")
Back to Journals » Pragmatic and Observational Research » Volume 11
Patient, Rheumatologist and Therapist Perspectives on the Implementation of an Allied Health Rheumatology Triage (AHRT) Initiative in Ontario Rheumatology Clinics
Authors Fullerton LM, Brooks S , Sweezie R, Ahluwalia V, Bombardier C, Gagliardi AR
Received 8 May 2019
Accepted for publication 15 October 2019
Published 28 January 2020 Volume 2020:11 Pages 1—12
DOI https://doi.org/10.2147/POR.S213966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Laura M Fullerton,1 Sydney Brooks,2 Raquel Sweezie,2 Vandana Ahluwalia,3 Claire Bombardier,4 Anna R Gagliardi4
1Ontario Best Practices Research Initiative, Toronto General Research Institute, Toronto, ON, Canada; 2Ontario Division, Arthritis Society, Toronto, ON, Canada; 3Department of Rheumatology, William Osler Health System, Brampton, ON, Canada; 4Toronto General Research Institute, University of Toronto, Toronto, ON, Canada
Correspondence: Sydney Brooks
Arthritis Society, 393 University Avenue, Suite 1700, Toronto M5G 3E6, Canada
Tel +416 979-7228
Fax +416 979-8366
Email [email protected]
Purpose: The objective of this qualitative study was to explore patient, rheumatologist, and extended role practitioner (ERP) perspectives on the integration of an allied health rheumatology triage (AHRT) intervention in Ontario rheumatology clinics. Triage is the process of identifying the urgency of a patient’s condition to ensure they receive specialist care within an appropriate length of time. This research explores the clinical/logistical impact of triage by occupational and physical therapists with advanced arthritis training (ERPs), including facilitators and barriers of success, and recommendations for future application.
Participants and Methods: Semi-structured telephone interviews were held with participating rheumatologists, ERPs, and a sample of patients from each clinical site (4 community, 3 hospital) in five Ontario cities. Interviews were audio-recorded and transcribed verbatim. Transcripts were analyzed using basic qualitative description. Two independent researchers compared coding and achieved consensus.
Results: Patients (n=10), rheumatologists (n=6), and ERPs (n=5) participated in the study and reported reduced wait-times to rheumatology care, diagnosis, and treatment for those with inflammatory arthritis (IA). Rheumatologists and ERPs perceived that the intervention improved clinical efficiency and quality of care. Patients reported high satisfaction with ERP assessments, valuing early joint examination/laboratory tests, urgent referral if needed, and the provision of information, support, and management strategies. Facilitators of success included: supportive clinical staff, regular communication and collaboration between rheumatologist and ERP, and sufficient clinical space. Recommendations included extending ERP roles to include stable patient follow-up, and ERP care between scheduled rheumatology appointments.
Conclusion: Findings support the integration of ERPs in a triage role in the community and hospital-based rheumatology models of care. Future research is needed to explore the impact of utilizing ERPs for stable patient follow-up in rheumatology settings.
Keywords: health service needs and demand, rheumatic diseases, connective tissue disease, patient satisfaction
Plain Language Summary
Some types of arthritis, such as inflammatory arthritis (IA), progress rapidly and can cause joint destruction resulting in loss of function and affecting a person’s ability to work and enjoy life. Early diagnosis and treatment are important however many people still wait over 6 months to see an arthritis specialist (rheumatologist) and start appropriate treatment. In this study, occupational and physical therapists with advanced training in arthritis care assessed patients on rheumatologists’ waitlists and identified those requiring urgent care for an early rheumatologist appointment. The team then interviewed 23 patients, rheumatologists, and therapists to explore the benefit of this new approach to care. Patients reported high satisfaction with the therapists’ assessments, valuing: early joint assessment and laboratory tests, urgent referral if needed, education and support. Patients, rheumatologists, and therapists perceived reduced wait-times to care. Rheumatologists and therapists believed that the model improved office efficiency and quality of care. Our findings support the inclusion of therapists with advanced training into Ontario rheumatology clinics.
Introduction
Inflammatory Arthritis (IA) is a rapidly progressing joint disease affecting approximately 3% of the population and causing significant burden through progressive joint destruction, disability, lost work productivity, and premature mortality.1–3 With an aging population, rates of IA and other rheumatic conditions are on the rise, placing increased pressure on an already overloaded rheumatology care system.4,5
While the established benchmark time from referral to seeing a rheumatologist is 4 weeks, only 35–38% of patients with IA in Ontario are seen within this timeframe,6 and fewer than 50% receive treatment with a disease-modifying anti-rheumatic drug (DMARD) within 6 months of symptom-onset.7 Reducing wait-times to rheumatology care is important for individuals with IA, as early and aggressive treatment with traditional and/or biologic DMARDs can induce remission, prevent irreversible joint damage and long-term disability8,9 and reduce long-term costs.10 For example, according to the Arthritis Alliance of Canada, the early diagnosis and treatment of rheumatoid arthritis (the most common type of IA) with a DMARD or biologic could result in $5 billion of savings in direct costs (and up to $34 billion for indirect costs) in Canada over the next 30 years.5
To cope with higher patient volumes and meet recommended benchmarks for care, health system changes are needed to ensure those requiring urgent care are identified and treated without delay. One way to reduce wait-times is to enhance the efficiency of patient triage.11 Triage is the process of identifying the urgency of a patient’s condition to ensure they receive specialist care within an appropriate length of time.
Advanced Clinician Practitioners in Arthritis Care (ACPAC) are experienced physical therapists (PTs), occupational therapists (OTs), or nurses with specialized post-licensure training in joint examination and the management of IA. As extended role practitioners (ERPs), ACPAC therapists can work beyond their normal scope of practice, often in non-traditional roles or under medical directives to assess, diagnose, triage, and manage patients with IA. The ACPAC program (https://acpacprogram.ca/) was developed by St. Michael’s Hospital and the Hospital for Sick Children as a university-based curriculum to address shortages in rheumatology care, improve clinical efficiency, and reduce wait-times to specialty care for patients with arthritis and MSK conditions.12 Since its inception in 2005, 90 professionals have achieved ACPAC certification.
