Back to Journals » Journal of Inflammation Research » Volume 19
Paradoxical Cutaneous Reaction: Secukinumab–Associated PLEVA in Palmoplantar Pustulosis
Authors Liu W, Chen Y, Lin Z, Zhang J ![]() , Li C
, Li C ![]()
Received 25 December 2025
Accepted for publication 21 January 2026
Published 11 February 2026 Volume 2026:19 590485
DOI https://doi.org/10.2147/JIR.S590485
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Anish R. Maskey
Waner Liu,1,* Yuan Chen,2,* Zhimin Lin,3 Jianglin Zhang,1 Chen Li1
1Department of Dermatology, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology; The Second Clinical Medical College, Jinan University), Shenzhen, 518020, People’s Republic of China; 2School of Traditional Chinese Medicine, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3Capital Medical University Beijing Hospital of Traditional Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chen Li, Department of Dermatology, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology; The Second Clinical Medical College, Jinan University), Shenzhen, 518020, People’s Republic of China, Email [email protected] Jianglin Zhang, Department of Dermatology, Shenzhen People’s Hospital (The First Affiliated Hospital, Southern University of Science and Technology; The Second Clinical Medical College, Jinan University), Shenzhen, 518020, People’s Republic of China, Email [email protected]
Abstract: Palmoplantar pustulosis (PPP) is a chronic inflammatory dermatosis often treated with IL-17 inhibitors like secukinumab. Paradoxical cutaneous reactions to such biologics, though rare, are increasingly recognized. We report a case of a 25-year-old woman with PPP who developed a biopsy-confirmed acute pityriasis lichenoides et varioliformis acuta (PLEVA) eruption following six weeks of secukinumab therapy. Upon switching treatment to tofacitinib, both the PPP and the paradoxical PLEVA showed significant improvement. This case highlights PLEVA as a potential paradoxical reaction to IL-17 inhibition and suggests JAK inhibitors may be an effective alternative in this scenario.
Keywords: IL-17, secukinumab, palmoplantar pustulosis, paradoxical reaction, JAK inhibitors, case report
Introduction
Palmoplantar pustulosis (PPP) is a chronic, inflammatory dermatosis primarily affecting the palms and soles, characterized by recurrent sterile pustules that often cause significant pain and impair quality of life.1 Although the pathogenesis of PPP has not been fully elucidated, it shares several immunopathological features with psoriasis, including upregulation of interleukin-17 (IL-17) in lesional skin, leading some to consider it as a localized variant of pustular psoriasis.2 Based on these shared immune pathways, monoclonal antibodies targeting IL-17A, such as secukinumab, have been used off-label in refractory PPP with encouraging clinical outcomes.3
With the growing use of IL-17A inhibitors, a series of paradoxical cutaneous adverse reactions has been increasingly recognized. Previous reports have described Behçet-like lesions, alopecia areata, eczematous eruptions, and other paradoxical manifestations occurring during IL-17A blockade.4–6 These reactions are thought to result from immune imbalance and compensatory activation of alternative cytokine pathways following inhibition of a dominant inflammatory axis. However, to the best of our knowledge, the development of acute pityriasis lichenoides et varioliformis acuta (PLEVA) as a paradoxical reaction specifically to secukinumab has not been previously reported.
Here, we report a rare case of acute PLEVA emerging during secukinumab therapy for PPP. This case highlights a potential but uncommon adverse effect of IL-17A inhibition and provides additional insight into the complex immune consequences associated with this therapeutic class.
Case Presentation
A 25-year-old woman presented with a 4-year history of PPP. She had previously been treated with oral acitretin and topical corticosteroids, with inadequate response. Secukinumab therapy was initiated at a dose of 300 mg weekly for 5 consecutive weeks, resulting in marked improvement of PPP symptoms.
However, at week 6 of treatment, the patient developed erythematous papules, papulovesicles, small erosions, and crusts on the face, back, and lower extremities (Figure 1). Skin biopsy revealed parakeratosis and hyperkeratosis of the epidermis, focal vacuolar degeneration of basal cells, and dense perivascular lymphocytic infiltration with scattered plasma cells in the dermis (Figure 2). Based on the clinical manifestations and histopathological findings, a diagnosis of PLEVA was established.
 |
Figure 1 Clinical presentation of acute PLEVA eruption six weeks after initiating secukinumab therapy for palmoplantar pustulosis. The widespread eruption consisted of erythematous papules, vesicles, and small crusted ulcers, involving the (A) face, (B) back, and (C) lower extremities. |
 |
Figure 2 Histopathological findings of a skin biopsy from a PLEVA eruption (Hematoxylin and eosin stain). The image demonstrates characteristic features of acute pityriasis lichenoides et varioliformis acuta, including parakeratosis, basal cell vacuolization, and a dense perivascular lymphocytic infiltrate in the superficial dermis. |
Given the temporal association between the onset of PLEVA and the administration of secukinumab, the biologic agent was considered the likely trigger. Secukinumab was discontinued, and the patient was switched to tofacitinib 5 mg twice daily, leading to gradual resolution of the papules and papulovesicles. After 12 weeks of treatment, her skin lesions had markedly improved, with only residual post-inflammatory hyperpigmentation (Figure 3).
