Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Patient Outcomes from Student-Run Health Services: An Integrative Review
Authors Broman P ![]() , Tokolahi E
, Tokolahi E ![]() , Wilson OWA
, Wilson OWA ![]() , Haggie M, Andersen P, Brownie S
, Haggie M, Andersen P, Brownie S
Received 8 November 2021
Accepted for publication 12 January 2022
Published 30 March 2022 Volume 2022:15 Pages 641—665
DOI https://doi.org/10.2147/JMDH.S348411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Patrick Broman,1 Ema Tokolahi,1,2 Oliver WA Wilson,1,3 Marrin Haggie,4 Patrea Andersen,1,5,6 Sharon Brownie1,7,8
1Centre for Health and Social Practice, Waikato Institute of Technology, Hamilton, New Zealand; 2School of Occupational Therapy, Otago Polytechnic, Hamilton, New Zealand; 3Department of Kinesiology, Pennsylvania State University, University Park, PA, USA; 4Centre for Sport Science and Human Performance, Waikato Institute of Technology, Hamilton, New Zealand; 5School of Nursing, Midwifery and Social Science, Central Queensland University, Rockhampton, QLD, Australia; 6School of Nursing, Midwifery and Paramedicine, University of the Sunshine Coast, Sippy Downs, QLD, Australia; 7School of Nursing, Midwifery & Public Health, University of Canberra, Canberra, ACT, Australia; 8School of Medicine & Dentistry, Griffith University, Southport, QLD, Australia
Correspondence: Patrick Broman, Waikato Institute of Technology, Tristram Street, Hamilton, New Zealand, Tel +64 272070249, Email [email protected]
Background: Student-run clinics (SRCs) offer an innovative approach to expand healthcare access and equity and increase clinical placement opportunities for students. However, research on the health benefits and/or outcomes of such clinics is currently fragmented.
Methods: An integrative review was conducted to capture and synthesize findings across a range of study types involving varied student disciplines, student delivered intervention types, and health conditions addressed or care areas of focus. Only published and peer reviewed studies were included. Studies needed to report outcomes in a defined study group measured over time, or report SRC data with explicit comparisons to non-SRC settings. Data were analyzed using inductive content analysis to identify major themes and natural clustering of health outcomes measured.
Results: Fifty-one articles were selected for review based on the eligibility criteria. Studies were predominantly from the United States, and most (n = 34, 67%) adopted a case review methodology for measuring outcomes. Health outcomes were evaluated in relation to a range of health conditions that, for the purposes of this review, were considered to naturally cluster into eight categories: diabetes, hypertension, functional health/quality of life, depression, hospital utilization, substance use, weight, health screening/vaccinations, and others.
Conclusion: This integrative review sought to evaluate the health outcomes accrued by patients in student-run health clinics. Taken as a whole, the literature suggests positive health outcomes resulting from student-run clinics across a range of health conditions. Greater confidence in care-related findings would be achieved from future research utilizing more robust and prospective study designs.
Keywords: student-run clinic, student-led clinic, student-delivered, patient outcomes, interprofessional education, medical education
Background
Student-run, student-led or student-assisted health services or clinics (hereafter described as student-run clinics or SRCs) are dedicated settings where students are integrally engaged in delivering healthcare delivery during their studies. Such clinics offer expanded clinical placement opportunities, “real world” learning experiences for students, and improved access to care for underserved populations by delivering care at no or low cost.1–3 SRCs have been established in various countries, operate under various labels and models, and may involve students in single, or multiple health professions, providing care under professional supervision.
The literature related to health outcomes achieved through SRCs is growing, if somewhat fragmented. A preliminary search of the literature revealed a wide range of health outcomes measured and study methodologies used (both experimental and non-experimental). Descriptive accounts of SRCs and their patient or student characteristics are common (see, for example,4–12). Evaluative studies, while less common, have measured a range of outcomes in particular clinical contexts, but overviews of available evidence have generally been lacking. Earlier reviews have examined the learning outcomes that result for students involved in such clinics.13–15 Smaller-scale reviews have also been published on health outcomes specifically for SRC patients with cardiovascular disease or risk factors16 and on student-delivered care in a physical rehabilitation context,17 but the totality of evidence related to patient outcomes for patients in SRCs has not yet been systematically explored. Seeking to address this gap in knowledge, this integrative review aims to synthesize literature evaluating clinical patient outcomes of SRCs.
Integrative reviews are the broadest type of research review, allowing for a diverse range of the literature on a topic to be usefully summarized.18 By drawing together diverse and siloed knowledge, the objective is to reach a more comprehensive understanding of the patient outcomes associated with SRCs.
Methods
Study Design
An integrative review methodology was adopted as this enables wide inclusion criteria, incorporating a multiplicity of study methodologies and purposes to capture the depth and breadth of a topic.18,19 Current SRC outcome evidence is fragmented across health disciplines/professions and areas of care focus, and has not previously been synthesized for analysis. Whittemore and Knafl’s18 five-stage approach to undertaking integrative reviews by was followed, involving a) problem identification; b) literature search; c) data evaluation; d) data analysis and e) presentation of findings.
Literature Search
A systematic search of several databases, including PubMed (MedLine), CINAHL (EBSCOHost), and Web of Science (Clarivate) was conducted in September 2020. The search strategy and queries were reviewed and approved by a reference librarian. Strategies were uniquely designed relative to each database, and integrated controlled vocabulary for databases (for example, MeSH terms for PubMed). Additional sources were identified by checking the reference lists and subsequent citations of all included articles.
Three search term groups were included in the search strategies (see Box 1). The first included terms indicating college/university/higher education students, including “tertiary” – which, while not a term common in all jurisdictions, indicates education after secondary schooling, including at universities as well as technical or trade schools or colleges. The second search included terms that implied students were facilitating interventions, such as “run” or “led”. Finally, the third used various terms indicating that the texts related to clinics or health delivery settings. Regarding search filters, the search was restricted to English only, and no restrictions were placed on year or location.
 |
Box 1 Search Terms Used |
Following the database search, sources were aggregated within a database manager (EndNote). Next, duplicates were removed using The Systematic Review Assistant-Deduplication Module (SRA-DM), a program shown to reliably remove duplicate records with excellent sensitivity and specificity.20 The remaining duplicates were removed using EndNote software de-duplication function,21 and manually during title and abstract review.
Inclusion Criteria
Authors PB, ET, and OW collectively screened the remaining sources at the level of title and abstract to exclude ineligible records. Source selection was guided by the inclusion and exclusion criteria detailed in Table 1. Studies could be published in any year and relate to SRCs in any country, but only peer reviewed, English-language studies were included. Studies needed to clearly establish that students delivered a health-related intervention, regardless of location, degree of student supervision, or the nature or extent of student–patient interactions. Studies needed to focus on human health outcomes, broadly defined, so that studies of, for example, student veterinary or legal clinics were not included.
 |
Table 1 Eligibility Criteria for Articles |
Studies reporting patient satisfaction in SRC settings were excluded. While indicative of patient experiences and, arguably, broad SRC effectiveness, satisfaction is subjective and not a measure of clinical outcome which is the focus of this review. Given the focus on outcomes and impact, studies of non-comparator design were also excluded. Studies needed to report outcomes in a defined study group measured over time, or report SRC data with explicit comparisons to non-SRC settings (for example, rates for patients in a SRC compared to statewide or national standards). Information on the health status of SRC patients or of procedures performed in SRC settings may be of clinical interest but do not indicate outcome or impact. To expand on this point, studies were excluded where the health status of SRC patients were described without further data reported on how SRC engagement impacted on their health status, or where studies provided information on the number of treatments or level of services provided in an SRC setting but did not expand on this to identify how these rates compared to other populations or national standards to demonstrate impact.
Data Evaluation
Data evaluation involved extraction of specific methodological and design features of each of the included studies by authors PB, ET and OW. As the sampling frame was deliberately wide, incorporating a diverse range of clinical outcomes and study methodologies, a systematic quality appraisal approach was not adopted. Sources were evaluated via careful narrative consideration of the authenticity, methodological quality, informational value, and representativeness18 of included studies, as outlined in the discussion section. This approach reflects both the complex and differing nature of “quality”, and the primary review focus on informing SRC service development as opposed to clinical practice.
