Back to Journals » Journal of Pain Research » Volume 19
Pain as Lived Experience: Philosophical Perspectives in Pain Medicine – A Narrative Review
Received 30 October 2025
Accepted for publication 21 February 2026
Published 26 February 2026 Volume 2026:19 577740
DOI https://doi.org/10.2147/JPR.S577740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Andrea Tinnirello
Dong Ah Shin,1 Min Cheol Chang2
1Department of Neurosurgery, Yonsei University College of Medicine, Seoul, Republic of Korea; 2Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daegu, Republic of Korea
Correspondence: Min Cheol Chang, Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, 317-1 Daemyungdong, Namku, Daegu, 705-717, Republic of Korea, Tel +82-53-620-4862, Email [email protected]
Abstract: Pain is a prevalent clinical complaint that often defies explanation within conventional biomedical frameworks, particularly in chronic and idiopathic conditions, frequently leading to patient invalidation and inadequate care. We evaluate the potential of philosophy to expand the understanding of pain beyond biological reductionism by conceptualizing pain as a lived experience. This narrative review aims to integrate key philosophical perspectives with contemporary pain medicine and to examine their relevance for clinical practice. A narrative review of philosophical and medical literature was conducted, focusing on phenomenology, existential philosophy, philosophy of language, biopolitics, and neurophilosophy. These frameworks conceptualize pain as a disruption of embodied existence, a challenge to identity and autonomy, a phenomenon that resists full linguistic expression, a condition shaped by institutional and sociopolitical structures, and an inferential process influenced by prior experience and context. Together, these perspectives suggest that effective pain management requires more than symptom reduction and objective measurement. Attending to patients’ lived experiences may strengthen therapeutic alliances, enhance clinical communication, and support more ethical, person-centered, and clinically meaningful approaches to pain care.
Keywords: pain, phenomenology, existential philosophy, biopolitics, neurophilosophy, medicine
Introduction
Despite being a common source of human suffering and one of the reasons patients most frequently cite for seeking medical care, pain remains one of the least understood clinical phenomena. Despite its ubiquity, pain often resists straightforward diagnostic classification or treatment, particularly when chronic and idiopathic.1
While acute nociceptive pain, arising from tissue injury or inflammation, is generally well understood within the biomedical paradigm, chronic pain often escapes this framework. Patients with conditions, such as fibromyalgia, complex regional pain syndrome (CRPS), or other medically unclear pain syndromes frequently report invalidation, stigmatization, and frustration when their pain cannot be explained by imaging findings or measurable biomarkers.2,3
The mismatch between patients’ complaints and received medical explanations has profound consequences, not only undermining the therapeutic alliance but also exposing a blind spot within modern medicine. Pain often becomes most debilitating when it eludes objective verification.4 Under these circumstances, the limitations of the biomedical model become apparent because the absence of objective biomarkers of pain does not guarantee the absence of pain. Pain is not simply a physiological malfunction but a lived experience that demands interpretation and philosophical insight.5
This paper argues that philosophy provides indispensable tools to address these limitations. Pain is not simply a neurophysiological event but a lived, embodied, and meaning-laden experience. Philosophical traditions such as phenomenology, existentialism, philosophy of language, biopolitics, and neurophilosophy offer conceptual frameworks that expand our understanding of pain beyond that provided by medical science. By integrating these perspectives into clinical practice, medicine can move closer to honoring the full reality of pain, thereby restoring patient dignity, fostering ethical responsiveness, and improving therapeutic outcomes.
Our goal is not to replace medical science with philosophy but to propose a synthesis of the two—a humanistic medicine in which scientific precision and philosophical depth converge. This work advocates for approaching pain not merely as a symptom to be eliminated but as a phenomenon that demands recognition, interpretation, and accompaniment.
Despite advances in contemporary pain models, important challenges remain in explaining persistent pain without clear pathology and in translating theoretical frameworks into individualized clinical care. This review addresses this gap by synthesizing philosophical perspectives and clarifying their concrete relevance to pain medicine. We will first discuss the limits of modern medicine, then examine the perspectives of phenomenology, existential philosophy, philosophy of language, biopolitics, and neurophilosophy in turn, and finally discuss how these perspectives can be integrated into clinical practice.
Positioned alongside integrative models such as the biopsychosocial and narrative approaches, this narrative review offers a philosophically grounded synthesis of selected traditions relevant to clinical pain experience.
