Back to Journals » Infection and Drug Resistance » Volume 16
Pacemaker Associated Aspergillus fumigatus Endocarditis: A Case Report
Authors Chen W ![]() , Ji Y, Hong X, Zhu Y, Gou X, Chen M, Lv H, Ge Y
, Ji Y, Hong X, Zhu Y, Gou X, Chen M, Lv H, Ge Y
Received 22 October 2022
Accepted for publication 7 January 2023
Published 19 January 2023 Volume 2023:16 Pages 329—335
DOI https://doi.org/10.2147/IDR.S393917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wanyuan Chen,1,2 Youqi Ji,2 Xin Hong,2 Yongze Zhu,2 Xiaoyu Gou,2 Mengyuan Chen,2 Huoyang Lv,2 Yumei Ge1– 3
1Department of Pathology, Cancer Center, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, 310014, People’s Republic of China; 2Department of Clinical Laboratory, Laboratory Medicine Center, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, 310014, People’s Republic of China; 3Key Laboratory of Biomarkers and in vitro Diagnosis Translation of Zhejiang Province, Hangzhou, 310063, People’s Republic of China
Correspondence: Yumei Ge, Department of Clinical Laboratory, Laboratory Medicine Center, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, No. 158, Shang-Tang Road, Gong-Shu District, Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel +86-0571-85893264, Email [email protected]
Abstract: Aspergillus endocarditis (AE) is a highly fatal infection that can occur in heart valve replacement, pacemaker implantation and other heart surgeries, and early recognition and sufficient diagnosis are challenging. Here, we report the case of a 68-year-old male with a history of dilated cardiomyopathy and pacemaker implantation who had a repeated fever with failed antibacterial treatment and sterile blood culture. He developed endocarditis, and the culture and biopsy of vegetation tissue showed the abundant presence of septate hyphae, which was subsequently identified as Aspergillus fumigatus by internal transcribed spacer (ITS) sequencing. Although the patient had serious side effects from voriconazole, he had a good prognosis following surgery and prolonged caspofungin antifungal therapy of 42 consecutive days. We discuss the diagnosis and treatment strategy of AE, and recommend galactomannan assays and next-generation sequencing for a timely diagnosis. Early surgical intervention combined with prompt antifungal therapy appears significant for survival.
Keywords: Aspergillus endocarditis, AE, Aspergillus fumigatus, vegetation, culture, fever
Background
Invasive aspergillosis is a prevailing superinfection as the global medical community confronts population aging and the ongoing COVID-19 pandemic with increasing invasive surgeries and secondary infection after lung injury.1 Invasive pulmonary aspergillosis mainly caused by Aspergillus fumigatus is the most typical clinical phenotype.2 However, emerging extrapulmonary infections with unusual manifestations of invasive aspergillosis have increased significantly in recent years, such as Aspergillus endocarditis (AE).3 AE is an extremely rare and devastating disease associated with poor prognosis and mortality greater than 50%, and it is most prevalent in immunocompromised patients, intravenous drug abusers, patients with artificial heart valves or those undergoing cardiac reconstruction and recipients of prolonged antibiotics.4–6 Aspergillus is the second most common factor causing fungal endocarditis (FE) after Candida, accounting for 20–25% of FE and 0.2–2.5% of all infective endocarditis (IE) and occurring mostly in prosthetic heart valves.7 Most AE cases present with constitutional symptoms, including fever, hemoptysis, chest pain, dyspnea, murmur, emboli, sepsis and cardiac failure, which are indistinguishable from bacterial or viral endocarditis.8 However, the antibiotic and treatment strategies used to treat these three types of infective endocarditis are quite different. Positive blood culture is the most important indicator of IE However, unlike bacterial or Candida endocarditis, the negative rate of blood culture in AE exceeds 96%.9 The diagnosis and treatment of AE remains a great challenge in the clinic; less than half of AE cases are diagnosed preoperatively, and approximately one-third of AE cases are diagnosed postmortem.9 Here, we present the case of an elderly patient with fever and chills of unknown cause, continuous increases in the white blood cell (WBC) count and C-reactive protein (CRP) level, ineffectiveness of antibacterial treatment, and sterile blood culture who was finally diagnosed with AE by culture and biopsy of vegetation tissue.
