Back to Journals » Patient Preference and Adherence » Volume 19
Patient-Centred Gestational Diabetes Care: Preference Elicitation Methods and Machine Learning Innovations
Authors Alharmoodi S, Al Nweran M, El-Kebbi I, Everett D, Ibrahim SM, Farhat J, Al-Omari B ![]()
Received 12 September 2025
Accepted for publication 11 November 2025
Published 24 December 2025 Volume 2025:19 Pages 4219—4231
DOI https://doi.org/10.2147/PPA.S567113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Shaikha Alharmoodi,1,* Mariam Al Nweran,1,* Imad El-Kebbi,2 Dean Everett,1,3 Saleh Mohamed Ibrahim,4,5 Joviana Farhat,1 Basem Al-Omari1
1Department of Public Health and Epidemiology, College of Medicine and Health Sciences, Khalifa University of Science and Technology, Abu Dhabi, United Arab Emirates; 2Division of Endocrinology, Sheikh Shakhbout Medical City (SSMC), Abu Dhabi, United Arab Emirates; 3Infection Research Unit, Khalifa University of Science and Technology, Abu Dhabi, United Arab Emirates; 4College of Medicine and Health Sciences, Khalifa University of Science and Technology, Abu Dhabi, United Arab Emirates; 5Center for Biotechnology, Khalifa University of Science and Technology, Abu Dhabi, United Arab Emirates
*These authors contributed equally to this work
Correspondence: Basem Al-Omari, Department of Public Health and Epidemiology, College of Medicine and Health Sciences, Khalifa University of Science and Technology, P.O. Box 127788, Abu Dhabi, United Arab Emirates, Tel +971 2 312 4452, Email [email protected] Joviana Farhat, Department of Public Health and Epidemiology, College of Medicine and Health Sciences, Khalifa University of Science and Technology, P.O. Box 127788, Abu Dhabi, United Arab Emirates, Email [email protected]
Abstract: Gestational Diabetes Mellitus (GDM) requires long-term management, frequent visits, and additional financial costs compared to normal pregnancies. Patients often express preferences for services that save time, reduce expenses, and simplify screening. Virtual and telehealth services are valued as they shorten travel and waiting times, lower costs, and improve satisfaction. Screening preferences emphasize accuracy, affordability, and convenience, while recent machine learning (ML) models have enhanced prediction and early detection, supporting more personalized strategies. Patients’ preferences have been explored through qualitative, quantitative, and mixed methods, which capture lived experiences, quantify trade-offs, and contextualize results. This review aims to examine GDM patients’ experiences with time, costs, and screening, highlight the role of machine learning in screening, and synthesize evidence from preference-elicitation methods to inform patient-centred care. By linking patient preferences with technological advances in ML, this review provides a broader and more integrated perspective than previous reviews, helping to guide future GDM research and service design.
Keywords: gestational diabetes mellitus, patient preferences, quantitative, qualitative, machine learning
Introduction
In recent years, the evaluation of healthcare services has been considered a crucial component for achieving high-quality care and limiting illnesses and deaths across individuals.1 This is highly relevant to clinical conditions that require long-term management, regular hospital visits, and follow-ups, such as Gestational Diabetes Mellitus (GDM).2 Women with GDM may experience multiple care needs that can make healthcare delivery complex and expensive.3 Recent GDM literature focuses on assessing the quality, accessibility, and utilization of healthcare services among patients.4 Some studies evaluated the link between service quality, patient satisfaction, hospital utilization, and financial performance.5 For example, the lack of available and accessible maternal healthcare services has been associated with limited health outcomes and adverse events in low to middle-income countries.1 In other cases, postpartum screening and follow-up could be affected by social and demographic factors, as well as patient and healthcare providers’ awareness and attitude.6 This justifies the direction of some studies to evaluate the possible variation in healthcare experiences and GDM patients’ preferences based on the model of care applied alongside patients’ inter-individual factors.7 Thus, medical services should be regularly improved based on patients’ needs to ensure adequate health care.8
Multiple qualitative methods, including semi-structured interviews and focus groups, have been widely used to explore GDM patients’ needs, perceptions, and preferences toward healthcare services.9,10 Studies across different regions have shown that women often describe GDM as emotionally demanding and time-consuming, emphasizing challenges in balancing dietary control, self-monitoring, and family responsibilities.11,12 These approaches have helped uncover barriers to self-management, such as limited time, emotional burden, and challenges in adhering to treatment, while also highlighting how cultural beliefs, family support, and communication with healthcare providers influence women’s care experiences and decisions.13 Quantitative methods, primarily Discrete Choice Experiment (DCE), have been used to quantify how patients value different aspects of care, such as visit frequency, screening type, and cost, thereby generating real-world preference data.14 In the past few years, advanced analytical strategies, including Machine Learning (ML) models, have enhanced prediction accuracy and disease classification in GDM.15 Clinically, these models support early diagnosis, guide individualized interventions, and improve patient experience by optimizing healthcare delivery and outcomes.16
This review aims to examine GDM patients’ experiences with time, financial costs, and screening, while highlighting the emerging role of ML in improving screening and diagnosis. It also synthesizes evidence from preference-elicitation methods, including qualitative, quantitative, and mixed approaches, to better understand how women perceive and value different aspects of GDM care.
Materials and Methods
Literature searches utilizing PubMed (MEDLINE), EMBASE, and Web of Science were conducted using terms related to GDM, Patient Preferences, Quantitative, Qualitative, and Machine Learning concepts. No language, age, or date restrictions or filters were applied.
LibreOffice software was used to develop the tables in this manuscript to support high-quality data presentation and differentiation. Figures were designed and structured using PowerPoint.
