Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Pain Physicians’ Attitudes and Experiences Regarding Clinical Pharmacy Services in China: A National Cross-Sectional Survey
Authors Qin W ![]() , Yuan S, Zhao L, Liu Y, Xu L, Zhang Y, Liu L, Fan B
, Yuan S, Zhao L, Liu Y, Xu L, Zhang Y, Liu L, Fan B
Received 10 November 2022
Accepted for publication 23 December 2022
Published 10 January 2023 Volume 2023:16 Pages 21—29
DOI https://doi.org/10.2147/JMDH.S397039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wangjun Qin,1 Siyu Yuan,2 Li Zhao,1 Ying Liu,1 Liyuan Xu,3 Yi Zhang,3 Lihong Liu,1 Bifa Fan3
1Department of Pharmacy, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 2Department of Pharmacy, Siping Central Hospital, Siping, Jilin Province, People’s Republic of China; 3Department of Pain Management, China-Japan Friendship Hospital, Beijing, People’s Republic of China
Correspondence: Lihong Liu; Bifa Fan, China-Japan Friendship Hospital, 2 Yinghua Road, Heping District, Beijing, 100029, People’s Republic of China, Tel +860184205959, Fax +860184205559, Email [email protected]; [email protected]
Purpose: Pharmacists are key members of the pain management interdisciplinary team in many developed countries. However, the implementation of clinical pharmacy services in pain management is impeded by the imbalance between the pain physicians and clinical pharmacists specializing in pain management in China. The purpose of this study was to elucidate the perceptions, expectations and current experience of Chinese pain physicians regarding clinical pharmacy services.
Patients and Methods: An anonymous, self-administered questionnaire was designed according to previously published studies with minor modifications and distributed online to 1100 pain physicians selected randomly in hospitals across all 31 provinces of mainland China in 2021. Data were analyzed using descriptive and inferential statistics.
Results: A total of 1071 valid questionnaires were included for analysis. The pain physicians were from all 31 provinces of mainland China and most of them were from tertiary hospitals holding an undergraduate degree. Among listed kinds of clinical pharmacy services, pain physicians were less comfortable with pharmacists treating minor illnesses (p < 0.001). Pain physicians’ experiences with clinical pharmacy services were far less than their expectations (p < 0.001), which is in line with the results that most of pain physicians (65.9%) interacted with pharmacists at a frequency of less than once a week. Significant differences in the experiences were found among ages (p < 0.01) and among years of work experience (p < 0.05) of pain physicians. Pain physicians’ expectations of pharmacists were positively correlated with their experiences with clinical pharmacy services (p < 0.001).
Conclusion: Pain physicians in China had positive perceptions and high expectations, but relatively low experiences regarding clinical pharmacy services. Expanding clinical pharmacist pain management credentialing and increasing pain physicians’ exposure to clinical pharmacy services are favourable to support the interdisciplinary collaboration in pain management in China.
Keywords: clinical pharmacy services, pain management, interdisciplinary collaboration, professional competence, primary health care
Introduction
The profession of hospital pharmacy in the health care system is gradually changing from medicine dispensing services to clinical pharmacy services.1,2 The term “clinical pharmacy” was first used in 1953, and since then pharmacists were encouraged to provide patient-centered pharmaceutical care to promote the rational use of medicines, which has been demonstrated to have a positive impact on the patients’ treatment outcome.3–5 Nowadays, clinical pharmacists are important members of the multi-disciplinary team in patient care in the United States and many other developed countries, but there are still many challenges in the paradigm shift in the profession of hospital pharmacy in most developing countries.6–11
The Chinese Ministry of Health issued a series of documentations regarding clinical pharmacists to begin the clinical pharmacy services in China in 2005.12,13 By 2021, there are more than 17,000 credentialed clinical pharmacists playing an important role in the Chinese health care and the majority of them are specializing in anti-infective and anti-tumour therapies. Chinese clinical pharmacists participate in patients’ treatment by performing drug selection, dose adjustment and adverse drug reaction monitoring etc., in ways such as consultation and prescription evaluation.14 Clinical pharmacist-led interventions were demonstrated to be helpful in reducing the length of stay and readmission rate, improving the treatment outcome and compliance rate, and decreasing antibiotic use density and the cost of medicines in China.12,15,16 However, the impact of clinical pharmacist-led interventions varied among different studies, depending mainly on the collaboration between clinical pharmacists and physicians.17
The implementation of clinical pharmacy services in pain management is impeded by the imbalance between the pain physicians and clinical pharmacists specializing in pain management in China. The growth of pain physicians is exponential in China as secondary and tertiary hospitals have been required to set up the department of pain management since 2007. There are now more than 20,000 pain physicians in China according to data from the Pain Physician Branch of Chinese Medical Doctor Association (PPBCMDA). However, the pharmacist credentialing in pain management started in 2017 and there were only 190 clinical pharmacists specializing in pain management in 2021 in China. Hence, most of pain physicians might have little experience in clinical pharmacy services and are not aware of what clinical pharmacists can do in pain management.
