Back to Journals » Journal of Pain Research » Volume 19
Pain Catastrophizing: Mechanisms and Clinical Implications
Authors Zhang Q, Ma Y, Dai Z, Wang Q, Yin W, Liu S, Li J
Received 30 December 2025
Accepted for publication 16 April 2026
Published 18 May 2026 Volume 2026:19 592713
DOI https://doi.org/10.2147/JPR.S592713
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rocío de la Vega
Qi Zhang,* Yuexiang Ma,* Zheng Dai, Qianmei Wang, Wen Yin, Shanshou Liu, Junjie Li
Department of Emergency, Xijing Hospital, The Fourth Military Medical University, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junjie Li, Department of Emergency, Xijing Hospital, The Fourth Military Medical University, No. 127 Changlexi Road, Xincheng District, Xi’an, 710032, People’s Republic of China, Email [email protected] Shanshou Liu, Department of Emergency, Xijing Hospital, The Fourth Military Medical University, No. 127 Changlexi Road, Xincheng District, Xi’an, 710032, People’s Republic of China, Email [email protected]
Objective: This study aims to summarize current perspectives on the underlying mechanisms, conceptual frameworks, and potential clinical implications of pain catastrophizing (PC).
Methods: A narrative review approach was employed.
Results: Existing studies suggest that PC may be associated with functional activity in several brain regions, including the anterior cingulate cortex, amygdala, and prefrontal cortex, which are involved in pain perception and emotional regulation. From a psychosocial perspective, catastrophizing has been linked to psychological distress, social support, and behavioral responses to pain. Various interventions, including psychological therapies, pain neuroscience education, exercise-based approaches, and complementary therapies have been explored as potential strategies for addressing PC. However, findings across studies remain heterogeneous.
Discussion: This study integrates current evidence on neurobiological mechanisms and psychosocial models related to PC and discusses their potential clinical implications. By summarizing existing findings and highlighting areas of uncertainty, this work aims to provide a more comprehensive understanding of the multidimensional nature of PC and may inform future research and clinical approaches in chronic pain management.
Keywords: pain, pain catastrophizing, neurobiological mechanisms, psychosocial factors, chronic pain
Introduction
Psychosocial factors have increasingly been recognized as significant moderators and essential elements of chronic pain.1 Among various psychological factors, catastrophism has received considerable empirical attention.1,2 Catastrophizing is generally regarded as a maladaptive cognitive pattern in response to stress, both within the chronic pain literature and in the broader psychological context, and is characterized by diminished confidence and a reduced sense of control.3–5 It is commonly observed among individuals with anxiety,6,7 depressive disorders,8 and chronic pain conditions.9
Pain catastrophizing (PC) is conceptualized as a maladaptive cognitive-emotional response characterized by an exaggerated negative orientation toward actual or anticipated pain experiences, encompassing three core dimensions: rumination, magnification, and perceived helplessness.10 Available evidence suggests that PC may account for a substantial proportion of the variance in the transition from acute to chronic pain, indicating its potential relevance in pain chronification.11 PC has been associated with higher levels of perceived pain, longer hospital stays, and an increased risk of opioid misuse in patients undergoing total joint arthroplasty.12,13
Previous studies have also reported associations between PC and a range of adverse outcomes, including functional disability, mood disorders, and substance use in patients with chronic musculoskeletal conditions.14–19 In addition, PC has been linked to poorer treatment adherence and unfavorable clinical outcomes.20–22 Together, these findings suggest that PC may contribute to substantial individual and societal burden of chronic pain, potentially increasing the demand for analgesics and antidepressants and contributing to rising healthcare costs.23,24
Current evidence suggests that PC may involve amplification of distress and pain-facilitating neural processes.25 Individuals with higher levels of catastrophizing tend to show greater attention to pain signals and heightened emotional responses.26 While increased pain awareness may facilitate early recognition of potential tissue damage in some contexts, excessive attention to pain-related cues may also contribute to maladaptive pain experiences.27 Additionally, PC has been associated with alterations in neural mechanisms related to pain processing, attention, emotion, physical activity, and reduced top-down pain inhibition.28,29 However, the available evidence remains heterogeneous, and the underlying pathways are not yet fully understood.
Nevertheless, relatively few studies have systematically summarized PC from underlying mechanisms to clinical management. Therefore, integrating findings from functional neuroimaging with anatomical, physiological, and psychosocial investigations may help clarify the mechanisms of PC and its potential clinical implications. In this review, we proposed a framework for interpreting the influence of PC on clinical outcomes (Figure 1). Specifically, this review examines the mechanistic underpinnings, conceptual and psychosocial frameworks, and therapeutic approaches related to PC, with the aim of providing a clearer overview of current evidence and informing future research and clinical practice.
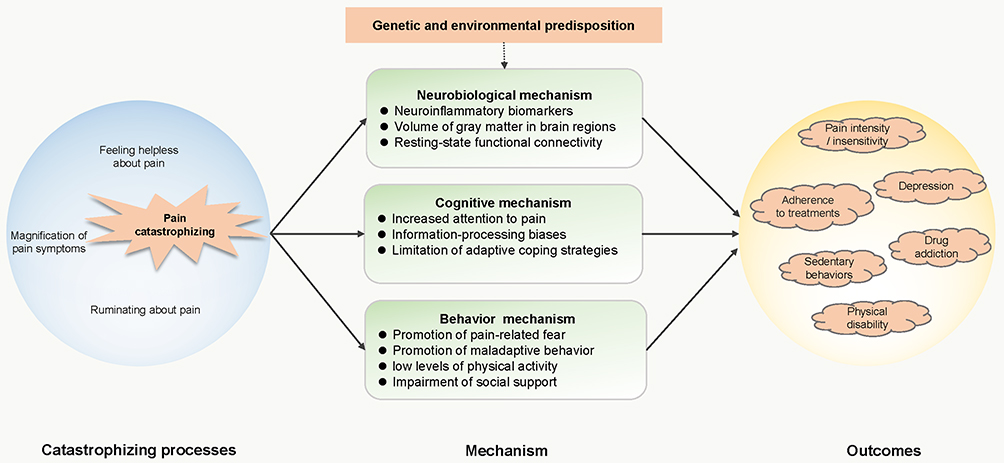 |
Figure 1 Conceptual framework of pain catastrophizing and its impact on clinical outcomes. The schematic illustrates the self-perpetuating cycle of pain catastrophizing (magnification, rumination, and helplessness) and its influence on adverse clinical prognosis. Underpinned by genetic and environmental predispositions, this cognitive-emotional process may affect clinical endpoints—including pain intensity, depression, and physical disability—through three primary mediating pathways: neurobiological alterations, cognitive biases, and maladaptive behavioral patterns. |
Methods
A narrative review was conducted to identify studies relevant to pain catastrophizing (PC), its underlying mechanisms, and clinical implications. Electronic databases, including PubMed, Web of Science, and Scopus, were searched for articles published up to March 2025. The search strategy combined terms related to PC and its associated mechanisms, including “pain catastrophizing”, “catastrophizing”, “pain perception”, “neurobiological mechanisms”, “cognitive mechanisms”, “behavioral mechanisms”, and “clinical management”. In addition, the reference lists of relevant articles were manually screened to identify further studies.
Studies were considered eligible if they examined PC or related cognitive processes and reported findings on neurobiological, psychological, behavioral, or clinical aspects relevant to the scope of this review. Only articles published in English in peer-reviewed journals were included. Conference abstracts, editorials, commentaries, and studies not directly relevant to the topic were excluded.
Titles and abstracts were screened first, followed by full-text review of potentially relevant articles. Study selection was guided by relevance to the objectives of this review, with emphasis on three main domains: underlying mechanisms, conceptual and psychosocial frameworks, and clinical management strategies related to PC. Given the narrative nature of this review, studies were selected to provide a representative overview of key themes rather than an exhaustive systematic synthesis. Owing to the heterogeneity of study designs, populations, and outcome measures, findings were synthesized narratively.
Neurobiological and Psychosocial Mechanisms of Pain Catastrophizing
Neurobiological Mechanisms of Pain Catastrophizing
Molecular Biomarkers Associated with Pain Catastrophizing
Neurobiological mechanisms may contribute to PC (Figure 2). Both genetic and environmental factors have been suggested to influence the neurobiology of pain, potentially contributing to individual differences in pain perception, emotional regulation, and coping strategies. Pain experience is shaped by prior exposures and learning processes that affect cognitive, emotional, and pain modulatory systems.