Patients’ Time
Patients’ time is an important factor to consider when examining patients’ preferences for healthcare services.17 The increase in patient numbers and treatment options requiring services from multiple healthcare professionals (HCPs) may cause long waiting times for consultation.18 This can impact patients’ satisfaction and their responsiveness to the medical information and treatment instructions given by HCPs.19 Some GDM patients correlate the long waiting times in the clinic to their inability to control their glucose levels.20 Another factor is travel time, as some studies reported that 44.5% of GDM patients travelled for more than 30 minutes each way to the hospital.21 Moreover, around 65.1% of pregnant women with diabetes spent more than 2 hours in the clinic, and this percentage increased to 78% when considering travel times that exceeded 15 minutes.21 A travel time of over 30 minutes, with appointment durations varying from 5 to 60 minutes, was also reported.22 Thus, it is understandable that GDM patients prefer to manage their condition remotely through virtual platforms.21
GDM patients require more frequent doctor visits compared to those with normal pregnancies due to a higher risk for complications.23 Therefore, it is recommended that regular clinic visits be made to ensure better glycemic levels, lower risk of premature infant birth, and neonatal intensive care unit (NICU) admissions.24 In many low- and middle-income countries, GDM patients are still non-adherent to the essential services.25 In the northern area of Tanzania, 23% of GDM patients who were screened and scheduled for a next-day appointment and one month for fasting plasma glucose (FPG) and Oral Glucose Tolerance Test (OGTT) did not return.26 Around 35.7% of pregnant South African women designated for GDM testing did not undergo it because of inaccessible telephone lines and relocation from the area.27 This non-adherence may be correlated to obstetric history, financial commitments, transportation limitations, and sociocultural practices.28 A recent Chinese study reported that the majority of pregnant women expressed a preference for fewer hospital visits, especially those with poor socioeconomic backgrounds and residing in remote locations.29
In recent years, advanced technologies have enabled either in-person or remote consultations between clinicians and patients.30 Current evidence shows a high level of patient satisfaction with remote consultations.31 It was reported that 83% of GDM patients had a positive experience with virtual care, particularly due to the benefits of saving both money and time.32 Women residing in rural areas preferred virtual care to avoid long travel times and time off work.22 Women with a history of GDM, who have experienced multiple hospital visits and long wait times at clinics, strongly preferred remote care.21 These patients expressed a willingness to self-manage their condition at home while being monitored remotely by their medical team.21 In developed countries like Singapore, smartphone applications have become a more preferred alternative to in-person visits for pregnant women with GDM.33 However, limited use of digital devices, language obstacles, and older age can affect patient preferences for in-person appointments,34 especially among those with a history of GDM who received limited education.35 Despite the benefits of remote care, some GDM patients continue to prefer the occasional face-to-face appointments.22
However, the effectiveness of telehealth and virtual care is not uniform across all populations. Limited digital literacy, poor internet connectivity, and unequal access to smart devices create a “digital divide” that may exclude women from low-income, rural, or older age groups.36 These barriers can lead to frustration, disengagement, and lower adherence, particularly in regions where health systems lack technical support or user training. Therefore, while telehealth enhances efficiency and accessibility for many, future models must incorporate strategies to improve digital literacy, provide affordable technologies, and ensure equitable access to virtual services for all GDM patients.37
Patients’ Expenses
The financial costs associated with GDM care services are an important factor that impacts patients’ preferences and adherence. The cost of health care associated with GDM is 25.1% higher than the cost for healthy pregnant women.38 The financial costs of hospital visits and neonatal ICU use are 44% and 49% higher in GDM cases, respectively.38 During the pregnancy and delivery stages, maternity insurance does not always include,39 and often does not cover the full costs.40 For instance, in China, women and their families are responsible for covering a large amount of financial expenses associated with GDM healthcare,41 leading to approximately 60% of the delivery costs being paid by patients even after the introduction of the insurance system.42 It is also suggested that the limited number of experienced HCPs may compel some GDM patients to choose private hospital care, where considerably higher costs are paid, often through out-of-pocket (OOP) payments that add further financial burden.43,44 Another added financial burden is the need to purchase healthy food options, which is an added cost during GDM management.45
Addressing these financial challenges requires accessible and flexible healthcare appointments, along with physician-led lifestyle counselling, to help reduce overall costs by preventing complications and unnecessary hospital visits.38 This emphasizes the need to follow a standardized model in diabetes centres that includes scheduling appointments, activating reminders, structuring communication sheets, and reallocating work responsibilities.46 Recent studies further highlight that redesigning care pathways into integrated maternity units can generate cost savings of nearly 10% while maintaining patient satisfaction and clinical outcomes.47 Early diagnosis and timely treatment of GDM have also been shown to be more cost-effective than delayed intervention, preventing escalation into more resource-intensive care.48 In addition, lifestyle programs—particularly those delivered in group settings or healthcare facilities—significantly reduce the incidence of GDM and related expenses.49 Telehealth-based dietitian counselling and virtual lifestyle coaching offer additional scalable solutions, proving both cost-saving and effective in reducing complications by providing patients with accessible support outside traditional care settings.50,51 Together, these insights underscore that screening models aligned with patient preferences—combining diagnostic accuracy, reduced costs, minimal inconvenience, and supportive counselling—can improve participation, satisfaction, and overall acceptance of GDM screening.
Patients’ Screening
The screening for GDM plays a vital role in identifying asymptomatic pregnant women and preventing adverse outcomes associated with the disease.52 A recent study reported that GDM patients prefer a screening strategy associated with a high diagnostic rate, reduced out-of-pocket expenses, a low number of blood draws, limited screening waiting times, and minimal hospital visits.29 These findings highlight that women value not only the accuracy of screening but also its affordability and convenience, particularly when balancing pregnancy with work and family responsibilities. For instance, qualitative studies have shown that women often perceive repeated blood tests and extended hospital visits as stressful and disruptive, which can reduce willingness to attend screening.33,53 Patients also emphasized the importance of supportive elements during the screening process, such as clear communication of results and counselling aimed at safeguarding the baby’s health. These elements increase women’s willingness to undergo and complete screening. Together, these insights underscore that screening models aligned with patient preferences—combining diagnostic accuracy, reduced costs, minimal inconvenience, and supportive counselling—can improve participation, satisfaction, and continuity of care.
Recent advances highlight the potential of machine learning (ML) models to strengthen GDM screening by moving beyond traditional risk-factor–based approaches. These models integrate multiple maternal characteristics—such as age, BMI, family history, ethnicity, and early pregnancy biomarkers—to predict GDM risk with greater accuracy than conventional clinical criteria.54 For example, a large multicenter study showed that ML-based prediction models achieved higher sensitivity and specificity compared to current screening guidelines, allowing for earlier identification of high-risk women.55 Such tools can help design personalized screening strategies, reducing unnecessary tests for low-risk women while ensuring timely and efficient testing for those at high risk.56 In addition, ML-driven digital platforms can be linked with electronic health records to automate risk alerts and support clinicians in making screening decisions.57 By combining predictive analytics with patient preferences for fewer visits and reduced costs, these solutions have the potential to make GDM screening more accurate, affordable, and patient-centered. Table 1 presents a summary of ML models applied across different aspects of GDM management, outlining their role in screening, diagnosis, glycemic control, postpartum follow-up, and cost evaluation.
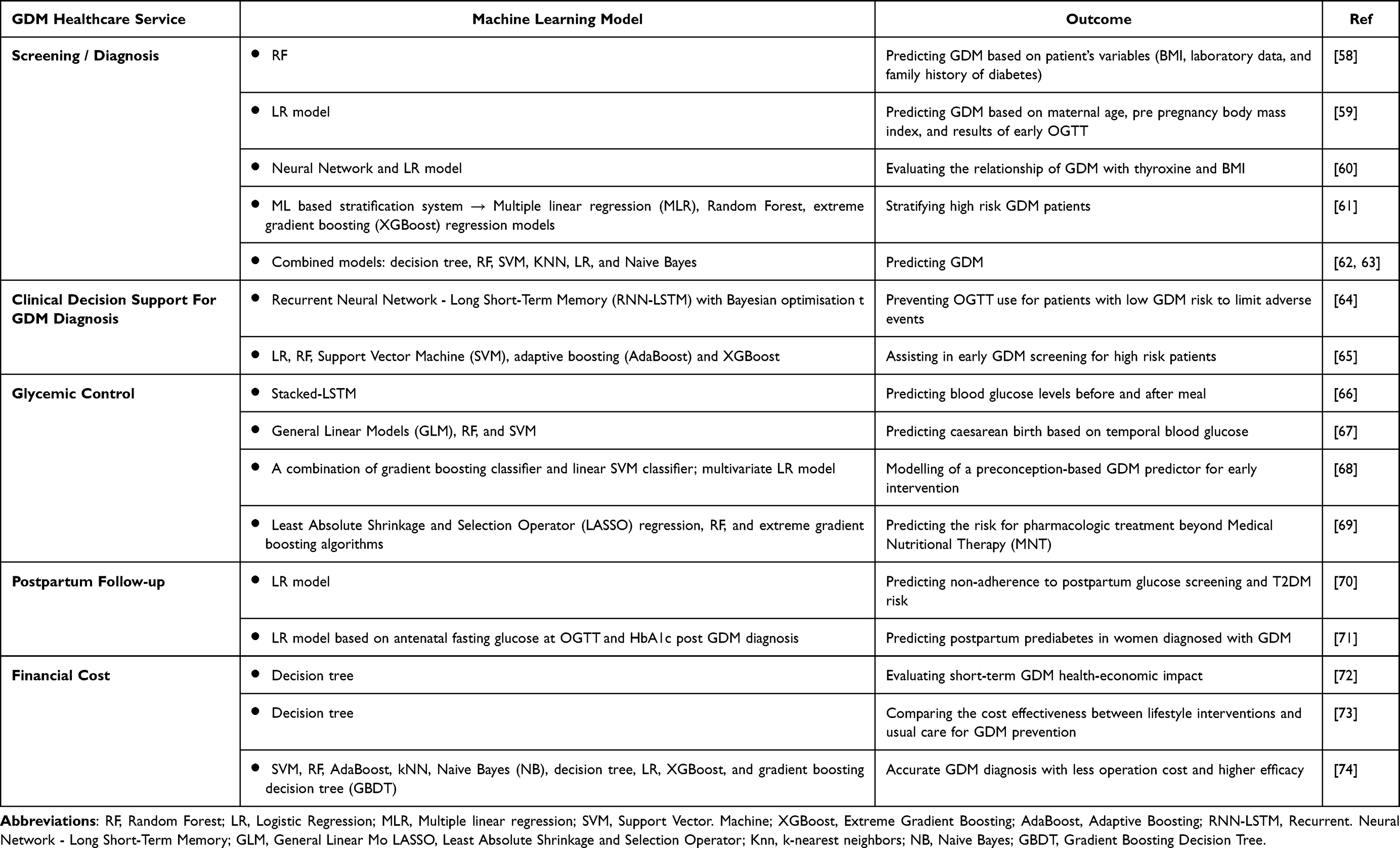 |
Table 1 Application of Machine Learning Models in GDM Care |
Despite these advances, several challenges limit clinical translation of ML-based screening tools. Data quality and completeness vary widely across hospitals and populations, often introducing bias and limiting model reliability.75 Many algorithms are developed on small or single-center datasets, reducing their generalizability to diverse ethnic or socioeconomic groups. Model interpretability also remains a significant barrier, as complex algorithms can act as “black boxes”, making it difficult for clinicians to understand or trust the decision process.76 In addition, real-world adoption is slowed by integration issues with electronic health systems, lack of clinician training, and regulatory uncertainties.77 Addressing these limitations through standardized data collection, transparent model reporting, and validation in multicultural settings is essential for ML to become a trusted component of GDM screening.
