Back to Journals » Patient Preference and Adherence » Volume 17
Patient Education with New Media Integration Self-Management Support Model Improves Therapeutic Outcomes of Rosacea Patients
Authors Liu X ![]() , Kim MK
, Kim MK ![]() , Du D
, Du D ![]() , Zhou X, Wang L, Jiang X
, Zhou X, Wang L, Jiang X ![]()
Received 23 July 2023
Accepted for publication 22 September 2023
Published 27 September 2023 Volume 2023:17 Pages 2395—2400
DOI https://doi.org/10.2147/PPA.S431955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xu Liu,1,2,* Min-Kyu Kim,1,2,* Dan Du,1,2 Xinyu Zhou,1,2 Lian Wang,1,2 Xian Jiang1,2
1Department of Dermatology, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2Laboratory of Dermatology, Clinical Institute of Inflammation and Immunology, Frontiers Science Center for Disease-Related Molecular Network, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lian Wang; Xian Jiang, Department of Dermatology, West China Hospital, Sichuan University, #37 Guoxue Alley, Wuhou District, Chengdu, Sichuan, 610041, People’s Republic of China, Tel +86-28-85423315, Fax +86-28-85422560, Email [email protected]; [email protected]
Objective: To retrospectively analyze the factors influencing the treatment of rosacea patients with regular follow-up by self-management support in the new media chronic disease management model, to explore the effect of self-management support and to provide an objective basis for clinical application.
Methods: Female patients with rosacea who were regularly followed up for more than 6 months at the rosacea follow-up clinic of the Department of Dermatology, West China Hospital, Sichuan University, from March 2022 to June 2023, with erythema and capillary dilation as the main clinical phenotype, met the rosacea diagnostic criteria of the American Rosacea Expert Committee 2017 edition, and received medications recommended by the Chinese Rosacea Treatment Guidelines (2021 edition). A total of 125 patients were treated with combined photobiomodulation therapy (PBMT), and the patients were divided into a standardized group (CEA< 1, IGA< 1) and a non-standardized group (CEA≥ 1, IGA≥ 1) based on significant rosacea efficacy (CEA< 1, IGA< 1) within 6 months. The age, gender, education level, duration of rosacea, treatment regimen, education intensity, CEA, and IGA baseline data were compared between the two groups, and logistic regression analysis was performed to analyze the factors influencing the significant efficacy of rosacea.
Results: There was a significant difference in the mean length of education between the two groups (P< 0.05), and the differences between the rest of the baseline information of the two groups were not statistically significant (P> 0.05). Logistic regression analysis showed that the variable that significantly influenced the efficacy of treatment was the mean length of education (≥ 130.5 min/month), and the intensity of education was significantly associated with the efficacy of treatment.
Conclusion: Self-management support in the new media chronic disease management model has a positive impact on the treatment of rosacea patients.
Keywords: new media chronic disease management model, self-management support, rosacea, patient education
Introduction
Rosacea is a prevalent chronic skin disorder primarily affecting the facial area. It is commonly observed in women between the ages of 30 and 55 and presents with a diverse range of clinical manifestations, including erythema, flushing, capillary dilation, papules, pustules, and ocular symptoms, among others1,2. The condition significantly impacts an individual’s physical appearance and psychosocial well-being, often leading to feelings of shame, embarrassment, low self-esteem, diminished self-confidence, negative body image, and even anxiety disorders3,4. In addition, the severity of erythema in rosacea is associated with disease burden, and patients’ adverse effects on mood and quality of life increase with the severity of erythema, further aggravating the disease burden5. Therefore, it is crucial to explore a patient-centred chronic disease management program that encompasses comprehensive management strategies for rosacea. Recent studies focusing on patient education in chronic skin disorders have substantiated the significance of self-management support behaviors within the context of a chronic disease management model, highlighting their influential role in disease control.6–9 In addition, the use of individualized, patient-centered chronic disease management protocols has been advocated in the management of patients with rosacea10,11. On top of that, It has been reported that follow-up is important to reduce disease recurrence, and new media is a useful tool for follow-up.12 The findings of a qualitative analysis, focusing on the content of online communication among individuals with rosacea, revealed that proactive health education encompassing topics such as etiology, treatment, diet, and skincare exhibited a positive impact. This educational approach effectively reduced patient confusion regarding the disease, patient’s adherence to the medications and fostered a positive doctor-patient relationship13,14. The objective of this study was to conduct a retrospective analysis of the factors that impact the treatment of rosacea patients who engage in regular follow-up through self-management support within the framework of the new media chronic disease management model. The study aimed to investigate the effects of self-management support and provide an objective foundation for its clinical application.