Data Analyses
Data analyses followed established integrative review processes for data reduction, data display, and data comparison.18 Data reduction involved determining an overall classification system for managing data followed by extraction and coding of data independently by authors PB, ET and OW. Data were extracted for the study setting (state and country), student disciplines involved, study design, sample size and characteristics, descriptions of the intervention, outcome measures used and study findings. Only data relating to patient clinical outcomes were extracted, and any broader data in each study that did not directly pertain to patient clinical outcomes (for example, parallel measures of patient satisfaction) were excluded. Discrepancies or uncertainties in how to reduce data were resolved through discussion. Whittemore and Knafl have noted how sources included in the integrative review need to be divided into subgroups according to some logical system to facilitate analysis.18 Inductive content analysis was therefore used to identify major themes and natural clustering18 of clinic outcomes evaluated before being displayed on a table and prepared for comparison in a narrative synthesis.
Results
From an initial result of 665 articles, 152 progressed to full-text review against the eligibility criteria, leaving 51 articles evaluating health outcomes for clients attending a SRC (see Figure 1).
 |
Figure 1 PRISMA flow diagram. Notes: Adapted from: Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of Clinical Epidemiology. 2009;62(10)e1-e34. Creative Commons.95 |
Most studies were conducted in the United States with the exceptions of two studies of outcomes from SRCs in Australia22,23 and one in each of the United Kingdom,c Ecuador,25 and Canada.26 The most common study method used were case reviews (n = 34) either in the context of a pre-post or a cohort study design. Health outcomes were evaluated in relation to a range of health conditions and, for the purposes of this review, were clustered into eight categories: diabetes, hypertension, functional health/quality of life, depression, hospital utilization, substance use, weight, health screening/vaccination, and others (see Table 2). There was some overlap in the specific outcomes evaluated across the various health conditions, as represented in Figure 2.
 |  |  |  | 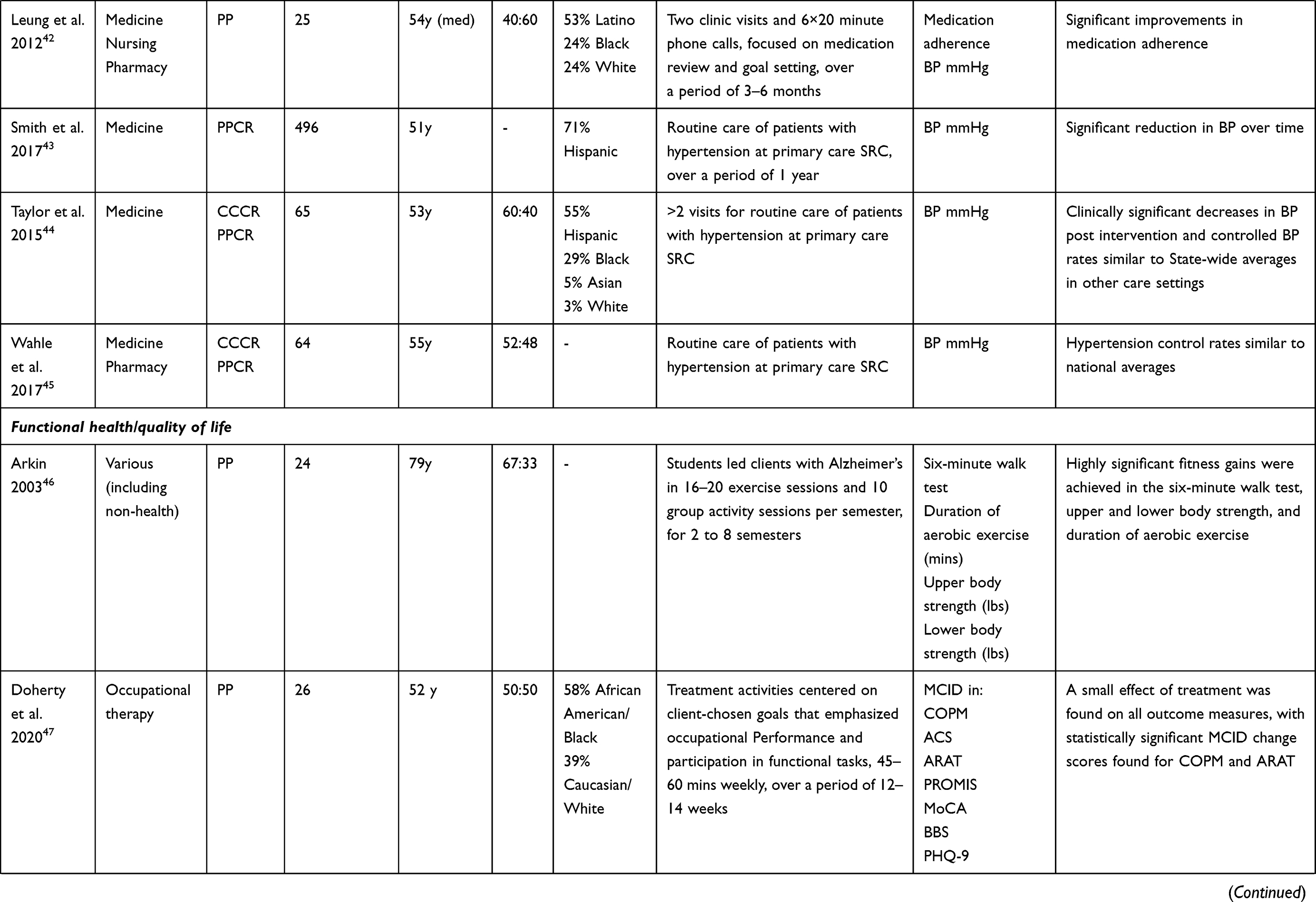 | 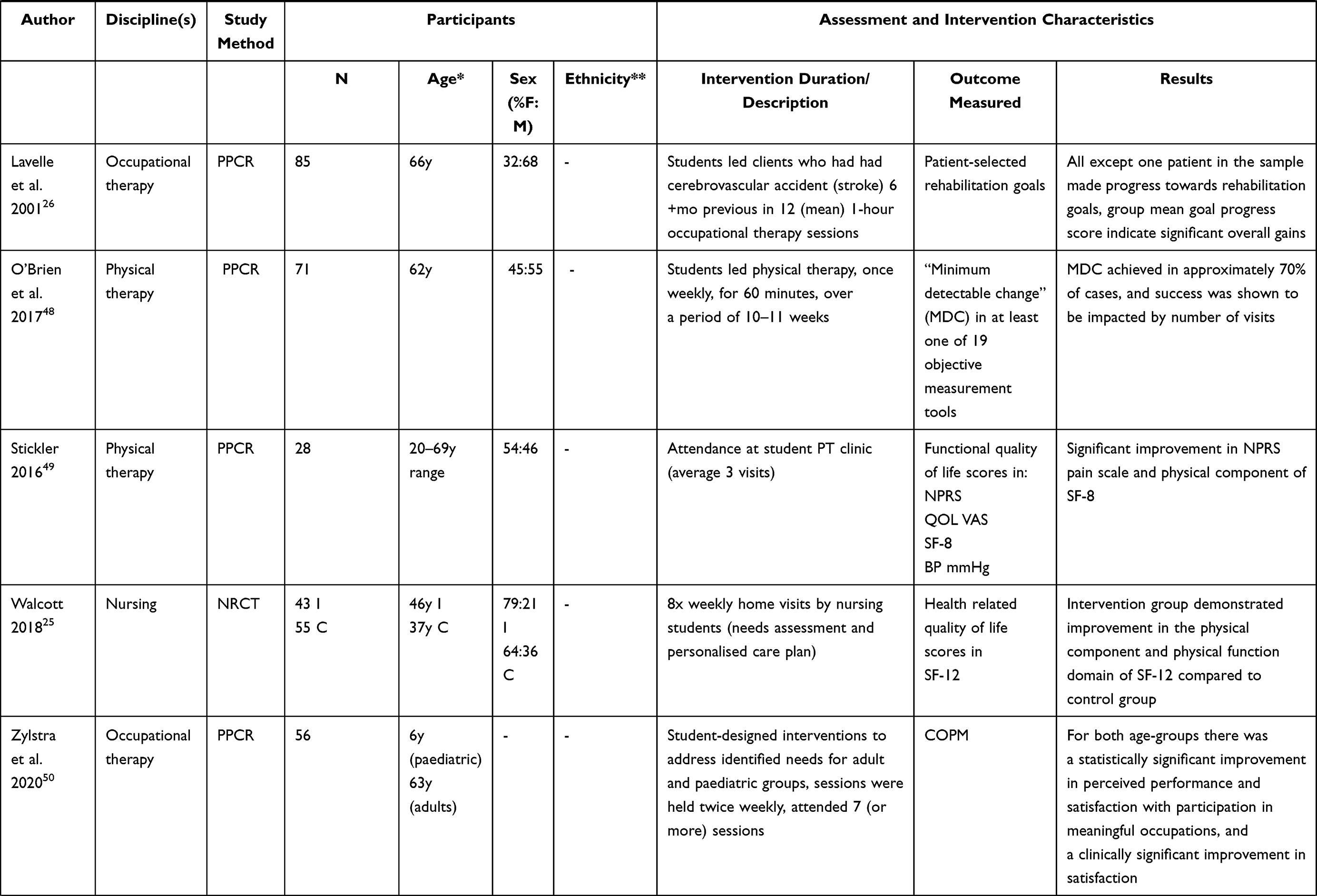 |  | 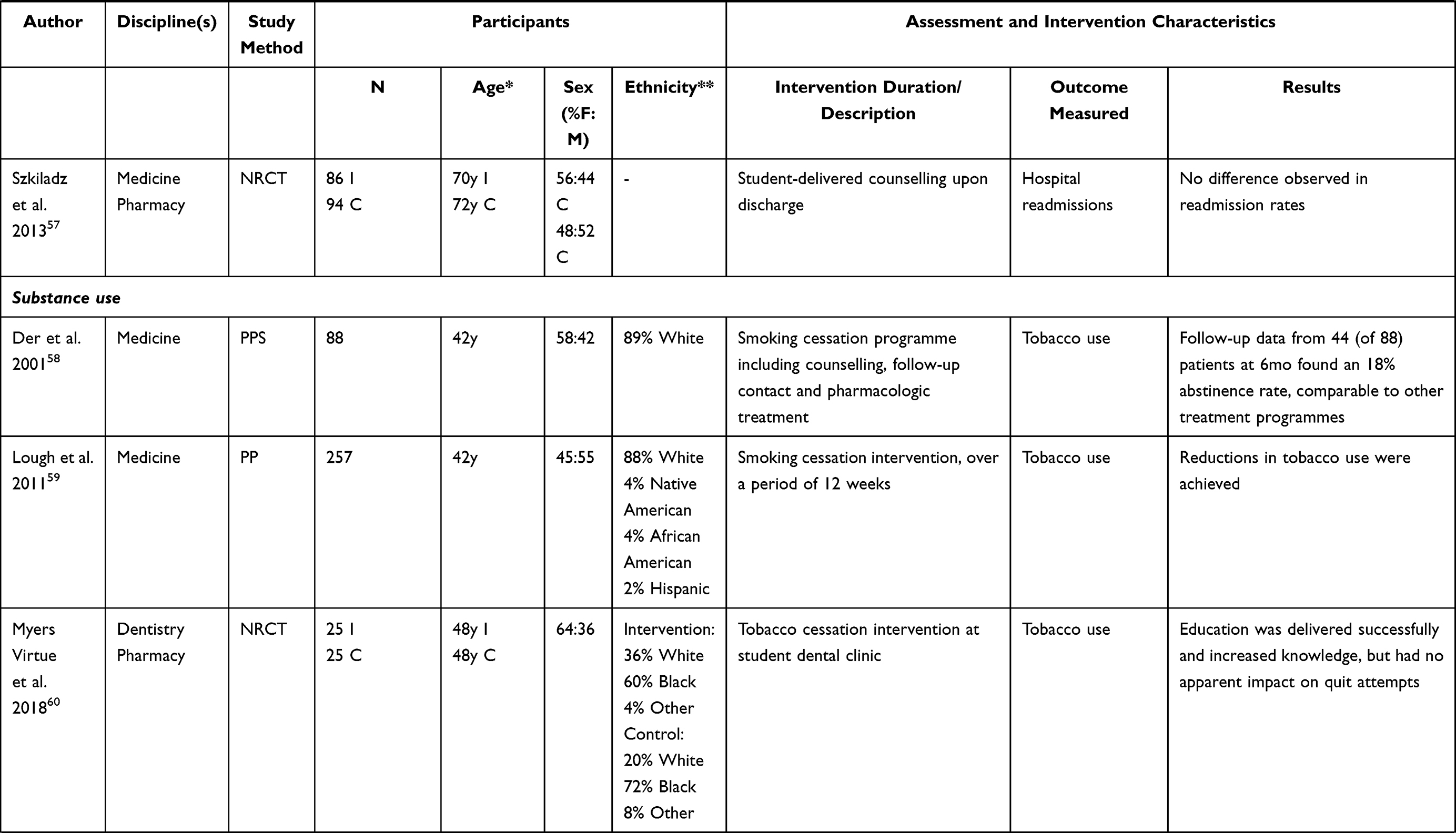 | 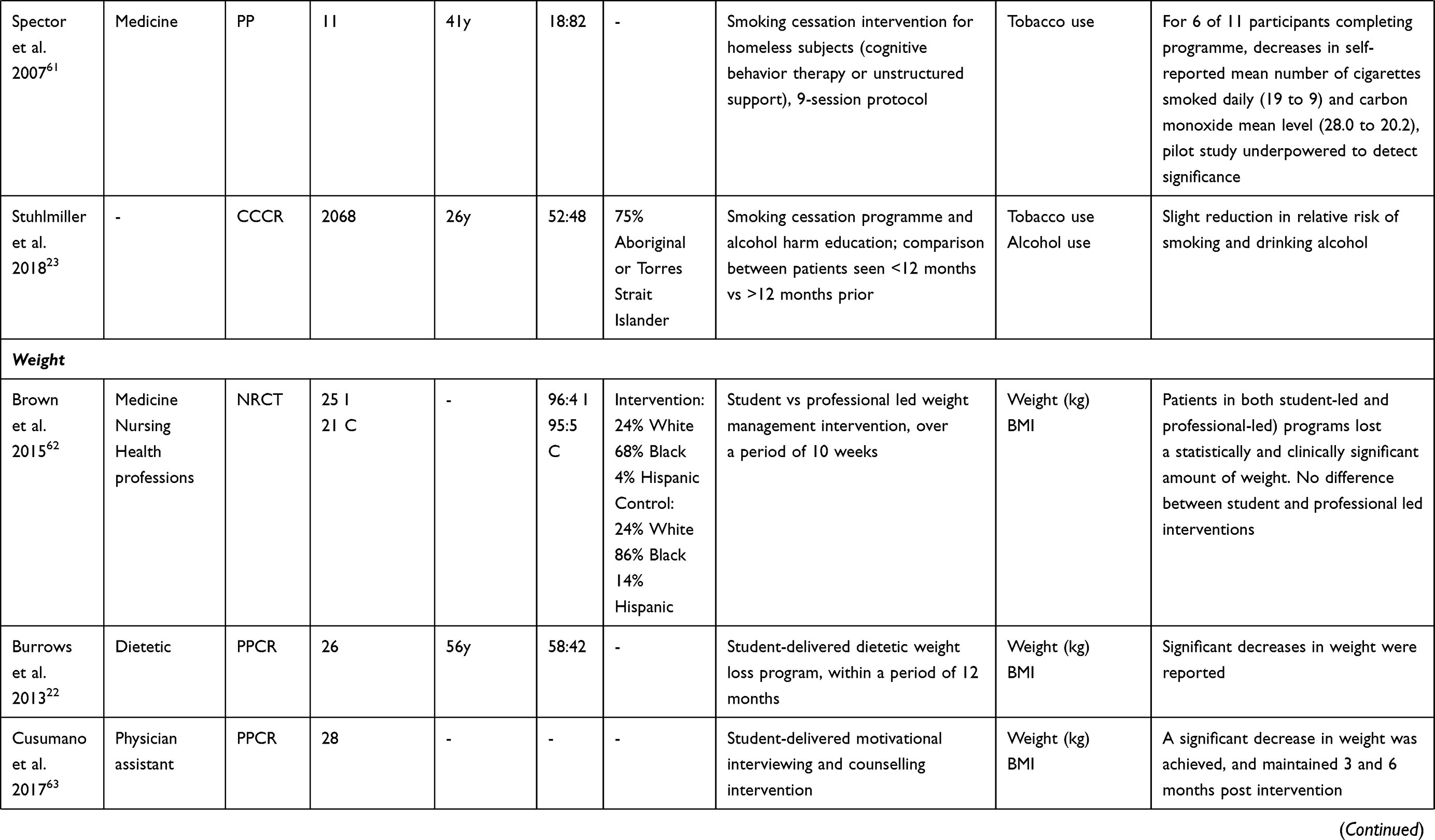 |  |  |  |
