluations, ultimately complicating individualized risk assessments. On the other hand, limited clinical exposure undermines their confidence when collaborating with other healthcare professionals or communicating with patients, leading to inadequate information exchange or passive compliance with instructions—both of which can compromise patient risk identification.
What I learned is still very textbook-based, and I’m far from being truly clinical. Because of that, I often can’t tailor my assessment to the individual patient, so I may miss some of their problems. (P2)
Honestly, our communication skills aren’t as strong as those of the senior nurses… Plus, matching doctors and nurses and working together is demanding—you have to be ready to correct or challenge any inappropriate suggestions. (P8)
Insufficient of Specialty-Specific Knowledge
Although newly graduated nurses have acquired foundational professional knowledge through academic coursework and routine clinical placements, they lacked an in-depth understanding of specialty-specific diseases and medications. This knowledge gap hindered their ability to recognize patient-related risks.
My knowledge of rare diseases is limited. I lack both the pathophysiological understanding and the hands-on experience needed for these conditions, so when I’m caring for a patient with a rare disease, I find it very hard to judge whether certain risks are present. (P5)
In the ICU we use a huge range of medications—besides the standard emergency drugs, some patients need highly specialized ones… But I’m not yet clear on their exact mechanisms of action or on which patients might experience adverse reactions. (P4)
Heavy Clinical Workload
The substantial volume of daily tasks—including continuous patient admissions, intensive delivery of basic treatments, and documentation—leaves newly graduated nurses severely time-constrained. This pressure forces them into repetitive mechanical routines, diminishes their capacity to focus on patients, and results in risk assessment procedures being overlooked or omitted.
Like today, I admitted a patient just after 8 a.m., but I didn’t start his charting until after 5 p.m., right after handover. I was so swamped that all I could do was give the scheduled injections. Unless the patient called me, I simply had no time to check on him. (P1)
Our day-to-day work is just very busy. Honestly, every single time slot has its own tasks that have to get done then. That means during the day, you don’t have much spare time to check on every single patient. (P10)
Facilitators
Patient-Risk-Related Training
Newly graduated nurses widely believe that enhanced training focused on patient risk is crucial for improving their risk identification abilities. They anticipate addressing knowledge gaps by participating in more systematic learning activities, including focused training on patient observation and emergency management, patient safety case discussions, and scenario-based drills. Such activities effectively enable new nurses accumulate experience in recognizing risks, thereby boosting their clinical alertness and ability to make timely judgment calls regarding patient risks.
We need more training—extra sessions aimed at sharpening our clinical observation skills and our ability to handle emergencies… or run more of those simulation drills. (P1)
I also think we should take part in more departmental or hospital-wide lectures and case-analysis meetings. Our unit occasionally holds case conferences where we discuss and share the risks a patient faced during treatment and how to spot those risks. Going through real cases like that really boosts my risk-identification skills. (P9)
Guidance from Senior Colleagues
A critical enabler for newly graduated nurses to enhance their ability to identify patient risks was the guidance provided by senior colleagues. Structured departmental initiatives, such as “one-to-one” preceptorship programs and team-based peer mentoring models, fostered continuous knowledge transfer. This environment accelerated the transformation of passively received guidance into proactive risk anticipation skills, effectively bridging gaps in clinical experience.
Our department assigns each of us a senior nurse for one-to-one mentoring. In the clinical setting I always work alongside my preceptor; right from my first shifts she showed me how to spot patient risks, so I can draw on her experience and steadily sharpen my own risk-identification skills. (P5)
As I just mentioned, risk-identification improves when the whole team collaborates—experienced nurses guiding new ones. (P6)
Accessible Professional Resources
Standardized risk assessment tools offered newly graduated nurses objective evaluation methods that reduced the chances of omitting assessments. Collaborative support from specialized nurses (eg, certified catheter specialists, nutrition support nurses) provided domain-specific risk anticipation expertise, enhancing new graduates’ precision in identifying complex issues. Furthermore, interprofessional learning through medical team interactions—such as participating in case discussions and understanding the logic behind clinical decision-making—deepened new nurses’ comprehension of potential risks and disease progression. These professional resources effectively bridge experience deficits and foster growth in risk identification capabilities.
