Back to Journals » Cancer Management and Research » Volume 12
Parity as a Prognostic Factor in Patients with Advanced-Stage Epithelial Ovarian Cancer
Authors Khalafi-Nezhad A ![]() , Ebrahimi V, Ahmadpour F, Momtahan M, Robati M, Saraf Z, Ramzi M, Jowkar Z
, Ebrahimi V, Ahmadpour F, Momtahan M, Robati M, Saraf Z, Ramzi M, Jowkar Z ![]() , Ghaffari P
, Ghaffari P
Received 2 November 2019
Accepted for publication 16 February 2020
Published 26 February 2020 Volume 2020:12 Pages 1447—1456
DOI https://doi.org/10.2147/CMAR.S237073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Abolfazl Khalafi-Nezhad,1 Vahid Ebrahimi,2 Fatemeh Ahmadpour,3 Mozhdeh Momtahan,3 Minoo Robati,3 Zahra Saraf,3 Mani Ramzi,1 Zahra Jowkar,4 Parvin Ghaffari5
1Hematology Research Center, Department of Hematology, Medical Oncology and Stem Cell Transplantation, Shiraz University of Medical Sciences, Shiraz, Iran; 2Department of Biostatistics, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran; 3Department of Obstetrics and Gynecology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran; 4Oral and Dental Disease Research Center, Department of Operative Dentistry, School of Dentistry, Shiraz University of Medical Sciences, Shiraz, Iran; 5Department of Obstetrics and Gynecology, School of Medicine, Yasuj University of Medical Sciences, Yasuj, Iran
Correspondence: Abolfazl Khalafi-Nezhad
Department of Hematology, Medical Oncology and Stem Cell Transplantation, Shiraz University of Medical Sciences, Shiraz, Iran
Tel/Fax +98-7136474301
Email [email protected]
Fatemeh Ahmadpour
Department of Obstetrics and Gynecology, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran
Tel/Fax +98-7136474301
Email [email protected]
Aim: This study aimed to determine the prognostic factors influencing the overall survival (OS) of Iranian women with epithelial ovarian cancer (EOC).
Methods: Information about newly diagnosed patients with confirmed EOC at Motahari Clinic, Shiraz, Iran, from January 1, 2001, to December 31, 2016, was retrospectively reviewed and analyzed. Cox-adjusted proportional hazards (PH) and stratified Cox (SC) models were used to determine the potential prognostic factors.
Results: The mean (±SD) age at the diagnosis of 385 patients with EOC was 49.0 (± 13.2) years old. Early-stage EOC (ESEOC) and advanced-stage EOC (ASEOC) were diagnosed in 34.3% and 65.7% of the total patients, respectively. The median (95% CI) OS was 35 (28− 41) months. For ESEOC patients, a stage II-tumor led to a lower OS in the multivariable analysis compared to a lower stage tumor (P= 0.025). For ASEOC patients, age≥ 65 years at diagnosis (P=0.008) led to a lower OS. ASEOC patients with 2– 5 parities (P=0.014) and > 5 parity (P=0.001) demonstrated better OS than nulliparous women.
Conclusion: Patients with ESEOC, higher tumor stage was associated with a shorter OS. The age at diagnosis harmed the OS of patients with ASEOC. More than one parity improved OS in ASEOC patients.
Keywords: advanced-stage epithelial ovarian cancer, early-stage epithelial ovarian cancer, parity, overall survival, stratified Cox-adjusted regression
Introduction
The seventh most common cancer in women worldwide is ovarian cancer (OC).1 The poor overall survival (OS) of patients with ovarian cancer can be attributed to the difficulties in the early detection of tumor, diagnosis, and treatment.2 About 90% of all ovarian cancers are of the epithelial ovarian cancer (EOC) type which is the most lethal gynecologic malignancy in women.1 Histological type, early recognition, cancer stage, patient management, type of hospital, comorbidities, and age might be used to predict the OS of patients with EOC.2–4 Upfront surgery followed by combinationct 3 chemotherapy with a platinum drug and paclitaxel has been considered as the recommended therapy for EOC.5 The treatment for recurrent ovarian cancer should be adjusted based on individualized assessments.6 Although chemotherapy remains the main treatment option for recurrent or advanced EOCs, the chemotherapeutic agents contributing the most to a favorable prognosis are yet unknown.7 Early diagnosis has been considered as one of the most effective determinants of EOC. However, a clear cell carcinoma diagnosed at an advanced stage had the poorest prognosis compared to other histological subtypes of ovarian cancer such as the more common serous carcinoma. Furthermore, the molecular events, pathogeneses, behaviors, and disease prognoses of high- and low-grade serous carcinomas are different.8 Therefore, the individualized treatment of EOC should be possible using histology-specific researches.
In spite of the highest response rate to chemotherapy and remission achievement in the majority of patients with EOC after initial treatment, most of them will also eventually relapse. Therefore, follow-up care including imaging tests, physical exams, and the close monitoring of CA-125 levels is necessary to influence disease outcomes.9 Median OS after recurrence has been reported as approximately two years. Post-recurrence treatment goals are different from those of first-line treatments and include alleviating symptoms, extending OS, and improving the quality of life.10
A previous study showed that the OS of patients with EOC was correlated with the stage and histological type. Therefore, personalized medicine was recommended for the treatment of different histological types of EOC. Also, patients ≥60 years old had poorer overall survival than those <60 years old.11 In contrast, tumor grade, chemotherapeutic regimens/cycles, and stage were found to be independent prognostic factors for early-stage EOC in another study. Moreover, no significant differences were found between histologic types and the 5-year OS.12
To the best of our knowledge, no prior studies have assessed the OS among Iranian women patients with EOC. Therefore, the objective of this study was to evaluate the relationship between OS, stage, and clinicopathologic characteristics of patients with EOC in terms of demographics, survival outcomes, and prognostic factors including histological types.
