")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
Patient Perspectives of Disease Activity, Medications and Substance Use in People with Fibromyalgia
Authors Khoo T , Hill CL , Hoon E, Whittle S
Received 9 February 2022
Accepted for publication 14 April 2022
Published 5 May 2022 Volume 2022:14 Pages 87—95
DOI https://doi.org/10.2147/OARRR.S361804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Thomas Khoo,1 Catherine L Hill,1– 3 Elizabeth Hoon,4,5 Samuel Whittle1
1Rheumatology Unit, The Queen Elizabeth Hospital, Adelaide, South Australia, Australia; 2Rheumatology Unit, The Royal Adelaide Hospital, Adelaide, South Australia, Australia; 3Discipline of Medicine, University of Adelaide, Adelaide, South Australia, Australia; 4Discipline of General Practice, University of Adelaide, Adelaide, South Australia, Australia; 5School of Public Health, The University of Adelaide, Adelaide, South Australia, Australia
Correspondence: Thomas Khoo, Rheumatology Unit, The Queen Elizabeth Hospital, Adelaide, South Australia, 5011, Australia, Email [email protected]
Objective: To explore patient perspectives on disease activity and experiences, as well as medication use of a group of fibromyalgia patients attending a single-centre rheumatology public hospital outpatient setting.
Methods: Patients seen in fibromyalgia clinic within a rheumatology unit from July 2016 to December 2019 were posted a voluntary survey with questionnaires pertaining to patient-reported measures of disease impact (FIQR), fatigue (MFI-20) and psychological distress (K10). A free-text section allowed description of disease impact. Patients were also asked to record medication use and comorbidities, which were then compared to the electronic medical records (EMR) of the overall clinic cohort.
Results: Forty-five patients responded to the survey (43/45, 95.6% female; mean age 56.5 years). Respondents had generally severe fibromyalgia (mean FIQR 67.1/100, range 23.7– 92.8), moderate psychological distress (mean K10 27.5/50, range 14– 45) and high fatigue (mean MFI 74.9/100, range 40– 96). Free-text responses generated themes of pervasive disease impact and the necessity of adjusting life around unpredictable symptoms. Almost half reported opioid (21/45, 46.7%) and gabapentinoid (19/45, 42.2%) use. 16/41 (39%) use cannabinoids for their fibromyalgia symptoms. Comparing medication use with survey non-respondents (n=85), there was generally similar representation except for significantly greater NSAID use among survey respondents (33/45, 73.3% vs 22/85, 25.9%, p< 0.001).
Conclusion: For patients living with fibromyalgia in this study, there were high levels of disease activity, psychological distress and fatigue. Patients described the need to accept disease-imposed limitations and life adjustments. Almost half reported opioid use, despite evidence suggesting poor efficacy and possible harm.
Keywords: fibromyalgia, comorbidity, analgesics, opioid, cannabinoids, anti-inflammatory agents
Introduction
Fibromyalgia is a condition characterised by symptoms including chronic widespread pain, hyperalgesia and allodynia.1 It is estimated to affect 2–8% of the population2 and imparts a significant burden not just on patients’ quality of life and participation, but also the healthcare system.3
Despite these burdens, fibromyalgia is still poorly understood. While thought to involve aberrant central pain processing mechanisms perpetuating an abnormal experience of pain, peripheral and local factors may also constitute triggering events.4 Furthermore, physical inactivity and fear avoidant behaviour as a result of fibromyalgia may themselves result in deconditioning and secondary pathology such as tendinopathies and bursitis.5
Treatment of fibromyalgia is particularly challenging given the poorly elucidated mechanisms of disease and the complex phenomenology of chronic pain. Pharmacological approaches thus far have focused on increasing serotonin/noradrenaline with reuptake inhibitors or enhancing inhibitory pathways involving the neurotransmitter gamma-aminobutyric acid (GABA).6 Non-pharmacological interventions, though, are at least as important with regular exercise in patients with fibromyalgia being associated with improved quality of life, patient-reported well-being, improved mood and lower work absence.7
There is a need to better characterise the patient experience of fibromyalgia including the use of both pharmacological and non-pharmacological interventions. With the recognition that patients often use non-prescribed drugs and therapies which may not be discussed or disclosed during the medical consultation, there is also a need to detect discrepancies between physician and patient expectations of management. With this, there may be greater opportunity for effective collaboration in dealing with a complex heterogeneous disease for which there are still few effective evidence-based management strategies.
Methods
Patients seen in the Fibromyalgia Clinic of The Queen Elizabeth Hospital Rheumatology Unit, between 1st July 2016 and 30th November 2019, were invited to complete a mailed survey. Ethics approval was obtained from the Central Adelaide Local Health Network Human Research Ethics Committee (protocol number 12669, approved 30th January 2020). Written informed consent was obtained from each patient for inclusion of survey results in this research and for publication. This research was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
The survey included questions about age, gender, comorbidities and medication use as well as other substance use (smoking, alcohol, cannabis and other recreational drugs).