Furthermore, clinical pharmacists are key members of the pain management multidisciplinary team and play a pivotal role in the management of patients with both acute and chronic pain with various strategies acquired in the process of pain management credentialing in the United States.10,18,19 However, clinical pharmacists specializing in pain management provide clinical pharmacy services at a small scale in China.5,20 Thus, it is necessary for clinical pharmacists to learn pain physicians’ perceptions and expectations regarding clinical pharmacy services.
The purpose of this study was to elucidate the perceptions, expectations and current experiences of Chinese pain physicians regarding clinical pharmacy services in pain management. The results could be of help to enhance strategies in promoting collaborations between pain physicians and clinical pharmacists and then to optimize pain management in China.
Materials and Methods
A national cross-sectional survey was carried out to assess pain physicians’ perceptions, expectations and current experiences regarding clinical pharmacy services in China from July to December 2021. This study was approved by the ethical committee of China–Japan Friendship Hospital (Registration number: 2019–182-K123). Verbal informed consent was obtained from all individual participants included in the study. The verbal informed consent procedure was approved by the ethical committee of China–Japan Friendship Hospital as it was an online survey and collected only non-identifiable information. Participants were asked for informed consent and could only access the questionnaire when informed consent was given.
Questionnaire Development
The self-administrated questionnaire used in this study was designed according to previously published studies with minor modifications based on the legislation and pharmacy practices in China (Supplementary Figure 1).21,22 There were 34 questions classified into four sections: (1) demographic profile, professional background and the frequency and intention of interacting with pharmacists; (2) the perceptions about clinical pharmacy services; (3) the expectations of clinical pharmacy services; and (4) the experiences with clinical pharmacy services. Pain physicians were asked whether they are comfortable with each statement about clinical pharmacy services in section 2. Their expectations and experiences regarding clinical pharmacy services were measured using a three-point scale (disagree, neutral or agree) in section 3 and 4. Each question in section 3 and 4 was scored as −1, 0 or 1 corresponding to the option disagree, neutral or agree, and the sum scores of questions in section 3 and section 4 of one questionnaire were used as the pain physician’s expectation value and experience value respectively. There were eight questions in both section 3 and section 4. Thus, the maximum scores of expectation value and experience value were 8, while the minimum scores were −8. The content validity of the questionnaire was evaluated by ten experts on clinical pharmacy using a four-point Likert scale. The content validity index (CVI) for each item (I-CVI) ranged from 0.80 to 1.0. The universal agreement scale-level CVI (S-CVI/UA) and the average scale-level CVI (S-CVI/Ave) were 0.63 and 0.94, respectively. A pilot test was conducted among 15 pain physicians at the China-Japan Friendship Hospital to ensure the charity of the items and estimate the time required to complete the questionnaire. The results of the pilot test were used to test internal reliability of the questionnaire (Cronbach’s alpha=0.90).
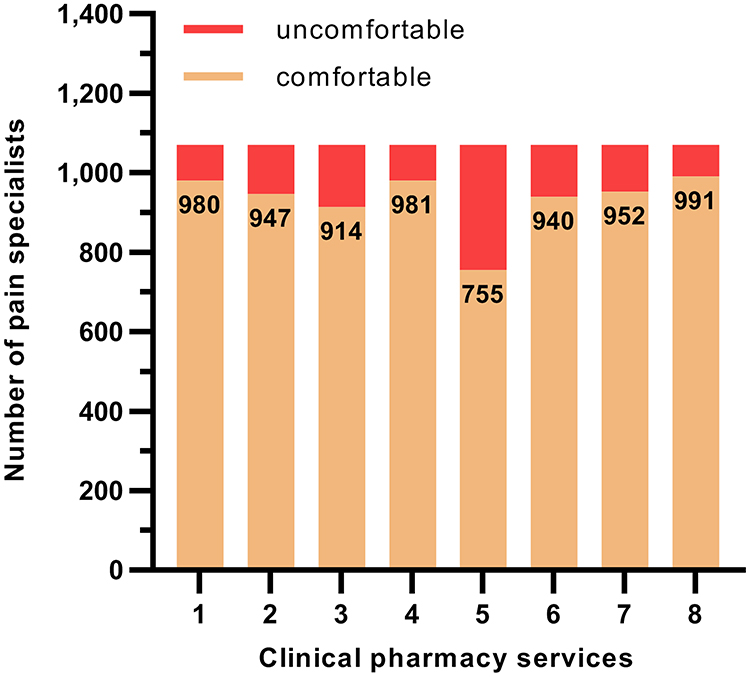 |
Figure 1 Pain physicians’ perceptions about specific kinds of clinical pharmacy services. A significant difference was observed among pain physicians’ attitudes towards specific kinds of clinical pharmacy services. Almost one-third (29.5%) of pain physicians were uncomfortable with pharmacists treating minor illnesses. 1: providing patient education, 2: suggesting use of non-prescription medications, 3: suggesting use of prescription medications to patients, 4: suggesting use of prescription medications to physicians, 5: treating minor illnesses, 6: designing and monitoring therapeutic regimes, 7: monitoring outcomes of therapeutic regimes, 8: detecting and preventing prescription errors. |
Sampling and Data Collection
An automated online calculator (RAOSOFT) was used to estimate the sample size in this survey. A minimum sample size of 377 was recommended assuming a 5% alpha error rate and 95% confidence level. In order to make the survey more accurate and more reliable as well as to reduce the regional bias, 1100 pain physicians were randomly selected from the member list of PPBCMDA via a simple random sampling without replacement by using the rand function in Excel to complete the questionnaires. The online links to the questionnaires, along with an explanation of the background and purpose of the study, were sent to the selected pain physicians via the WeChat platform, which has become an important social network in China. All the selected pain physicians were contacted and asked to complete the questions via the WeChat platform by a staff in PPBCMDA. A total of 1081 questionnaires were collected, and ten questionnaires were identified to be invalid and excluded for a short response duration (less than 180 seconds). Thus, a total of 1071 valid questionnaires were received in this survey.
