Back to Journals » Patient Preference and Adherence » Volume 20
Patient Preferences for Direct versus Indirect Dental Veneers: Associations with Durability, Socioeconomic Status, and Satisfaction
Authors Hamad SA, Ameen ZAH, Saber DB, Hawrami GR, Zangana AM, Younis HF, Salih TS, Ismael DS, Hashemi R
Received 18 April 2026
Accepted for publication 7 July 2026
Published 10 July 2026 Volume 2026:20 618019
DOI https://doi.org/10.2147/PPA.S618019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Samir A Hamad,1 Zana A H Ameen,1 Diyar Bakr Saber,1 Ghalib R Hawrami,1 Aso M Zangana,1 Halat Farhad Younis,1 Tanya Salam Salih,2 Dldar Saleh Ismael,1 Reza Hashemi3,4
1Department of Dental Assistant, Erbil Medical Technical Institute, Erbil Polytechnic University, Erbil, Kurdistan Region, Iraq; 2Department of Nutrition and Dietetics, College of Health Technology, Cihan University-Erbil, Erbil, Kurdistan Region, Iraq; 3Department of Nutrition, School of Public Health, Zanjan University of Medical Sciences, Zanjan, Iran; 4Department of Nutrition and Dietetics, College of Health Sciences, Hawler Medical University, Erbil, Kurdistan Region, Iraq
Correspondence: Reza Hashemi, Department of Nutrition, School of Public Health, Zanjan University of Medical Sciences, Zanjan, Iran, Email [email protected]
Background: Expatriates represent a growing patient group seeking aesthetic dental treatments in cosmopolitan settings, yet limited evidence is available regarding factors associated with their choice between direct and indirect veneers. This study aimed to examine factors associated with veneer preference, assess the association of educational level and economic status with treatment interest, and evaluate the relationship between satisfaction and recommendation intent among expatriates in Erbil.
Methods: A cross-sectional survey was conducted from January to June 2023 among 439 expatriates recruited from private dental clinics and cosmetic centres in Erbil using stratified convenience sampling. A validated 48-item questionnaire assessed demographics, prior dental experience, decision-making factors using 5-point Likert scales, veneer preference, satisfaction, and recommendation intent. Data were analysed using χ2 tests, Spearman correlations, multinomial logistic regression for veneer preference, ordinal logistic regression for satisfaction, and binary logistic regression for recommendation intent, with adjustment for relevant covariates.
Results: Durability showed the strongest independent association with preference for indirect veneers compared with direct veneers (adjusted OR 2.65 per 1-point increase, 95% CI 1.78– 3.95, p< 0.001). Aesthetic outcome was ranked as the most important consideration overall by 44.4% of participants, but it was no longer statistically significant after adjustment. A significant education × economic status interaction was observed (p=0.03), indicating that the association between higher education and interest in veneers was more evident among participants with good or very good economic status. Among veneer recipients (n=68), 76.5% were very or somewhat satisfied; higher satisfaction was strongly associated with recommendation intent (adjusted OR 4.21 per 1-point increase, 95% CI 2.84– 6.24, p< 0.001). Overall, 40.3% of participants remained undecided about veneer type.
Conclusion: In this cross-sectional study of expatriates in Erbil, durability was associated with preference for indirect veneers, while socioeconomic status appeared to shape treatment interest. Higher satisfaction was also associated with greater willingness to recommend veneer treatment. These findings support the use of targeted patient education, transparent discussions of expected longevity, and flexible financing strategies to facilitate informed decision-making in mobile expatriate populations. Because of the cross-sectional design, these findings should be interpreted as associations rather than causal effects.
Keywords: dental veneers, direct veneers, indirect veneers, expatriates, patient preference, durability, patient satisfaction, socioeconomic factors, cosmetic dentistry
Introduction
The pursuit of an aesthetically pleasing smile has become a defining feature of contemporary society, fuelled by social media, professional expectations and heightened awareness of self-image.1 Cosmetic dentistry, once considered a luxury, now occupies a central position in oral healthcare, with dental veneers representing one of the most requested minimally invasive interventions for correcting discoloration, chipping, spacing and minor malalignment. The term “Hollywood Smile” has entered everyday language as shorthand for a bright, symmetrical and youthful dentition that conveys confidence and success.2 Veneers achieve this outcome through two fundamentally different approaches: direct composite veneers, fabricated and placed chairside in a single visit, and indirect ceramic or composite veneers, prepared in the laboratory and bonded in a subsequent appointment. Each technique carries distinct advantages and limitations in terms of durability, aesthetics, chair time, cost and repairability.3
Clinical evidence consistently shows that indirect veneers generally offer superior resistance to staining, wear and fracture compared with direct composite restorations, particularly in the long term. Recent randomized trials have confirmed better survival and colour stability for indirect ceramic laminate veneers in anterior diastema closure and for indirect composite restorations in posterior applications, although direct techniques remain faster and more conservative of tooth structure.4 Despite these objective differences, patient choice is rarely driven solely by material properties. Instead, decisions are shaped by a complex interplay of cost, perceived longevity, treatment convenience, prior knowledge and individual socioeconomic circumstances. Patients who prioritise durability and natural appearance tend to favour indirect options, whereas those constrained by time or budget often select direct veneers.5 Yet literature remains surprisingly silent on how these preferences manifest in mobile, multicultural populations such as expatriates.
Erbil has become a regional hub for private healthcare, education, business and professional mobility and the expatriate population is an increasingly visible patient group. Expatriates seeking aesthetic dental care in this setting often do not fit neatly into the assumptions that tend to inform studies of local patient populations. The patient may have different cultural expectations of what dental appearance should be, different levels of familiarity with the available veneer techniques, varying insurance coverage, and uncertain access to long-term follow-up care should they move. Such practical and cultural considerations can complicate the decision between direct and indirect veneers beyond the straightforward comparison of cost, appearance and durability. This population is also of importance as expatriate patients are often making treatment decisions within dense social and professional networks. Thus, their satisfaction with cosmetic dental procedures may affect not only their own future care-seeking behaviour but also the perceptions and recommendations shared within wider expatriate communities. Considering the clinical relevance, there is a lack of patient-preference research in aesthetic dentistry with expatriates in Erbil. Most existing studies have focused on general dental populations or single-country samples, and the intersection of mobility, socioeconomic position, and cross-cultural expectations in veneer-related decision-making is little evidenced.6–9
The present cross-sectional study therefore addresses a clear evidence gap by systematically evaluating the factors that influence expatriates’ choice between direct and indirect veneers in Erbil. Specifically, it examines the relative importance of durability, aesthetics, cost, treatment time and reversibility; quantifies the moderating effects of educational level, economic status and prior knowledge; and determines whether post-treatment satisfaction predicts recommendation intent. By integrating validated patient-reported measures with multivariate modelling, the study moves beyond simple descriptive comparisons to provide clinically actionable insights for practitioners who treat increasingly international patient cohorts.