In practice, the evidence across time, expenses, and screening dimensions highlights that GDM care remains shaped by structural and socioeconomic barriers that limit accessibility and adherence.78 Long travel distances, high out-of-pocket costs, and time-intensive screening procedures create overlapping challenges that directly influence women’s satisfaction and participation in care.79 While digital health solutions and ML models have introduced promising ways to reduce these burdens, their success depends on ensuring equity, cultural sensitivity, and patient engagement. Future work should focus on integrating these technological and organizational innovations within patient-centered care models that recognize women’s lived realities and preferences, rather than relying solely on efficiency-driven solutions.
Beyond time, cost, and screening factors, substantial heterogeneity exists among GDM patients in terms of socioeconomic status, education, and cultural background. Women with higher education or income levels may engage more readily with self-management and digital tools, while those from disadvantaged or rural settings often face barriers related to health literacy, financial limitations, and access to care.80 Cultural beliefs and language differences further shape women’s perceptions of risk, diet adherence, and communication with healthcare providers.81 These disparities highlight that patient preferences are not uniform but context-dependent, limiting the generalizability of findings across populations. Future studies should stratify analyses by socioeconomic and cultural variables and include more diverse populations to develop inclusive, globally relevant patient-centered care strategies.
Another limitation concerns the geographic distribution of existing evidence. Most available studies on GDM preferences, telehealth adoption, and screening models originate from high-income countries such as Australia, Singapore, the United Kingdom, and the United States.82 In contrast, research from low- and middle-income countries (LMICs) remains scarce, despite differing healthcare infrastructures, insurance coverage, and sociocultural contexts that may strongly influence patient experiences and preferences.83 This imbalance restricts the applicability of current findings to resource-limited settings, where barriers such as transportation costs, healthcare accessibility, and digital connectivity are often more pronounced. Expanding research efforts and data collection in LMICs is therefore essential to capture a more representative and equitable understanding of GDM care preferences worldwide.
Methods Used in Eliciting Patients’ Preferences
Several qualitative and quantitative methods have been adopted to determine patients’ relative desirability or acceptability for these services.84
Qualitative Methods
Qualitative methods are used to collect descriptive data about patients’ observations, their subjective experiences, and decisions made by them.85 Semi-structured interviews are a qualitative method that uses open-ended questions and enables researchers to explore participants’ beliefs about a particular topic, and delve into sensitive health-related issues.86 This method was used to investigate women’s beliefs about GDM during and post pregnancy, and assess their impact on the progression.87 These interviews were also conducted to explore patients’ attitudes toward lifestyle changes and to enable them to provide advice to those newly diagnosed with GDM.11 In the follow-up stage, interviews were conducted to identify the barriers and facilitators of diabetes screening based on HCPs’ experience.88,89 For example, Jane et al evaluated the impact of patients’ experience with GDM management on the degree of participation in the follow-up phase.90 In the high-risk GDM population, women were interviewed to understand their views on the development of advanced technologies such as mobile health applications.91
Another qualitative method used to elicit GDM patients’ preferences is focus groups. In comparison to individual interviews, the process of focus groups can help people better clarify their views.92 Focus groups allow participants to respond in their own words and to choose discussion topics.93 This method also helps in reflecting the experiences of certain social groups, empowering and motivating patients toward behavioral changes.94 In some instances, arranging focus groups may require additional time and effort compared to individual interviews.95 For GDM, focus groups have been organized to evaluate the self-management experiences of newly diagnosed women96 and assess patients’ experience with insulin and anti-diabetic agents.97 The implementation of focus groups helped in determining the concerns, needs, and knowledge of GDM patients.98 In the postpartum stage, focus groups were used to identify the key factors that may improve GDM patients’ participation in the TDM2 prevention program.99
In the low-income population, semi-structured interviews and focus groups were used to evaluate the preferences of women in self-managing GDM.100 These methods were also used to assess the factors that may affect the health behaviors of GDM patients and their preferences for lifestyle support,101 especially in women of culturally and linguistically diverse (CALD) backgrounds.102 In the postpartum stage, the combination of these qualitative methods revealed factors that may affect healthy lifestyle changes and facilitate participation in a lifestyle intervention program.103
Quantitative Methods
Quantitative or stated preference (SP) methods are mainly implemented for collecting quantifiable data that can be assessed through statistical inferences or analysis.104 One of the most commonly employed SP methods for eliciting patients’ preferences is DCE.105 This method is used for quantifying preferences, evaluating alternative options, and understanding preference variations among subgroups.106 DCE has been contributing to the generation of data used for clinical and policy decision-making.107 It has also been implemented to improve treatment adherence, identify patients’ preferences for complex health choices, and develop health programs and technologies that match patients’ demands.108 Overall, this methodology was applied to elicit pregnant women’s views for screening strategies in terms of frequency of blood draws and hospital visits, extra pocket costs, screening waiting time, and positive diagnosis rate.29 DCE has also been implemented to assess the relative importance of healthcare services specific to pregnant women searching for a health facility for delivery.109 Therefore, DCE is a promising tool for investigating understudied patients’ care experiences and preferences110 in multiple illnesses such as GDM.