Data Analysis
Data were computed and analyzed using SPSS 22 (IBM Corp., Armonk, United States). The Chi-square test was used to determine the relationship between perceptions and demographic profiles. The differences in expectation values and experience values among demographic profiles were analyzed by one-way analysis of variance (ANOVA) and post hoc Tukey’s test. The difference between expectation values and experience values was compared by the Mann–Whitney U-test. Bivariate correlation (Pearson) was used to test the relationship between expectation values and experience values. Statistical significance was determined at p < 0.05.
Results
Pain Physicians’ Characteristics
Out of the 1100 questionnaires distributed, 1071 valid questionnaires were used in the analysis, accounting for a response rate of 97.36%. The pain physicians surveyed covered all the 31 provinces of mainland China, mainly from Anhui (13.2%), Henan (8.8%) and Hunan (8.5%). Most of them were from tertiary (66.9%) and general (80.5%) hospitals. More than three quarters of pain physicians were man (75.2%) and around half (45.0%) fell within the age range of 36–45 years. The vast majority (69.2%) held an undergraduate degree as their highest level of education and worked in the department of pain management (57.1%), whilst almost a quarter (26.6%) worked in the department of anesthesiology. Less than a third had become pain physicians for 6–10 years (30.9%), and almost equal proportion of pain physicians worked for less than 5 years (27.8%) and 11–20 years (27.2%). As judged by job titles, more than a third of pain physicians were classed as vice chief physician (37.5%) and attending physician (34.5%). Table 1 shows more details about the demographics and other characteristics of the pain physicians.
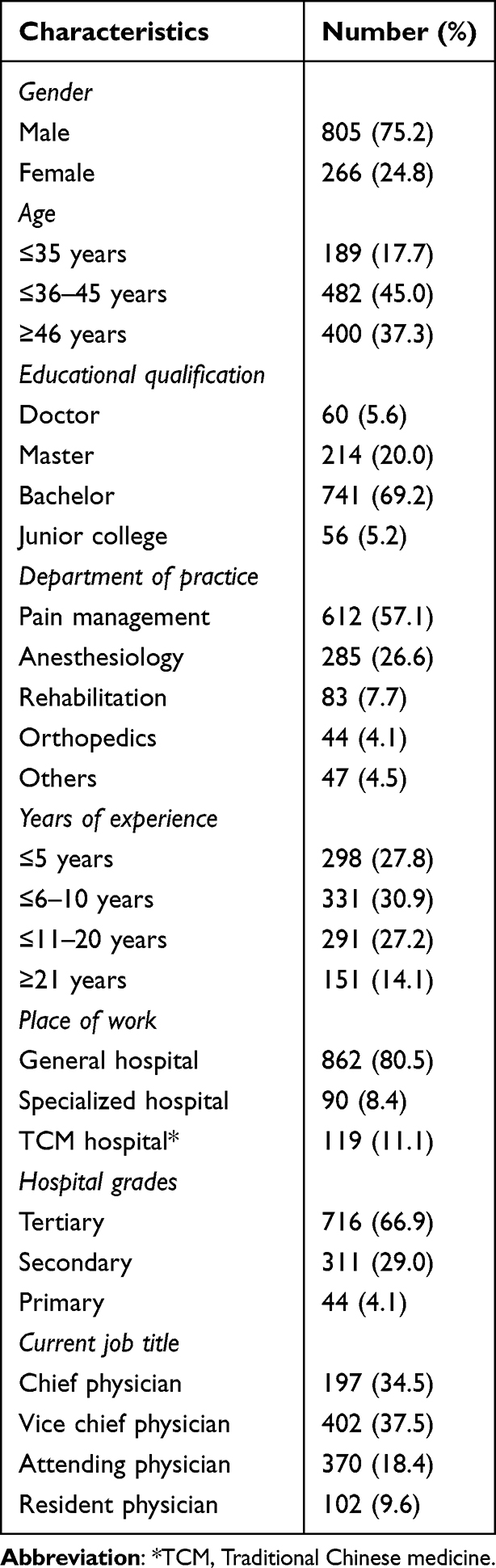 |
Table 1 Demographic Information |
Interactions Between Pain Physicians and Pharmacists
As shown in Table 2, about two-thirds (65.9%) of pain physicians stated that they interacted with pharmacists at a frequency of less than once a week. More than a quarter (28.7%) interacted with pharmacists at least once a week, while only 5.4% of pain physicians reported a frequency of once daily or more when referring to the interactions with pharmacists. The majority of the reasons for the interactions were drug alternatives (43.0%), drug availability (42.3%), drug interactions (40.0%) and side effects (35.7%).