The ACPAC program is based on an inter-professional collaborative model, which can improve clinical efficiency and quality of care by enabling health professionals to work in their highest capacity.13,14 Inter-professional collaboration has been shown to improve health service coordination, resource use, access to care, and clinical outcomes,15,16 while reducing clinical errors, tension among care providers, length of hospitalization, and health-related complications.15–17 Improving health service integration can help mitigate negative outcomes of an overwhelmed system (i.e, excessive wait-times) through the reallocation of resources and careful distribution of clinical expertise.14 Allied health professionals have been utilized in primary care and rheumatology settings to improve clinical efficiency and access to care,18–21 however, few studies have looked at system level outcomes such as rheumatology wait times. In addition, most studies examining triage interventions involve a single ERP working with a single rheumatologist, limiting the generalization of results. A recent study examined the impact of triage by Arthritis Society ACPAC-trained occupational and physical therapists in several Ontario rheumatology clinics and found a significant reduction in wait times (improved access to rheumatology consultation and treatment).22 This qualitative study evaluates the impact of this intervention from the perspectives of the participating patients, rheumatologists and ERPs.
Methods
Approach
The following PICO framework applies:23 Population: rheumatologists, ERPs, patients; Intervention: triage performed by ERPs within rheumatology clinical settings; Comparison: experiences with intervention compared among and between population groups (ERPs, rheumatologists and patients; those expedited and those not expedited); Outcome(s): satisfaction, acceptability and perceived impact of intervention, facilitators and barriers of success, recommendations for future implementation.
Qualitative data were collected using semi-structured telephone interviews. The basic qualitative description was employed, as interviews were not meant to generate theory, but to generate factual information about the experience and satisfaction of research participants with the study intervention.24 The basic qualitative description focuses on the clear description and comprehensive communication of research phenomena, in this case, experiences with the triage intervention.24 The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist25 was used to ensure qualitative procedures were followed. Ethics approval was obtained from the University Health Network (#15-9130-AE); Queen’s University; St. Joseph’s Care Group and Sunnybrook Health Sciences Centre. All participants provided written informed consent before being interviewed. Access to qualitative data is available from the author on request. Quantitative results on time to diagnosis/treatment for patients with IA are published elsewhere.22
Setting
At each clinical site, an ACPAC-trained ERP worked in a triage role one day/week to improve access to rheumatologists for people with suspected IA. Patients were assessed by an ERP if their primary care referral contained insufficient information for the rheumatologist to make an informed triage decision. The ERP captured demographic information, a chief complaint, a brief medical history, systems review and functional status. ERPs provided care within their scope of practice, had access to electronic medical records, and the ability to order laboratory tests/imaging under medical directives. They performed a full joint count (tender and swollen joints), provided education and made conservative treatment recommendations that included referrals to community programs and services, as needed. ERPs then made one or more differential diagnoses and a triage decision (ie, expedited referral to the rheumatologist [within 2 weeks] or the next available appointment [routine care]). Patients with possible IA/SARD, defined as polyarthritis with functional impairment, poorly controlled gout, polymyalgia rheumatica, connective tissue disease, temporal arteritis or systemic vasculitis, were expedited. When unsure, ERPs were advised to expedite.
Sampling and Recruitment
Rheumatologists & ERP
To be eligible for participation, rheumatologists agreed to integrate an ERP into their clinic one day/week for the study duration, allow for a retrospective chart review, complete a site agreement for data sharing, delegate labs/imaging to ERPs using medical directives and complete a half-day training session in Toronto. Eligibility criteria for ERPs included current employment with the Arthritis Society as an ACPAC-trained OT or PT, agreement to provide patient joint assessments in their assigned rheumatology clinic one day/week for the study duration, and the completion of a half-day training session in Toronto. Rheumatologists were recruited for participation through the Ontario Rheumatology Association, while ERPs were recruited through the Arthritis Society. Rheumatologists and ERPs had no pre-existing relationship prior to the intervention. ERPs were paid their usual salary. Rheumatologists billed for their time as usual. All participating rheumatologists and ERPs were invited to participate in an interview following the completion of the intervention at their clinical site.
Patients
To be eligible, patients had to be 18+ years of age, have the potential for an IA based on paper triage information (determined by rheumatologist), and be referred to a rheumatologist by a general practitioner or nurse practitioner within the previous month. Patients were excluded if they were referred by other specialists or an emergency department, had seen a rheumatologist in the past 5 years, had a pre-existing diagnosis of osteoarthritis, fibromyalgia, or IA, or were already on a DMARD. Once identified by the rheumatologist, office clerical staff called the patient to explain the study. If the patient was interested, the research coordinator (RS) called the patient to provide greater details. If still interested, an appointment was booked with the ERP and a consent form was mailed to the patient to sign and bring to the ERP visit. The consent included that the patient was willing for a researcher to call them to arrange an interview following the triage intervention.
In total, 218 patients were examined by an ERP, of which 106 were expedited to see their rheumatologist. Six months following the triage intervention, a random sample of 4–8 patients from each clinical site were invited to participate in an interview. Purposive sampling was applied to ensure sample diversity with respect to age, triage decision (expedited vs non-expedited), type of clinical site (community vs hospital), and clinical site (all sites represented). After the triage intervention, a qualitative researcher (LF), unknown to study participants, called the patient to explain the study, Consent forms were mailed to interested patients, and when returned, interviews were scheduled. Patient sampling occurred until thematic saturation (the emergence of no new content/themes) was achieved.
