Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Parental Perception of a Dental Home for Children with Special Needs
Authors Hendaus MA ![]() , Shaltout D, Yasrab D, Al-Noubani A, Hamad SG, Alamri M, Alhammadi AH
, Shaltout D, Yasrab D, Al-Noubani A, Hamad SG, Alamri M, Alhammadi AH ![]()
Received 18 May 2020
Accepted for publication 9 August 2020
Published 21 September 2020 Volume 2020:11 Pages 379—384
DOI https://doi.org/10.2147/PHMT.S263358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Mohamed A Hendaus,1– 3 Deena Shaltout,1,4 Dure Yasrab,4 Aya Al-Noubani,4 Sara G Hamad,4 Mohammed Alamri,2 Ahmed H Alhammadi1– 3
1Department of Pediatrics, Section of Academic General Pediatrics, Sidra Medicine, Doha, Qatar; 2Department of Pediatrics, Hamad Medical Corporation, Doha, Qatar; 3Department of Clinical Pediatrics, Weill-Cornell Medicine, Doha, Qatar; 4Pediatric Residency Program, Hamad Medical Corporation, Doha, Qatar
Correspondence: Deena Shaltout
Department of Pediatrics, Sidra Medicine, Doha 26999, Qatar
Tel +974-4003-6559
Fax +974-4443-9571
Email [email protected]
Background and Objectives: There is a major gap in the literature that addresses parental perception of acquiring a dental home for children with special healthcare needs (CSHCN). The objectives of this study are to assess parental perceptions and challenges in acquiring a dental home for their CSHCN.
Methods: Cross-sectional prospective study using a questionnaire.
Results: A total of 302 questionnaires were completed by caregivers. More than 70% of children had developmental delay, 20% had musculoskeletal disabilities, and the rest had respiratory compromise on non-invasive ventilation, learning disability, and visual and hearing disabilities; 75% of the caregivers do not believe pediatricians are qualified to contribute in oral hygiene. Moreover, 70% of children had not had a routine dentist visit in the 12 months preceding the interview. The reasons given for the lack of such visits included the long time of appointments (25%), difficulty in child’s mobility (17%), the perception that dental care is expensive (9%), and a lack of dentist experience in dealing with children with special needs (5%). When asked what factors would encourage caregivers to choose a dental home for their children, 63% mentioned quick appointments, followed by dentists specialized in children with special needs (51%), child friendly atmosphere (21%), low cost (26.6%), close to home (20%), and others (6%). Interestingly, the majority of parents (75%) believed that the primary pediatrician of the child should initiate the dental home process.
Conclusion: Despite proper resources, children with special healthcare needs lack proper oral healthcare. This could be attributed to the lack of a dental home. A pediatrician’s role is crucial in initiating the process of acquiring a dental home for this special population.
Keywords: dental home, children, special needs, pediatric
Introduction
The Maternal and Child Health Bureau has defined children with special healthcare needs (CSHCN) as those who “have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.”1
Oral health issues in patients with special needs are often linked to mental and physical abilities,2 and put them at high risk for poor dental health. The causes could be attributed to frequent oral infections and periodontal disease, craniofacial birth defects, and enamel abnormalities.3,4 Certain medications, special diets, and hardship in sustaining daily hygiene further disturb dental health and increase the risk of dental caries in CSHCN.5,6 The American Academy of Pediatric Dentistry (AAPD) emphasizes that a dental home should provide comprehensive, easily available, family-centered, considerate, culturally sensitive, and resourceful care for children.7 A dental home is comparable to a primary care clinic where the child receives continuity of medical care.8 The establishment of a dental home may shadow the medical home as an efficient, anticipatory, and cost-effective prototype.9
The overall prevalence of dental caries in the State of Qatar is 73%.10 However, there are no specific figures about the prevalence of dental caries in CSHCN.