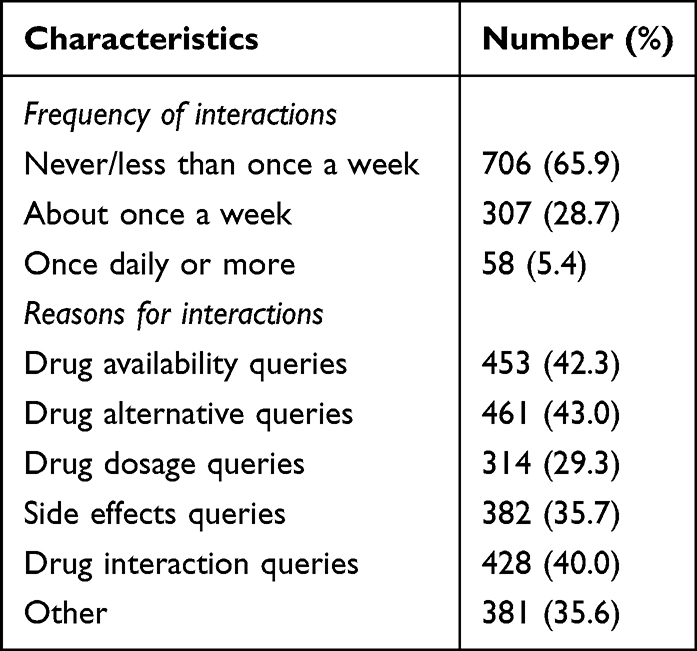 |
Table 2 Frequency of Interactions and Their Reasons |
Pain Physicians’ Perceptions About Clinical Pharmacy Services
We investigated the pain physicians’ perceptions about pharmacists by asking their attitudes towards clinical pharmacy services. As shown in Figure 1, there was a significant difference among pain physicians’ perceptions about specific kinds of clinical pharmacy services (χ2=336.1, p<0.001). The majority of pain physicians were comfortable with pharmacists detecting and preventing prescription errors (92.5%), suggesting use of prescription medications to physicians (91.6%), and providing patient education (91.5%), while almost one-third (29.5%) of pain physicians were uncomfortable with pharmacists treating minor illnesses.
Pain Physicians’ Expectations on Clinical Pharmacy Services
Pain physicians had high expectations on clinical pharmacy services in the pain management. As shown in Table 3, except for the statement expecting pharmacists to take personal responsibility for resolving any drug-related problems with an agree rate of 64.9%, more than 80% of pain physicians expected pharmacists to provide patient-centered pharmaceutical care to promote rational use of medicines, such as monitoring patients’ response to drug therapy and any drug-related problem (89.8%), educating patients about the safe and appropriate use of their medications (88.6%) and knowing the specific indication of each drug prescribed (88.5%).
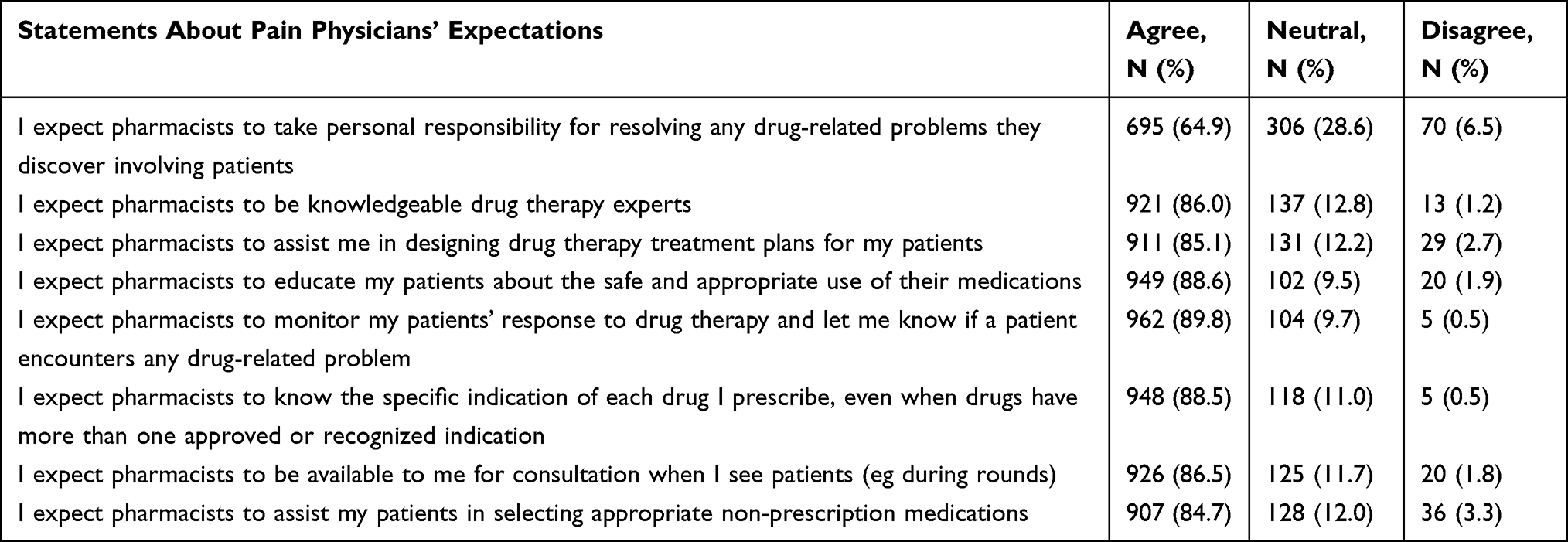 |
Table 3 Pain Physicians’ Expectations of Pharmacists |
There is no significant association between expectation values and demographic profiles of pain physicians. Pain physicians with a junior college degree (7.1±1.4) showed a trend to have higher expectation values than those with a bachelor degree (6.6±2.2), a master degree (6.4±2.4) or a doctor degree (6.2±2.3), but it did not produce a statistical significance (F=2.6, p=0.053).