Materials and Methods
The study protocol was approved by the Ethics Committee for Research of Shiraz University of Medical Sciences (SUMS) (protocol number: 8910-01-01-93). The study protocol was conducted in compliance with the Declaration of Helsinki. All patients had given written informed consent to allow the collection of personal and clinical data retrospectively. The medical records of newly diagnosed patients with confirmed EOC at Motahari Clinic, a tertiary referral center for all women with ovarian cancer in the south of Iran, from January 1, 2001, to December 31, 2016, were retrospectively reviewed. The following cases were excluded from the study: non-analyzable patients, patients with non-epithelial ovarian cancer, with tumors with an unknown or not applicable stage, with ages less than 18 years old, with undefined histological types, with borderline histology tumor, and those without pathology confirmation. Moreover, the patients who did not provide signed informed consent to allow analysis of their clinical data were excluded.
The demographic and clinical data were collected in a database after being extracted from individual medical records. The investigated items included the age at diagnosis, the FIGO (International Federation of Gynecology and Obstetrics) stage, tumor histology, type of chemotherapy, and follow-up data. FIGO classification was used for histological grading and disease staging.13 The date of the first positive cytology or the date of the primary surgery in patients without cytology before primary surgery was defined as the date of diagnosis. The front-line chemotherapy regimen was platinum-paclitaxel for patients who were eligible for chemotherapy. Based on the patients’ tolerance to the side effects of chemotherapy regimens and the physician’s suggestion, 3 to 6 cycles of chemotherapy were administered.
OS was considered as the duration of time from the date of diagnosis until death or the last recorded follow-up (December 31, 2016) for alive patients. Patients who were alive until their last follow-up (December 31, 2016) in the database were regarded as censored. Stage I and II were considered as early-stage epithelial ovarian cancer (ESEOC) and stage III and IV were considered as advanced-stage epithelial ovarian cancer (ASEOC).
Continuous variables were summarized with means (±SD), medians, and 95% confidence interval (95% CI). Overall survival (OS) was calculated from the date of diagnosis to the time of the last follow-up or death from any cause. The OS rate was determined by Kaplan Meier (KM) estimates and compared using the non-parametric Log rank test. The primary outcome was death from EOC.
Univariate and multiple covariate semi-parametric Cox adjusted proportional hazards (PH) regression models were applied to investigate simultaneously the effects of several covariates on the probability of survival.14 Variable selection was based on the clinical importance and the result of the univariate Cox PH model such that variables with P<0.2 were included in the multiple covariate analyses. P-values for testing the PH assumption were reported based on Schoenfeld residuals. After checking PH assumption (using the goodness-of-fit (GOF) approach), the Cox-adjusted results were interpreted using an adjusted hazard ratio (HR) along with the corresponding confidence interval (CI) of 95% as the average hazard of death.
The stratified Cox (SC) adjusted model that allows for control by stratification of a variable that does not satisfy the PH assumption, used to investigate simultaneously the effects of several variables on the probability of survival. Variables that satisfy the PH assumption are included in the multiple SC adjusted model, while the variable being stratified is not included.
All the statistical analyses were done using an R package named “survival” in R software version 3.6.1 (2019-07-05). P-values<0.05 were assumed as statistically significant.
Results
Characteristics of the OC Patients
At first, 600 patients were identified in our study. Only 385 patients met the inclusion criteria for the analysis. Of the 385 EOC patients eligible for the analysis, 243 (63.1%) experienced death. The mean (±SD) age at diagnosis of the cohort was 49.0 (±13.2) years old and married patients represented 340 (88.3%) of the cases. The distribution of disease stage was as follows: stage I: 113 (29.4%), stage II: 19 (4.9%), stage III: 185 (48.1%), and stage IV: 68 (17.6%) patients. Therefore, based on disease stage (early/advanced), 132 (34.3%) and 253 (65.7%) women were with ESEOC and ASEOC, respectively (Log rank test: Chi-squired statistics=101.5, P<0.0001).
The patients were divided into four groups based on histologic subtype: (a) serous carcinoma: 319 (82.9%), (b) mucinous carcinoma: 39 (10.1%), (c) endometrioid carcinoma: 12 (3.1%), and the other types (clear cell, undifferentiated carcinoma, Brenner) of tumor: 15 (3.9%) (Log rank test: Chi-squired statistics=5.08, P=0.1662).
The patients were divided into four groups based on parity: nulliparous: 88 (22.9%), 1 parity 31 (8.1%), 2 to 5 parity: 158 (41.0%), and >5 parity: 108 (28.0%) (Log rank test: Chi-squired statistics=3.2, P=0.3643).
The Global OS of All 385 EOC Patients
The median (95% CI) follow-up time for the surviving EOC patients was 35 (28–41) months. This means that, in general, fifty percent of the EOC patients survived at least 35 months. Using the KM method, the global overall one-, three-, five-, seven-, ten-, and fourteen-year survival rates (95% CI) for the EOC patients were determined to be 79.6% (75.2–83.3%), 49.1% (43.7–54.3%), 34.3% (28.9–39.7%), 24.1% (18.8–29.8%), 18.3% (12.8–24.5%), and 6.1% (1.8–2.9%), respectively (Figure 1A).
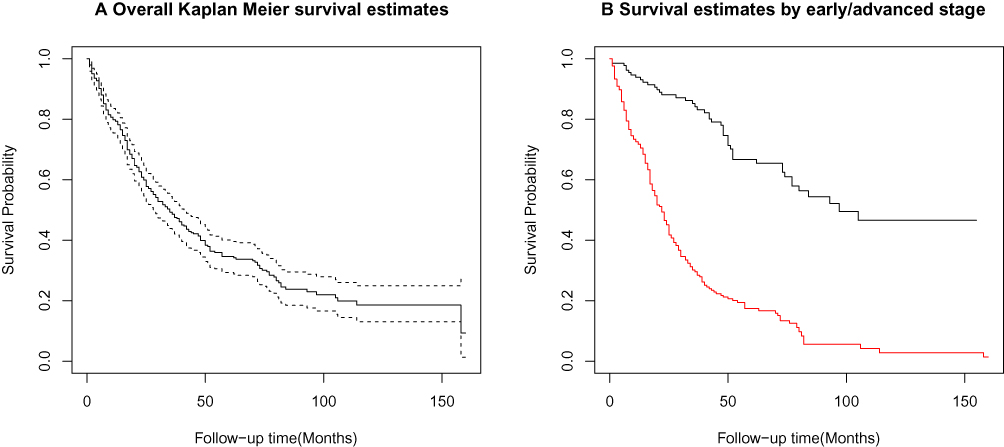 |
Figure 1 (A) Overall Kaplan-Meier (KM) survival estimates for the study population (______) and its corresponding 95% confidence intervals (------) [n=385, number of occurred event= 243, Median (95% CI) survival time equals to 35 (28–41) months]; (B) Overall KM survival estimates of early (black, n=132) and advanced (red, n=253) stages EOC patients (Log rank test for equality of survivor functions: Chi-squired statistics=101.5, P<0.0001), Iran, 2001–2016. |
Univariate semi-parametric Cox PH analyses demonstrated that age at diagnosis, child-bearing (parity), stage, and histology had a significant impact on the OS of patients with EOC (all Ps<0.05) (Table 1).