Parents are the major decision-makers in the child’s health. Delineating their perception about dental homes can be crucial in the establishment of such a model for preventative and treatment options. There is a major gap in the literature regarding parental perception of acquiring a dental home for children with special needs. The intent of this paper is to tackle the gap in the literature by assessing parental perceptions and acceptability of a dental home for their children with special needs and by identifying factors that influence the underutilization of dental healthcare.
Materials and Methods
Study Design, Ethics, and Setting
A cross-sectional prospective study was conducted at Hamad Medical Corporation, the only tertiary pediatric hospital at the time of the study. It was approved by the Medical Research Center at Hamad Medical Corporation (IRB, #MRC 01–17-102), and conducted in the pediatric department (inpatient and outpatient) between July 1, 2017 and April 2019.
Research Tool
The content of the questionnaire was adopted from published studies,11–13 and was validated by experts at our institution. Translation and back translation of the questionnaire from English to Arabic was executed by the translation services at the research center in Hamad Medical Corporation. Parents were offered questionnaires in both Arabic and English languages. The self-administered questionnaire comprised of 26 items as follow:
- Parent and children demographics (8 questions);
- Knowledge and awareness of dental health (9 questions);
- Specific questions about oral hygiene habits (4 questions);
- Specific questions about dental home (4 questions); and
- Open ended question for parental comments (1 question).
Procedure and Participants
There are no similar studies investigating the specific topics of our questionnaire within the context of parental perception, and thus we could not extrapolate or calculate the needed sample size. We then chose a convenient sample of 300 caregivers. The inclusion criteria comprise of parents of children with special needs and aged 1–14 years visiting the outpatient pediatric clinic and the inpatient department. The conditions included are development delay, learning disability, hearing/visually impaired, musculoskeletal disability, and respiratory compromise. We excluded children not having the above inclusion criteria. Parents were approached during their visits to our pediatric outpatient department and inpatient ward, checked for eligibility, and, if eligible, were invited to participate in the study.
After explaining the aims and objectives of the study, verbal consent was attained and parents were informed of why the data was being collected and how it would be utilized. The IRB of our institution (The Hamad Medical Corporation, Qatar) deemed verbal consent as appropriate. Parents were provided with an information sheet explaining the details of the study. Parents were told that their involvement was voluntary and that their answers were confidential and anonymous. There was no monetary or non-monetary compensation for participating.
Statistical Analysis
Statistical analyses were carried out using statistical package SPSS, version 21.0 (IBM corporation, Armonk, NY), and a two-sided P-value <0.05 was statistically significant. Qualitative and quantitative data values were exhibited as percentages. Descriptive statistics described the demographics and other characteristics of parents and children. Associations between two or more categorical variables were assessed using chi-square test. For small cell frequencies, chi-square test with continuity correction factor or Fisher’s exact test was used. Univariate and multivariate logistic regression analysis was used to assess the associations of various potential predictors and covariates. Missing data were not accounted for in the analysis.
Results
In total, 302 questionnaires were completed by caregivers of children with special needs (response rate=92%). Approximately 50% (n=150) of participating parents were between 30–39 years of age, and 85% (n=259) of them were females. Table 1 summarizes the demographic characteristics of participants. More than 70% (n=217) of children had developmental delay, 20% (n=60) had musculoskeletal disabilities, and the rest had respiratory compromise on non-invasive ventilation, learning disability, and visual and hearing disabilities. Moreover, 92% (n=277) of the children had other co-morbidities.