Mixed Methods
In the context of stated preference methods such as DCE, qualitative approaches are mainly used to identify attributes and levels, and to pilot surveys.111 Focus groups and semi-structured interviews are instrumental in the early stages of DCE development, as they allow researchers to explore women’s lived experiences and perceptions of GDM care.29 These discussions highlight which aspects of care—such as waiting times, number of blood draws, dietary counselling, or costs— are most meaningful to patients, ensuring that attributes reflect real concerns rather than researcher assumptions.112
Once attributes and levels are defined, specialized software is used to construct choice sets that present different combinations of these attributes.113 This allows the DCE to measure quantifiable preferences by observing trade-offs that women are willing to make across attributes.114 For example, qualitative pre-studies in GDM settings have shown that women often highlight the inconvenience of repeated hospital visits, long waiting times, and high out-of-pocket costs during focus groups.29 These insights informed the inclusion of attributes such as the number of clinic visits and the cost of screening in DCE surveys on GDM.25,115,116
Therefore, mixed methods add value not only to survey design but also to the interpretation of results. Qualitative findings explain why women prioritize specific attributes, while the DCE quantifies how much those attributes matter. Hewage et al showed that combining qualitative interviews with DCE helped contextualize women’s preferences for GDM services.33 Follow-up focus groups have also clarified unexpected results; for instance, some women valued convenience—such as fewer hospital visits and shorter waiting times—more highly than clinical accuracy, and qualitative discussions helped explain these choices.29
Overall, integrating qualitative and quantitative methods ensures that GDM preference studies are grounded in patient experience while also producing robust, generalizable estimates. This strengthens the ability of DCEs to inform patient-centered healthcare design for GDM. Table 2 presents a comparative overview of preference elicitation methods (qualitative, quantitative, mixed) used in practice, while Figure 1 summarizes the manuscript framework, showing how mixed methods and ML approaches align with key GDM services to support patient-centered care.
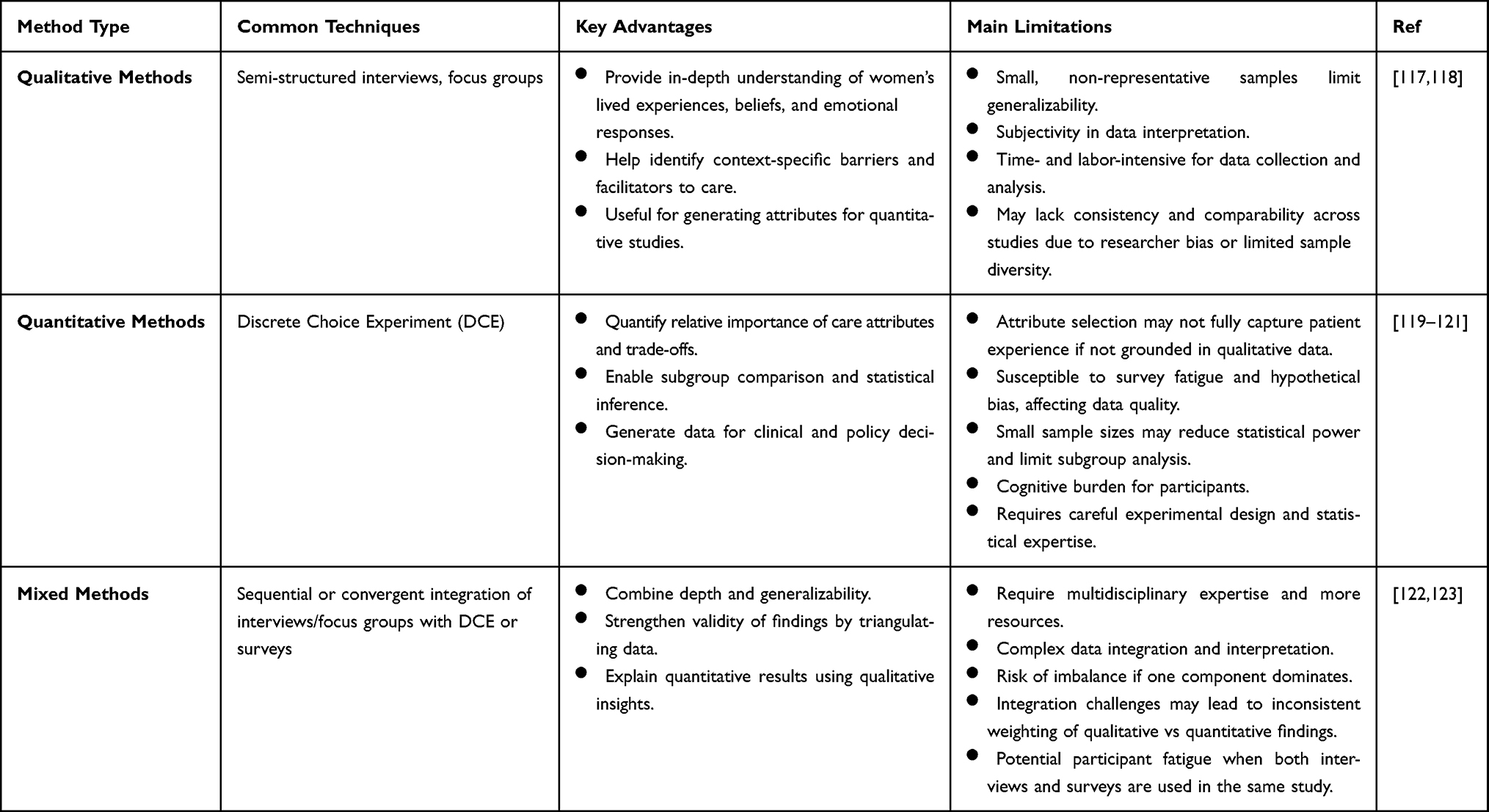 |
Table 2 Comparison of Qualitative, Quantitative, and Mixed Methods for Eliciting Patient Preferences in GDM |
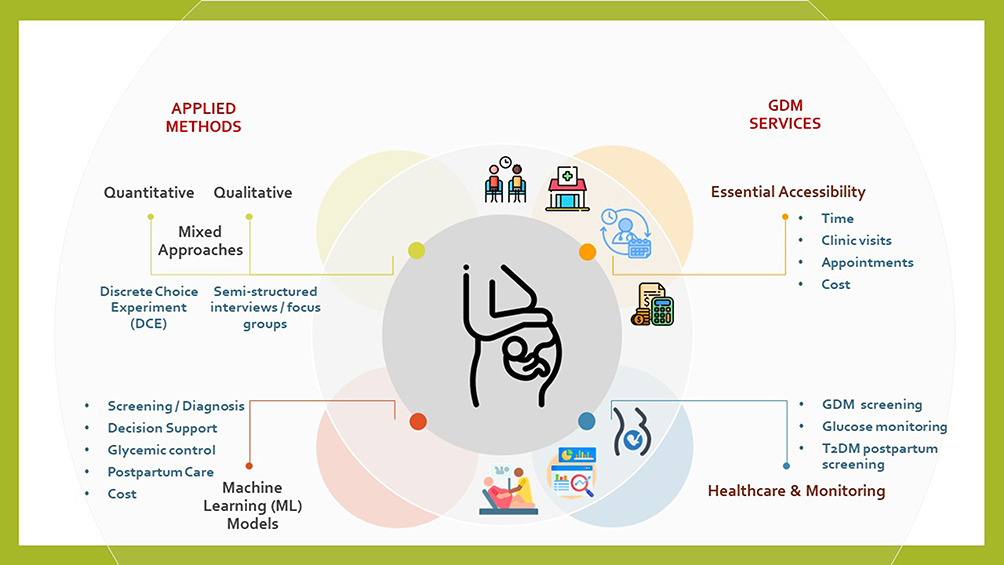 |
Figure 1 Methods for Eliciting Patient Preferences and Enhancing GDM Services in Literature. |
Together, these insights indicate that while mixed methods have improved understanding of patient preferences, they are still rarely integrated into real-world healthcare design or policy. Most studies remain descriptive and limited to specific cultural or clinical settings. Future research should aim to bridge the gap between preference elicitation and implementation by combining patient-centered evidence with technological innovations—such as ML-driven decision support—to develop more inclusive and responsive GDM care models.
Conclusion
GDM care involves complex needs shaped by patients’ time, financial costs, and access to screening. Evidence shows that women prioritize convenient, affordable, and supportive services, with strong preferences for fewer hospital visits, shorter waiting times, and clear counselling. Addressing these needs requires flexible appointments, cost-effective care pathways, lifestyle programs, and digital solutions such as telehealth. Recent advances in ML further enhance screening accuracy and support personalized strategies. Qualitative, quantitative, and mixed methods together provide robust insights into these preferences. Consequently, integrating patient perspectives into service design is essential to ensure GDM care that is effective, affordable, and patient-centered.
