")
Back to Journals » Cancer Management and Research » Volume 15
Pandemic-Induced Depression Among Older Adults with a History of Cancer During the COVID-19 Pandemic: Findings from the Canadian Longitudinal Study on Aging
Authors Bird MJ, Li G, MacNeil A , Jiang Y, de Groh M, Fuller-Thomson E
Received 17 May 2023
Accepted for publication 8 August 2023
Published 6 September 2023 Volume 2023:15 Pages 937—955
DOI https://doi.org/10.2147/CMAR.S421675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Meghan J Bird,1,2 Grace Li,3 Andie MacNeil,1,2 Ying Jiang,4 Margaret de Groh,4 Esme Fuller-Thomson1,2,5,6
1Factor-Inwentash Faculty of Social Work, University of Toronto, Toronto, ON, Canada; 2Institute for Life Course and Aging, University of Toronto, Toronto, ON, Canada; 3Department of Sociology, University of Victoria, Victoria, BC, Canada; 4Applied Research Division, Centre for Surveillance and Applied Research, Public Health Agency of Canada, Ottawa, ON, Canada; 5Department of Family and Community Medicine, Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada; 6Bloomberg Faculty of Nursing, University of Toronto, Toronto, ON, Canada
Correspondence: Esme Fuller-Thomson, Factor-Inwentash Faculty of Social Work, University of Toronto, 246 Bloor Street West, Toronto, ON, M5S 1V4, Canada, Tel +1 416 978-3269, Fax +1 416 978-7072, Email [email protected]
Purpose: The objectives of this study were to identify the prevalence of, and factors associated with, incident and recurrent depression in a sample of older adults with a history of cancer during the COVID-19 pandemic.
Materials and Methods: Data were drawn from four waves of the Canadian Longitudinal Study on Aging Comprehensive Cohort (n=2486 with cancer). The outcome of interest was a positive screen for depression based on the CES-D-10 during the autumn of 2020.
Results: Among older adults with cancer and no pre-pandemic history of depression (n=1765), 1 in 8 developed first onset depression during the pandemic. Among respondents with cancer and a history of depression (n=721), 1 in 2 experienced a recurrence of depression. The risk of both incident and recurrent depression was higher among those who were lonely, those with functional limitations, and those who experienced an increase in family conflict during the pandemic. The risk of incident depression only was higher among older women, those who did not engage in church or religious activities, those who experienced a loss of income during the pandemic, and those who became ill or had a loved one become ill or die during the pandemic. The risk of recurrent depression only was higher among those who felt isolated from others and those whose income did not satisfy their basic needs.
Conclusion: Health care providers should continue to screen and provide mental health support to their cancer patients and those with a lifetime history of cancer, with consideration for those with the aforementioned vulnerabilities.
Keywords: COVID-19, depression, cancer, older adults, CLSA
Introduction
Cancer is the leading cause of death in Canada and the second leading cause of death in the United States, accounting for 21% and 28% of all deaths, respectively.1 There is robust literature indicating that those with cancer are more likely to experience depression than those without cancer.2–4 According to a recent meta-analysis, approximately one in five cancer patients experience comorbid depression.5 Cancer patients with depression are more vulnerable to many adverse outcomes when compared to cancer patients without depression, including decreased immune function,6 lower quality of life,7 increased emergency department use, longer hospitalizations,8 and higher mortality.9 Recent research has emphasized the importance of addressing comorbid depression to support the physical and mental well-being of cancer patients.10
The relationship between cancer and depression is of particular concern during the COVID-19 pandemic. The pandemic and associated lockdowns have had detrimental impacts on numerous areas of life, including job losses and reduced economic security, disruptions to healthcare access, and increased social isolation. It is unsurprising that this global disruption of activities was associated with a rise in depression in the general population.11 Simultaneously, individuals with cancer have also had to navigate the stress of being particularly vulnerable to severe COVID-19 related morbidity and mortality.12 While strict adherence to lockdowns was an important step for many cancer patients to minimize their risk of COVID-19 infection, for many individuals this also meant forgoing social support, which is an important source of strength during cancer treatment and recovery.13 Furthermore, many cancer patients faced potentially life-threatening delays and barriers to healthcare access due to medical systems being overwhelmed by COVID-19 patients.11
When considering the elevated risk of depression among cancer patients prior to the pandemic, combined with the unprecedented pandemic-related stressors for cancer patients during the past few years, it is evident that there is an urgent need for longitudinal research to examine mental health during the pandemic of individuals with a history of cancer. The current study addresses this gap by analyzing data from the Canadian Longitudinal Study on Aging (CLSA) to achieve the following objectives: (1) to examine the prevalence of incident and recurrent depression during the COVID-19 pandemic among adults aged 50 and older with a history of cancer; and (2) to identify factors associated with incident and recurrent depression among these individuals during the pandemic.
Materials and Methods
Data Source
As has been described elsewhere,14,15 the CLSA is a large, prospective study that recruited Canadians aged 45 to 85 years in 10 provinces between 2011 and 2015.16,17 Participation in the CLSA cohort is voluntary and all individuals provided written informed consent.16 The baseline comprehensive cohort recruited 30,097 participants and 27,737 participants went on to complete Follow-up 1. To assess the impact of COVID-19 on older adults, CLSA participants were invited to participate in the COVID Spring and COVID Autumn questionnaires. We analyzed data from participants recruited in the Baseline (conducted between 2011 and 2015), Follow-up 1 (conducted between 2015 and 2018), COVID Spring 2020 (conducted between April 15 to May 30, 2020), and COVID Autumn 2020 (conducted between September 29 to December 29, 2020) waves of the comprehensive cohort of Canadian Longitudinal Study on Aging (CLSA). The detailed CLSA methodology are described elsewhere.16,17
All Canadian Longitudinal Study on Aging (CLSA) waves of data collection have been approved by research ethics boards at all collaborating Canadian institutions. The CLSA was conducted in accordance with the 1964 Helsinki declaration and its later amendments, and with the ethical standards of each institutional research committee. The current study was approved by the University of Toronto’s Research Ethics Board (Protocol #41167; approved June 4, 2021).