In addition, three validated questionnaires were included in the survey to assess patient-reported disease activity and symptom scores. The revised fibromyalgia impact questionnaire (FIQR) comprises 21 questions separated into three domains (fibromyalgia symptoms, functional impairment and overall disease impact) wherein patients rate the severity of their experiences from 0 to 10.8
The multidimensional fatigue inventory (MFI-20) is a set of 20 statements covering the dimensions of general, physical and mental fatigue as well as reduced activity and motivation. Respondents rate their agreement with statements on a scale of 1 to 5 with reversed scoring of statements which detract from fatigue. It has predominantly been used and validated in cancer research and cancer-related illness9 but has also been previously utilised in studies about fibromyalgia10 and chronic fatiguing illnesses.11
The Kessler 10 psychological distress scale (K10) is a validated screening tool in community healthcare for the likelihood of having a mental disorder. It involves 10 questions covering common symptoms of depression and anxiety with respondents rating on a scale of 1 to 5 how much they have felt each symptom over the preceding four weeks.12 It has not previously been used in studies of fibromyalgia.
The survey concluded with a free-text question, “Is there anything else that you would like to tell us about your fibromyalgia?”. Responses to this question were analysed using thematic analysis with a semantic focus,13 to identify commonly reported informative themes.14 The data were coded with the assistance of NVivo12 software, with input to the initial coding by an experienced qualitative researcher. This thematic analysis produced themes and sub-themes that elaborated the quantitative results through providing detail of respondents’ subjective lived experiences, attitudes and priorities in managing their condition. Inclusion of these qualitative findings adds depth and value to the respondents’ quantitative symptoms scores.