Acknowledgments
The authors would like to thank Khalifa University for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors would like to thank Khalifa University for Science and Technology for funding this project (Grant No. 8474000490, Project Reference: ESIG-2023-012). The authors would like to thank Khalifa University for Science and Technology for funding this project (Grant FSU-2023-017).
Disclosure
The authors declare that they have no competing interests.
References
1. Obongo A, Tallarek M, Spallek J. Determinants of access to and use of gestational diabetes mellitus services in Kenya: a multimethod case study protocol. BMJ Open. 2023;13:e074916. doi:10.1136/bmjopen-2023-074916
2. Zhou B, Lu Y, Hajifathalian K, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4·4 million participants. Lancet. 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8
3. Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv Res. 2019;19:13. doi:10.1186/s12913-018-3818-y
4. Daley B, Hitman G, Fenton N, McLachlan S. Assessment of the methodological quality of local clinical practice guidelines on the identification and management of gestational diabetes. BMJ Open. 2019;9:e027285. doi:10.1136/bmjopen-2018-027285
5. Self DR, Hegji CE, Self RM. The link between hospital quality and profitability of outpatient services offered. J Hosp Mark Public Relations. 2009;19:88–100. doi:10.1080/15390940903041500
6. Sievenpiper JL, McDonald SD, Grey V, Don-Wauchope AC. Missed follow-up opportunities using a two-step screening approach for gestational diabetes. Diabetes Res Clin Pract. 2012;96:e43–e46. doi:10.1016/j.diabres.2012.01.030
7. Pham S, Churruca K, Ellis LA, Braithwaite J. A scoping review of gestational diabetes mellitus healthcare: experiences of care reported by pregnant women internationally. BMC Pregnancy Childbirth. 2022;22:627. doi:10.1186/s12884-022-04931-5
8. Butkus R, Rapp K, Cooney TG, Engel LS. Health and Public Policy Committee of the American College of Physicians. Envisioning a better U.S. health care system for all: Reducing barriers to care and addressing social determinants of health. Ann Intern Med. 2020;172:S50–S59. doi:10.7326/M19-2410
9. Busetto L, Wick W, Gumbinger C. How to use and assess qualitative research methods. Neurol Res Pract. 2020;2:14. doi:10.1186/s42466-020-00059-z
10. Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Global Qual Nurs Res. 2017;4:2333393617742282. doi:10.1177/2333393617742282
11. Toxvig L, Hyldgård Nielsen J, Jepsen I. Women’s experiences with managing advice on gestational diabetes - a qualitative interview study. Sex Reproduct Healthcare. 2022;34:100780. doi:10.1016/j.srhc.2022.100780
12. Björk Javanshiri A, Modig S, Nymberg P, Calling S. Women’s experience of gestational diabetes and healthcare in southern Sweden – a qualitative study. BMC Pregnancy Childbirth. 2025;25:224. doi:10.1186/s12884-025-07328-2
13. Yihune Teshale M, Bante A, Gedefaw Belete A, et al. Barriers and facilitators to maternal healthcare in East Africa: a systematic review and qualitative synthesis of perspectives from women, their families, healthcare providers, and key stakeholders. BMC Pregnancy Childbirth. 2025;25(1):111. doi:10.1186/s12884-025-07225-8
14. Rivara AC, Galárraga O, Selu M, et al. Identifying patient preferences for diabetes care: a protocol for implementing a discrete choice experiment in Samoa. PLoS One. 2023;18(12):e0295845. doi:10.1371/journal.pone.0295845
15. Ghaffar Nia N, Kaplanoglu E, Nasab A. Evaluation of artificial intelligence techniques in disease diagnosis and prediction. Discover Artificial Intelligence. 2023;3(5). doi:10.1007/s44163-023-00049-5
16. Alowais SA, Alghamdi SS, Alsuhebany N, et al. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. 2023;23(1):689. doi:10.1186/s12909-023-04698-z
17. Alraddadi KS, Al-Adwani F, Taher ZA, Al-Mansour M, Khan M. Factors influencing patients’ preferences for their treating physician. Saudi Med J. 2020;41:866–873. doi:10.15537/smj.2020.8.25192
18. Grot M, Kugai S, Degen L, et al. Small changes in patient arrival and consultation times have large effects on patients’ waiting times: simulation analyses for primary care. Int J Environ Res Public Health. 2023;20(3):1767. doi:10.3390/ijerph20031767
19. Clifford Bleustein MD, Rothschild DB, Valen A, Valatis E, Schweitzer L, Jones R. Wait times, patient satisfaction scores, and the perception of care. Am J Manag Care. 2014 ;20(5):393–400.
20. Martis R, Brown J, McAra-Couper J, Crowther CA. Enablers and barriers for women with gestational diabetes mellitus to achieve optimal glycaemic control - a qualitative study using the theoretical domains framework. BMC Pregnancy Childbirth. 2018;18:91. doi:10.1186/s12884-018-1710-8
21. Alqudah A, McMullan P, Todd A, et al. Service evaluation of diabetes management during pregnancy in a regional maternity hospital: potential scope for increased self-management and remote patient monitoring through mHealth solutions. BMC Health Serv Res. 2019;19(1):662. doi:10.1186/s12913-019-4471-9
22. Rasekaba T, Nightingale H, Furler J, et al. Women, clinician and IT staff perspectives on telehealth for enhanced gestational diabetes mellitus management in an Australian rural/regional setting. Rural Remote Health. 2021;21:5983. doi:10.22605/RRH5983
23. Hanson E, Ringmets I, Kirss A, Laan M, Rull K. Screening of gestational diabetes and its risk factors: pregnancy outcome of women with gestational diabetes risk factors according to glycose tolerance test results. J Clin Med. 2022;11:4953. doi:10.3390/jcm11174953
24. Carter EB, Tuuli MG, Odibo AO, Macones GA, Cahill AG. Prenatal visit utilization and outcomes in pregnant women with type II and gestational diabetes. J Perinatol. 2016. doi:10.1038/jp.2016.175
25. Agbozo F, Schuler C, Jahn A. Adherence to appointments for gestational diabetes testing and experiences with two-hour postprandial glucose test: a mixed-methods study in Ghana. BMC Pregnancy Childbirth. 2022;22:287. doi:10.1186/s12884-022-04559-5
26. Njete HI, John B, Mlay P, Mahande MJ, Msuya SE. Prevalence, predictors and challenges of gestational diabetes mellitus screening among pregnant women in northern Tanzania. Trop Med Int Health. 2018;23:236–242. doi:10.1111/tmi.13018
27. Pell C, Meñaca A, Were F, et al. Factors affecting antenatal care attendance: results from qualitative studies in Ghana, Kenya and Malawi. PLoS One. 2013;8(1):e53747. doi:10.1371/journal.pone.0053747
28. Okedo-Alex IN, Akamike IC, Ezeanosike OB, Uneke CJ. Determinants of antenatal care utilisation in sub-Saharan Africa: a systematic review. BMJ Open. 2019;9:e031890. doi:10.1136/bmjopen-2019-031890
29. Xu T, Jiang Y, Guo X, et al. Maternal choices and preferences for screening strategies of gestational diabetes mellitus: a exploratory study using discrete choice experiment. Front Public Health. 2022;10:864482. doi:10.3389/fpubh.2022.864482