Materials and Methods
Study Population
Female patients with rosacea with erythema and capillary dilation as the main phenotype, who met the American Rosacea Expert Committee’s 2017 edition of rosacea diagnostic criteria and received the drug combination recommended by the Chinese Rosacea Treatment Guidelines (2021 edition), were selected for regular follow-up at the Rosacea Follow-up Clinic of the Department of Dermatology, West China Hospital, Sichuan University from March 2022 to June 2023. Photobiomodulation therapy (PBMT).15 The study was approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University (ChiCTR2019.248), and all study subjects signed an informed consent form. The research was conducted in accordance with the ethical guidelines outlined in the Declaration of Helsinki.
Methods
Subjects entered a 6-month new media chronic disease management model for rosacea and received at least 3 on-site assessments, including a rosacea facial erythema score (CEA) based on VISIA facial photographic images, and an investigator overall assessment (IGA). Follow-up physicians relied on live video platforms, voice communication platforms, Internet communities, and on-site instructions to intervene with patients, and monitoring results were based on media back-end data, community conversation records, visit records, and telephone survey collection.
The New Media Chronic Disease Management Model consists of four educational programs: Program A is a live video broadcast with disease introduction, Program B is a voice communication with life coaching and medication guidance, Program C is a personalized problem-solving dialogue within a rosacea-specific community, and Program D is an on-site assessment and educational guidance at the hospital (Figure 1).
 |
Figure 1 Overview of the study design. |
The follow-up physicians track the length of education, content of questions, and trends in disease severity, and provide regular feedback to outpatient physicians to inform treatment plan adjustments.
Considering the different degree of influence of each educational item on patients, the weighting of the degree of influence of each educational item was calculated using the hierarchical analysis method (AHP). The factors were compared by experts, and the comparison results were marked according to the relative importance score criteria (Table S1) to obtain the relative importance assignment, thus establishing the judgment matrix. Finally, the weights of individual indicators were calculated by the judgment matrix (Table S2). This design questionnaire survey was participated by 10 dermatologists with master’s degree or above and 5 years or more clinical experience, and the weights of the experts’ scores on the index system were calculated separately, and the weights of this evaluation index system were obtained by finding the mean value. The following is an example of one of the experts (Table S3), and the weight of each index was calculated for their scoring data. The scoring matrix of the remaining 9 experts was used in the same way as above, and the weights of each indicator were measured, and the mean value was found to obtain the weight results: item A (0.2729), item B (0.2177), item C (0.2032), and item D (0.3062).
Patient education intensity was defined as the time cost as the main intensity grading basis, and the average monthly education hours = total number of A items × average time required per A item × weighting factor + total number of B items × average time required per B item × weighting factor + total number of C items × average time required per C item × weighting factor + total number of D items × average time required per D item × weighting factor / total Number of months of education.
The total number of Project A is the total number of video broadcast participation, with an average of 60 min/time; the total number of Project B and C is the total number of problems recorded in the platform information including drug counseling, diet counseling, exercise counseling, psychological counseling, risk prevention, and problem solving, with an average time required for each problem solving of about 5 min; the total number of Project D is the total number of on-site hospital education, with an average time required for each face-to-face consultation and on-site education guidance of about 10 min. The intensity level was divided into 2 intensities of high and low whether ≥ median (130.5 min/month).
Based on the significant efficacy of rosacea within 6 months (CEA<1, IGA<1), patients were divided into the attainment group (CEA<1, IGA<1) and the non-attainment group (CEA≥1, IGA≥1), and the baseline information of age, gender, education level, duration of rosacea, treatment regimen, education intensity, CEA, and IGA were compared between the two groups, respectively. Logistic regression analysis was performed to analyze the factors influencing the significant efficacy of rosacea.
Statistical Methods
Data satisfying the normal distribution measures are expressed as  , and t-test was used. The non-normally distributed measures are expressed as median and upper and lower quartiles [M (P25, P75)], and the rank sum test was used. The statistical data were expressed as n (%) using the χ2 test. Logistic regression was used to analyze the factors influencing the significant efficacy of rosacea. The test level α was taken as 0.05, and differences were considered statistically significant if P<0.05. SPSS 21.0 statistical software was used for data analysis.