In order to assess how representative survey respondents were of the broader Fibromyalgia Clinic population, self-reported medication use and comorbidities were subsequently compared with the Electronic Medical Records (EMR) documentation. This EMR system is completed by clinicians on each clinic encounter in the outpatient setting, designed to be regularly updated with new or changed information from patients as well as referral letters. The EMR does not yet have the capacity for the application of diagnostic criteria and consequently, the patient group was filtered to include those with “primary fibromyalgia syndrome”, “chronic widespread pain” or “widespread non-inflammatory pain” in the clinician reported “reason for visit” section of the clinic letter. Medication use and comorbidities were compared between survey responders and non-respondents using Fisher’s Exact Test.
Results
Forty-five patients (34.6% of the clinic population of 130 patients with fibromyalgia) responded to the posted survey (95.6% female) and were in general older than survey non-responders (mean age 56.5 years vs 47.9 years). Their self-reported medication use and comorbidities are included in Table 1. Almost half reported using opioids for their fibromyalgia (21/45, 46.7%) with the most commonly used opioid being tramadol, which significantly differed from survey non-responders (10/45, 22.2% vs 7/85, 8.2%, p=0.03). Gabapentinoids, predominantly pregabalin, were used by 19/45, (42.2%) and similar use was found in survey non-responders (31/85, 36.5%, p=0.71).
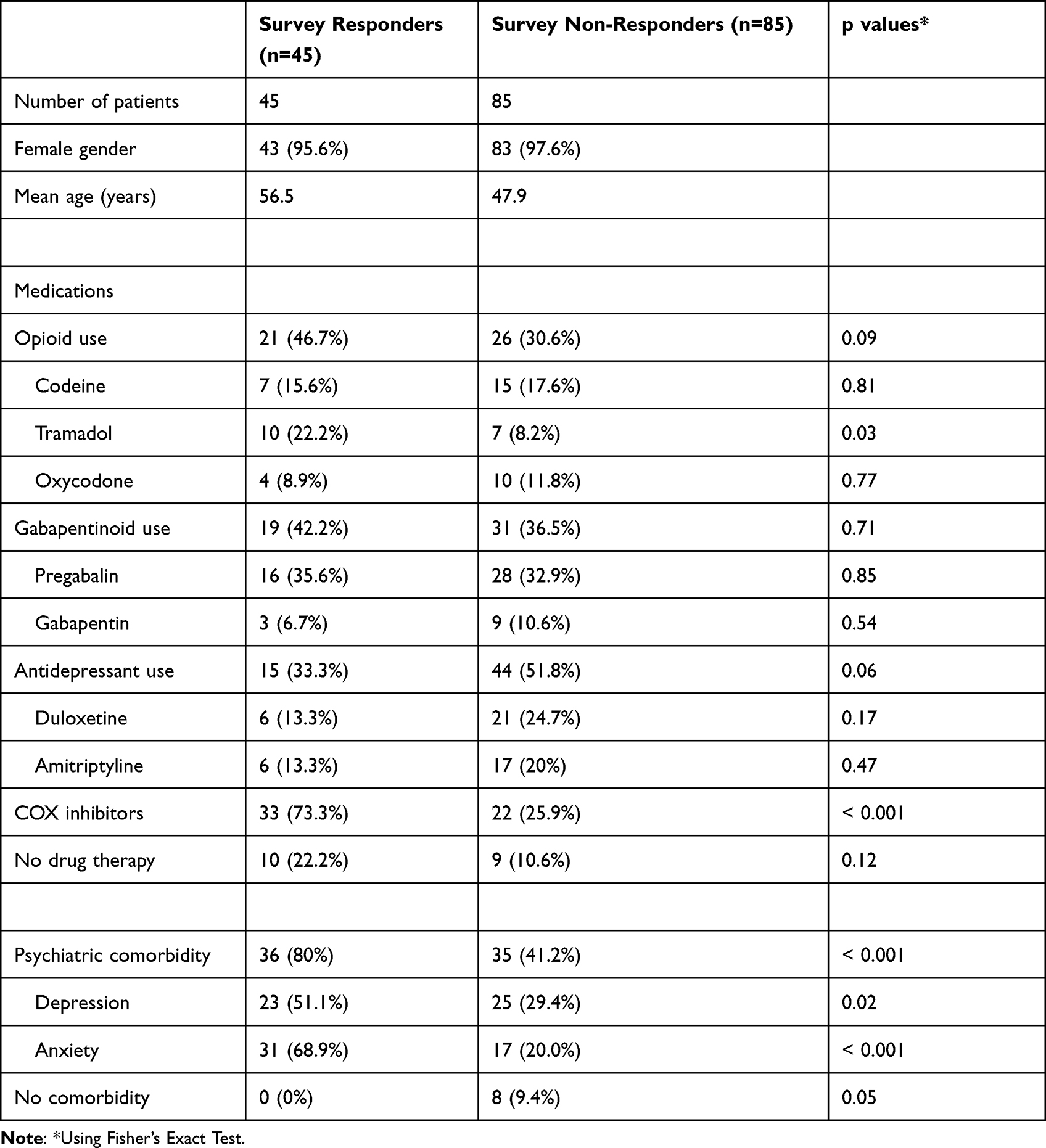 |
Table 1 Demographics, Medications and Comorbidities Comparing Survey Responses with Non-Responders (Information Drawn from Electronic Medical Records) |
Non-steroidal anti-inflammatory drug (NSAID) use was more commonly reported by survey respondents than documented in the EMR for survey non-responders (33/45, 73.3% vs 35/85, 41.2%, p < 0.001).