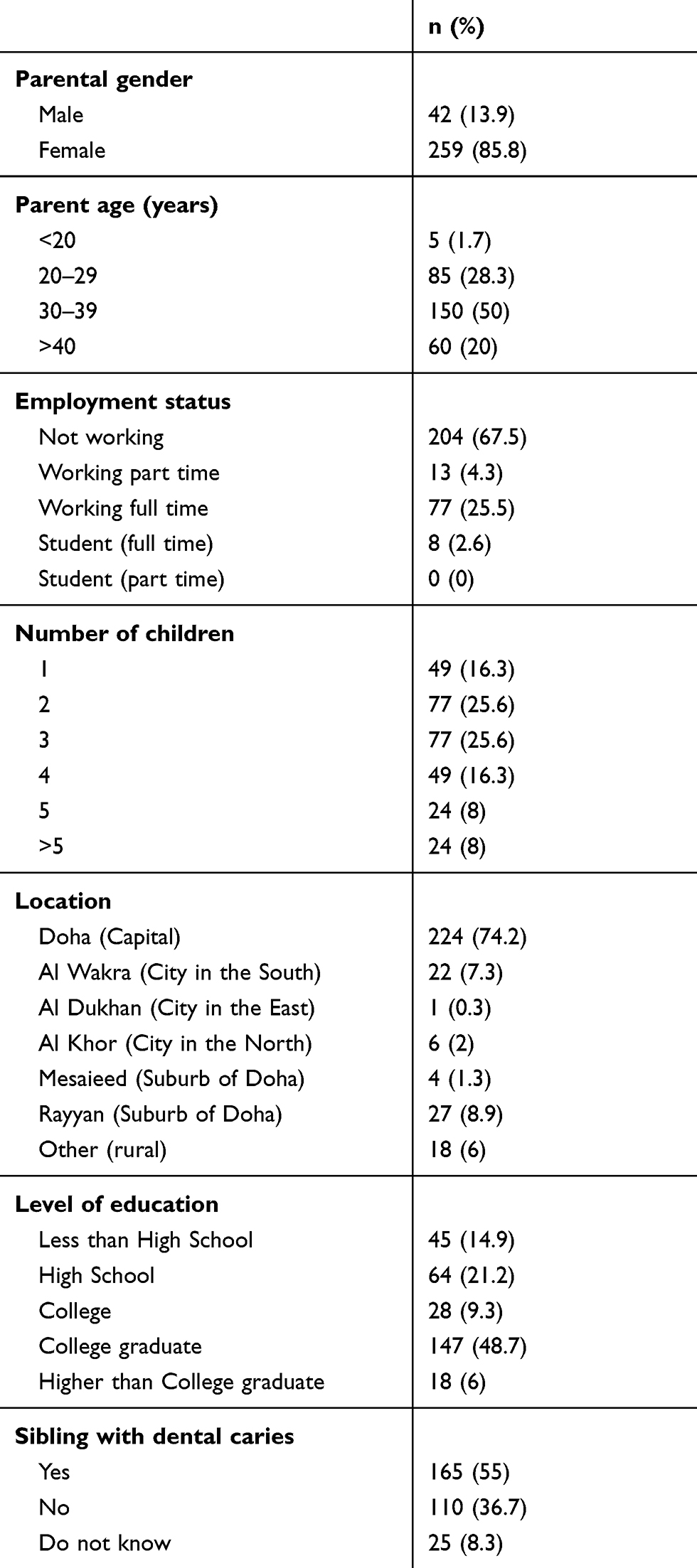 |
Table 1 Demographic Characteristics of Participant |
Upon asking parents about their child’s dental problems, 45% (n=135) stated multiple problems (pain, cavities, halitosis, broken teeth, and teeth discoloration), whereas 10% (n=30) complained only of cavities. When assessing parental awareness of dental health, 80% (n=241) of participants believed that oral health and dentition affects total body wellbeing. Interestingly, 83% (n=252) of these children has no primary dentist, despite all having a primary pediatrician. Almost 50% (n=149) of parents reported their children’s dental problems to their pediatrician, and 72% (n=218) of the caregivers did not believe pediatricians are qualified to contribute in oral hygiene. Table 2 highlights the parents’ knowledge and awareness of dental health.
 |
Table 2 Knowledge and Awareness of Dental Health |
When examining oral hygiene habits performed by participating parents, around 70% (n=210) of them use a toothbrush, toothpaste, and mouthwash. Yet, 8% (n=24) of them did not have routine oral hygiene.