Limits of Modern Medical Approaches
Modern medicine has been remarkably successful in elucidating the biological mechanisms of many diseases. The discovery of nociceptors, the process of peripheral and central sensitization, and neurochemical mediators has enabled clinicians to more effectively manage pain related to tissue damage or inflammation. Analgesics, anti-inflammatory drugs, interventional procedures, and surgical strategies provide effective relief in many cases of nociceptive pain.6
However, chronic pain exposes the limitations of this paradigm. Patients often experience persistent suffering in the absence of identifiable pathology or have a reported pain severity disproportionate to observable injury. Conditions such as fibromyalgia and CRPS have historically been dismissed as “psychogenic” or “functional” precisely because they do not fit within established biomedical categories. The diagnostic classifications intended to provide clarity—“idiopathic”, “functional”, “somatoform”—often obscure more than they reveal, serving as placeholders for ignorance rather than explanations. For patients, these labels can be devastating, indicating that the medical establishment views their pain as “not real” or “mild,” which erodes trust in clinicians and the healthcare systems in which they work.
Modern medicine tends to equate truth with visibility and measurability. What can be imaged, quantified, or biochemically verified is considered legitimate, while subjective reports are relegated to secondary status. Therefore, pain that is not objectively verified is overlooked, not because it is unreal, but because it exceeds the limits of the epistemic frame. Philosophically, this constitutes a crisis of knowledge. Modern medicine, while invaluable, is incomplete. To address this incompleteness, clinical reasoning should evolve to include phenomenological and narrative approaches. Phenomenological understanding emphasizes how pain is experienced by the patient, attending to its subjective structures rather than its physiological correlates.7 Narrative understanding situates pain within the arc of a patient’s personal story, tracing its development, context, and meaning over time.8 The application of this approach does not diminish the importance of scientific inquiry. Rather, it deepens it by restoring dimensions of pain that science alone cannot capture.
Clinically, the consequences of neglecting this perspective could be severe. When pain is dismissed or inadequately addressed, patients may withdraw from the healthcare system, turn to unregulated treatments, or develop secondary psychiatric conditions such as depression or anxiety. Conversely, clinicians can strengthen therapeutic alliances and improve adherence to treatment by engaging with patients’ narratives and validating their suffering. Pain requires an epistemology broad enough to include subjective experience alongside objective measurement (Table 1).
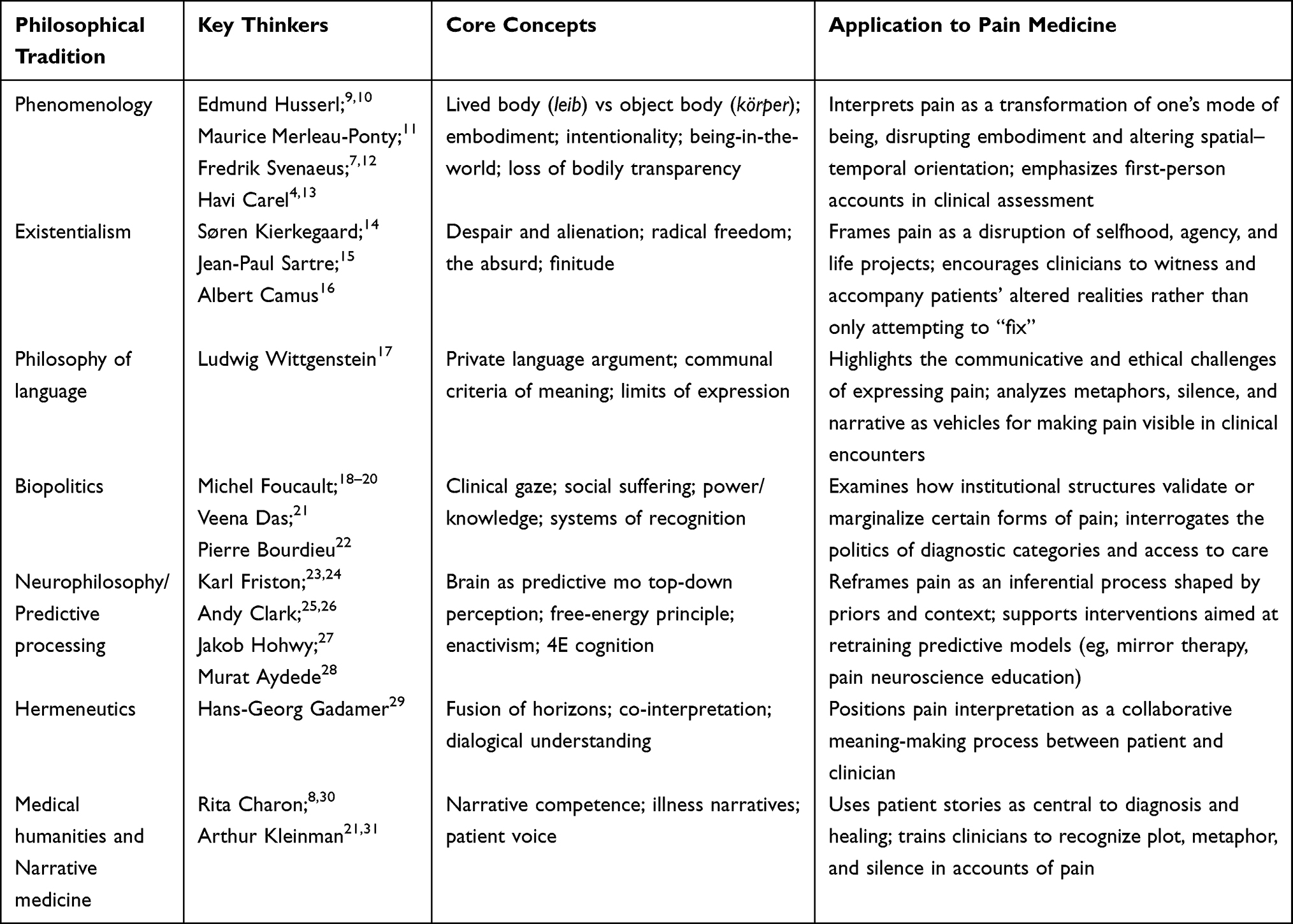 |
Table 1 Philosophical Traditions Referenced in This Study and Their Relevance to Pain Medicine |
Phenomenology and the Lived Structure of Pain
Phenomenology, first introduced by Edmund Husserl and later expanded on by Maurice Merleau-Ponty, offers a philosophical method for understanding human experience that starts not with abstract theorizing or empirical data, but with the structures of consciousness as they appear to the experiencing subject.9,11 Husserl emphasized the importance of bracketing naturalistic assumptions to ask not only “What causes pain?” but also “What is it like to live through pain?” This shift reframes pain as a phenomenon that must be described in its subjective complexity, not merely explained in objective terms. Merleau-Ponty deepened this perspective by asserting that the body is not simply a mechanical object but the condition of being-in-the-world,11 which pain profoundly disrupts.32 Actions that once felt effortless—walking, breathing, typing—may suddenly become burdensome or even impossible when in pain.13
