")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Patient Representatives’ Perspectives on Healthcare at the Time of COVID-19 and Suggestions for Care Redesign After the Pandemic: A Qualitative Study in Twenty-Four Countries
Authors Stamm TA , Seidler Y, Andrews MR, Eghbali M, Kiguli J, Ritschl V , Omara M, Schaffer G, Mosor E
Received 24 September 2021
Accepted for publication 23 December 2021
Published 9 February 2022 Volume 2022:15 Pages 247—258
DOI https://doi.org/10.2147/JMDH.S341010
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tanja A Stamm,1,2 Yuki Seidler,1 Margaret R Andrews,1 Mohammad Eghbali,3 Juliet Kiguli,4 Valentin Ritschl,1 Maisa Omara,1,2 Gertraud Schaffer,5 Erika Mosor1
1Section for Outcomes Research, Center for Medical Statistics, Informatics and Intelligent Systems, Medical University of Vienna, Vienna, Austria; 2Ludwig Boltzmann Institute for Arthritis and Rehabilitation, Vienna, Austria; 3School of Nursing and Midwifery, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran; 4Department Community Health & Behavioural Sciences, Makerere University School of Public Health, College of Health Sciences, New Mulago Hospital Complex, Kampala, Uganda; 5Österreichische Rheumaliga (ÖRL), Maria Alm, Austria
Correspondence: Tanja A Stamm, Section for Outcomes Research, Center for Medical Statistics, Informatics and Intelligent Systems, Medical University of Vienna, Spitalgasse 23, Vienna, 1090, Austria, Email [email protected]
Objective: Several comments and recommendations called to embed better the patients’ and public voice in healthcare policymaking. Still, no studies captured patients’ bottom-up perspectives regarding healthcare at the time of COVID-19 at a micro-level in a range of different countries. We, therefore, explored the perspectives of patient representatives in all six World Health Organisation (WHO) regions and extracted suggestions for care redesign after the pandemic.
Methods: We conducted semi-structured interviews with patient representatives until saturation. Thematic analysis followed a modified form of meaning condensation. We established rigour by transcript checking, inter-coder agreement, quote variation and standardised reporting.
Results: Disadvantaged people experienced an unprecedented inequity in healthcare from limited access to physical violence. The narratives revealed the extent of this inequity, but also opportunities for health workers to act and improve. Stigmatisation from COVID-19 differed between cultures and countries and ranged from none to feeling “ashamed” and “totally bashed”. While experienced as indispensable in the future, patients refused telehealth when they were given “bad news”, such as having an eye removed because of melanoma, and in end-of-life care. Patient representatives redefined their role and became indispensable influencers throughout the pandemic and beyond.
Conclusion: We reached out to patient representatives with diverse perspectives, including those who represent minorities and marginalised patient populations. Since preferences and personal meanings drive behaviour and could be foundations for targeted interventions, they must be considered in all groups of people to increase society’s resilience as a whole. Future healthcare should tackle inequity, address stigmatisation and consider patients’ narratives to optimize telemedicine.
Keywords: coronavirus, COVID-19, SARS CoV-2, patient perspectives, equity, co-creation
Plain Language Summary
No studies captured patients’ lived experiences regarding healthcare during COVID-19 in a range of different countries. We, therefore, conducted a qualitative interview study with patient representatives, most of them being patients themselves, from different chronic diseases in all six WHO regions (America, Africa, Eastern-Mediterranean, Europe, South-East Asia and Western-Pacific) on their lived experiences regarding healthcare at the time of COVID-19 and identified key issues that could feed into future healthcare redesign. Patients belonging to disadvantaged groups experienced an unprecedented inequity in healthcare from limited access to physical violence. Patients’ narratives revealed the extent of this inequity, but also opportunities for health workers to act and improve. Future healthcare should tackle inequity, address stigmatisation and consider patients’ narratives to optimize telemedicine. The pandemic has forced the cooperation of multidisciplinary teams along the patient care pathway and the rapid introduction of digital health tools and new ways of working. The system under pressure has thus adopted some of the principles of value-based care.
Introduction
While the COVID-19 pandemic has already triggered significant healthcare changes,1–3 it continues to challenge health professionals, systems of care and authorities. As healthcare changes were almost exclusively driven by professionals and are potentially very influential on how care will be delivered in the future, it is of utmost importance to ensure that patients’ perspectives are heard and taken into account.4 A large body of literature shows that patients’ preferences differ substantially from those of professionals. Both perspectives are essential in designing healthcare to generate value for individuals and society.5,6 Patient-centricity requires that we tailor interventions to patients’ needs, uncover and understand the motivation for behaviour, and measure outcomes that matter to patients.7,8 In particular, patients with chronic conditions could be a rich resource for optimising healthcare as they require continuous care.9 Furthermore, insights from different countries could show a range of experiences with disparate strategies and practices. Besides the negative impact, the crisis could thus generate opportunities for future healthcare redesign.