In doing so, this work contributes to the broader discourse on patient-centred cosmetic dentistry at a time when global mobility and aesthetic expectations continue to rise. Understanding the unique decision-making pathways of expatriates is no longer an academic curiosity but a practical necessity for delivering equitable, high-quality care in cosmopolitan clinical settings.
Materials and Methods
Study Design and Reporting
This cross-sectional analytical study was conducted among expatriates attending private dental clinics and cosmetic dental centers in Erbil, Iraq. The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, and the statistical reporting followed the Statistical Analyses and Methods in the Published Literature (SAMPL) recommendations where applicable.
Ethical approval was obtained from the Institutional Review Board of the College of Dentistry, University of Kurdistan-Hewlêr (reference UKH-CoD-2022-018, 15 December 2022). The study was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was prospectively registered on the Open Science Framework (osf.io/7k9p3) to support transparency and reproducibility.
Participants and Setting
Participants were recruited between 1 January and 30 June 2023 from eight private dental clinics and two specialised cosmetic dental centres in Erbil, Iraq, all of which serve a substantial expatriate clientele. Inclusion criteria were: (1) self-identified expatriate status (living outside the country of birth for ≥ 6 months), (2) age ≥ 18 years, (3) having considered or received veneer treatment (direct, indirect, or both), and (4) ability to provide informed consent and complete the questionnaire in English or Kurdish. Individuals undergoing active orthodontic treatment, those with severe systemic illness likely to confound aesthetic perception, or those unable to complete the questionnaire independently were excluded.
To enhance diversity in the expatriate sample and maintain feasibility in a busy private-clinic setting, a quota-based stratified convenience sampling approach was used. The ten sites involved were treated as recruitment units prior to the commencement of recruitment and were grouped by site type, ie private dental clinics and specialised cosmetic dental centres. The research team attempted to recruit eligible expatriate participants from a wide range of demographic strata of gender, age group and nationality/region of origin within each site. Economic status was measured by questionnaire and was unknown before enrolment; hence it was monitored during recruitment but not used as a formal pre-enrolment stratum.
Trained research assistants screened patients attending clinics during their recruitment time slot. Eligible expatriates were approached one-by-one in the waiting area and provided with information on the study and asked to participate. If there were multiple eligible patients present at the same time, they were approached in order of arrival. Recruitment at each site continued until the overall planned sample size was reached and the sample was reasonably representative of the predefined demographic strata. The sampling strategy should be understood as a pragmatic stratified convenience sampling, not as a probability-based stratified sampling, since no random selection procedure was employed.
Sample Size Considerations
The minimum required sample size was calculated using G*Power based on χ2 tests, assuming a medium effect size (w = 0.3), α = 0.05, and 80% power. This produced a minimum required sample of 387 participants. The final analytical sample included 439 participants, exceeding this threshold and providing adequate power for the main descriptive, bivariate, and multivariable analyses of veneer preference.
Analyses involving satisfaction and recommendation intent were restricted to participants who had received veneer treatment, because these outcomes were only clinically meaningful among individuals with direct treatment experience. This subgroup included 68 participants. Although this subgroup was appropriate for evaluating post-treatment experience, its smaller size was expected to reduce model precision and widen confidence intervals. For this reason, satisfaction- and recommendation-related models were interpreted cautiously as exploratory adjusted associations rather than definitive predictive models.
Data Collection Instrument
A 48-item structured questionnaire was developed specifically for this study after an extensive review of patient-reported outcome measures in cosmetic dentistry and consultation with three prosthodontists, two behavioral scientists, and a panel of expatriate patients. The questionnaire included five sections: (1) socio-demographic characteristics, (2) prior dental experience and sources of information, (3) decision-making factors rated on 5-point Likert scales, (4) veneer-type preference and reasons for preference, and (5) satisfaction and recommendation-related outcomes. The content, structure, and scaling of the questionnaire were informed by previously validated instruments used in cosmetic dentistry research. The full English version of the questionnaire is provided as Supplementary File 1.
Content validity was reviewed by the expert panel and was considered strong, with a content validity index of 0.92. Face validity and comprehensibility were assessed through cognitive debriefing interviews with 12 expatriates. The questionnaire was forward–backward translated into Kurdish by two independent bilingual translators, reconciled by the research team, and pilot-tested before field administration. Internal consistency was high, with Cronbach’s α values of 0.87 for the decision-making scale and 0.91 for the satisfaction scale. Test–retest reliability was assessed in a separate subsample of 30 participants and was also strong, with intraclass correlation coefficients ranging from 0.82 to 0.89. The final questionnaire was administered either electronically through Google Forms or on paper in a quiet area of the clinic.
Data Collection Procedure
Data collection was conducted over a six-month period (1 January to 30 June 2023) in a standardized manner across all participating sites to minimize temporal and site-specific bias. Prior to fieldwork, four research assistants (two dentists and two postgraduate public-health students) underwent a two-day intensive training program delivered by the principal investigator. Training covered standardized script delivery, neutral response to participant queries, recognition and avoidance of leading prompts, and strict adherence to ethical protocols. A detailed operations manual, including verbatim instructions and troubleshooting scenarios, was provided and reviewed in mock sessions.
Upon arrival at each clinic, eligible participants were approached in the waiting area by a trained assistant who first provided a one-page, plain-language information sheet (available in English and Kurdish) outlining study aims, voluntary participation, right to withdraw at any time without consequence, potential risks (none anticipated), and data confidentiality measures. Written or electronic informed consent was then obtained using a separate form that explicitly reiterated these elements and was witnessed by the assistant. Only after consent was documented did the participant proceed to the questionnaire.
To ensure independence and reduce social-desirability bias, participants completed the 48-item questionnaire alone in a quiet, private consultation room or via a secure tablet provided on-site. Assistants remained available in an adjacent area solely for clarification of wording or technical assistance with the digital version and were instructed never to view responses or offer opinions. The electronic version (Google Forms) automatically timestamped submissions and prevented back-editing once completed; paper versions were collected immediately upon finishing and placed in sealed envelopes. No personal identifiers (name, address, phone number, or national ID) were recorded at any stage. Each questionnaire was assigned to a unique alphanumeric code generated by a secure random-number algorithm.