Although one half of the participating parents (n=149) believed that their children needed to get a bi-annual dental checkup, 70% (n=206) of children had not had a routine dentist visit in the 12 months preceding the interview. The motives (Table 3) given for the lack of such visits included the long time of appointments (25%, n=75), difficulty in child’s mobility (17%, n=51), the perception that dental care is expensive (9%, n=27), lack of dentist experience in dealing with children with special needs (5%, n=15), and a combination of the above factors (25%, n=75).
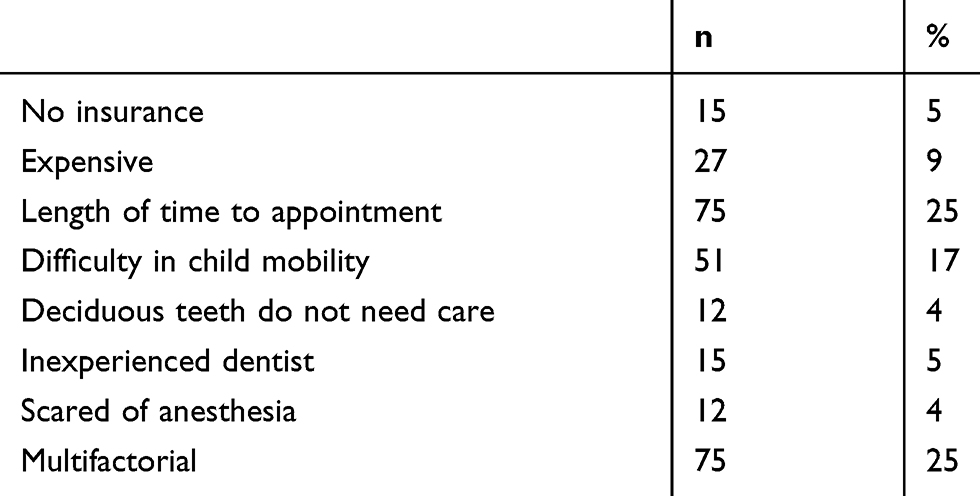 |
Table 3 The Reasons for Not Having Visited a Dentist |
When inquiring of what factors will encourage caregivers to start a dental home for their children, 63% (n=190) mentioned quick appointments, followed by dentists specialized in children with special needs (51%, n=154), a child friendly atmosphere (21%, n= 63), low cost (26.6%, n=80), close to home (20%, n=60), and others (6%, n=18). Interestingly, the majority of parents (75%, n=227) believed that the child’s primary pediatrician should initiate the dental home process.
It is worth mentioning that parental gender (female) and being a caregiver of more than three children was associated with the belief that the primary pediatrician should initiate the dental home process (P=0.047). Furthermore, parental educational level (high school and less) was associated with not having a routine preventative care visit for children in the year preceding the interview (P=0.003). Finally, caregivers who reported fair and poor oral health were more encouraged to initiate a dental home process (P=0.008). The remaining associations among sociodemographic factors, such as level of employment status, place of residence, insurance status, and questions related to the perception of parents toward acquiring a dental home were not statistically significant (P>0.05).
Discussion
The current study is the first study in Qatar and in the Middle East to examine parental perceptions of a dental home for children with special needs. It assessed parental views and concerns about the general and specific aspects of factors involved in acquiring a dental home for this special population.
Caregivers, in addition to nurses and physicians, play a crucial part in the pediatric healthcare system. They are in an exceptional role to report on the care their children obtain and make choices for their beloved ones.14 Their insights and understanding of obstacles to care may differ in significant ways from those perceived by clinicians and policy-makers. Delineating parental perceptions is fundamental to developing programs and interventions to diminish obstacles and is vital to the establishment of patient-centered care.15
Early intervention with preventive steps might be crucial in preventing dental caries in children with special needs. Oral health screening can be set up in routine clinic visits.16 As advised by the American Academy of Pediatrics, the initial dental risk assessment for all children should be completed at the age of 6 months and a dental home should be founded for all children by the age of 12 months given the risk for dental caries.17
A large number of the participants in our study had developmental delay, musculoskeletal disabilities, learning disabilities, visual and hearing disabilities, and the rest had respiratory compromise on non-invasive ventilation. Almost 50% of the parents of such children reported not one but multiple dental problems including cavities, halitosis, broken teeth, and teeth discoloration. That was expected, as CSHCN are at higher risk of acquiring oral health issues as compared to other children.3–6
Despite the fact that most parents believe that sound dental health affects the general wellbeing of the body, most of these children did not have a primary dentist, not even as a part of the complex care team visit.
