")
Back to Journals » Cancer Management and Research » Volume 13
Pathology Behind Constant Watery Vaginal Discharge: A Rare Case of Uterine Cervical Minimal Deviation Adenocarcinoma
Authors Xie Y , Zhou Q, Chen L, Sui L
Received 23 August 2021
Accepted for publication 3 October 2021
Published 19 October 2021 Volume 2021:13 Pages 7929—7935
DOI https://doi.org/10.2147/CMAR.S334660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Supplementary video of "A rare case of Uterine Cervical MDA" [ID 334660].
Views: 4914
Yu Xie,* Qi Zhou,* Limei Chen, Long Sui
Cervical Diseases Diagnosis and Treatment Center, Obstetrics and Gynecology Hospital of Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Long Sui; Limei Chen Tel +86-021-33189900
Fax +86-021-63450900
Email [email protected]; [email protected]
Abstract: Minimal deviation adenocarcinoma (MDA) of uterine cervix is a rare malignant disease with rather poorer prognosis partially due to the early misdiagnosis. Hence, better understanding of early-stage symptoms is critical. We report a case of a 39-year-old woman came to hospital with a chief complaint of “a watery vaginal discharge for 9 months”. She was further diagnosed as having uterine cervical minimal deviation adenocarcinoma in cervical LEEP specimen and MDA stage IIIC1 (FIGO 2018 staging-after correction) in post-hysterectomy histopathology. Currently, the definitive treatment is hysterectomy with adjuvant therapy based on staging. This article gives concise symptoms, history, and images of MDA colposcopy finding and histopathology, through the whole process of diagnosis and treatment for future clinical reference.
Keywords: LEEP, vaginal discharge, minimal deviation adenocarcinoma, hysterectomy
Minimal deviation adenocarcinoma (MDA) is a rare type of cervical adenocarcinoma. In histopathology slices, it has relatively normal appearing structure and cell differentiation. Patients have atypical clinical symptoms, which are confusing with benign diseases. Early diagnosis is difficult, comparing to its severe aggressiveness, rapid progression, and poor prognosis.1–3
For the diagnosis of MDA, it is necessary to make a comprehensive judgment based on clinical symptoms, gynecological examination, imaging and cytology. It should be noted that the sensitivity of cytological diagnosis of MDA is not satisfactory, which is why cytological examination cannot be solely relied on.3 For patients with suspicious symptoms, colposcopy + pathological biopsy or even diagnostic conization should be considered. In addition, immunohistochemical staining and tumor markers can also be used as important auxiliary examinations.
Here, we report a case of patient with MDA, with the whole disease progression surveillance, diagnosis, treatment and follow-up. Signed consent to publish was obtained from the patient with full disclosure, and all the files were reviewed and exemplified by the Institutional Review Board of Obstetrics and Gynecology Hospital of Fudan University.
Case Report
The patient is a 39-year-old woman without any comorbidities, G1 P1. She came to hospital with a chief complaint of “a watery vaginal discharge for 9 months”. She had regular menstrual periods, with a menstrual cycle of 5–7 days/30 days, moderate menstrual flow and no dysmenorrhea. She had one vaginal delivery in 2005, patient’s father suffered from rectal cancer, and her younger sister suffered from gastric cancer.
In September 2018, first symptom emerged as a large amount of vaginal discharge without any incentives, and the nature of the secretions was clear and odorless. The patient claimed no abdominal pain with twice postcoital bleeding.
In October 2018, cervical and gynecological ultrasound at the local hospital showed no abnormalities, oral medication was prescribed (drug unknown), and the symptoms were not relieved.
The patient was referred to a tertiary center in February 2019, where LCT was rechecked as negative and HPV test was not checked.