Of note, almost one-quarter of survey respondents reported not currently taking any medications (10/45, 22.2%).
Many more survey respondents reported a diagnosis of depression and/or anxiety compared with non-responders (36/45, 80% vs 35/85, 41.2%, p < 0.001).
Substance use is summarised in Table 2. 15/45 (33.3%) had smoked cigarettes previously and 7/45 (15.6%) were current smokers. 41/45 survey respondents answered the question, “Have you ever used cannabis or cannabis-derived products for your fibromyalgia?” Of these, 16/41 (39%) had used cannabinoids for fibromyalgia and the majority of these reported daily use (15/16) with nine of them using multiple times a day. The most common route of administration was via an oil-based oral preparation (7/16, 43.8%).
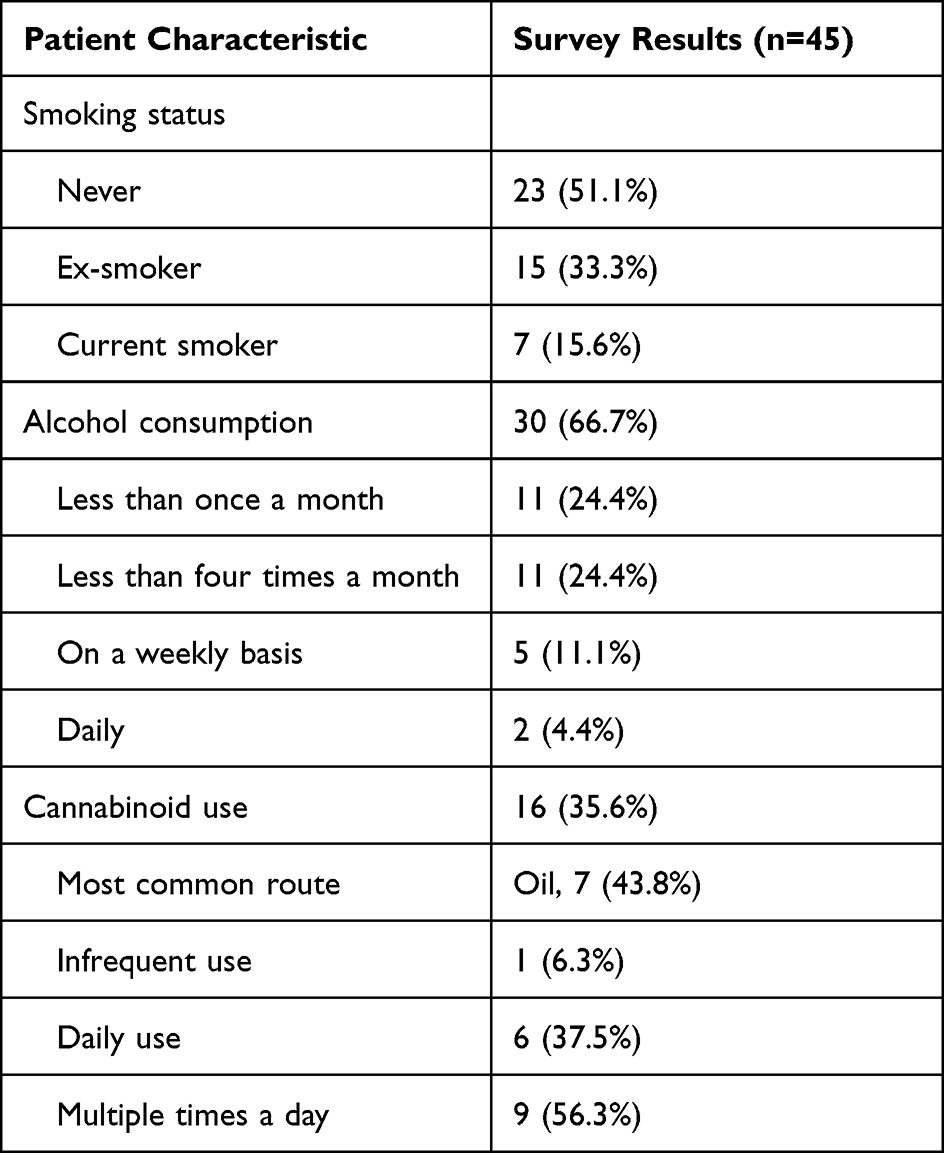 |
Table 2 Substance Use from Patient Completed Surveys |
All patients completed the disease activity and symptom score questionnaires and the results are summarised in Table 3. The mean score on the FIQR was 67.1 (range 23.7–92.8) falling into the severe fibromyalgia category (60–74). On the MFI-20 questionnaire, the mean scores were consistent with prominent fatigue (general fatigue – 17.9/20, physical fatigue – 16.3/20 and mental fatigue – 14.3/20) which were greater than those pertaining to motivation (reduced activity – 14.3/20 and low motivation – 12.3/20). Finally, on screening with the K10 scale, a minority of patients (8/45, 17.8%) were in the “mentally well” category, 10/45 (22.2%) respondents were rated as likely to have a mild mental disorder, 9/45 (20%) moderate and 18/45 (40%) severe.
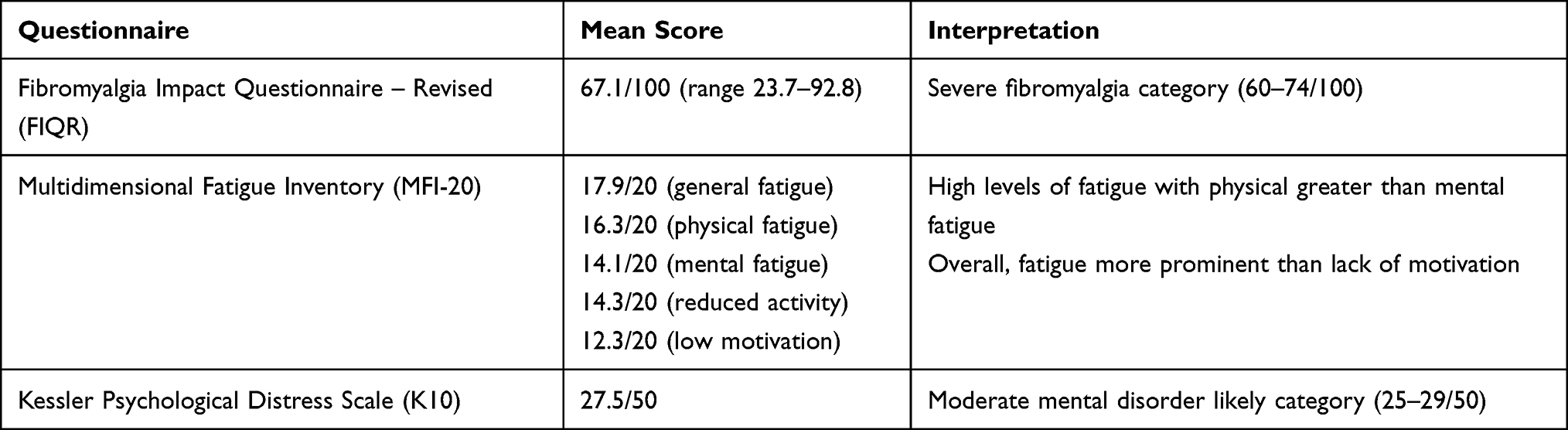 |
Table 3 Summary of Patient-Reported Questionnaire Results |
Twenty-four respondents answered the free-text question at the conclusion of the survey. The results of the qualitative analysis of these responses are in Table 4. The major themes were: the physical and psychological experience of fibromyalgia, adjusting live and living around the disease, and relating and interacting with others.