Completed data were transferred daily to a password-protected, encrypted database (Microsoft SQL Server hosted on a university server compliant with ISO 27001 standards) accessible exclusively to the principal investigator via two-factor authentication. Daily backups were performed automatically and stored on an encrypted external drive kept in a locked cabinet. At the end of the recruitment period, paper forms were scanned, verified for completeness against the electronic database, and then securely shredded in accordance with institutional data-protection policy. Any participant who withdrew after starting the questionnaire had their partial data permanently deleted.
Because the study relied on self-reported data, additional quality-control procedures were used during data collection and cleaning. The questionnaire was pilot-tested and validated before use and trained research assistants provided standardised instructions without influencing participants’ responses. Participants completed the questionnaire privately to reduce social-desirability pressure. During data screening, responses were checked for missing values, inconsistent patterns, implausible entries, and straight-line responding across Likert-scale items. Questionnaires with substantial incompleteness or internally inconsistent responses were reviewed before inclusion in the final dataset. These procedures cannot remove measurement error entirely, but they were used to reduce avoidable misclassification and improve the reliability of the self-reported measures.
Statistical Analysis
All statistical analyses were conducted using R software, version 4.3.1, and IBM SPSS Statistics, version 21. Statistical significance was defined as a two-sided p-value <0.05. Effect estimates were reported with 95% confidence intervals where appropriate.
Participant characteristics, prior dental experience, information sources, decision-making factors, veneer preference, satisfaction, and recommendation intent were first summarized descriptively. Continuous variables were reported as means and standard deviations or medians and interquartile ranges, depending on distributional characteristics. Categorical variables were reported as frequencies and percentages. Denominators were specified according to the relevant analytical population. Veneer preference and most decision-making variables were analyzed in the full sample of 439 participants, whereas veneer type received, satisfaction, and recommendation intent were analyzed only among the 68 participants who had received veneer treatment.
Bivariate associations between categorical variables were examined using χ2 tests of independence or Fisher’s exact tests when expected cell counts were small. Effect sizes for χ2 analyses were reported using Cramer’s V. Associations involving ordinal variables, including satisfaction and recommendation intent, were assessed using Spearman rank-order correlation. These analyses were used to describe unadjusted relationships before fitting multivariable models.
Three multivariable regression models were fitted to examine adjusted associations relevant to the study objectives. First, multinomial logistic regression was used to assess factors associated with veneer-type preference, categorized as direct veneers, indirect veneers, or undecided. Direct veneer preference was used as the reference category. The main predictors included durability rating, cost rating, aesthetic importance, educational level, and economic status. An interaction term between educational level and economic status was included to examine whether the association between education and veneer-related preference differed by perceived economic position. The model was adjusted for age, gender, and nationality or region of origin.
Second, ordinal logistic regression was used to examine factors associated with overall satisfaction level among participants who had received veneers. This analysis was restricted to veneer recipients because satisfaction with treatment was not applicable to participants without prior veneer experience. Predictors included prior veneer experience variables, durability rating, aesthetic importance, educational level, economic status, age, gender, and nationality or region of origin. The proportional-odds assumption was assessed before interpreting the model.
Third, binary logistic regression was used to examine factors associated with willingness to recommend veneer treatment among veneer recipients. Recommendation intent was coded as yes versus no or uncertain. Satisfaction score was the main exposure of interest. The model was adjusted for durability rating, educational level, economic status, veneer type received, age, gender, and nationality or region of origin. Because this model was fitted in the smaller veneer-recipient subgroup, the estimates were interpreted with particular attention to confidence-interval width and model precision, rather than p-values alone.
Several procedures were used to reduce the risk of unstable or over-interpreted findings. Covariates were selected a priori based on clinical relevance and the study objectives, rather than through automated variable selection. Multicollinearity was assessed using variance inflation factors. Model fit was evaluated using appropriate goodness-of-fit statistics, including Nagelkerke pseudo-R2 and the Hosmer–Lemeshow test for logistic models where applicable.
Missing data was minimal, affecting less than 2% of the dataset. Little’s MCAR test was used to examine the missing-data mechanism. Complete-case analysis was used for the main models, and multiple imputations by chained equations were performed as a sensitivity analysis. Additional sensitivity checks included alternative coding of educational and economic categories and subgroup analyses stratified by gender and nationality or region of origin. No variance inflation factor suggested problematic multicollinearity. Where sparse data were present in subgroup models, estimates were interpreted conservatively and reported with appropriate caution.
Results
Of the 512 expatriates approached across the eight private dental clinics and two specialized cosmetic centers in Erbil between January and June 2023, 73 were excluded (42 did not meet the expatriate residency criterion, 18 were undergoing active orthodontic treatment, and 13 were unable to complete the questionnaire independently), resulting in a final analyzed sample of 439 participants (response rate 85.7%). Figure 1 presents the participant flow in accordance with STROBE guidelines.
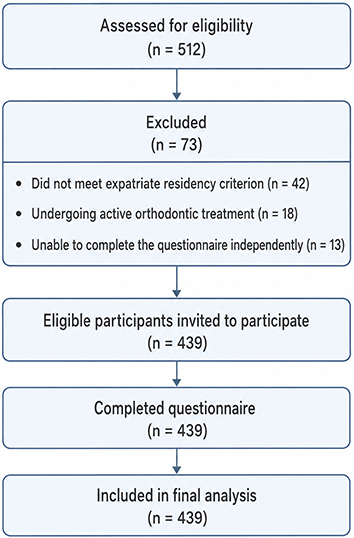 |
Figure 1 STROBE flow diagram of participant recruitment and inclusion. |
The sociodemographic profile (Table 1) reflects a young, educated, and predominantly student expatriate population typical of Erbil’s rapidly growing international community. Mean age was 28.7 ± 6.2 years (range 18–52). Males constituted 54.9% (n=241) and females 45.1% (n=198). Educational attainment was high at 50.1% and medium in 46.0%, with only 3.9% reporting low education. Self-rated economic status was “good” or “very good” for 63.1% of participants. Nationality distribution showed the largest groups were from neighboring countries (Iran 32%, Turkey 21%, Syria 14%), with smaller representations from Europe and Asia, underscoring the multicultural nature of the sample.