In March 2019, the patient came to our hospital. In her gynecological specialist examination and after using the speculum, there was a large amount of clear secretion in the vagina, which was colorless and odorless. The cervix had a hypertrophic appearance and a barrel-like appearance. There was no obvious contact bleeding when wiping the surface of the cervix with a cotton swab. In the bimanual gynecological examination, the cervical hypertrophy can be felt, with clear contour, and the tactile feedback is hard and slightly resilient. The vaginal fornix is soft and has no obvious mass. No masses were touched on both sides of the para-uterine spaces. In the trimanual gynecological examination and digital rectal examination, soft rectal mucosa was touched without abnormal masses. No other abnormality was found during the palpation of the uterus and bilateral adnexal area. The imaging consultation of MRI scan in our hospital has the following findings: 1. Small cystic lesion in the right adnexal area, prone to physiological changes, and recommended to follow-up; 2. cervical nabothian cyst; and 3. few pelvic effusions.
In April 2019, transvaginal ultrasound was performed and has the following findings: uneven texture of the uterus, possible adenomyosis, and small amount of fluid in the uterine cavity.
On May 30, 2019, colposcopy was performed (Figure 1). Persistent large amount of watery discharge from the cervix can be seen under colposcopy, with a hypertrophy cervix. The colposcopy impression suspected cervical glandular epithelial lesions. Multi-point colposcopy directed biopsy (CDB) of the four quadrants of the cervix with endocervical curettage (ECC) histopathology was performed, and the results were as follows: gastric-type differentiated cervical gland lesions, biopsy tissue cannot distinguish between phyllode hyperplasia and minimal deviation adenocarcinoma, imaging examination of cervical lesion recommended for further diagnosis, and immunohistochemical results such as P16 negative, Ki67 sporadic positive, MUC-1 positive, MUC6 positive, and in situ hybridization: HPV high-risk type negative.
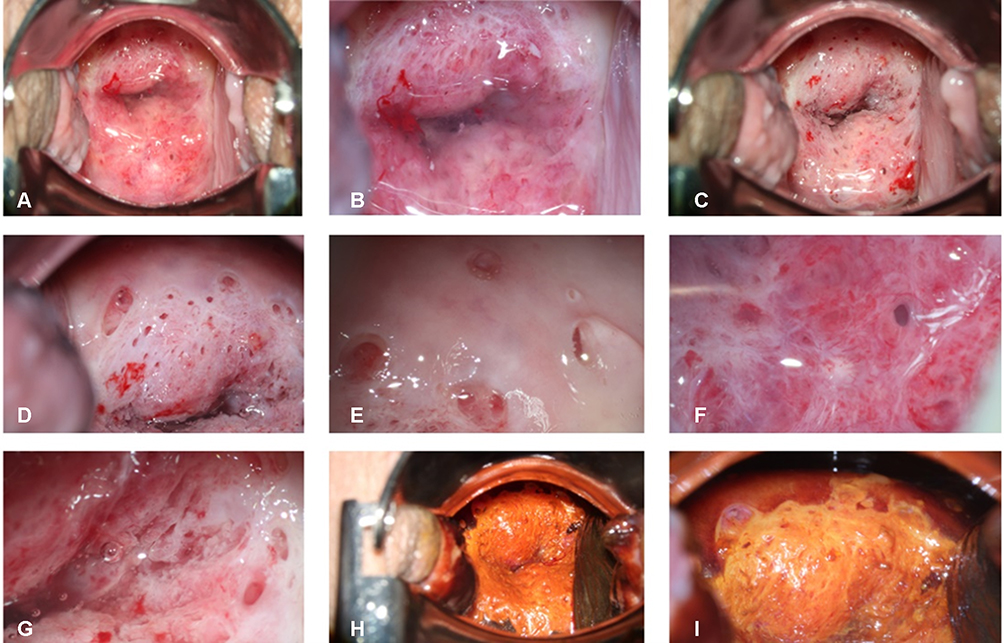 |
Figure 1 Colposcopy image. (A) After placing the speculum, the appearance of the cervix; (B) After magnification of the cervical colposcopy image, clear watery secretions covering the cervix can be seen; (C) The appearance of the cervix after the secretion is wiped off with a cotton swab (D–F). A lot of large gland openings can be observed on the surface of the cervix, and the gland opening is continuously secreting huge amount of watery secretions. (G) Abnormal blood vessels on the surface of the cervix can be observed. (H and I) Colposcopy image of the cervix after using Lugol’s iodine. |
On June 18, 2019, cervical LEEP was performed, and the pathology of conization was as follows: 1. Cervical conization tissue: cervical minimal deviation adenocarcinoma, involving all margins. 2. Cervical canal further resection tissue: cervical minimal deviation adenocarcinoma. 3. ECC: dissociative abnormal glandular epithelium of the cervical canal (Figure 2).