Table 2 Overview of Articles Selected for Review |
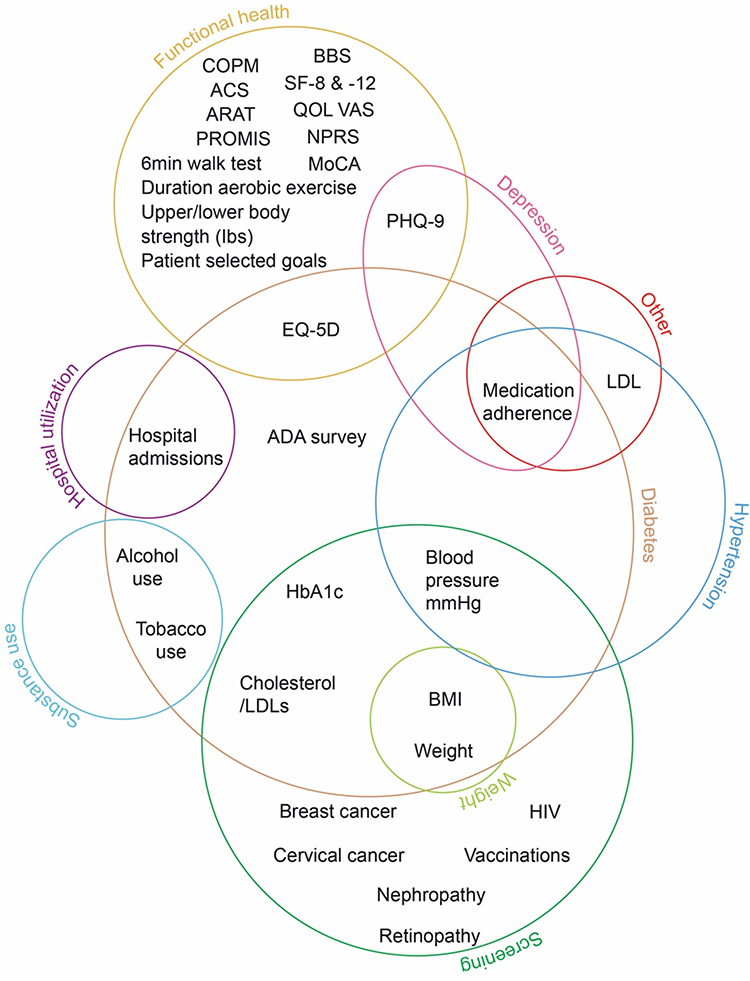 |
Figure 2 Summary and overlap of outcome measures in reviewed studies. Abbreviations: ACS, Activities Card Sort; ADA, American Diabetes Association; ARAT, Action Research Arm Test; BBS, Berg Balance Scale; BMI, Body Mass Index; COPM, Canadian Occupational Performance Measure; EQ-5D, EQ-5D self-rated quality of life scale; HbH1c, glycated haemoglobin/blood glucose levels; HIV, human immunodeficiency virus; lbs, weight in pounds; LDL = low-density lipoproteins; MoCA, Montreal Cognitive Assessment; mmHg, millimetre of mercury; NPRS, Numeric Pain Rating Scale; PHQ-9, Patient Health Questionnaire-9; PROMIS, Patient Reported Outcomes Measurement Information System; QOL VAS, Quality Of Life Visual Analog Scale; SF-8, Short Form 8 health survey; SF-12, Short Form 12 health survey. |
Diabetes
Diabetes was the most evaluated outcome, and the focus of 14 articles. Five evaluated health outcomes for SRCs run by medical students,27,30,33,36,37 four by pharmacy students,24,32,35,38 three medical and pharmacy students with either trainee physician assistants or nursing students,28,29,34 and two studies did not define student’s programme/s of study.31,39 Glycated haemoglobin (HbA1c) was used to measure diabetes status in all 14 studies, with blood pressure (n = 7) and cholesterol (LDLs; n = 7) also commonly measured. Interventions described ranged from routine care and drug therapy alone, medication management, patient education, screening, and follow-up phone calls. Periods of engagement ranged from two sessions involving assessment and one follow-up, to ongoing involvement and follow-up over a period of 2.6 years, although most commonly about 12 months. In most studies, an improvement (significant or non-significant) in blood glucose levels,24,27,29,33,35,37 or outcomes comparable to national standards36,37 were observed. Three studies28,38,73 found no statistically significant differences between groups; it should be noted that the student-run interventions in these studies were more focused on screening/diagnosis and patient education rather than ongoing intervention/treatment. Some studies that included blood pressure as an outcome found improvements35,37 or outcomes comparable to national standards,73 while others24,28,34,38 found no significant differences. Of studies that included cholesterol as an outcome, two found no significant difference in lipid levels post intervention,28,38 while four noted some improvements24,34,35,37 and one outcome comparable to national standards.36