Sample
The Baseline and Follow-up 1 data of the CLSA identified respondents with cancer prior to the COVID-19 pandemic (n = 2486). Self-reported cancer was defined by the question “Has a doctor ever told you that you had cancer?” (1 = yes; 0 = no). Respondents who were lost to follow-up or had missing data on key covariates were excluded from the analysis.
Measures
To determine the history of depression prior to the pandemic, the 10-item Center for Epidemiologic Studies Depression Scale (CES-D-10) and self-report of a medical diagnosis of depression were used at both Baseline and Follow-up 1. The CES-D-10 contains 10 items on depressive symptoms such as feelings of depression, loneliness, hope for the future, and restless sleep in the past 7 days. This reliable and validated tool is widely used to screen for depressive symptoms.18 The total score ranges from 0 to 30, with higher scores indicating higher severity. A score of 10 or more (CES-D 10 total score ≥10) was used to identify those with depression. Moreover, at Baseline and Follow-up 1, respondents were also asked: “Did your doctor ever tell you that that you had clinical depression?”. Respondents were categorized as not having pre-pandemic depression if, at both waves of data collection, they had scores less than 10 on the CES-D-10 and they reported they had never been diagnosed with clinical depression by a medical professional. If at least one of the four measures above indicated depression, the respondent was classified as having pre-pandemic depression.
We included the following sociodemographic variables: age at the Autumn 2020 wave, sex (female; male), marital status (married/common-law; separated/divorced/widowed; single), immigrant status (yes; no), visible minority status (non-white; white), education (less than secondary school; some post-secondary school; post-secondary degree/diploma), annual household income (less than $50,000; $50,000 - $99,999; $100,000 or more; missing), house ownership (rent; own with mortgage; own without mortgage), and total savings (less than $50,000; $50,000 - $99,999, $100,000 or more, missing).
Health-related variables included Body Mass Index (BMI), chronic pain, and multimorbidity. BMI was divided into three categories: underweight or normal weight (BMI < 25), overweight (BMI = 25.0–29.99), obese (BMI ≥30.0). Chronic pain was measured by the question: “Are you usually free of pain or discomfort?” (yes; no). Multimorbidity was defined as having multiple chronic conditions (0; 1; 2; 3 or more; missing), including 1) Diabetes, (2) Heart disease (3) peripheral vascular disease or poor circulation in the extremities, (4) Dementia or Alzheimer’s disease, (5) Multiple sclerosis, (6) Epilepsy, (7) Migraine headache, (8) Intestinal or gastric ulcers, (9) Intestinal disorders, (10) Asthma, (11) COPD, (12) Stroke or CVA (cerebrovascular accident), (13) Glaucoma, (14) Kidney disease, (15) Macular degeneration, (16) Mini-stroke or TIA (transient ischemic attack), and (17) Parkinson’s disease.
Respondents were queried about the frequency of experiencing emotions related to lacking companionship, feeling left out, and feeling isolated from others. The response options included 1 = hardly ever, 2 = some of the time, and 3 = often. To simplify the analysis, categories 1 and 2 were merged and recoded as “no”, indicating the absence of such emotions, while category 3 was recoded as “yes”, indicating the presence of these emotions.
Religiosity was measured by asking respondents how often they participated in church or religious or spiritual activities at home or in any other location. The variable assessing church activities is derived from the following question: “Over the last 12 months, how frequently did you engage in church or religious activities, such as services, committees, or choirs?” The response options ranged from 1 = at least once a day, 2 = at least once a week, 3 = at least once a month, 4 = at least once a year, to 5 = never. For analysis purposes, we combined categories 1, 2, and 3 into the “often” category, while categories 4 and 5 were merged into the “rare” category. The variable measuring religious or spiritual activities at home was constructed based on the following question: “Within the last 12 months, how frequently did you participate in religious or spiritual activities (such as prayer, meditation) either at home or in any other location?” The response options consist of six categories: 1 = at least once a day, 2 = at least once a week, 3 = at least once a month, 4 = at least 3 times a year, 5 = once or twice a year, 6 = not at all. To simplify the analysis, categories 1, 2, and 3 are grouped together and referred to as “often”, while categories 4, 5, and 6 are combined and referred to as “rare”.
We collected retrospective data on Adverse Childhood Experiences (ACEs), which were evaluated by computing a cumulative score based on childhood physical abuse, childhood sexual abuse, childhood exposure to intimate partner violence, and neglect. Childhood physical abuse was present if respondents reported being kicked, bit or punched, or chocked, burned or physically attacked in some other way one or more times. Childhood sexual abuse was present if respondents reported that an adult forced them or attempted to force them into any unwanted sexual activity by threatening them, holding them down, or hurting them in some way one or more times. Childhood exposure to intimate partner violence was present if respondents reported seeing or hearing parents, stepparents or guardians hitting each other more than 10 times. Respondents who reported that their parents or guardians had not taken care of their basic needs such as keeping clean or providing food or clothing one or more times were defined as “neglected”. Each of these experiences was coded as either 0 or 1, resulting in an ACE score ranging from 0 to 4.
At the beginning of the COVID-19 pandemic, respondents were asked in the Spring 2020 questionnaire if they had left home in the past month (yes; no). Respondents were also asked if they felt lonely (rarely or never/some of the time [0–2 days per week] vs occasionally/all the time [3–7 days per week]). Respondents’ type of dwelling was categorized as house, apartment, and other. Respondents were also asked if they lived alone at the start of the COVID-19 pandemic.
We developed the functional limitation scale based on three questions: “Do you have any difficulty standing up after sitting in a chair?”, “Do you have any difficulty walking alone up and down a flight of stairs?”, and “Do you have any difficulty walking 2 to 3 neighborhood blocks?” Each question had four response categories: 1 = yes, 2 = no, 3 = unable to do, and 4 = Do not do on doctor’s advice. We recoded the categories 1, 3, 4 as “yes”, and the category 2 as “no” for each question. If respondents answered all three questions as 0, then the functional limitation scale variable was coded as 0. Otherwise, if they answered “yes” to any of the questions, the functional limitation scale variable was coded as 1.