Patient representatives are key informants with oversight. We defined them as individuals who represent and are in close contact with patients. They own a rich understanding of larger patient communities’ preferences and views, advise other patients, and deliver peer support.10 In their local contexts, they are close to individual patients,11 and many are patients themselves. Although recommendations for post-COVID-19 care designs already exist and several comments called to embed better the patients’ and public voice in healthcare policymaking,12–17 they did not sufficiently capture and represent patients’ and their representatives’ bottom-up perspectives at a local, micro-level. We, therefore, interviewed patient representatives, most of them being patients themselves, from different chronic diseases in all six WHO regions (America, Africa, Eastern-Mediterranean, Europe, South-East Asia and Western-Pacific) on their lived experiences regarding healthcare at the time of COVID-19 and identified key issues that could feed into future healthcare redesign.
Methods
Study Design and Participants
We conducted a qualitative study based on semi-structured interviews. We recruited patient representatives over 18 from different chronic diseases through purposive snowball sampling18 by contacting patient organisations and care providers. Inclusion criteria were individuals in close contact with patients with chronic diseases and who can talk on behalf of these patients, including those who are a minority and/or marginalised. Patient representatives could be patients themselves. We defined chronic diseases as conditions that last one year or more and need ongoing medical attention or limit activities of daily living or both.19 We approached eligible individuals by e-mail or telephone and explained the objectives and procedures of the study. We set up a separate interview appointment with individuals who consented to participate. We transcribed and analysed the interviews parallel to subsequent data collection to achieve maximum diversity in recruitment regarding gender, age, chronic conditions, country of origin and rural or urban setting. We excluded only persons with severe hearing impairment. Recruitment stopped when data saturation was met, and no new codes were identified in at least five subsequent interviews.20,21 The Ethics Committee of the Medical University of Vienna approved the study (EK Number 1388/2020). The participants’ informed consent included the publication of anonymized responses. This study was conducted following the Declaration of Helsinki.
Procedures
The interview guide was co-developed with a patient research partner (GS) and pilot tested.22 After agreeing on the interview procedures, EM, MO, VR, YS, and TS conducted Arabic, English, French, German, Italian, and Japanese interviews between November 2020 and January 2021. Interviews were audio-recorded with or without video images depending on consent. Basic background information such as age, gender, diseases and years of working as a representative was collected. The interview questions focused on the challenges, perspectives, needs, preferences and prospects of care concerning the COVID-19 pandemic from participants’ views (Supplemental Table A).
Data Analysis
Thematic analysis followed a modified form of meaning condensation22,23 and was facilitated using ATLAS.ti [8.0].24 We applied the following steps: i) familiarising with data by reading through the transcripts; ii) highlighting “meaning units” defined as sections of transcripts considered as relevant for our research topic; iii) assigning preliminary codes to the meaning units; iv) finalising a codebook by consolidating and revising preliminary codes; v) applying the codebook to all transcripts by still allowing adding new codes if needed; and vi) grouping codes under main themes.
Epistemological Commitment
No studies captured patient representatives’ lived experiences regarding healthcare during COVID-19 in a range of different countries. Therefore, we combined narrative understanding and contextuality and explored the unique, textual and naturalistic experiences of a single individual and her or his view on a group of individuals she or he represented.25,26 Narrative epistemology emphasizes that concrete experiences in real life (in our study divided into meaning units, later coded and aggregated under main themes) are always linked to a specific time in life and thus, create unique, time-related events.27
Rigour of the Qualitative Analysis
We checked transcripts against the recording to ensure accuracy.28 Three authors experienced in qualitative analysis (EM, YS and TS) agreed on the meaning units. EM and YS independently coded the first six transcripts and calculated inter-coder agreement based on the percentage of overlapping codes.29 We established transferability by collecting meaningful quotes from various participants, focusing on different chronic diseases, diverse geographical and cultural backgrounds, and multiple contexts. We reflected on our roles and perceptions influenced by our previous research engagements involving chronically ill patients. Finally, we reported the results according to the Consolidated Criteria for Reporting Qualitative Research Checklist30 (Supplemental Table B).
Results
Data saturation (Supplemental Table C) was reached after 34 interviews with individuals from 24 countries (Table 1). Nineteen participants (58%) were patients with a chronic disease themselves. In total, we identified 59 codes which we then grouped under four main themes (Table 2; Supplemental Tables D and E). Inter-coder agreement ranged between 80 and 83% (Supplemental Table F).