Hypertension
Treatment outcomes regarding hypertension were the second-most examined after diabetes, with six studies published since 2012. All studies relate to US-based SRCs involving medical school students, with one also including pharmacy students45 and another pharmacy and nursing students.42 Five40,41,43–45 involved chart review of recorded blood pressure (mmHg) for patients receiving care in a primary care SRC. Usually, this was via a pre-post methodology measuring rates over time, sometimes incorporating cohort comparison of clinic rates with national or statewide averages. All found clinically significant decreases in blood pressure for hypertensive SRC patients, and – where assessed – control rates similar to those for hypertensive patients cared for in other clinical settings. The remaining study42 investigated antihypertensive medication adherence rates for patients in a student-delivered medication review, education, and goal setting initiative. Significant improvements were observed in medication adherence and systolic BP, but not diastolic BP.
Functional Health and Quality of Life
Seven studies explored the impact of SRCs on the functional health or quality of life of participants across the lifespan and with a wide range of health conditions. A range of measurement tools, not all named, were utilized. Five functional health studies26,46–48,50 included participants with diagnoses of Alzheimer’s disease, stroke and/or traumatic brain injury. Interventions were provided by students of physical48 or occupational therapy,26,47,50 across a number of (10+) sessions, typically of one-hour duration. In the physical therapy study, routine care, not described in more detail, was provided. In the studies involving occupational therapy, students provided client-driven, tailored interventions to address identified needs and goals relevant to everyday functional tasks. All five studies measured outcomes based on clinically significant levels of change. Varying effects of treatment, from small to large, were noted. In the two quality of life studies, in which no specific health conditions were described, interventions were provided by physical therapy students in a clinic setting49 or nursing students undertaking home visits.25 In both cases, significant improvements in physical quality of life ratings were observed, with no significant changes found in other areas of health quality of life.