30. Greenhalgh T, Vijayaraghavan S, Wherton J, et al. Virtual online consultations: advantages and limitations (VOCAL) study. BMJ Open. 2016;6(1):e009388. doi:10.1136/bmjopen-2015-009388
31. Bradwell H, Baines R, Edwards KJ, et al. Exploring patient and staff experiences with video consultations during COVID-19 in an english outpatient care setting: secondary data analysis of routinely collected feedback data. JMIR Form Res. 2022;6(3):e30486. doi:10.2196/30486
32. Clark A, Jung E, Prusky C, Shah BR, Halperin IJ. An evaluation of virtual care for gestational diabetes using the quadruple aim framework: assessment of patient and provider experience, cost, and clinical outcomes. Can J Diab. 2023;47:236–242.e3. doi:10.1016/j.jcjd.2022.12.002
33. Hewage S, Audimulam J, Sullivan E, et al. Barriers to gestational diabetes management and preferred interventions for women with gestational diabetes in singapore: mixed methods study. JMIR Form Res. 2020;4(6):e14486. doi:10.2196/14486
34. Cheshmehzangi A, Zou T, Zhang Y, et al. Commentary: reflecting on the neglected digital divide barriers of telemedicine during COVID-19. Front Public Health. 2022;10:915401. doi:10.3389/fpubh.2022.915401
35. Golob M, Turk N, Mangione CM, et al. Predictors of online vs. in-person preference for lifestyle change programs among women with a history of gestational diabetes mellitus (GDM). Obes Med. 2022;33:100424. doi:10.1016/j.obmed.2022.100424
36. Zhang K, Cheng X, Li D, Meng X. The digital divide of older people in communities: urban-rural, gender, and health disparities and inequities. Health Soc Care Commun. 2025;2025:1361214. doi:10.1155/hsc/1361214
37. Ebekozien O, Fantasia K, Farrokhi F, Sabharwal A, Kerr D. Technology and health inequities in diabetes care: how do we widen access to underserved populations and utilize technology to improve outcomes for all? Diab Obes Metab. 2024;26:3–13. doi:10.1111/dom.15470
38. Kolu P, Raitanen J, Rissanen P, Luoto R. Health care costs associated with gestational diabetes mellitus among high-risk women – results from a randomised trial. BMC Pregnancy Childbirth. 2012;12:71. doi:10.1186/1471-2393-12-71
39. Zhang X, Liu X, Wang Y, Zhou L, Cheng X. Sustainable development of China’s maternity insurance system in the context of population policy changes: using a grounded theory approach. Sustainability. 2022;14:2138. doi:10.3390/su14042138
40. Audibert M, Huang X, Huangfu X, et al. Health insurance reforms and health policies in rural China. China Perspectives. 2016;2016(4):29–38. doi:10.4000/chinaperspectives.7098
41. Xu T, Dainelli L, Yu K, et al. The short-term health and economic burden of gestational diabetes mellitus in China: a modelling study. BMJ Open. 2017;7(12):e018893. doi:10.1136/bmjopen-2017-018893
42. You H, Gu H, Ning W, Zhou H, Dong H. Comparing maternal services utilization and expense reimbursement before and after the adjustment of the new rural cooperative medical scheme policy in Rural China. PLoS One. 2016;11:e0158473. doi:10.1371/journal.pone.0158473
43. Nielsen KK, de Courten M, Kapur A. Health system and societal barriers for gestational diabetes mellitus (GDM) services - lessons from World Diabetes Foundation supported GDM projects. BMC Int Health Hum Rights. 2012;12:33. doi:10.1186/1472-698X-12-33
44. Steigenberger C, Flatscher-Thoeni M, Siebert U, Leiter AM. Determinants of willingness to pay for health services: a systematic review of contingent valuation studies. Eur J Health Econ. 2022;23:1455–1482. doi:10.1007/s10198-022-01437-x
45. Mutabazi JC, Bonong PRE, Trottier H, et al. Integrating gestational diabetes screening and care and type 2 diabetes mellitus prevention after GDM into community based primary health care in south africa-mixed method study. Int J Integr Care. 2022;22:20. doi:10.5334/ijic.5600
46. Middleton P, Crowther CA. Reminder systems for women with previous gestational diabetes mellitus to increase uptake of testing for type 2 diabetes or impaired glucose tolerance. Cochrane Database Syst Rev. 2014;2014:CD009578. doi:10.1002/14651858.CD009578.pub2
47. van den Berg M, Spaan J, van der Kooy J, et al. Value-based evaluation of gestational diabetes mellitus care pathway redesign by using cost and outcome data. BMC Pregnancy Childbirth. 2025;25(1):608. doi:10.1186/s12884-025-07576-2
48. Haque MM, Tannous WK, Herman WH, et al. Cost-effectiveness of diagnosis and treatment of early gestational diabetes mellitus: economic evaluation of the TOBOGM study, an international multicenter randomized controlled trial. EClinicalMedicine. 2024;71:102610. doi:10.1016/j.eclinm.2024.102610
49. Takele WW, Vesco KK, Josefson J, et al. Effective interventions in preventing gestational diabetes mellitus: a systematic review and meta-analysis. Commun Med. 2024;4:75. doi:10.1038/s43856-024-00491-1
50. de Jersey S, Keramat SA, Chang A, et al. A cost-effectiveness evaluation of a dietitian-delivered telephone coaching program during pregnancy for preventing gestational diabetes mellitus. Cost Eff Resour Allocation. 2024;22(1):18. doi:10.1186/s12962-024-00520-9
51. Montori S, Lugli F, Monesi M, et al. Telemedicine in the treatment of gestational diabetes: an observational cohort study on pregnancy outcomes and maternal satisfaction. Diabet Med. 2024;41(2):e15201. doi:10.1111/dme.15201
52. Bulletins-Obstetrics C. ACOG practice bulletin No. 190: gestational diabetes mellitus. Obstetrics Gynecol. 2018;131:e49–e64.
53. Carolan M, Steele C, Margetts H. Knowledge of gestational diabetes among a multi-ethnic cohort in Australia. Midwifery. 2010;26:579–588. doi:10.1016/j.midw.2009.01.006
54. Zhang Z, Yang L, Han W, et al. Machine learning prediction models for gestational diabetes mellitus: meta-analysis. J Med Internet Res. 2022;24(3):e26634. doi:10.2196/26634
55. Zhang J, Cao Q, Mao C, et al. Development and validation of a prediction model for gestational diabetes mellitus risk among women from 8 to 14 weeks of gestation in Western China. BMC Pregnancy Childbirth. 2025;25(1):385. doi:10.1186/s12884-025-07442-1
56. Gallardo-Rincón H, Ríos-Blancas MJ, Ortega-Montiel J, et al. MIDO GDM: an innovative artificial intelligence-based prediction model for the development of gestational diabetes in Mexican women. Sci Rep. 2023;13(1):6992. doi:10.1038/s41598-023-34126-7
57. Germaine M, O’Higgins AC, Egan B, Healy G. Evaluation of machine learning models for early prediction of gestational diabetes using retrospective electronic health records from current and previous pregnancies. medRxiv. 2025;2025:1. doi:10.1101/2025.05.12.25327431
58. Kadambi A, Fulcher I, Schor J, et al. Using machine learning to predict the risk of developing gestational diabetes using a contemporary cohort. Am J Clin Exp Obstet Gynecol. 2023;228(1):S752–S753. doi:10.1016/j.ajog.2022.11.1254
59. Wu S, Li L, Hu K-L, et al. A prediction model of gestational diabetes mellitus based on OGTT in early pregnancy: a prospective cohort study. J Clin Endocrinol Metab. 2023;108(8):1998–2006. doi:10.1210/clinem/dgad052