For instance, those risk-assessment scales I mentioned earlier, plus the growing number of specialized nurses—putting all these tools together really strengthens our ability to spot risks. (P2)
Closer communication with doctors—talking through a patient’s condition—lets us understand how physicians assess the case and plan treatment. Learning from their clinical reasoning helps us identify different risks in our patients. (P5)
A Sense of Responsibility
The primary intrinsic driver for newly graduated nurses to enhance their risk identification abilities stemmed from their sense of clinical accountability. This responsibility compelled a deeper commitment to patient monitoring and fueled continuous learning through knowledge refinement and critical reflection, thereby strengthening their capacity to detect clinical risks.
I believe a nurse’s sense of responsibility is paramount. We may be busy, but that’s no excuse for cutting corners. We must be meticulous and never overlook a single detail. (P5)
I also need to analyse and reflect on individual cases—asking myself what I should focus on for this particular illness and how it differs from others. By keeping up with the latest evidence—reading the newest literature—I can continually update my knowledge. (P8)
Integration of Quantitative and Qualitative Results
The integration of quantitative and qualitative findings demonstrates that qualitative results support and extend the quantitative ones; however, a discordance emerged regarding the impact of workload on newly graduated nurses’ risk identification abilities (Table 4).
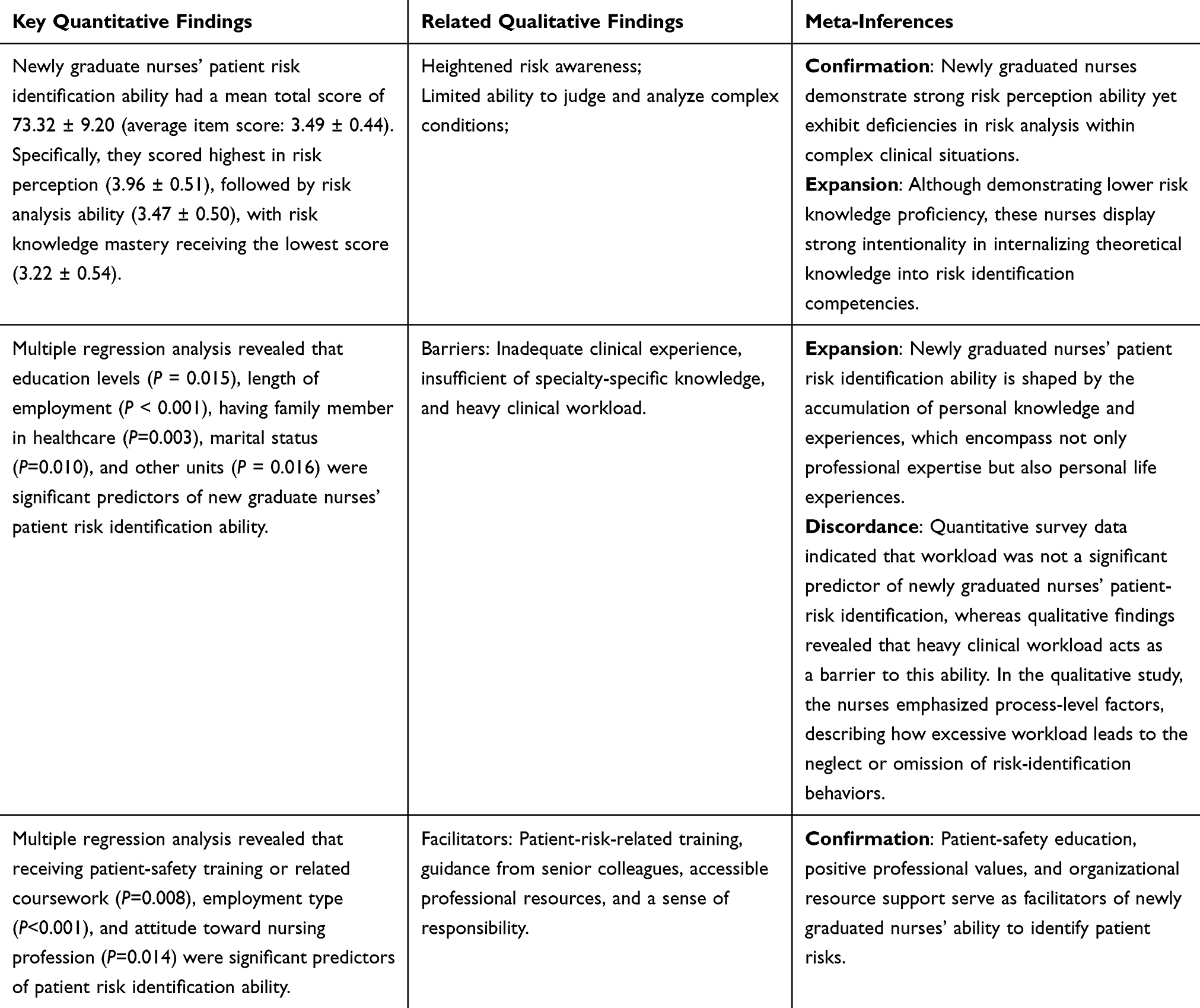 |
Table 4 Integration of Quantitative and Qualitative Findings to Facilitate Mixed Methods Meta-Inferences |
Discussion
In this study, quantitative findings indicate that newly graduated nurses self-reported a patient risk identification ability score of 73.32 ± 9.20, which was higher than that of nursing interns (54.29 ± 6.37)30 and lower than that of experienced nurses (82.79 ± 11.84).15 More specifically, their risk perception ability is relatively strong, while their mastery of risk knowledge and risk analysis abilities are comparatively weaker. Qualitative research findings further support this observation, notably highlighting deficiencies in risk analysis within complex clinical situations. This phenomenon may be attributed to the limited clinical experience of newly graduated nurses, who demonstrate a strong awareness of patient safety but lack adequate clinical preparedness and practical risk knowledge. Willman et al31 similarly indicate that insufficient holistic nursing competence hampers new nurses’ ability to identify changes and deteriorations in patient conditions, particularly when caring for patients with multiple comorbidities