Depression
Three studies51–53 focused on treatment outcomes for SRC patients with depression. Two related to the same SRC, the earlier of which found that the percentage of depressed clinic patients who had three follow-up visits within 12 weeks of diagnosis exceeded state averages for patients with commercial health plans or on Medicaid; and patients with newly diagnosed acute depression had better medication adherence rates than these comparison groups.51 By contrast, the more recent measured antidepressant medication adherence rates and found generally lower rates than in these comparison groups.52 Another study, of a program attempting depression screening of all patients presenting to a SRC, diagnosed 19 previously undiagnosed cases of depression amongst 206 patients screened. Of patients with depression cared for in this clinic with two or more PHQ-9 tests at least four weeks apart, 57.1% saw clinically significant improvement.53
Hospital Utilization
Of four studies that examined the impact of SRCs on hospital utilization, three54–56 focused on the impact of SRC care on emergency department visits (and one of these56 also on hospital observation admissions). Of these, one surveyed new and returning SRC patients regarding their ED visits in the past 3 months, finding returning patients had around half the per-patient ED visits of new patients.54 The other two used pre-post chart review to assess hospital utilization prior to and subsequent to enrolling in a SRC, one finding a qualified lessening in hospitalizations56 and the other, with a larger sample, a significant decrease in ED utilization in the 18 months subsequent to SRC enrolment compared to the 18 months previous.55 A further non-randomized control study,57 of the results from a medical resident/pharmacy student-delivered counselling programme for heart failure patients prior to their discharge from hospital, found no difference in readmission rates compared to a control group.
Substance Use
Five studies looked at the success of substance use prevention/cessation in SRC contexts: four in the United States involving tobacco cessation interventions delivered to SRC patients58–60 and one in Australia that examined both alcohol and tobacco use.23 One US study evaluated an intervention where smokers identified in a student-delivered dentistry clinic were referred to smoking cessation education delivered by pharmacy students.60 An increase in these patients’ knowledge regarding tobacco cessation was found, but there was little impact on the likelihood of making a quit attempt compared to the control group. In the three other US studies, tobacco cessation programmes delivered by students resulted in reduced tobacco use.58,59,61 The Australian study observed a slight reduction in the relative risk of alcohol use or smoking amongst those who had attended an SRC within the previous 12 months, compared to those who had last attended 12+ months previously.23
Weight Loss
Three studies reported on weight loss interventions delivered or facilitated by students. These studies, from the US62,63 and Australia,22 involved physician assistant students,63 medicine/nursing and other health professional students62 and dietetics students.22 Interventions differed: physician-assisted students delivered motivational interviewing and counselling, students in the mixed-discipline study led a ten-week weight loss program (compared to one similarly delivered by professional psychologists and dietitians) and dietetics students ran a weight loss counselling program. The reported results were positive, with significant decreases in weight loss and minimal difference in comparison to professional-led interventions.
Health Screening/Vaccination
Another group of five studies, all from the US, measured SRC rates of health condition screening or vaccination rates, population-level public health interventions where improved coverage is the care goal. These studies used a cohort comparison methodology, whereby in-clinic coverage rates were determined by chart review and compared to reported state or national rates. Only one64 was focused solely on vaccination rates – in this case, in a medical student-run clinic in Florida with a vaccination programme – and found vaccination rates in the clinic near or exceeding national rates. Two studies regarding screening, related to the same Florida clinic, found breast cancer screening rates greater than national rates for insured and uninsured women66 and rates of cervical cancer screening exceeding national rates.67 Two further studies explored coverage more comprehensively. One looked at rates of HIV, cholesterol (fasting lipid panel), diabetes (fasting blood glucose), and cervical cancer (pap smear) screening at a Connecticut SRC, observing rates lower than national averages but exceeding national uninsured averages.65 A further study examined rates of smoking cessation counselling, alcohol abuse screening, colposcopy, mammography, pap smear, and pneumococcal and influenza vaccination rates in a New Jersey SRC, with some rates greater and some lower than state or national rates.68
Other
Four studies did not fit into the aforementioned categories. One measured longitudinal outcomes for 96 patients newly diagnosed with high cholesterol in a San Diego SRC, finding over a mean follow-up period of 5.5 months that mean LDL levels decreased from baseline to a level exceeding national care standards.72 Another compared medication adherence rates for patients with latent tuberculosis infection undertaking a 9-month isoniazid treatment regimen in a SRC setting, finding adherence rates comparable to other clinics.71 One focused on the impact of a SRC quality improvement intervention, finding improvements in some areas of care,69 while a study of both diabetes and hypertension care in a Colorado SRC found diabetes care standards better, but hypertension care standards worse, than those of patients in comparable settings.
Discussion
This integrative review sought to evaluate the health outcomes, broadly defined, and accrued by patients in student-run health clinics. A total of 51 studies were reviewed, representing a recent and burgeoning literature, with the first studies having been published in 200126,58 and 32 in 2015 or later. For context, the first SRC in the United States opened in 1967.74
Taken as a whole, the literature suggests that positive patient outcomes are associated with SRCs. For diabetes, the condition with the largest body of published evidence, the preponderance of studies indicated routine SRC care resulted in clinically significant improvements in clinical indicators and/or levels of care comparable to other settings. Although all studies measuring the impact of routine in-clinic SRC diabetes primary care were positive, one study38 could not demonstrate clinically significant decreases in blood glucose in patients completing a student-delivered 24-month diabetes home visitation programme, and another34 found a student-delivered education programme improved blood glucose only in a sub-sample of patients with especially poor baseline measures. Positive results were observed in all the published studies examining functional health/quality of life, those examining SRC hypertension care, those examining SRC depression treatment (relative to other settings), and those investigating student-run weight-loss interventions. It is important to caution, however, that while the literature is almost universally favourable, for most areas of patient care it remains limited, and evidence may be impacted by publication bias whereby null/negative results have remained unreported. This may be especially the case for this review, which does not include “grey” literature produced informally or remaining unpublished. Moreover, as Felder-Heim and Mader70 have pointed out, it may be that only robust and well-established SRCs have the resources to conduct patient outcome evaluations, thus positively skewing reported results.
Diabetes, followed by hypertension, have been the subject of the greatest number of articles published to-date, reflecting the preponderance of these conditions in the US context where most studies were based.75,76 A survey of US SRCs published in 2014 found diabetes and hypertension amongst the most commonly treated diseases.77 Patient status for these conditions can also be measured by relatively straightforward biomarkers (ie, blood glucose/blood pressure), and so outcomes can be more practically and accurately assessed than can those for other conditions.
The patient groups and student-delivered interventions described in the reviewed studies merit some discussion. Patient characteristics in each of the studies were generally well described – as recorded in Table 2, almost all studies reported patient age, sex and ethnicity. Other characteristics not shown in the table but commonly reported, depending on clinic setting, were insurance status, employment status, housing/homeless status, migration status/origins and languages spoken. Some patient groups are not widely represented in the literature, notably Indigenous peoples (with some exceptions23,32), and also rural populations (except23,25,35), reflecting the urban nature of most medical schools and SRCs. Most reviewed studies involved only medical students in care delivery (n = 27, 51%). Compared to patient characteristics, details of clinic operations and the interventions provided were often limited. Future studies should clearly describe the duration, frequency, activity, intensity, etc., of interventions and the precise degree of student involvement, to aid readers in determining relevance to their interests and seeking to replicate successes.
In terms of coverage, some areas of care seem notably absent. A 2005 survey of the prevalence and operation of SRCs in all US medical schools78 found 36% of SRC visits (across 57 clinics reporting) were for acute/emergent complaints, but these are essentially missing from studies of patient outcomes. Respiratory diseases are also missing (except for one study of a student-led tuberculosis treatment regimen), despite being a leading cause of death and disability79 and also having been reported as amongst the chief clinical presentations in SRC contexts.9,11,12 Notably, no included outcomes studies assessed SRC care for COVID-19. Many student-delivered interventions have been recorded during the pandemic – in various contexts, students have been engaged in administering vaccinations,80–82 in telemedicine-based outreach and delivery,83–85 and in screening, testing and contact tracing activities.86–89 However, the safe and appropriate level of COVID care able to be provided by students remains a matter of debate (see90–92). Certainly, students may be better equipped to provide care for some conditions than others with greater complexity and risk. In this context, it may not be surprising that three studies related to medication adherence rates for depression care in SRCs51–53 were the only studies examining the quality of student-run interventions in mental health. While a small number of studies have looked at SRC health screening or vaccination rates, or the impact of student-run substance use and weight loss interventions, the potential for, and impact of, student-delivered health promotion initiatives more widely also seems underexplored.