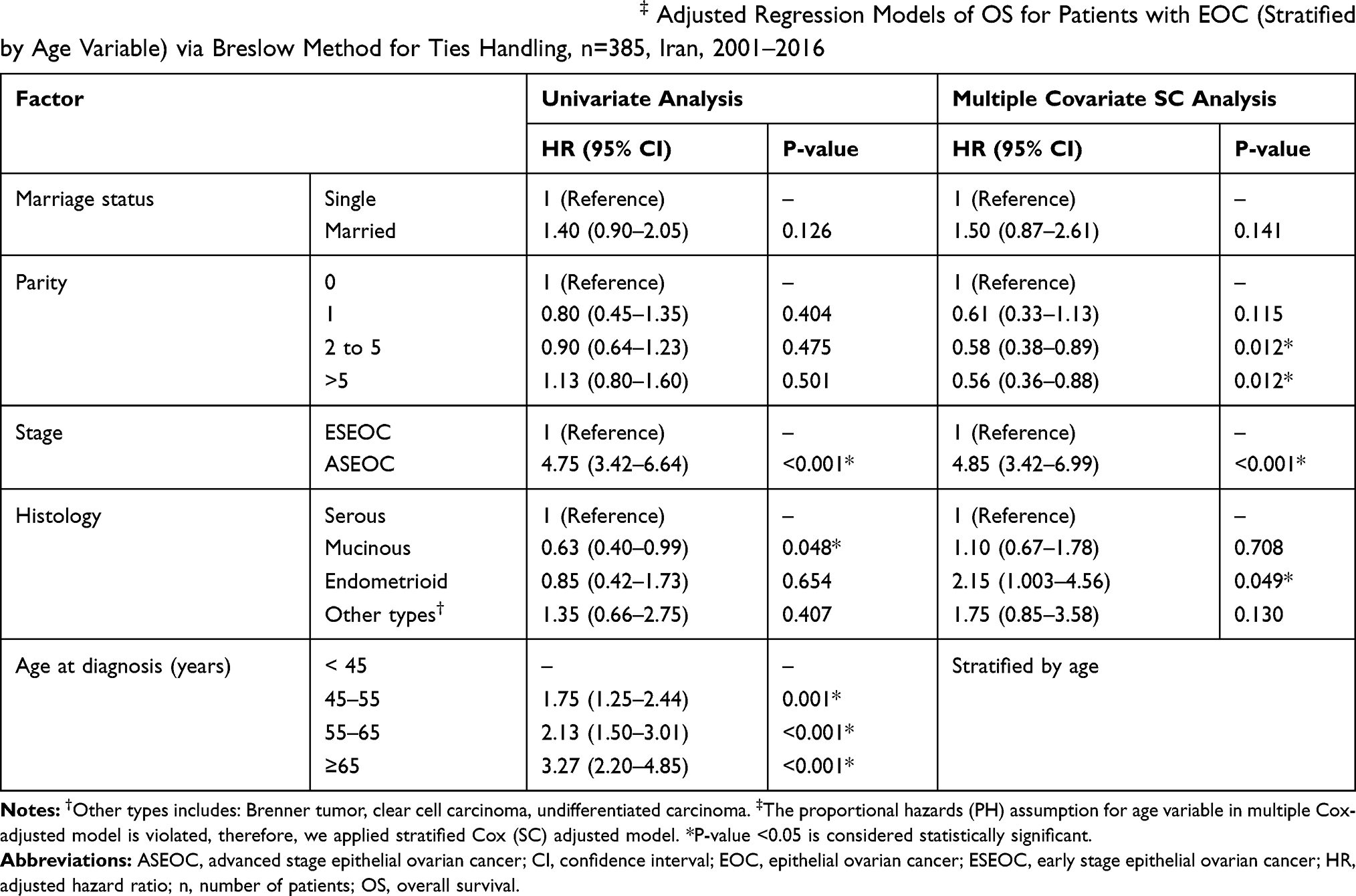 |
Table 1 Univariate and Multiple Covariate Stratified Cox (SC)‡ Adjusted Regression Models of OS for Patients with EOC (Stratified by Age Variable) via Breslow Method for Ties Handling, n=385, Iran, 2001–2016 |
Multiple stratified Cox-adjusted analysis (stratified by age variable) showed that 2 to 5 parity [HR (95% CI) = 0.58 (0.38–0.89), P=0.012], >5 parity [HR (95% CI) = 0.56 (0.36–0.88), P=0.012] led to a better OS compared to nulliparous patients. Moreover, ASEOC: [HR (95% CI) = 4.85 (3.42–6.99), P<0.001], and endometrioid histology [HR (95% CI) = 2.15 (1.003–4.56), P=0.049] were poor prognostic factors in patients with EOC when compared to ESEOC and serous type histology, respectively (Table 1 and Figure 1B).
The Global OS of ESEOC Patients (n=132)
The median follow-up time for surviving ESEOC patients was 97 months. Lower bound for 95% CI is equaled to 77 months and upper bound cannot be determined numerically (Figure 2A). This means that, in general, fifty percent of the ESEOC patients survived at least 97 months.