, and t-test was used. The non-normally distributed measures are expressed as median and upper and lower quartiles [M (P25, P75)], and the rank sum test was used. The statistical data were expressed as n (%) using the χ2 test. Logistic regression was used to analyze the factors influencing the significant efficacy of rosacea. The test level α was taken as 0.05, and differences were considered statistically significant if P<0.05. SPSS 21.0 statistical software was used for data analysis.
Results and Discussion
Results
A total of 125 patients were included in the study, all female, median age 37.0 (30.0, 48.0) years, median duration of rosacea 3.0 (1.0, 4.0) years, education level (primary to university), mean median education intensity 130.5 (72.5, 180.8) min/month; 67 patients in the attainment group and 58 patients in the non-attainment group, attainment group The median age of patients in the standardized group was 37.0 (29.0, 45.0) years, the median disease duration was 3.0 (2.0, 4.0) years, and the median mean educational intensity was 170.4 (110.8, 198.8) min/month; the median age of patients in the non-standardized group was 37.0 (30.0, 48.3) years, the median disease duration was 2.0 (1.0, 2.3) years, and the mean educational intensity was 86.9 (1.0, 2.3) min/month. The median education intensity was 86.9 (52.00, 152.3) min/month. There was a significant difference in the mean length of education between the two groups (P<0.05), and the rest of the differences between the two groups at baseline were not statistically significant (P>0.05) (Table 1).
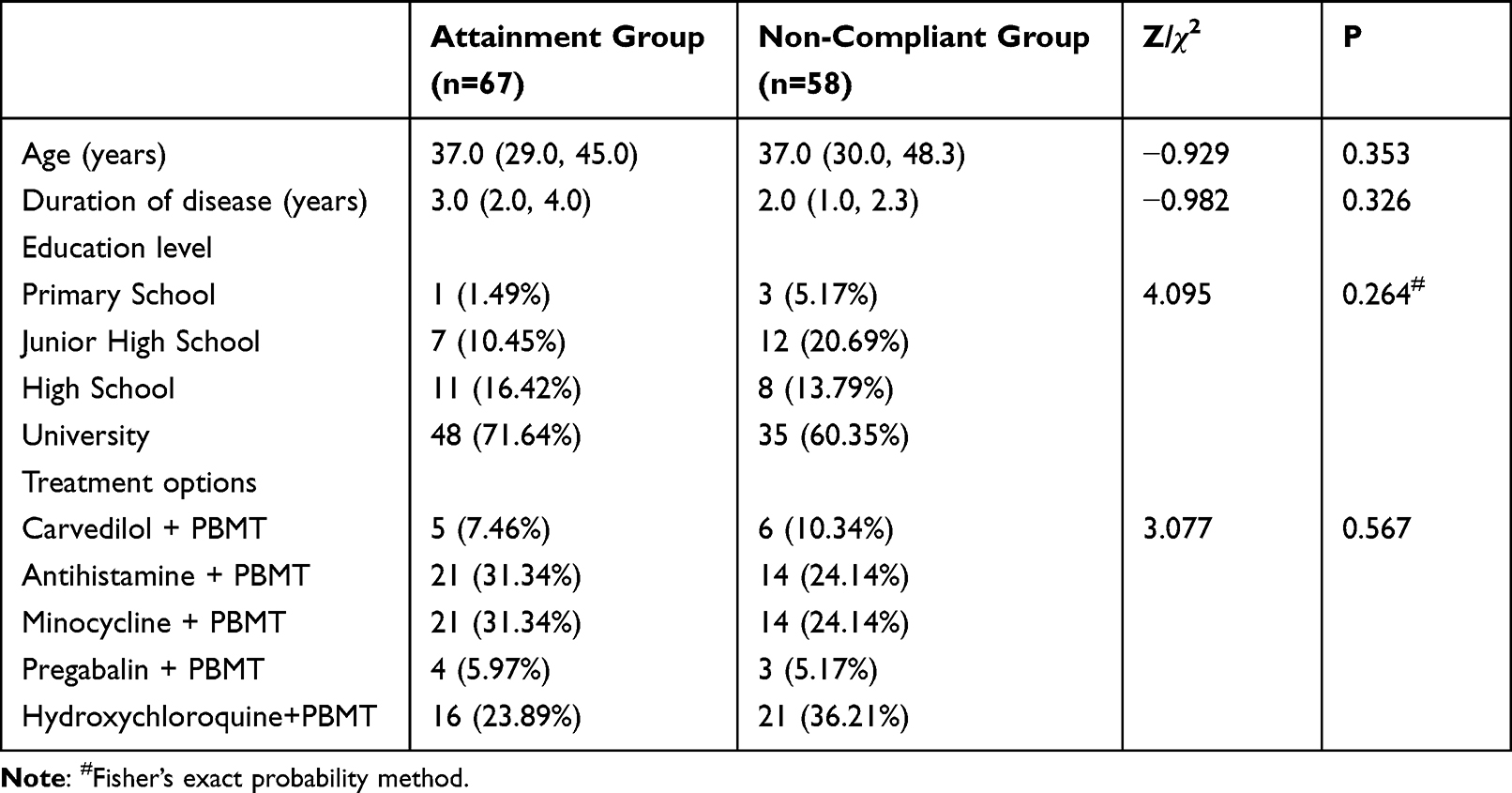 |
Table 1 Comparison of Baseline Information Between the Two Groups [M (P25, P75), n (%) |
Criteria for rosacea treatment efficacy (CEA score <1, IGA score <1) was used as the dependent variable, and age (<45 years, ≥45 years), duration of disease (<5 years, ≥5 years), education, treatment regimen, baseline CEA (<3, ≥3), baseline IGA (<3, ≥3), and education intensity (<130.5 min/month is defined as low, and ≥130.5 min/month is classified as high). Logistic regression analysis showed that the variable that significantly affected the treatment efficacy of rosacea was the mean length of education (≥130.5 min/month), and education intensity was significantly associated with rosacea treatment efficacy. High education intensity accounted for 67.16% (45 cases) in the attainment group and 31.03% (18 cases) in the non-attainment group (Table 2).