Stressors associated with the COVID-19 were measured at the Autumn 2020 wave, and they were categorized into five composite indicators. Experiences were categorized as yes if participants responded yes to at least one experience in a given category and categorized as no if they responded no to all questions in that category. Health-related questions included: “You were ill”, “People close to you were ill”, and/or “Death of a person close to you”. Questions related to difficulties in accessing resources included: “Loss of income” and/or “Unable to access necessary supplies or food”. Questions related to family conflict included “Increased verbal or physical conflict” and/or “Breakdown of family/marital relationship”. Problems related to other family issues included “Separation from family”, “Increased time caregiving”, and/or “Unable to care for people who require assistance due to health condition or limitation”. Problems related to health care included “Unable to access to my usual health care”. Problems related to medication included “Unable to get my usual prescription drugs and treatments”.
Statistical Analyses
The analysis was conducted in several steps. First, we compared the characteristics of CLSA participants with a cancer history, but without a pre-pandemic history of depression to those with a cancer history and a pre-pandemic history of depression. Means and standard deviations were reported for continuous variables and frequencies and percentages for categorical variables. Statistical differences between these two groups were tested using Chi-square tests and independent t-tests. Second, we examined the predictors of incident depression and recurrent depression at Autumn 2020 using logistic regression models. For all predictors, we reported adjusted odds ratios and 95% Confidence Intervals (CIs). Finally, we performed a sensitivity analysis to examine the prevalence of incident and recurrent depression at the pre-pandemic Follow-up 1 questionnaire compared to the Autumn 2020 questionnaire. This was done to examine differences in depression before and during the pandemic. Additionally, we conducted this sensitivity analysis among individuals with a history of cancer in comparison to those without a history of cancer nor several other serious health conditions (ie, peripheral vascular disease or poor circulation in the extremities, epilepsy, intestinal or gastric ulcers, intestinal disorders, asthma, COPD, glaucoma, macular degeneration, mini-stroke, or TIA (transient ischemic attack). This was done to examine how the COVID-19 pandemic specifically impacted individuals with cancer in comparison to older adults without cancer and other serious health conditions. All hypothesis tests were two-sided and statistical significance was assessed using alpha = 0.05. We reported Nagelkerke R square to evaluate the goodness-of-fit of logistic models. We calculated the variance inflation factor (VIF) to assess the multicollinearity among the independent variables in the logistic regression analyses, and we did not find any potential problems. All analyses were conducted using R version 4.1.3.
Results
Approximately 1 in 8 older adults (11.8%, 95% CI [10.3%; 13.3%]) with cancer and no pre-pandemic history of depression developed depression for the first time during the COVID-19 pandemic, while almost 1 in 2 older adults (45.8%, 95% CI [42.2%; 49.5%]) with cancer and a history of depression experienced a recurrence of depression during the pandemic. Table 1 displays the characteristics of the study sample, comparing individuals with a history of cancer but no pre-pandemic history of depression to those with a history of both cancer and a pre-pandemic depression. The results indicate that a higher proportion of individuals with cancer and a history of pre-pandemic depression were female, unmarried (separated/divorced/widowed/single), renting their homes, had obesity, had total savings less than $49,999, lacked sufficient income to meet their needs, experienced chronic pain, reported feeling lonely occasionally/all the time during the pandemic, lived in an apartment and alone, had functional limitations, and were more likely to experience stressors related to COVID.
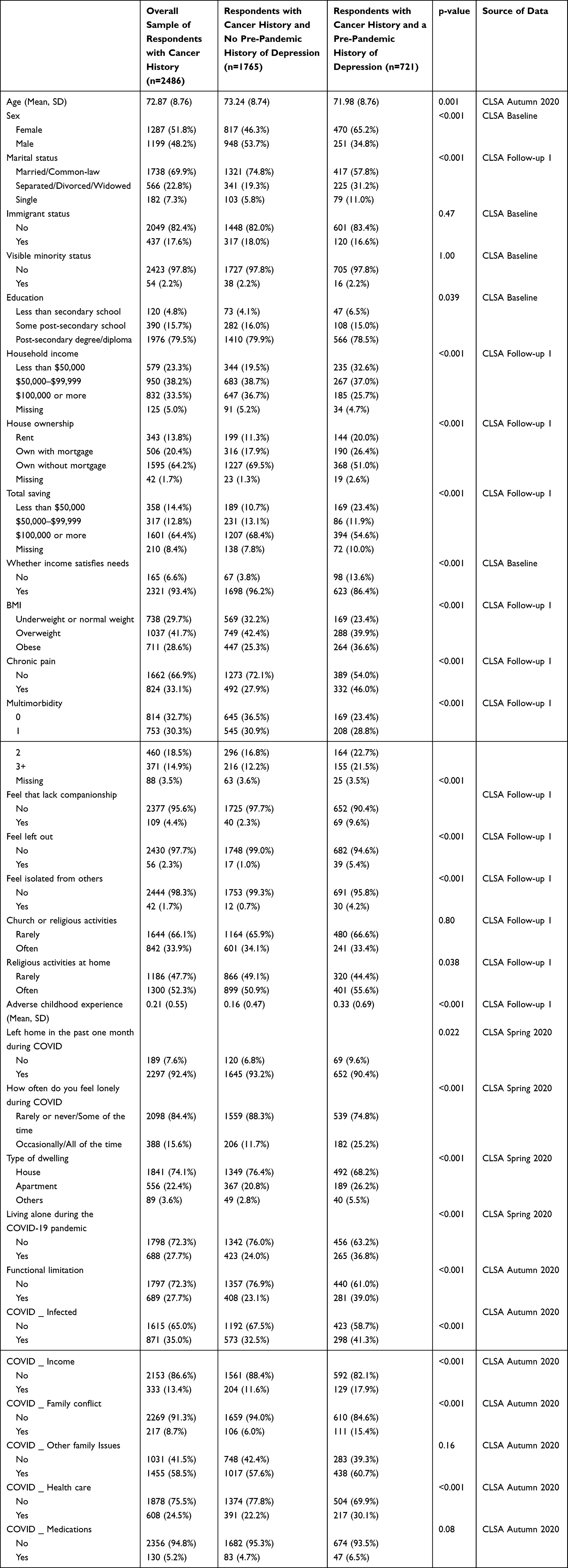 |
Table 1 Characteristics of CLSA Respondents with a History of Cancer (n=2486) by Pre-Pandemic History of Depression |
Table 2 presents the characteristics of respondents according to their pre-pandemic history of depression, as well as their depression status during the COVID-19 pandemic. The results show that respondents with a history of cancer and a history of pre-pandemic depression had a much higher rate of depression (45.8%) during Autumn 2020 than those without a history of pre-pandemic depression (11.8%). Furthermore, more than 76.6% of the respondents who had screened positive for depression based on CES-D-10 scores both at Baseline and Follow-up 1 were depression during the pandemic. More than half (53.5%) of those who screened positive for depression at Follow-up 1 based on CES-D-10 scores, but not at Baseline, experienced recurrent depression during the pandemic. Nearly 50% who were depressed at Baseline according to CES-D-10 scores, but not at Follow-up 1, experienced depressive symptoms during the pandemic. Among those who had reported that they had been diagnosed by a health professional with depression at some point in their lives but had not been depressed according to the CES-D-10 scores at Baseline or Follow-up 1, approximately 1 in 4 (22.8%) screened positive for depression based on CES-D-10 scores in the autumn of 2020.
