Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Secukinumab-Induced Alopecia Areata Successfully Treated with Tofacitinib in a Patient with Palmoplantar Pustulosis
Authors Zhang C ![]() , Kang T
, Kang T ![]() , Qian T, Ma M, Hou X, Li C
, Qian T, Ma M, Hou X, Li C ![]()
Received 10 August 2023
Accepted for publication 30 September 2023
Published 16 October 2023 Volume 2023:16 Pages 2879—2883
DOI https://doi.org/10.2147/CCID.S430156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Chen Zhang,1 Tianlun Kang,1 Tangliang Qian,1 Mingwei Ma,2 Xiujuan Hou,1,* Chen Li3,*
1Department of Rheumatology, Dongfang Hospital Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2School of Clinical Medicine, Peking Union Medical College Hospital (PUMC and CAMS), Beijing, People’s Republic of China; 3Department of Rheumatology, Fangshan Hospital Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiujuan Hou, Department of Rheumatology, Dongfang Hospital Beijing University of Chinese Medicine, No. 6, Fangxing Park District 1, Fangzhuang, Fengtai District, Beijing, People’s Republic of China, Email [email protected] Chen Li, Department of Rheumatology, Fangshan Hospital, Beijing University of Chinese Medicine, No. 4, Chengguan Health Road, Fangshan District, Beijing, People’s Republic of China, Email [email protected]
Abstract: Secukinumab, a monoclonal antibody targeting interleukin-17 (IL-17), has exhibited encouraging results in the therapeutic management of palmoplantar pustulosis (PPP). The development of alopecia areata (AA) is closely related to IL-17, and IL-17A inhibitors were considered as a potential treatment modality. Therefore, the development of AA during secukinumab treatment for PPP is a rare adverse event that has been rarely reported worldwide. Here we report a 35-year-old female patient with PPP who developed AA after completing the induction period of secukinumab treatment. Discontinuing secukinumab and initiating treatment with tofacitinib resulted in a significant improvement in both PPP and AA. The emergence of AA in this patient can be attributed to paradoxical skin reactions associated with IL-17 inhibitors. Tofacitinib appears to alleviate biologic-induced AA during PPP syndrome treatment.
Keywords: alopecia areata, IL-17, secukinumab, palmoplantar pustulosis
Introduction
Palmoplantar pustulosis (PPP) is a chronic and recurrent skin disease characterized by erythema, scales and sterile pustules on the palms and soles, significantly impacting the patient’s quality of life. Emerging evidence suggests the involvement of the IL-17 pathways in the pathogenesis of PPP.1 Consequently, secukinumab, an anti-IL-17 monoclonal antibody, has garnered increasing attention as a therapeutic option for PPP.2 Clinical studies have demonstrated positive responses and good tolerability of secukinumab in treating PPP, with the primary adverse effect being an elevated risk of infections.3,4 However, the available evidence regarding other potential adverse events remains limited. In this case report, we present a noteworthy occurrence of secukinumab-induced alopecia areata (AA) in a patient undergoing therapy for PPP.
Case Report
A 35-year-old female patient was diagnosed with PPP two years ago after noticing sterile pustules on her palms. Initial treatment with calcipotriol ointment proved to be ineffective, and subsequent treatment with acitretin 20mg/day resulted in a temporary response followed by a relapse. The patient then started treatment with adalimumab 40mg/week, but experienced anaphylactic reactions with generalized urticaria after just one week and had to discontinue the medication. In October 2022, because PPP was still active, the patient began a trial of secukinumab 300 mg/week induction regimens. However, after one week, she began to experience sudden hair loss (Figure 1A), which initially was not severe enough to warrant discontinuation of secukinumab. By the completion of the induction period, at week 5, the hair loss worsened and the patient developed significant AA (Figure 1B), characterized by a scaly rash on the scalp and distinct borders of hair loss. There were no apparent emotional stressors, history of diseases (atopic dermatitis, vitiligo, or thyroid disease) associated with AA, or significant blood test changes. Considering the timing of AA onset in relation to the biological therapy, secukinumab was considered a possible causative factor and subsequently discontinued. The patient then initiated monotherapy with tofacitinib (5mg po bi-diurnally). After three months of treatment, gradual improvement in AA was observed (Figure 1C). By the eighth month, significant alleviation of AA lesions was evident (Figure 1D). Additionally, the patient’s palm pustules (Figure 2Ai) and nail damage (Figure 2Aii) associated with PPP showed improvement following completion of the induction period of secukinumab (Figure 2Bi and Bii). Notably, significant alleviation of PPP symptoms was observed based on clinical photographs after 3 months (Figure 2Ci and Cii) and 8 months (Figure 2Di and Dii) of discontinuing secukinumab and initiating treatment with tofacitinib. The patient continues to be followed up.