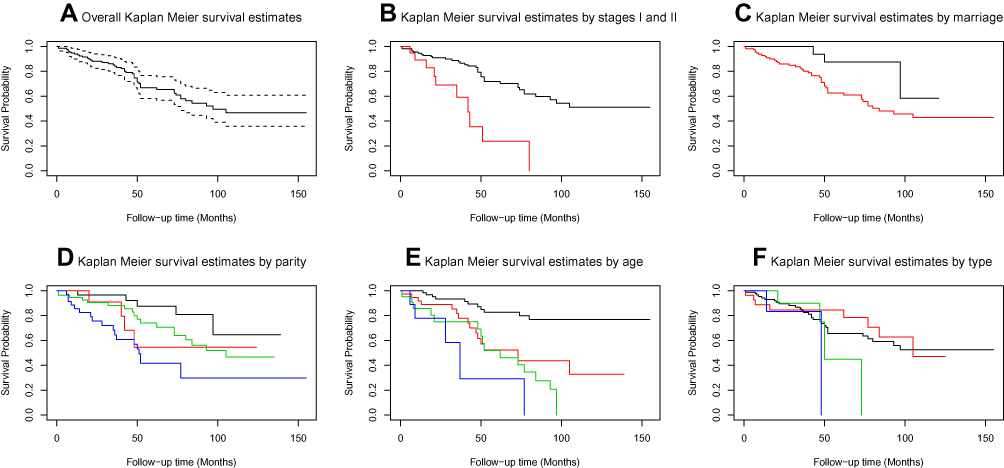 |
Figure 2 Overall non-parametric Kaplan-Meier (KM) survival probabilities of ESEOC patients (n=132, number of occurred event=46): (A) Overall survival (OS) curve of all ESEOC patients [survivor function ________, 95% confidence intervals -------]; (B) Stages I (black), and II patients (red) [Chi-squired statistics=14.9, P=0.0001] (C) Marriage status: married (black), single (red) [Chi-squired statistics= 4.7, P=0.0301]; (D) Parity: 0 delivery (black), 1 delivery (red), 2 to 5 delivery (green), and > 5 delivery (blue) [Chi-squired statistics=13.7, P=0.0034]; (E) Different age groups at diagnosis age < 45 years (black), 45 ≤ age < 55 years (red), 55 ≤ age < 55 years (green), age ≥ 65 (blue) [Chi-squired statistics=30.2, P<0.0001]; (F) Different histological types: serous carcinoma (black), mucinous carcinoma (red), endometrioid carcinoma (green), and other types (includes: Brenner tumor, clear cell carcinoma, undifferentiated carcinoma) (blue) [Chi-squired statistics=6.0, P=0.1099], Iran, 2001–2016. |
Using the nonparametric KM survival estimates, the global overall one-, three-, five-, seven-, and thirteen-year survival rates (95% CI) for the ESEOC patients were determined to be 93.8% (88.0–96.8%), 85.2% (77.4–90.4%), 66.0% (55.6–74.5%), 55.0% (43.5–65.0%), and 45.3% (32.6–57.2%), respectively.
Based on the univariate semi-parametric Cox PH analysis, marriage status, child-bearing (parity), staging, and age at diagnosis had significant effects on the survival time of the ESEOC patients (all Ps<0.05) (Table 2). These findings have been depicted graphically in Figure 2.
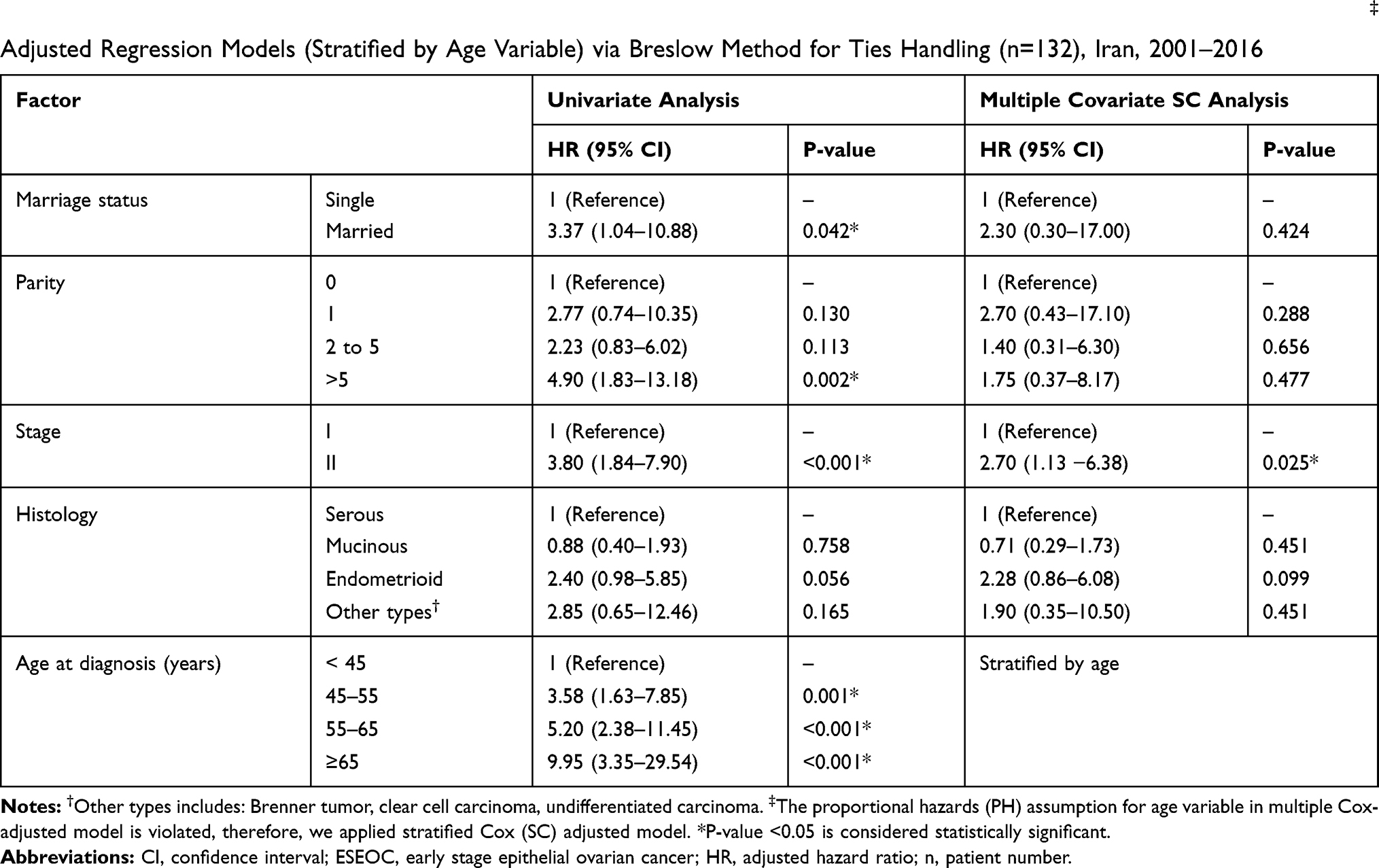 |
Table 2 Overall Survival Prognostic Variables in ESEOC Patients Using Univariate and Multiple Covariate Stratified Cox (SC)‡ Adjusted Regression Models (Stratified by Age Variable) via Breslow Method for Ties Handling (n=132), Iran, 2001–2016 |
After adjusting these significant variables by using multiple stratified Cox regression (stratified by age variable), stage II [HR (95% CI) = 2.70 (1.13 −6.38), P=0.025] was poor prognostic variable when compared with stage I patients (Table 2).