One central insight of phenomenology is that pain can cause the loss of bodily transparency. In everyday life, the body usually recedes into the background, enabling us to act without consciousness awareness of it. However, pain makes the body hyper-present, bringing it into sharp focus as an intrusive object that dominates awareness. This transformation from the lived body (leib), where the body is experienced as part of the self and taken for granted, to the objectified suffering body (körper), where the body is viewed as an external object of pain, is not merely a semantic distinction.10 Rather, it represents a profound existential shift in how one inhabits the world—pain disrupts the seamless integration of body and self, turning the body into something alien and hostile. Clinically, this perspective highlights the limitations of conventional pain assessments, such as numeric rating scales or localization charts. Patients often describe their suffering in existential terms: “It feels like my body no longer belongs to me,” or “I feel as though I am being dissolved from the inside.” Such statements are not simply metaphors but reflect ontological realities that demand interpretation.
A phenomenological approach calls for a kind of listening that attends not only to symptoms but to the shape of suffering as it unfolds in speech, silence, gesture, and relational withdrawal.12 It suggests the need for a clinical practice that is not merely diagnostic but hermeneutic, recognizing that pain is embedded in narrative, shaped by memory, trauma, expectation, and context. It also demands that practitioners be trained in philosophical sensitivity—not to turn them into philosophers, but to enhance their ability to respond to patients’ pain with deep understanding. Clinically, this perspective supports incorporating narrative descriptions and functional disruption into pain assessment, complementing numerical pain scales with attention to how pain alters patients’ every activities and bodily experience.
Existential Philosophy: Pain as a Condition of Being
Existential philosophy regards suffering not as an accidental disruption of human life but as a fundamental part of existence. Philosophers such as Søren Kierkegaard, Jean-Paul Sartre, and Albert Camus emphasized that pain—whether physical, psychological, or existential—forces us to inevitably confront the limits and fragility of human existence.14–16 From this perspective, pain is not simply a medical symptom but a profound challenge to one’s selfhood, agency, and continuity of being.
Kierkegaard described despair as a condition of being estranged from oneself.14 Accordingly, individuals with chronic pain often experience a rupture between their former identity and their present reality: “I used to be a runner; now I am only a patient,” or “I don’t recognize the person I’ve become.” This disruption is not merely psychological but existential, producing a sense of despair rooted in the collapse of personal continuity.
Sartre’s philosophy further complicates our understanding of pain. He argued that human beings are “condemned to be free”—always faced with the necessity of choosing, even within constraints.15 However, chronic pain undermines this freedom by shrinking the possible choices. Pain narrows the world, paralyzes intentionality, and reduces agency, leaving once-independent people dependent on caregivers, medications, or institutions. In this sense, the burden of pain lies not only in suffering itself but also in the erosion of autonomy.
Camus highlighted the absurdity of human existence, particularly our impulse to search for meaning in an inherently meaningless world. Unexplained or incurable pain exemplifies this absurdity.16 Patients frequently ask, “Why me?” or “What did I do to deserve this?”—questions that echo without answers. For Camus, the task is not to resolve the absurd but to endure it: “One must imagine Sisyphus happy.” Translated into clinical care, this means affirming the patient’s right to suffer without justification and to demand care even in the absence of a clear explanation.