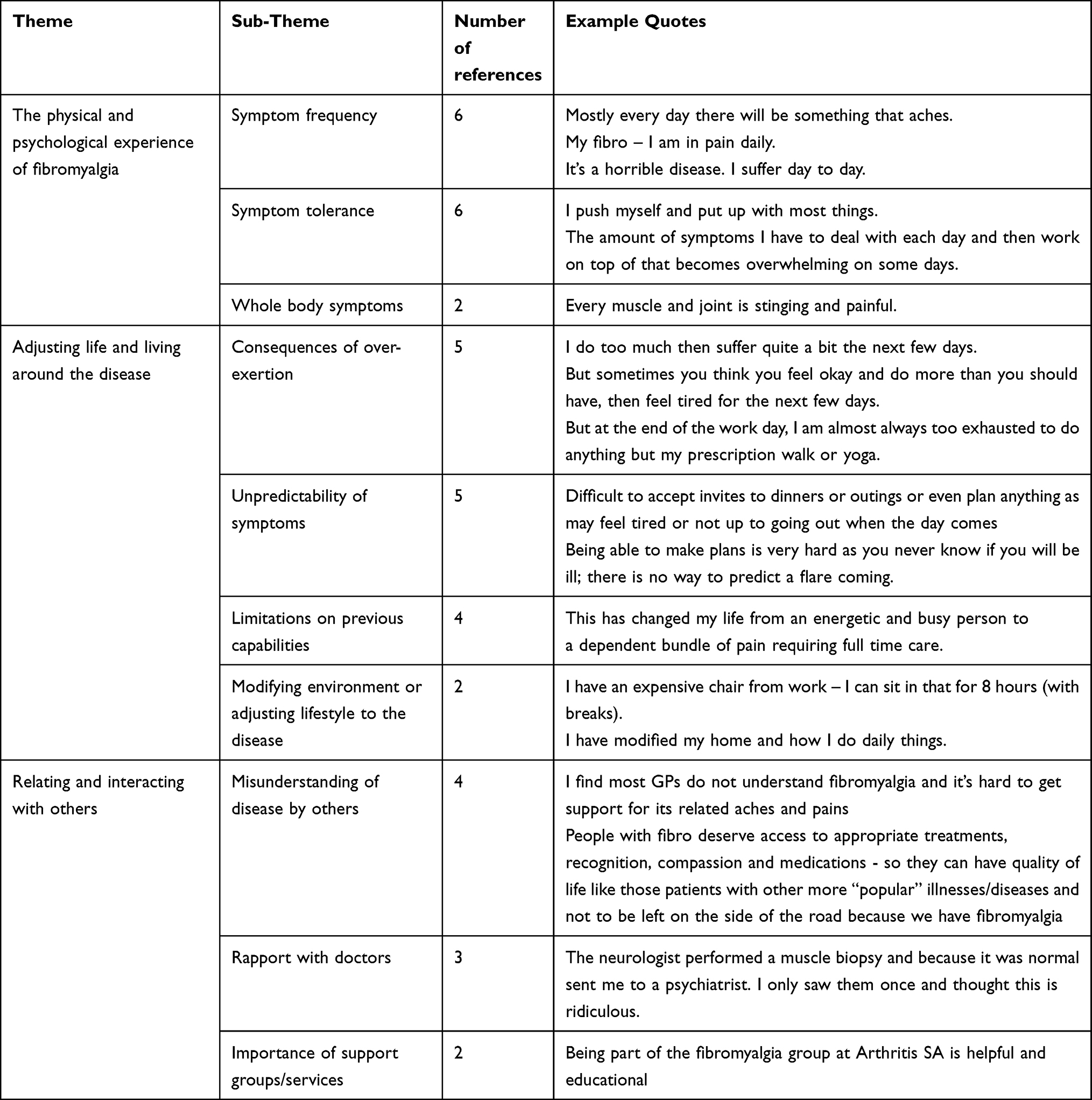 |
Table 4 Summary of Responses to Free-Text Question Including Examples of Quotes |
Respondents reported not only a wide symptom distribution, stating, “Every joint is stinging and painful” and “it affects eyes, hair, skin etc.” but also reported high symptom frequency, for example, “I’m in pain daily”, “Every day there will be something that aches” and “It’s a horrible disease. I suffer day to day.” Respondents also reported difficulties with functional tasks that are not covered in the FIQR and MFI-20. For example, participants reported that “chewing is difficult” and “just the height of putting arms above shoulder level makes me feel tired or ache”, suggesting that even these most basic necessities can be a challenge for people living with fibromyalgia.
Beyond this, respondents reported that functional impairment tended to fluctuate through time and that the unpredictability of impairment was debilitating. The reported necessity of adjusting their life and living around fibromyalgia was a prominent theme, exemplified in statements such as, “You never know if you will be ill, there is no way to predict a flare coming” and “I do too much then suffer quite a bit the next few days.”