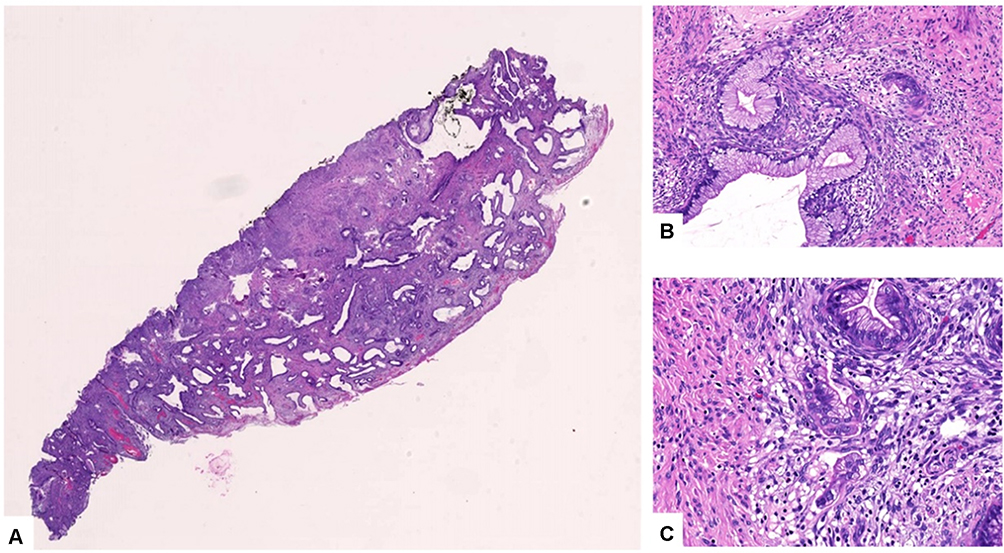 |
Figure 2 Histopathology of LEEP specimen. HE staining of minimal deviation adenocarcinoma and loss of lobular structure with invasive growth. (A) Tumorous glands are diffusely distributed and infiltrate extensively, and cancerous involvement can be seen on the cervical intimal margin (upper border). (B) The glands are well differentiated, similar to the gastric glands. (C) Fibrous reaction and chronic inflammatory cell infiltration can be seen around the gland. |
On June 26, 2019, MRI was performed, the cervix showed a mass shadow, the size was about 3.6cm*3.4cm*4.4cm, T1 showed equally low signal, T2 showed slightly higher signal, DWI and other sequence high signal, and after enhancement, uneven enhancement was established, while no obviously abnormal signal foci were seen near the uterus. There is a slightly larger lymph node shadow next to the right iliac blood vessel and a small amount of free fluid signal in the posterior cavity. The conclusion is cervical cancer, with enlarged lymph nodes next to the right iliac vessels and a small amount of pelvic effusion (Figure 3). Blood tumor markers such as CA125, CA199, CA153, CEA, AFP, HE4, and SCCA were all within the normal range.