Pain Physicians’ Experiences with Clinical Pharmacy Services
The actual experiences of pain physicians with pharmacists are shown in Table 4. The majority of pain physicians (70.8%) stated that pharmacists routinely informed them if pharmacists discover problems with the prescriptions. Nearly half of pain physicians agreed that pharmacists frequently asked them to clarify the pharmacotherapy objectives they have in mind (58.5%) and informed them about more cost-effective alternatives (58.2%).
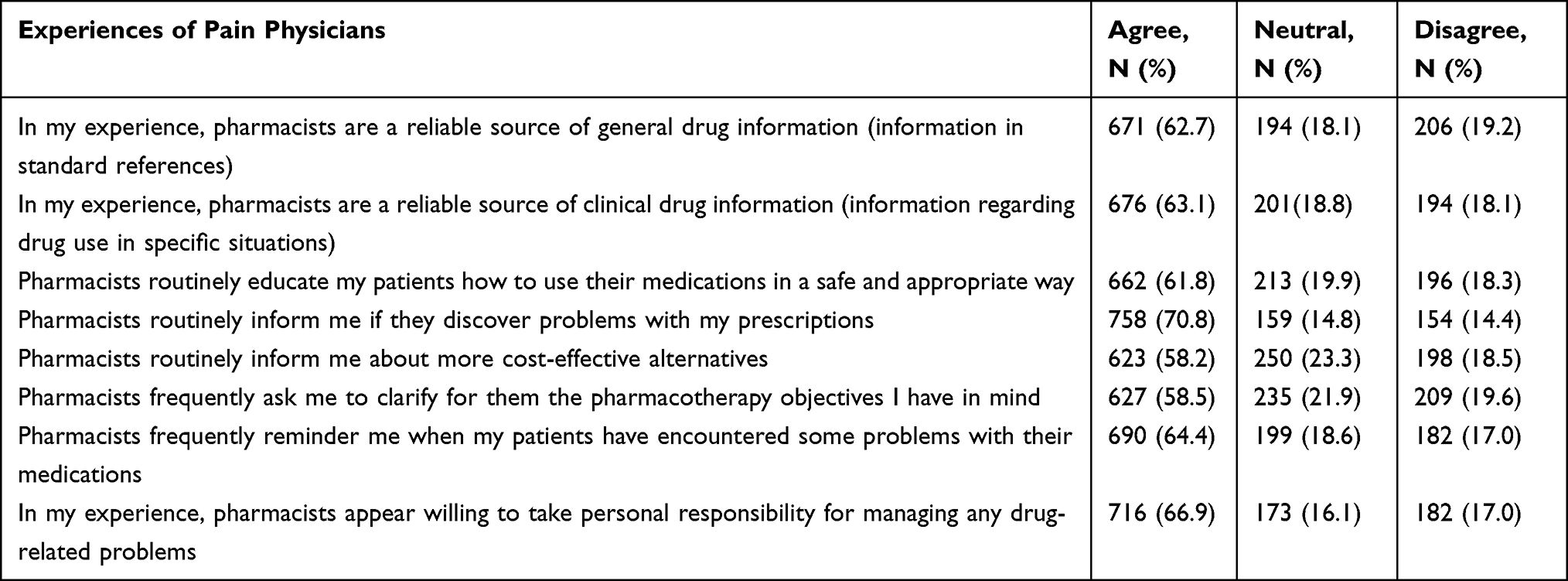 |
Table 4 Pain Physicians’ Experiences with Pharmacists |
There are significant differences in experience values among ages (F=5.2, p=0.0054) and among years of work experience (F=2.8, p=0.040) of pain physicians. Pain physicians between the ages of 36 and 45 years were more experienced in interacting with pharmacists than those above 46 years (p=0.0036), and pain physicians with work experience between 11 and 20 years had more experience values than those with work experience under 5 years (p=0.027).