The existential perspective urges clinicians to acknowledge the ontological dimension of pain. Patients are not simply malfunctioning organisms; they are persons navigating disrupted projects, fractured futures, and altered relationships. Silence, hesitation, or gestures of withdrawal may communicate as much as spoken words, revealing the depth of existential rupture.12
Importantly, in the medical context, existential engagement does not mean romanticizing suffering. Rather, it involves resisting the temptation to dismiss pain with quick medical fixes or rationalizations.33 Existential care involves dwelling with the patient’s altered reality, bearing witness to their struggle, and honoring the moral weight of their endurance. Healing, in this sense, may not mean eliminating pain but reconstructing meaning, restoring authorship, and reestablishing the possibility of being-with-others despite suffering.
In sum, existential philosophy teaches that pain is not only what hurts—it is what disrupts being one’s self. Addressing pain, therefore, requires more than symptom relief; it requires an ethical commitment to helping patients renegotiate meaning, identity, and presence in the midst of their suffering. In clinical practice, this approach encourages clinicians to address changes in identity, autonomy, and life roles during patient interviews, rather than focusing solely on symptom severity.
Philosophy of Language: Pain, Expression, and the Limits of Understanding
Patients commonly report that “no one can really understand what I’m feeling,” or “words don’t capture it.” These expressions are not failures of articulation; they are disclosures of the inherent limits of language when applied to bodily suffering. The philosophy of language—particularly as developed by Ludwig Wittgenstein—offers a framework for understanding these limits and their clinical implications.
Wittgenstein explores the idea of a “private language”—a language whose meanings are accessible only to the speaker.17 He argues that such a language is incoherent because the very concept of meaning presupposes shared public criteria. Pain, however, occupies a peculiar space in this framework. The utterance “I am in pain” is both a subjective report and a social signal. Yet, no external test can verify the content of that utterance. The experience of pain is essentially private: only the person who feels it can truly know it, while others can at best make inferences about it from external signs. This asymmetry creates communicative challenges in clinical settings. Clinicians should make judgments about the reality and severity of pain based on verbal and non-verbal cues—tone of voice, facial expression, posture—but these are not infallible indicators. Some patients may underreport pain due to cultural stoicism; others may overemphasize it out of desperation.34,35 Metaphorical language often emerges in this gap. Patients say things like “It feels like being stabbed with ice,” “My bones are screaming,” or “It’s like fire crawling under my skin.” These metaphors are not poetic excesses; they are attempts to render visible what is invisible, translating the ineffable into a shared experiential framework. Yet, all too often, clinical documentation reduces such language to vague descriptors or omits it altogether, privileging numerical pain scores over narrative specificity.36
Wittgenstein also draws attention to the communal aspect of language: the fact that pain expressions acquire meaning through social use. In this light, pain is not a private event but a relational one.17 To express pain is to make a claim on the other—to request acknowledgment, care, and sometimes, intervention. When such expressions are ignored, the person in pain may experience a denial of the credibility of their suffering.5
Clinicians must, therefore, cultivate a heightened sensitivity to the linguistic textures of pain. This approach involves listening for what is said, how it is said, and what remains unsaid, because silence can be as informative as speech. The refusal or inability to articulate pain may signal emotional trauma, social isolation, or mistrust of the medical system. Thus, beyond merely decoding symptoms, understanding pain requires interpreting expressions as situated acts of meaning-making.
To improve clinical responsiveness, training in narrative medicine and interpretive listening should be integrated into healthcare education.8,37 Encouraging patients to describe their pain in their own words—not just to rate it on a numerical scale—can reestablish their agency and deepen clinician empathy. The goal is not to “solve” the language problem of pain, but to acknowledge its complexity and respond to it with humility and attentiveness. The philosophy of language suggests that the pain symptoms expressed by the patient should not be seen merely as a description of sensation, but as a form of communication. Moreover, like all forms of communication, it depends on trust, reciprocity, and recognition. This framework highlights the importance of attending to patients’ metaphor, silences, and narrative patterns during consultations, thereby improving doctor-patient communication and reducing misinterpretation of pain reports.
Biopolitics: What Pain or Whose Pain Counts?