60. Wu Y-T, Zhang C-J, mol BW, et al. Early prediction of gestational diabetes mellitus in the Chinese population via advanced machine learning. J Clin Endocrinol Metab. 2021;106(3):e1191–e1205. doi:10.1210/clinem/dgaa899
61. Yang J, Clifton D, Hirst JE, et al. Machine learning-based risk stratification for gestational diabetes management. Sensors. 2022;22(13):4805. doi:10.3390/s22134805
62. Jader R, Aminifar S. Predictive model for diagnosis of gestational diabetes in the kurdistan region by a combination of clustering and classification algorithms: an ensemble approach. Appl Comput Intell Soft Comput. 2022;2022:e9749579. doi:10.1155/2022/9749579
63. Ali N, Khan W, Ahmad A, et al. Predictive modeling for the diagnosis of gestational diabetes mellitus using epidemiological data in the United Arab Emirates. Information. 2022;13(10):485. doi:10.3390/info13100485
64. Kurt B, Gürlek B, Keskin S, et al. Prediction of gestational diabetes using deep learning and Bayesian optimization and traditional machine learning techniques. Med Biol Eng Comput. 2023:1–12. doi:10.1007/s11517-023-02800-7
65. Du Y, Rafferty AR, McAuliffe FM, Wei L, Mooney C. An explainable machine learning-based clinical decision support system for prediction of gestational diabetes mellitus. Sci Rep. 2022;12:1170. doi:10.1038/s41598-022-05112-2
66. Lu H, Clifton D, Lu P, Hirst J, MacKillop L. A deep learning approach of blood glucose predictive monitoring for women with gestational diabetes. 2023. doi:10.21203/rs.3.rs-2653408/v1
67. Lu H, Hirst J, Yang J, Mackillop L, Clifton D. Standardising the assessment of caesarean birth using an Oxford caesarean prediction score for mothers with gestational diabetes. Healthcare Technol Lett. 2022;9:1–8. doi:10.1049/htl2.12022
68. Kumar M, Ang LT, Png H, et al. Automated machine learning (AutoML)-derived preconception predictive risk model to guide early intervention for gestational diabetes mellitus. Int J Environ Res Public Health. 2022;19(11):6792. doi:10.3390/ijerph19116792
69. Liao LD, Ferrara A, Greenberg MB, et al. Development and validation of prediction models for gestational diabetes treatment modality using supervised machine learning: a population-based cohort study. BMC Med. 2022;20(1):307. doi:10.1186/s12916-022-02499-7
70. Periyathambi N, Parkhi D, Ghebremichael-Weldeselassie Y, et al. Machine learning prediction of non-attendance to postpartum glucose screening and subsequent risk of type 2 diabetes following gestational diabetes. PLoS One. 2022;17(3):e0264648. doi:10.1371/journal.pone.0264648
71. Parkhi D, Periyathambi N, Ghebremichael-Weldeselassie Y, et al. Prediction of postpartum prediabetes by machine learning methods in women with gestational diabetes mellitus. iScience. 2023;26(10):107846. doi:10.1016/j.isci.2023.107846
72. Lenoir-Wijnkoop I, van der Beek EM, Garssen J, Nuijten MJC, Uauy RD. Health economic modeling to assess short-term costs of maternal overweight, gestational diabetes, and related macrosomia - a pilot evaluation. Front Pharmacol. 2015;6:103. doi:10.3389/fphar.2015.00103
73. Bailey C, Skouteris H, Harrison CL, et al. Cost effectiveness of antenatal lifestyle interventions for preventing gestational diabetes and hypertensive disease in pregnancy. PharmacoEcon Open. 2020;4:499–510. doi:10.1007/s41669-020-00197-9
74. Shen J, Chen J, Zheng Z, et al. An innovative artificial intelligence–based app for the diagnosis of gestational diabetes mellitus (GDM-AI): development study. J Med Internet Res. 2020;22(9):e21573. doi:10.2196/21573
75. Cross JL, Choma MA, Onofrey JA. Bias in medical AI: implications for clinical decision-making. PLOS Digit Health. 2024;3:e0000651. doi:10.1371/journal.pdig.0000651
76. Mohammed S, Malhotra N. Ethical and regulatory challenges in machine learning-based healthcare systems: a review of implementation barriers and future directions. Bench Council Transactions Benchmarks Standards Eval. 2025;5:100215. doi:10.1016/j.tbench.2025.100215
77. Olakotan O, Samuriwo R, Ismaila H, Atiku S. Usability challenges in electronic health records: impact on documentation burden and clinical workflow: a scoping review. J Eval Clin Pract. 2025;31:e70189. doi:10.1111/jep.70189
78. Dubois N, Giroux I. Gestational diabetes mellitus: efficacy of non-pharmacological interventions for management and prevention. Healthcare. 2025;13:2261. doi:10.3390/healthcare13182261
79. Alam CE, Abou-Abbas L, Ramadan MS, Asmar MK. Exploring the barriers to accessing antenatal care at the primary health care center level of a tertiary hospital in Lebanon: a qualitative study. BMC Health Serv Res. 2025;25:304. doi:10.1186/s12913-025-12444-y
80. Terefe B, Workneh BS, Zeleke GA, et al. Uncovering women’s healthcare access challenges in low- and middle-income countries using mixed effects modelling approach: insights for achieving the sustainable development goals. PLoS One. 2025;20(1):e0314309. doi:10.1371/journal.pone.0314309
81. Otaigboria R. Cultural models of illness and health communication strategies improving healthcare access and equity for immigrant patients’ populations. GSC Bio Pharmaceut Sci. 2024;29:390–410. doi:10.30574/gscbps.2024.29.3.0468
82. Rasekaba T, Furler J, Young D, et al. Using technology to support care in gestational diabetes mellitus: quantitative outcomes of an exploratory randomised control trial of adjunct telemedicine for gestational diabetes mellitus (TeleGDM). Diabetes Res Clin Pract. 2018;142:276–285. doi:10.1016/j.diabres.2018.05.049
83. Dawkins B, Renwick C, Ensor T, et al. What factors affect patients’ ability to access healthcare? An overview of systematic reviews. Trop Med Int Health. 2021;26(10):1177–1188. doi:10.1111/tmi.13651
84. van Overbeeke E, Janssens R, Whichello C, et al. Design, conduct, and use of patient preference studies in the medical product life cycle: a multi-method study. Front Pharmacol. 2019;10:1395. doi:10.3389/fphar.2019.01395
85. Renjith V, Yesodharan R, Noronha JA, Ladd E, George A. Qualitative Methods in Health Care Research. Int J Prev Med. 2021;12:20. doi:10.4103/ijpvm.IJPVM_321_19
86. DeJonckheere M, Robinson CH, Evans L, et al. Designing for clinical change: creating an intervention to implement new statin guidelines in a primary care clinic. JMIR Hum Factors. 2018;5:e19. doi:10.2196/humanfactors.9030
87. Hjelm K, Bard K, Apelqvist J. A qualitative study of developing beliefs about health, illness and healthcare in migrant African women with gestational diabetes living in Sweden. BMC Women’s Health. 2018;18(34). doi:10.1186/s12905-018-0518-z
88. Nielsen JH, Fonager K, Kristensen JK, Overgaard C. Follow-up after gestational diabetes: a qualitative study of perspectives from general practices. BJGP Open. 2022;6:
89. Lucas HR, Williams RC, Hollar LN, et al. Understanding gestational diabetes, future diabetes risk, and diabetes prevention: a qualitative study of patient, provider, and staff perspectives. Clin Diab. 2022 ;40(1):39–50.