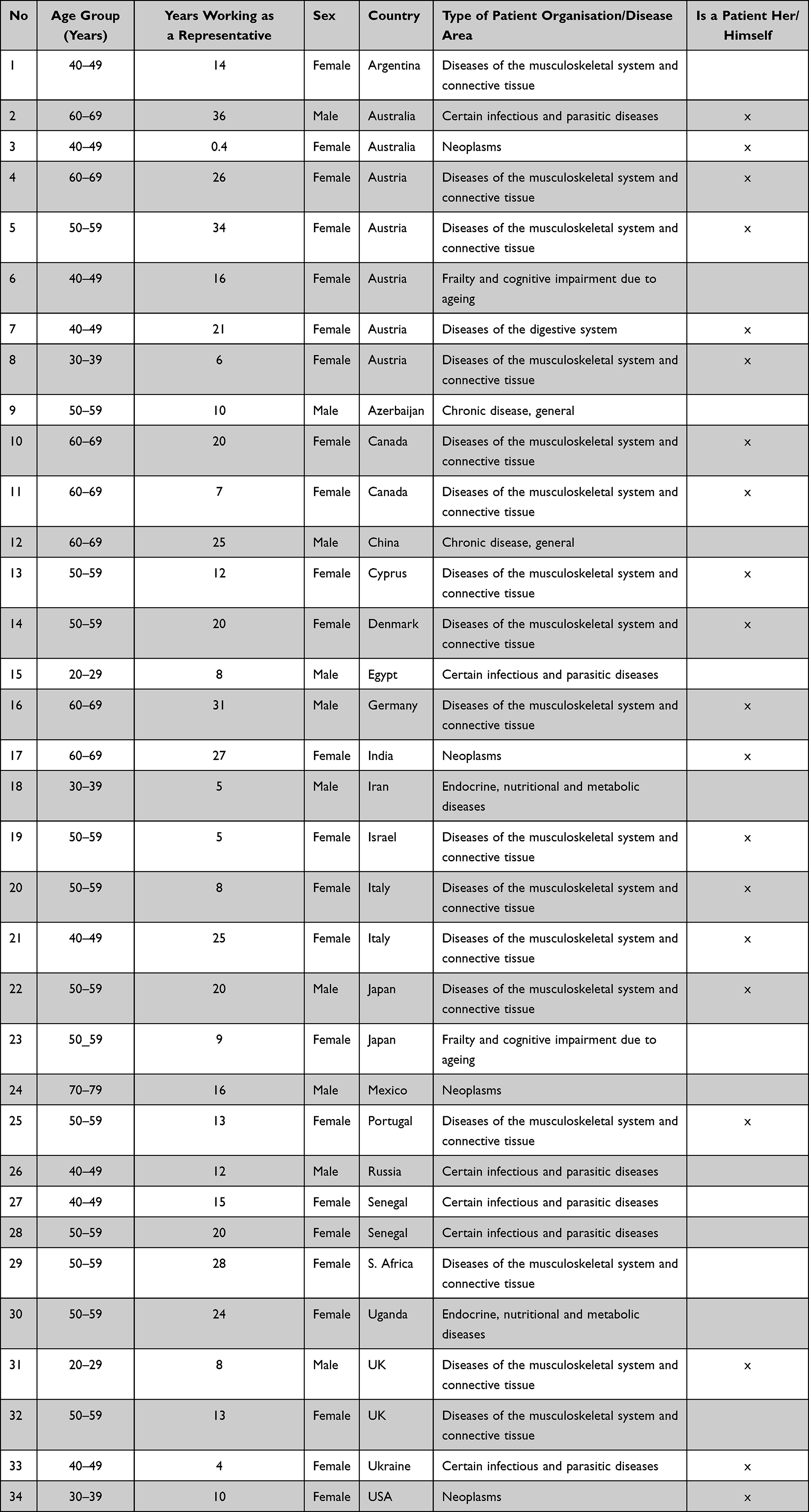 |
Table 1 Characteristics of the Patient Representatives |
 |
Table 2 Main Themes and Related Codes |
Theme 1: Increasing Inequity in the Context of Care
While inequity in governance and infrastructure in care was evident between countries, the interviewees also described unprecedented disparities within their own countries. Patients with low self-efficacy, health literacy, education and socioeconomic status, and people with mobility limitations, migration background, older age or limited access to technologies and transportation experienced disadvantages in care. While these disparities had already existed before the pandemic, they got significantly worse due to COVID-19.