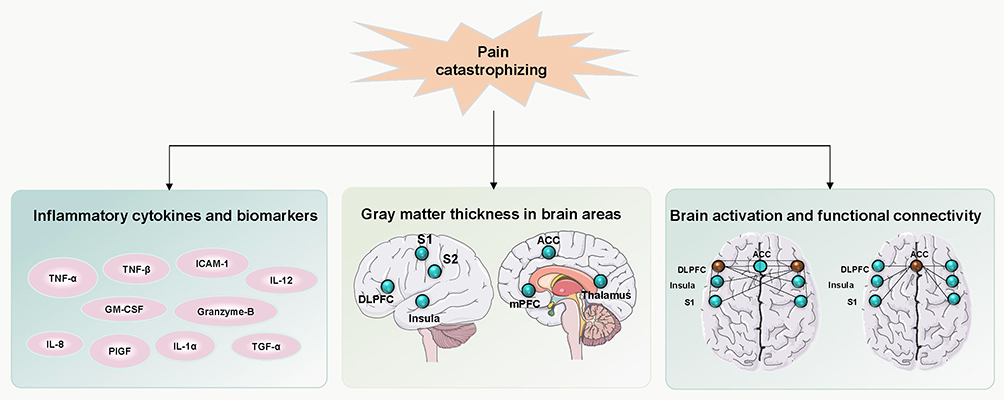 |
Figure 2 Proposed neurobiological mechanisms associated with pain catastrophizing. The schematic illustrates the multi-dimensional neurobiological framework of pain catastrophizing: Systemic inflammation, characterized by pro-inflammatory cytokines and biomarkers; Structural alterations, indicated by variations in cortical thickness across key pain-processing regions (e.g., S1, S2, ACC, DLPFC); and Functional dysconnectivity, reflecting disrupted neural network communication within the pain matrix. These components may contribute to the transition from acute pain to chronic pain states. Abbreviations: S1, primary somatosensory cortex; S2, secondary somatosensory area; DLPFC, dorsolateral prefrontal cortex; mPFC, medial prefrontal cortex; ACC, anterior cingulate cortex; ICAM-1, intercellular adhesion molecule 1. |
Emerging evidence suggests that neuroinflammatory processes may be involved in the biological pathways associated with PC.30 For example, in veterans with chronic residual limb pain, higher levels of PC were associated with increased levels of IL-8, IL-12, TNF-β, PIGF, and ICAM-1, as well as lower levels of IL-13.30 In patients with bladder pain syndrome, higher catastrophizing scores have been associated with lower urinary levels of BDNF and VEGF.31 In addition, reduced expression of IL-1α and Granzyme-B has been reported in arthritis patients with elevated PC, suggesting possible involvement in inflammatory pathways related to pain and disease progression.32 Experimental studies have also suggested that GM-CSF may participate in pain-related processes in animal models.33
However, biomarker findings related to PC remain heterogeneous across pain conditions and study populations. These differences may reflect variation in study design, sample source, and underlying pain mechanisms. Although several candidate markers have been proposed, current evidence remains preliminary, and their specific roles in PC require further validation.
Brain Regions and Functional Connectivity Associated with Pain Catastrophizing
PC has been associated with structural and functional alterations in several brain regions involved in pain processing and emotional regulation. Previous neuroimaging studies have reported that PC is correlated with changes in gray matter morphology and density in multiple brain areas.34 For example, a negative association between PC and cortical thickness in the dorsolateral prefrontal cortex (DLPFC) has been observed in patients with irritable bowel syndrome.35 Similar relationships have been reported in the nucleus accumbens and the left anterior insula among individuals with fibromyalgia.36 Comparable structural associations have also been identified in other regions, including the primary somatosensory cortex (S1), anterior midcingulate cortex (ACC), and prefrontal cortex (PFC) in patients with migraine.37 One study also suggested that reductions in PC following CBT were associated with increased gray matter in regions involved in pain perception (insula, ACC, S1, and PFC) and pain modulation (DLPFC).38
PC has also been associated with alterations in resting-state functional connectivity (rsFC),39 particularly in brain regions related to pain perception, pain cognition, and the default neural network (DMN).40 A previous study41 reported a positive association between pain rumination and activity in regions involved in pain perception, including S1, the anterior insula, and the thalamus, in patients with temporomandibular disorders. Altered functional connectivity between the medial prefrontal cortex (mPFC) and other regions—including the posterior cingulate cortex (PCC), precuneus, thalamus, retrosplenial cortex, and periaqueductal gray (PAG) has also been reported in relation to PC.36,37,42
Catastrophizing-related cognition has also been linked to altered DMN activity,43 and some studies have suggested that individuals with elevated PC show stronger connectivity between the DMN and motor-related networks.44,45 Conversely, reductions in pain catastrophizing following treatment have been associated with decreased DMN connectivity.46 The DMN is thought to interact with circuits of the medial system, which are involved in affective and evaluative aspects of pain processing. Self-referential tasks have been shown to activate the DMN, particularly in individuals with depressive symptoms.47 The insula, a brain region associated with interoception and the subjective awareness of bodily states, has also been reported to show heightened activation in individuals with elevated levels of PC. Additionally, rsFC between the posterior cingulate cortex (PCC) and the DLPFC was positively associated with PC in individuals with migraine, whereas a negative correlation was observed in control subjects.37
Task-based neuroimaging studies have also explored the neural correlates of PC using experimental pain paradigms. Despite differences in experimental stimuli (such as pressure pain and saline infusion), several brain regions have been consistently implicated, including the DLPFC,48,49 insula,48,50,51 ACC,23,42,52 PCC,51,53 and portions of the supplementary motor area.50 Furthermore, anticipatory brain activity in the anterior and ventrolateral prefrontal cortex and posterior parietal cortex has been negatively associated with PC.54,55 In addition, a working memory study reported a positive association between PC and medial prefrontal cortex responses to increasing task load.56
However, findings across studies remain heterogeneous, and the direction and magnitude of these associations may vary across pain conditions and experimental paradigms. Overall, although neuroimaging findings suggest that PC is associated with alterations in brain structure and connectivity, the underlying mechanisms remain incompletely understood.
Psychosocial Theories and Models of Pain Catastrophizing
Several theoretical frameworks have been proposed to explain the role of PC in pain perception and related outcomes.26 These frameworks include appraisal theory, the communal coping model, the fear-avoidance model, the bio-psychomotor model, and the behavioral inhibition/activation system (BIS-BAS) model (Figure 3).
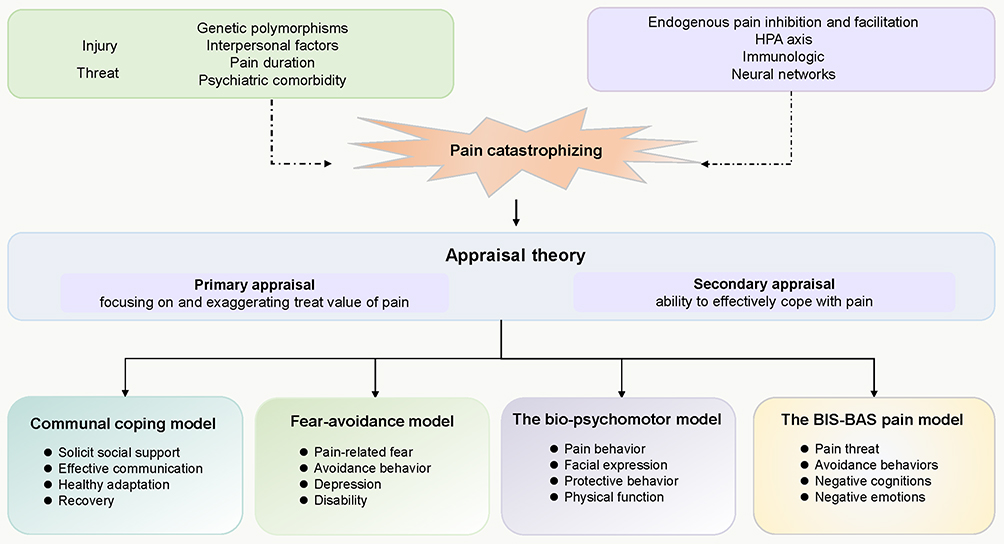 |
Figure 3 Psychosocial framework and theoretical models of pain catastrophizing. The schematic depicts the theoretical underpinnings of pain catastrophizing within the context of appraisal theory. (Top) Pre-existing genetic, environmental, and neuro-endocrine factors are potential contributors to pain catastrophizing. (Middle) According to the appraisal model, pain catastrophizing involves primary appraisal (overestimation of pain threat) and secondary appraisal (underestimation of coping resources). (Bottom) These cognitive processes manifest through four validated psychosocial models: Communal Coping, Fear-Avoidance, Bio-psychomotor, and BIS-BAS models, which may help explain behavioral and recovery outcomes. Abbreviations: HPA, hypothalamic-pituitary-adrenal axis; BIS, behavioral inhibition system; BAS, behavioral activation system. |
Appraisal Theory
PC has been conceptualized as part of the cognitive appraisal process and may influence the coping strategies that individuals subsequently adopt.9 Previous studies have suggested that individuals with elevated PC may exhibit a negative cognitive bias.57 Such biases may involve selective attention to negative information and reduced attention to positive or neutral stimuli, thereby amplifying the perceived severity of pain and related emotional distress. In addition, individuals with high levels of PC may show cognitive distortions, including overgeneralization and exaggerated expectations regarding negative outcomes.