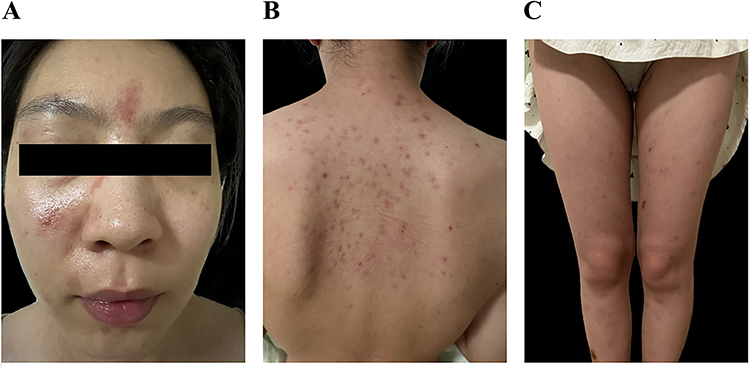 |
Figure 3 Clinical resolution following discontinuation of secukinumab and initiation of tofacitinib therapy. Photographs taken at the 12-week follow-up show near-complete resolution of the acute PLEVA eruption with residual post-inflammatory hyperpigmentation on the (A) face, (B) back, and (C) lower extremities. |
Discussion
Paradoxical reactions can occur during biologic therapy for inflammatory dermatoses, manifesting as exacerbation of the primary disease, phenotype shifts, or the emergence of new lesions.7 These reactions encompass a wide spectrum of clinical presentations, including psoriasis, eczematous eruptions, and alopecia areata.8,9 Although current evidence suggests that cytokine imbalance and altered T-cell polarization may contribute to their pathogenesis, the precise mechanisms remain unclear. Here, we report a case of PLEVA that developed in a patient with PPP during treatment with secukinumab. As a single case report, a definitive causal relationship cannot be established; however, the clear temporal sequence following drug initiation and the subsequent resolution upon its discontinuation support a probable paradoxical reaction. This extends the known spectrum of adverse events associated with IL-17 blockade.
The immunopathogenesis of such reactions is multifactorial, often attributed to cytokine network imbalance. Inhibition of a dominant pathway like IL-17A may precipitate compensatory shifts in the immune milieu.10 For instance, cross-regulation between the IL-17 and TNF-α pathways is well-documented; inhibition of one may lead to upregulation of the other.11 Given the implicated role of TNF-α in PLEVA,12 this compensatory mechanism represents a plausible hypothesis for our observation. The occurrence of PLEVA with other targeted therapies (eg, checkpoint inhibitors, TNF-α antagonists) further underscores immune disequilibrium as a shared cornerstone of paradoxical reactions across drug classes.9,10 In the context of this report, serial cytokine or immunophenotyping data before and after treatment were not available; such profiling in future cases would be invaluable for directly testing this hypothesis and elucidating the precise pathways involved.
A key clinical insight from this case is the observed response to the JAK inhibitor tofacitinib. The JAK-STAT pathway is a convergence point for multiple cytokines potentially involved in both PPP (eg, IL-23) and PLEVA (eg, type I interferons).13 Therefore, its inhibition may simultaneously modulate the disparate inflammatory drivers of the primary disease and the paradoxical eruption. Clinical evidence has accumulated supporting the effectiveness of JAK inhibitors in the treatment of PPP.14,15 Similarly, several case reports have suggested that upadacitinib, a selective JAK1 inhibitor, may also be beneficial for PLEVA.16,17 While this single case provides preliminary, hypothesis-generating evidence for JAK inhibition as a potential therapeutic alternative in this specific scenario, it is not yet a broadly established strategy. Its efficacy and safety in managing biologic-induced paradoxical reactions require validation in larger studies.
Conclusion
In summary, we report a case in which secukinumab, an IL-17A inhibitor used for PPP, was associated with the development of PLEVA. While based on a single observation, the simultaneous improvement of both conditions with a JAK inhibitor suggests this drug class may be a potential therapeutic alternative supported by emerging case-level evidence. Clinicians should remain vigilant for these uncommon adverse reactions to ensure timely recognition and appropriate management.
Data Sharing Statement
The datasets analyzed for this study are available from the corresponding author Dr. Chen Li ([email protected]) upon reasonable request.
Acknowledgments
This case report was prepared in accordance with the CARE guidelines. This study complies with the Declaration of Helsinki. Written informed consent was provided by patient to have the case details and any accompanying images published.
Author Contributions
WL and YC (These authors contributed equally as co-first authors): Investigation, Data Curation, Writing – Original Draft
ZL: Writing – Original Draft
LC (*Corresponding author): Investigation, Supervision, Project Administration, Writing – Review & Editing
JZ (*Corresponding author): Supervision, Project Administration, Writing – Review & Editing
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the National Natural Science Foundation of China (82374272, 82074246) for CL, and Sanming Project of Medicine in Shenzhen (No.SZSM202211025) for JZ.
Disclosure
None of the authors has any financial disclosures or conflicts of interest to declare.