or acute changes in condition.32 The strong theoretical internalization observed among new nurses in qualitative studies further corroborates their high cognitive understanding of the importance of risk identification. However, dedicated patient safety courses are still absent from nursing education in Mainland China, with relevant content fragmented across other courses and failing to meet new graduates’ clinical needs.33 Therefore, academic education and clinical training should prioritize addressing gaps in risk knowledge and analysis skills among new graduate nurses through systematically developed patient safety curricula and specialized training programs, working together to advance patient safety education.
Both quantitative and qualitative findings consistently indicate that newly graduated nurses’ patient risk identification ability is influenced by individual knowledge and accumulated experience. Newly graduated nurses with higher education levels, longer employment duration, or those working in core clinical departments demonstrate stronger risk identification abilities, likely due to richer knowledge reserves and clinical experience, consistent with previous research.13,14,16 Clinical experience and knowledge are essential for enabling nurses to discern relevant information, recognize critical cues, and integrate findings to formulate appropriate hypotheses and judgments.34 Studies indicate that extensive clinical experience allows nurses to rapidly identify abnormalities and develop intuitive responses to complex conditions.35,36 Regarding personal knowledge, participants in our quantitative study specifically highlighted limitations in specialized disease knowledge and medication management as constraints on their risk identification competence. Willman et al31 emphasize that newly graduated nurses’ limited clinical competence in complex patient contexts directly jeopardizes care quality and patient safety; furthermore, medication safety management is a critical component of nursing care in such complex cases.37 Therefore, prioritizing the targeted development of newly graduated nurses’ abilities in managing specialized diseases and medication safety is essential. Furthermore, this study also found that newly graduated nurses who had family members in healthcare or who were married demonstrated enhanced risk identification abilities. This may be attributed to the fact that early exposure to medical settings helps acquire tacit risk knowledge,16 while marriage may enhance observational and perspective-taking skills through richer life experience.13 This finding suggests that risk identification ability is not solely influenced by professional knowledge and accumulated experience but is also shaped by personal life experiences.