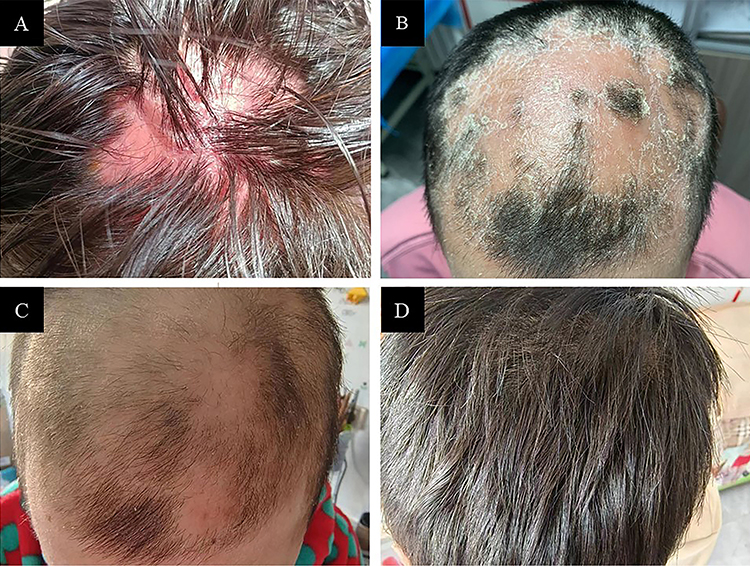 |
Figure 1 (A) Hair loss observed after starting therapy with secukinumab. (B) Alopecia areata was evident after completing the induction period (5 weeks) of secukinumab. Gradual improvement of Alopecia areata after 3 months (C) and 8 months (D) of secukinumab discontinuation and treatment with tofacitinib. |
 |
Figure 2 Presentation of severe erythematous keratotic lesions and pustules on the palms (Ai) and yellowing of nails (Aii), suggestive of palmoplantar pustulosis. Improvement of palms (Bi) and nails (Bii) after treatment with secukinumab. The palmoplantar pustules were alleviated after 3 months (Ci, Cii) and 8 months (Di, Dii) of discontinuing secukinumab and receiving treatment with tofacitinib. |
Discussion
The development of AA during treatment of PPP with secukinumab is a rare occurrence that has been rarely reported worldwide. While there have been five reported cases of AA in patients using secukinumab, all of these cases occurred in the treatment of psoriasis vulgaris. It is important to note that patients with psoriasis are more likely to develop AA.5 However, it is difficult to determine whether the development of AA in these cases was a direct adverse effect of secukinumab or simply a coincidental coexistence of AA with psoriasis. PPP is considered a separate disease from pustular psoriasis in Japan due to differences in genetic background.6 Therefore, the relationship between AA and PPP has not been well-established. There have only been four case reports indicating the presence of AA prior to the onset of PPP.7 When compared to other reported cases of secukinumab-induced AA in psoriasis patients, the coexistence of AA and PPP appears less likely in this particular case, suggesting a closer association between AA and the use of secukinumab.