Imbalance Between Expectations and Experiences Regarding Clinical Pharmacy Services
A big gap was observed between pain physicians’ expectations and experiences regarding clinical pharmacy services, as the Mann–Whitney U-test showed that the experience values were significantly lower than the expectation values (Z=−2.0, p<0.001) (Figure 2A). Interestingly, the correlation between experience values and the expectation values was significantly positive in Pearson’s analysis (r=0.23, p<0.001, n=1071; Figure 2B).
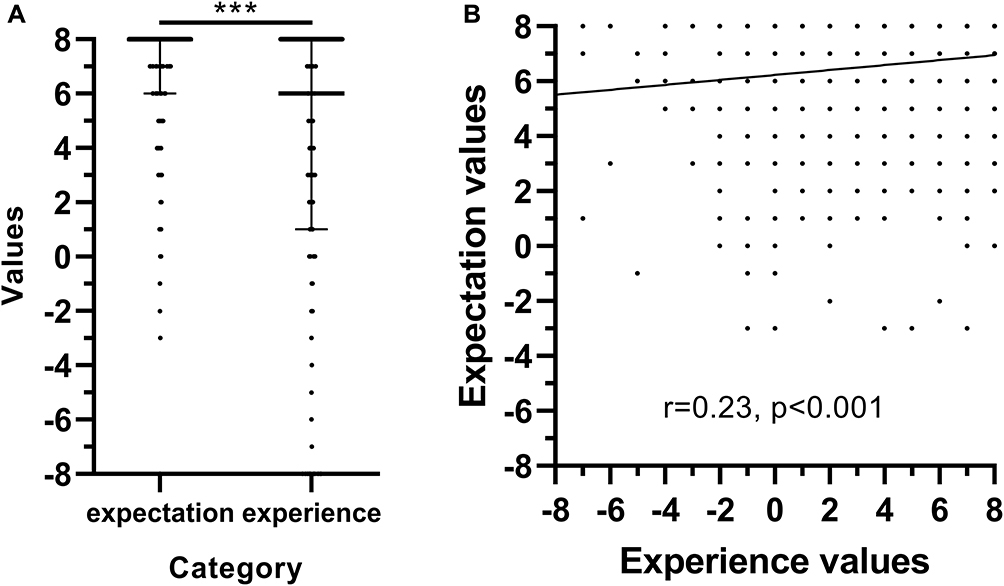 |
Figure 2 Relationship between pain physicians’ expectations and experiences regarding clinical pharmacy services. The experience values were significantly lower than the expectation values (A) and there was a direct correlation between expectation values and experience values (B). Data are expressed as median (75% interquartile range). ***p < 0.001 vs expectation values. |
Discussion
This national cross-sectional survey assessed pain physicians’ perceptions, expectations and experiences regarding clinical pharmacy services in China. The results showed that pain physicians had positive perceptions and high expectations, but relatively low experiences regarding clinical pharmacy services in China. The lack of experience might be attributed to the imbalance between pain physicians and clinical pharmacists specializing in pain management. Thus, expanding clinical pharmacist pain management credentialing could make up for pain physicians’ experiences, which is helpful in raising their expectations and further increasing interactions between pain physicians and pharmacists.
Pain physicians in China stated positive responses on the perceptions towards clinical pharmacy services, which suggests they have been aware of the complementary effect of clinical pharmacy services in ensuring patients’ pain control and treatment safety.23 However, many pain physicians were uncomfortable with pharmacists prescribing medication to treat minor illnesses independently. The situations are similar among physicians from other departments in China and other developing countries.13,21–23 It is mainly because pharmacists do not have prescribing authority according to the Chinese legislation. Pain physicians may also question pharmacists’ competency in such activities.13 In many developed countries, pharmacists are key members of the pain management interdisciplinary team and could be licensed to prescribe and revise medications under a collaborative practice agreement with physicians.10,18,24,25 This model has produced positive impacts in both financial and clinical aspects, and could be adapted in China and other developing countries.26
Chinese pain physicians had high expectations on clinical pharmacy services such as providing patient education, monitoring treatment responses and adverse effects, and being available for consultation, indicating a promising new role for pharmacists in China.27 It is notable that pain physicians were somewhat in doubt about the statement expecting pharmacists to take personal responsibility for resolving any drug-related problems. It reflects the lack of collaboration with pharmacists and confidence in pharmacists’ skills, which could be improved by more training programs and more exposure to pain physicians.19,28 Although there is no association between demographic profiles of pain physicians and expectation values, pain physicians with a junior college degree seemed to have higher expectations on clinical pharmacy services than others. In China, a junior college degree could be obtained by completing a 2–3 years of courses in junior college after graduating from senior high school.29 The higher expectation values of pain physicians with a junior college degree suggest their shortage of knowledge in drug therapy for pain management and pharmacists may give priority to this group in the beginning of clinical pharmacy service practices.