It is noteworthy that in the qualitative component of this study, heavy clinical workload were identified as a barrier to new nurses’ ability to identify patient risks, a result not reflected in the quantitative component. This discrepancy may relate to new nurses in qualitative interviews placing greater emphasis on influencing factors during the implementation process of risk identification. Dresser et al38 indicate that when ward bed occupancy reaches full capacity, patients with complex conditions, high nurse-to-patient ratios, time constraints, and frequent interruptions can compromise nurses’ capacity to promptly detect and respond to changes in patients’ conditions. Heavy workloads in this study notably limited new graduate nurses’ time for conducting ward rounds, completing basic patient assessments, responding to dynamic patient needs, and monitoring treatment responses. Murray et al18 illustrated that new nurses transitioning into clinical roles often face a dilemma between patient safety and time management, frequently failing to prioritize patients effectively, thereby impairing their ability to integrate patient safety practices into clinical practice. Consequently, clinical nursing managers should comprehensively evaluate both the actual and subjectively perceived workloads of new nurses, implement robust measures to optimize nursing staffing allocation, and carefully consider patient complexity in scheduling.
Patient safety-related education and positive professional values serve as facilitators for new nurses’ patient risk identification abilities. Xiao et al5 demonstrated that receiving safety training and possessing an affinity for nursing work constitute protective factors for nurses’ patient safety competence. Patient safety-related education encompasses formal coursework and specialized training; such instruction enables healthcare staff to master diverse methodologies for detecting and mitigating potential hazards in clinical environments, ultimately enhancing patient safety practices.17 Cho et al39 showed that nurses who have undergone repeated patient safety education achieve higher scores in safety awareness, risk knowledge, and risk attitudes. Given the critical importance of patient safety education, it remains essential to explore innovative pedagogical approaches. Integrating traditional centralized training with innovative formats—such as case studies and scenario simulations—can strengthen nurses’ capacity for comprehensive clinical analysis and effective risk judgment in complex situations.5 Professional values significantly influence nurses’ decision-making processes and care quality.40 In this study, a stronger risk identification ability correlated with more positive professional attitudes among new graduates. This relationship may arise from the proactive assumption of patient safety responsibilities driven by such attitudes. Crucially, this sense of responsibility motivates increased vigilance toward patients’ therapeutic progress and clinical changes while fostering greater self-efficacy through self-directed learning and reflective practice.5,38,41 These findings underscore the necessity for sustained cultivation of professional values throughout nursing education and career development.
Organizational resource support contributes to enhancing newly graduated nurses’ risk identification abilities. Such support resources include mentorship programs, guidance from experienced supervisors, professional risk assessment tools, collaborative communication with specialized nurses and physician teams, and the security of permanent positions. These components align with the staff education, incident evaluation, teamwork, and personnel management dimensions of the Manchester Patient Safety Framework.42 Additional evidence indicates that translating risk identification into measurable reductions in hospital error requires a shift toward an inclusive safety culture among all staff.17 Thus, improving nurses’ risk identification ability requires multidimensional intervention strategies that integrate staff education, teamwork, and employee support to collectively build organizational safety culture.
Limitations
Participants in this study were newly graduated nurses from only two universities in Hunan Province, which limits the geographic and institutional representativeness of the sample. Additionally, the qualitative component carries inherent limitations, such as potential bias in the recruitment of interviewees. These factors may restrict the generalizability of the findings to all newly graduated nurses. Further empirical studies on this topic are warranted; future research should encompass a larger sample size from diverse regions and healthcare institutions. Regarding variable measurement, workload was assessed solely through rough self-evaluation without the use of specialized scales, which might affect the results of the research. Furthermore, the study did not fully account for the potential influence of intrinsic individual traits (such as personality) and cognitive-behavioral variables on risk recognition ability at the personal level.