For example, children who catastrophize in response to pain may also display similar cognitive-emotional patterns when responding to non-pain-related stressors. This generalized tendency has been suggested as one possible explanation for the observed associations between PC and psychological conditions such as anxiety and depression. This interpretation is also supported by findings from a previous meta-analysis.58 However, it should be noted that the relationship between PC and negative mood states may, in part, reflect conceptual and measurement overlap between these constructs. Therefore, although associations between PC, anxiety, and depression have been consistently reported, the directionality and underlying mechanisms of these relationships remain unclear.
Communal Coping Model
Sullivan et al59 proposed PC as a key component in the communal coping model, which has been suggested as a framework for understanding adjustment to chronic illness.60 Within this framework, PC is conceptualized as a coping strategy through which individuals communicate their pain experience in order to elicit support, empathy, and assistance from others.61 When individuals experience pain-related distress, increased attention to pain and its consequences may contribute to a greater focus on pain interference.59
Individuals with higher levels of PC may therefore be more likely to engage in communal coping behaviors, such as expressing distress through verbal or non-verbal cues (eg, grimacing or vocalization), particularly in the presence of others. Such behaviors may function to attract attention and solicit emotional or instrumental support from the social environment. In this context, the expression of pain may influence others’ perceptions and responses, potentially enhancing perceived empathy and social connectedness.62–64 This pattern may be adaptive in certain contexts, particularly when adequate social support is available and responsive.
Nevertheless, individuals who have lower levels of catastrophizing may adopt solitary coping strategies and downplay their discomfort in order to avoid drawing social attention. However, current evidence remains limited, and it is difficult to distinguish adaptive support-seeking from maladaptive reinforcement of pain behaviors.
Fear-Avoidance Model
The fear-avoidance model (FAM) provides a widely used framework for understanding the relationship between catastrophizing and physical function.65–68 According to this model, individuals who interpret pain as threatening may engage in PC and threat-related appraisals. Such interpretations may increase fear of future pain, which in turn may lead to avoidance of activities and ultimately contribute to disuse and disability.68
Within this framework, PC has been proposed as an important cognitive factor associated with chronic pain and psychological distress, including depressive symptoms.69,70 The model suggests that individuals with elevated levels of PC may be more vulnerable to persistent pain-related problems following injury, thereby contributing to a self-perpetuating cycle. Individuals with higher levels of catastrophizing may show heightened responses to actual or perceived threats, resulting in greater attention to pain sensations and prior negative experiences.69
Moreover, this model suggests that PC may interfere with engagement in health-related exercise and rehabilitation, which are often important components of chronic pain management.24,38,71 This may reduce the likelihood that individuals will use exercise as an effective self-management strategy. As a result, PC may be associated with poorer functional outcomes, although the strength and direction of this relationship may vary across studies. Overall, the role of PC within this model may differ across individuals and clinical conditions.
The Bio-Psychomotor Model
Although catastrophizing has been associated with heightened pain-related communicative behaviors, particularly facial expressions of pain,72–74 the bio-psychomotor model provides a useful framework for understanding its relationship with physical function. Within this model, pain behaviors are conceptualized as integral components of the pain system that serve communicative, protective, and social-relational functions.75 From this perspective, individuals who interpret pain catastrophically may be more likely to adopt protective behaviors (eg, guarding, bracing), which may contribute to reduced physical function over time.76 However, the specific contribution of catastrophizing within this model remains difficult to disentangle from other interacting psychological and motor factors.
BIS-BAS Model
PC has been linked to the Behavioral Inhibition System (BIS) component of the BIS-BAS pain model.77 When pain is perceived as a threat, activation of the BIS may be associated with avoidance behaviors (eg, reduced movement), negative cognitions (eg, catastrophic thinking), and anxiety, which may in turn contribute to heightened pain perception. PC has been proposed as an important cognitive factor related to BIS activity and has been associated with greater pain intensity and distress. However, the underlying neurobiological pathways remain to be fully elucidated.
Clinical Management Strategies
Various strategies have been implemented in clinical settings to address PC, and this review focuses on three main therapeutic approaches (Figure 4).
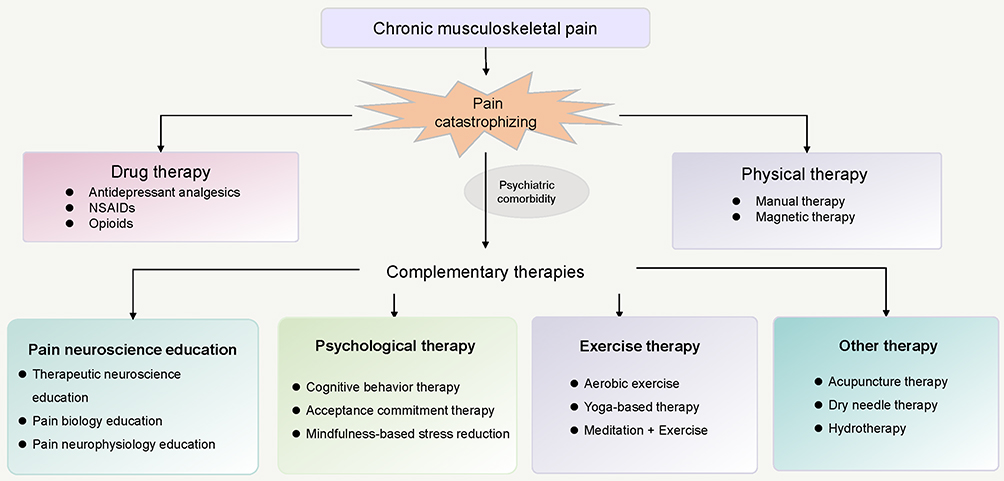 |
Figure 4 Clinical management strategies for chronic musculoskeletal pain associated with pain catastrophizing. The schematic illustrates the therapeutic pathways targeting chronic musculoskeletal pain through pain catastrophizing (central node). Treatments are structured across conventional (Drug and Physical therapy) and complementary approaches (PNE, psychological, exercise, and other adjunctive therapies). Solid arrows indicate established interventional routes directed at mitigating the reinforcement cycle of catastrophizing. |
Pharmacotherapeutics
Non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used as first-line agents for pain management because of their analgesic and anti-inflammatory effects.78 Opioids are typically reserved for moderate to severe pain requiring central analgesia.79 However, their use is limited by potential adverse effects, including gastrointestinal complications, renal impairment, and platelet dysfunction, as well as the risk of dependence.
Chronic pain frequently coexists with comorbid conditions such as anxiety, depression, and sleep disturbances, which may require adjunctive pharmacotherapy. Nevertheless, there remains a dearth of standardized guidelines regarding optimal dosing and the management of addiction risk in clinical practice. Previous studies have reported associations between PC and substance abuse behaviors, suggesting that interventions targeting PC may help reduce related adverse outcomes.80 The mechanism by which PC increases substance use is hypothesized to be driven by the motivation to achieve relief.81
Participants with high levels of catastrophizing have been reported to have lower awareness of opioid-related risks, including side effects and dependence, which may contribute to increased expectations for opioid prescriptions.81,82 However, current evidence does not support a definitive relationship between opioid dependence and the reinforcement of catastrophizing behavior.
Some pharmacological agents have shown potential associations with reductions in both pain severity and catastrophizing. For example, a prospective study suggested that the non-opioid agent (ziconotide) may improve neuropathic pain and related emotional components, including disability and catastrophizing.83 Similarly, limited evidence from specific populations indicates that atypical antipsychotic risperidone for ASD irritability and an ADHD medication, atomoxetine may be associated with improvements in pain, anxiety, depression, and pain-related catastrophic thinking.84 However, these findings remain preliminary and may not be generalizable.
Furthermore, the clinical use of glucocorticoids remains variable, with both overuse and underuse reported in practice. Antidepressants are also commonly used in pain management, although their role in targeting PC specifically remains unclear. Overall, pharmacological strategies should be individualized, taking into account patient characteristics, comorbidities, and potential risks.
Manual Therapy
The effects of manual therapy have been attributed to neurophysiological mechanisms as well as placebo-related responses. It may also be associated with improvements in psychological resilience, including potential changes in patients’ perceptions and beliefs.85,86 Cervical manipulation, a commonly used manual therapy, has been suggested to influence sensory and motor processing and may help modulate communication between the brain and spinal cord.87,88 However, previous studies have reported no significant short-term improvement in PC among patients with fibromyalgia, whereas some studies have observed statistically significant changes at longer-term follow-up (eg, one year).89
These inconsistent findings may be related to differences in treatment duration, patient characteristics, and study design.90,91 Although previous systematic reviews86,92,93 have examined the effects of manual therapy on psychological and pain-related outcomes, evidence specifically addressing PC remains limited. Overall, further research is needed to clarify the effectiveness and consistency of different forms of manual therapy in relation to PC across short-, intermediate-, and long-term follow-up periods.