Pain physicians’ experiences with pharmacists were far less than their expectations. Of all statements, pain physicians had less experiences regarding pharmacists frequently asking them to clarify the pharmacotherapy objectives and informing them about more cost-effective alternatives, which may be explained by the lack of confidence in pharmacists’ selves and the shortage of clinical pharmacists specializing in pain management, resulting in the rare interaction on confirming the pharmacotherapy objectives and proposing cost-effective alternatives.30 Our results showed pain physicians between 36 and 45 years old or with work experience between 11 and 20 years had more experiences in interacting with pharmacists than others. It is reasonable to infer that they are from the same group as physicians usually start their careers upon graduation at about 25 years old in China. The middle-aged pain physicians may be more open and favourable to receive clinical pharmacy services. We are pleased to notice that the pain physicians’ expectations of clinical pharmacy services were positively correlated with their experiences with pharmacists, indicating a good performance of pharmacists and a favourable impression on pain physicians.13
There are some limitations in the present study. The present results only represent the views of pain physicians in China. Therefore, the applicability of our findings in other countries is limited. Also, pharmacists’ attitudes towards clinical pharmacy services in pain management were not included and should be investigated in further studies to provide a more comprehensive view. The present study was a survey-based research with only close-ended questions, while some open-ended questions may be helpful to obtain more information about pain physicians’ views. Moreover, more attention should be paid to interdisciplinary collaborations between nurses and clinical pharmacists.31 Regional bias would not be a big concern in this study as the pain physicians surveyed covered all the 31 provinces of mainland China.
Conclusion
Pain physicians in China were comfortable with most kinds of clinical pharmacy services except prescribing medication to treat minor illnesses independently. Pain physicians also had high expectations on clinical pharmacy services, which did not match their actual experiences. Our results suggest that expanding clinical pharmacist pain management credentialing and increasing pain physicians’ exposure to clinical pharmacy services are favourable to the improvement of pain physicians’ expectations and will further support the interdisciplinary collaboration in pain management in China.
Acknowledgments
We appreciate contributions of all the pain physicians in the study.
Funding
This work was supported by the National High Level Hospital Clinical Research Funding (2022-NHLHCRF-YSPY-02-05), the Capital's Funds for Health Improvement and Research (CFH 2020-1-2031), the Fundamental Research Funds for the Central Universities (3332020075) and the National Key Clinical Specialty Discipline Construction Program of China (Pain Management).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hepler CD. Clinical pharmacy, pharmaceutical care, and the quality of drug therapy. Pharmacotherapy. 2004;24(11):1491–1498. doi:10.1592/phco.24.16.1491.50950
2. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–543.
3. Elmaaty MA, Elberry AA, Hussein RR, Khalil DM, Khalifa AE. Applicability of American College of Clinical Pharmacy (ACCP) competencies to clinical pharmacy practice in Egypt. Pharm Pract (Granada). 2020;18(3):1951. doi:10.18549/PharmPract.2020.3.1951
4. Olea AJ, Grochowski J, Luetkemeyer AF, Robb V, Saberi P. Role of a clinical pharmacist as part of a multidisciplinary care team in the treatment of HCV in patients living with HIV/HCV coinfection. Integr Pharm Res Pract. 2018;7:105–111. doi:10.2147/IPRP.S169282
5. Liu J, Wang C, Chen X, et al. Evaluation of pharmacist interventions as part of a multidisciplinary cancer pain management team in a Chinese academic medical center. J Am Pharm Assoc (2003). 2020;60(1):76–80. doi:10.1016/j.japh.2019.09.005
6. Alshakka M, Mohamed IM, Bahattab A, Badulla W, Shankar PR. An insight into the pharmaceutical sector in Yemen during conflict: challenges and recommendations. Med Confl Surviv. 2020;36(3):232–248. doi:10.1080/13623699.2020.1794287
7. Armor BL, Britton ML, Dennis VC, Letassy NA. A review of pharmacist contributions to diabetes care in the United States. J Pharm Pract. 2010;23(3):250–264. doi:10.1177/0897190009336668
8. Dosea AS, Brito GC, Santos L, et al. Establishment, Implementation, and Consolidation of Clinical Pharmacy Services in Community Pharmacies: perceptions of a Group of Pharmacists. Qual Health Res. 2017;27(3):363–373. doi:10.1177/1049732315614294