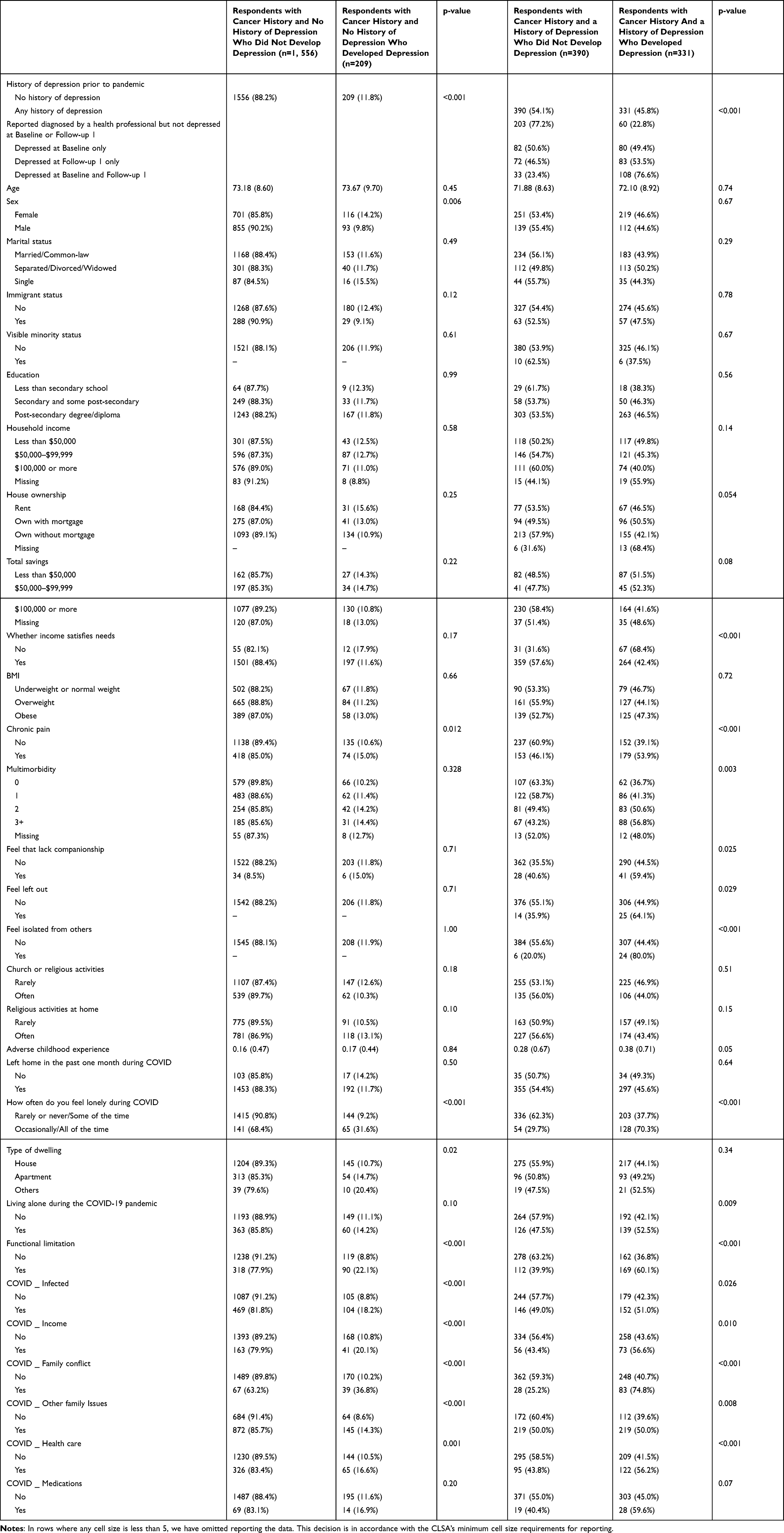 |
Table 2 Profile of CLSA Participants with Cancer According to their Pre-Pandemic History of Depression and their Depression Status in Autumn 2020. |
The findings on the relationships between the risk factors and depression status during the Autumn 2020 wave for older adults with a history of cancer and no pre-pandemic history of depression are presented in Table 3. The analysis revealed that female respondents had a statistically higher odds of incident depressive symptoms than male respondents during the COVID-19 pandemic (OR = 1.46, 95% CI [1.02; 2.08], p =0.039). Furthermore, individuals who rarely attended church or religious activities prior to the pandemic were significantly more likely to experience depressive symptoms than those who often attended church or religious services (OR = 1.79, 95% CI [1.17;2.74], p =0.007). Older adults with a history of cancer who reported feeling lonely occasionally/all the time in the Spring 2020 wave had quadruple the odds of experiencing depressive symptoms during the Autumn of 2020 than those who felt lonely rarely or never / some of the time (OR=4.40, 95% CI [2.91;6.63], p<0.001). There was a significant and substantial difference in depression between respondents with functional limitations and those without (OR = 3.08, 95% CI [2.11; 4.48], p <0.001). Moreover, COVID-related stressors were significantly associated with depressive symptoms. Individuals who had COVID or those who had people around them infected with COVID (OR = 3.08, 95% CI [2.11; 4.48], p < 0.001), those with income loss during the pandemic (OR = 2.24, 95% CI [1.61; 3.11], p < 0.001), and people who had family conflict during the pandemic (OR = 4.19, 95% CI [2.54; 6.90], p = 0.001) had significantly higher odds of incident depressive symptoms. The Nagelkerke R square for this model was 0.23.