References
1. Murakami M, Terui T. Palmoplantar pustulosis: current understanding of disease definition and pathomechanism. J Dermatol Sci. 2020;98(1):13–5. doi:10.1016/j.jdermsci.2020.03.003
2. Misiak-Galazka M, Wolska H, Rudnicka L. What do we know about palmoplantar pustulosis? J Eur Acad Dermatol Venereol JEADV. 2017;31(1):38–44. doi:10.1111/jdv.13846
3. Xia R, Diao Z, Chen D, et al. Efficacy of anti-interleukin-17A biological agents for palmoplantar psoriasis and palmoplantar pustulosis: a network meta-analysis. Int Immunopharmacol. 2024;130:111716. doi:10.1016/j.intimp.2024.111716
4. Liu K, Sun J. Behcet’s-like disease induced by secukinumab in a patient with psoriasis: a case report and literature review. J Dermatol Treat. 2024;35(1):2347440. doi:10.1080/09546634.2024.2347440
5. Zhang C, Kang T, Qian T, Ma M, Hou X, Li C. Secukinumab-induced alopecia areata successfully treated with tofacitinib in a patient with palmoplantar pustulosis. Clin Cosmet Invest Dermatol. 2023;16:2879–2883. doi:10.2147/CCID.S430156
6. Caldarola G, De Luca E, Amato S, et al. Predictive factors for eczematous eruptions and candidiasis during anti-interleukin-17 treatment in patients with psoriasis: a multicentre real-life experience in Lazio region, Italy. Clin Exp Dermatol. 2025;50(11):2185–2191. doi:10.1093/ced/llaf271
7. Wendling D, Prati C. Paradoxical effects of anti-TNF-α agents in inflammatory diseases. Expert Rev Clin Immunol. 2014;10(1):159–169. doi:10.1586/1744666X.2014.866038
8. Murphy MJ, Cohen JM, Vesely MD, Damsky W. Paradoxical eruptions to targeted therapies in dermatology: a systematic review and analysis. J Am Acad Dermatol. 2022;86(5):1080–1091. doi:10.1016/j.jaad.2020.12.010
9. Miyagawa F. Pathogenesis of paradoxical reactions associated with targeted biologic agents for inflammatory skin diseases. Biomedicines. 2022;10(7):1485. doi:10.3390/biomedicines10071485
10. Chong WP, Mattapallil MJ, Raychaudhuri K, et al. The cytokine IL-17A limits Th17 pathogenicity via a negative feedback loop driven by autocrine induction of IL-24. Immunity. 2020;53(2):384–397.e5. doi:10.1016/j.immuni.2020.06.022
11. Ren J, Deng L, Guo S, Liu H. Paradoxical reaction to IL-17A inhibitor: a case report and literature review. Front Med. 2024;11:1364127. doi:10.3389/fmed.2024.1364127
12. Tsianakas A, Hoeger PH. Transition of pityriasis lichenoides et varioliformis acuta to febrile ulceronecrotic Mucha-Habermann disease is associated with elevated serum tumour necrosis factor-alpha. Br J Dermatol. 2005;152(4):794–799. doi:10.1111/j.1365-2133.2005.06485.x
13. Solimani F, Meier K, Ghoreschi K. Emerging Topical and Systemic JAK Inhibitors in Dermatology. Front Immunol. 2019;10:2847. doi:10.3389/fimmu.2019.02847
14. Dong B, Meng F, Wei J, et al. Palmoplantar pustulosis during pregnancy was successfully treated with tofacitinib: a case report. Skin Appendage Disord. 2025;11(4):335–338. doi:10.1159/000544921
15. Xu Q, Wang X, Yang A, Wei G. Refractory palmoplantar pustulosis successfully treated with JAK inhibitor tofacitinib: a case series. Infect Drug Resist. 2023;16:5165–5172. doi:10.2147/IDR.S421299
16. Houpe J, Gibons R, Nguyen GB, Medepalli V, Inglese M. Bullous pityriasis lichenoides et varioliformis acuta successfully treated with upadacitinib. JAAD Case Rep. 2025;64:158–160. doi:10.1016/j.jdcr.2025.06.051
17. Zeng X, Tong Z, Huang F, Bao C, Gong T, Ji C. Successful treatment of refractory pityriasis lichenoides chronica with upadacitinib in two patients. Indian J Dermatol. 2025;70(6):380–382. doi:10.4103/ijd.ijd_6_25
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Secukinumab-Induced Alopecia Areata Successfully Treated with Tofacitinib in a Patient with Palmoplantar Pustulosis
Zhang C, Kang T, Qian T, Ma M, Hou X, Li C
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2879-2883
Published Date: 16 October 2023
Tofacitinib for Pityriasis Rubra Pilaris: A Case Report
Tan H, Zhang B, Kang X, Wang L, Qiu X, Hu X
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1917-1920
Published Date: 26 August 2024
Awareness of the Risk of Paradoxical Psoriasis in Patients with SAPHO Syndrome Undergoing Treatment with Secukinumab: A Case Series
Xu C, Xu X, Han Y
Journal of Inflammation Research 2025, 18:3705-3712
Published Date: 12 March 2025