With such a profound impact of fibromyalgia reported on patients’ lives, there was a broad range of levels of acceptance and adjustment evident, from comments such as, “It is a life of hopelessness and poverty. Waiting to what? Die. No life” to “I try to be as positive as I can. ‘This is what I have’ attitude and get on with things.”
Discussion
Fibromyalgia remains poorly understood in both its pathogenesis and the mechanisms of its perpetuation. The range of symptoms that it encompasses is broad and can sometimes be non-specific. Furthermore, it also lacks objective physical examination findings or laboratory markers to monitor disease activity and consequently relies strongly on patients’ articulation of their experiences as well as a focus on functional impairment as the final pathway of both physical and psychological symptoms.
Typically, a non-pharmacological approach to fibromyalgia treatment is first line. Education, exercise (including physical therapies) and cognitive behavioural therapy are the three main evidence-based therapies and their importance with or without medications should not be underestimated.2,15 The useful role of support groups was also highlighted in our study's qualitative responses.
Regarding pharmacotherapy, there is most evidence for the use of antidepressants including amitriptyline as well as serotonin and/or noradrenaline reuptake inhibitors16 and gabapentinoids.17 Though in clinical practice, combinations are often trialled due to inadequate relief with monotherapy, there is currently no trial evidence to support such an approach.18
One of the more concerning findings of the present study is that almost half of the survey respondents reported using opioids for fibromyalgia which were generally not prescribed by their rheumatologist. It is well recognised that in fibromyalgia, as with many other non-cancer conditions characterised by chronic pain, opioid use is associated with a risk of important adverse effects, as well as the potential for misuse, dependence and abuse.2,19 However, there is no trial evidence to support their use20 and in fact, they may be detrimental in the long term.21 Cerebrospinal fluid studies in patients with fibromyalgia have actually demonstrated raised endogenous opioid levels, supporting a model of decreased opioid sensitivity contributing to the experience of pain.22
Our findings highlight the ongoing importance of the rheumatologist in encouraging de-prescribing of opioids, educating on the detriments of inappropriate use and collaborating with patients and their general practitioners on alternative methods of symptom management.
Despite the lack of evidence to suggest a beneficial effect of NSAIDs in the treatment of fibromyalgia,23 73.3% of survey respondents reported using this class of medication for their fibromyalgia. This may be a result of NSAIDs being easily accessible over-the-counter, without a prescription. We were unable to reliably quantify this use and whether it was regular or as required. It is acknowledged that physical inactivity and fear avoidant behaviour as a result of fibromyalgia may result in deconditioning and secondary pathology such as tendinopathies and bursitis.5 Potentially, NSAIDs have a role in addressing these complications.
Almost a quarter of survey respondents reported no current fibromyalgia medication use. It is unclear whether this is due to their symptoms being adequately controlled with non-pharmacological methods or because they have ceased medications due to inefficacy or adverse effects.
It is well recognised that mood symptoms and a comorbid diagnosis of depression are common in fibromyalgia.24 A much higher proportion of survey respondents identified with a diagnosis of depression or anxiety than was found in the EMR of non-responders. This may reflect a selection bias though it is also possible that while patients may self-identify with symptoms of these diseases, formal diagnosis and inclusion in the EMR problem list is more stringent.
Medicinal cannabis has generated significant attention recently for a number of indications, one of which has been chronic pain25 and the results of our survey parallel this interest with more than a third of patients using non-prescribed cannabinoids for their fibromyalgia symptoms. Although there is limited evidence to support the use of cannabinoids in treating fibromyalgia,26 our survey adds further evidence that cannabis is currently widely used in this population.
Survey respondents in the present study had generally severe fibromyalgia on the fibromyalgia impact questionnaire (FIQR) with profound functional impairment. It is possible that a voluntary survey in a hospital outpatient setting may have selected for a group with very severe disease. It is also worth noting that in the index study testing of the FIQR, patients with dual diagnoses of fibromyalgia and depression were excluded given the intent to compare patient groups with each diagnosis whereas we did not do this given limitations of sample size.
Using the multidimensional fatigue inventory (MFI-20), survey respondents demonstrated generally high levels of fatigue with physical outweighing mental fatigue. On average, respondents also scored higher on fatigue scores than activity and motivation, suggesting that functional impairment stems more from the prominent fatiguing symptoms of fibromyalgia than a lack of impetus.
Though the Kessler 10 (K10) psychological distress scale has been used as a screening tool for depression and anxiety previously,12 it has not been used specifically in fibromyalgia in the literature. However, the high rates of respondents in this survey scoring in the medium or high level of psychological distress categories is of concern. Notably, however, two of the questions of the K10 pertain to fatigue and this may confound results because it is a common, prominent feature of fibromyalgia without necessarily implicating an underlying mood disorder.