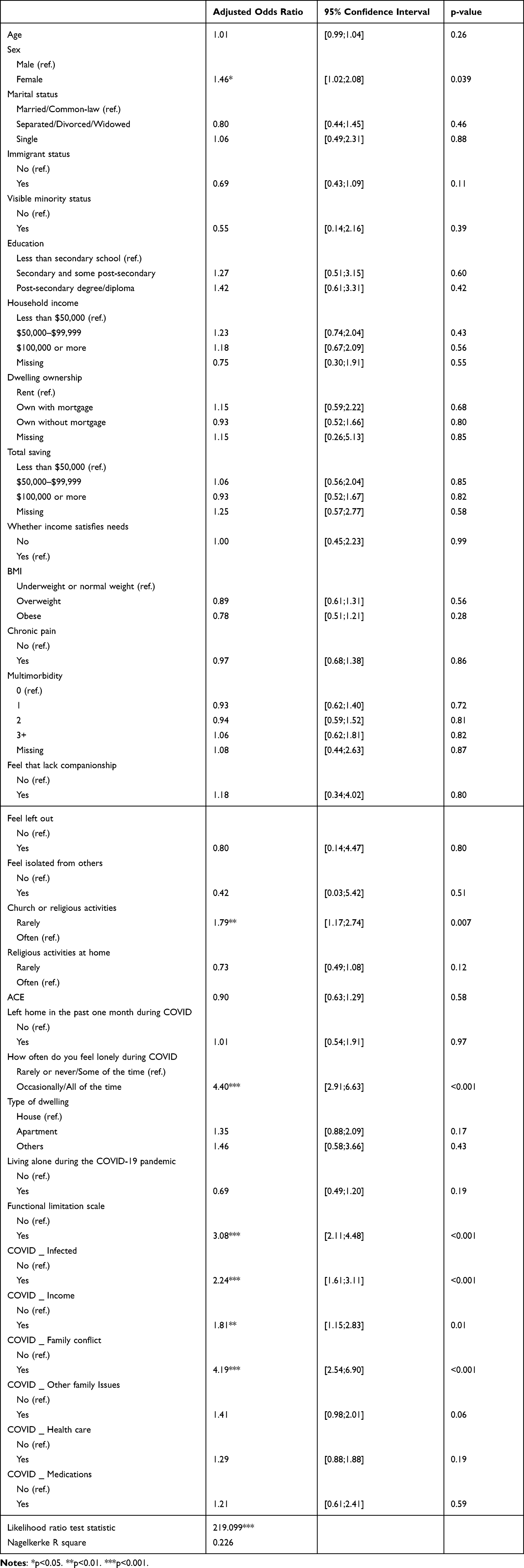 |
Table 3 Logistic Regression Results for Incident Depression During Autumn 2020 Among Respondents with a History of Cancer and No Pre-Pandemic History of Depression (n=1765) |
Table 4 presents the association of depression status during the Autumn 2020 wave and covariates among respondents with a history of cancer and a pre-pandemic history of depression. Respondents who reported that their income did not meet their needs prior to the pandemic were more likely to report depression during the pandemic (OR = 2.86; 95% CI [1.63;5.01], p < 0.001). People who felt isolated from others prior to the pandemic were more likely to suffer from depression in Autumn 2020 than those who did not (OR=5.02, 95% CI [1.27;9.83], p = 0.021). Those who felt lonely occasionally / all the time during the Spring of 2020 were more likely to suffer from depression during the Autumn of 2020 than respondents who felt lonely rarely / some of the time (OR=3.42, 95% CI [2.23;5.25], p<0.001). Older adults with a history of cancer and functional limitations had a higher risk for depressive symptoms during the Autumn 2020 compared to those without such limitations (OR = 2.17, 95% CI [1.47; 3.21], p <0.001). Respondents who experienced family conflict during the pandemic were 4.48 times more likely to have depression in Autumn 2020 than those without (95% CI [2.68;7.49], p=<0.001). The Nagelkerke R square for this model was 0.31.
 |
Table 4 Logistic Regression Results for Depression During Autumn 2020 Among Respondents with a History of Cancer and a Pre-Pandemic History of Depression (n=721) |
The results of the sensitivity analysis are presented in Table 5. This indicates that the incidence and recurrence of depression were significantly higher among older adults with a history of cancer during the pandemic (ie, Autumn 2020) than it had been during the Follow-up 1 wave of data collection (2015–2018) when incident depression was 5.9% (95% CI [4.7%; 7.1%]) and recurrent depression was 31.3% (95% CI [27.0%; 35.6%]). Additionally, respondents with a history of cancer had a significantly higher prevalence of recurrent depression during the pandemic (45.8% 95% CI [42.2%; 49.5%]) when compared to individuals with no serious health conditions (39.7% with 95% CI [37.0%, 42.4%]).
 |
Table 5 Sensitivity Analysis of CLSA Respondents with Cancer Compared to Respondents Without Any Serious Health Conditions with Respect to Incident and Recurrent Depression During the Follow-up 1 Wave of Data Collection and During the Autumn 2020 Wave of Data Collection |
Discussion
The objectives of this study were to examine the prevalence of incident and recurrent depression among older adults with a history of cancer during the COVID-19 pandemic, as well as to identify factors associated with incident and recurrent depression among these sub-populations during the pandemic. Approximately 1 in 8 older adults with a history of cancer and no pre-pandemic history of depression experienced incident depression during the COVID-19 pandemic, while approximately 1 in 2 older adults with a history of cancer and a history of depression experienced a recurrence of depression during the pandemic. We also found that when the sample was restricted to those with a pre-pandemic history of depression, the recurrence of depression during the pandemic was significantly higher for respondents with cancer when compared to individuals without any serious health conditions. These findings underlie the substantial mental health toll of the COVID-19 pandemic on older adults with a history of cancer, emphasizing the importance of screening and targeted outreach to this population. The current study also identified several factors that were associated with a higher risk of incident and recurrent depression among older adults with cancer during the COVID-19 pandemic.