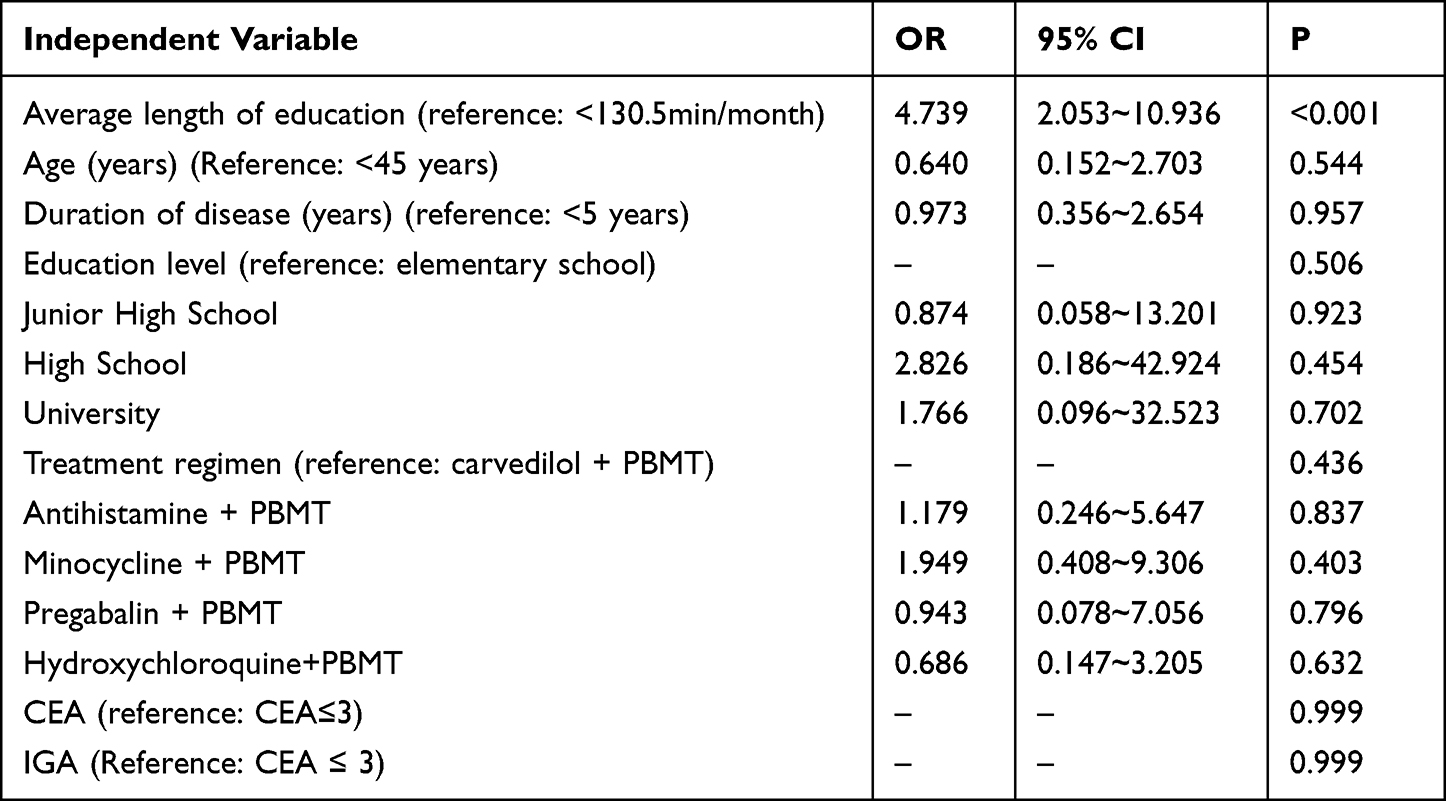 |
Table 2 Logistic Regression Analysis of Factors Influencing Significant Efficacy of Rosacea After 6 Months of Regular Follow-Up |
Discussion
This study conducted a retrospective analysis to examine the factors influencing the treatment of rosacea patients who received regular follow-up with self-management support within the new media chronic disease management model. The findings revealed a notable disparity in educational intensity between the treatment attainment group and the treatment non-attainment group after six months of regular follow-up. The treatment attainment group demonstrated a high educational intensity of 67.16%, whereas the treatment non-attainment group had a significantly lower educational intensity of 31.03%. Furthermore, a significant correlation was observed between high-intensity patient education and favorable outcomes in rosacea management. Patients who received more intensive educational support were more likely to achieve significant improvements. However, no significant correlations were found between age, duration of illness, literacy, treatment regimen, baseline CEA, baseline IGA, and rosacea outcomes.
Our findings indicated that patients belonging to the treatment-attainment group exhibited a higher level of responsiveness towards live video streaming, voice communication, problem-solving dialogues, and in-hospital education. Additionally, these patients actively engaged in proactive disease introduction and home care education. During the course of treatment, patients in the treatment-attainment group demonstrated a greater willingness to engage in open discussions regarding medication, diet, exercise, psychological well-being, and risk prevention. Consequently, their overall self-management skills were significantly enhanced.
One plausible explanation is that patients with higher educational intensity tend to possess a more comprehensive understanding of the disease and possess stronger self-management skills. Consequently, they are more likely to adopt and implement medical advice.16 These patients exhibit a better grasp of rosacea’s characteristics, its progression, and the significance of