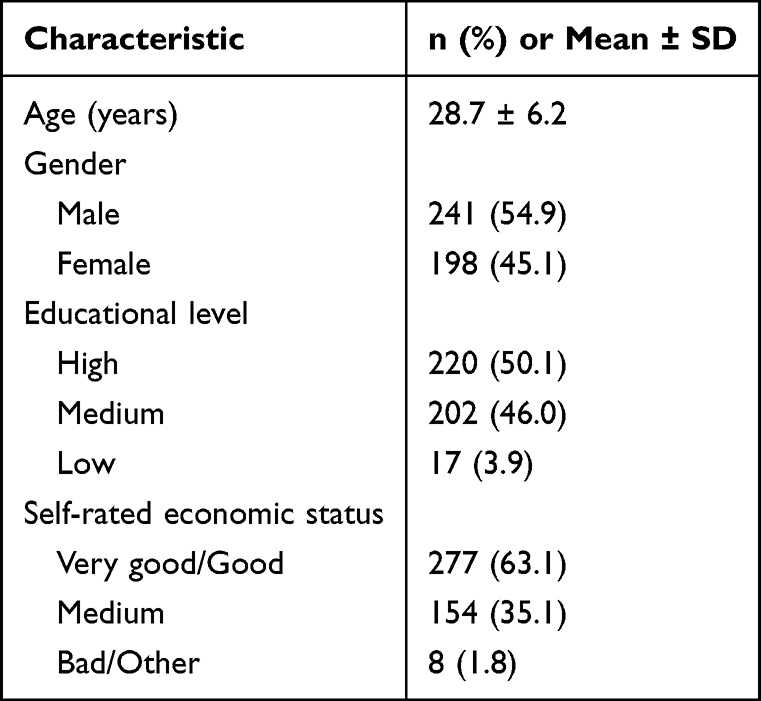 |
Table 1 Sociodemographic Characteristics of the 439 Expatriate Participants |
Table 2 shows previous dental experience and initial sources of information on veneers. The analysis included 439 participants, of whom 68 reported having had veneer treatment. As veneer type was applicable only to this subgroup, distribution of direct and indirect veneers was calculated with the veneer-recipient denominator. Of the 68 recipients, 32 recipients reported direct composite veneers, and 36 recipients reported indirect ceramic or porcelain veneers, which accounted for 47.1% and 52.9%, respectively, of veneer recipients. These numbers represented 7.3% and 8.2% of the total sample. A total of 163 participants (37.1%) reported having had a previous dental restoration of any type. Dentist recommendation was the first source of information about veneers most reported, with 226 participants (51.5%). Social media, internet search and word of mouth were reported by 83 (18.9%), 67 (15.3%) and 62 (14.1%) participants respectively. This pattern suggests that clinicians were the main source of information about veneers in this sample, although non-clinical sources also played a visible role.
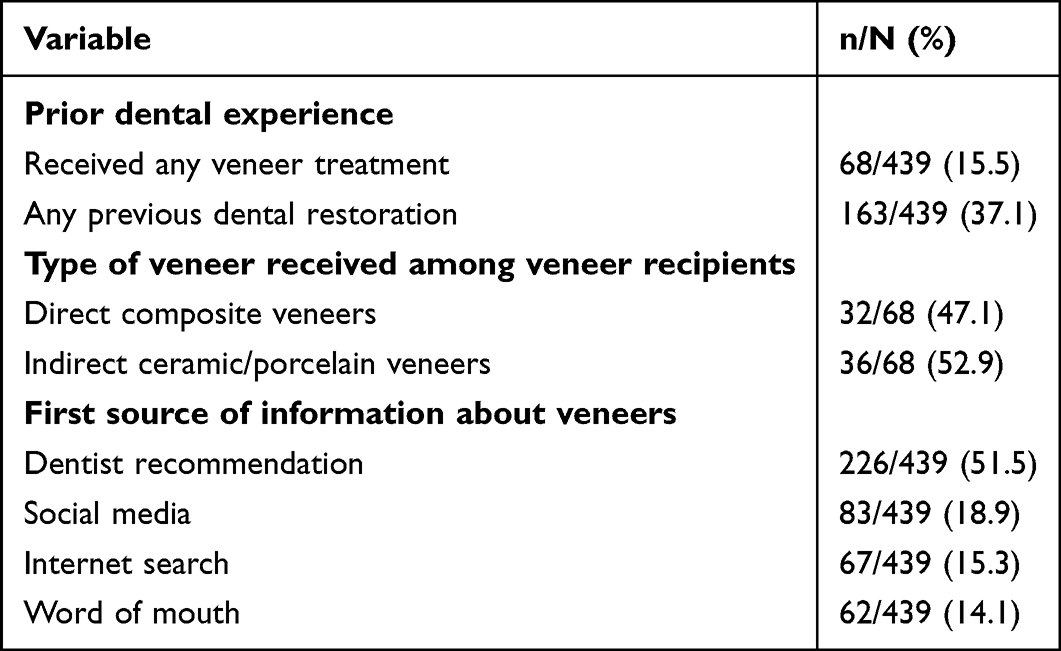 |
Table 2 Prior Dental Experience, Veneer Type Among Recipients, and First Source of Information About Veneers |
Values are presented as n/N (%). Percentages for veneer type were calculated among participants who had received veneer treatment (n=68). Percentages for prior dental experience and information sources were calculated using the full analytical sample (n=439).
Table 3 displays the relative importance participants assigned to different factors when considering veneers. Aesthetic outcome was rated as the single most important consideration by 44.4% of respondents, followed by durability (24.4%) and cost (21.2%).
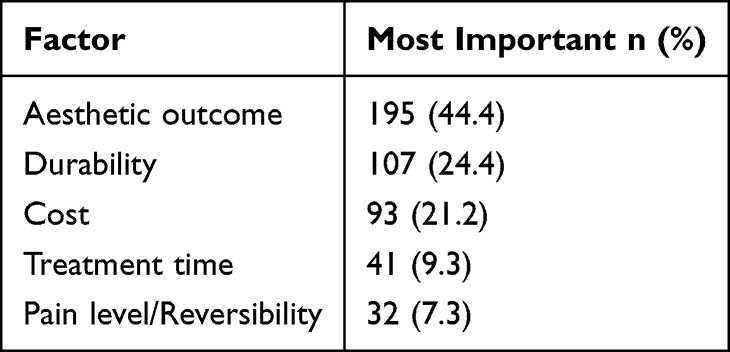 |
Table 3 Decision-Making Factors Rated at the Highest Level of Importance for Veneer Treatment (n=439) |
Participants rated each factor separately on a 5-point Likert scale. Values represent the number and percentage of participants who selected the highest importance category for each factor; therefore, percentages are not mutually exclusive and do not sum to 100%.