Older women in the current study were more likely to develop incident depression than older men. This is in keeping with a large body of pre-pandemic research which indicates that women in Canada and abroad consistently have a higher risk of depression than men.19 The increased risk among women may also be, in part, because older women are more likely to fall into caretaking roles, which is associated with an increased risk of depression.20 For many women, caregiving responsibilities were severely exacerbated during the pandemic, resulting in increased caregiver burden21 and declines in mental health.22
Older adults with a history of cancer who had functional limitations had more than double the odds of both incident and recurrent depression when compared to their counterparts without functional limitations. Functional limitations have been identified as a major risk factor for depression later in life.23 The pandemic may have exacerbated functional limitations in those with a history of cancer, as socially restricted older adults are often more sedentary, which is a risk factor for the development of functional limitations.24
Experiencing family conflict during the pandemic was also associated with an approximate four-fold risk of incident and recurrent depression among older adults with a history of cancer. This finding aligns with research that has identified interpersonal conflict to be a risk factor for depression among older adults.25 Extended periods of lockdown and quarantine have been found to increase familial conflict.26 The pandemic also reduced access to many coping strategies that can help mitigate family conflict, such as time spent outside the home and time spent with friends.
Multiple measures of socioeconomic status were also associated with a higher risk of incident and recurrent depression for older adults with cancer history. Respondents who experienced a loss of income and/or difficulty accessing necessary resources during the pandemic had almost double the odds of experiencing incident depression compared to those who did not experience such financial strain. Among those with a history of depression, respondents who reported that their income did not satisfy their basic needs prior to the pandemic had nearly triple the risk of recurrent depression compared to those whose income satisfied their basic needs. These findings support existing literature on the impact of financial stressors on the development of depression.12 Financial stressors that have been found to contribute to depression include food insecurity, job precarity, uncertainty about the future, and lack of paid sick days.27 Many of these stressors were also severely exacerbated by the COVID-19 pandemic which often intensified financial strain and stress levels among vulnerable older adults. A study conducted prior to the pandemic found that approximately 50% of older adults aged 55 and older in the United States did not have at least three months of emergency savings.28
Older adults with a history of cancer who often felt lonely during the Spring of 2020 were three times more likely to experience incident and recurrent depression during the Autumn of 2020. This finding is consistent with other research on depression during the pandemic. A recent study on depression among cancer patients in the United Kingdom found that respondents who were lonely had more than quadruple the risk of depression that those who were not lonely.29 Cancer patients were especially vulnerable to loneliness during the COVID-19 due to the pressure to adhere to lockdown restriction to minimize infection risk.30
Among those with a history of cancer and no previous history of depression, those who reported not engaging in religious or spiritual activities prior to the pandemic had 79% higher odds of incident depression in Autumn 2020. This aligns with research that has identified the protective effect of religious participation on depression risk.31 For cancer patients, religious and spiritual observance is associated with overall physical health and functional wellbeing32 and fewer adverse mental health outcomes.33 Although the pandemic disrupted access to many in-person religious services, many religious groups found creative ways to continue gathering as a community, whether that be online, outdoors, or in small groups that adhered to public health guidelines.34,35 For older adults with cancer, the ability to attend virtual religious services may have provided critical opportunities for social engagement in the absence of in-person gatherings.
Older persons with a history of cancer who became ill or had a loved one become ill or die during the pandemic were twice as likely to experience incident depression. Previous studies have found that the loss of a loved one during the pandemic or having a loved one develop COVID-19 amplified psychological distress and depression among older adults.36,37 Furthermore, periods of lockdown and physical distancing limitations disrupted many important aspects of the grieving process, such a being present at the death of a loved one38 and holding funeral and memorial services.39 Individuals who experienced the death of a loved one during the COVID-19 pandemic may have a greater likelihood for developing pathological grief,40 which is an identified risk for depression.41
Limitations
The current study has some limitations to consider. First, depression was based on the CES-D-10, which is a self-report measure. Although a clinical assessment would have been preferable, the CES-D-10 is a frequently utilized instrument to measure depression with high reliability and validity.42 Second, although our regression models offer valuable insight on cancer history and depression during the pandemic, it is important to note that despite incorporating a large number of variables, the variance explained in the models for incident and recurrent depression remains somewhat low (23% and 31%, respectively). This suggests that there may be other unidentified risk factors contributing to the outcomes observed in our study. For example, the data drawn from the CLSA does not specify details on the participants’ cancer diagnoses, such as the type of cancer, the stage at diagnosis, prognosis, treatment information, length of time since their diagnosis, and whether or not they are in remission. It is likely that the mental health effects of the COVID-19 pandemic vary greatly depending on these factors. Additionally, some of the covariates that were included in the analysis had some limitations in their scope. For example, while our measure of multimorbidity included 17 common chronic health conditions, some conditions were missing from this analysis (eg, arthritis). Fourth, several of the covariates utilized in the current study were dichotomized for this analysis. Although merging categories of categorical variables can potentially improve statistical power and make regression results more robust, it may also result in the loss of nuanced information contained within the original categories. Fine-grained distinctions among groups might be important for a comprehensive understanding of the data. In some situations, combining categories may lead to generalizations in which characteristics of different groups are blurred. Fifth, the CLSA dataset excluded residents who were living in long-term care institutions during the baseline wave of data collection. Those living in long-term care were a particularly vulnerable subset of older adults due to the intensive lockdown restrictions implemented during the pandemic.43 Finally, the CLSA is restricted to respondents who are fluent in English or French, limiting the generalizability of these findings to older immigrants without fluency in one of these languages.