Electrostimulation
Transcutaneous electrical nerve stimulation (TENS) and transcranial direct current stimulation (tDCS) have been extensively investigated as electrotherapeutic modalities for the management of chronic pain syndrome, primarily due to their potential to modulate nociceptive processing. These interventions are thought to exert their effects by activating descending central inhibitory pathways and attenuating excitatory neurotransmission within the dorsal horn of the spinal cord.94 Notably, anodal tDCS applied to the left primary motor cortex has been associated with improvements in pain intensity and sleep quality, possibly through its neuromodulatory effects on central pain processing.95
Although the existing evidence remains limited, anodal tDCS applied to the DLPFC has been associated with improvements in both pain perception and cognitive performance in patients with fibromyalgia.96,97 However, findings are not consistent. For example, a trial combining multicomponent therapy (including aerobic training, relaxation, education, and swimming) with electrostimulation did not demonstrate additional reductions in PC compared to multicomponent treatment alone.98 This suggests that observed improvements in PC may be primarily driven by non-electrostimulation components, although the specific contribution of each component remains unclear.
In addition, higher levels of PC have been associated with lower adherence to treatment, including medication use, clinical follow-up, and engagement in physical therapy.99 This may further influence treatment outcomes and complicate the interpretation of intervention effects.
Psychotherapy
Psychological therapies encompass diverse modalities aimed at addressing pain syndromes. As a typical psychotherapy, CBT combines the principles of fundamental cognitive and behavioral techniques to modify maladaptive thoughts and behaviors, thereby supporting adaptive changes in pain-related outcomes.100–104 It is targeted at specific problems such as pain interference, psychological distress and sleep disturbances.105,106 CBT has been associated with improvements in psychological symptoms in individuals with chronic musculoskeletal conditions.107,108 As an extension of CBT, acceptance and commitment therapy (ACT) focuses on enhancing psychological flexibility and promoting acceptance of pain-related experiences.109,110 Similarly, mindfulness-based stress reduction (MBSR) is a structured training program that emphasizes psychological flexibility. Specifically, it aims to help patients become more aware of the present experience and contextual changes, as well as to evaluate their physical and psychological circumstances in a more accepted and nonjudgmental way.111,112
Previous reviews have suggested that CBT may reduce PC among individuals with various chronic musculoskeletal disorders.113 In clinical practice, CBT typically involves active patient participation in structured interventions delivered over 8–12 sessions. One study reported greater improvements in PC scores in the CBT group compared with a health education control at 3-month follow-up, with a mean reduction of 10.94 points (approximately 48.4% from baseline).114
The association between PC and psychological comorbidity suggests that interventions targeting catastrophic thinking may also potentially alleviate anxiety and depressive symptoms. A prior systematic review has also indicated that ACT, administered individually or in groups, may improve function, anxiety, and depression in patients with chronic pain.115
MBSR training has also been suggested to modulate immune-inflammatory pathways in conditions such as fibromyalgia. Some studies have reported a trend toward improvement in the pro/anti-inflammatory (IL-6/IL-10) ratio in fibromyalgia patients who attend six or more sessions of MBSR. However, these findings remain preliminary. Despite the potential benefits of these psychotherapeutic interventions, time, cost, and therapist availability may impede patient access.116 There is a need for more accessible and scalable approaches, particularly for patients with higher levels of PC.
Other psychotherapeutic approaches, such as hypnotherapy117 and guided imagery therapy,118 have also been explored, although they typically require delivery by trained professionals. In clinical practice, interventions should be individualized based on patient characteristics and clinical context.
Pain Neuroscience Education
Education enables individuals to better understand their condition and may facilitate self-management.119,120 Pain neuroscience education (PNE), a form of biopsychosocial education, aims to help individuals reconceptualize their pain experience. Multiple terminologies for PNE have been employed in the literature, such as Explain Pain,121,122 therapeutic neuroscience education,123 pain biology education,124 and pain neurophysiology education.125
Previous research has suggested that PNE may modulate maladaptive pain perceptions and reduce PC and fear-avoidance behaviors in patients with chronic low back pain,126 osteoarthritis,127,128 and fibromyalgia.129 A fundamental tenet of PNE posits that pain perception does not always correspond directly to the extent of tissue damage.121 The traditional format of PNE is educational booklets, videos, or manuals, either individually or in group settings. However, some studies have reported limited long-term effects of PNE on PC reduction in fibromyalgia.130 Generally, fibromyalgia symptoms are often considered to be related to altered threat processing within neural networks, which may be influenced by maladaptive beliefs, cultural factors, and prior experiences.129 In contrast, structured face-to-face PNE interventions have shown more favorable outcomes in some studies, possibly by facilitating changes in maladaptive cognitions and health perceptions.130 PNE has also been proposed to support gradual re-exposure to activities by modifying maladaptive interpretations of pain and symptoms.131
A previous systematic review has suggested that PNE may be associated with improvements in pain, psychological distress, physical activity, and healthcare utilization.132 Given its relatively low cost, PNE may represent a promising complementary approach for reducing reliance on pharmacological therapy.133 However, further research is needed to optimize its delivery and determine its long-term effectiveness.
Exercise Therapy
Among conservative non-pharmacological therapies, exercise therapy, particularly aerobic exercise, has emerged as a widely accepted modality due to its cost-effectiveness and potential benefits in improving sleep quality and mood disorders.134–136 Exercise therapy is widely recognized as a cornerstone in the management of chronic musculoskeletal pain and is consistently endorsed in clinical practice guidelines.137,138 Regular exercise may influence hypothalamic-pituitary function and neurotransmitter levels, particularly endorphins, which are linked to improved pain sensitivity and psychological symptoms. In addition, physical activity may promote the production of anti-inflammatory cytokines such as IL-10 and reduce TNF-α levels, as reported in healthy populations139 and in patients with cardiovascular and autoimmune diseases.140–142
Additionally, increasing acceptance may have substantial effects on the rehabilitation of severe pain.61,143 Exercise therapy combined with PNE (eg, twice weekly sessions of 60 minutes over 10 weeks) has been associated with greater improvements in PC and disease impact than exercise therapy alone in the treatment of chronic musculoskeletal pain.144–146 It is possible that PNE as an adjunct reduces participants’ fear and anxiety regarding movement, thereby enhancing exercise engagement and reducing the affective–emotional burden of pain.121 This effect, in conjunction with mechanisms of exercise-induced hypoalgesia, may explain why these interventions produce greater benefits when combined.147 Therefore, future research should consider the impact of exercise dosage and cumulative exposure to PNE on disability outcomes.148
Moreover, lack of adherence is common among patients with chronic conditions. Kinesiophobia represents a major barrier to exercise and is associated with more sedentary behavior.137,149 It remains challenging for patients to maintain consistent exercise routines and incorporate them into daily life. Practice-based interventions in natural settings may help improve adherence to physical activity.150–152 In addition, interventions incorporating meditation and mindfulness-based breathing strategies into home-based exercise programs, such as yoga, have been associated with reductions in PC.153 These approaches may enhance awareness of maladaptive responses and make physical activity more tolerable, meaningful, and sustainable.153
Furthermore, for patients with restricted mobility, such as those with spinal cord injury, hydrotherapy has been reported as a potentially beneficial intervention.154 This modality may reduce mechanical stress on musculoskeletal structures and improve peripheral circulation and joint mobility. Some studies have suggested that this approach may improve neuropathic pain symptoms and reduce PC.
Regular exercise is generally beneficial for overall health. However, promoting sustained engagement remains a key challenge. The implementation of these interventions should consider practical constraints, economic factors, and resource utilization within healthcare systems.
Other Complementary Therapies
Several complementary therapeutic modalities have been explored in relation to PC. Acupuncture,155 a systemic intervention derived from traditional Chinese medicine, is thought to exert analgesic effects through multiple mechanisms, including stimulation of specific acupoints that may influence neural transmission and circulation. Specifically, it has been suggested that acupuncture may reduce pain-related cognition and PC, potentially through modulation of neural activity and the release of endogenous opioids such as endorphins. Additionally, dry needling therapy156,157 targets myofascial trigger points in muscles and has been associated with improvement in PC. However, these interventions typically require delivery by trained practitioners to ensure safety and appropriate application.
Conclusion
PC has emerged as an important cognitive–emotional construct associated with pain perception, psychological distress, and functional outcomes in individuals with chronic pain. Growing evidence suggests that PC may influence pain experiences through complex interactions involving neurobiological mechanisms, psychosocial processes, and maladaptive behavioral responses. Nevertheless, the strength and consistency of the available evidence vary across studies, and the underlying pathways remain incompletely understood.
Recent research integrating neuroimaging findings, psychological assessments, and inflammatory biomarkers has provided preliminary insights into the potential mechanisms linking catastrophizing to altered pain processing. These findings highlight the multifactorial nature of PC and suggest that cognitive and behavioral factors should be considered when interpreting pain-related outcomes. Interventions such as PNE, CBT-based psychological approaches, and structured physical activity have been associated with reductions in catastrophizing and improvements in some pain-related outcomes in certain populations. Multidisciplinary care models integrating medical and nursing perspectives may further support patient education, self-management, and individualized treatment planning.