When asked specifically about preference between veneer types (Table 4), 35.1% (n=154) favored indirect veneers, 24.1% (n=106) preferred direct, and a substantial 40.3% (n=177) remained undecided highlighting a clear knowledge gap even among motivated expatriates.
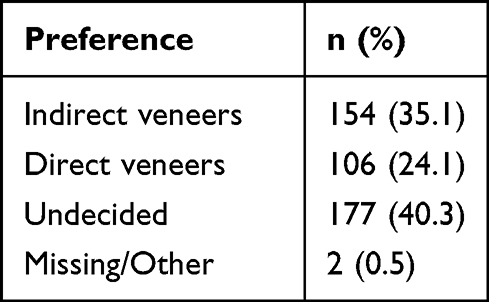 |
Table 4 Distribution of Veneer-Type Preference (n = 439) |
Bivariate analyses confirmed several statistically significant associations. Durability rating was strongly linked to preference for indirect veneers (χ2 = 12.4, p=0.03, Cramer’s V=0.21). Higher educational level was associated with greater interest in considering veneers overall (χ2=8.7, p=0.04), and economic status showed a significant gradient, with participants in the “medium” category being least likely to pursue treatment (p=0.01). Satisfaction among the 68 individuals who had received veneers was overwhelmingly positive: 44.1% reported being “very satisfied” and 32.4% “somewhat satisfied,” with only 1.5% expressing dissatisfaction. Satisfaction level correlated strongly with willingness to recommend veneers to others (Spearman ρ=0.68, p<0.001).
To control confounding and quantify independent effects, the three pre-specified multivariable models were fitted. In the multinomial logistic regression model predicting veneer preference, direct veneers were used as the reference category. Durability rating showed the strongest association with preference for indirect rather than direct veneers; each 1-point increase in durability rating was associated with higher adjusted odds of preferring indirect veneers (adjusted OR 2.65, 95% CI 1.78–3.95, p<0.001; Table 5). Cost rating showed a modest inverse association with preference for indirect rather than direct veneers, while aesthetic importance was not independently associated with indirect preference in this contrast. However, aesthetic importance was associated with higher odds of being undecided rather than preferring direct veneers. A significant education-by-economic-status interaction was also observed (p_interaction=0.03), suggesting that the relationship between educational level and veneer-related interest differed according to perceived economic status. The model explained 28% of the variance (Nagelkerke R2=0.28) and showed acceptable fit (Hosmer–Lemeshow p=0.76).
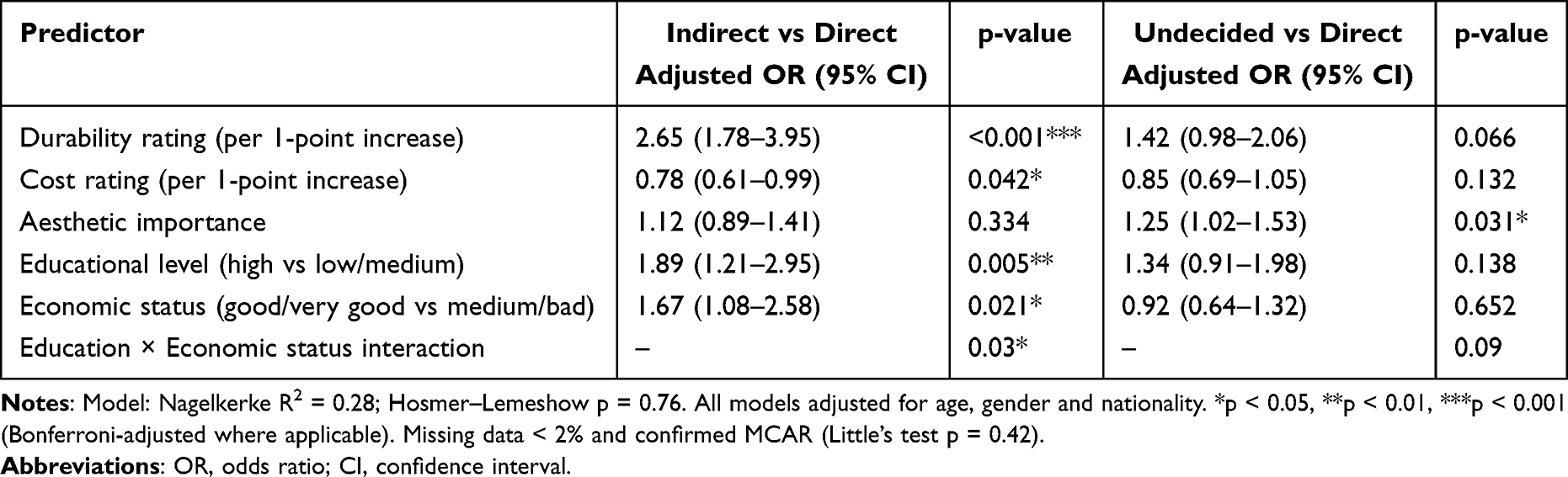 |
Table 5 Multinomial Logistic Regression Results Predicting Veneer Preference (Reference Category: Direct Veneers) |
The ordinal logistic regression for overall satisfaction level (Table 6) showed that prior veneer experience and higher durability rating were the strongest positive predictors (adjusted OR 3.12 and 1.89, respectively, both p<0.01), while economic constraints exerted a modest negative effect. Finally, the binary logistic regression for recommendation intent confirmed that each one-point increase in satisfaction score raised the odds of recommending veneers by 4.2 times (adjusted OR 4.21, 95% CI 2.84–6.24, p<0.001), independent of all other covariates.