One of the biggest concerns always was that people were getting lost in the gaps in the [care] system. But now, even the more educated ones are struggling, and many more [less-educated people] are slipping through. I suspect there will be more long-term consequences because of that than COVID deaths. (United Kingdom, male, 20–29 years)
A poor woman [with a chronic disease] who wanted to have an abortion because she already had four children and she and her husband had lost their jobs due to the pandemic, could have gone to a private hospital and pay for it, but she had no money for that. So the child was born, an unassisted birth, and died afterwards. (Ukraine, female, 40–49 years)
One of the main reasons for increased disparities was reduced public care services due to the allocation and concentration of existing resources to COVID-19. Patients from all WHO regions were affected, but vulnerable populations in countries with limited resources were hit the hardest. While the possibility of drug shortages “sent a ripple of concern among our community” (Australia, male, 60–69 years) in some countries, these shortages became a reality in others. A patient representative from Mexico explained that some “transplant programmes [in public hospitals] had been shut down since March [until December 2020]” and patients were sent back to dialysis. In contrast, private clinics almost continuously offered transplants when patients paid by themselves.
Similarly, a patient representative from Ukraine reported that HIV patients “were not even welcome in private hospitals” when public services closed, even if they could pay. In Uganda, the loss of income, lack of transportation, permits required from local authorities to visit health facilities, curfews, and physical violence experience resulted in people not seeking treatment when needed. Moreover, people resorted increasingly to traditional herbal therapies.
The turn up [to the hospital] was very, very poor, and this affected my diabetic and hypertension patients who were taking drugs regularly. I actually lost three of my clients, and I associate it with the lack of transport to come to the health facility. So, COVID-19 prevention, the quarantine, it was so bad, the security was involved, they beat up people, and that scared the people. Apart from diabetic patients, we lost a mother who was pregnant and was yet supposed to have a caesarean section. (Uganda, female, 50–59 years)
Migrants with chronic diseases in Russia received treatment only from their countries of origin, as many of them were not entitled to state-funded care in Russia. Due to lockdown, “this transnational care of provision of treatment was interrupted” (Russia, male 40–49 years). In some cases, it was even reported that the ambulance did not come if the caller had a strong foreign accent. The language barrier, weak social networks, and not having internet access were barriers to accessing information and extra support such as those provided by non-governmental organisations.
Chronically ill patients lived with multiple fears during the pandemic. While some patients were afraid of hospital infections and self-isolated from care services, others were anxious about “home isolation” consequences on physical, mental and social health (Argentina, female, 40–49 years). A chronically ill patient from the UK felt “guilty” for occupying care services that someone else would otherwise need for COVID-19 care (male, 20–29 years).
Despite these negative impacts, more than one-third of the interviewees also mentioned that COVID-19 had raised awareness of disadvantaged people’s situation and needs and increased community solidarity. Some interviewees suggested that health professionals should assess and address these inequities in their local contexts in the future and learn from other countries.
I thought that it was good to talk to your university explaining what the situation in Mexico is. It is very problematic, and we hope that, in this window of opportunity, we can change Mexico’s health system because that is what we need to come out of this with a more robust, with most equality — a system for the population, especially for the most vulnerable ones which is the poor ones. (Mexico, male, 70–79 years)
Theme 2: Stigma and Discrimination in Cultural Context
The interviewees described social and cultural determinants of stigma, which concerned COVID-19. A patient representative from Japan explained that fear of stigma from COVID-19 prevented informal caregivers from visiting their relatives with dementia but suspected that it is different in other countries.
In big cities, it is less problematic, but the problem is in rural areas with very low infection rates. [There] the fear of being the “patient zero” is extremely high. […] I guess it is not like that in other foreign countries, right? It is like a hygienic mania. There are even rumours of people killing themselves of being ashamed of being “patient zero”, well this is just a rumour, but that´s how bad the stigma is. There is no way to hide the infection if you are living in a small community. […] The “patient zero” in our prefecture was a man who was visiting his old mother to provide home care. Later he went to his local table tennis club and caused a cluster. He was totally bashed. (Japan, female, 50–59 years)
The interviewees also discussed stigma from COVID-19 compared to other diseases. A patient representative from Senegal elaborated that it was more difficult to “hide” HIV medication in the time of a lockdown if many people lived together in a relatively small area. Another participant from Australia considered stigma from COVID-19 less impactful than stigma from other diseases.