It is known that poor oral health utterly affects a child’s overall health and quality-of-life. If not well-managed within a timely manner this problem can broaden and lead to a substantial increase in the cost of later dental care.18,19
Since the children included in our target population are not able to take care of themselves it was alarming to know that 8% of the caregivers reported that they performed no oral hygiene routine whatsoever. This reflects a lack of community awareness regarding the importance of dental health and the oblivion towards the ramifications of not acquiring timely hygienic dental care habits and dental care.
Around two thirds of the participating caregivers reported having not even a single dental checkup for their children in the last 12 months and the main reasons given for the lack of visits were reported as long appointment time, followed by difficulty in the child’s mobility, etc. Those barriers can be overcome by integrating a specialized dental home for children with special needs during the routine visit to their pediatrician. Elements reckoned by caregivers that will encourage parents to start a dental home for their children included quick appointments and having access to pediatric dentistry. In our area, the majority of pediatric medicine centers and pediatric dental centers are usually in different locations, and we believe that this could contribute to not achieving utmost communication between a pediatrician and a dental specialist. Working on that communication is one of our goals for better oral health to CSHCN. The State of Qatar is a very well resourced country and these programs are very feasible to be applied. Qatar’s health system was ranked 13th best in the world and topped the list in the Middle East in the 2017 Legatum Prosperity Index.20
This study has substantial strengths, specifically both the quantitative and qualitative comments. Our study will assist in illustrating the need for dental homes and will contribute to creating a better framework of such programs in Qatar and perhaps around the world.
This study also has limitations. We chose a convenience sample. The limitations to external validity are for the most part due to being a very new concept. Moreover, there might be a possibility that there are certain aspects related to parental preference in this subject that were not evaluated in this study. Some of the parents selected to have an interview rather than completing a survey. Although there was no coercion or interference from the research team, we consider collecting data by two different methods a limitation. The sample also included parents of children with medical comorbidities, which could be recognized as more important than oral health. Further investigation with larger multicenter studies is required for more definite conclusions.
We aim to present our data to the Qatar’s health ministry and propose the unique concept of starting a dental home for children with special needs with the results of our study.
Conclusion
Despite proper resources, children with special healthcare needs lack proper oral healthcare. This could be attributed to the lack of a dental home. A pediatrician’s role is crucial in initiating the process of acquiring a dental home for this special population. We will share our results with the ministry of public health with a goal to provide awareness among primary care physicians to consider oral health as an important aspect of the overall well-being and to create an easy referral system to obtain a dental home.
Summary
This study describes parental perspectives and challenges in acquiring a dental home for their children with special needs.
Abbreviation
CSHCN, Children with special health care needs.
Ethical Approval
The Hamad Medical Corporation Ethics Committee approved this study (#MRC 01-17-102)
Acknowledgments
Open Access funding provided by the Qatar National Library.
The authors would like to thank the Medical Research Center of Hamad Medical Corporation for its support and ethical approval. This study was presented in the American Academy of pediatrics National Conference and Exhibition, held in New Orleans, USA on October 26, 2019. An abstract of the presentation has been published in pediatrics.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no financial relationships relevant to this article to disclose.
References
1. McPherson M, Arango P, Fox H, et al. A new definition of children with special health care needs. Pediatrics. 1998;102(1 Pt 1):137–140. doi:10.1542/peds.102.1.137
2. Bayarsaikhan Z, Stephanie Cruz BA, Ј N, Donald L. Transitioning from pediatric care to adult care for adolescents with special health care needs: dentist perspectives (part 2). Pediatr Dent. 2015;37(5):447–451.