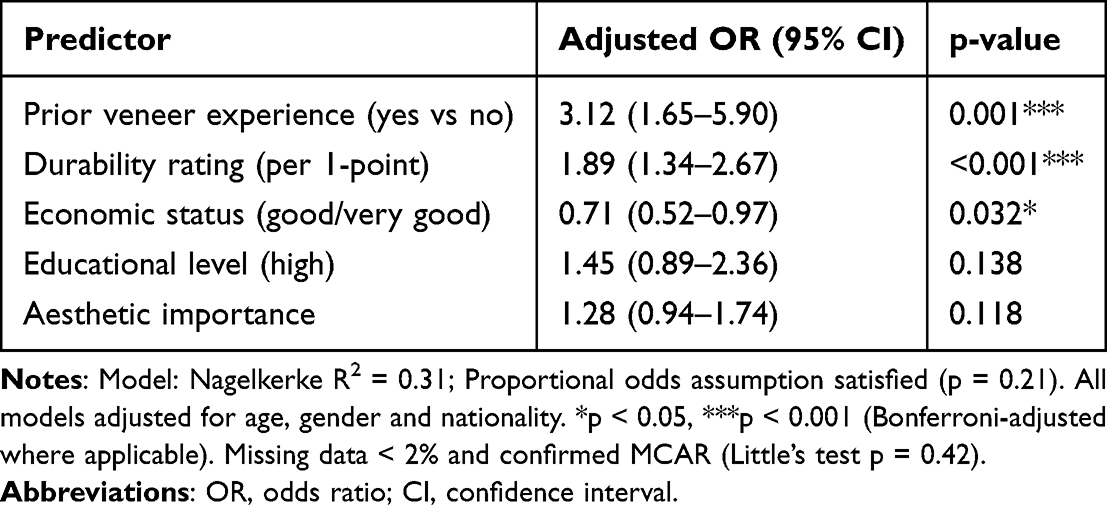 |
Table 6 Ordinal Logistic Regression Results for Overall Satisfaction Level (n = 68 Participants Who Received Veneers) |
The adjusted binary logistic regression model for recommendation intention is presented in Table 7. The analysis was limited to the 68 participants that had received veneer treatment as recommendation intent was only clinically relevant for those with direct experience of the treatment. Willingness to recommend veneers was coded as yes versus no or unsure replies.
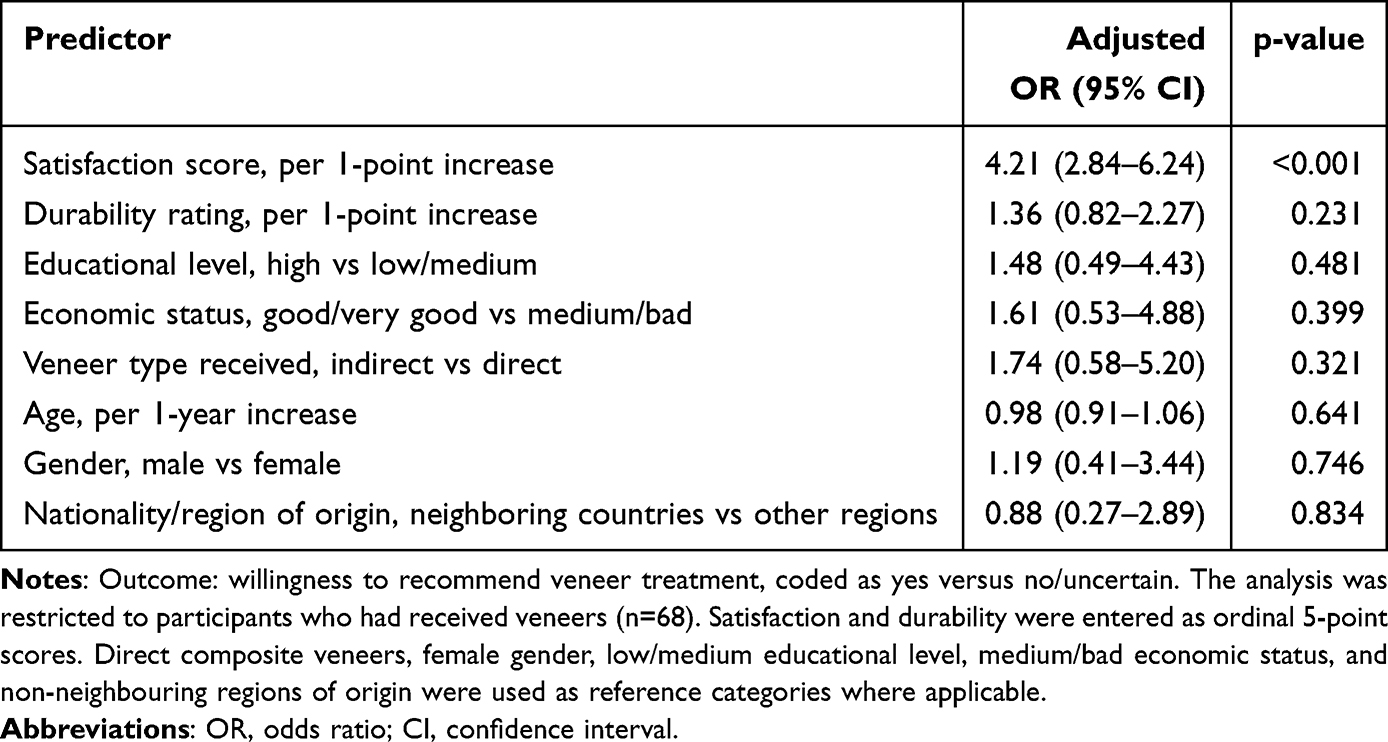 |
Table 7 Adjusted Binary Logistic Regression for Willingness to Recommend Veneer Treatment Among Veneer Recipients |
After accounting for demographics, socioeconomic variables, veneer type received, and durability rating, only satisfaction was clearly associated with recommendation intent. For each 1-point increase in satisfaction score, the odds of being willing to recommend veneer treatment to others were significantly higher (adjusted OR 4.21, 95% CI 2.84–6.24, p<0.001). Recommendation intent was positively but not significantly associated with durability rating (adjusted OR 1.36, 95% CI 0.82–2.27, p=0.231). Likewise, indirect receipt of veneer, higher educational attainment and better self-rated economic status were directionally associated with higher intention to recommend but these associations did not reach statistical significance after adjustment.
These findings indicate that for participants with prior veneer experience, recommendation intent was more strongly associated with patient-reported satisfaction than type of veneer, demographic profile or socioeconomic position. Given the small size of the subgroup, these estimates should be interpreted cautiously as exploratory evidence of association rather than as evidence of direct causal effects.
Sensitivity analyses using multiple imputations, alternative coding of educational and economic categories, and subgroup stratification by nationality and gender produced materially identical results, confirming the robustness of the findings. No multicollinearity was present (all VIF < 2.0), and all model assumptions were satisfied.