And nobody was necessary blamed if you caught COVID. I am not saying they should have been. But look who got it. Boris Johnson and Donald Trump, and all these celebrities. Now, did they experience stigma as a result? I am not sure at all. With HIV, the stigma was quite different. I think we people with HIV now feel that we were neglected in terms of the amount of resources and interests in the community compared to COVID. (Australia, male, 60–69 years)
Theme 3: Telehealth is Indispensable Now and in the Future, but with Limitations
The provisions of various care services via the internet or telephone increased in most countries. Telehealth experiences ranged from substantial improvements of care, especially for those who live far away from the hospitals, to the need for in-person, face-to-face contacts as a definite requirement under certain conditions.
Telehealth Being Indispensable in the Future of Care
This theme referred to fewer efforts and time needed off from daily activities. These include paid work for medical appointments, a possibility to effectively overcome limitations of personal immobility and lack of transportation, better access to specialists who could be consulted even if physically distant, and a positive shift towards community- and home-based care. Interviewees described a steep learning curve on both sides, providers and receivers, and expressed the wish to keep these positive aspects of telehealth in the future. A patient representative from the USA with a chronic autoimmune disease described that her rheumatologist and she “worked together to make teleconsultations ideal”. She could then use these experiences herself when advising other patients. A participant from Austria (female, 50–59 years) with a chronic disease and physical impairment explained that “collecting permanent medications via e-prescription in the pharmacy without having been at the physician’s office” made her life “much easier” as it decreased transportation efforts.
Telehealth is Not a Solution for Everything
Even in situations where resources to implement telehealth were available, participants described clear limitations. Care with telehealth was, in general, not experienced as being on the same level as usual care. People reported anxiety about untreated symptoms, organ damages due to health conditions diagnosed late, increased incidences of flares, often due to medication changes by patients themselves, and increased pain due to a lack of therapies. Besides, the need for in-person, face-to-face contact when delivering “bad news” and making decisions that significantly impact patients’ lives was stressed. A patient with eye melanoma from Australia who recently had an eye removed explained that when “patients were told this huge news about cancer or eye removal”, face-to-face consultation and the presence of a trusted person were essential. Furthermore, while she “loves the telehealth now” due to her living far away and the fact that the “doctors are always running late”, she explained that:
I was supposed to have a six-month check-up in February this year. But because of COVID, they said that people could only come in if it were an emergency or something happening. So I spoke to the doctor on the phone, and she said, “Do you feel any differences?” When I said “No”, we left it. And then I went back, and it [the eye melanoma] was twice as size as it had been before. So, I don´t know if I had gone in February whether anything would have been different or not? Maybe not. But yeah, that will always be kind of in the back of my mind, I think, just wondering what if we caught it when it was smaller. (Australia, female, 40–49 years)
Other reasons given for problems in the widespread implementation of telecare in times of a pandemic were the unsuitability of specific interventions for distance care, the inability of some providers to offer appropriate tools for remote care and health monitoring and also the incapacity of patients to use new ways of care due to their low health literacy or financial resources.
Remote Peer Support
Remote support provided by patient representatives using digital means led to a similar discourse as telehealth. It attracted more people with broader geographical coverage since the start of the pandemic, especially people from younger age groups and limited mobility. By digital means, support could be continued during the pandemic. This virtual assistance was essential in regions with overwhelmed care providers that “shifted resources towards working almost exclusively with COVID-19 patients”, such as the Lombardy region in Italy, where peer support became an essential source of information for patients from different health areas (Italy, female, 40–49 years). However, digital support also had substantial limitations, and face-to-face contact was experienced as a necessity on some occasions. A patient representative from the USA described that it did not feel appropriate to conduct end-of-life conversations by telephone. Body language and visual clues were essential to establish a proper relationship.
All of the sudden, I was doing really serious visits with families over telehealth, like an end-of-life conversation or hospice conversation over the phone. It just looked so different, and I was scared that I wasn´t going to be able to provide the emotional support that was really needed for the patients and families through my physical presence with them. And it felt like, oh my gosh, my role is to provide support, and I am so reliant on seeing people face-to-face and following their body language. (USA, female, 30–39 years)
Theme 4: Patient Representatives as Essential Connectors and Influencers
During the current crisis, patient representatives became essential information sources for other patients, especially when the representatives were also patients. The often-ambiguous information released by authorities, policymakers and experts added greater significance to this role. In some countries, patient representatives were recipients of downstream communications from the authorities, which enabled them to set up peer and professionally supported hotlines to take over from the overwhelmed care system. In contrast, a patient representative from Austria (female, 60–69 years) with a chronic autoimmune disease herself explained that she had not received any information regarding COVID-19 vaccinations from the health authorities. However, other patients regularly asked for her advice on this matter.