Conclusion
This mixed-methods study reveals the current status and key influencing factors of patient risk identification ability among newly graduated nurses. The patient risk identification ability of newly graduated nurses still has substantial room for improvement. Although they show relatively strong awareness in identifying patient risks, notable deficiencies persist in their mastery of risk-related knowledge and in the risk analysis of complex clinical situations. Their risk identification ability is influenced by multiple factors, including individual-level factors (personal knowledge and accumulated experience, professional values) and organizational-level factors (workloads, patient safety education, and organizational resource support). Therefore, systematically developed patient safety courses and specialized training programs should be implemented, with an emphasis on introducing innovative teaching methods to strengthen newly graduated nurses’ risk analysis and knowledge application skills, as well as fostering professional values to enhance their professional commitment and sense of responsibility. At the organizational support level, it is necessary to optimize the allocation of nursing human resources and actively build an organizational safety culture centered on teamwork, continuous learning, and open communication.
Abbreviations
VIF, Variance Inflation Factor.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Xiangnan University (No. 2023YXLL025). All research procedures in this study were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained from all participants involved in both the quantitative and qualitative phases of the study, and this consent included permission for the publication of anonymized responses and direct quotes.
Acknowledgments
The authors would like to thank the participants for their support and cooperation in this study.
Funding
This study was supported by the General Research Project of the Hunan Provincial Social Sciences Achievements Evaluation Committee (grant no. XSP25YBC494) and Hunan Province Undergraduate Innovation and Entrepreneurship Training Program (grant no. S202510545100).
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Ammouri AA, AK T, Muliira JK, Geethakrishnan R, Al Kindi SN. Patient safety culture among nurses. Int Nurs Rev. 2015;62(1):102–14. doi:10.1111/inr.12159
2. Park JH, NJ L, Lee H, Park G. Determinants of clinical nurses’ patient safety competence: a systematic review protocol. BMJ Open. 2024;14(8):e080038. doi:10.1136/bmjopen-2023-080038
3. Wu C, Zhang W, Shang L, Wang R, Lu X. Preliminary construction of an indicator system for nurses’ patient risk identification ability. Chin Med Innov. 2016;13(27):64–67.
4. Simsekler MCE, Gurses AP, Smith BE, Ozonoff A. Integration of multiple methods in identifying patient safety risks. Safety Science. 2019;118:530–537. doi:10.1016/j.ssci.2019.05.057
5. Xiao Q, Huang X, Ren X, Wen X, Zhao Y. Analysis of the current status and influencing factors of nurses’ patient safety competence: a potential profile analysis. Front Med. 2024;11:1481261. doi:10.3389/fmed.2024.1481261
6. Frank JR, Brien S. The Safety Competencies: Enhancing Patient Safety Across the Health Professions. Ottawa, ON: Canadian Patient Safety Institute; 2008.
7. Wang Q. Development of the Patient Safety Competency Nurse Evaluation Scale[Dissertation]. Peking Union Medical College; 2018.
8. Hwang JI. What are hospital nurses’ strengths and weaknesses in patient safety competence? Findings from three Korean hospitals. Int. J Qual Health Care. 2015;27(3):232–238. doi:10.1093/intqhc/mzv027
9. Wen X, Chu X, Zeng W, Lü M, Wang J. Meta analysis on influencing factors of clinical nurses’ safety competency for patients. Health Vocat Educ. 2024;42(22):121–126.
10. Boamah SA, Spence Laschinger HK, Wong C, Clarke S. Effect of transformational leadership on job satisfaction and patient safety outcomes. Nurs Outlook. 2018;66(2):180–189. doi:10.1016/j.outlook.2017.10.004
11. Forbes TH, Scott ES, Swanson M. New graduate nurses’ perceptions of patient safety: describing and comparing responses with experienced nurses. J Contin Educ Nurs. 2020;51(7):309–315. doi:10.3928/00220124-20200611-06
12. Chipps E, Wills CE, Tanda R, et al. Registered nurses’ judgments of the classification and risk level of patient care errors. J Nurs Care Qual. 2011;26(4):302–310. doi:10.1097/NCQ.0b013e31820f4c57
13. Wu C. Preliminary study on evaluation index system of nurses’ ability to identify patient risks [Dissertation]. Shanxi Medical University; 2016.