Data Collection
Participants were informed about the purpose of the research and asked to provide feedback on their experience with the intervention, feelings about its impact/implementation, satisfaction, and opportunities for improvement. One-on-one interviews were 30–50 mins in length and took place between December 15, 2015 and August 15, 2016. Interviews were conducted by telephone and facilitated by an independent qualitative interviewer (PV) who had an MHSc in Health Promotion and over 20 years’ experience in conducting qualitative research. She was unknown to participants and utilized solely for interview facilitation. A semi-structured interview guide was used for all interviews (Appendix 1). The general themes for the guide were developed by the research team based on comments we had heard back from participating rheumatologists and ERPs and were informed by the literature. Interviews were audio-recorded and transcribed verbatim using a professional transcription service. All identifying information was removed to protect confidentiality.
Data Analysis
Interview transcripts were analyzed using basic qualitative description. Unique themes were identified in an inductive manner using the constant comparative technique.26 One master's level (LF) and one senior PhD level (AG) university-based qualitative researcher were responsible for the analyses. Transcripts were read by LF and AG to identify, define, and organize themes (first-level coding). A codebook was used to capture emerging codes, their definition, and sample data illustrating each code. Transcripts were reviewed by LF to identify all instances that matched and did not match the coding framework to assess whether to expand or merge thematic codes (second-level coding).LF and AG independently reviewed second-level coding, discussed themes/sub-themes, removed redundancies, and achieved consensus. Data were tabulated by theme and clinical site to identify trends and facilitate interpretation. Exemplar quotes were selected to demonstrate each theme/sub-theme. All members of the research team including two qualitative researchers, two rheumatologists, one health systems researcher and one research coordinator (LF, AG, VA, CB, SB, RS) reviewed outcomes and discussed themes and interpretation.
Results
Thirty-five rheumatologists were invited to participate in the study and seven rheumatologists (3 hospital-based, 4 community-based) from five cities met inclusion criteria and agreed to participate (57% female; 57% community-based). Participant characteristics are presented in Table 1. Although there were seven clinical sites, there were five participating ERPs, as two worked in the rheumatology triage role at two separate clinics. These ERPs were interviewed separately for each clinical location, for a total of seven ERP interviews. All ERPs and six of seven rheumatologists participated in an interview. One hospital-based rheumatologist closed her practice and moved out of province mid-way through the intervention for reasons unrelated to the study. Although triage assessments had been completed, patients did not receive the full intervention (appointment with rheumatologist). For this reason, patient and rheumatologist interviews were not conducted at this site. ERP assessments were not impacted by the site closure, so this interview was included.
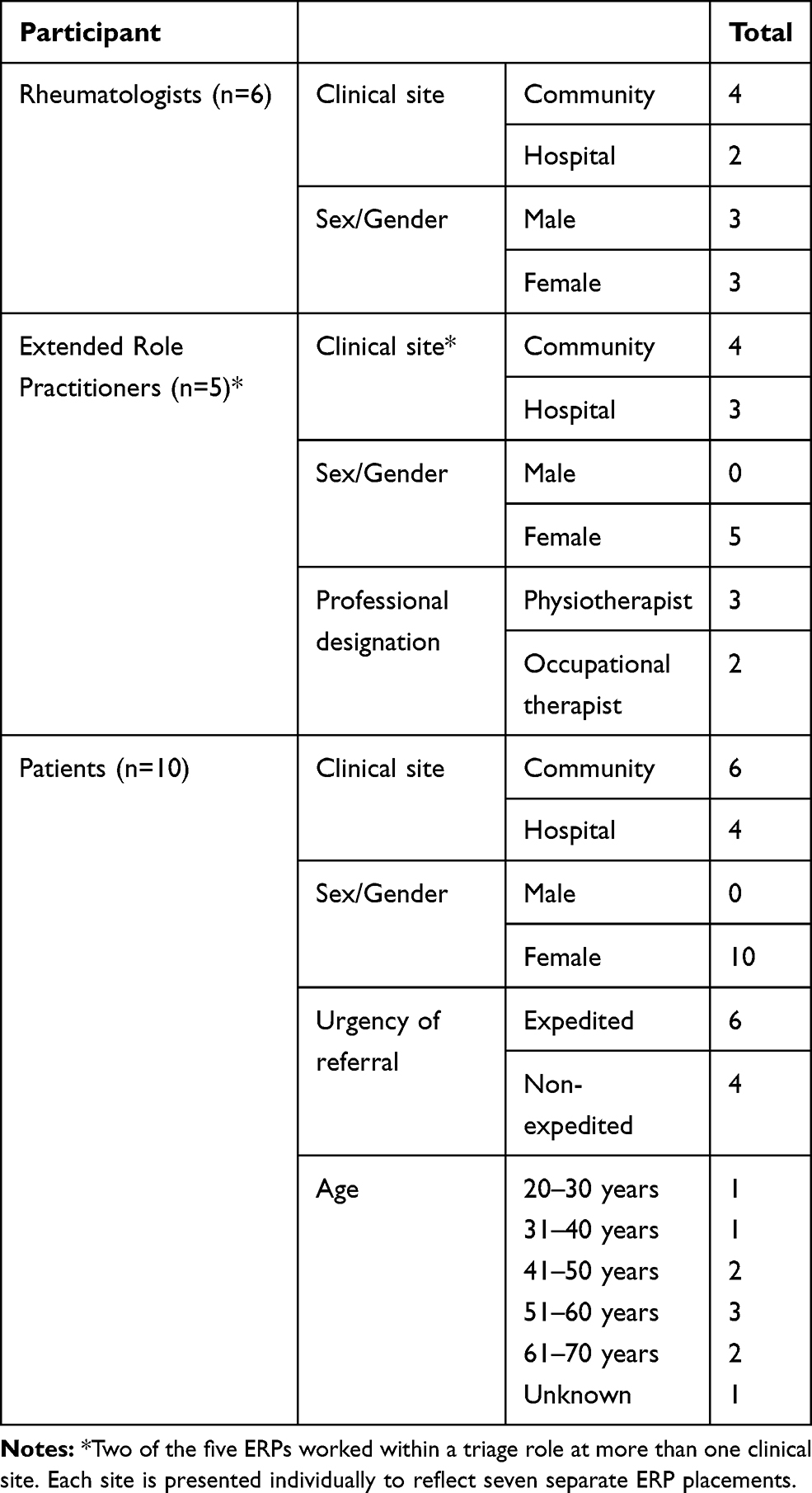 |
Table 1 Participant Characteristics |
Twenty patients were invited to participate in a telephone interview, and 17 expressed interest in participating. Thematic saturation occurred at 10 interviews when researchers determined no new thematic content was emerging from transcripts.