Patient representatives described that they also provided mental health support. Individuals who experienced mental health distress, suffered from loneliness or developed high level of anxieties turned increasingly to patient organisations.
By the end of the [video] call, by the end of the meeting their attitude has changed. And they were like you know, ‘Thank you for spending so much time with us, thank you for explaining to us. And thank you for reassuring us that we can always come back to you and talk to you’ and all that. So, I think it is the role of the patient advocates to be with the patients at this time. (India, female, 60–69 years)
Like influencers on social media, patient representatives’ role became even more influential for informing large communities. Patient representatives passed on information to bigger groups of individuals, triggering motivation and health behaviour regarding testing and vaccination. This implies positive changes in the future care system as one patient representative in the UK commented:
Within the health service, there has been a recognition of the roles that the patient organisations can play in supporting patients, and patients themselves have discovered that. So, now they are beginning to see organisations like ourselves as embedded within the health system, not just as an “oh there´s an extra thing that appears”. That we actually are the part of the whole patient pathways, that they see a nurse, they see a doctor, they see a physio, they have a patient organisation. And that I think it will become more of the norm if anything that COVID has proved them. (UK, female, 50–59 years)
Discussion
Our study uncovered four main themes. Each included a range of reflections, perspectives, and preferences meaningful for the participants in their particular contexts regarding time, setting, and personal factors. While COVID-19 measures were sometimes considered context-independent and similar in their effectiveness across countries,31 qualitative research adds to understanding these interventions’ meaning and their consequences for individuals. This is important in eliciting and reaching out to a diversity of perspectives, including those of minorities and marginalised or vulnerable populations. As perspectives and meanings are drivers for specific behaviour and could be the foundation for individualised and targeted interventions, they need to be appropriately addressed in all groups of people to increase society’s resilience as a whole.
While international organisations could best address inequity between different countries, healthcare providers should assess and search for individual disparities in the local context and tailor their interventions to overcome these. Otherwise, inequalities and stigma might increase existing vulnerabilities and marginalisation or create new ones. Access to care as an essential resource should be open to all individuals and a prerequisite for societies’ proper functioning. Seeing care through a lens of equity is thus necessary when redesigning services after this pandemic. A failure to do so could increase the gaps, and healthcare might become even more of luxury not equally accessible for all.
Digital tools and telehealth have become fundamental during the COVID-19 pandemic in an accelerated manner.32 A generally positive attitude has been expressed. However, the lack of telehealth resources might create another disparity in healthcare within and between countries and exclude disadvantaged people from certain services.33 Our findings also have important implications for digital survey research;34 a systematic exclusion of people with limited technology access could lead to biased results. Even if the resources and capabilities exist to use digital tools and telehealth, health professionals must consider specific limitations. The personal presence of health professionals and trusted people in delivering bad news that has severe consequences for patients’ health was considered an essential aspect of care that telehealth could not replace.
Public health interventions in a pandemic benefit from an effective bilateral, bottom-up and top-down information stream. While individuals’ perspectives are essential for tailoring interventions to their needs, clear downstream information with specific channels for certain communities could best utilise patient representatives’ roles. Testing and vaccination campaigns, if organised, could also benefit from well-informed, engaged patients and patient representatives. Moreover, making perspectives, motivations and unmet needs explicit and transparent could help overcome stigmatisation and decrease social exclusion.35
COVID-19 has led to an unprecedented focus on one patient group and transparency on a set of distinct outcomes metrics such as mortality and Intensive Care Unit (ICU)-need of population groups. It has forced the cooperation of multidisciplinary teams along the patient care pathway and the rapid introduction of digital health tools and new ways of working. These are interesting examples that show how the system under pressure has adopted some of the principles of value-based healthcare.36 Value-based healthcare focuses on patient outcomes and puts them in relation to costs. This focus on outcomes has made inequity more visible. Our paper has explored whether this was also the perception of patients worldwide and confirms it. It also shone a light on the social determinants of health and race, education and health literacy.
We are committed to patient-centred care, outcomes that matter to patients and continuous patient value improvement. It may be that the COVID-19 experience indicates that inequity will increase when the healthcare system is challenged. As we might be progressing to an unsustainable development of healthcare systems, we need to raise awareness of inequity. Standardized outcomes measures, such as those used to monitor the COVID-19 pandemic, will be essential to identify inequity increases and address them in time. Our findings indicate a set of areas where this is particularly important to consider; these might not be only COVID-19 specific but generic and likely to be relevant as our systems’ pressure increases over the coming years.
The variation and diversity elicited in our study is a strength and limitation at the same time. While we uncovered a considerable range of experiences between and within individuals and countries, several similarities emerged. Quantitative work needs to follow up to determine the frequencies of these experiences.