Despite these advances, current evidence remains heterogeneous and, in some cases, limited by methodological variability. Future longitudinal and mechanistic studies are needed to clarify causal relationships and to determine how interventions targeting catastrophizing may contribute to improved clinical outcomes across different pain conditions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shaanxi Province Natural Science Foundation Project (2025JC-YBMS-871).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Fillingim RB, Ohrbach R, Greenspan JD, et al. Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain. 2013;14(12 Suppl):T75–15. doi:10.1016/j.jpain.2013.06.009
2. Osiewicz M, Lobbezoo F, Ciapała B, et al. Pain predictors in a population of temporomandibular disorders patients. J Clin Med. 2020;9(2):452. doi:10.3390/jcm9020452
3. Beck AT. Cognitive Therapy of Depression. Guilford press; 1979.
4. Ellis A. Reason and emotion in psychotherapy. 1962.
5. Sullivan MJ, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychological Assessment. 1995;7(4):524. doi:10.1037/1040-3590.7.4.524
6. Carleton RN, Sharpe D, Asmundson GJ. Anxiety sensitivity and intolerance of uncertainty: requisites of the fundamental fears? Behav Res Therapy. 2007;45(10):2307–2316. doi:10.1016/j.brat.2007.04.006
7. Starcevic V, Berle D. Cognitive specificity of anxiety disorders: a review of selected key constructs. Depression Anxiety. 2006;23(2):51–61. doi:10.1002/da.20145
8. Garnefski N, Kraaij V. Relationships between cognitive emotion regulation strategies and depressive symptoms: a comparative study of five specific samples. Pers Individ Dif. 2006;40(8):1659–1669. doi:10.1016/j.paid.2005.12.009
9. Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Exp Rev Neurotherapeut. 2009;9(5):745–758.
10. Boomershine CS. Fibromyalgia: the prototypical central sensitivity syndrome. Curr Rheumatol Rev. 2015;11(2):131–145. doi:10.2174/1573397111666150619095007
11. Burton AK, Tillotson KM, Main CJ, et al. Psychosocial predictors of outcome in acute and subchronic low back trouble. Spine. 1995;20(6):722–728. doi:10.1097/00007632-199503150-00014
12. Dunn LK, Durieux ME, Fernández LG, et al. Influence of catastrophizing, anxiety, and depression on in-hospital opioid consumption, pain, and quality of recovery after adult spine surgery. J Neurosurg Spine. 2017;28(1):119–126. doi:10.3171/2017.5.SPINE1734
13. Wright D, Hoang M, Sofine A, et al. Pain catastrophizing as a predictor for postoperative pain and opiate consumption in total joint arthroplasty patients. Archiv Orthopaedic Trauma Surg. 2017;137(12):1623–1629. doi:10.1007/s00402-017-2812-x
14. Rodero B, García-Campayo J, Casanueva B, Buriel Y. Tratamientos no farmacológicos en fibromialgia: una revisión actual. Revista de Psicopatología Y Psicología Clínica. 2009;14(3).
15. Edwards RR, Bingham III CO, Bathon J, Haythornthwaite JA. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Care Res. 2010;55(2).
16. Toth C, Brady S, Hatfield M. The importance of catastrophizing for successful pharmacological treatment of peripheral neuropathic pain. J Pain Res. 2014;327. doi:10.2147/JPR.S56883
17. van Wilgen CP, van Ittersum MW, Kaptein AA, et al. Illness perceptions in patients with fibromyalgia and their relationship to quality of life and catastrophizing. Arthritis Rheum. 2008;58(11):3618–3626. doi:10.1002/art.23959
18. Häggman-Henrikson B, Bechara C, Pishdari B, et al. Impact of catastrophizing in patients with temporomandibular disorders-A systematic review. J Oral Facial Pain Headache. 2020;34(4):379–397. doi:10.11607/ofph.2637
19. Beesdo K, Jacobi F, Hoyer J, et al. Pain associated with specific anxiety and depressive disorders in a nationally representative population sample. Soc Psychiatry Psychiatr Epidemiol. 2010;45(1):89–104. doi:10.1007/s00127-009-0045-1
20. Fillingim RB, Ohrbach R, Greenspan JD, et al. Potential psychosocial risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J Pain. 2011;12(11 Suppl):T46–60. doi:10.1016/j.jpain.2011.08.007
21. Turner JA, Brister H, Huggins K, et al. Catastrophizing is associated with clinical examination findings, activity interference, and health care use among patients with temporomandibular disorders. J Orofac Pain. 2005;19(4):291–300.
22. Turner JA, Dworkin SF, Mancl L, et al. The roles of beliefs, catastrophizing, and coping in the functioning of patients with temporomandibular disorders. Pain. 2001;92(1–2):41–51. doi:10.1016/S0304-3959(00)00469-3
23. Gracely RH, Geisser ME, Giesecke T, et al. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain. 2004;127(Pt 4):835–843. doi:10.1093/brain/awh098
24. Edwards RR, Bingham CO, Bathon J, et al. Catastrophizing and pain in arthritis, fibromyalgia, and other rheumatic diseases. Arthritis Rheum. 2006;55(2):325–332. doi:10.1002/art.21865
25. Cooke ME, Edwards RR, Wheeler GL, et al. Pain catastrophizing is associated with reduced neural response to monetary reward. Front Pain Res. 2023;4:1129353. doi:10.3389/fpain.2023.1129353
26. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. doi:10.1097/00002508-200103000-00008
27. Ong WY, Stohler CS, Herr DR. Role of the prefrontal cortex in pain processing. Mol Neurobiol. 2019;56(2):1137–1166. doi:10.1007/s12035-018-1130-9
28. Chang X, Zhang H, Chen S. Neural circuits regulating visceral pain. Commun Biol. 2024;7(1):457. doi:10.1038/s42003-024-06148-y
29. Su N, Cai P, Dou Z, et al. Brain nuclei and neural circuits in neuropathic pain and brain modulation mechanisms of acupuncture: a review on animal-based experimental research. Front Neurosci. 2023;17:1243231. doi:10.3389/fnins.2023.1243231
30. Chamessian A, Van de Ven T, Buchheit T, et al. Differential expression of systemic inflammatory mediators in amputees with chronic residual limb pain. Pain. 2017;158(1):68–74. doi:10.1097/j.pain.0000000000000728
31. Soriano A, Allen A, Malykhina AP, et al. Relationship of pain catastrophizing with urinary biomarkers in women with bladder pain syndrome. Female Pelvic Med Reconstr Surg. 2021;27(12):746–752. doi:10.1097/SPV.0000000000001041
32. Giordano R, Capriotti C, Gerra MC, et al. A potential link between inflammatory profiles, clinical pain, pain catastrophizing and long-term outcomes after total knee arthroplasty surgery. Eur J Pain. 2024;28(7):1202–1212. doi:10.1002/ejp.2254
33. Cook AD, Pobjoy J, Sarros S, et al. Granulocyte-macrophage colony-stimulating factor is a key mediator in inflammatory and arthritic pain. Ann Rheum Dis. 2013;72(2):265–270. doi:10.1136/annrheumdis-2012-201703
34. Liu S, You B, Zhang X, et al. Individual differences in pain catastrophizing and regional gray matter volume among community-dwelling adults with chronic pain: a voxel-based morphology study. Clin J Pain. 2023;39(5):209–216. doi:10.1097/AJP.0000000000001103
35. Blankstein U, Chen J, Diamant NE, et al. Altered brain structure in irritable bowel syndrome: potential contributions of pre-existing and disease-driven factors. Gastroenterology. 2010;138(5):1783–1789. doi:10.1053/j.gastro.2009.12.043
36. Ceko M, Bushnell MC, Fitzcharles M-A, et al. Fibromyalgia interacts with age to change the brain. Neuroimage Clin. 2013;3:249–260. doi:10.1016/j.nicl.2013.08.015
37. Hubbard CS, Khan SA, Keaser ML, et al. Altered brain structure and function correlate with disease severity and pain catastrophizing in migraine patients. eNeuro. 2014;1(1):e2014. doi:10.1523/ENEURO.0006-14.2014
38. Seminowicz DA, Shpaner M, Keaser ML, et al. Cognitive-behavioral therapy increases prefrontal cortex gray matter in patients with chronic pain. J Pain. 2013;14(12):1573–1584. doi:10.1016/j.jpain.2013.07.020
39. Terry EL, Tanner JJ, Cardoso JS, et al. Associations between pain catastrophizing and resting-state functional brain connectivity: ethnic/race group differences in persons with chronic knee pain. J Neurosci Res. 2022;100(4):1047–1062. doi:10.1002/jnr.25018
40. Ellingsen DM, Beissner F, Moher Alsady T, et al. A picture is worth a thousand words: linking fibromyalgia pain widespreadness from digital pain drawings with pain catastrophizing and brain cross-network connectivity. Pain. 2021;162(5):1352–1363. doi:10.1097/j.pain.0000000000002134
41. Kucyi A, Moayedi M, Weissman-Fogel I, et al. Enhanced medial prefrontal-default mode network functional connectivity in chronic pain and its association with pain rumination. J Neurosci. 2014;34(11):3969–3975. doi:10.1523/JNEUROSCI.5055-13.2014
42. Lazaridou A, Kim J, Cahalan CM, et al. Effects of Cognitive-Behavioral Therapy (CBT) on brain connectivity supporting catastrophizing in fibromyalgia. Clin J Pain. 2017;33(3):215–221. doi:10.1097/AJP.0000000000000422