Interview data were organized into four categories reflecting interview topics: (1) motivation for participation, (2) perceived impact of the intervention, (3) facilitators/barriers of implementation, and (4) recommendations for program improvement and future implementation. All themes were derived inductively from interview data, and are presented with exemplar quotes in Table 2, and summarized in the text using quotes. Discrepancies are noted where relevant.
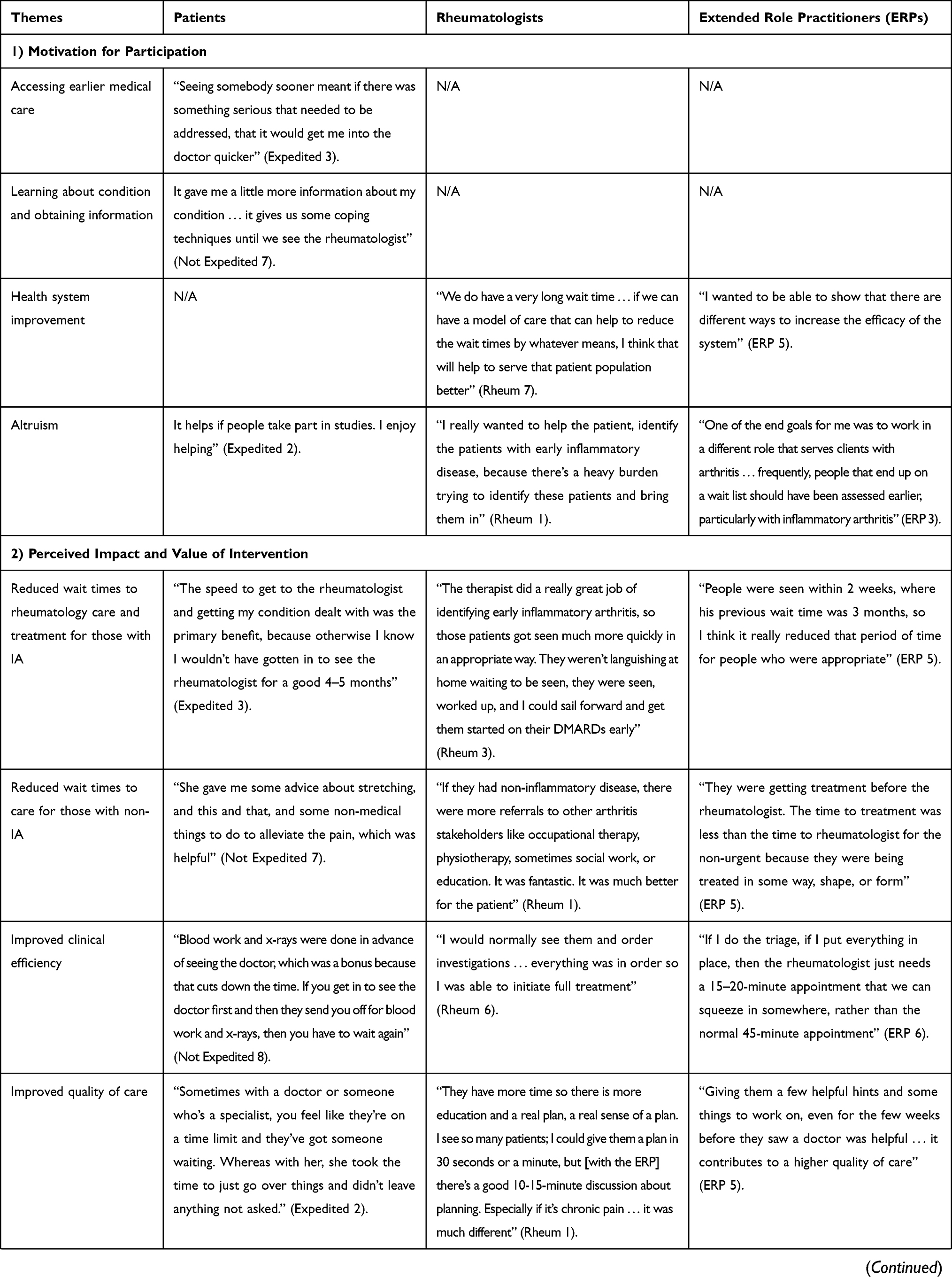 | 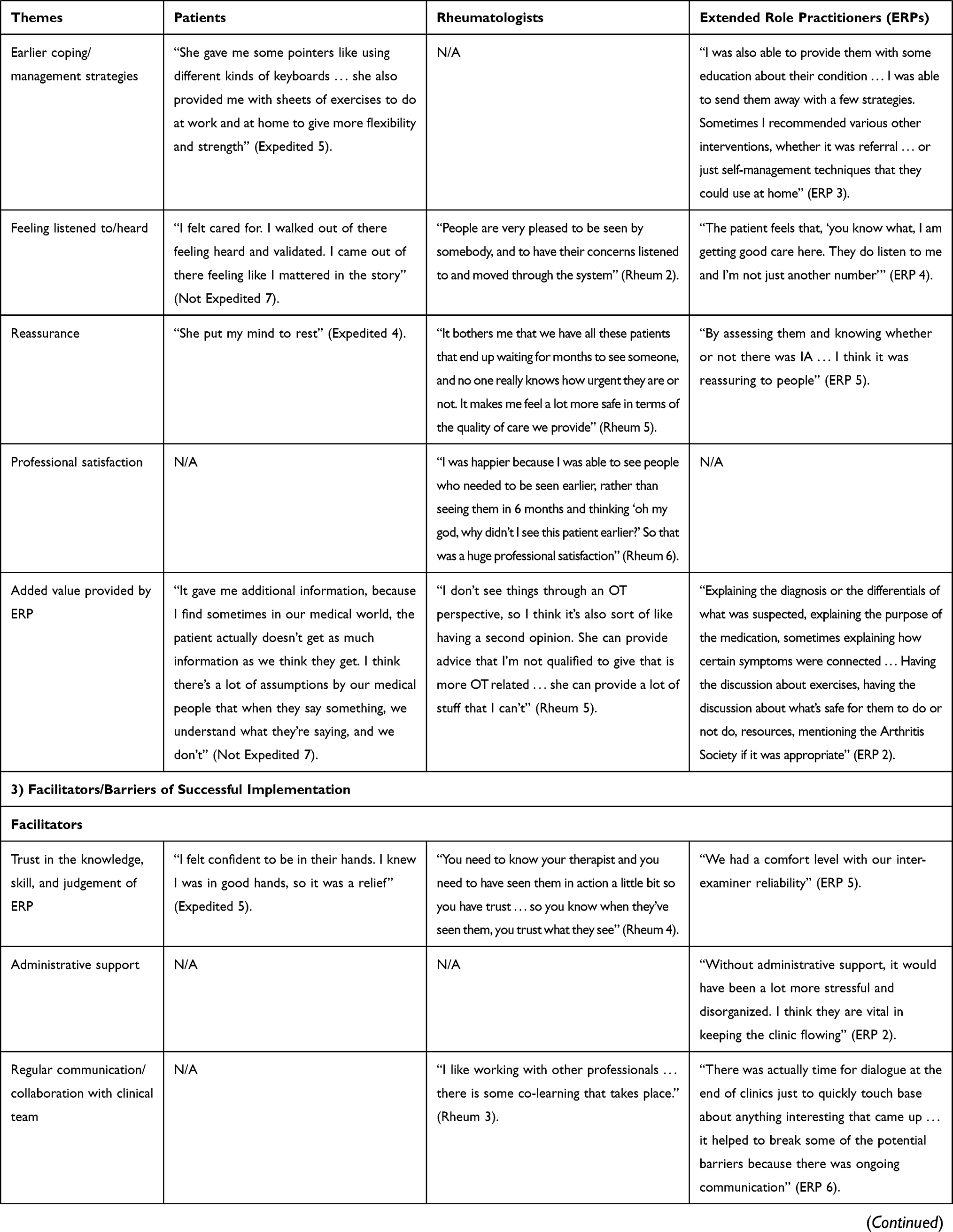 | 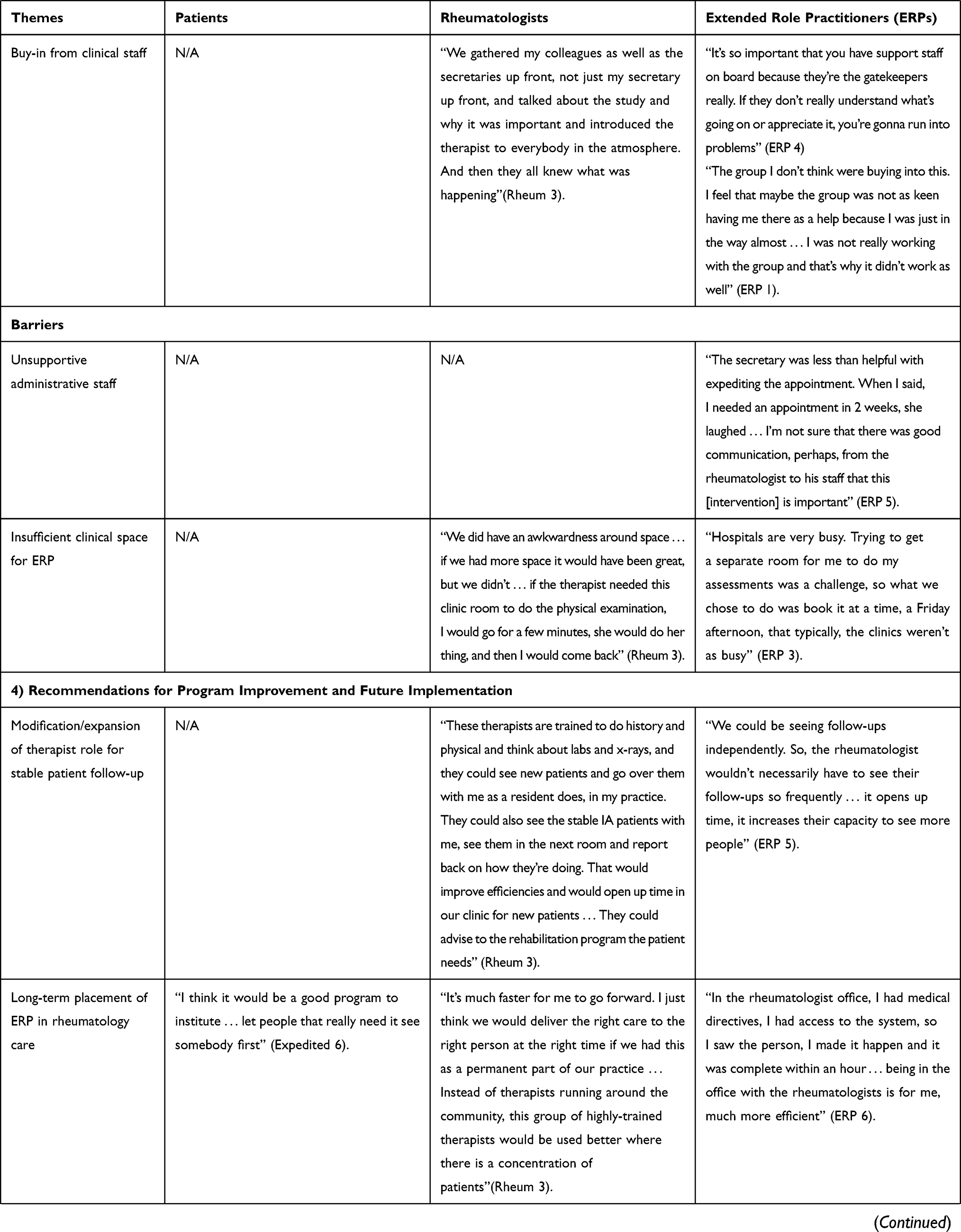 |  |
Table 2 Thematic Categories and Emerging Themes with Exemplar Quotes |
Motivation for Participation
The potential to access earlier rheumatology care was cited by patients as their primary motivator for participation in the intervention. Patients also mentioned the ability to learn about their medical condition and obtain useful information as strong motivators for participation.