Integrative reviews allow for findings to be incorporated and integrated into practice from a diverse range of methodologies.18,19 Most studies reviewed here followed observational methodological approaches, either as pre-post (or case series) studies, comparing patients’ status from baseline over a specified period of SRC care, or as cohort comparison studies, comparing SRC results with outcome data for patients in other settings, for example, amongst all local state Medicaid patients. Data collection approaches for both these types of observational studies varied. Most commonly data were gathered via retrospective chart review (PPCR or CCCR), but patient surveys (PPS or CCS) or, more rarely, prospective measurements (PP) were used. Observational methods can allow for meaningful and valid conclusions, particularly as in these cases where baseline or comparator data are included.93 However, greater confidence in care-related findings would result from more robust future research designs. Few studies used experimental or even quasi-experimental methodologies.
Study quality in this field could also be improved in other important ways. Many of the reviewed studies are underpowered, with a median study sample (including controls where applicable) of 85.0. Detecting anticipated effects with any degree of confidence requires a certain number of subjects, but very few of the studies include any evidence of power calculations being considered or conducted.94 Data were also typically collected retrospectively and out of convenience. While acknowledging the limited resources of SRCs, robustly planned prospective data collection would maximize study reliability and validity. Studies (with some exceptions35,43,72) measured outcomes only at single clinic sites, which may limit the generalizability of findings. This is also true at the national scale: most (n = 46, 90%) located studies related to US SRCs. Given the uniqueness of the US healthcare system, may not be comparable to other national contexts.
Some limitations of the present review must be acknowledged. First is that this study did not incorporate a systematic quality appraisal of reviewed studies. A key strength of integrative reviews lies in allowing for various perspectives on a phenomenon to be synthesized,18 but the wide and heterogeneous range of interventions and outcomes measured largely precluded an analysis of study quality on a like-for-like, systematic basis. The analyses have nevertheless allowed for drawing conclusions and recommendations for the field from a wide basis. Other limitations include the exclusion of non-English language studies, as well as the possibility of the search not having captured all relevant literature (especially given the plethora of possible terms to describe care or interventions provided by students). Confidence in the findings is nevertheless supported by the broad range of included studies and the general consensus in findings observed in each of the grouped patient outcome types.
Conclusion
Of 51 studies measuring the health outcomes associated with SRCs, nearly all indicate improvements in patient conditions, or outcomes comparable to those of similar patients treated in non-SRC settings. Generally positive findings are observed over a range of clinical focus areas, timeframes, and interventions. As noted, future research would benefit from improvements in study design and reporting, with generalizability of studies limited and some areas of care underexplored. Nevertheless, the evidence published to date suggests that SRCs can achieve positive health outcomes across a range of patient conditions.
Acknowledgments
The authors thank Dr Christina Wissinger, a Librarian at Pennsylvania State University, for assisting with the development of the search strategy. We also gratefully acknowledge our colleagues Greg Smith, Amy Pearce, Dr Glynis Longhurst, and Dr Ricky Bell for their helpful assistance.
Disclosure
The authors report no potential conflicts of interest in this work. This research was supported by Waikato Institute of Technology (Wintec) research seed funding.
References
1. Kavanagh J, Kearns A, McGarry T. The benefits and challenges of student-led clinics within an Irish context. J Pract Teach Learn. 2015;13(2–3):58–72. doi:10.1921/jpts.v13i2-3.858
2. Peninsula Health. Mornington Peninsula CPN student led clinic final project report: increasing capacity through student led clinics; 2012.
3. Stuhlmiller CM, Tolchard B. Developing a student-led health and wellbeing clinic in an underserved community: collaborative learning, health outcomes and cost savings. BMC Nurs. 2015;14(1):1–8. doi:10.1186/s12912-015-0083-9
4. Douglass KM, Polcari A, Najjar N, Kronenfeld J, Deshpande AR. Health care for the homeless transgender community: psychiatric services and transition care at a student-run clinic. J Health Care Poor Underserved. 2018;29(4):940–948. doi:10.1353/hpu.2018.0087
5. Duke P, Brunger F. The MUN Med Gateway Project: marrying medical education and Social accountability. Can Fam Physician. 2015;61(2):e81–e87.
6. Moskowitz D, Glasco J, Johnson B, Wang G. Students in the community: an interprofessional student-run free clinic. J Interprof Care. 2006;20(3):254–259. doi:10.1080/13561820600721091
7. Khonsari N, Davis K, Wolf D. Implementing a psychiatry clinic in a student-run setting: a medical student perspective. Acad Psych. 2019;43:340–343. doi:10.1007/s40596-020-01207-y
8. Hemba KE, Plumb J. JeffHOPE: the development and operation of a student-run clinic. J Prim Care Community Health. 2011;2(3):167–172. doi:10.1177/2150131911404239
9. Johnston D, McInerney P, Miot J. A profile of the health of homeless at an inner city primary health care clinic in South Africa. J Health Care Poor Underserved. 2019;30(4):1455–1466. doi:10.1353/hpu.2019.0093
10. Jimenez M, Tan-Billet J, Babineau J, et al. The Promise Clinic: a service-learning approach to increasing access to health care. J Health Care Poor Underserved. 2008;19(3):935–943. doi:10.1353/hpu.0.0046
11. Wang R, Guth A, Tate A, Ly M, Plumb J. Filling gaps and setting boundaries: examining utilization of health and social services at JeffHOPE Student Run Clinics. J Prim Care Community Health. 2021;12:1–7. doi:10.1177/21501327211037532
12. Rogers O, Heck A, Kohnert L, Paode P, Harrell L. Occupational therapy’s role in an interprofessional student-run free clinic: challenges and opportunities identified. Open J Occup Ther. 2017;5(3):1–15. doi:10.15453/2168-6408.1387
13. Schutte T, Tichelaar J, Dekker RS, van Agtmael MA, de Vries TPGM, Richir MC. Learning in student-run clinics: a systematic review. Med Edu Rev. 2015;49(3):249–263. doi:10.1111/medu.12625
14. Hopkins S, Bacon R, Flynn A. Student outcomes for interprofessional education in student led clinics: a rapid review. J Interprof Care. 2021;1–11. doi:10.1080/13561820.2020.1858767
15. Briggs L, Fronek P. Student experiences and perceptions of participation in student-led health clinics: a systematic review. J Soc Work Educ. 2020;56(2):238–259. doi:10.1080/10437797.2019.1656575
16. Suen J, Attrill S, Thomas JM, Smale M, Delaney CL, Miller MD. Effect of student-led health interventions on patient outcomes for those with cardiovascular disease or cardiovascular disease risk factors: a systematic review. BMC Cardiovasc Disord. 2020;20(1):1–10. doi:10.1186/s12872-020-01602-1
17. Wynne D, Cooper K. Student-led rehabilitation groups and clinics in entry-level health education: a scoping review. JBI Evid Synth. 2021;19(11):2958–2992. doi:10.11124/JBIES-20-00340
18. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546–553. doi:10.1111/j.1365-2648.2005.03621.x
19. Cronin MA, George E. The why and how of the integrative review. Organ Res Methods. 2020;1094428120935507. doi:10.1177/1094428120935507
20. Rathbone J, Carter M, Hoffmann T, Glasziou P. Better duplicate detection for systematic reviewers: evaluation of systematic review assistant-deduplication module. Syst Rev. 2015;4(1):1–6. doi:10.1186/2046-4053-4-6