The experience of pain is not only biological or personal—it is also political.18 Michel Foucault’s concept of biopolitics offers a critical framework for examining how institutions, policies, and discourses govern the body, particularly in medical contexts.18 Pain, from this perspective, is not simply a physiological phenomenon to be measured and treated but also a matter of power, shaped by regulation, visibility, and legitimacy.18 Some forms of pain are recognized, recorded, and reimbursed.18 Others are ignored, silenced, or pathologized—not because they are less real, but because they fall outside the categories that can be biomechanically explained.18
Foucault describes how modern medicine emerged alongside mechanisms of surveillance, standardization, and documentation.18 The clinical gaze transforms the patient from a person to a case, from a subject to a body to be examined.19 Pain, in this context, becomes real only when it is codified—when it appears on a diagnostic chart, fits an ICD code, or triggers an insurance claim. Invisible pain, or pain without a clear etiology, thus becomes institutionally nonexistent,19 resulting in what anthropologist Veena Das calls “social suffering”—pain that is intensified by structural neglect.38
One of the most insidious forms of biopolitical exclusion occurs through diagnostic ambiguity. Conditions such as fibromyalgia and CRPS have historically been met with skepticism, resulting in underfunding for related research. Patients with these diagnoses often face a double bind: their symptoms are debilitating, but their legitimacy is questioned. Their pain becomes not only untreated but also unrecognized, leading to secondary trauma.
Foucault also introduced the idea that modern power operates not by repression but by management.21 Health becomes not only a right but a duty of the state, where the body is monitored, normalized, and optimized.18,21 Within this framework, pain that disrupts productivity, deviates from statistical norms, or complicates standard treatment pathways becomes a bureaucratic nuisance. The unclassifiable patient becomes a burden, and their narrative is dismissed through administrative silence.
This biopolitical lens reveals how clinical neutrality often fails to be actualized. Medical categories are shaped by funding priorities, pharmaceutical interests, legal standards, and cultural narratives.20 For instance, military veterans in some countries receive robust pain management resources, while low-income women of color with similar symptoms may be dismissed as drug-seeking or hysterical.39,40
To resist these patterns, clinicians and policymakers must recognize the institutional structures that frame pain visibility.41 This includes advocating for more inclusive diagnostic criteria, expanding research funding for under-recognized conditions, and training providers to detect and correct for implicit biases.40 Interdisciplinary pain clinics should include social workers, ethicists, and patient advocates who can amplify marginalized voices and intervene in systems of exclusion.39
Moreover, healthcare systems should develop mechanisms to record and respond to pain narratives that fall outside conventional metrics.8 This might involve qualitative documentation, narrative summaries, or ethical review panels for contested cases.22 By restoring narrative complexity to clinical assessment, medicine can resist reductionism and reengage with its central moral imperative: to care for those who suffer.13 Biopolitics shows us that pain is never purely personal—it is structured by systems of recognition. Accordingly, clinicians should not abandon medical rigor but, rather, apply it more equitably. From a clinical perspective, this lens calls for greater awareness of diagnostic bias and institutional barriers, encouraging more equitable recognition and documentation of pain experiences.
Neurophilosophy and Predictive Processing: The Constructed Nature of Pain
In recent decades, cognitive neuroscience has increasingly converged with philosophical inquiry, giving rise to neurophilosophy—a discipline concerned with the philosophical implications of brain function.42 One of the most influential paradigms within this field is the predictive processing framework, developed by Karl Friston23,25,43 and elaborated by thinkers such as Andy Clark and Jakob Hohwy.24,26 This model proposes that perception, including the perception of pain, is not a passive reception of sensory data but an active, top-down process in which the brain continuously generates predictions about incoming stimuli and minimizes error signals between expected and actual inputs.
In this framework, pain is not simply the result of noxious stimuli traveling from the periphery to the brain; rather, it emerges from the interaction between sensory inputs and expectations from prior experiences.24–26 This interpretation reconfigures our understanding of pain from a bottom-up alarm system to a dynamic inferential process, where pain results from persistent prediction errors, hyperactive prior beliefs about threat or damage, or a failure to update the brain’s model of the body in response to new sensory data.27,44
This paradigm aligns with and deepens phenomenological accounts of embodiment. Where Merleau-Ponty emphasizes the lived body’s openness to the world, predictive processing explains how that openness is mediated by the brain’s anticipatory structures.24,25 When in pain, this mediation becomes dysfunctional. For instance, in individuals experiencing phantom limb pain, the brain continues to predict sensory input from a limb that has been amputated or otherwise removed, generating a dissonant perceptual experience.27 Similarly, in individuals with fibromyalgia or CRPS, heightened vigilance and defensive postures may be embedded in the brain’s priors, perpetuating pain even in the absence of new injury.45
This theory has substantial clinical implications: it supports interventions aimed at retraining the brain’s predictions, such as graded motor imagery,27 mirror therapy,46 virtual reality rehabilitation,47 and cognitive-behavioral techniques focused on expectation modulation.48 These treatments do not merely suppress symptoms; they attempt to revise the predictive models that generate those symptoms. This approach marks a shift from treating the body as a passive site of injury to engaging the mind–body system as a learning organism.
