Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Patient Characteristics Associated with NPO (Nil Per Os) Non-Compliance in the Pediatric Surgical Population
Authors Ghimire A, Maves GS, Kim SS, Raman VT, Tobias JD ![]()
Received 10 February 2022
Accepted for publication 30 May 2022
Published 16 June 2022 Volume 2022:13 Pages 235—242
DOI https://doi.org/10.2147/PHMT.S361866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Anuranjan Ghimire,1 Gregory S Maves,1,2 Stephani S Kim,1,2 Vidya T Raman,1,2 Joseph D Tobias1,2
1Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Anesthesiology & Pain Medicine, the Ohio State University College of Medicine, Columbus, OH, USA
Correspondence: Anuranjan Ghimire, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Dr, Columbus, OH, 43235, USA, Tel +1 614-722-4200, Fax: +1 614-722-4203, Email [email protected]
Introduction: Cancellation of surgery or delay on the day of service is a huge burden for the patient, family, and healthcare system. Preventable delays impact efficiency and workflow, which may increase costs due to overtime and idle rooms during peak hours. Non-compliance to nil per os (NPO) guidelines remains one of the most common preventable causes for surgical cancellations. The current study sought to investigate and understand patient factors that may be associated with non-compliance to NPO guidelines.
Methods: After IRB approval, a retrospective review of completed and cancelled pediatric procedures requiring the use of anesthesia over a 5-year period was performed. Emergency procedures and inpatient surgeries were excluded. Data regarding patient demographics and surgical service were extracted from the electronic medical records for comparison. A logistic regression model was used to identify factors associated with cancellations due to NPO non-compliance.
Results: There were 825 cancellations due to NPO non-compliance of 144,049 cases for an incidence of 0.57% over the 5-year period. Patients in the 6– 12 year old age range and those who self-identified as non-White or non-English speaking had a higher incidence of cancelling due to NPO non-compliance. Compared to ear, nose, and throat (ENT) procedures, cancellations due to NPO non-compliance were more likely in radiology, dental, and urology procedures.
Discussion: Many factors may impact a family’s compliance with NPO guidelines. Patient-related factors included those who self-identified as non-White or non-English speaking. Patients having ENT surgery were less likely to have NPO non-compliance than those having radiologic procedures, dental surgery, or urologic surgery. Future interventions focused on these groups may be most effective in limiting day of surgery cancellations.
Keywords: nil per os, pediatric anesthesia, cancellation
Introduction
Surgery is a stressful process for both patients and their families, requiring significant physical and mental preparation, even for minor outpatient procedures.1,2 Day of surgery cancellation results in a significant burden for families both emotionally and economically. In addition, these potentially preventable cancellations impact operating room efficiency and workflow, increasing costs to hospitals when operating rooms are idle during peak hours or when overtime is required to finish the surgical list.3 Despite education, use of preoperative evaluations, and frequent communication, a significant number of scheduled pediatric surgical procedures are cancelled every day throughout the United States and beyond.4–6 In pediatric surgery, reasons for surgical cancellation most commonly include the development of acute medical conditions (including upper respiratory infections), scheduling miscommunications, and non-compliance with nil per os (NPO status).
Preoperative fasting is intended to decrease the volume and acidity of gastric contents and decrease the risk of pulmonary aspiration.7,8 According to the Practice Guidelines for Preoperative Fasting from the American Society of Anesthesiologists, fasting should be 2 hours for clear liquids, 4 hours for human milk, 6 hours for infant formula and non-human milk, and 8 hours for solid food.8 Given the potential consequences of perioperative aspiration, strict adherence to NPO guidelines is necessary. Various written, verbal, electronic, and social media devices have been used in an effort to ensure effective communication, improve compliance with NPO guidelines, and decrease day of surgery cancellations due to NPO non-compliance. However, NPO non-compliance remains a frequent cause of preventable surgical cancellations.
Various demographic and clinical characteristics may impact the risk of NPO non-compliance. Identification of such factors may provide a framework for targeted interventions to change these behavior patterns and decrease the incidence of NPO non-compliance in at-risk groups. These interventions would serve to lessen the emotional and economic burdens associated with NPO non-compliance for both the family and the healthcare system. The current study sought to investigate patient, family-related, and surgical service demographics that may be associated with non-compliance to NPO guidelines in infants and children presenting for scheduled surgery in a tertiary care children’s hospital.