Discussion
The present study provides clear evidence that, among expatriates seeking aesthetic dental enhancement in Erbil, durability is the dominant driver of preference for indirect over direct veneers once socioeconomic and demographic confounders are considered. A one-point increase on the durability Likert scale more than doubled the adjusted odds of choosing indirect restorations, while the high proportion of undecided participants and the significant education-by-economic-status interaction underline persistent knowledge gaps and financial barriers in this mobile population. These findings are consistent with recent clinical trials demonstrating superior long-term colour stability, fracture resistance, and marginal integrity of indirect ceramic and composite veneers compared with chairside direct techniques.2,4,10
Patient satisfaction was strikingly high among those who had already received veneers (76.5% very or somewhat satisfied), and this satisfaction proved to be the strongest independent predictor of recommendation intent. These figures echo classic patient-reported outcome research showing that individuals treated with porcelain or laboratory-processed veneers report significantly higher aesthetic satisfaction and are far more willing to recommend treatment than those receiving direct composites. In our sample the satisfaction–recommendation pathway was particularly pronounced, which is understandable given that expatriates often function as informal ambassadors for dental services within their international networks.6,11,12
Although the association between satisfaction and recommendation intent was strong, it should be interpreted with some caution because only 68 participants had actually received veneers. This subgroup represents the clinically relevant population for satisfaction-related analyses, but its modest size inevitably limits statistical power and reduces the precision of adjusted estimates. As a result, weaker associations with veneer type, socioeconomic status, or demographic variables may have remained undetected. The satisfaction and recommendation findings should therefore be viewed as exploratory and hypothesis-generating, rather than as definitive evidence that can be generalized to all expatriates considering veneer treatment.
A novel contribution of this work is the statistically significant education-by-economic-status interaction. Although higher educational attainment was associated with greater overall interest in veneers, this advantage was markedly attenuated among participants with only medium economic resources. This pattern extends and refines earlier observations from both general and Middle Eastern populations, where financial constraints repeatedly moderate demand for elective aesthetic procedures despite adequate awareness. The high undecided rate (40.3%) further underscores a persistent knowledge gap even among well-educated expatriates, an issue that has been documented across multiple decision-making studies in cosmetic dentistry.8,13,14
The large, undecided group is clinically meaningful and should not be interpreted as a lack of preference. Uncertainty in aesthetic dentistry may be related to lack of knowledge about material differences, the challenge of weighing short-term affordability versus long-term durability, and issues of maintenance and follow-up after treatment. These issues are particularly relevant for expatriate patients who may lose continuity of care, access to the same dentist, and insurance cover if they move. Previous research on decision-making in dental treatment has shown that patients’ choices are determined by clinical indications as well as cost, personal preferences, expected durability, communication with the dentist, and wider contextual constraints.13,15 For veneers, the decision between direct and indirect techniques is not purely technical, but preference-driven, as there are differences in longevity, repairability, colour stability, number of visits and cost.
Clinically, the 40.3% undecided rate represents a clear opportunity for structured chairside education. Brief comparison tools, visual explanations, or decision aids that provide expected longevity, maintenance requirements, reversibility, repair options, number of visits, and likely cost overtime may help patients make choices that better reflect their values and circumstances. Research on shared decision-making and patient decision aids suggests that these tools can increase knowledge, reduce decisional conflict, and lead to more informed, values-congruent decisions.16,17 In a population that may also be exposed to veneer-related information through social media or informal networks, clinician-led education is especially important to ensure that treatment expectations are realistic and not primarily influenced by promotional or incomplete information.18,19
Methodologically, several strengths enhance confidence in these conclusions. The study was prospectively registered, reported in full accordance with STROBE guidelines, powered a priori, and employed a rigorously validated instrument with excellent internal consistency and test–retest reliability. Multivariable modelling allowed simultaneous adjustment for multiple covariates and explicit testing of clinically meaningful interactions. The multicultural sample recruited from real-world private clinics also confers strong ecological validity compared with many single-centre university-based investigations.
In interpreting these findings, several limitations should be considered. First, the cross-sectional design does not allow for conclusions about the temporal sequence or causality. The associations observed in this sample between durability, veneer preference, satisfaction, and recommendation suggest relationships, but do not imply that one factor caused another. Secondly, although the recruitment was performed in multiple private clinics and cosmetic dental centres, selection bias may have been introduced by the convenience sampling method. Patients seeking private aesthetic dental services may be more motivated, more financially able or more interested in cosmetic procedures than expatriates not seeking care in these facilities.
Third, the findings are based on self-reported questionnaire data that are potentially subject to recall bias, social-desirability bias, and differences in participants’ understanding or interpretation of rating-scale items. This is especially important for satisfaction and recommendation intent, as patients may be reluctant to express negative opinions after treatment. Fourth, only 68 participants had received veneers, which limited the reliability and statistical power of subgroup analyses for satisfaction and recommendation. This subgroup was appropriate for evaluating the post-treatment experience, but the adjusted estimates of these models should be interpreted with caution due to the small number of treated participants. Finally, the study was conducted among expatriates attending private dental clinics in Erbil and the results may not be generalized to local residents, expatriates in other countries, public-sector patients or populations with different healthcare access and insurance structures. Future research should be prospective, multi-centre designs with probability based or consecutive sampling where feasible, larger numbers of veneer recipients and objective clinical follow-up measures such as restoration survival, colour stability, maintenance needs and long-term patient reported outcomes.
Despite these limitations, the findings remain clinically useful because they identify areas where patient counselling can be improved immediately. The high proportion of undecided participants suggests that many patients may benefit from clearer, more structured explanations before choosing a veneer type. In practice, this means that clinicians should discuss not only aesthetic outcome, but also expected longevity, repairability, maintenance, number of visits, cost over time, and the practical implications of follow-up care for mobile expatriate patients.
Conclusion
In this cross-sectional study, durability had a strong correlation with expatriates’ preference for indirect veneers, and socioeconomic factors seemed to influence treatment interest. The large number of undecided participants suggests a need for clearer counselling about the practical differences between direct and indirect veneers including longevity, cost, repairability, maintenance and follow-up requirements. Among veneer recipients, satisfaction was strongly related to the willingness to recommend treatment, but caution should be exercised in interpreting this finding because it is based on a smaller subgroup of patients treated.