21. Clarivate. EndNote; 2020.
22. Burrows T, Patterson A, Bacon A, et al. Client satisfaction and weight loss outcomes of student centred dietetic outpatient clinics. Obes Res Clin Pract. 2013;7(5):e421–e430. doi:10.1016/j.orcp.2012.05.003
23. Stuhlmiller CM, Tolchard B. Population health outcomes of a student-led free health clinic for an underserved population: a naturalistic study. J Community Health. 2018;43(1):193–200. doi:10.1007/s10900-017-0402-z
24. Adams RP, Barton G, Bhattacharya D, et al. Supervised pharmacy student-led medication review in primary care for patients with type 2 diabetes: a randomised controlled pilot study. BMJ Open. 2015;5(11):1–11. doi:10.1136/bmjopen-2015-009246
25. Walcott RL, Murcia AM, Berry GM, Juna CF, Roldós MI, Corso PS. The impact of nursing students on the health-related quality of life and perceived social support of a rural population in Ecuador: effects of a service-based learning course. Int J Equity Health. 2018;17(1):1–8. doi:10.1186/s12939-018-0734-z
26. Lavelle P, Tomlin GS. Occupational therapy goal achievement for persons with postacute cerebrovascular accident in an on-campus student clinic. Am J Occup Ther. 2001;55(1):36–42. doi:10.5014/ajot.55.1.36
27. Gorrindo P, Peltz A, Ladner TR, et al. Medical students as health educators at a student-run free clinic: improving the clinical outcomes of diabetic patients. Acad Med. 2014;89(4):625–631. doi:10.1097/ACM.0000000000000164
28. Janson SL, Cooke M, McGrath KW, Kroon LA, Robinson S, Baron RB. Improving chronic care of type 2 diabetes using teams of interprofessional learners. Acad Med. 2009;84(11):1540–1548. doi:10.1097/ACM.0b013e3181bb2845
29. Kahkoska AR, Brazeau NF, Lynch KA, et al. Implementation and evaluation of shared medical appointments for type 2 diabetes at a free, student-run clinic in Alamance County, North Carolina. J Med Educ Training. 2018;2(1):1–10.
30. Laitman B, Mosley G, Thomas DC, Meah YS. How well does a student-run free clinic care for diabetic patients? J Student-Run Clin. 2017;3(1):1–9.
31. Lee TC, Frangos SN, Torres M, Winckler B, Ji SG, Dow E. Integrating undergraduate patient partners into diabetes self- management education: evaluating a free clinic pilot program for the underserved. J Health Care Poor Underserved. 2016;27(4):1689–1708. doi:10.1353/hpu.2016.0156.Integrating
32. Martin SL, Williams E, Huerth B, et al. A pharmacy student-facilitated interprofessional diabetes clinic with the Penobscot nation. Prev Chronic Dis. 2015;12(11):1–6. doi:10.5888/pcd12.150295
33. Mehta PP, Santiago-Torres JE, Wisely CE, et al. Primary care continuity improves diabetic health outcomes: from free clinics to federally qualified health centers. J Am Board Fam Med. 2016;29(3):318–324. doi:10.3122/jabfm.2016.03.150256
34. Nagelkerk J, Thompson ME, Bouthillier M, et al. Improving outcomes in adults with diabetes through an interprofessional collaborative practice program. J Interprof Care. 2018;32(1):4–13. doi:10.1080/13561820.2017.1372395
35. Nuffer W, McCollum M, Ellis SL, Turner CJ. Further development of pharmacy student-facilitated diabetes management clinics. Am J Pharm Educ. 2012;76(3):50. doi:10.5688/ajpe76350
36. Ryskina KL, Meah YS, Thomas DC. Quality of diabetes care at a student-run free clinic. J Health Care Poor Underserved. 2009;20(4):969–981. doi:10.1353/hpu.0.0231
37. Smith SD, Marrone L, Gomez A, Johnson ML, Edland SD, Beck E. Clinical outcomes of diabetic patients at a student-run free clinic project. Fam Med. 2014;46(3):198–203.
38. Stroup J, Kane MP, Busch RS, Bakst G, Hamilton RA. Instructional design and assessment: the diabetes home visitation progam. Am J Pharm Educ. 2003;67(3):1–8. doi:10.5688/aj670391
39. Wilcox S, Okut H, Badgett R, Hassouneh S, Ablah E. Effectiveness of flow sheet implementation on diabetes progression screening at a student-run free clinic. Kansas J Med. 2020;13:285–289. doi:10.17161/kjm.vol13.13423
40. Atkinson B, Uichanco L, Kattih Z, et al. Review of hypertension management at University of South Florida BRIDGE Clinic. J Student-Run Clin. 2018;4(1):1–5.
41. Berman R, Powe C, Carnevale J, et al. The crimson care collaborative: a student-faculty initiative to increase medical students’ early exposure to primary care. Acad Med. 2012;87(5):651–655. doi:10.1097/ACM.0b013e31824d5269
42. Leung LB, Busch AM, Nottage SL, et al. Approach to antihypertensive adherence: a feasibility study on the use of student health coaches for uninsured hypertensive adults. Behav Med. 2012;38(1):19–27. doi:10.1080/08964289.2011.651174
43. Smith SD, Rojas SM, Huang J, Yang K, Vaida F. Longitudinal hypertension outcomes at four student-run free clinic sites. Fam Med. 2017;49(1):28–34.
44. Taylor J, Thomas D, Tornheim J, Meah Y. Hypertension outcomes at a student-run clinic for the uninsured. J Student-Run Clin. 2015;11(1):1–8.
45. Wahle B, Meyer K, Faller M, Kochhar K, Sevilla J. Assessment of hypertension management and outcomes at an Indianapolis student-run free clinic. J Health Care Poor Underserved. 2017;28(2):694–706. doi:10.1353/hpu.2017.0068
46. Arkin SM. Student-led exercise sessions yield significant fitness gains for Alzheimer’s patients. Am J Alzheimer’s Dis Other Dement. 2003;18(3):159–170. doi:10.1177/153331750301800302
47. Doherty M, Dyer M, Wilson E, Russell-Thomas D. Rehabilitation outcomes of an occupational therapy student-run free clinic for individuals with acquired brain injury. J Allied Health. 2020;49(1):60–66.
48. O’Brien SR, Bulas M, Metcalfe A, Mix Z, Richert T, Wagner R. Meaningful functional change achieved from physical therapy provided in a student-run pro bono clinic. J Allied Health. 2017;46(3):138–142.
49. Stickler K, Sabus C, Gustafson H, Kueser M, Lavaveshkul B, Denney L. Pro-bono service through student-run clinics: how does physical therapy measure up? J Allied Health. 2016;45(3):207–211.
50. Zylstra SE, Doyle S. Measuring client-centered outcomes in an occupational therapy student teaching clinic using the Canadian Occupational Performance Measure. Am J Occup Ther. 2020;74(4):1–8. doi:10.5014/ajot.2020.034892
51. Liberman KM, Meah YS, Chow A, Tornheim J, Rolon O, Thomas DC. Quality of mental health care at a student-run clinic: care for the uninsured exceeds that of publicly and privately insured populations. J Community Health. 2011;36(5):733–740. doi:10.1007/s10900-011-9367-5
52. Mann CL, Rifkin RA, Nabel EM, Thomas DC, Meah YS, Katz CL. Exploring antidepressant adherence at a student-run free mental health clinic. Community Ment Health J. 2019;55(1):57–62. doi:10.1007/s10597-018-0301-5
53. Soltani M, Smith S, Beck E, Johnson M. Universal depression screening, diagnosis, management, and outcomes at a student-run free clinic. Acad Psych. 2015;39(3):259–266. doi:10.1007/s40596-014-0257-x
54. Kramer N, Harris J, Zoorob R. The impact of a student-run free clinic on reducing excess emergency department visits. J Student-Run Clin. 2015;4:1–7.