Methods
This study was approved by the Institutional Review Board at Nationwide Children’s Hospital (Columbus, Ohio). The study was conducted within the guidelines of the Declaration of Helsinki. Due to the retrospective nature of the study and the absence of impact on clinical care, the need for written informed consent was waived. Patient confidentiality was maintained by the use of deidentified data for publication. Further protection is provided as all research records are stored in a locked cabinet in a secure location or in a password-protected computer file. The list linking the assigned code number to individual subjects is maintained separately from the other research data. Only certified research personnel will be given access to identifiable subject information.
Electronic medical records were queried for all completed and cancelled procedures requiring or scheduled for anesthesia over a 5-year period. Age, gender, race, ethnic group, language spoken at home, type of insurance, American Society of Anesthesiologists (ASA) physical status, and primary surgical service were collected. Age was categorized into less than 1 year, 1–2 years, 3–5 years, 6–9 years, 10–12 years, and greater than 13 years. Race and ethnic group were categorized as White, African American, Other, and did not or chose not to answer. Language was categorized as English, Spanish, Somali, and Other. Insurance was categorized as private/commercial, public, and other. Primary surgical service categories were ENT, radiology, dental, urology, ophthalmology, plastic surgery, pediatric surgery, orthopedic surgery, and other. The other category was used due to a large discrepancy in surgical volume between the surgical services listed above and other surgical services at our institution after exclusion of inpatients and emergencies. The other category included cardiology, dermatology, gastroenterology, hematology/oncology, neurosurgery, gynecology, oral maxillary, pediatric and adolescent gynecology, and thoracic services.
Statistical Analysis
Number and percentage were calculated for categorical variables. Differences between patients who cancelled because of NPO non-compliance and patients who did not cancel were calculated using Fisher’s exact test or chi-square test. Univariate and multivariate logistic regression models were used to calculate odds ratios (OR) and 95% confidence intervals (CI) for predictors of NPO cancellation. All analyses were performed using SAS 9.4 (Cary, NC).
Results
A total of 144,049 patients underwent elective surgery over the 5 year study period. Of the study cohort, 64,070 (44%) were male and 79,979 (56%) were female. The demographic data and procedure characteristics of cancelled cases due to NPO non-compliance versus non-cancelled cases are shown in Table 1. The odds ratio (OR) and 95% confidence intervals (CI) for risk of cancellation due to NPO non-compliance are listed in Table 2. Patients in the 10–12 year age group had the highest odds of surgical cancellation due to NPO non-compliance compared to other groups, with an odds ratio of 1.63 (CI: 1.28, 12.07) when compared to the reference point set at the 3–5 year age group. Similarly patient in 6–9 years age group had a higher odds of surgical cancellation with an OR of 1.25 (CI: 1.05, 1.50). Children who were more than 13 years of age had a lower odds of same day surgical cancellation due to NPO non-compliance (OR: 0.68; CI: 0.51, 0.89). Other factors noted to be associated with a higher odds ratio of cancellation due to NPO non-compliance included patients who identified as non-White ethnic background or chose not to identify, non-English or Spanish speaking patients, and those with public or other insurance compared to private or commercial insurance. There was also a higher OR for day of surgery cancellation due to NPO non-compliance in patients presenting for dental procedures, radiologic imaging or urologic surgery when compared to ENT surgery.