Qualitative research in fibromyalgia has previously proved to be a powerful tool to describe the experiences of patients with this disease.27 Though the design and focus of the present study was not qualitative in nature, the open-ended free-text question at the conclusion of the survey offered an opportunity for analysis of patients’ perspectives as summarised in Table 4.
As an open-ended question at the conclusion of the survey, the responses received varied quite considerably, covering a broad range of experiences of fibromyalgia. Previous qualitative research has taken a more granular approach, focusing on flares of disease activity,27 the use of exercise28 and the importance of sleep.29
Though our study was not able to centre on any one of these specific features of fibromyalgia, it uniquely offered respondents an unprompted opportunity to discuss what they perceived to be of importance to their experience and which might otherwise be missed from quantitative symptom scores alone. The FIQR asks for the respondent to evaluate the last seven days, the MFI-20 how they have been feeling “lately” and the K10 the last month. Consequently, in asking respondents to examine a period of time, they are at risk of averaging the experience and obscuring certain characteristics of the patient experience of fibromyalgia, which were highlighted in the qualitative analysis, namely the unpredictability of its marked fluctuations and the avoidance of over-exertion for fear of subsequent exacerbation of impairment.
There are some salient limitations to our study. Analysis was limited by small sample size and a low response rate (34.6%) to the patient completed survey. Data collection from the EMR relied on physician diligence during consultations in updating the patient medication lists as well as problem lists which, within the time constraints of an appointment, may be compromised. This process is also reliant on other sources of information which may be of variable completeness – referrals from primary care providers and other specialists as well as patient recollection of their active medications. For this reason, we were unable to quantify medication dosing and in some situations, it was difficult to differentiate between regular and as-required usage. It was also difficult to gather information on what non-pharmacological approaches patients use for fibromyalgia and how effective they perceive these to be, though this would be an important consideration in future studies.
Though involving mixed quantitative and qualitative methodologies, our study was limited in its assessment of correlations between specific medications and patient attitudes. More targeted patient interviews or focus groups could explore patient perspectives on their drug and non-drug therapies as well as substance use, particularly cannabis given our finding of its frequent use in patients with fibromyalgia. This may also allow a more complete appreciation of why opioid use continues to be so prevalent in this patient group and what interventions could be trialled in addressing this problem.
Furthermore, the survey used in this study was extensive, covering thirty question domains and almost ninety individual questions. With a disease so characterised by fatigue, it is possible that this selected for patients with the energy and persistence to complete the survey.
Despite the length of the survey, many still responded to the final open-ended question. However, the comments made in response to this, though useful in contributing insights into lived experiences, cannot be interpreted to be representative of the whole sample or indeed, of patients with fibromyalgia in general.
Longitudinal assessment of patients with a particular focus on quantifying trends of medication use and questionnaire scores could also be a future option to better understand the fluctuations in disease activity described in qualitative responses as well as the efficacy or lack of effect of pharmacotherapy.
Conclusions
This cohort of patients with fibromyalgia, seen in a tertiary hospital outpatient setting, reported a concerning level of opioid use as well as the frequent use of cannabis for symptom management. They had high levels of fibromyalgia disease activity, functional impairment and comorbid psychiatric illness. Long-term and larger cohort studies spanning populations managed in hospital outpatients as well as in the community would yield more information on the complexities of this poorly understood condition, and eventually may cast light on more effective treatment strategies.
Disclosure
The authors report no conflicts of interest.
References
1. Sumpton JE, Moulin DE Fibromyalgia. Handbook of Clinical Neurology. 2014;119:513–527. doi:10.1016/b978-0-7020-4086-3.00033-3
2. Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555. doi:10.1001/jama.2014.3266
3. Annemans L, Le Lay K, Taieb C. Societal and patient burden of fibromyalgia syndrome. Pharmacoeconomics. 2009;27(7):547–559. doi:10.2165/11313650-000000000-00000
4. Staud R. Peripheral pain mechanisms in chronic widespread pain. Best Pract Res Clin Rheumatol. 2011;25(2):155–164. doi:10.1016/j.berh.2010.01.010
5. Cohen H. Controversies and challenges in fibromyalgia: a review and a proposal. Ther Adv Musculoskelet Dis. 2017;9(5):115–127. doi:10.1177/1759720X17699199
6. Chinn S, Caldwell W, Gritsenko K. Fibromyalgia pathogenesis and treatment options update. Curr Pain Headache Rep. 2016;20(4):25. doi:10.1007/s11916-016-0556-x
7. Sieczkowska SM, Vilarino GT, de Souza LC, Andrade A. Does physical exercise improve quality of life in patients with fibromyalgia? Ir J Med Sci. 2019;189(1):341–347. doi:10.1007/s11845-019-02038-z
8. Bennett RM, Friend R, Jones KD, Ward R, Han BK, Ross RL. The Revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther. 2009;11(4):R120. doi:10.1186/ar2783
9. Smets EM, Garssen B, Bonke B, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995;39(3):315–325. doi:10.1016/0022-3999(94)00125-o
10. Ericsson A, Bremell T, Mannerkorpi K. Usefulness of multiple dimensions of fatigue in fibromyalgia. J Rehabil Med. 2013;45(7):685–693. doi:10.2340/16501977-1161
11. Lin JM, Brimmer DJ, Maloney EM, Nyarko E, Belue R, Reeves WC. Further validation of the Multidimensional Fatigue Inventory in a US adult population sample. Popul Health Metr. 2009;7(1):18. doi:10.1186/1478-7954-7-18
12. Furukawa TA, Kessler RC, Slade T, Andrews G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol Med. 2003;33(2):357–362. doi:10.1017/s0033291702006700
13. University of Auckland SoP. Thematic analysis - a reflexive approach. Available from: https://www.psych.auckland.ac.nz/en/about/thematic-analysis.html#83bf374147ee4b701783e13961ad4ab1.