Moreover, predictive processing challenges dualistic models that separate mind and body, or psyche and soma, encouraging us to view pain as a distributed, embodied, and interpretive phenomenon. Research suggests that pain perception is shaped by the interaction between the brain, body, and environment.49,50 Thus, pain is not confined to being “in the head” or “in the tissue” but exists in the dynamic relation between the organism and the world.28,51,52 This perspective allows for a conception of pain that is both biologically grounded and experientially rich.53,54 It also underscores the importance of context—social, emotional, environmental—in shaping how pain is felt, interpreted, and endured.53–55
Clinicians who adopt this model must be prepared to treat not only tissues but beliefs, habits, and environments.28,54 In this context, pain education becomes a vital therapeutic tool, empowering patients to understand that although their pain is real, it is also modifiable and treatable.56,57 In summary, neurophilosophy and predictive processing provide a scientifically rigorous yet deeply human framework for understanding pain, revealing it to be an ongoing negotiation between brain, body, and world—one that can go awry, but also one that can be reshaped through insight, care, and adaptive learning. Clinically, this model supports interventions that target maladaptive expectations and predictive processes, such as pain neuroscience education and graded exposure-based rehabilitation.
Toward Integration: Philosophical Tools for Clinical Practice
Having examined pain through various philosophical lenses—phenomenology, existentialism, language philosophy, biopolitics, and neurophilosophy—we now turn to the question of integration: How can these diverse frameworks be synthesized into a meaningful and actionable model for clinical practice? Although these philosophical traditions differ in their assumptions and methods, they are not mutually exclusive and often illuminate complementary dimensions of pain. Tensions between subjective experience, linguistic expression, sociopolitical structures, and neurobiological models highlight the need for an integrative framework rather than a single explanatory approach.
The first step toward integration is to practice epistemological humility. Clinicians must acknowledge that medical science, while powerful, does not completely explain pain. Objective markers, laboratory tests, and imaging scans cannot fully capture what it means to hurt,45 rendering them incomplete. Philosophical thinking can cultivate in clinicians the capacity to sit with ambiguity, to tolerate uncertainty, and to recognize that truth in medicine often emerges through dialogue, narrative, and moral imagination rather than algorithmic thinking alone.8,38
Philosophy encourages what Hans-Georg Gadamer called a “fusion of horizons” —a meeting point between the world of the clinician and that of the patient.58 Pain, in this hermeneutic context, is not simply to be interpreted through the clinician’s lens; it requires co-interpretation. This approach demands time, attentiveness, and a deep commitment to understanding patients’ lived experience with pain. Clinicians should actively listen, ask open-ended questions, and remain present, fostering a space where the patient feels heard and that their pain is taken seriously. It involves recognizing the nuances of a patient’s narrative, being sensitive to the emotional and existential aspects of their suffering, and engaging in a continuous dialogue that goes beyond just diagnosing symptoms.
One promising approach is narrative medicine, which views the patient’s story not as an accessory to the diagnosis but as a central component of healing.8,38 Training in narrative competence helps clinicians recognize plot, metaphor, voice, and silence in patient accounts.8,22 This approach is not only ethically sensitive but also diagnostically useful, often revealing patterns and meanings that elude biomedical logic.22 Philosophy deepens this practice by offering conceptual tools to interpret the existential, political, and epistemological dimensions embedded in each story.38
Moreover, philosophy can inform institutional reform. Healthcare systems often reward speed, certainty, and efficiency over reflection, ambiguity, and empathy.29,59,60 Philosophical integration challenges this logic by asserting that slowness, uncertainty, and attentiveness are not inefficiencies—they are forms of care.60,61 Interdisciplinary pain clinics might include not only physicians, psychologists, and physiotherapists but also ethicists, medical humanists, and even philosophers.30,31 Rather than merely theorizing from a distance, their role is to actively engage in case discussions, help debrief challenging situations, and create spaces for reflection within institutions.29,30,59 Lastly, integration requires an ontological shift. Rather than seeing the body as a malfunctioning machine and the patient as a bearer of problems, clinicians might begin to see patients as meaning-making beings embedded in social, cultural, and existential worlds.11,13,33 Pain, in this model, is not only a disruption of tissue but a rupture in worldhood.7,13 Responding to it effectively requires not simply medical intervention but also ethical accompaniment.7,33
Rather than reject medical science, philosophical integration humanizes it. It offers clinicians expanded tools for understanding, communicating, and responding to pain while fostering humility, curiosity, and ethical depth. Above all, it reaffirms that medicine is not only a science of the body but also a craft of meaning and a discipline of presence.
Contemporary pain medicine has made substantial advances, particularly in areas such as nociplastic pain, interdisciplinary pain management, and translational neuroscience. The philosophical perspectives discussed here are intended not to correct biomedical models, but to complement and conceptually enrich these ongoing developments.