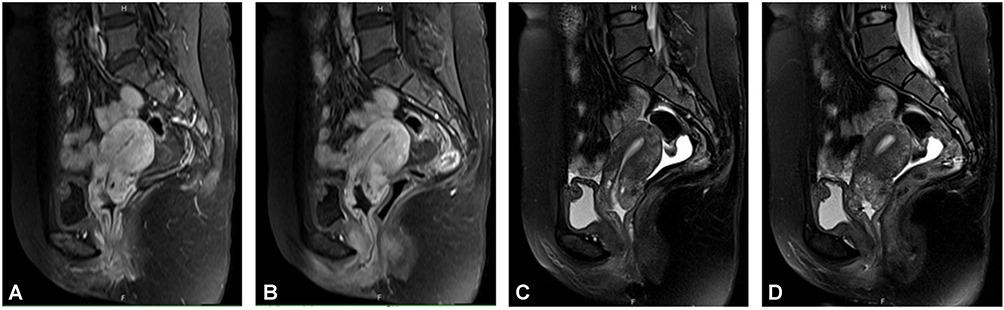 |
Figure 3 MRI image of the patient. The uterus presents posterior flexion, and the size of the uterus is 5.4cm × 6.0cm × 4.5cm. The endometrium is not thickened, without obvious abnormal signal. The cervix has a mass shadow, the size is about 3.6cm × 3.4cm × 4.4cm, T1WI showed iso-low signal (A and B), T2WI showed a little high signal (C and D), DWI showed high signal, uneven enhancement was seen after enhancement, and no obvious abnormal signal foci were seen around the uterus. There were no obvious abnormalities in bilateral ovaries and bilateral appendage areas. The bladder is well filled, the bladder wall is not thickened, and there is no obvious abnormal signal shadow on the bladder wall. There was no obvious abnormal signal shadow in the vagina, urethra and rectum, and there was a slight swollen lymph node shadow beside the right iliac blood vessel. A small amount of free fluid signal in recto-uterine pouch. |
On June 28, 2019, she was admitted to hospital for definitive treatment as follows: 1. 3D laparoscopic extensive total hysterectomy; 2. 3D laparoscopic pelvic lymph node dissection; 3. 3D laparoscopic bilateral salpingo-oophorectomy; 4. laparoscopic vaginal lengthening; and 5. cystoscopic bilateral ureteral stent placement.
The postoperative histopathological diagnosis was cervical minimal deviation adenocarcinoma stage IIIC1 (p) (FIGO 2018 staging-after correction), and the pathological diagnosis was (1) extensive whole uterus: 1. Cervical minimal deviation adenocarcinoma, the size of the lesion was 3.5*3cm, infiltrating the cervical deep fibromuscular layer, with the deepest infiltration 0.1cm away from the lateral wall; cancer thrombus was seen in the vessel; the cancerous focus upwardly invaded the deep muscle layer of the lower segment of the uterus and downwardly invaded the fibrous interstitium of the vaginal wall with a length of 0.5cm. There was no cancer involvement in bilateral para-uterine tissues and the margins of the vaginal wall; 2. Endometriosis is seen on the outer wall of the cervical canal; 3. Mid-secretory period endometrium. (2) (Bilateral) ovarian cystic follicles. (3) (Left side) Endometriosis on the serous surface of the fallopian tube. (Right side) Chronic inflammation of the fallopian tubes. (4) 22 lymph nodes (bilateral pelvic cavity + bilateral total iliac), of which 1/10 (right pelvic cavity) and 3/10 (left pelvic cavity) have cancer metastasis. Immunohistochemistry: AE1/AE3/CD31 (cancer thrombus in the vessel), AE1/AE3/D240 (cancer thrombus in the vessel), P16 (-), P53 (sporadic +), Ki-67 (+, 20%), MUC6 (+). In situ hybridization: HPV high-risk type (-). (Right pelvic cavity) Lymph nodes: AE1/AE3 (+).
On July 10, 2019, Anzatax 270mg + Cisplatin 120mg intravenous chemotherapy was performed. Radiotherapy started in the cancer hospital in mid-July 2019 without concurrent chemotherapy. Radiotherapy ended on August 28, 2019. After the treatment course, chemotherapy was continued 3 times, the last time was at the end of November 2019. The patient was reviewed regularly after the operation. The last follow-up time was April 29, 2021. There were no obvious abnormalities in LCT, HPV, B-ultrasound, pelvic MRI, and tumor markers.