55. Thakkar AB, Chandrashekar P, Wang W, Blanchfield BB. Impact of a student-run clinic on emergency department utilization. Fam Med. 2019;51(5):420–423. doi:10.22454/FamMed.2019.477798
56. Trumbo SP, Schuering KM, Kallos JA, et al. The effect of a student-run free clinic on hospital utilization. J Health Care Poor Underserved. 2018;29(2):701–710. doi:10.1353/hpu.2018.0053
57. Szkiladz A, Carey K, Ackerbauer K, Heelon M, Friderici J, Kopcza K. Impact of pharmacy student and resident-led discharge counseling on heart failure patients. J Pharm Pract. 2013;26(6):574–579. doi:10.1177/0897190013491768
58. Der DE, You YQ, Wolter TD, Bowen DA, Dale LC. A free smoking intervention clinic initiated by medical students. Mayo Clin Proc. 2001;76(2):144–151. doi:10.1016/s0025-6196(11)63120-0
59. Lough LE, Ebbert JO, McLeod TG. Evaluation of a student-run smoking cessation clinic for a medically underserved population. BMC Res Notes. 2011;4. doi:10.1186/1756-0500-4-55
60. Myers Virtue S, Rotz ME, Boyd M, Lykon JL, Waldron EM, Theodorou J. Impact of a novel interprofessional dental and pharmacy student tobacco cessation education programme on dental patient outcomes. J Interprof Care. 2018;32(1):52–62. doi:10.1080/13561820.2017.1378171
61. Spector A, Alpert H, Karam-Hage M. Smoking cessation delivered by medical students is helpful to homeless population. Acad Psych. 2007;31(5):402–405. doi:10.1176/appi.ap.31.5.402
62. Brown J, Lydecker JA, Turner T, Knackstedt RW, O’Neil PM. A novel approach to training students in delivering evidence-based obesity treatment. Fam Med. 2015;47(5):378–382.
63. Cusumano J, Martin CS, Butler B, Bixler B, Shirk K. Efficacy of a physician assistant student-developed behavior change program at a local free clinic. J Physician Assist Educ. 2017;28(1):41–44. doi:10.1097/JPA.0000000000000106
64. Abuelenen T, Khalil S, Simoneit E, et al. Prevent and protect: a vaccination initiative for uninsured patients at a student-run free clinic. J Community Health. 2020;45(5):910–915. doi:10.1007/s10900-020-00808-w
65. Butala NM, Murk W, Horwitz LI, Graber LK, Bridger L, Ellis P. What is the quality of preventive care provided in a student-run free clinic? J Health Care Poor Underserved. 2012;23(1):414–424. doi:10.1353/hpu.2012.0034
66. Khalil S, Hatch L, Price CR, et al. Addressing breast cancer screening disparities among uninsured and insured patients: a Student-Run Free Clinic Initiative. J Community Health. 2020;45(3):501–505. doi:10.1007/s10900-019-00767-x
67. Price CR, Hatch LA, Radisic A, et al. Enhancing adherence to cervical cancer screening guidelines at a student-run free clinic. J Community Health. 2020;45(1):128–132. doi:10.1007/s10900-019-00724-8
68. Zucker J, Lee J, Khokhar M, Schroeder R, Keller S. Measuring and assessing preventive medicine services in a student-run free clinic. J Health Care Poor Underserved. 2013;24(1):344–358. doi:10.1353/hpu.2013.0009
69. Burger M, Taddeo MS, Hushla D, Pasarica M. Interventions for increasing the quality of preventive care at af ree clinic. Cureus. 2020;12(1):1–10. doi:10.7759/cureus.6562
70. Felder-Heim C, Mader K. Quality of diabetes and hypertension management at the dawn (Dedicated to Aurora’s Wellness and Needs) student-run free clinic. Cureus. 2020;12(8):1–9. doi:10.7759/cureus.9539
71. Peluso MJ, Hung A, Lukasiewicz A, et al. Successful management of latent tuberculosis infection in an underserved community by a student-run free clinic. J Health Care Poor Underserved. 2014;25(2):837–862. doi:10.1353/hpu.2014.0109
72. Rojas SM, Smith SD, Rojas S, Vaida F. Longitudinal hyperlipidemia outcomes at three student-run free clinic sites. Fam Med. 2015;47(4):309–314.
73. Ryskina KL, Meah YS, Thomas DC. Quality of diabetes care at a student-run free clinic. Free Clin. 2013;9781421408(4):969–981.
74. Chen K. Exploring the frontier: the Journal of Student-Run Clinics. J Student-Run Clin. 2015;1(1):1–2.
75. Centers for Disease Control and Prevention (CDC). Hypertension Cascade: hypertension Prevalence, Treatment and Control Estimates Among US Adults Aged 18 Years and Older Applying the Criteria From the American College of Cardiology and American Heart Association’s 2017 Hypertension Guideline—NHANES 2015–2. Atlanta, GA: US Department of Health and Human Services; 2021. Available from: https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html.
76. US Department of Health and Human Services. National diabetes statistics report, 2020: estimates of diabetes and its burden in the United States; 2020.
77. Smith S, Thomas R, Cruz M, Griggs R, Moscato B, Ferrara A. Presence and characteristics of student-run free clinics in medical schools. JAMA. 2014;312(22):2407–2410. doi:10.1001/jama.2014.16066
78. Simpson SA, Long JA. Medical student-run health clinics: important contributors to patient care and medical education. J Gen Intern Med. 2007;22:352–356. doi:10.1007/s11606-006-0073-4
79. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
80. Gregory N. Pharmacy students play crucial role in COVID-19 mass vaccinations. Am J Health-Syst Pharm. 2021;78(8):663–664. doi:10.1093/ajhp/zxab081
81. Hanrahan JR, Carroll PR. Student-led interprofessional influenza vaccination clinic in a time of coronavirus. Med Edu. 2020;54(11):1078–1079. doi:10.1111/medu.14323
82. Cuschieri S, Agius S, Souness J, Brincat A, Grech V. The fastest national COVID vaccination in Europe - Malta’s strategies. Health Sci Rev. 2021;1:100001. doi:10.1016/j.hsr.2021.100001
83. Cook E, Arboleda B, Stewart H, et al. Responding to COVID-19: implementing a telemedicine program at a student-run free clinic. Telemed Rep. 2021;2(1):97–107. doi:10.1089/tmr.2020.0037
84. Shatskikh ME, Kirillova A, Shi LZ. Students leading a free clinic: lessons learned about digital health in the age of COVID-19. Int. J Med Stud. 2020;8(3):303–304. doi:10.5195/ijms.2020.803
85. Martinez DJ, Hamamsy KC, Hines SE, et al. Interprofessional student-led outreach to high-risk older adults during the COVID-19 pandemic. Gerontol Geriatr Educ. 2021;43:34–42. doi:10.1080/02701960.2021.1958326
86. Cowie MJ, Barron CVM. How were medical students from Christchurch, New Zealand, involved in their COVID-19 response? NZ Med J. 2021;134:1538.
87. Bosveld MH, van Doorn DPC, Stassen PM, et al. Lessons learned: contribution to healthcare by medical students during COVID-19. J Crit Care. 2021;63:113–116. doi:10.1016/j.jcrc.2020.09.015
88. Pelton M, Medina D, Sood N, et al. Efficacy of a student-led community contact tracing program partnered with an academic medical center during the coronavirus disease 2019 pandemic. Ann Epidemiol. 2021;56:26–33.e1. doi:10.1016/j.annepidem.2020.10.004
89. Stachteas P, Vlachopoulos N, Smyrnakis E. Deploying medical students during the COVID-19 pandemic. Med Sci Edu. 2021;31(6):2049–2053. doi:10.1007/s40670-021-01393-w
90. Bank I, Wijnen-Meijer M. Why should medical students (not) be recruited to care for patients with COVID-19? BMC Med Educ. 2020;20(1). doi:10.1186/s12909-020-02261-8
91. Hong J, Jung I, Park M, et al. Attitude of medical students about their role and social accountability in the COVID-19 pandemic. Front Psych. 2021;12. doi:10.3389/fpsyt.2021.645340
92. Riva MA, Paladino ME, Belingheri M. The role of medical students during the COVID-19 pandemic. Ann Intern Med. 2020;173(10):858–859. doi:10.7326/L20-1194
93. Carlson MDA, Morrison RS. Study design, precision, and validity in observational studies. J Palliat Med. 2009;12(1):77–82. doi:10.1089/jpm.2008.9690
94. Tooth L, Ware R, Bain C, Purdie DM, Dobson A. Quality of reporting of observational longitudinal research. Am J Epidemiol. 2005;161(3):280–288. doi:10.1093/aje/kwi042
95. Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. 2009;62(10)e1–e34.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.