43. Lee J, Protsenko E, Lazaridou A, et al. Encoding of self-referential pain catastrophizing in the posterior cingulate cortex in fibromyalgia. Arthritis Rheumatol. 2018;70(8):1308–1318. doi:10.1002/art.40507
44. Kim J, Loggia ML, Cahalan CM, et al. The somatosensory link in fibromyalgia: functional connectivity of the primary somatosensory cortex is altered by sustained pain and is associated with clinical/autonomic dysfunction. Arthritis Rheumatol. 2015;67(5):1395–1405. doi:10.1002/art.39043
45. Kim J, Mawla I, Kong J, et al. Somatotopically specific primary somatosensory connectivity to salience and default mode networks encodes clinical pain. Pain. 2019;160(7):1594–1605. doi:10.1097/j.pain.0000000000001541
46. Lee J, Lazaridou A, Paschali M, et al. A randomized controlled neuroimaging trial of cognitive behavioral therapy for fibromyalgia pain. Arthritis Rheumatol. 2024;76(1):130–140. doi:10.1002/art.42672
47. Davey CG, Breakspear M, Pujol J, et al. A brain model of disturbed self-appraisal in depression. Am J Psychiatry. 2017;174(9):895–903. doi:10.1176/appi.ajp.2017.16080883
48. Henderson LA, Akhter R, Youssef AM, et al. The effects of catastrophizing on central motor activity. Eur J Pain. 2016;20(4):639–651. doi:10.1002/ejp.781
49. Hiramatsu T, Nakanishi K, Yoshimura S, et al. The dorsolateral prefrontal network is involved in pain perception in knee osteoarthritis patients. Neurosci Lett. 2014;581:109–114. doi:10.1016/j.neulet.2014.08.027
50. Hubbard CS, Hong J, Jiang Z, et al. Increased attentional network functioning related to symptom severity measures in females with irritable bowel syndrome. Neurogastroenterol Motil. 2015;27(9):1282–1294. doi:10.1111/nmo.12622
51. Mathur VA, Moayedi M, Keaser ML, et al. High frequency migraine is associated with lower acute pain sensitivity and abnormal insula activity related to migraine pain intensity, attack frequency, and pain catastrophizing. Front Hum Neurosci. 2016;10:489. doi:10.3389/fnhum.2016.00489
52. Lin CS, Niddam DM, Hsu M-L, et al. Pain catastrophizing is associated with dental pain in a stressful context. J Dent Res. 2013;92(2):130–135. doi:10.1177/0022034512467804
53. Seminowicz DA, Davis KD. Cortical responses to pain in healthy individuals depends on pain catastrophizing. Pain. 2006;120(3):297–306. doi:10.1016/j.pain.2005.11.008
54. Loggia ML, Berna C, Kim J, et al. The lateral prefrontal cortex mediates the hyperalgesic effects of negative cognitions in chronic pain patients. J Pain. 2015;16(8):692–699. doi:10.1016/j.jpain.2015.04.003
55. Burgmer M, Petzke F, Giesecke T, et al. Cerebral activation and catastrophizing during pain anticipation in patients with fibromyalgia. Psychosom Med. 2011;73(9):751–759. doi:10.1097/PSY.0b013e318236588a
56. Čeko M, Gracely JL, Fitzcharles M-A, et al. Is a responsive default mode network required for successful working memory task performance? J Neurosci. 2015;35(33):11595–11605. doi:10.1523/JNEUROSCI.0264-15.2015
57. Beck AT. Cognitive models of depression. Cognitive Psychother Int Quart. 1987;1(1):5–37.
58. Miller MM, Meints SM, Hirsh AT. Catastrophizing, pain, and functional outcomes for children with chronic pain: a meta-analytic review. Pain. 2018;159(12):2442–2460. doi:10.1097/j.pain.0000000000001342
59. Sullivan M, Adams H, Sullivan M. Communicative dimensions of pain catastrophizing: social cueing effects on pain behaviour and coping. Pain. 2004;107(3):220–226. doi:10.1016/j.pain.2003.11.003
60. Helgeson VS, Jakubiak B, Van Vleet M, et al. Communal coping and adjustment to chronic illness: theory update and evidence. Pers Soc Psychol Rev. 2018;22(2):170–195. doi:10.1177/1088868317735767
61. Baranoff J, Hanrahan SJ, Kapur D, et al. Acceptance as a process variable in relation to catastrophizing in multidisciplinary pain treatment. Eur J Pain. 2013;17(1):101–110. doi:10.1002/j.1532-2149.2012.00165.x
62. Goubert L, Craig KD, Vervoort T, et al. Facing others in pain: the effects of empathy. Pain. 2005;118(3):285–288. doi:10.1016/j.pain.2005.10.025
63. Hadjistavropoulos T, Craig KD. A theoretical framework for understanding self-report and observational measures of pain: a communications model. Behav Res Therapy. 2002;40(5):551–570. doi:10.1016/S0005-7967(01)00072-9
64. Williams ACDC. Facial expression of pain: an evolutionary account. Behav Brain Sci. 2002;25(4):439–455.
65. Asmundson GJ, Noel M, Petter M, et al. Pediatric fear-avoidance model of chronic pain: foundation, application and future directions. Pain Res Manag. 2012;17(6):397–405. doi:10.1155/2012/908061
66. Leeuw M, Goossens MEJB, Linton SJ, et al. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30(1):77–94. doi:10.1007/s10865-006-9085-0
67. Pincus T, Smeets RJEM, Simmonds MJ, et al. The fear avoidance model disentangled: improving the clinical utility of the fear avoidance model. Clin J Pain. 2010;26(9):739–746. doi:10.1097/AJP.0b013e3181f15d45
68. Simons LE, Kaczynski KJ. The fear avoidance model of chronic pain: examination for pediatric application. J Pain. 2012;13(9):827–835. doi:10.1016/j.jpain.2012.05.002
69. Peters ML, Vlaeyen JW, van Drunen C. Do fibromyalgia patients display hypervigilance for innocuous somatosensory stimuli? Application of a body scanning reaction time paradigm. Pain. 2000;86(3):283–292. doi:10.1016/S0304-3959(00)00259-1
70. Martínez MP, Sánchez AI, Miró E, et al. The relationship between the fear-avoidance model of pain and personality traits in fibromyalgia patients. J Clin Psychol Med Settings. 2011;18(4):380–391. doi:10.1007/s10880-011-9263-2
71. Taylor SS, Davis MC, Yeung EW, et al. Relations between adaptive and maladaptive pain cognitions and within-day pain exacerbations in individuals with fibromyalgia. J Behav Med. 2017;40(3):458–467. doi:10.1007/s10865-016-9811-1
72. Lynch AM, Kashikar-Zuck S, Goldschneider KR, et al. Sex and age differences in coping styles among children with chronic pain. J Pain Sympt Manage. 2007;33(2):208–216. doi:10.1016/j.jpainsymman.2006.07.014
73. Vervoort T, Craig KD, Goubert L, et al. Expressive dimensions of pain catastrophizing: a comparative analysis of school children and children with clinical pain☆. Pain. 2008;134(1–2):59–68. doi:10.1016/j.pain.2007.03.038
74. Vervoort T, Goubert L, Crombez G. Parental responses to pain in high catastrophizing children: the moderating effect of child attachment. J Pain. 2010;11(8):755–763. doi:10.1016/j.jpain.2009.11.012
75. Sullivan MJ. Toward a biopsychomotor conceptualization of pain: implications for research and intervention. Clin J Pain. 2008;24(4):281–290. doi:10.1097/AJP.0b013e318164bb15
76. Sullivan MJ, Thibault P, Savard A, et al. The influence of communication goals and physical demands on different dimensions of pain behavior. Pain. 2006;125(3):270–277. doi:10.1016/j.pain.2006.06.019
77. Jensen MP, Ehde DM, Day MA. The behavioral activation and inhibition systems: implications for understanding and treating chronic pain. J Pain. 2016;17(5):529.e1–529.e18. doi:10.1016/j.jpain.2016.02.001
78. Fraquelli M, Casazza G, Conte D, et al. Non-steroid anti-inflammatory drugs for biliary colic. Cochrane Database Syst Rev. 2016;9(9):Cd006390. doi:10.1002/14651858.CD006390.pub2
79. Weibel S, Rücker G, Eberhart LH, et al. Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis. Cochrane Database Syst Rev. 2020;10(10):Cd012859. doi:10.1002/14651858.CD012859.pub2
80. Bichon JA, Bailey AJ, Ford SF, et al. Pain catastrophizing and substance misuse: a scoping review of the literature. Harv Rev Psychiatry. 2025;33(1):8–30. doi:10.1097/HRP.0000000000000415
81. Onishi E, Lucas JA, Maeno T, et al. Associations between high pain catastrophizing and opioid-related awareness and beliefs among patients in primary care. J Am Board Fam Med. 2023;36(2):267–276. doi:10.3122/jabfm.2022.220311R2
82. Martel MO, Jamison RN, Wasan AD, et al. The association between catastrophizing and craving in patients with chronic pain prescribed opioid therapy: a preliminary analysis. Pain Med. 2014;15(10):1757–1764. doi:10.1111/pme.12416
83. Shao MM, Khazen O, Hellman A, et al. Effect of first-line ziconotide intrathecal drug therapy for neuropathic pain on disability, emotional well-being, and pain catastrophizing. World Neurosurg. 2021;145:e340–e347. doi:10.1016/j.wneu.2020.10.079
84. Kasahara S, Takao C, Matsudaira K, et al. Case report: treatment of persistent atypical odontalgia with attention deficit hyperactivity disorder and autism spectrum disorder with risperidone and atomoxetine. Front Pain Res. 2022;3:926946. doi:10.3389/fpain.2022.926946