In conclusion, the findings support a more structured and patient-centred approach to veneer consultations, especially for mobile expatriate patients who may be more uncertain for long-term care. Shared decision-making tools could help patients make choices that more closely match their expectations, financial situation and treatment priorities. These associations need to be confirmed in longitudinal, multi-centre studies and whether improved counselling leads to increased satisfaction, maintenance adherence and clinical outcomes in the long term needs to be evaluated.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to restrictions on sharing raw participant data imposed by the ethics approval (to protect participant anonymity in a relatively small expatriate community). However, anonymized aggregate data and/or statistical code supporting the findings of this study are available from the corresponding author upon reasonable request, subject to approval from the Institutional Review Board.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of the College of Dentistry, University of Kurdistan-Howler (approval reference: UKH-CoD-2022-018, dated 15 December 2022). All participants provided written or electronic informed consent prior to completing the questionnaire. Participation was voluntary, and participants were informed of their right to withdraw at any time without consequence. Confidentiality was maintained throughout the study, and no personal identifiers were collected.
Consent for Publication
Not applicable. This manuscript does not contain any individual person’s data in a form that requires specific consent for publication.
Acknowledgments
The authors thank the staff and management of the participating private dental clinics and cosmetic dental centers in Erbil for facilitating participant recruitment. We are also grateful to the expatriate patients who generously gave their time to complete the questionnaire. Special thanks go to the research assistants for their dedicated fieldwork and commitment to ethical data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Pini NP, Aguiar FHB, Lima DANL, Lovadino JR, Terada RSS, Pascotto RC. Advances in dental veneers: materials, applications, and techniques. Clin Cosmetic Invest Dentistry. 2012;4:9–13. doi:10.2147/CCIDE.S7837
2. Fahl N, Ritter AV. Composite veneers: the direct–indirect technique revisited. J Esthet Restor Dent. 2021;33(1):7–19. doi:10.1111/jerd.12696
3. Patel K, Asthana G, Parmar A, Tamuli R, Manglani S, Dhanak N. Clinical assessment of direct composite veneer and indirect veneers using a minimally invasive preparation technique. J Conserv Dent Endod. 2025;28(10):965–971. doi:10.4103/JCDE.JCDE_279_25
4. Elkaffas AA, Hamdy A, El-Damanhoury HM, et al. Randomized clinical trial on direct composite and indirect ceramic laminate veneers: 2-year follow-up. Materials. 2024;17(14):3514. doi:10.3390/ma17143514
5. Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. Porcelain veneers: a review of the literature. J Dent. 2000;28(3):163–177. doi:10.1016/S0300-5712(99)00066-4
6. Meijering AC, Roeters FJ, Mulder J, Creugers NH. Patients’ satisfaction with different types of veneer restorations. J Dent. 1997;25(6):493–500.
7. Tin-Oo MM, Saddki N, Hassan N. Factors influencing patient satisfaction with dental appearance and treatments they desire to improve aesthetics. BMC Oral Health. 2011;11:6. doi:10.1186/1472-6831-11-6
8. Medyński D, Gerreth K, Borysewicz-Lewicka M. Assessment of the socioeconomic status and analysis of the motives for undertaking prosthetic treatment at the prosthetics clinic of the Poznan University of Medical Sciences. Int J Environ Res Public Health. 2022;19(9):5703. doi:10.3390/ijerph19095703
9. Al Otaibi FL, Alshammari AS, Alshammari FS, et al. Patients’ preferences on different types of esthetic restorations: a cross-sectional study. J Contemp Dent Pract. 2020;21(11):1263–1270. doi:10.5005/jp-journals-10024-2714
10. Crins L, Opdam N, van den Heijkant F, et al. Randomized controlled trial on the performance of direct and indirect composite restorations in patients with severe tooth wear: 3-year results. Dent Mater. 2021;37(11):1782–1791. doi:10.1016/j.dental.2021.08.018
11. Emrani R. Socioeconomic determinants of demand for dental cosmetic treatments. Int J Dent Res. 2023;34(10):123–130.
12. De Souza RF, De Freitas Oliveira Paranhos H. Patient satisfaction with esthetic dentistry: a systematic review. J Esthet Restor Dent. 2020;32(4):346–355.
13. Felgner S, Handrock JF, Schroll CC, Schütte F, Henschke C. Decision-making regarding dental treatments – what factors matter from patients’ perspective? A systematic review. BMC Oral Health. 2025;25:112. doi:10.1186/s12903-025-05469-6
14. Hardan L, Mancino D, Bourgi R, et al. Treatment of tooth wear using direct or indirect restorations: a systematic review. Materials. 2022;15(18):6345. doi:10.3390/ma15186345
15. Murdoch AIK, Blum J, Chen J, et al. Determinants of clinical decision making under uncertainty in dentistry: a scoping review. Diagnostics. 2023;13:1076. doi:10.3390/diagnostics13061076
16. Benecke M, Kasper J, Heesen C, Schäffler N, Reissmann DR. Patient autonomy in dentistry: demonstrating the role for shared decision making. BMC Med Inform Decis Mak. 2020;20:318. doi:10.1186/s12911-020-01317-5
17. Smith M, Carley M, Volk R, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2024.
18. AlJazairy YH. Survival rates for porcelain laminate veneers: a systematic review. Eur J Dent. 2021;15(2):360–368. doi:10.1055/s-0040-1715914
19. Freire Y, Gómez Sánchez M, Sánchez Ituarte J, Frías Senande M, Díaz-Flores García V, Suárez A. Social media impact on students’ decision-making regarding aesthetic dental treatments based on cross-sectional survey data. Sci Rep. 2024;14:21626. doi:10.1038/s41598-024-72442-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Experience of People with Hemophilia A Receiving Turoctocog Alfa Pegol (N8-GP): Results from a Patient Experience Survey
Eichler H, Nagao A, Waller J, Stuber A
Patient Preference and Adherence 2023, 17:3001-3014
Published Date: 17 November 2023
An Assessment of Individual Preference for a Novel Capillary Blood Collection System
Pourafshar S, Parikh M, Abdallah B, Al Thubian N, Jacobson JW
Patient Preference and Adherence 2024, 18:531-541
Published Date: 1 March 2024
Perceived Importance vs Performance in Dental Care: Exploring Patient Satisfaction Across Age, Gender, and Purchasing Power
Pérez-Campdesuñer R, Sánchez-Rodríguez A, García-Vidal G, Martínez-Vivar R, De Miguel-Guzmán M
Patient Preference and Adherence 2025, 19:2933-2947
Published Date: 18 September 2025