14. O’Cathain A, Thomas KJ. “Any other comments?” Open questions on questionnaires – a bane or a bonus to research? BMC Med Res Methodol. 2004;4(1):25. doi:10.1186/1471-2288-4-25
15. Arnold LM. Strategies for managing fibromyalgia. Am J Med. 2009;122(12 Suppl):S31–S43. doi:10.1016/j.amjmed.2009.09.009
16. Arnold LM. Duloxetine and other antidepressants in the treatment of patients with fibromyalgia. Pain Med. 2007;8(Suppl 2):S63–S74. doi:10.1111/j.1526-4637.2006.00178.x
17. Wiffen PJ, Derry S, Moore RA, et al. Antiepileptic drugs for neuropathic pain and fibromyalgia - an overview of Cochrane reviews. Cochrane Database Syst Rev. 2013;(11):CD010567. doi:10.1002/14651858.CD010567.pub2
18. Thorpe J, Shum B, Moore RA, Wiffen PJ, Gilron I. Combination pharmacotherapy for the treatment of fibromyalgia in adults. Cochrane Database Syst Rev. 2018;2:CD010585. doi:10.1002/14651858.CD010585.pub2
19. Kaye AD, Jones MR, Kaye AM, et al. Prescription opioid abuse in chronic pain: an updated review of opioid abuse predictors and strategies to curb opioid abuse: part 1. Pain Physician. 2017;20(2S):S93–S109. doi:10.36076/ppj.2017.s109
20. Atzeni F, Gerardi MC, Masala IF, Alciati A, Batticciotto A, Sarzi-Puttini P. An update on emerging drugs for fibromyalgia treatment. Expert Opin Emerg Drugs. 2017;22(4):357–367. doi:10.1080/14728214.2017.1418323
21. Goldenberg DL, Clauw DJ, Palmer RE, Clair AG. Opioid use in fibromyalgia: a cautionary tale. Mayo Clinic Proceedings. 2016;91(5):640–648. doi:10.1016/j.mayocp.2016.02.002
22. Baraniuk JN, Whalen G, Cunningham J, Clauw DJ. Cerebrospinal fluid levels of opioid peptides in fibromyalgia and chronic low back pain. BMC Musculoskelet Disord. 2004;5(1):48. doi:10.1186/1471-2474-5-48
23. Derry S, Wiffen PJ, Hauser W, et al. Oral nonsteroidal anti-inflammatory drugs for fibromyalgia in adults. Cochrane Database Syst Rev. 2017;3:CD012332. doi:10.1002/14651858.CD012332.pub2
24. Kleykamp BA, Ferguson MC, McNicol E, et al. The prevalence of psychiatric and chronic pain comorbidities in fibromyalgia: an ACTTION systematic review. Semin Arthritis Rheum. 2021;51(1):166–174. doi:10.1016/j.semarthrit.2020.10.006
25. Romero-Sandoval EA, Kolano AL, Alvarado-Vazquez PA. Cannabis and cannabinoids for chronic pain. Curr Rheumatol Rep. 2017;19(11):67. doi:10.1007/s11926-017-0693-1
26. Walitt B, Klose P, Fitzcharles MA, Phillips T, Hauser W. Cannabinoids for fibromyalgia. Cochrane Database Syst Rev. 2016;7:CD011694. doi:10.1002/14651858.CD011694.pub2
27. Vincent A, Whipple MO, Rhudy LM. Fibromyalgia Flares: a qualitative analysis. Pain Med. 2016;17(3):463–468. doi:10.1111/pme.12676
28. Larsson A, Feldthusen C, Mannerkorpi K. Factors promoting physical activity in women with fibromyalgia: a qualitative interview study. BMJ Open. 2020;10(8):e031693. doi:10.1136/bmjopen-2019-031693
29. Climent-Sanz C, Morera-Amenos G, Bellon F, et al. Poor sleep quality experience and self-management strategies in fibromyalgia: a qualitative metasynthesis. J Clin Med. 2020;9(12):12. doi:10.3390/jcm9124000
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.