85. Bialosky JE, Bishop MD, Penza CW. Placebo mechanisms of manual therapy: a sheep in wolf’s clothing? J Orthop Sports Phys Ther. 2017;47(5):301–304. doi:10.2519/jospt.2017.0604
86. Williams NH, Hendry M, Lewis R, et al. Psychological response in spinal manipulation (PRISM): a systematic review of psychological outcomes in randomised controlled trials. Complementary Ther Med. 2007;15(4):271–283. doi:10.1016/j.ctim.2007.01.008
87. Haavik-Taylor H, Murphy B. Cervical spine manipulation alters sensorimotor integration: a somatosensory evoked potential study. Clin Neurophysiol. 2007;118(2):391–402. doi:10.1016/j.clinph.2006.09.014
88. Haavik Taylor H, Murphy B. The effects of spinal manipulation on central integration of dual somatosensory input observed after motor training: a crossover study. J Manipulative Physiol Ther. 2010;33(4):261–272. doi:10.1016/j.jmpt.2010.03.004
89. Moustafa IM, Diab AA. The addition of upper cervical manipulative therapy in the treatment of patients with fibromyalgia: a randomized controlled trial. Rheumatol Int. 2015;35(7):1163–1174. doi:10.1007/s00296-015-3248-7
90. Harrison DE, Harrison DD, Janik TJ, et al. Comparison of axial and flexural stresses in lordosis and three buckled configurations of the cervical spine. Clin Biomech. 2001;16(4):276–284. doi:10.1016/S0268-0033(01)00006-7
91. Diab AA, Moustafa IM. The efficacy of forward head correction on nerve root function and pain in cervical spondylotic radiculopathy: a randomized trial. Clin Rehabil. 2012;26(4):351–361. doi:10.1177/0269215511419536
92. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, et al. Conservative interventions reduce fear in individuals with chronic low back pain: a systematic review. Arch Phys Med Rehabil. 2020;101(2):329–358. doi:10.1016/j.apmr.2019.08.470
93. Schütze R, Rees C, Smith A, et al. How can we best reduce pain catastrophizing in adults with chronic noncancer pain? A systematic review and meta-analysis. J Pain. 2018;19(3):233–256. doi:10.1016/j.jpain.2017.09.010
94. DeSantana J, Da Silva LFS, De Resende MA, et al. Transcutaneous electrical nerve stimulation at both high and low frequencies activates ventrolateral periaqueductal grey to decrease mechanical hyperalgesia in arthritic rats. Neuroscience. 2009;163(4):1233–1241. doi:10.1016/j.neuroscience.2009.06.056
95. Deus-Yela J, Soler MD, Pelayo Vergara R, et al. Transcranial direct current stimulation for the treatment of fibromyalgia: a systematic review. Rev Neurol. 2017;65(8):353–360. doi:10.33588/rn.6508.2017025
96. Mylius V, Jung M, Menzler K, et al. Effects of transcranial direct current stimulation on pain perception and working memory. Eur J Pain. 2012;16(7):974–982. doi:10.1002/j.1532-2149.2011.00105.x
97. Santos V, Zortea M, Alves RL, et al. Cognitive effects of transcranial direct current stimulation combined with working memory training in fibromyalgia: a randomized clinical trial. Sci Rep. 2018;8(1):12477. doi:10.1038/s41598-018-30127-z
98. Guinot M, Maindet C, Hodaj H, et al. Effects of repetitive transcranial magnetic stimulation and multicomponent therapy in patients with fibromyalgia: a randomized controlled trial. Arthritis Care Res. 2019;73.
99. Currado D, Saracino F, Ruscitti P, et al. Pain catastrophizing negatively impacts drug retention rate in patients with psoriatic arthritis and axial spondyloarthritis: results from a 2-years perspective multicenter GIRRCS (Gruppo Italiano di Ricerca in Reumatologia Clinica) study. Arthritis Res Ther. 2024;26(1):162. doi:10.1186/s13075-024-03396-5
100. An H, He R-H, Zheng Y-R, et al. Cognitive-behavioral therapy. Advances in experimental medicine and biology. Advanc Exp Med Biol. 2017;1010:321–329. doi:10.1007/978-981-10-5562-1_16
101. Worm-Smeitink M, Janse A, van Dam A, et al. Internet-Based cognitive behavioral therapy in stepped care for chronic fatigue syndrome: randomized noninferiority trial. J Med Internet Res. 2019;21(3):e11276. doi:10.2196/11276
102. Daniels S. Cognitive behavior therapy for patients with cancer. J Advanc Practitioner Oncol. 2015;6(1):54–56.
103. Turner J, Mancl L, Aaron L. Brief cognitive-behavioral therapy for temporomandibular disorder pain: effects on daily electronic outcome and process measures. Pain. 2005;117(3):377–387. doi:10.1016/j.pain.2005.06.025
104. Cai L, Gao H, Xu H, et al. Does a program based on cognitive behavioral therapy affect kinesiophobia in patients following total knee arthroplasty? A randomized, controlled trial with a 6-month follow-up. J Arthroplasty. 2018;33(3):704–710. doi:10.1016/j.arth.2017.10.035
105. Turner JA, Holtzman S, Mancl L. Mediators, moderators, and predictors of therapeutic change in cognitive-behavioral therapy for chronic pain. Pain. 2007;127(3):276–286. doi:10.1016/j.pain.2006.09.005
106. Turner JA, Mancl L, Aaron LA. Short- and long-term efficacy of brief cognitive-behavioral therapy for patients with chronic temporomandibular disorder pain: a randomized, controlled trial. Pain. 2006;121(3):181–194. doi:10.1016/j.pain.2005.11.017
107. Sanson N, Hach S, Moran R, et al. Behavioural activation and inhibition systems in relation to pain intensity and duration in a sample of people experiencing chronic musculoskeletal pain. Musculoskelet Sci Pract. 2020;47:102129. doi:10.1016/j.msksp.2020.102129
108. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, et al. Which interventions enhance pain self-efficacy in people with chronic musculoskeletal pain? A systematic review with meta-analysis of randomized controlled trials, including over 12 000 participants. J Orthop Sports Phys Ther. 2020;50(8):418–430. doi:10.2519/jospt.2020.9319
109. Lin J, Scott W, Carpenter L, et al. Acceptance and commitment therapy for chronic pain: protocol of a systematic review and individual participant data meta-analysis. Syst Rev. 2019;8(1):140. doi:10.1186/s13643-019-1044-2
110. McCracken L, DaSilva P, Skillicorn B, et al. The cognitive fusion questionnaire: a preliminary study of psychometric properties and prediction of functioning in chronic pain. Clin J Pain. 2014;30(10):894–901. doi:10.1097/AJP.0000000000000047
111. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4(1):33–47. doi:10.1016/0163-8343(82)90026-3
112. Andres-Rodriguez L, Borràs X, Feliu-Soler A, et al. Immune-inflammatory pathways and clinical changes in fibromyalgia patients treated with Mindfulness-Based Stress Reduction (MBSR): a randomized, controlled clinical trial. Brain Behav Immun. 2019;80:109–119. doi:10.1016/j.bbi.2019.02.030
113. Bernardy K, Füber N, Köllner V, et al. Efficacy of cognitive-behavioral therapies in fibromyalgia syndrome - a systematic review and metaanalysis of randomized controlled trials. J Rheumatol. 2010;37(10):1991. doi:10.3899/jrheum.100104
114. Darnall BD, Roy A, Chen AL, et al. Comparison of a single-session pain management skills intervention with a single-session health education intervention and 8 sessions of cognitive behavioral therapy in adults with chronic low back pain: a randomized clinical trial. JAMA Network Open. 2021;4(8):e2113401. doi:10.1001/jamanetworkopen.2021.13401
115. Veehof M, Trompetter HR, Bohlmeijer ET, et al. Acceptance- and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cognitive Behav Ther. 2016;45(1):5–31. doi:10.1080/16506073.2015.1098724
116. Turner JA, Anderson ML, Balderson BH, et al. Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial. Pain. 2016;157(11):2434–2444. doi:10.1097/j.pain.0000000000000635
117. Dorta DC, Colavolpe PO, Lauria PSS, et al. Multimodal benefits of hypnosis on pain, mental health, sleep, and quality of life in patients with chronic pain related to fibromyalgia: a randomized, controlled, blindly-evaluated trial. Explore. 2024;20(6):103016. doi:10.1016/j.explore.2024.103016
118. Jensen MP, Patterson DR. Hypnotic approaches for chronic pain management: clinical implications of recent research findings. Am Psychol. 2014;69(2):167–177. doi:10.1037/a0035644
119. Gifford L. Pain, the tissues and the nervous system: a conceptual model. Physiotherapy. 1998;84(1):27–36. doi:10.1016/S0031-9406(05)65900-7
120. Robinson V, King R, Ryan CG, et al. A qualitative exploration of people’s experiences of pain neurophysiological education for chronic pain: the importance of relevance for the individual. Manual Ther. 2016;22:56–61. doi:10.1016/j.math.2015.10.001
121. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807–813. doi:10.1016/j.jpain.2015.05.005
122. Moseley GL, Butler DS. Explain Pain Supercharged. The Clinician’s Handbook. Vol. 1. Painos. Australia: Noigroup publication. Liite; 2017:1.