14. Du J, Feng Y, Niu J, Yang C, Yan H, Zhang Y. Analysis on the status quo and influencing factors of patients’ risk identification ability of cardiology nurses in general hospitals of Shandong province. Evid Based Nurs. 2022;8(20):2836–2840.
15. Nie C, Chen M, Feng W, Zha Q, Huang Q. Analysis of nurses’ nursing risk identification ability and influencing factors of cognition on structured nursing risk assessment system. Mod Med Health. 2020;36(22):3661–3664.
16. Jiang H, Zhang J. Study on current status of intern nursing students’ ability to identify patients’ risk and its influencing factors. Chin Nurs Res. 2020;34(4):621–624.
17. Simsekler MCE. The link between healthcare risk identification and patient safety culture. Int J Health Care Qual Assur. 2019;32(3):574–587. doi:10.1108/IJHCQA-04-2018-0098
18. Murray M, Sundin D, Cope V. New graduate registered nurses’ knowledge of patient safety and practice: a literature review. J. Clin Nurs. 2018;27(1–2):31–47. doi:10.1111/jocn.13785
19. Lavoie P, Pepin J, Boyer L. Reflective debriefing to promote novice nurses’ clinical judgment after high-fidelity clinical simulation: a pilot test. Dynamics. 2013;24(4):36–41.
20. Levett-Jones T, Hoffman K, Dempsey J, et al. The ‘five rights’ of clinical reasoning: an educational model to enhance nursing students’ ability to identify and manage clinically ‘at risk’ patients. Nurse Educ Today. 2010;30(6):515–520. doi:10.1016/j.nedt.2009.10.020
21. Chua WL, Legido-Quigley H, Ng PY, McKenna L, Hassan NB, Liaw SY. Seeing the whole picture in enrolled and registered nurses’ experiences in recognizing clinical deterioration in general ward patients: a qualitative study. Int J Nurs Stud. 2019;95:56–64. doi:10.1016/j.ijnurstu.2019.04.012
22. Labrague LJ, De Los Santos JAA. Transition shock and newly graduated nurses’job outcomes and select patient outcomes:a cross sectional study. J Nurs Manag. 2020;28(5):1070–1079. doi:10.1111/jonm.13033
23. Kavanagh JM, Sharpnack P. Crisis in competency: a defining moment in nursing education. Online J Issues Nurs. 2021;26(1). doi:10.3912/OJIN.Vol26No01Man02
24. Creswell JW, Plano Clark VL. Designing and Conducting Mixed Methods Research.
25. Xie A, Chen J. Sample size determination of qualitative studies - the concept, operation, and controversy of saturation. J East Chin Norm Univ Educ Sci. 2021;39(12):15–27.
26. Steffen MW, Murad MH, Hays JT, et al. Self-report of tobacco use status: comparison of paper-based questionnaire, online questionnaire, and direct face-to-face interview--implications for meaningful. Use Popul Health Manag. 2014;17(3):185–189. doi:10.1089/pop.2013.0051
27. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
28. Lincoln YS, Guba EG. Naturalistic Inquiry.
29. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6):2134–2156. doi:10.1111/1475-6773.12117
30. Meng L, He L, Ouyang L, Fu M, Li P, He Y. Factors associated with management of workplace violence competence among Chinese nursing interns. Risk Manag Healthc Policy. 2025;18:33–42. doi:10.2147/RMHP.S491989
31. Willman A, Bjuresäter K, Nilsson J. Insufficiently supported in handling responsibility and demands: findings from a qualitative study of newly graduated nurses. J Clin Nurs. 2021;30(1–2):83–92. doi:10.1111/jocn.15483
32. Gellerstedt L, Moquist A, Roos A, Karin B, Åg C. Newly graduated nurses’ experiences of a trainee programme regarding the introduction process and leadership in a hospital setting-A qualitative interview study. J. Clin Nurs. 2019;28(9–10):1685–1694. doi:10.1111/jocn.14733
33. Huang FF, Shen XY, Chen XL, He LP, Huang SF, Li JX. Self-reported confidence in patient safety competencies among Chinese nursing students: a multi-site cross-sectional survey. BMC Med Educ. 2020;20(1):32. doi:10.1186/s12909-020-1945-8
34. Mohamed Bayoumy H, Albeladi GA. Clinical judgment skills among junior-level nursing students enrolled in adult health nursing courses: errors and risk level classification. Nurse Educ Pract. 2020;48:102888. doi:10.1016/j.nepr.2020.102888
35. Astroth KS, Woith WM, Stapleton SJ, Degitz RJ, Jenkins SH. Qualitative exploration of nurses’ decisions to activate rapid response teams. J. Clin Nurs. 2013;22(19–20):2876–2882. doi:10.1111/jocn.12067
36. Brier J, Carolyn M, Haverly M, et al. Knowing ‘something is not right’ is beyond intuition: development of a clinical algorithm to enhance surveillance and assist nurses to organise and communicate clinical findings. J Clin Nurs. 2015;24(5–6):832–843. doi:10.1111/jocn.12670
37. Willman A, Bjuresäter K, Nilsson J. Newly graduated nurses’ clinical competencies and need for further training in acute care hospitals. J Clin Nurs. 2020;29(13–14):2209–2220. doi:10.1111/jocn.15207
38. Dresser S, Teel C, Peltzer J. Frontline Nurses’ clinical judgment in recognizing, understanding, and responding to patient deterioration: a qualitative study. Int. J Nurs Stud. 2023;139:104436. doi:10.1016/j.ijnurstu.2023.104436
39. Cho OH, Lee D, Hwang KH. Patient safety awareness, knowledge and attitude about fire risk assessment during time-out among perioperative nurses in Korea. Nurs Open. 2022;9(2):1353–1361. doi:10.1002/nop2.1180
40. Hlebichuk J, Lancaster R, Tuzik Micek W, Perusich S, Fick K, Perumalswamy K. Exploring nurses’ personal and professional values and care quality: a convergent mixed-methods analysis. West J Nurs Res. 2025;47(2):61–70. doi:10.1177/01939459241304528
41. Sümen A, Ünal A, Teskereci G, et al. The relationship between nursing students’ professional attitudes and caring behaviors: a cross-sectional study. Perspect. Psychiatr Care. 2022;58(3):1103–1111.
42. Parker D. Managing risk in healthcare: understanding your safety culture using the Manchester Patient Safety Framework (MaPSaF). J Nurs Manag. 2009;17(2):218–222. doi:10.1111/j.1365-2834.2009.00993.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between Patient Safety Culture and Accreditation at Primary Care Centers in Kuwait: A Country-Wide Multi-Method Study
ALFadhalah T, Al Mudaf B, Al Salem G, Alghanim HA, Abdelsalam N, El Najjar E, Abdelwahab HM, Elamir H
Risk Management and Healthcare Policy 2022, 15:2155-2169
Published Date: 22 November 2022
A Systematic Literature Review of Safety Culture in Hemodialysis Settings
Albreiki S, Alqaryuti A, Alameri T, Aljneibi A, Simsekler MCE, Anwar S, Lentine KL
Journal of Multidisciplinary Healthcare 2023, 16:1011-1022
Published Date: 11 April 2023
Patient Safety Culture, Infection Prevention, and Patient Safety in the Operating Room: Health Workers’ Perspective
Juliasih NN, Dhamanti I, Semita IN, Wartiningsih M, Mahmudah M, Yakub F
Risk Management and Healthcare Policy 2023, 16:1731-1738
Published Date: 4 September 2023
The Association of Transformational Leadership on Safety Practices Among Nurses: The Mediating Role of Patient Safety Culture
Hamdan M, Jaaffar AH, Khraisat O, Issa MR, Jarrar M
Risk Management and Healthcare Policy 2024, 17:1687-1700
Published Date: 26 June 2024
Shaping Safety: Unveiling the Dynamics of Incident Reporting and Safety Culture in Saudi Arabian Healthcare
Alsahli H, Al-Wathinani AM, Althobaiti TA, Abahussain MA, Goniewicz K
Journal of Multidisciplinary Healthcare 2024, 17:3775-3789
Published Date: 6 August 2024