treatment, enabling them to effectively employ self-management techniques and adhere to appropriate medication usage. On the contrary, patients with low educational intensity may face cognitive limitations and encounter challenges in self-management, impeding their ability to effectively manage the progression of the disease on their own. Therefore, the level of educational intensity significantly impacts the treatment of rosacea patients, and by offering more intensive educational support, patients are more likely to attain noteworthy outcomes.
It is important to note that this study is a retrospective study and has some limitations. Firstly, the sample size was relatively small, which may introduce selective bias17. Conducting larger-scale studies would offer more robust evidence to substantiate these findings. Secondly, our analysis focused solely on the association between educational intensity and treatment efficacy, while other factors such as psychological status and lifestyle might also exert an influence on treatment outcomes. These factors warrant further investigation and study.
Furthermore, in our efforts to enhance the quality of clinical decision-making, we utilized a hierarchical analysis of power (AHP) to determine the actual level of impact associated with each educational program18. However, due to the absence of established guidelines or broadly accepted standards for the rosacea self-management support model, we were unable to account for all potential confounding variables, introducing the possibility of influence on the observed results.
Conclusions
In conclusion, the findings of this study suggest that increased educational intensity positively influences the treatment of individuals with rosacea. Subsequent research can delve into strategies for providing more effective educational support to empower patients in acquiring self-management skills, ultimately enhancing treatment outcomes and improving the overall quality of life for rosacea patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The National Natural Science Foundation of China (82273559; 82073473); Clinical Research Innovation Project, West China Hospital, Sichuan University (19HXCX010).
Disclosure
Xu Liu and Min-Kyu Kim are co-first authors for this study. All authors declare no conflicts of interest in this work.