Rheumatologists and ERPs reported a desire for health system improvement focused on reducing rheumatology wait-times as a primary motivator for participation. As a rheumatologist shared, “If we can have a model of care that can help to reduce the wait-times by whatever means, I think that will help to serve that patient population better” (Rheum 7). Altruism was also a strong motivator, as many expressed a desire to help patients by improving system efficiency.
Impact of Triage Intervention
Patients, rheumatologists and ERPs consistently reported reduced wait-times to rheumatology care, diagnosis, and treatment for urgent patients who received the intervention. An ERP shared, “People were seen within 2 weeks, where his previous wait-time was 3 months, so I think it really reduced that time for people who were appropriate” (ERP 5). Similarly, a rheumatologist stated,
Patients got seen much more quickly and in an appropriate way. They weren’t languishing at home waiting to be seen, they were seen, worked up, and then I could sail forward and get them started on their DMARDs early. (Rheum 3)
Although many patients did not know how long they would have waited for care without the intervention, most expressed belief that their wait-time was reduced.
Wait-times to care were also reported as reduced for non-expedited patients, as they often received some form of care from the ERP before their first appointment with the rheumatologist. An ERP noted,
They were getting treatment before the rheumatologist. The time to treatment was less than the time to rheumatologist for the non-urgent [patient] because they were being treated in some way, shape, or form. (ERP 5)
Surprisingly, in no case was a non-expedited patient unhappy about waiting to see the rheumatologist at the next routine appointment.
All participant groups believed the triage intervention improved clinical efficiency. They noted that the medical history and joint assessment completed by the ERP, along with ordered laboratory tests/imaging, sped up their movement through the system by providing rheumatologists with the information needed to diagnose at the first appointment. As a patient expressed,
Blood work and x-rays were done in advance of seeing the doctor, which was a bonus because that cuts down the time. If you get in to see the doctor first and then they send you off for blood work and x-rays, then you have to wait again. (Non-Expedited, Patient 8)
Rheumatologists and ERPs noted that the triage assessment reduced the length of time needed at the first rheumatology appointment and the total number of appointments needed to diagnose.
Patients consistently reported receiving helpful coping/management strategies and feeling listened to/heard by their ERP. As one stated:
I felt cared for. I walked out of there feeling heard and validated. I came out of there feeling like I mattered in the story… I liked how thorough her examination was, I liked that she took the time to explain things to me, I liked that I was heard. (Non-Expedited, Patient 7)
Participants from each group consistently communicated a belief that the intervention improved the overall quality of care.
Regardless of triage outcome, most patients expressed reassurance after their assessment. Expedited patients were reassured to know they were being seen in a timely manner, while non-expedited patients were reassured that their condition was not too serious. Rheumatologists reported feelings of reassurance and improved professional satisfaction, as they trusted that urgent patients were being identified and seen in a timely manner.
Facilitators and Barriers of Success
Trust in the knowledge, skill, and judgement of the ERP was consistently reported by rheumatologists as an important facilitator of program success. In no case was lack of trust in the ERP’s knowledge, skill or judgement raised.
ERPs consistently mentioned administrative support and buy-in from clinical staff as an important facilitator of program success. Those who did not receive adequate administrative support reported its absence as a major barrier to their work, resulting in additional stress and workload related to scheduling and paperwork. Those who reported a lack of buy-in from non-participating clinical staff noted less cooperation/collaboration in the clinic, and a less welcoming work environment.
ERPs emphasized the importance of regular communication and collaboration with the rheumatologist in the clinic. In most cases, frequent interaction and collaboration was the norm; however, where it was lacking, it was raised as a barrier to care. ERPs expressed a desire to ask questions and engage with rheumatologists about cases when needed. Rheumatologists expressed satisfaction with their communication/collaboration with ERPs.
A clinical environment with sufficient space for the ERP was discussed as important for efficiency and the prevention of disruptions to clinical flow. Rheumatologists and ERPs consistently mentioned the need for a designated exam room for triage assessments. Clinical space appeared to be more of a problem in hospital-based rheumatology settings than community settings.
Recommendations for Future
Patients and rheumatologists expressed a desire for the long-term placement of ERPs in rheumatology care settings. A rheumatologist shared:
We could deliver the right care to the right person at the right time if we had this as a permanent part of our practice… instead of therapists running around the community, this group of highly-trained therapists would be used better where there is a concentration of patients. (Rheum 3)
Interestingly, many ERPs recommended ERP placement in primary care settings rather than specialty care. As one stated: “the ideal place for ACPAC would be in a family health team in GP offices, where we could do exactly the same, and then expedite the referral to rheumatology with all the findings” (ERP 7). Although most expressed a desire for placement in primary care, one ERP thought services were better utilized within specialist care: “In the rheumatologist office, I had medical directives, I had access to the system, so I saw the person, I made it happen and it was complete within an hour” (ERP 6). A few participants also recommended the placement of ERPs in underserviced areas.