From a pathogenetic perspective, IL-17 and its main source, T helper (Th)17 cells, are considered critical inducers of AA. However, the clinical significance of IL-17 in the development of AA is still a matter of debate and not fully understood. Elevated levels of IL-17 have been observed in both intralesional and serum samples of AA patients, suggesting its potential involvement in the disease progression.8 This finding has led to the exploration of IL-17 inhibitors as potential treatments for AA. Paradoxically, there have been reported cases of AA developing during treatment with IL-17 inhibitors.9 This paradoxical reaction is similar to what has been observed with tumor necrosis factor-alpha (TNF-ɑ) inhibitors, which also induced cutaneous reactions with AA-like manifestations.10,11 The similarity in clinical presentations between these two groups of biological drugs has prompted the proposal of common underlying mechanisms for their paradoxical effects. Some suggested hypotheses include the modification of cytokine balance, activation of alternative inflammatory pathways, and changes in the polarization of T-cell responses.12 The IL-17 cytokine family comprises 6 family members (IL-17A to IL-17F) and receptor subunits. The specific involvement of secukinumab, a targeted IL-17A inhibitor, in the paradoxical reaction might be speculated to be associated with its modulation of signaling pathways involving other family members, such as IL-17E and IL-17C.13 However, the precise mechanism is still under investigation. These mechanisms may disrupt the delicate immune regulation and lead to the development of paradoxical reactions, including AA. Furthermore, the appearance of abnormal skin lesions has also been observed in patients with synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome who were treated with IL-17 inhibitors.14 In this case, we consider the development of AA to be a paradoxical skin lesion caused by IL-17A inhibitor.
As for treatment, tofacitinib, an oral pan Janus-kinase (JAK) inhibitor, has shown effectiveness in the treatment of certain conditions, including PPP and AA.15,16 Its mechanism of action involves inhibiting JAKs, particularly JAK1 and JAK3, which play crucial roles in cytokine and growth factor signaling pathways. This inhibition helps to modulate immune responses and reduce inflammation, making it a potential therapeutic option for conditions like PPP and AA. In the case mentioned, the patient’s PPP and AA both improved after monotherapy with tofacitinib. It is possible that tofacitinib played a role in relieving biologic-induced AA during the treatment of PPP syndrome.
We present a case of secukinumab-induced AA in a patient undergoing treatment for PPP, which has been rarely reported in the literature. In our point of view, the emergence of AA is also a paradoxical skin reaction associated with IL-17 inhibitors. Tofacitinib may be a good option for biologic-induced AA during PPP syndrome treatment, but larger sample sizes and multi-ethnic clinical trials are needed in the future to provide stronger evidence.
Ethics Approval
This work was approved by the medical ethics committee of Fangshan Hospital of Beijing University of Chinese Medicine with the following reference numbers: FZJ JS-2021-002. Participants gave informed consent to participate in the study before taking part.
Consent Statement
Written informed consent was provided by patient to have the case details and any accompanying images published.
Funding
This work was supported by the National Natural Science Foundation of China (No.82074246) for CL and construction project of clinical key specialty in Fengtai district of Beijing.
Disclosure
The authors report there are no competing interests to declare in this work.