Discussion
Epidemiology
Cervical epithelial tumors have been largely reported due to HPV infection, and over 90% squamous cancer and 40% adenocarcinoma were related to HPV infection.4 Minimal deviation adenocarcinoma of the uterine cervix is highly differentiated cervical mucinous adenocarcinoma. The incidence of MDA of the uterine cervix is rare, comprising 1% to 3% of cervical adenocarcinoma and 0.15% to 0.45% of all cervical cancers.5 The average age of patients at diagnosis is 42–57 years old. Dating back, this was first discovered by German gynecologist Gusserow in 1870. In 1975, Silverberg and Hurt renamed it “minimal deviation adenocarcinoma”, meaning that its cells and structures only have tiny atypia in histopathology. In 2003, the WHO defined it as the “minimal deviation type of cervical mucinous adenocarcinoma”, while in 2014, the WHO reclassified it as a subtype of highly differentiated gastric mucinous adenocarcinoma.6
Pathophysiology
Cervical minimal deviation adenocarcinoma is highly differentiated, its histological characteristics are difficult to distinguish from other benign lesions or even normal glands, clinical symptoms are atypical, and early diagnosis is difficult.7 However, it is highly aggressive and rapidly progressing, with a poor prognosis. Notably, MDA is not related to HPV infection in this case, which is concordant with literature review, implying its tumorigenic origin.1
The precancerous lesion of MDA is lobular endocervical glandular hyperplasia (LEGH), which is seen in women of childbearing age. In LEGH patients, some cases have clinical symptoms of watery vaginal discharge. In LEGH cervical pathological specimens, nodules containing large and small cysts are formed, which are characterized by lobular hyperplasia of the cervical glands, often surrounding large gland ducts, and the cells may have pyloric gland differentiation (Figure 4).
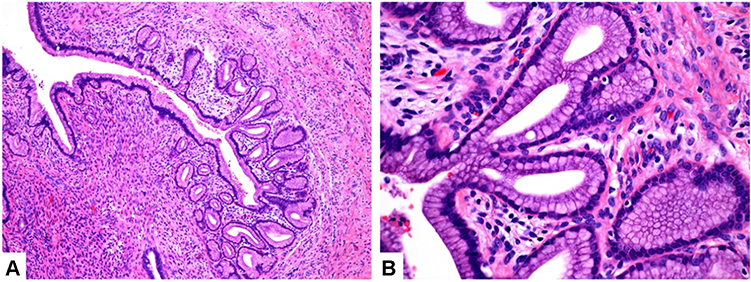 |
Figure 4 Lobular endocervical glandular hyperplasia (LEGH). Lobular endocervical glandular hyperplasia (LEGH) is also called cervical gland phyllodes hyperplasia. The phyllodes hyperplasia is generally located on the upper half of the cervical epithelium, and the glands are well differentiated. At a smaller magnification, the nuclei gather at the base like a necklace. ((A), magnified ten times) Gastric type differentiated glands, no fibrous reaction and inflammatory cell infiltration ((B), magnified forty times). |
LEGH is usually limited to the 1/2 layer of the cervical wall, with a lobular structure under the microscope. The lobules are hyperplastic medium and small glands, with a large gland in the center. The glandular epithelium comprises tall columnar mucinous epithelium, which is well differentiated. The differences between LEGH and MDA focus on the retainment of the lobular structure and whether there is invasive growth.1
MDA occurs in 10% Peutz–Jeghers syndrome (PJS) patients, while STK11 (serine/threonine kinase) gene as the pathogenic gene of PJ syndrome (50–80%).5 Peutz–Jeghers syndrome (PJS), autosomal dominant inheritance, is a type of polyposis of the whole gastrointestinal tract with mucosal and skin pigmentation, with higher risk for cancer, including 70% gastrointestinal cancer, 50% breast cancer, 11% to 36% pancreatic cancer, while cancers of other parts (such as lung, uterus, ovaries, and testes) are also common. The STK11 gene is mapped on chromosome 19p 13.3 as a tumor suppressor gene. According to past research, the STK11 gene triggers cell cycle arrest through p21, which involves apoptosis, metabolism, cell polarity, and proliferation by activating the AMP-activated serine/threonine protein kinase (AMPK) pathway.8 Neyaz et al described the case of a Peutz–Jeghers syndrome associated with a composite synchronous cervical neoplasia comprising precursor LEGH, MDA and gastric-type adenocarcinoma (GTA) along with a serous tubal intraepithelial lesion (STIL) in the right fallopian tube.9
Peng et al reported the case of 33-year-old female patient with Peutz–Jeghers syndrome (PJS) with both cervical micro-deviation adenocarcinoma (MDA) and gastric-type adenocarcinoma (GTA). According to the analysis of immunohistochemical indexes such as MUC6, CK7, p16, ER, PgR, CEA, HIK1083 and CK20 in the two pathological areas, it proved the continuity between gastric adenocarcinoma and MDA, supporting the hypothesis that GTA originated from MDA de-differentiation.10 Besides, Ito et al reported a case of lobular endocervical glandular hyperplasia (LEGH) of the uterine cervix, associated with Peutz–Jeghers syndrome (PJS).11
Hence, gynecologists should also pay attention to high possibility of concurrent ovary lesions, such as mucinous or sex cord tumors and rarely tubal pathology. One more thing to keep in mind is that it is important for gynecologists to screen early and monitor patients with PJS to detect possible cervical adenocarcinomas.