The Global OS of ASEOC Patients (n=253)
Current results demonstrated that the median (95% CI) follow-up survival time for surviving ASEOC patients was 22 (18–25) months. This means that, in general, fifty percent of the ASEOC patients survived at least 22 months. Using the nonparametric KM survival estimates, the global overall one-, three-, five-, seven-, ten-, and fourteen-year survival rates (95% CI) for the ASEOC patients were determined to be 72.2% (66.2–77.4%), 30.1% (24.2–36.3%), 17.5% (12.5–23.2%), 7.1% (3.4–12.6%), 3.6% (0.88–9.6%), and 1.2% (0.04–8.3%), respectively (Figure 3A).
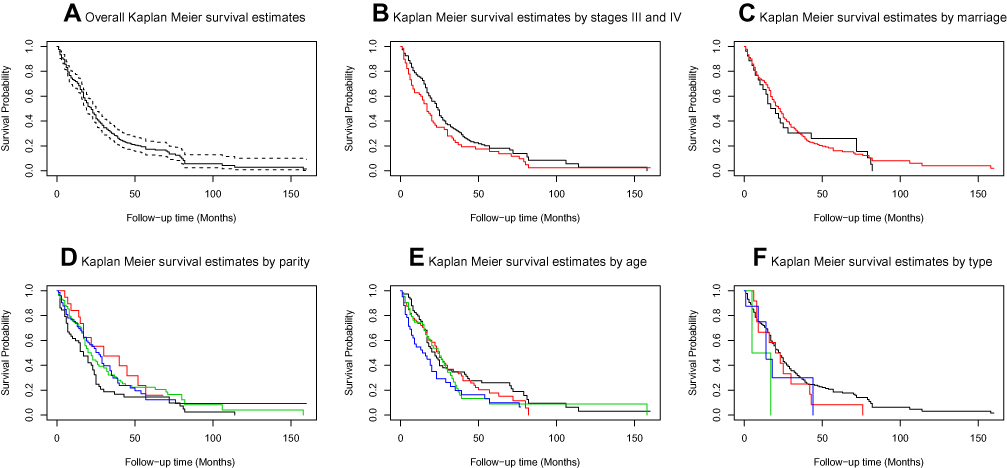 |
Figure 3 Overall non-parametric Kaplan-Meier (KM) survival probabilities of ASEOC patients (n=253, number of occurred event=197): (A) Overall survival (OS) curve of all ASEOC patients [survivor function ________, 95% confidence intervals -------]; (B) Stages III (black), and IV patients (red) [Chi-squired statistics=3.2, P=0.0734] (C) Marriage status: married (black), single (red) [Chi-squired statistics=0.1, P=0.7090]; (D) Parity: 0 delivery (black), 1 delivery (red), 2 to 5 delivery (green), and > 5 delivery (blue) [Chi-squired statistics=6.2, P=0.1038]; (E) Different age groups at diagnosis age < 45 years (black), 45 ≤ age < 55 years (red), 55 ≤ age < 65 years (green), age ≥ 65 (blue) [Chi-squired statistics=6.3, P=0.0976]; (F) Different histological types: serous carcinoma (black), mucinous carcinoma (red), endometrioid carcinoma (green), and other types (includes: Brenner tumor, clear cell carcinoma, undifferentiated carcinoma) (blue) [Chi-squired statistics=4.1, P=0.2508], Iran, 2001–2016. |
The results of the univariate semi-parametric Cox PH model indicated that the hazard of death for ASEOC women with the age at diagnosis of ≥65 years was approximately twice more than that of patients aged <45 years [HR (95% CI) = 1.70 (1.10–2.56), P=0.016]. In addition, ASEOC patients with 2 to 5 parity [HR (95% CI) = 0.70 (0.49–0.99), P=0.045] led to a better OS compared to nulliparous patients (Table 3). These results are better shown graphically in Figure 3.