3. Foster H, Fitzgerald J. Dental diseases in children with chronic illness. Arch Dis Child. 2005;90:703–708. doi:10.1136/adc.2004.058065
4. Weddell J, Sanders B, Jones J. Dental problems of children with disabilities. In: McDonald RE, Avery DR, Dean JA, editors. Dentistry for the Child and Adolescent. St. Louis, Mo: Mosby; 2004:524.
5. Newacheck P, McManus M, Fox H, et al. Access to health care for children with special health care needs. Pediatrics. 2000;105:760–766. doi:10.1542/peds.105.4.760
6. Lewis C, Robertson A, Phelps S. Unmet dental care needs among children with special health care needs: implications for the medical home. Pediatrics. 2005;116:e426–e431. doi:10.1542/peds.2005-0390
7. The American Academy of Pediatric Dentistry (AAPD). Policy on the dental Home. Reference Manual V 37/NO 6 15/16. Available from: http://www.aapd.org/media/policies_guidelines/p_dentalhome.pdf.
8. McGrath C, Bedi R, Dhawan N. Factor’s influencing older people’s self-reported use of dental services in the UK. Gerodontol. 1999;16:97–102. doi:10.1111/j.1741-2358.1999.00097.x
9. Allareddy V, Nalliah RP, Haque M, Johnson H, Tech SRB, Lee MK. Hospital-based emergency department visits with dental conditions among children in the United States: nationwide epidemiological data. Pediatr Dent. 2014;36(5):393–399.
10. Bener A, Al Darwish MS, Tewfik I, Hoffmann GF. The impact of dietary and lifestyle factors on the risk of dental caries among young children in Qatar. J Egypt Public Health Assoc. 2013;88(2):67–73. doi:10.1097/01.EPX.0000430962.70261.8e
11. Hendaus MA, Jama HA, Siddiqui FJ, Elsiddig SA, Alhammadi AH. Parental preference for fluoride varnish: a new concept in a rapidly developing nation. Patient Prefer Adherence. 2016;10:1227–1233. doi:10.2147/PPA.S109269
12. Kenney MK, Kogan MD, Crall JJ. Parental perceptions of dental/oral health among children with and without special health care needs. Ambul Pediatr. 2008;8(5):312–320. doi:10.1016/j.ambp.2008.04.005
13. Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70(2):179–187. doi:10.1002/j.0022-0337.2006.70.2.tb04074.x
14. Sobo EJ, Kurtin P. Variation in physicians’ definitions of the competent parent and other barriers to guideline adherence: the case of pediatric minor head injury management. Soc Sci Med. 2003;56(12):2479–2491. doi:10.1016/S0277-9536(02)00283-6
15. Sobo EJ, Seid M, Reyes Gelhard L. Parent-identified barriers to pediatric health care: a process-oriented model. Health Serv Res. 2006;41(1):148–172. doi:10.1111/j.1475-6773.2005.00455.x
16. Phelan C. The Blue Book oral health program: a collaborative partnership with statewide implications. Health Promot J Austr. 2006;17(2):109–113. doi:10.1071/HE06109
17. Hale KJ. American academy of pediatrics section on pediatric dentistry oral health risk assessment timing and establishment of the dental home. Pediatrics. 2003;111(5 Pt 1):1113–1116. doi:10.1542/peds.111.5.1113
18. Sheller B, Williams BJ, Lombardi SM. Diagnosis and treatment of dental caries-related emergencies in a children’s hospital. Pediatr Dent. 1997;19(8):470–475.
19. Kanellis MJ, Damiano PC, Momany ET. Medicaid costs associated with the hospitalization of young children for restorative dental treatment under general anesthesia. J Public Health Dent. 2000;60(1):28. doi:10.1111/j.1752-7325.2000.tb03288.x
20. Qatar’s Health System Hukoomi. Available from: http://portal.www.gov.qa/wps/portal/media-center/news/news-details/qatarshealthsystem-rankedthirteenthworldwidefirstinme.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.