Conclusion
Despite these limitations, this longitudinal study makes a substantial contribution to the literature by examining the prevalence of, and factors associated with, incident and recurrent depression in a large sample of more than 2000 older adults with a history of cancer. We found that approximately 1 in 8 participants with no history of depression experienced depression for the first time during the pandemic, while approximately 1 in 2 participants with a history of depression experienced recurrent depression during the pandemic. These findings highlight the considerable toll of the COVID-19 pandemic on the mental health of older adults with a history of cancer, particularly those who may be at greater risk, such as older women, those with functional limitations, and those who experienced COVID-19 related stressors including increased family conflict and income-related stress. Clinicians and other health professionals should continue to screen their cancer patients for depression and be aware of the long shadow left by the challenges of the pandemic.
Data Sharing Statement
The research reported in this study was conducted using the CLSA Baseline Comprehensive Dataset version 6.0, Baseline Tracking Dataset version 3.7, Follow-up 1 Comprehensive Dataset version 3.0 and Follow-up 1 Tracking Dataset version 2.2, COVID-19 Questionnaire Study Dataset version 1.0 under Application ID 2104024. Under the requirements of our contract, the authors of this study are not permitted to share the data. However, data are available directly from the Canadian Longitudinal Study on Aging (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data by contacting [email protected].
Acknowledgments
This research was made possible using the data collected by the Canadian Longitudinal Study on Aging (CLSA). This research has been conducted using the CLSA Baseline Comprehensive Dataset version 6.0, Baseline Tracking Dataset version 3.7, Follow-up 1 Comprehensive Dataset version 3.0 and Follow-up 1 Tracking Dataset version 2.2, COVID-19 Questionnaire Study Dataset version 1.0 under Application ID 2104024. The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. The opinions expressed in this manuscript are the author’s own and do not reflect the views of the Canadian Longitudinal Study on Aging.
Funding
Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. Funding for support of the CLSA COVID-19 questionnaire-based study is provided by the Juravinski Research Institute, Faculty of Health Sciences, McMaster University, the Provost Fund from McMaster University, the McMaster Institute for Research on Aging, the Public Health Agency of Canada/CIHR grant reference CMO 174125 and the government of Nova Scotia. This research was supported, in part, by the Canadian Institutes of Health Research (CIHR) grant #172862, PI: Fuller-Thomson. Andie MacNeil received funding from the Public Health Agency of Canada to support this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ahmad FB, Anderson RN. The leading causes of death in the US for 2020. JAMA. 2021;325(18):1829–1830. doi:10.1001/jama.2021.5469
2. Ng CG, Boks MP, Zainal NZ, de Wit NJ. The prevalence and pharmacotherapy of depression in cancer patients. J Affect Disord. 2011;131(1–3):1–7. doi:10.1016/j.jad.2010.07.034
3. Krebber AM, Buffart LM, Kleijn G, et al. Prevalence of depression in cancer patients: a meta‐analysis of diagnostic interviews and self‐report instruments. Psychooncology. 2014;23(2):121–130. doi:10.1002/pon.3409
4. Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. BMJ. 2018;361:k1415. doi:10.1136/bmj.k1415
5. Mitchell AJ, Chan M, Bhatti H, et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 2011;12(2):160–174. doi:10.1016/S1470-2045(11)70002-X
6. Smith HR. Depression in cancer patients: pathogenesis, implications and treatment (Review). Oncol Lett. 2015;9(4):1509–1514. doi:10.3892/ol.2015.2944
7. Satin JR, Linden W, Phillips MJ. Depression as a predictor of disease progression and mortality in cancer patients: a meta-analysis. Cancer. 2009;115(22):5349–5361. doi:10.1002/cncr.24561
8. Mausbach BT, Decastro G, Schwab RB, et al. Healthcare use and costs in adult cancer patients with anxiety and depression. Depress Anxiety. 2020;37(9):908–915. doi:10.1002/da.23059
9. Wang X, Wang N, Zhong L, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25(12):3186–3197. doi:10.1038/s41380-020-00865-6
10. Seiler A, Jenewein J. Resilience in cancer patients. Front Psychiatry. 2019;10:208. doi:10.3389/fpsyt.2019.00208
11. Bueno-Notivol J, Gracia-García P, Olaya B, et al. Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. Int J Clin Health Psychol. 2021;21(1):100196. doi:10.1016/j.ijchp.2020.07.007
12. Amaniera I, Bach C, Vachani C, et al. Psychosocial impact of the COVID-19 pandemic on cancer patients, survivors and caregivers. J Psychosoc Oncol. 2021;39(3):485–492. doi:10.1080/07347332.2021.1913780
13. Jafari A, Rezaei-Tavirani M, Karami S, et al. Cancer care management during the COVID-19 pandemic. Risk Manag Healthc Policy. 2020;13:1711–1721. doi:10.2147/RMHP.S261357
14. MacNeil A, Birk S, Villeneuve PJ, et al. Incident and recurrent depression among adults aged 50 years and older during the COVID-19 pandemic: a longitudinal analysis of the Canadian Longitudinal Study on Aging. Int J Environ Res Public Health. 2022;19(22):15032. doi:10.3390/ijerph192215032
15. MacNeil A, Li G, Jiang Y, et al. Incident and recurrent depression among older adults with asthma during the COVID-19 pandemic: findings from the Canadian Longitudinal Study on Aging. Respir Med. 2023;213:107003. doi:10.1016/j.rmed.2022.107003