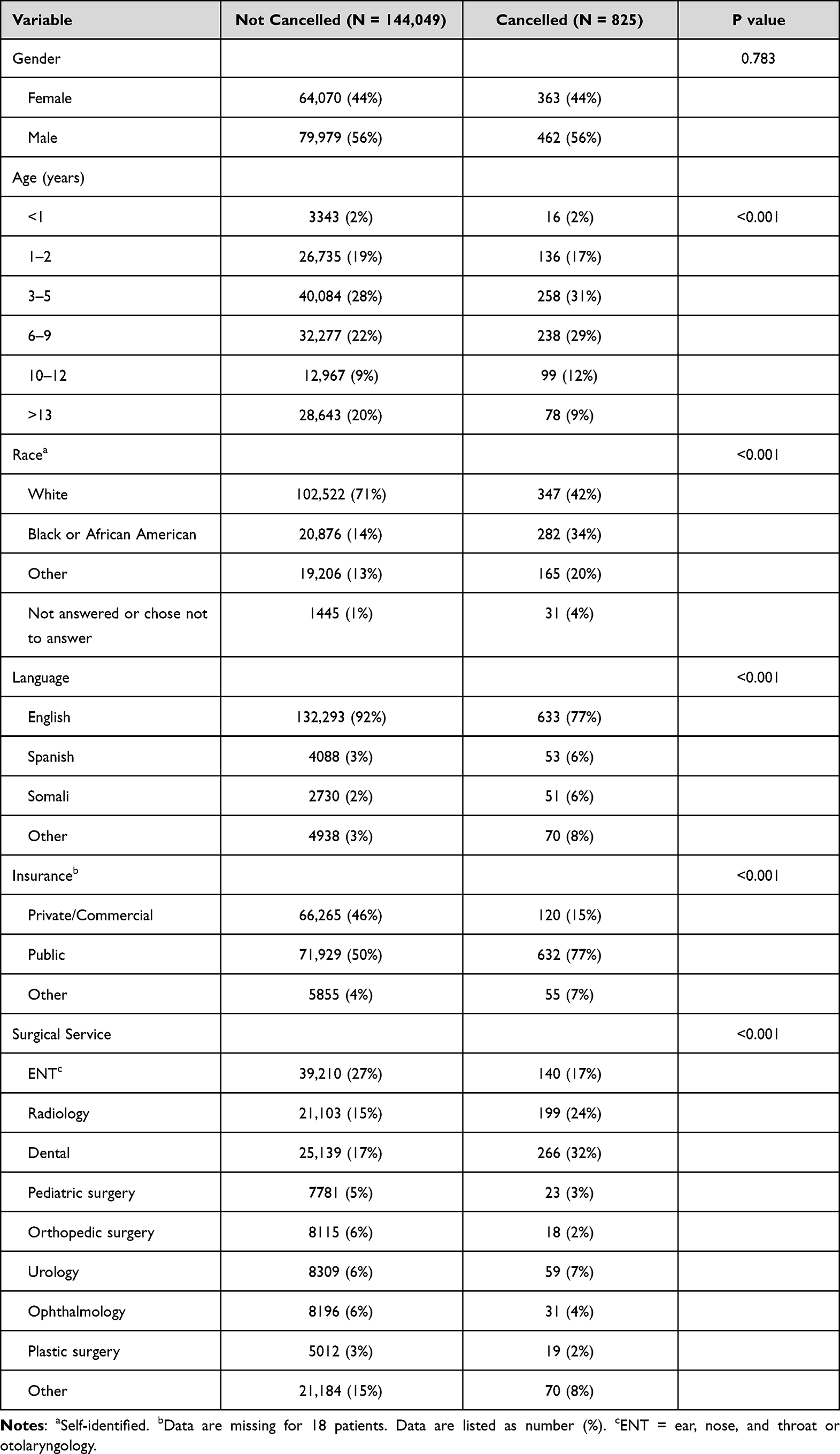 |
Table 1 Demographic and Patient Characteristics |
 |
Table 2 Odds Ratios and 95% Confidence Intervals for Predictors of NPOa Violations |
Discussion
In this large cohort of more than 140,000 non-emergency procedures in patients presenting to the hospital on the day of surgery, we noted an incidence of same-day surgery cancellation of 0.57% over the 5-year period. Patients in the 6–9 year and the 10–12 year age group had a higher incidence of surgical cancellation due to NPO non-compliance compared to other groups with the 3–5 year age group used as the reference point. Other factors associated with a higher incidence of cancellation included non-White ethnic groups, non-English speaking patients, and insurance other than private or commercial. Furthermore, we noted a higher incidence in patients presenting for radiologic imaging, dental surgery or urologic surgery. This incidence is on the lower end of what has been previously reported and reinforces the efficacy of our preoperative process, which includes a discussion of NPO regulations at 3 times during the preoperative process including the surgeon during the preoperative visit, during our preoperative assessment, which is performed during a scripted phone call by a trained group of preoperative admission testing (PAT) registered nurses, and a reminder phone call by a registered nurse the day before surgery.