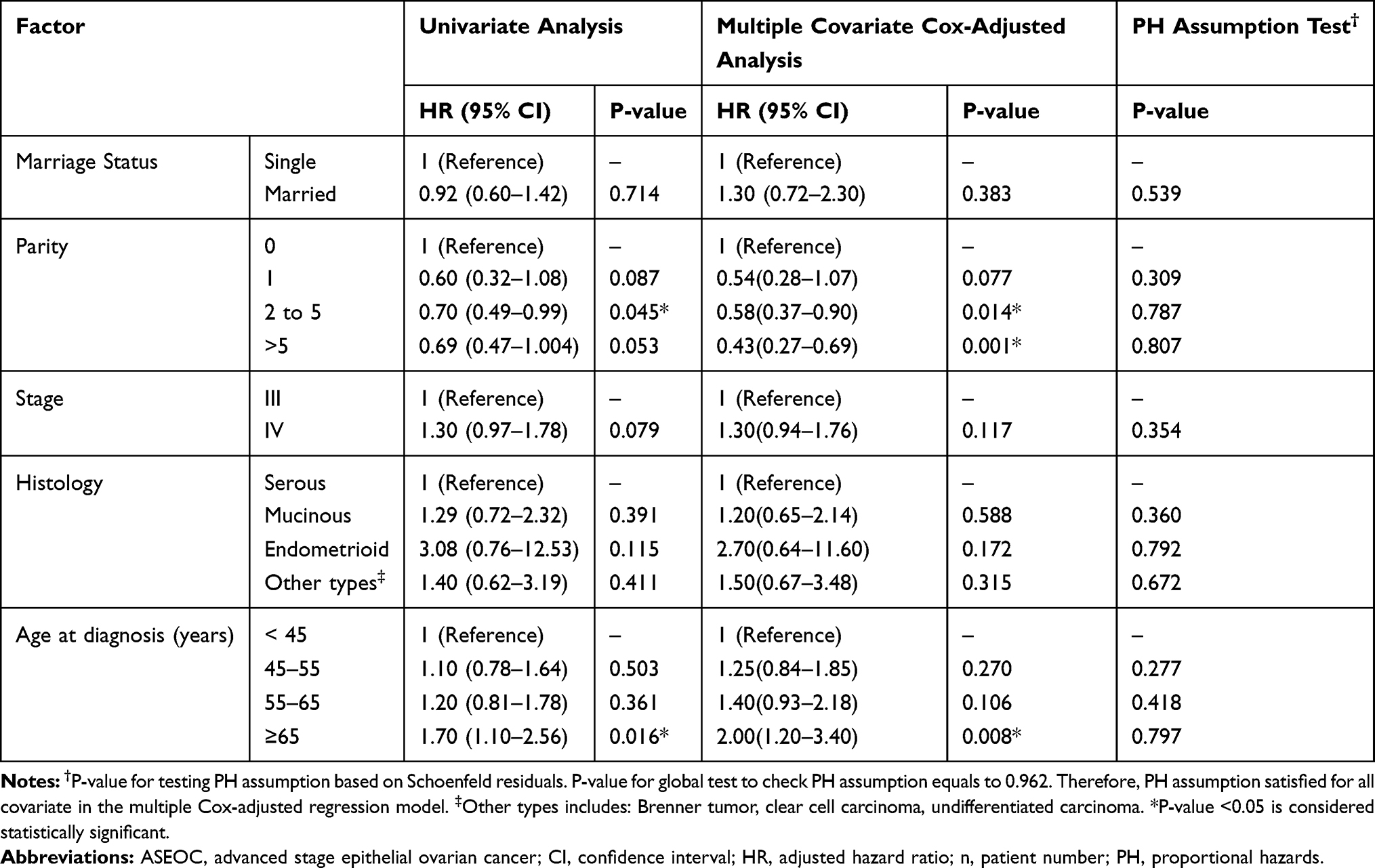 |
Table 3 Overall Survival Prognostic Variables in ASEOC Patients Using Univariate and Multiple Covariate Semi-Parametric Cox-Adjusted PH Regression Models via Breslow Method for Ties (n=253), Iran, 2001–2016 |
Using multiple semi-parametric Cox-adjusted PH regression model, age at diagnosis of equal or more than 65 years old [HR (95% CI) = 2.00 (1.20–3.40), P=0.008] had an adverse effect on OS compared to age at diagnosis of <45 years old. In addition, women with parity of equal to or more than 2 [2–5 parities: HR (95% CI) = 0.58(0.37–0.90), P=0.014; >5 parties: HR (95% CI) = 0.43(0.27–0.69), P=0.001] had better OS than nulliparous women (Table 3).
Discussion
Overall survival (OS) has long been considered as the gold standard primary endpoint in evaluating the efficacy of cancer treatment.7 To the best of our knowledge, this is the first study to investigate the relationship between OS, stage, and clinicopathologic characteristics of Iranian women patients with EOC in terms of demographics, survival outcomes, and prognostic factors. It was found that the stage, histologic type, and parity were the prognostic factors influencing the survival of patients with EOC in the present study. Also, in ASEOC patients, parity had a significant influence on the survival of the patients. In contrast to ESEOC patients, ASEOC patients with 2 to 5 parities and more than five parities had a significantly higher OS than nulliparous or single parity women. This study was the first publication to provide a strong relationship between parity and survival rate in ASEOC patients.
A change in the peak age at diagnosis from approximately 60 years old to 50 years old From 1979 to 2008 was reported in a study by Chiang et al.2 The mean age at diagnosis of the patients with EOC was reported as 52.8 years old in another study.11 However, the mean age at diagnosis in the present study was 49 years old which was lower than those of the previously mentioned studies.2,11 The percentage of ESEOC patients was 34.3% during the study period in the present study. The percentage of ESEOC patients in the current study was lower than a previous study which reported the percentage of early-stage patients as 44.4%.11 Regarding the histologic subtype, the most common histologic subtype of EOC in the present study was serous carcinoma (82.9%) followed by mucinous carcinoma (10.1%). The pattern of histological types varied across the studies. The most common histologic subtype of EOC was mucinous carcinoma in two previous studies.2,11 However, the percentages of patients with serous carcinoma were lower (43.3% and 41.4%, respectively) than that of the current study.2,11 Besides, the percentage of patients with mucinous carcinoma in the present study was less than those of the two previous studies (11.2% and 24.5%, respectively).2,11
Polverino et al demonstrated that histologic type, age, and residual tumor after surgery are the determinants of 5-year OS in EOC patients with complete response after first-line surgery and chemotherapy.15
In line with some previous observations, this study demonstrated that stage I ovarian cancer has a better clinical course than the other stages of ovarian cancer.16,17 The average survival time in stage III and IV was significantly less than that of stage I in the current study. The decrease of OS in EOC patients as the stage advances has been reported by some previous studies.18,19
Regarding the potential prognostic factors, age at diagnosis and parity were found to affect significantly the OS of patients with advanced-stage disease. ASEOC patients with the age of 55–65 and more than 65 years old at diagnosis had a significantly lower OS than the younger patients (<45 years old). Patients with more than 65 years old at diagnosis had twice fewer OS rates than those with less than 45 years old at diagnosis. Therefore, younger groups had better survival rates. Age at diagnosis was an important prognostic factor for patients with EOC in the majority of previous studies2,11,20 which is in line with the findings of the current research. Some possible explanations for the better survival of younger patients than older ones include their better response to paclitaxel/platinum-based chemotherapy, more tolerance to intensive chemotherapeutic regimens, and earlier stage diagnosis.21,22
Also, a significantly increased OS rate was found in ASEOC patients with 2–5 and more than 5 deliveries. ASEOC patients with 2–5 and more than 5 parities had 1.7 and 2.3 times more survival rates, respectively, compared to the nulliparous patients.