Modifying/expanding ERP roles to allow for stable patient follow-up and rehabilitation in rheumatology settings was recommended by most rheumatologists and ERPs. An ERP shared:
We could be seeing follow-ups independently. So, the rheumatologist wouldn’t necessarily have to see their follow-ups so frequently… it opens up time, it increases their capacity to see more people. (ERP 5)
There was widespread agreement that ERP roles could include stable patient follow-up and rehabilitation.
When asked about future recommendations, a few patients suggested an ability to see/contact the ERP after their assessment and/or between routine rheumatology appointments for additional follow-up care and information. A few ERPs also recommended the option of additional follow-up with patients. The vast majority of patients indicated they would not change anything about their care.
Discussion
This research is the first known study to explore patient, rheumatologist, and ERP perspectives on the integration of ACPAC-trained ERPs in a triage role in Canadian rheumatology clinics. Results suggest that ACPAC-trained ERPs were effectively able to reduce wait-times to rheumatology care, diagnosis, and treatment for patients with IA. Improved clinical efficiency was widely reported by all participant groups, as ERP history-taking, joint assessment, and lab and imaging orders appeared to reduce the length of time required by the rheumatologist at the first appointment, and the number of visits required to diagnose/treat patients. Finally, feedback on the type and quality of care received suggests ERPs added value to the rheumatology model of care by providing information and resources that would otherwise have not been provided.
Results compare favorably with research exploring the impact of integrating ACPAC-trained ERPs into MSK models of care. When placed in a range of inter-professional settings, rheumatologists, clinicians, and administrators found ERPs to be clinically competent, effective at triaging urgent patients, reducing wait-times, and improving clinical efficiency by reducing multiple patient visits.27 Similarly, previous assessments of patient satisfaction with ERPs show high satisfaction with the quality of care and wait-times.28
Lack of administrative support/buy-in from clinical staff and regular communication between rheumatologists and ERPs were raised as barriers to optimal implementation. It is not uncommon for ERPs to encounter barriers related to role recognition and acceptance by health care practitioners, as professional culture and inter-professional competition can affect successful integration in clinical practice.27 Research on optimal features of MSK triage identifies multidisciplinary support as critical for efficient patient triage.29 Effective teamwork requires shared goals and ongoing collaboration, participation, conflict resolution, and support for innovation,15,30 highlighting the importance of engaging stakeholders, including administrative personnel, in the integration of new team members into clinical practice. Training as a team, strategic planning, and identifying roles/responsibilities are recommended to remove barriers and promote collaboration.16
While opinions differed on the optimal placement of ERPs for patient triage (primary vs specialty care) our findings suggest placement in specialty care as both effective and appropriate. Although primary care settings may be more appropriate for the management of patients with osteoarthritis and MSK conditions that do not require specialty care, triage for IA in settings where IA is rare may under-utilize ERP resources.
Although ACPAC-trained ERPs were used solely for triage in this research, they are highly trained professionals who could work within a broader capacity in rheumatology and other clinical settings. Research exploring ERP utilization for stable patient follow-up in rheumatology settings and in novel roles that offer comprehensive and holistic care to patients (education, rehab, co-morbidity management, etc.) is recommended. Research is also needed to assess the costs of integrating ERPs within a publicly funded health care system.
The following study limitations apply: (I) research was conducted as a short-term (9-month) pilot initiative; (II) rheumatologists participating in this research did so voluntarily and may have greater acceptance/desire to work with ERPs, or an enhanced willingness to innovate practice; (III) patients participating in a qualitative interview did so voluntarily, which may select for positive experience; (IV) the need to re-consent patients for qualitative research at each clinical site delayed interviews by 1–3 months, potentially leading to recall bias; (V) all patients interviewed were female, as consent forms from contacted males were not returned within the established timeframe of 4 months post-intervention; (VI) including two interviews for two participating ERPs may have biased the results towards their perspectives; (VII) findings may only be applicable within a Canadian setting. In addition, the introductory questions posed to rheumatologists, ERPs and patients indicating that we were exploring how the project might have reduced rheumatology wait times may have biased the results. However, improvements in access to care (wait times) compared to usual care are substantiated by the quantitative results of this study published elsewhere.22
Conclusion
With specialized training in arthritis care and management, data suggest ACPAC-trained ERPs were able to fill an important role within the medical system by working closely with rheumatologists to ensure patients receive optimal care. Findings support the integration of ACPAC-trained ERPs working within a triage role in community and hospital-based rheumatology settings. These results may have implications nationally and internationally for impacting the delivery of arthritis care. Future research is needed to explore the expansion of ERP roles to include stable-patient follow-up within specialty care, and the optimal placement of ERPs within primary and specialty care.
Acknowledgments
We would like to extend our thanks to the three partner organizations in this project: the Ontario Best Practices Research Initiative including administrative support from Angela Cesta; the Ontario Rheumatology Association including administrative support and coordination from Sandra Couto; and the Arthritis Society (Ed Ziesmann and Joanne Simons). We would also like to thank our qualitative interviewer, Paula Veinot, participating Arthritis Society ERPs (Anne MacLeod, Danielle McCormack, Lynn Richards, Mercedes Reeb, Sue MacQueen), rheumatologists (Drs. Andrew Chow, Angela Montgomery, Art Karasik, Irene Vasiliu, Marie Clements-Baker, Mary Bell, Sanjay Dixit), and patients for their participation in this study. We appreciate the input and guidance from our advisory committee members: Cathy Hofstetter (consumer) and Tiffany Larsen and Angelo Papachristos (ACPAC physical therapists). Financial support for this work was received from the Arthritis Society; the Ontario Rheumatology Association, and the Ontario Best Practices Research Initiative. The study investigators are representatives of these organizations and were involved in all aspects of the study design, implementation and interpretation of the results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allaire S, Wolfe F, Niu J, Lavalley M, Michaud K. Work disability and its economic effect on 55-64-year-old adults with rheumatoid arthritis. Arthritis Rheum. 2005;53(4):603–608. doi:10.1002/(ISSN)1529-0131
2. Escalante A, Haas RW, Del Rincon I. A model of impairment and functional limitation in rheumatoid arthritis. BMC Musculoskelet Disord. 2005;6:16. doi:10.1186/1471-2474-6-16
3. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–656.