References
1. Thiboutot D, Anderson R, Cook-Bolden F, et al. Standard management options for rosacea: the 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2020;82(6):1501–1510. doi:10.1016/j.jaad.2020.01.077
2. Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: the 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018;78(1):148–155. doi:10.1016/j.jaad.2017.08.037
3. Yang F, Zhang Q, Song D, Liu X, Wang L, Jiang X. A cross-sectional study on the relationship between rosacea severity and quality of life or psychological state. Clin Cosmet Investig Dermatol. 2022;15:2807–2816. doi:10.2147/ccid.S390921
4. Dai R, Lin B, Zhang X, Lou Y, Xu S. Depression and anxiety in rosacea patients: a systematic review and meta-analysis. Dermatol Ther. 2021;11(6):2089–2105. doi:10.1007/s13555-021-00613-w
5. Harper J, Del Rosso JQ, Ferrusi IL. Cross-sectional survey of the burden of illness of rosacea by erythema severity. J Drugs Dermatol. 2018;17(2):150–158.
6. Bubak C, Schaarschmidt ML, Schöben L, Peitsch WK, Schmieder A. Analyzing the value of an educational program for psoriasis patients: a prospective controlled pilot study. BMC Public Health. 2019;19(1):1535. doi:10.1186/s12889-019-7778-x
7. Bostoen J, Bracke S, De Keyser S, Lambert J. An educational programme for patients with psoriasis and atopic dermatitis: a prospective randomized controlled trial. Br J Dermatol. 2012;167(5):1025–1031. doi:10.1111/j.1365-2133.2012.11113.x
8. Pickett K, Frampton G, Loveman E. Education to improve quality of life of people with chronic inflammatory skin conditions: a systematic review of the evidence. Br J Dermatol. 2016;174(6):1228–1241. doi:10.1111/bjd.14435
9. Sahin U, Reeve K, Tochtermann G, et al. HautTief multidisciplinary educational program for patients with psoriasis or atopic dermatitis: a randomized controlled study. Dermatology. 2022;238(6):1050–1059. doi:10.1159/000524225
10. Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 1: a status report on the disease state, general measures, and adjunctive skin care. Cutis. 2013;92(5):234–240.
11. Cices A, Alexis AF. Patient-focused solutions in rosacea management: treatment challenges in Special Patient Groups. J Drugs Dermatol. 2019;18(7):608–612.
12. Trave I, Micalizzi C, Cozzani E, Gasparini G, Parodi A. Papulopustular rosacea treated with ivermectin 1% cream: remission of the demodex mite infestation over time and evaluation of clinical relapses. Dermatol Pract Concept. 2022;12(4):e2022201. doi:10.5826/dpc.1204a201
13. Li H, Wu X, Shen J, Lou S. Perspective and experience of patients with aplastic anemia on medication adherence. Patient Prefer Adherence. 2023;17:2215–2225. doi:10.2147/ppa.S390409
14. Alinia H, Moradi Tuchayi S, Farhangian ME, et al. Rosacea patients seeking advice: qualitative analysis of patients’ posts on a rosacea support forum. J Dermatolog Treat. 2016;27(2):99–102. doi:10.3109/09546634.2015.1133881
15. Rosacea Research Center CSoD, Rosacea Professional Committee, Chinese Dermatologist Association. Guidelines for the diagnosis and treatment of rosacea in China (2021 edition). Chin J Dermatol. 2021;54(4):279–288. doi:10.35541/cjd.20201078
16. M’Imunya JM, Kredo T, Volmink J. Patient education and counselling for promoting adherence to treatment for tuberculosis. Cochrane Database Syst Rev. 2012;2012(5):Cd006591. doi:10.1002/14651858.CD006591.pub2
17. Talari K, Goyal M. Retrospective studies - utility and caveats. J R Coll Physicians Edinb. 2020;50(4):398–402. doi:10.4997/jrcpe.2020.409
18. Dolan JG. Shared decision-making--transferring research into practice: the Analytic Hierarchy Process (AHP). Patient Educ Couns. 2008;73(3):418–425. doi:10.1016/j.pec.2008.07.032
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of the Reliability and Clinical Applicability of ChatGPT’s Responses to Patients’ Common Queries About Rosacea
Yan S, Du D, Liu X, Dai Y, Kim MK, Zhou X, Wang L, Zhang L, Jiang X
Patient Preference and Adherence 2024, 18:249-253
Published Date: 31 January 2024