Decreased parity accompanied by a westernized lifestyle has been previously shown to contribute to the progressive rise of ovary cancer incidence.23
It has been previously demonstrated that one pregnancy decreases the risk of EOC by as much as one third and each additional pregnancy reduces the OC risk.24 Moreover, a late-age pregnancy (a pregnancy after the age of 35) is more protective than early-age pregnancy (a pregnancy before the age of 25). This observation has been related to the probable protective effect of pregnancy on clearing premalignant or damaged cells from the ovary.25,26 Also, a 2-fold increase in the hazard of EOC has been reported for infertility.27 It has been reported that parity has a long-term, tumor-concurrent effect on inflammation markers at menopause which might be a contributing factor in decreasing the OC risk.28 One explanation for this finding is that child-bearing might reduce immunosuppression (which typically allows tumor spread) and thus counteract aging-associated systemic inflammation.28 A previous study about the combined effects of age and parity on the systemic inflammation markers relevant to OC initiation revealed two mechanisms responsible for this protection. These mechanisms are the decreased stimulation of regulatory B-cells and the partial impairment of the M2 shift in tumor-associated macrophages observed in multiparous aged mice compared with virgin aged mice.28 It has also been demonstrated that the preexisting parity-associated micro-environmental niche in the omental fat band of parous mice might slow the metastatic tumor seeding and outgrowth due to the greater proportion of both T and B lymphocytes.29
The relationship between histological types and survival of EOC patients varied across studies.2,11,17,20 The results of this research also indicated that patients with endometrioid type EOC had a worse OS than serous histological type. Also, the prognosis of the mucinous type was similar to that of the serous type. However, the histological type did not affect OS in ESEOC or ASEOC patients in the current study. Previous researches demonstrated that the histological type was related to the risk of death in ASEOC patients.2 Chang et al showed that patients with clear cell carcinoma had better outcomes than those with serous carcinoma.11 In contrast, clear cell carcinoma showed poorer outcomes compared to the serous carcinoma in ESEOC patients in other studies.17,20 The difference between the findings of this study and those of other studies could be justified by the fact that antineoplastic drug regimens affect the outcomes of different histologic types especially those of clear cell histology.12 In contrast to previous studies, in this study, a few numbers of patients with clear cell carcinoma were included and were considered as having other types of tumors. This may be the reason for the difference between the results obtained in the present study and those of the other studies.10,16,17 Therefore, a direct comparison between the results of this study and those of the other studies was not possible.
In line with previous studies, the tumor stage had a significant effect on the survival of patients with EOC in the present study.17,20
The relatively large sample size and the follow-up period are the factors that make the findings of the present study more reliable. The presence of gynecologic pathologists in most hospitals in Iran could be the reason for the high quality of the histology information in this study despite the inaccessibility of the central review for histology. The front-line chemotherapy regimen was platinum-paclitaxel for patients who were eligible for chemotherapy. Also, the collected demographic information at the time of enrollment might not reflect the status of the patients throughout the treatment and follow-up periods. Retrospective and institutional biases were two other limitations of the present study. Nonetheless, the present study found that parity, stage, and histological type had prognostic roles in the survival of EOC patients.
This study was conducted based on the data collected from the patients in one referral medical center in Shiraz, Iran. Therefore, multi–institutional and prospective studies in the future would be worthwhile. As the amount of residual tumor after cytoreductive surgery is a determinant of 5-year OS in EOC patients,15 it would be valuable to evaluate this important prognostic factor in future studies.
The effect of different chemotherapy regimens on OS was not assessed in the present study. Therefore, a unique chemotherapy regimen (platinum-paclitaxel) was used for patients who were eligible for chemotherapy. The results of the present study should be confirmed in future studies evaluating the effects of different chemotherapy regimens on OS.
Conclusion
Patients with ESEOC, higher tumor stage was associated with a shorter OS. Also, though the age at diagnosis harmed the OS of patients with ASEOC, bearing more than one child improved the OS of these patients.