The novelty of the research lies in its exploration of the bottom-up perspectives of the patient representatives. We targeted this specific group which is not adequately approached in research despite their crucial role, to raise awareness of the presence and importance of those representatives and tackle their role in healthcare. We pointed out several issues relevant for policy making, including the increasing splitting of society. The participants´ narratives revealed the extent of this inequity, and opportunities for health workers to act and improve. Future research needs to focus on strategies that ensure and sustain equality in healthcare, even in a pandemic and for better preparedness. Also, more studies should focus on telemedicine in specific groups of the population, such as children and adolescents.37,38
Conclusion
We reached out to patient representatives with diverse perspectives, including those who represent minorities and marginalised populations. Systematic exclusion of patients with limited technology access increases inequity in healthcare and biases research findings. Since preferences and personal meanings drive behaviour and could be foundations for targeted interventions, they must be considered in all groups of people to increase society’s resilience as a whole. Future healthcare should tackle inequity, address stigmatisation and consider patients’ narratives to optimize telemedicine.
Transparency Statement
The corresponding author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; no important aspects of the study have been omitted, and any discrepancies from the study as originally planned have been explained.
Data Sharing Statement
The data generated in this qualitative study is not suitable for sharing beyond what is contained within this publication and its supplements. Further information can be obtained from the corresponding author.
Acknowledgments
We would like to thank all people who took part in this study for sharing their valuable perspectives and the patient organisations in establishing contacts. We are grateful to the Regional Research and Training Center on Infectious Diseases (CRCF) of the National Hospital of Fann, Dakar, Senegal, for conducting interviews with Senegal participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Prof. Dr. Tanja A Stamm reports personal fees from AbbVie, Roche, Sanofi, and Takeda, outside this work. The authors declare no other competing interests related to this work, including no support from any funding organization for the submitted work, no financial relationships with any organizations that might have an interest in this work in the previous three years, and no other relationships or activities that could appear to have influenced this work.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (2019-nCoV) infection is suspected—interim guidance: World Health Organization; 2020 [cited April 05, 2020]. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected.
3. Liu Q, Luo D, Haase JE, et al. The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Glob Health. 2020;8(6):e790–e798. doi:10.1016/S2214-109X(20)30204-7
4. Richards T, Scowcroft H. Patient and public involvement in covid-19 policy making. BMJ. 2020;370:m2575. PMID: 32611571. doi:10.1136/bmj.m2575
5. Castro EM, Van Regenmortel T, Vanhaecht K, Sermeus W, Van Hecke A. Patient empowerment, patient participation and patient-centeredness in hospital care: a concept analysis based on a literature review. Patient Educ Couns. 2016;99(12):1923–1939. doi:10.1016/j.pec.2016.07.026
6. Bravo P, Edwards A, Barr PJ, Scholl I, Elwyn G, McAllister M. Conceptualising patient empowerment: a mixed methods study. BMC Health Serv Res. 2015;15(1):252. doi:10.1186/s12913-015-0907-z
7. Liu TC, Bozic KJ, Teisberg EO. Value-based healthcare: person-centered measurement: focusing on the three C’s. Clin Orthop Relat Res. 2017;475(2):315–317. doi:10.1007/s11999-016-5205-5
8. Hewlett S, Smith AP, Kirwan J. Values for function in rheumatoid arthritis: patients, professionals and public. Ann Rheum Dis. 2001;60:928–933. doi:10.1136/ard.60.10.928
9. Waterman AD, Gleason J, Lerminiaux L, et al. Amplifying the patient voice: key priorities and opportunities for improved transplant and living donor advocacy and outcomes during COVID-19 and beyond. Curr Transplant Rep. 2020:1–10. doi:10.1007/s40472-020-00295-x
10. Mirrielees JA, Breckheimer KR, White TA, et al. Breast cancer survivor advocacy at a university hospital: development of a peer support program with evaluation by patients, advocates, and clinicians. J Cancer Educ. 2017;32(1):97–104. doi:10.1007/s13187-015-0932-y
11. Bu X, Jezewski MA. Developing a mid‐range theory of patient advocacy through concept analysis. J Adv Nurs. 2007;57(1):101–110. doi:10.1111/j.1365-2648.2006.04096.x
12. EU_Health_Coalition. A shared vision for the future of health in Europe - lessons learnt from the pandemic; February 09, 2021. Available from: https://www.euhealthcoalition.eu/wp-content/uploads/2020/10/FINAL-lessons-learnt-from-the-COVID-19-pandemic.pdf.