References
1. Misiak-Galazka M, Zozula J, Rudnicka L. Palmoplantar Pustulosis: recent Advances in Etiopathogenesis and Emerging Treatments. Am J Clin Dermatol. 2020;21(3):355–370. doi:10.1007/s40257-020-00503-5
2. Galluzzo M, Talamonti M, Atzori L, et al. Secukinumab for the treatment of palmoplantar psoriasis: a 2-year, multicenter, real-life observational study. Expert Opin Biol Ther. 2022;22(4):547–554. doi:10.1080/14712598.2022.2029841
3. Reolid A, Armesto S, Sahuquillo-Torralba A, et al. Secukinumab is effective in the treatment of recalcitrant palmoplantar psoriasis and palmoplantar pustular psoriasis in a daily practice setting. J Am Acad Dermatol. 2022;87(3):705–709. doi:10.1016/j.jaad.2022.05.047
4. Fujita H, Ohtsuki M, Morita A, et al. Safety and Effectiveness of Secukinumab in Psoriasis Vulgaris and Psoriatic Arthritis: real-world Evidence in Japan. J Dermatol. 2021;48(2):175. doi:10.1111/1346-8138.15655
5. Jung JM, Yang HJ, Lee WJ, et al. Association between psoriasis and alopecia areata: a systematic review and meta-analysis. J Dermatol. 2022;49(9):912–915. doi:10.1111/1346-8138.16420
6. Murakami M, Terui T. Palmoplantar pustulosis: current understanding of disease definition and pathomechanism. J Dermatol Sci. 2020;98(1):13–19. doi:10.1016/j.jdermsci.2020.03.003
7. Hiraiwa T, Yamamoto T. Alopecia Areata and Palmoplantar Pustulosis: report of 4 Cases. Actas Dermosifiliogr. 2018;109(8):751–752. doi:10.1016/j.ad.2017.09.022
8. Ramot Y, Marzani B, Pinto D, et al. IL-17 inhibition: is it the long-awaited savior for alopecia areata? Arch Dermatol Res. 2018;310(5):383–390. doi:10.1007/s00403-018-1823-y
9. Antoury L, Maloney N, Cheng K. Development of alopecia in patients treated with interleukin-17 inhibitors. Dermatol Ther. 2020;33(6):e14527. doi:10.1111/dth.14527
10. Tauber M, Buche S, Reygagne P, et al. Alopecia areata occurring during anti-TNF therapy: a national multicenter prospective study. J Am Acad Dermatol. 2014;70(6):1146–1149. doi:10.1016/j.jaad.2014.03.005
11. Ferran M, Calvet J, Almirall M, et al. Alopecia areata as another immune-mediated disease developed in patients treated with tumour necrosis factor-α blocker agents: report of five cases and review of the literature. J Eur Acad Dermatol Venereol. 2011;25(4):479–484. doi:10.1111/j.1468-3083.2010.03770.x
12. Murphy MJ, Cohen JM, Vesely MD, Damsky W. Paradoxical eruptions to targeted therapies in dermatology: a systematic review and analysis. J Am Acad Dermatol. 2022;86(5):1080–1091. doi:10.1016/j.jaad.2020.12.010
13. Miyagawa F. Pathogenesis of Paradoxical Reactions Associated with Targeted Biologic Agents for Inflammatory Skin Diseases. Biomedicines. 2022;10(7):1485. doi:10.3390/biomedicines10071485
14. Luan L, Lv C. Secukinumab-induced paradoxical skin lesions, but successful treatment with tofacitinib in SAPHO syndrome: a case report. J Dermatolog Treat. 2023;20:1–16. doi:10.1080/09546634.2023.2193662
15. Li C, Li Z, Cao Y, et al. Tofacitinib for the Treatment of Nail Lesions and Palmoplantar Pustulosis in Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis Syndrome. JAMA Dermatol. 2021;157(1):74–78. doi:10.1001/jamadermatol.2020.3095
16. Kennedy Crispin M, Ko JM, Craiglow BG, et al. Safety and efficacy of the JAK inhibitor tofacitinib citrate in patients with alopecia areata. JCI Insight. 2016;1(15):e89776. doi:10.1172/jci.insight.89776
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness of the Risk of Paradoxical Psoriasis in Patients with SAPHO Syndrome Undergoing Treatment with Secukinumab: A Case Series
Xu C, Xu X, Han Y
Journal of Inflammation Research 2025, 18:3705-3712
Published Date: 12 March 2025
Paradoxical Cutaneous Reaction: Secukinumab–Associated PLEVA in Palmoplantar Pustulosis
Liu W, Chen Y, Lin Z, Zhang J, Li C
Journal of Inflammation Research 2026, 19:590485
Published Date: 11 February 2026