4. Widdifield J, Paterson JM, Bernatsky S, et al. The rising burden of rheumatoid arthritis surpasses rheumatology supply in Ontario. Can J Public Health. 2013;104(7):e450–455. doi:10.17269/cjph.104.4115
5. Arthritis Alliance of Canada. The Impact of Arthritis in Canada: Today and Over the Next 30 Years. Toronto:Arthritis Alliance of Canada; 2011.
6. Widdifield J, Bernatsky S, Thorne JC, et al. Wait times to rheumatology care for patients with rheumatic diseases: a data linkage study of primary care electronic medical records and administrative data. CMAJ Open. 2016;4(2):E205–E212. doi:10.9778/cmajo.20150116
7. Tavares R, Pope JE, Tremblay JL, et al. Time to disease-modifying antirheumatic drug treatment in rheumatoid arthritis and its predictors: a national, multicenter, retrospective cohort. J Rheumatol. 2012;39(11):2088–2097. doi:10.3899/jrheum.120100
8. Combe B. Early rheumatoid arthritis: strategies for prevention and management. Best Pract Res Clin Rheumatol. 2007;21(1):27–42. doi:10.1016/j.berh.2006.08.011
9. Courvoisier N, Dougados M, Cantagrel A, et al. Prognostic factors of 10-year radiographic outcome in early rheumatoid arthritis: a prospective study. Arthritis Res Ther. 2008;10(5):R106. doi:10.1186/ar2498
10. Huscher D, Mittendorf T, von Hinuber U, et al. Evolution of cost structures in rheumatoid arthritis over the past decade. Ann Rheum Dis. 2015;74(4):738–745. doi:10.1136/annrheumdis-2013-204311
11. Villeneuve E, Nam JL, Bell MJ, et al. A systematic literature review of strategies promoting early referral and reducing delays in the diagnosis and management of inflammatory arthritis. Ann Rheum Dis. 2013;72(1):13–22. doi:10.1136/annrheumdis-2011-201063
12. ACPAC: Advanced Clinician Practitioners in Arthritis Care. 2017. Available from: https://acpacprogram.ca/.
13. Reeves S, Zwarenstein M, Goldman J, et al. Interprofessional education: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2008;(1):CD002213.
14. World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. Geneva, Switzerland:World Health Organization; 2010.
15. Lemieux-Charles L, McGuire WL. What do we know about health care team effectiveness? A review of the literature. Med Care Res Rev. 2006;63(3):263–300. doi:10.1177/1077558706287003
16. Canadian Health Services Research Foundation. Teamwork in Healthcare: Promoting Effective teamwork in healthcare in Canada. Ottawa, ON:Canadian Health Services Research Foundation; 2006.
17. Mickan SM. Evaluating the effectiveness of health care teams. Aust Health Rev. 2005;29(2):211–217. doi:10.1071/AH050211
18. Desmeules F, Roy JS, MacDermid JC, Champagne F, Hinse O, Woodhouse LJ. Advanced practice physiotherapy in patients with musculoskeletal disorders: a systematic review. BMC Musculoskelet Disord. 2012;13:107. doi:10.1186/1471-2474-13-107
19. Holoyen PK, Stensdotter AK. Patients with spondyloarthritis are equally satisfied with follow-up by physiotherapist and rheumatologist. Musculoskeletal Care. 2018;16(3):388–397. doi:10.1002/msc.1241
20. Fennelly O, Blake C, FitzGerald O, et al. Advanced practice physiotherapy-led triage in Irish orthopaedic and rheumatology services: national data audit. BMC Musculoskelet Disord. 2018;19(1):181. doi:10.1186/s12891-018-2106-7
21. Ahluwalia V, Larsen T, Kennedy C, Inrig T, Lundon K. An Advanced Clinician Practitioner in Arthritis Care can improve access to rheumatology care in community-based practice. J Multidisciplinary Healthcare. 2019;12:63–71. doi:10.2147/JMDH.S183397
22. Ahluwalia V, Brooks S, Sweezie R, et al. The effect of triage assessments on identifying inflammatory arthritis and reducing rheumatology wait times in Ontario. J Rheumatol. 2019. doi:10.3899/jrheum.180734
23. Lou JQ, Durando P. Asking clinical questions and searching for the evidence. In: Law M, MacDermid JC, editors. Evidence-Based Rehabilitation: A Guide to Practice.
24. Sandelowski M. Using qualitative research. Qual Health Res. 2004;14(10):1366–1386. doi:10.1177/1049732304269672
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
26. Auerbach C, Silverstein LB. Qualitative Data: An Introduction to Coding and Analysis. New York: New York University Press; 2003.
27. Lundon K, Kennedy C, Rozmovits L, et al. Evaluation of perceived collaborative behaviour amongst stakeholders and clinicians of a continuing education programme in arthritis care. J Interprof Care. 2013;27(5):401–407. doi:10.3109/13561820.2013.783559
28. Warmington K, Kennedy CA, Lundon K, et al. The patient perspective: arthritis care provided by Advanced Clinician Practitioner in Arthritis Care program-trained clinicians. Open Access Rheumatol. 2015;7:45–53. doi:10.2147/OARRR.S85783
29. Joseph C, Morrissey D, Abdur-Rahman M, Hussenbux A, Barton C. Musculoskeletal triage: a mixed methods study, integrating systematic review with expert and patient perspectives. Physiotherapy. 2014;100(4):277–289. doi:10.1016/j.physio.2014.03.007
30. Borrill CWM, Shapiro D, Rees A. Team working and effectiveness in health care. Br J Health Care Manage. 2000;6:364–371. doi:10.12968/bjhc.2000.6.8.19300
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.