Cancellation of surgery accounts for a huge financial burden to the institution with additional economic and emotional impact to the patient and family. Turunen et al estimated the financial burden of day of surgery cancellations to be nearly a million euros during a 9-month study period in an academic hospital in Finland.9 The study was conducted after a structured preoperative protocol had been implemented to limit same day surgery cancellations. In addition to the impact on the hospital, there may be significant patient-related consequences including lost days at work and negative psychological effects in adults.10
The first step in the preoperative process to ensure an adequate NPO time is the delivery of appropriate instructions from the healthcare provider to the parents and the patient. At our institution for patients presenting on the day of surgery, NPO instructions are delivered at three different times including during the surgical preoperative visit, during our preoperative admissions testing process when a preoperative history is performed over the phone by a trained RN, and the day before surgery when preoperative instructions are given during a phone call. At our institution and at many, there is no formal preoperative examination performed by a physician or anesthesiologist prior to the day of surgery and written instructions are not given regarding NPO times. In an effort to cut healthcare costs and avoid unnecessary hospital visits, our preoperative evaluation is performed over the phone by a trained RN.
However, not all the patients instructed to fast before surgery follow perioperative fasting guidelines for various reasons. Surgical cancellation due to NPO non-compliance remains a common and potentially correctable cause if reasons for or factors associated with NPO non-compliance can be identified.4 Primary among these may be parental miscommunication with lack of understanding of the fasting requirements, parental anxiety levels, and a lack of understanding of the safety implications of appropriate fasting.11,12 In our large cohort, we noted that cancellation due to NPO non-compliance was higher based on age, race/ethnicity, primary language spoken, insurance type, and the surgical services involved. In the retrospective analysis of the data obtained via the EMR, we found some distinct differences between the NPO non-compliant and compliant groups. When compared to patients who were 3–5 years of age, slighting only patients (6–9 and 10–12 years of age) had a higher cancellation rate while patients who were more than 13 years of age had a lower incidence. It is likely that adolescents (˃13 years of age) are more likely to be at a cognitive level where they listen to and understand the importance of NPO status. Furthermore, the lower incidence in the 3–5 year group likely relates to increased direct parental supervision in various aspects of care including feeding and dietary intake. This group may also be subject to stricter parental supervision during NPO times as it is appreciated that their cognitive level may not result in the ability to closely follow rules and preoperative expectations.
Various other authors have investigated factors associated with surgery cancellation related to NPO non-compliance. In a retrospective evaluation of NPO non-compliance resulting in surgery cancellation, Billings et al reported a 1.5% incidence of NPO non-compliance in a cohort of 42, 495 patients.13 In contrast to our study, patients with NPO non-compliance had a median age of 3 years and the 0–6 year age group represented 67.4% of all patients with NPO non-compliance. Similar to our findings, they noted a higher incidence in patients who identified Spanish as their primary language, patients with Medicaid insurance, and patients presenting for otolaryngologic procedures. This represents a significant area that could be improved during our preoperative process and one that has been noted previously to impact healthcare.14 As the primary language at our institution is English, even with the use of an interpreter, misunderstandings between the perioperative staff and patient families may occur. Improvement in written and verbal communication for non-English speaking families appears to be an important intervention that may help decrease the incidence of NPO non-compliance.
There was a higher incidence of NPO non-compliance in patients requiring anesthesia for procedures in radiology and operative dentistry. Urology was also noted be at higher odds of cancellation, but to a lesser extent than the services mentioned previously. The etiology for the increased risk of NPO non-compliance in these particular services is likely multifactorial. For patients presenting to radiology requiring the use of anesthesia for imaging or procedures (MRI, CT, interventional radiology), these patients may not be seen by a medical physician prior to the procedure so that one aspect of the preoperative visit (the preoperative surgical visit) is absent. These patients are reviewed and follow the same process through our PAT and the pre-procedure phone call the night before. The anesthetic requirements for these children is often referred to as “sedation” or “procedural sedation” when in reality given our clinical practice, general anesthesia is used for the vast majority of our radiologic imaging as well as IR procedures. This may result in confusion for parents who do not understand that the NPO guidelines as the same whether presenting for an MR scan or a hernia repair. In addition, our radiologic procedures are often scheduled with more advanced planning than our surgical procedures so that other than the perioperative nursing phone call the day prior to the procedure, there may be a significant lag time before discussions with healthcare providers and the day of the procedure. Likewise for dental procedures, parents may not fully comprehend that these procedures will be performed under general anesthesia. Given the extent of the dental issues in most of our patients, these procedures are most easily accomplished using general anesthesia with endotracheal intubation unlike the twilight sedation (30–50% nitrous oxide with oral premedication) used in dental offices. Additionally, for patients presenting for operative dental procedures, this patient population may be at an increased risk of non-compliance as there is generally some component of non-compliance with routine dental care and hygiene that has resulted in significant tooth decay and the need for these services.