Conclusions
This narrative review explored pain through multiple philosophical frameworks, including phenomenology, existential philosophy, philosophy of language, biopolitics, and neurophilosophy, emphasizing pain as a lived and context-dependent experience beyond biological reductionism. These perspectives offer complementary insights into how pain affects embodiment, identity, communication, and clinical recognition. Clinically, integrating these frameworks may enhance pain assessment, patient communication, and person-centered care, while conceptually supporting contemporary pain research where existing models remain limited. By systematically linking philosophical analysis with pain medicine, this review provides a novel interdisciplinary perspective with clear relevance to both clinical practice and future research. These philosophical insights suggest practical implications for clinicians and educators, particularly in pain assessment, communication, and training that more fully acknowledge patients’ lived experiences. At the same time, this review is limited by its conceptual scope and does not claim empirical validation, underscoring the need for future interdisciplinary research.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest related to this work.
References
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–9. doi:10.1016/j.ejpain.2005.06.009
2. Lobo CP, Pfalzgraf AR, Giannetti V, Kanyongo G. Impact of invalidation and trust in physicians on health outcomes in fibromyalgia patients. Prim Care Companion CNS Disord. 2014;16(5): doi:10.4088/PCC.14m01664
3. Tan AC, Jaaniste T, Champion D. Chronic widespread pain and fibromyalgia syndrome: life-course risk markers in young people. Pain Res Manag. 2019;2019:6584753. doi:10.1155/2019/6584753
4. Carel H. Illness: The Cry of the Flesh.
5. Jackson JE. Stigma, liminality, and chronic pain: mind–body borderlands. American Ethnologist. 2005;32:(3)332–353. doi:10.1525/ae.2005.32.3.332
6. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
7. Svenaeus F. Illness as unhomelike being-in-the-world: heidegger and the phenomenology of medicine. Med Health Care Philos. 2011;14(3):333–343. doi:10.1007/s11019-010-9301-0
8. Charon R. Narrative Medicine: Honoring the Stories of Illness. New York; Oxford: Oxford University Press; 2006.
9. Husserl E. The Crisis of European Sciences and Transcendental Phenomenology; an Introduction to Phenomenological Philosophy. Evanston, IL: Northwestern University Press; 1970.
10. Husserl E. Ideas pertaining to a pure phenomenology and to a phenomenological philosophy. Kluwer Boston. 1980.
11. Merleau-Ponty M. Phenomenology of Perception. Routledge; 2013.
12. Svenaeus F. The phenomenology of chronic pain: embodiment and alienation. Continent Philosophy Rev. 2015;48(2):107–122. doi:10.1007/s11007-015-9325-5
13. Carel H. Phenomenology of Illness. Oxford: Oxford University Press; 2016.
14. Kierkegaard S. The Sickness Unto Death: A New Translation. New York: Liveright Publishing Corporation; 2023.
15. Sartre J-P. Being and Nothingness. New York: Gramercy Books; 1994.
16. Camus A. The Myth of Sisyphus.
17. Wittgenstein L. Philosophical Investigations. Oxford: Basil Blackwell; 1953.
18. Foucault M. The Birth of the Clinic: An Archaeology of Medical Perception. New York: Vintage Books; 1994.
19. Suijker CA. Foucault and medicine: challenging normative claims. Med Health Care Philos. 2023;26(4):539–548. doi:10.1007/s11019-023-10170-y
20. Bourke J. The Story of Pain: From Prayer to Painkillers. New York: Oxford University Press; 2014.
21. Foucault M, Bertani M, Fontana A, eds. Society Must Be Defended: Lectures at the Collège de France, 1975–1976. New York: Picador; 2003.
22. Greenhaigh T, Hurwitz B. Why study narrative? West J Med. 1999;170(6):367–369.
23. Friston K. A theory of cortical responses. Philos Trans R Soc Lond B Biol Sci. 2005;360(1456):815–836. doi:10.1098/rstb.2005.1622
24. Clark A. Whatever next? Predictive brains, situated agents, and the future of cognitive science. Behav Brain Sci. 2013;36(3):181–204. doi:10.1017/S0140525X12000477
25. Friston K. The free-energy principle: a unified brain theory? Nat Rev Neurosci. 2010;11(2):127–138. doi:10.1038/nrn2787
26. Hohwy J. The Predictive Mind. Oxford: Oxford University Press; 2013.
27. Moseley GL, Vlaeyen JWS. Beyond nociception: the imprecision hypothesis of chronic pain. Pain. 2015;156(1):35–38. doi:10.1016/j.pain.0000000000000014
28. Stanciu D. Consciousness, 4E cognition and Aristotle: a few conceptual and historical aspects. Front Comput Neurosci. 2023;17:1204602. doi:10.3389/fncom.2023.1204602
29. Wear D, Zarconi J. Can compassion be taught? Let’s ask our students. J Gen Intern Med. 2008;23(7):948–953. doi:10.1007/s11606–007–0501–0
30. Denzin NK, Giardina MD, eds. Qualitative Inquiry Through a Critical Lens. Routledge; 2016.
31. Charon R, Montello MM, eds. Stories Matter: The Role of Narrative in Medical Ethics. Routledge; 2002.
32. Leder D. The Absent Body. Chicago: University of Chicago Press; 1990.
33. Cassell EJ. The Nature of Suffering and the Goals of Medicine.
34. Givler A, Bhatt H, Maani-Fogelman PA. The Importance of Cultural Competence in Pain and Palliative Care. Treasure Island (FL): StatPearls Publishing; 2023.