9. Rezahi S, Mathers A, Benny GN, Mak KC, Dolovich L. Pharmacist contributions to patient care and medical conditions present among recipients of Ontario primary care team pharmacist-led medication reviews: a qualitative analysis. Int J Pharm Pract. 2021;29(4):385–388. doi:10.1093/ijpp/riab023
10. Semerjian M, Durham MJ, Mirzaian E, Lou M, Richeimer SH. Clinical Pharmacy Services in a Multidisciplinary Specialty Pain Clinic. Pain Pract. 2019;19(3):303–309. doi:10.1111/papr.12745
11. Strand MA, Scott DM, Undem T, et al. Pharmacist contributions to the ten essential services of public health in three National Association of Boards of Pharmacy regions. J Am Pharm Assoc (2003). 2017;57(3):395–401. doi:10.1016/j.japh.2017.02.021
12. Yi ZM, Sun SS, Li XX, Lu M, Zhai SD. An evaluation of clinical pharmacist service on a neurology care unit. Int J Clin Pharm. 2016;38(1):30–33. doi:10.1007/s11096-015-0224-y
13. Li X, Huo H, Kong W, Li F, Wang J. Physicians’ perceptions and attitudes toward clinical pharmacy services in urban general hospitals in China. Int J Clin Pharm. 2014;36(2):443–450. doi:10.1007/s11096-014-9919-8
14. Wang Y, Dai Y, Yang J, et al. A survey of Chinese pharmacists participating in anti-infective therapy and its related information technology support. J Clin Pharm Ther. 2020;45(4):707–714. doi:10.1111/jcpt.13152
15. Zhou Y, Ma LY, Zhao X, et al. Impact of pharmacist intervention on antibiotic use and prophylactic antibiotic use in urology clean operations. J Clin Pharm Ther. 2015;40(4):404–408. doi:10.1111/jcpt.12275
16. Wang J, Dong M, Lu Y, et al. Impact of pharmacist interventions on rational prophylactic antibiotic use and cost saving in elective cesarean section. Int J Clin Pharmacol Ther. 2015;53(8):605–615. doi:10.5414/CP202334
17. Qin SB, Zhang XY, Fu Y, et al. The impact of the clinical pharmacist-led interventions in China: a systematic review and Meta-Analysis. Int J Clin Pharm. 2020;42(2):366–377. doi:10.1007/s11096-020-00972-y
18. Bryan K, Menighan TE. What Does Good Pharmacist-Physician Pain Management Collaboration Look Like? AMA J Ethics. 2020;22(1):E675–80. doi:10.1001/amajethics.2020.675
19. Juba KM. Pharmacist credentialing in pain management and palliative care. J Pharm Pract. 2012;25(5):517–520. doi:10.1177/0897190012453907
20. Chen J, Lu XY, Wang WJ, et al. Impact of a clinical pharmacist-led guidance team on cancer pain therapy in China: a prospective multicenter cohort study. J Pain Symptom Manage. 2014;48(4):500–509. doi:10.1016/j.jpainsymman.2013.10.015
21. Matowe L, Abahussain EA, Al-Saffar N, et al. Physicians’ perceptions and expectations of pharmacists’ professional duties in government hospitals in Kuwait. Med Princ Pract. 2006;15(3):185–189. doi:10.1159/000092179
22. Khan N, McGarry K, Naqvi AA, Holden K. Doctors’ perceptions, expectations and experience regarding the role of pharmacist in hospital settings of Pakistan. Int J Clin Pharm. 2020;42(2):549–566. doi:10.1007/s11096-020-00991-9
23. Kabba JA, James PB, Hanson C, et al. Sierra Leonean doctors’ perceptions and expectations of the role of pharmacists in hospitals: a national cross-sectional survey. Int J Clin Pharm. 2020;42(5):1335–1343. doi:10.1007/s11096-020-01096-z
24. Boren LL, Locke AM, Friedman AS, Blackmore CC, Woolf R. Team-Based Medicine: incorporating a Clinical Pharmacist into Pain and Opioid Practice Management. PM R. 2019;11(11):1170–1177. doi:10.1002/pmrj.12127
25. Bourne RS, Baqir W, Onatade R. Pharmacist independent prescribing in secondary care: opportunities and challenges. Int J Clin Pharm. 2016;38(1):1–06. doi:10.1007/s11096-015-0226-9
26. Richter C. Implementation of a Clinical Pharmacist Service in the Hospice Setting: financial and Clinical Impacts. J Pain Palliat Care Pharmacother. 2018;32(4):256–259. doi:10.1080/15360288.2019.1615026
27. Bawazir SA. WHO Expert Committee on Specifications for Pharmaceutical Preparations. World Health Organ Tech Rep Ser. 2016;1(996):1–358.
28. Rule AM. American society of health-system pharmacists’ pain management network. J Pain Palliat Care Pharmacother. 2004;18(3):59–62. doi:10.1080/J354v18n03_06
29. Hou J, Wang Z, Liu X, et al. Public health education at China’s higher education institutions: a time-series analysis from 1998 to 2012. Bmc Public Health. 2018;18(1):679. doi:10.1186/s12889-018-5605-4
30. Alipour F, Peiravian F, Mehralian G. Perceptions, experiences and expectations of physicians regarding the role of pharmacists in low-income and middle-income countries: the case of Tehran hospital settings. BMJ Open. 2018;8(2):e19237. doi:10.1136/bmjopen-2017-019237
31. Rababa M, Al-Sabbah S, Hayajneh AA. Nurses’ Perceived Barriers to and Facilitators of Pain Assessment and Management in Critical Care Patients: a Systematic Review. J Pain Res. 2021;14:3475–3491. doi:10.2147/JPR.S332423
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.