Families without private insurance (non-private insurance carriers or no insurance) had higher odds of cancellation of surgery due to NPO non-compliance. Previous studies have demonstrated the potential association of various healthcare and hospital outcomes including NPO non-compliance based on the type of insurance.15,16 This association is even more difficult to truly define as it is likely multifactorial related to various family and socioeconomic factors. However, as with many of the factors discussed, improved communication through various venues (verbal, written, social media, text, etc.) should be considered as preliminary interventions.
Various limitations of the current study included its retrospective nature and the dependence on being able to extract information from the EMR. We caution when interpreting the data regarding correlation between patients that self-identify as non-white being higher risk of non-compliance. Differences in socioeconomic status were not able to be identified in our retrospective data set. The study included only patients that had their procedure cancelled due to the NPO non-compliance and not those who had an NPO non-compliance and had their procedure delayed to later in the day. This occurs most commonly in a busy ENT room when it is easiest to move a case to later in the day due to NPO non-compliance when there are multiple other patients arriving at the hospital awaiting their surgical procedures. As a result, NPO non-compliance may be slightly underreported in our study. As the study involved a 5-year period, there may have been variation in how the information regarding NPO rules is presented. Additionally, as the preoperative evaluations and phone call the night before surgery involve several staff, it is likely that there was some variation in how the information was presented. There is no specific script that is set to provide this information. Furthermore, although all patients had a formal review by our PAT nursing team, we were not able to identify patients who we could not contact the night before surgery due to phone calls that were not answered or returned. When evaluating other factors that may impact parental understanding of preoperative instructions, given the retrospective nature of the study, we were not able to obtain information on parental educational levels. When future, prospective trials are planned, the potential impact of these factors (parental education level and socio-economic status) on NPO compliance should be evaluated.
In summary, this large cohort of patients provided helpful information in identifying potential patient-related factors associated with non-compliance with NPO guidelines resulting in cancellation of surgical and radiologic procedures in patients presenting the day of surgery. In addition to specific age groups (6–9 and 10–12 years of age) and types of surgical/radiologic procedures that accounted for a higher incidence of non-compliance with NPO guidelines, we also noted specific patient demographic findings including those who identified as non-White and non-English speaking. When considering these findings, we postulate that there are certain interventions that might be effective in decreasing NPO non-compliance and surgical cancellations. These strategies should aim to increase education and augment effective communication. Key among these is a better explanation of the safety reasons behind the need to ensure NPO compliance. Along with this education, it may be helpful to further encourage the liberal administration of clear liquids up to 2 hours before surgery as prolonged NPO times may be equally disadvantageous for perioperative outcomes.17 Likely most important are the avenues along which we communicate. The majority if not all of our communication and information exchange during the preoperative period is verbal. While closed loop communication and the use of a specific script may improve the transmission of verbal information, other media can be used to provide the needed perioperative information. When such information is provided by written handouts, on-line videos, or text messages, families have ready access to and can review the information whenever they want. We have also previously demonstrated the efficacy of a video for providing postoperative instructions following adenotonsillectomy.18 Although we have ready access to translators for non-English speaking patients, written handouts can be provided in various languages based on patient preference. A similar process is already in place for our preoperative consent process as we use interpreters, but also have our standard preoperative anesthesia consent available in several of the most commonly spoken languages in our communities.
Funding
There was no internal or external funding acquired for this study.