Symptoms and Diagnosis
Common clinical manifestations and signs include cervical hypertrophy with ulcers, exogenous growth manifestations (74.9%), vaginal fluid or mucus discharge (60%), regular bleeding or contact bleeding (50%), pelvic pain or urinary tract obstruction (24.5%), and concordant ovarian tumors (6.7%).3 Another case series of 278 MDA patients carried out in our center in 2010 discovered consistent rates of clinical manifestation, as 69.4% presented with watery or mucoid vaginal discharge, 50% presented with irregular or contact bleeding and 24.5% with other non-specific symptoms (eg, pelvic pain and urinary obstruction).12
Regarding pathology examination, cytology is still controversial, and the detection rate is only 32.7%. The detection rate of single-site biopsy in histopathological examination was 28.17%, while the detection rate of multiple-site biopsy is up to 50.7%. It is recommended that either the biopsy depth should be more than 8 mm or cervical conization being performed. LEEP conization is one of the most widely used conservative treatment with better surveillance and easy to interpret histopathology results for MDA.13
Imaging examinations such as MRI provide detailed information, including the appearance of polycystic cervix, uterine effusion, disorder of gland arrangement and invasion of the deep cervical canal layer.14 Ultrasound evaluates blood flow signals, but the sensitivity needs to be improved.
Blood tumor markers normally stay in normal range, which is consistent with our case. A case was reported of MDA presented with elevated CA19-9 for more than 3 months before diagnosis.15 Various immunohistochemical indicators, such as mucin (MUC) 6, HIK1083, carcinoembryonic antigen (CEA), carbohydrate antigen 199 (CA199), and P53 are often positive in cells, while estrogen receptor (ER), progesterone receptor (PR), P16, MUC2, and CA125 are mostly negative.
Zhang et al reported five cases of tumor marker testing. Immunophenotype p16, estrogen receptor (ER), progesterone receptor (PR) negative (5/5, 100%), p53 mutant expression (5/5, 100%), cytokeratin (CK) 7, carbonic anhydrase IX (CAIX) is positive (5/5, 100%), mucin 6 (MUC6) is mostly positive (4/5, 80%), and CK20 is mostly negative (4/5, 80%). The immunophenotype of five cases of MDA HER2 showed 2 cases were negative, 2 cases were 1+, and 1 case was 2+, but FISH detection of staining 2+ showed no amplification of HER2. Some MDA cases show the expression of HER2 protein, whether it has the value of targeted therapy, and the evidence is lacking needing further research.16
Colposcopy impression could be misinterpreted as glandular lesion (Video 1). Common manifestations of MDA under colposcopy include the following: 1. The lesion located on the surface of the columnar epithelium that is not adjacent to the squamous–columnar junction; 2. Large gland openings; 3. The papillary lesion; 4. The epithelial budding; and 5. Heterotypic blood vessels. One important symptom is the persistent watery discharge of the cervix. However, because the lesions are often located in the cervical canal, with a multifocal and skipped distribution, gynecologist could easily miss diagnosis of this rather low incidence and infrequency disease.