123. Zimney K, Louw A, Puentedura EJ. Use of therapeutic neuroscience education to address psychosocial factors associated with acute low back pain: a case report. Physiother Theor Pract. 2014;30(3):202–209. doi:10.3109/09593985.2013.856508
124. Ryan CG, Gray HG, Newton M, et al. Pain biology education and exercise classes compared to pain biology education alone for individuals with chronic low back pain: a pilot randomised controlled trial. Manual Ther. 2010;15(4):382–387. doi:10.1016/j.math.2010.03.003
125. Colleary G, O’Sullivan K, Griffin D, et al. Effect of pain neurophysiology education on physiotherapy students’ understanding of chronic pain, clinical recommendations and attitudes towards people with chronic pain: a randomised controlled trial. Physiotherapy. 2017;103(4):423–429. doi:10.1016/j.physio.2017.01.006
126. Clarke CL, Ryan CG, Martin DJ. Pain neurophysiology education for the management of individuals with chronic low back pain: a systematic review and meta-analysis. Manual Ther. 2011;16(6):544–549. doi:10.1016/j.math.2011.05.003
127. Nijs J, Paul van Wilgen C, Van Oosterwijck J, et al. How to explain central sensitization to patients with ‘unexplained’chronic musculoskeletal pain: practice guidelines. Manual Ther. 2011;16(5):413–418. doi:10.1016/j.math.2011.04.005
128. Watson JA, Ryan CG, Cooper L, et al. Pain neuroscience education for adults with chronic musculoskeletal pain: a mixed-methods systematic review and meta-analysis. J Pain. 2019;20(10):1140.e1–1140.e22. doi:10.1016/j.jpain.2019.02.011
129. Barrenengoa-Cuadra MJ, Muñoa-Capron-Manieux M, Fernández-Luco M, et al. Effectiveness of a structured group intervention based on pain neuroscience education for patients with fibromyalgia in primary care: a multicentre randomized open-label controlled trial. Eur J Pain. 2021;25(5):1137–1149. doi:10.1002/ejp.1738
130. van Ittersum MW, van Wilgen CP, van der Schans CP, et al. Written pain neuroscience education in fibromyalgia: a multicenter randomized controlled trial. Pain Pract. 2014;14(8):689–700. doi:10.1111/papr.12137
131. Amer-Cuenca JJ, Pecos-Martín D, Martínez-Merinero P, et al. How much is needed? Comparison of the effectiveness of different pain education dosages in patients with fibromyalgia. Pain Med. 2019;21.
132. Louw A, Zimney K, Puentedura EJ, et al. The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiother Theory Pract. 2016;32(5):332–355. doi:10.1080/09593985.2016.1194646
133. Aguirrezabal I, De San Román MS, Cobos-Campos R, et al. Effectiveness of a primary care-based group educational intervention in the management of patients with migraine: a randomized controlled trial. Primary Health Care Res Develop. 2019;20.
134. Bidonde J, Busch AJ, Schachter CL, et al. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst Rev. 2017;6(6):Cd012700. doi:10.1002/14651858.CD012700
135. Miyamoto GC, Lin C-WC, Cabral CMN, et al. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: a systematic review with meta-analysis. Br J Sports Med. 2019;53(3):172–181. doi:10.1136/bjsports-2017-098765
136. Ambrose KR, Golightly YM. Physical exercise as non-pharmacological treatment of chronic pain: why and when. Best Pract Res Clin Rheumatol. 2015;29(1):120–130.
137. Vlaeyen JW, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
138. Society BT. Scottish intercollegiate guidelines network. In: British Guideline on the Management of Asthma. 2016:58.
139. Pedersen BK. Anti-inflammatory effects of exercise: role in diabetes and cardiovascular disease. Eur J Clin Invest. 2017;47(8):600–611. doi:10.1111/eci.12781
140. Gleeson M, Bishop NC, Stensel DJ, et al. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat Rev Immunol. 2011;11(9):607–615. doi:10.1038/nri3041
141. Petersen AM, Pedersen BK. The anti-inflammatory effect of exercise. J Appl Physiol. 2005;98(4):1154–1162. doi:10.1152/japplphysiol.00164.2004
142. Scheffer DDL, Latini A. Exercise-induced immune system response: anti-inflammatory status on peripheral and central organs. Biochim Biophys Acta Mol Basis Dis. 2020;1866(10):165823. doi:10.1016/j.bbadis.2020.165823
143. McCracken LM, Carson JW, Eccleston C, et al. Acceptance and change in the context of chronic pain. Pain. 2004;109(1–2):4–7. doi:10.1016/j.pain.2004.02.006
144. Tran ST, Guite JW, Pantaleao A, et al. Preliminary outcomes of a cross-site cognitive-behavioral and neuromuscular integrative training intervention for juvenile fibromyalgia. Arthritis Care Res. 2017;69(3):413–420. doi:10.1002/acr.22946
145. Giannotti E, Koutsikos K, Pigatto M, et al. Medium-/long-term effects of a specific exercise protocol combined with patient education on spine mobility, chronic fatigue, pain, aerobic fitness and level of disability in fibromyalgia. Biomed Res Int. 2014;2014:474029. doi:10.1155/2014/474029
146. Ang DC, Kaleth AS, Bigatti S, et al. Research to Encourage Exercise for Fibromyalgia (REEF): use of motivational interviewing design and method. Contemp Clin Trials. 2011;32(1):59–68. doi:10.1016/j.cct.2010.08.014
147. Rice D, Nijs J, Kosek E, et al. Exercise-induced hypoalgesia in pain-free and chronic pain populations: state of the art and future directions. J Pain. 2019;20(11):1249–1266. doi:10.1016/j.jpain.2019.03.005
148. Marris D, Theophanous K, Cabezon P, et al. The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: a systematic review and meta-analysis of randomized controlled trials. Physiother Theory Pract. 2021;37(4):461–472. doi:10.1080/09593985.2019.1633714
149. Luque-Suarez A, Martinez-Calderon J, Falla D. Role of kinesiophobia on pain, disability and quality of life in people suffering from chronic musculoskeletal pain: a systematic review. Br J Sports Med. 2019;53(9):554–559. doi:10.1136/bjsports-2017-098673
150. Preuß M, Nieuwenhuijsen M, Marquez S, et al. Low childhood nature exposure is associated with worse mental health in adulthood. Int J Environ Res Public Health. 2019;16(10):1809. doi:10.3390/ijerph16101809
151. Trøstrup CH, Christiansen AB, Stølen KS, et al. The effect of nature exposure on the mental health of patients: a systematic review. Qual Life Res. 2019;28(7):1695–1703. doi:10.1007/s11136-019-02125-9
152. Zijlema WL, Avila-Palencia I, Triguero-Mas M, et al. Active commuting through natural environments is associated with better mental health: results from the PHENOTYPE project. Environ Int. 2018;121:721–727. doi:10.1016/j.envint.2018.10.002
153. Carson JW, Carson KM, Jones KD, et al. Follow-up of yoga of awareness for fibromyalgia: results at 3 months and replication in the wait-list group. Clin J Pain. 2012;28(9):804–813. doi:10.1097/AJP.0b013e31824549b5
154. Campo AR, Pacichana-Quinayáz SG, Bonilla-Escobar FJ, et al. Effectiveness of hydrotherapy on neuropathic pain and pain catastrophization in patients with spinal cord injury: protocol for a pilot trial study. JMIR Res Protoc. 2022;11(4):e37255. doi:10.2196/37255
155. Zhang YJ, Wang C. Acupuncture and Chronic Musculoskeletal Pain. Curr Rheumatol Rep. 2020;22(11):80. doi:10.1007/s11926-020-00954-z
156. Vicente-Mampel J, Bautista IJ, Salvat I, et al. Dry needling in people with fibromyalgia: a randomized controlled trial of its effects on pain sensitivity and pain catastrophizing influence. Pm r. 2025;17(4):419–430. doi:10.1002/pmrj.13289
157. Ceballos-Laita L, Medrano-de-la-Fuente R, Mingo-Gómez MT, et al. Effects of dry needling on pain, disability, kinesiophobia, pain catastrophizing and psychological distress in patients with chronic neck pain: a randomized controlled pilot study. J Back Musculoskelet Rehabil. 2022;35(2):393–401. doi:10.3233/BMR-200322
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.