Disclosure
Dr Vidya T Raman reports personal fees from Merck for honorarium for panel participation, formerly owned personal stocks from Johnson and Johnson, equities from Nds Kalstars, Opus Influunt, and Face 2 Face, outside the content of the submitted work. The authors report no other conflicts of interest related to this study.
References
1. Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative anxiety in children: predictors and outcomes. Arch Pediatr Adolesc Med. 1996;150(12):1238–1245.
2. Kotiniemi LH, Ryhänen PT, Moilanen IK. Behavioural changes in children following day-case surgery: a 4-week follow-up of 551 children. Anaesthesia. 1997;52(10):970–976.
3. Tait AR, Voepel-Lewis T, Munro HM, Gutstein HB, Reynolds PI. Cancellation of pediatric outpatient surgery: economic and emotional implications for patients and their families. J Clin Anesth. 1997;9(3):213–219.
4. Boudreau SA, Gibson MJ. Surgical cancellations: a review of elective surgery cancellations in a tertiary care pediatric institution. J Peri Anesthesia Nurs. 2011;26(5):315–322.
5. Knox M, Myers E, Wilson I, Hurley M. The impact of pre-operative assessment clinics on elective surgical case cancellations. Surgeon. 2009;7(2):76–78.
6. Talalwah N, McIltrot KH. Cancellation of surgeries: integrative review. J Peri Anesthesia Nurs. 2019;34(1):86–96.
7. Ljungqvist O, Søreide E. Preoperative fasting. Br J Surg. 2003;90(4):400–406.
8. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures. An updated report by the American Society of Anesthesiologists Task Force on Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration. Anesthesiology. 2017;126(3):376–393.
9. Turunen E, Miettinen M, Setälä L, Vehviläinen-Julkunen K. Financial cost of elective day of surgery cancellations Financial cost of elective day of surgery cancellations. J Hosp Adm. 2018;7(6):30–36.
10. Lankoandé M, Bonkoungou P, Ki BK, et al. Economic and psychological burden of scheduled surgery cancellation in a sub-Saharan country (Burkina Faso). South Afr J Anaesth Analg. 2017;23(6):145–151.
11. Cantellow S, Lightfoot J, Bould H, Beringer R. Parents’ understanding of and compliance with fasting instruction for pediatric day case surgery. Pediatr Anesth. 2012;22(9):897–900.
12. Chahal N, Manlhiot C, Colapinto K, Van AJ, McCrindle BW, Rush J. Association between parental anxiety and compliance with preoperative requirements for pediatric outpatient surgery. J Pediatr Heal Care. 2009;23(6):372–377.
13. Billings KR, Schneider AL, Safri S, Kauffunger L, Valika T. Patient factors associated with NPO violations in a tertiary care pediatric otolaryngology practice. Laryngoscope Investig Otolaryngol. 2020;5(6):1227–1232.
14. Shamsi AH, Almutairi AG, Al MS, Al KT. Implications of language barriers for healthcare: a systematic review. Oman Med J. 2020;35(2):e122.
15. Todd J, Armon C, Griggs A, Poole S, Berman S. Increased rates of morbidity, mortality, and charges for hospitalized children with public or no health insurance as compared with children with private insurance in Colorado and the United States. Pediatrics. 2006;118(2):577–585.
16. Beazley B, Bulka C, Landsman IS, Ehrenfeld JM. Demographic predictors of NPO violations in elective pediatric surgery. J Perianesthes Nurs. 2016;31(1):36–40.
17. Thomas M, Morrison C, Newton R, et al. Consensus statement on clear fluids fasting for elective pediatric general anesthesia. Paediatr Anaesth. 2018;28(5):411–414.
18. Khan S, Tumin D, King A, et al. Utilization of a postoperative adenotonsillectomy teaching video: a pilot study. Int J Pediatr Otorhinolaryngol. 2017;102:76–79.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perioperative Management for Emergency Surgery in Pediatric Patients with COVID-19: Retrospective Observational Study
Giwangkancana G, Oktaliansah E, Ramlan AAW, Utariani A, Kurniyanta P, Arifin H, Widyastuti Y, Pratiwi A, Syukur R
Open Access Emergency Medicine 2022, 14:515-524
Published Date: 20 September 2022