To conclude, the diagnosis should rely on comprehensive judgments based on clinical symptoms, gynecological examination, imaging and cytology. Nevertheless, when confronting a patient with a large amount of vaginal watery discharge, MDA should be considered as a differential diagnosis.
Treatment
At present, because the incidence of MDA is relatively rare, there is currently no standardized treatment. Most of the treatment plans refer to the same stage of cervical adenocarcinoma.
For early-stage patients, it is recommended to perform extensive radical hysterectomy + pelvic lymphadenectomy. According to whether there are high-risk factors, postoperative adjuvant radiotherapy and chemotherapy are considered. It should be noted that for those who wish to preserve fertility, the former NCCN guidelines do not recommend patients with “small cell neuroendocrine carcinoma, gastric-type adenocarcinoma, minimal deviation adenocarcinoma, or malignant adenoma” to preserve fertility. However, the 2021 NCCN guidelines have deleted “Minimal deviation adenocarcinoma or malignant adenoma” as not-suitable for fertility preservation.17 In advanced-stage patients with lymph node and parauterine invasion, concurrent radiotherapy and chemotherapy are applied.
Due to its high degree of differentiation and low sensitivity to radiotherapy and chemotherapy, most gynecologists currently believe that surgical treatment is the best choice. Nevertheless, whether the selection of surgical methods in the MDA treatment plan is suitable for young patients and the therapeutic value of chemotherapy and radiotherapy still need to be further studied.18
Innovation and Deficiency
This article provides the typical symptoms of MDA and high-definition pictures under the colposcopy, so that readers have a more intuitive understanding. With the complete process from first clinical visit until follow-up after definitive treatment of hysterectomy, gynecologists can get a whole picture of the cervical MDA. After a complete literature review, the symptoms and signs, pathophysiology, diagnosis and treatment of MDA are collected.
However, there are still few shortcomings: Because of the patient’s own economic reasons, the patient has not authorized further related genetic testing, and the exploration of the mechanism is lacking due to limited testing method.
It is not clear whether this case of minimal deviation adenocarcinoma is related to PJ syndrome. We also recommended colonoscopy for this patient to rule out the possibility of P-J syndrome because of the frequent concurrent underlying disease.
Nevertheless, this work is the very first report with typical cervical visual image of MDA, which could facilitate gynecologists with abnormal physical examination presentations and theoretical basis for the diagnosis and treatment for this rare cervical adenocarcinoma.
Conclusion
In clinical practice, “vaginal discharge” is one of the most common main complaints of patients at the first visit, and it is very important to clarify the cause. In this case, through colposcopy + pathological biopsy, using the “three-step” principle of cervical disease diagnosis, the cause is finally identified and the diagnosis is confirmed. It is worth mentioning that the diagnosis and treatment model of “multi-disciplinary consultation” is embodied in the diagnosis and treatment process, actively communicating with the pathology department, radiology department, and gynecology department, so that patients can receive accurate and timely treatment. In addition, for patients with abnormal vaginal discharge, the possibility of various situations should be fully considered to avoid misdiagnosis. At present, there are still huge difficulties in the early diagnosis of minimal deviation adenocarcinoma. Only relying on cytology, imaging and other tests, the sensitivity is still not satisfactory. In clinical practice, if a large number of long-term vaginal discharges are found with cervical hypertrophy, even those with negative cytology and HPV tests should be wary of the possibility of minimal deviation adenocarcinoma.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mikami Y. Gastric-type mucinous carcinoma of the cervix and its precursors – historical overview. Histopathology. 2020;76(1):102–111. doi:10.1111/his.13993
2. Stoehr A, Nann D, Staebler A, Oberlechner E, Brucker SY, Bachmann C. Difficulties in diagnosis of a minimal deviation adenocarcinoma of uterine cervix diagnosed postoperatively: brief communication and literature review. Arch Gynecol Obstet. 2019;300(4):1029–1043. doi:10.1007/s00404-019-05286-7
3. Sui M, Pei Y, Li D, et al. Misdiagnosis analysis of cervical minimal deviation adenocarcinoma: a report of three rare cases and literature review. Ann Clin Lab Sci. 2016;46(6):680–690.