90. Nielsen JH, Olesen CR, Kristiansen TM, Bak CK, Overgaard C. Reasons for women’s non-participation in follow-up screening after gestational diabetes. Women Birth. 2015;28:e157–e163. doi:10.1016/j.wombi.2015.04.006
91. Duan B, Liu Z, Liu W, Gou B. Assessing the views and needs of people at high risk of gestational diabetes mellitus for the development of mobile health apps: descriptive qualitative study. JMIR Format Res. 2022;6:e36392. doi:10.2196/36392
92. Kitzinger J. Qualitative research Introducing focus groups. BMJ. 1995;311:299–302. doi:10.1136/bmj.311.7000.299
93. Nyumba O, Wilson T, Derrick K, J C, Mukherjee N. The use of focus group discussion methodology: insights from two decades of application in conservation. Meth Ecol Evolut. 2018;9:20–32. doi:10.1111/2041-210X.12860
94. Sawyer AT, McManus K. Understanding patient experiences in a motivational interviewing intervention to improve whole-person lifestyle among individuals with hypertension or type 2 diabetes: a qualitative focus group study. Int J Qual Stud Health Well-Being. 2021;16:1978373. doi:10.1080/17482631.2021.1978373
95. Coenen M, Stamm TA, Stucki G, Cieza A. Individual interviews and focus groups in patients with rheumatoid arthritis: a comparison of two qualitative methods. Qual Life Res. 2012;21:359–370. doi:10.1007/s11136-011-9943-2
96. Su M, Chang M, Sun J. Self‐management experience of first‐time diagnosed gestational diabetes mellitus: a focus group interview. Nurs Open. 2022;10:1744–1754. doi:10.1002/nop2.1431
97. Figueroa Gray M, Hsu C, Kiel L, Dublin S. ‘It’s a Very Big Burden on Me’: women’s experiences using insulin for gestational diabetes. Matern Child Health J. 2017;21:1678–1685. doi:10.1007/s10995-017-2261-8
98. Draffin CR, Alderdice FA, McCance DR, et al. Exploring the needs, concerns and knowledge of women diagnosed with gestational diabetes: a qualitative study. Midwifery. 2016;40:141–147. doi:10.1016/j.midw.2016.06.019
99. Dasgupta K, Da Costa D, Pillay S, et al. Strategies to optimize participation in diabetes prevention programs following gestational diabetes: a focus group study. PLoS One. 2013;8(7):e67878. doi:10.1371/journal.pone.0067878
100. Leziak K, Birch E, Jackson J, et al. Identifying mobile health technology experiences and preferences of low-income pregnant women with diabetes. J Diab Sci Technol. 2021;15(5):1018. doi:10.1177/1932296821993175
101. Parsons J, Sparrow K, Ismail K, et al. A qualitative study exploring women’s health behaviours after a pregnancy with gestational diabetes to inform the development of a diabetes prevention strategy. Diabet Med. 2019;36:203–213. doi:10.1111/dme.13794
102. Oxlad M, Whitburn S, Grieger JA. The complexities of managing gestational diabetes in women of culturally and linguistically diverse backgrounds: a qualitative study of women’s experiences. Nutrients. 2023;15:1053. doi:10.3390/nu15041053
103. Nicklas JM, Zera CA, Seely EW, et al. Identifying postpartum intervention approaches to prevent type 2 diabetes in women with a history of gestational diabetes. BMC Pregnancy Childbirth. 2011;11(23). doi:10.1186/1471-2393-11-23
104. Soekhai V, Whichello C, Levitan B, et al. Methods for exploring and eliciting patient preferences in the medical product lifecycle: a literature review. Drug Discovery Today. 2019;24(7):1324–1331. doi:10.1016/j.drudis.2019.05.001
105. Mühlbacher A, Johnson FR. Choice experiments to quantify preferences for health and healthcare: state of the practice. Appl Health Econ Health Policy. 2016;14:253–266. doi:10.1007/s40258-016-0232-7
106. O’Hara NN. Eliciting health care preferences with discrete choice experiments. JAMA Network Open. 2022;5:e228794. doi:10.1001/jamanetworkopen.2022.8794
107. Merlo G, van Driel M, Hall L. Systematic review and validity assessment of methods used in discrete choice experiments of primary healthcare professionals. Health Econ Rev. 2020;10:39. doi:10.1186/s13561-020-00295-8
108. Leng A, Maitland E, Wang S, et al. Preferences for end-of-life care among patients with terminal cancer in China. JAMA Network Open. 2022;5(4):e228788–e228788. doi:10.1001/jamanetworkopen.2022.8788
109. Mahumud RA, Alamgir NI, Hossain MT, et al. Women’s preferences for maternal healthcare services in bangladesh: evidence from a discrete choice experiment. J Clin Med. 2019;8(2):132. doi:10.3390/jcm8020132
110. Kurniati A, Efendi F, Ismawiningsih I, et al. Retention of doctors and dentists to serve in remote areas in indonesia: a discrete choice experiment. J Multidisciplinary Healthcare. 2024;17:2215. doi:10.2147/JMDH.S459158
111. Louviere JJ, Flynn TN, Carson RT. Discrete choice experiments are not conjoint analysis. J Choice Modelling. 2010;3:57–72. doi:10.1016/S1755-5345(13)70014-9
112. Vass C, Rigby D, Payne K. The role of qualitative research methods in discrete choice experiments. Med Decis Making. 2017;37:298–313. doi:10.1177/0272989X16683934
113. Que S, Huang Y, Awuah-Offei K, Wang L, Liu S. Discrete choice experiment consideration: a framework for mining community consultation with case studies. Sustainability. 2023;15:13070. doi:10.3390/su151713070
114. de Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–172. doi:10.1002/hec.1697
115. Holton S, Rasmussen B, Turner J, et al. Nurse, midwife and patient perspectives and experiences of diabetes management in an acute inpatient setting: a mixed-methods study. BMC Nursing. 2022;21(1):249. doi:10.1186/s12912-022-01022-w
116. Sperling MM, Leonard SA, Miller SE, et al. Fasting compared with fed and oral intake before the 1-hour oral glucose tolerance test: a randomized controlled trial. Obstet Gynecol. 2023;141(1):126–133. doi:10.1097/AOG.0000000000005013
117. Al Balushi K. The use of online semi-structured interviews in interpretive research. Int J Sci Res. 2018;7:726–732. doi:10.21275/ART20181393
118. Lim WM. What is qualitative research? An overview and guidelines. Austr Marketing J. 2025;33:199–229. doi:10.1177/14413582241264619
119. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user’s guide. PharmacoEconomics. 2008;26:661–677. doi:10.2165/00019053-200826080-00004
120. Schoot TS, van Til J, Groothuis-Oudshoorn CGM (Karin), et al. Health outcome preferences and trade-offs among older adults with advanced CKD: a discrete choice experiment. Am J Kidney Dis. 2025;86:624–633.e1. doi:10.1053/j.ajkd.2025.06.010
121. Chen J, Qian X, Su D, et al. An empirical comparison of discrete choice experiment and best-worst scaling to estimate patient preferences in infertility treatment in China. Patient Prefer Adherence. 2025;19:869–882. doi:10.2147/PPA.S501723
122. Ahmed A, Pereira L, Jane K. Mixed Methods Research: Combining Both Qualitative and Quantitative Approaches. 2024.
123. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs—principles and practices. Health Serv Res. 2013;48:2134–2156. doi:10.1111/1475-6773.12117
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Contribution of Scalp Regions to Machine Learning-Based Classification of Dementia Utilizing Resting-State qEEG Signals
Simfukwe C, An SSA, Youn YC
Neuropsychiatric Disease and Treatment 2024, 20:2375-2389
Published Date: 6 December 2024
Advanced Machine Learning did not Surpass Traditional Logistic Regression in First-Trimester Gestational Diabetes Mellitus Prediction: A Retrospective Single-Center Study From Eastern China
Ni H, Miao J, Chen J
International Journal of General Medicine 2025, 18:2263-2274
Published Date: 26 April 2025
Comparison of Interpretable Machine Learning Models Using Systemic Inflammation Index to Predict Preterm Birth in Gestational Diabetes Mellitus
Pang Q, Peng L, Wu J, Wang Y, Zhang R, Liu Z, Jiang L
International Journal of Women's Health 2026, 18:541610
Published Date: 10 February 2026
Multi-Omics Identification of Key Immune Molecules in Gestational Diabetes Mellitus: FKBP5 and HLA-DQA1 as Candidate Biomarkers
Zhang J, Qin Y, Chen N, Wang J
International Journal of General Medicine 2026, 19:601076
Published Date: 12 May 2026