Acknowledgments
The authors thank the vice-chancellery of Shiraz University of Medical Sciences for supporting this research (Grant #8910-01-01-93). This article was based on a thesis performed by Dr. Fatemeh Ahmadpour. The authors also thank Dr. Arash Moradi for editorial assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E86. doi:10.1002/ijc.29210
2. Chiang Y-C, Chen C-A, Chiang C-J, et al. Trends in incidence and survival outcome of epithelial ovarian cancer: 30-year national population-based registry in Taiwan. J Gynecol Oncol. 2013;24(4):342–351. doi:10.3802/jgo.2013.24.4.342
3. Bristow RE, Chang J, Ziogas A, Campos B, Chavez LR, Anton-Culver H. Impact of national cancer institute comprehensive cancer centers on ovarian cancer treatment and survival. J Am Coll Surg. 2015;220(5):940–950. doi:10.1016/j.jamcollsurg.2015.01.056
4. O’Malley CD, Shema SJ, Cress RD, et al. The implications of age and comorbidity on survival following epithelial ovarian cancer: summary and results from a centers for disease control and prevention study. J Womens Health. 2012;21(9):887–894. doi:10.1089/jwh.2012.3781
5. González-Martín A, Sánchez-Lorenzo L, Bratos R, Márquez R, Chiva L. First-line and maintenance therapy for ovarian cancer: current status and future directions. Drugs. 2014;74(8):879–889. doi:10.1007/s40265-014-0221-9
6. Jordan S, Steer C, DeFazio A, et al. Patterns of chemotherapy treatment for women with invasive epithelial ovarian cancer–a population-based study. Gynecol Oncol. 2013;129(2):310–317. doi:10.1016/j.ygyno.2013.02.007
7. Shimokawa M, Kogawa T, Shimada T, et al. Overall survival and post-progression survival are potent endpoint in Phase III trials of second/third-line chemotherapy for advanced or recurrent epithelial ovarian cancer. J Cancer. 2018;9(5):872. doi:10.7150/jca.17664
8. Schnack TH, Høgdall E, Nedergaard L, Høgdall C. Demographic clinical and prognostic factors of primary ovarian adenocarcinomas of serous and clear cell histology—A comparative study. Int J Gynecol Cancer. 2016;26(1):82–90. doi:10.1097/IGC.0000000000000585
9. Miller RE, Rustin GJ. How to follow-up patients with epithelial ovarian cancer. Curr Opin Oncol. 2010;22(5):498–502. doi:10.1097/CCO.0b013e32833ae8b6
10. Ozols RF. Systemic therapy for ovarian cancer: current status and new treatments. Semin Oncol. 2006;33:3–11. doi:10.1053/j.seminoncol.2006.03.011
11. Chang L-C, Huang C-F, Lai M-S, Shen L-J, Wu F-L-L, Cheng W-F. Prognostic factors in epithelial ovarian cancer: a population-based study. PLoS One. 2018;13(3):e0194993. doi:10.1371/journal.pone.0194993
12. Hsieh S-F, Lau H-Y, Wu -H-H, Hsu H-C, Twu N-F, Cheng W-F. Prognostic factors of early stage epithelial ovarian carcinoma. Int J Environ Res Public Health. 2019;16(4):637. doi:10.3390/ijerph16040637
13. Gadducci A, Cosio S, Zola P, Sostegni B, Fuso L, Sartori E. Prognostic factors and clinical outcome of patients with recurrent early-stage epithelial ovarian cancer: an Italian multicenter retrospective study. Int J Gynecol Cancer. 2013;23(3):461–468. doi:10.1097/IGC.0b013e318286665b
14. Lee M-LT, Whitmore GA. Threshold regression for survival analysis: modeling event times by a stochastic process reaching a boundary. Stat Sci. 2006;21(4):501–513. doi:10.1214/088342306000000330
15. Polverino G, Parazzini F, Stellato G, Scarfone G, Cipriani S, Bolis G. Survival and prognostic factors of women with advanced ovarian cancer and complete response after a carboplatin–paclitaxel chemotherapy. Gynecol Oncol. 2005;99(2):343–347. doi:10.1016/j.ygyno.2005.06.008
16. Kurman RJ, Shih I-M. Pathogenesis of ovarian cancer. Lessons from morphology and molecular biology and their clinical implications. Int J Gynecol Pathol. 2008;27(2):151.
17. Wei W, Li N, Sun Y, Li B, Xu L, Wu L. Clinical outcome and prognostic factors of patients with early-stage epithelial ovarian cancer. Oncotarget. 2017;8(14):23862. doi:10.18632/oncotarget.18066
18. Linasmita V, Pattaraarchachai J, Daengdeelert P. Prognostic factors for survival of epithelial ovarian cancer. Int J Gynaecol Obstet. 2004;85(1):66–69. doi:10.1016/j.ijgo.2003.05.001
19. Tufan Ö, Özalp SS, YALÇIN ÖT. Prognostic factors in epithelial ovarian carcinoma: a reference institution experience. Turk J Obstet Gynecol. 2011;8(1):51–56. doi:10.5505/tjod.2011.05902
20. Chan JK, Teoh D, Hu JM, Shin JY, Osann K, Kapp DS. Do clear cell ovarian carcinomas have poorer prognosis compared to other epithelial cell types? A study of 1411 clear cell ovarian cancers. Gynecol Oncol. 2008;109(3):370–376. doi:10.1016/j.ygyno.2008.02.006
21. Chan J, Urban R, Cheung M, et al. Ovarian cancer in younger vs older women: a population-based analysis. Br J Cancer. 2006;95(10):1314. doi:10.1038/sj.bjc.6603457
22. Kosary CL, editor. FIGO stage, histology, histologic grade, age and race as prognostic factors in determining survival for cancers of the female gynecological system: an analysis of 1973‐87 SEER cases of cancers of the endometrium, cervix, ovary, vulva, and vagina. In: Seminars in Surgical Oncology. Wiley Online Library; 1994.
23. Lin Y-C, Yen -L-L, Chen S-Y, et al. Prevalence of overweight and obesity and its associated factors: findings from National Nutrition and Health Survey in Taiwan, 1993–1996. Prev Med. 2003;37(3):233–241. doi:10.1016/S0091-7435(03)00119-1
24. Whittemore AS, Harris R, Ltnyre J; Group COC. Characteristics relating to ovarian cancer risk: collaborative analysis of 12 US case-control studies: IV. The pathogenesis of epithlial ovarian cancer. Am J Epidemiol. 1992;136(10):1212–1220. doi:10.1093/oxfordjournals.aje.a116429
25. Whiteman DC, Siskind V, Purdie DM, Green AC. Timing of pregnancy and the risk of epithelial ovarian cancer. Cancer Epidemiol Biomarkers Prev. 2003;12(1):42–46.
26. Rostgaard K, Wohlfahrt J, Andersen PK, et al. Does pregnancy induce the shedding of premalignant ovarian cells? Epidemiology. 2003;14(2):168–173. doi:10.1097/01.EDE.0000050701.99792.95
27. Tworoger SS, Fairfield KM, Colditz GA, Rosner BA, Hankinson SE. Association of oral contraceptive use, other contraceptive methods, and infertility with ovarian cancer risk. Am J Epidemiol. 2007;166(8):894–901. doi:10.1093/aje/kwm157
28. Urzua U, Chacon C, Lizama L, et al. Parity history determines a systemic inflammatory response to spread of ovarian cancer in naturally aged mice. Aging Dis. 2017;8(5):546. doi:10.14336/AD.2017.0110
29. Cohen CA, Shea AA, Heffron CL, Schmelz EM, Roberts PC. The parity-associated microenvironmental niche in the omental fat band is refractory to ovarian cancer metastasis. Cancer Prev Res (Phila). 2013;6(11):1182–1193. doi:10.1158/1940-6207.CAPR-13-0227
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.