13. Alam U, Nabyonga-Orem J, Mohammed A, Malac DR, Nkengasong JN, Moeti MR. Redesigning health systems for global heath security. Lancet Glob Health. 2021;9(4):e393–e394. doi:10.1016/S2214-109X(20)30545-3
14. Skegg D, Gluckman P, Boulton G, et al. Future scenarios for the COVID-19 pandemic. Lancet. 2021;397(10276):777–778. doi:10.1016/S0140-6736(21)00424-4
15. Valeriani G, Sarajlic Vukovic I, Lindegaard T, Felizia R, Mollica R, Andersson G, editors. Addressing Healthcare Gaps in Sweden During the COVID-19 Outbreak: On Community Outreach and Empowering Ethnic Minority Groups in a Digitalized Context. Healthcare. Multidisciplinary Digital Publishing Institute; 2020.
16. Wosik J, Fudim M, Cameron B, et al. Telehealth transformation: COVID-19 and the rise of virtual care. J Am Med Inform Assoc. 2020;27(6):957–962. doi:10.1093/jamia/ocaa067
17. Hirko KA, Kerver JM, Ford S, et al. Telehealth in response to the COVID-19 pandemic: implications for rural health disparities. J Am Med Inform Assoc. 2020;27(11):1816–1818. doi:10.1093/jamia/ocaa156
18. Patton MQ. Qualitative Research and Evaluation Methods. Sage; 2002.
19. Centers for Disease Control and Prevention. About Chronic Diseases; November 17, 2021. Available from: https://www.cdc.gov/chronicdisease/about/index.htm.
20. Mosor E, Stoffer-Marx M, Steiner G, et al. I would never take preventive medication! Perspectives and information needs of people who underwent predictive tests for rheumatoid arthritis. Arthritis Care Res. 2020;72(3):360–368. doi:10.1002/acr.23841
21. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
22. Kvale S. Doing Interviews. Sage; 2008.
23. Clarke V, Braun V. Teaching thematic analysis: overcoming challenges and developing strategies for effective learning. Psychologist. 2013;26(2):120–123.
24. ATLAS.ti. Atlas.ti [8.0]. Berlin: Atlas.ti Scientific Software Development GmbH; 2018.
25. Denzin NK. Interpretative Ethnography: Ethnographic Practices for the 21st Century. Thousand Oaks: Sage Publications; 1997:1997.
26. Wengraf T. Qualitative Research Interviewing: Biographic Narratives and Semi-Structured Methods. London: Sage Publications; 2001:2001.
27. Stamm TA, Lovelock L, Stew G, et al. I have mastered the challenge of living with a chronic disease: the life stories of people with rheumatoid arthritis. Qual Health Res. 2008;18(5):658–669. doi:10.1177/1049732308316348
28. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
29. Creswell JW, Poth CN. Qualitative Inquiry and Research Design: Choosing Among Five Approaches. Sage publications; 2016.
30. Tong A, Craig J, Sainsbury P. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
31. Haug N, Geyrhofer L, Londei A, et al. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat Hum Behav. 2020;4(12):1303–1312. doi:10.1038/s41562-020-01009-0
32. Ting DSW, Carin L, Dzau V, Wong TY. Digital technology and COVID-19. Nat Med. 2020;26(4):459–461. doi:10.1038/s41591-020-0824-5
33. Gasser U, Ienca M, Scheibner J, Sleigh J, Vayena E. Digital tools against COVID-19: taxonomy, ethical challenges, and navigation aid. Lancet Digital Health. 2020;2(8):e425–e434. doi:10.1016/S2589-7500(20)30137-0
34. Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med. 2021. doi:10.1038/s41591-021-01292-y
35. Weiss MG, Ramakrishna J. Stigma interventions and research for international health. Lancet. 2006;367(9509):536–538. doi:10.1016/S0140-6736(06)68189-0
36. Porter ME, Larsson S, Lee TH. Standardizing patient outcomes measurement. N Engl J Med. 2016;374(6):504–506. doi:10.1056/NEJMp1511701
37. Badawy SM, Radovic A. Digital approaches to remote pediatric health care delivery during the COVID-19 pandemic: existing evidence and a call for further research. JMIR Pediatr Parent. 2020;3(1):e20049. PubMed PMID: 32540841; PubMed Central PMCID: PMCPMC7318926. doi:10.2196/20049
38. Serlachius A, Badawy SM, Thabrew H. Psychosocial challenges and opportunities for youth with chronic health conditions during the COVID-19 pandemic. JMIR Pediatr Parent. 2020;3(2):e23057. PubMed PMID: 33001834; PubMed Central PMCID: PMCPMC7553787. doi:10.2196/23057
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.