16. Raina PS, Wolfson C, Kirkland SA, et al. The Canadian Longitudinal Study on Aging (CLSA). Can J Aging. 2009;28(3):221–229. doi:10.1017/S0714980809990055
17. Raina P, Wolfson C, Kirkland S, et al. Cohort profile: the Canadian Longitudinal Study on Aging (CLSA). Int J Epidemiol. 2019;48(6):1752–1753j. doi:10.1093/ije/dyz173
18. Andresen EM, Malmgren JA, Carter WB, Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D. Am J Prev Med. 1994;10(2):77–84. doi:10.1016/S0749-3797(18)30622-6
19. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–221. doi:10.1503/jpn.150205
20. Bom J, Bakx P, Schut F, van Doorslaer E. The impact of informal caregiving for older adults on the health of various types of caregivers: a systematic review. Gerontologist. 2019;59(5):e629–e642. doi:10.1093/geront/gny137
21. Del Río-Lozano M, García-Calvente M, Elizalde-Sagardia B, Maroto-Navarro G. Caregiving and caregiver health 1 year into the COVID-19 pandemic (CUIDAR-SE Study): a gender analysis. Int J Environ Res Public Health. 2022;19(3):1653. doi:10.3390/ijerph19031653
22. Connor J, Madhavan S, Mokashi M, et al. Health risks and outcomes that disproportionately affect women during the Covid-19 pandemic: a review. Social Science Med. 2020;266:113364. doi:10.1016/j.socscimed.2020.113364
23. Kok RM, Reynolds CF 3rd. Management of depression in older adults: a review. JAMA. 2017;317(20):2114–2122. doi:10.1001/jama.2017.5706
24. Kite C, Lagojda L, Clark CCT, et al. Changes in physical activity and sedentary behaviour due to enforced COVID-19-related lockdown and movement restrictions: a protocol for a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(10):5251. doi:10.3390/ijerph18105251
25. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5:363–389. doi:10.1146/annurev.clinpsy.032408.153621
26. Jin Y, Sun T, Zheng P, An J. Mass quarantine and mental health during COVID-19: a meta-analysis. J Affect Disord. 2021;295:1335–1346. doi:10.1016/j.jad.2021.08.067
27. Wang JL, Schmitz N, Dewa CS. Socioeconomic status and the risk of major depression: the Canadian National Population Health Survey. J Epidemiol Community Health. 2010;64(5):447–452. doi:10.1136/jech.2009.090910
28. Bhutta N, Dettling L. Money in the bank? Assessing families’ liquid savings using the survey of consumer finances. Board of Governors of the Federal Reserve System. Available from: https://www.federalreserve.gov/econres/notes/feds-notes/assessing-families-liquid-savings-using-The-survey-of-consumer-finances-20181119.html.
29. Gallagher S, Bennett KM, Roper L. Loneliness and depression in patients with cancer during COVID-19. J Psychosoc Oncol. 2021;39(3):445–451. doi:10.1080/07347332.2020.1853653
30. Miaskowski C, Paul SM, Snowberg K, et al. Loneliness and symptom burden in oncology patients during the COVID-19 pandemic. Cancer. 2021;127(17):3246–3253. doi:10.1002/cncr.33603
31. Li S, Okereke OI, Chang SC, et al. Religious service attendance and lower depression among women-A prospective cohort study. Ann Behav Med. 2016;50(6):876–884. doi:10.1007/s12160-016-9813-9
32. Jim HS, Pustejovsky JE, Park CL, et al. Religion, spirituality, and physical health in cancer patients: a meta-analysis. Cancer. 2015;121(21):3760–3768. doi:10.1002/cncr.29353
33. Puchalski CM. Spirituality in the cancer trajectory. Ann Oncol. 2012;23(Suppl 3):49–55. doi:10.1093/annonc/mds088
34. Johnston EF, Eagle DE, Headley J, Holleman A. Pastoral ministry in unsettled times: a qualitative study of the experiences of clergy during the COVID-19 pandemic. Rev Relig Res. 2022;64(2):375–397. doi:10.1007/s13644-021-00465-y
35. Shapiro E, Levine L, Kay A. A Jerusalem synagogue coping during the coronavirus pandemic: challenges and opportunities. J Relig Health. 2021;60(1):81–98. doi:10.1007/s10943-020-01131-3
36. Wang H, Verdery AM, Margolis R, Smith-Greenaway E. Bereavement from COVID-19, gender, and reports of depression among older adults in Europe. J Gerontol B Psychol Sci Soc Sci. 2022;77(7):e142–e149. doi:10.1093/geronb/gbab132
37. Zhang XR, Huang QM, Wang XM, et al. Prevalence of anxiety and depression symptoms, and association with epidemic-related factors during the epidemic period of COVID-19 among 123,768 workers in China: a large cross-sectional study. J Affect Disord. 2020;277:495–502. doi:10.1016/j.jad.2020.08.041
38. de Girolamo G, Cerveri G, Clerici M, et al. Mental health in the coronavirus disease 2019 emergency-the Italian response. JAMA Psychiatry. 2020;77(9):974–976. doi:10.1001/jamapsychiatry.2020.1276
39. MacNeil A, Findlay B, Bimman R, et al. Exploring the use of virtual funerals during the COVID-19 pandemic: a scoping review. Omega. 2021:302228211045288. doi:10.1177/00302228211045288
40. Diolaiuti F, Marazziti D, Beatino MF, Mucci F, Pozza A. Impact and consequences of COVID-19 pandemic on complicated grief and persistent complex bereavement disorder. Psychiatry Res. 2021;300:113916. doi:10.1016/j.psychres.2021.113916
41. Boelen PA, Smid GE. Disturbed grief: prolonged grief disorder and persistent complex bereavement disorder. BMJ. 2017;357:j2017. doi:10.1136/bmj.j2016
42. Weiss RB, Aderka IM, Lee J, et al. A comparison of three brief depression measures in an acute psychiatric population: CES-D-10, QIDS-SR, and DASS-21-DEP. J Psychopathol Behav Assess. 2021;37(2):217–230. doi:10.1007/s10862-014-9461-y
43. Bethell J, Aelick K, Babineau J, et al. Social connection in long-term care homes: a scoping review of published research on the mental health impacts and potential strategies during COVID-19. J Am Med Dir Assoc. 2021;22(2):228–237.e25. doi:10.1016/j.jamda.2020.11.025
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.