4. Olusola P, Banerjee HN, Philley JV, Dasgupta S. Human papilloma virus-associated cervical cancer and health disparities. Cells. 2019;8(6):622. doi:10.3390/cells8060622
5. Kuragaki C, Enomoto T, Ueno Y, et al. Mutations in the STK11 gene characterize minimal deviation adenocarcinoma of the uterine cervix. Lab Invest. 2003;83(1):35–45. doi:10.1097/01.LAB.0000049821.16698.D0
6. Talia KL, McCluggage WG. The developing spectrum of gastric-type cervical glandular lesions. Pathology. 2018;50(2):122–133. doi:10.1016/j.pathol.2017.09.009
7. Kwon SY, Choe MS, Lee HW, Lee HJ, Shin SJ, Cho CH. Minimal deviation adenocarcinoma of the cervix and tumorlets of sex-cord stromal tumor with annular tubules of the ovary in Peutz-Jeghers syndrome. J Gynecol Oncol. 2013;24(1):92–95. doi:10.3802/jgo.2013.24.1.92
8. Hardie DG. The AMP-activated protein kinase pathway – new players upstream and downstream. J Cell Sci. 2004;117(Pt 23):5479–5487. doi:10.1242/jcs.01540
9. Neyaz A, Husain N, Deodhar M, Khurana R, Shukla S, Arora A. Synchronous cervical minimal deviation adenocarcinoma, gastric type adenocarcinoma and lobular endocervical glandular hyperplasia along with STIL in Peutz-Jeghers syndrome: eliciting oncogenesis pathways. Turk Patoloji Derg. 2019;35(3):247–253.
10. Peng W-X, Kure S, Ishino K, et al. P16-positive continuous minimal deviation adenocarcinoma and gastric type adenocarcinoma in a patient with Peutz-Jeghers syndrome. Int J Clin Exp Pathol. 2015;8(5):5877–5882.
11. Ito M, Minamiguchi S, Mikami Y, et al. Peutz-Jeghers syndrome-associated atypical mucinous proliferation of the uterine cervix: a case of minimal deviation adenocarcinoma (‘adenoma malignum’) in situ. Pathol Res Pract. 2012;208(10):623–627. doi:10.1016/j.prp.2012.06.008
12. Li G, Jiang W, Gui S, Xu C. Minimal deviation adenocarcinoma of the uterine cervix. Int J Gynaecol Obstet. 2010;110(2):89–92. doi:10.1016/j.ijgo.2010.03.016
13. Ronnett BM. Endocervical adenocarcinoma: selected diagnostic challenges. Mod Pathol. 2016;29(Suppl 1):S12–S28. doi:10.1038/modpathol.2015.131
14. Zhang J, Zhao XM, Chen Y. [MRI findings of minimal deviation adenocarcinoma of cervix]. Zhonghua Zhong Liu Za Zhi. 2019;41(11):878–880. Chinese.
15. Dong Y, Lv Y, Guo J, Sun L. Minimal deviation adenocarcinoma with elevated CA19-9: a case report. World J Clin Cases. 2021;9(21):5999–6004. doi:10.12998/wjcc.v9.i21.5999
16. Zhang F, Shi M, Zhou CM, et al. [Clinicopathological analysis of 6 cases of minimal deviation adenocarcinoma of cervix with 5 ovarian metastasis]. Zhonghua Bing Li Xue Za Zhi. 2021;50(2):134–136. Chinese.
17. Panel NCC. NCCN clinical practice guidelines for cervical cancer (2021.v1). NCCN; 2020. https://www.nccn.org/professionals/physician_gls/pdf/cervical_blocks.pdf.
18. Lee H, Kim KR, Cho NH, et al. MicroRNA expression profiling and Notch1 and Notch2 expression in minimal deviation adenocarcinoma of uterine cervix. World J Surg Oncol. 2014;12:334. doi:10.1186/1477-7819-12-334
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.