35. Boring BL, Ng BW, Nanavaty N, Mathur VA. Over-rating pain is overrated: a fundamental self-other bias in pain reporting behavior. J Pain. 2022;23(10):1779–1789. doi:10.1016/j.jpain.2022.06.002
36. Munday I, Newton-John T, Kneebone I. Clinician experience of metaphor in chronic pain communication. Scand J Pain. 2022;23(1):88–96. doi:10.1515/sjpain-2022-0043
37. Zhao J, Xiantao O, Li Q, et al. Role of narrative medicine-based education in cultivating empathy in residents. BMC Med Educ. 2023;23(1):124. doi:10.1186/s12909-023-04096-5
38. Kleinman A, Das V, Lock MM, eds. Social Suffering. Berkeley; Los Angeles; London: University of California Press; 1997.
39. Green CR, Anderson KO, Baker TA, et al. The unequal burden of pain: confronting racial and ethnic disparities in pain. Pain Med. 2003;4(3):277–294. doi:10.1046/j.1526-4637.2003.03034.x
40. Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci U S A. 2016;113(16):4296–4301. doi:10.1073/pnas.1516047113
41. Bourdieu P. Distinction: A Social Critique of the Judgement of Taste. Cambridge, MA: Harvard University Press; 1984.
42. Churchland PM. Neurophilosophy at Work. Cambridge: Cambridge University Press; 2007.
43. Clark A. Surfing Uncertainty: Prediction, Action, and the Embodied Mind. Oxford University Press; 2016.
44. Tabor A, Burr C. Bayesian learning models of pain: a call to action. Curr Opin Behav Sci. 2019;26:54–61. doi:10.1016/j.cobeha.2018.10.006
45. Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021;397(10289):2098–2110. doi:10.1016/S0140-6736(21)00392-5
46. Ramachandran VS, Altschuler EL. The use of visual feedback, in particular mirror visual feedback, in restoring brain function. Brain. 2009;132(Pt 7):1693–1710. doi:10.1093/brain/awp135
47. Ding ME, Traiba H, Perez HR. Virtual reality interventions and chronic pain: scoping review. J Med Internet Res. 2025;27(e59922). doi:10.2196/59922
48. Vlaeyen JWS, Linton SJ. Fear-avoidance model of chronic musculoskeletal pain: 12 years on. Pain. 2012;153(6):1144–1147. doi:10.1016/j.pain.2011.12.009
49. Gallagher S. Enactivist Interventions: Rethinking the Mind. Oxford University Press; 2017.
50. Newen A, De Bruin L, Gallagher S. The Oxford Handbook of 4E Cognition. Oxford University Press; 2018.
51. Aydede M, ed. Pain: New Essays on Its Nature and the Methodology of Its Study. MIT Press; 2005.
52. Varela FJ. Neurophenomenology: a methodological remedy for the hard problem. J Conscious Stud. 1996;3(4):330–349.
53. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
54. Stilwell P, Harman K. An enactive approach to pain: beyond the biopsychosocial model. Phenomenol Cogn Sci. 2019;18(4):637–665. doi:10.1007/s11097-019-09624-7
55. Wade DT, Halligan PW. The biopsychosocial model of illness: a model whose time has come. Clin Rehabil. 2017;31(8):995–1004. doi:10.1177/0269215517709890
56. Moseley GL, Butler DS. Fifteen years of explaining pain: the past, present, and future. J Pain. 2015;16(9):807–813. doi:10.1016/j.jpain.2015.05.005
57. Louw A, Riera-Gilley V. Pain neuroscience education: teaching people about pain. J Pain Palliat Care Pharmacother. 2024;38(3):292–301. doi:10.1080/15360288.2024.2424853
58. Gadamer H-G. The Enigma of Health: The Art of Healing in a Scientific Age. Stanford University Press; 1996.
59. Bleakley A. Medical Humanities and Medical Education: How the Medical Humanities Can Shape Better Doctors. Routledge; 2015.
60. Halpern J. From Detached Concern to Empathy: Humanizing Medical Practice. Oxford University Press; 2011.
61. Kohli RKS. The sound of silence: listening to what unaccompanied asylum-seeking children say and do not say. Br J Soc Work. 2006;36(5):707–721. doi:10.1093/bjsw/bch305
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.