Case
A 68-year-old male with a history of dilated cardiomyopathy and pacemaker implantation 2 years prior was hospitalized with repeated chills, fever and weakness for 20 days. After examination in the local hospital, the WBC count (10.38×109/L) and CRP level (75 mg/L) were both increased. Moxifloxacin, meropenem and vancomycin were used for anti-infection treatment, but they were ineffective. The patient was transferred to the provincial hospital, indicating that the WBC count (11.5×109/L) and CRP level (173 mg/L) were further increased, but procalcitonin did not increase (0.08 ng/mL). To identify the pathogens causing infection, the patient came to our hospital for treatment. However, the patient’s condition further deteriorated, and the inflammatory markers continued to rise (18.26×109/L WBCs and 15.95×109/L neutrophils), with negative results for hepatitis B virus, hepatitis C virus, human immunodeficiency virus, and Treponema pallidum as well as culture of blood, sputum and urine. Acid-fast staining of sputum was also negative, indicating that pulmonary tuberculosis was preliminarily excluded. The erythrocyte sedimentation rate (32 mm/h) and procalcitonin (0.08 ng/mL) of the patient were negative. Serum 1,3-β-D-glucan (G) assay, galactomannan antigen (GM) assay and filamentous fungus examination of bronchoalveolar lavage fluid (BALF) were performed. The G assay showed that serum 1,3-β-D-glucan was 243.63 pg/mL (normal reference interval was 0–60 pg/mL), and the GM assay showed that galactomannan was 1.13 μg/L (normal reference interval was 0–0.5 μg/L), while BALF culture was negative. Echocardiography showed a 38.6×26.2×30.0 mm vegetation (white arrow) adhered to the right cardiac pacemaker and tiny mitral subvalvular vegetations, which aroused our concern (Figure 1). CT angiography showed pulmonary embolism, and laboratory examination showed coagulation dysfunction with abnormal elevation of prothrombin time (30.8 s), fibrinogen (4.33 g/L), D-dimer (3860 μg/L), and fibrin degradation product (13,000 μg/L). Doctors considered that pulmonary embolism was probably caused by the shedding of vegetation, so they performed pulmonary artery thrombectomy, removal of the cardiac pacemaker and implantation of a temporary pacemaker. Then, pathological examination and pathogenic examination of the cardiac tissues, cardiac pacemaker and vegetation were performed. According to the ultrasonic morphological characteristics of this vegetation accompanied by some tiny flocculent floaters and positive serological results, we suspected that it might be caused by filamentous fungal infection. Therefore, a resident physician used caspofungin as an empirical antifungal treatment, administering 70 mg on the first day and 50 mg once a day thereafter. Histopathological digital slices of the vegetations demonstrated multiple fibrinoid and hemorrhagic necrosis with extensive inflammatory infiltration, accompanied by hyaline sporophores and filamentous hyphae, 2–7 μm in diameter, dark in HE staining (Figure 2). Antler-like filamentous hyphae were stained by Gram staining of the vegetations (Figure 3A). Septate hyphae with branches at acute angles were shown in bright blue by fluorescence staining (Figure 3B). The colony cultured from vegetations was grayish-green and velutinous (Figure 3C). Lactophenol cotton blue staining showed that the top of the smooth conidia stalk expanded to form an inverted flask-shaped top cyst with a single-layer sterigma, and unstained conidia were spherical, forming a blue chrysanthemum (Figure 3D). A phylogram was constructed utilizing the ITS sequence of the isolated strain Aspergillus fumigatus ZJPPH1 along with 18 available sequences with the highest homology retrieved from GenBank by MEGA11 (Figure 3E). After confirming that the infection factor was Aspergillus fumigatus, we changed caspofungin to 0.2 g of voriconazole every 12 hours for anti-Aspergillus fumigatus infection treatment. However, on the second day, the patient had severe liver and kidney dysfunction with abnormal decreases in serum albumin (55.2 g/L), albumin (32.4 g/L), and cholinesterase (3824 U/L) and abnormal increases in glutamic pyruvic transaminase (3214 U/L), glutamic oxaloacetic transaminase (2199 U/L), glutamyl transpeptidase (214 U/L), lactate dehydrogenase (1259 U/L), total bilirubin (83.7 μmol/L), direct bilirubin (42.2 μmol/L), total bilirubin (41.5 μmol/L), creatinine (185.2 μmol/L) and urea (17.21 mmol/L). The liver and kidney function indices of the patient were normal and stable during treatment with caspofungin, so we reused caspofungin as the antifungal drug at 50 mg once a day and continued to use caspofungin for 42 consecutive days of continuous antifungal treatment. We performed a series of surgical interventions on the patient (we described the operation process in detail in the Supplementary Materials). G and GM assays were performed again, and the results showed that serum 1.3-β-D-glucan (14.87 pg/mL) and galactomannan (0.79 μg/L) decreased significantly compared with the previous levels, which suggested that the anti-Aspergillus treatment was effective. The patient improved; his inflammatory markers, including WBCs (7.54×109 /L) and CRP (9.3 mg/L), returned to normal, and he was discharged. One year later, the patient had recovered well, with normal routine blood and inflammatory indicators. He underwent permanent pacemaker implantation and was discharged from the hospital. According to our latest follow-up, he had recovered well.
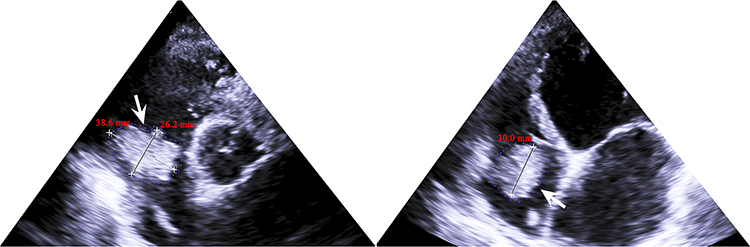 |
Figure 1 Echocardiography of the patient. White arrow represents a 38.6×26.2×30.0 mm vegetation adhered to right cardiac pacemaker. |
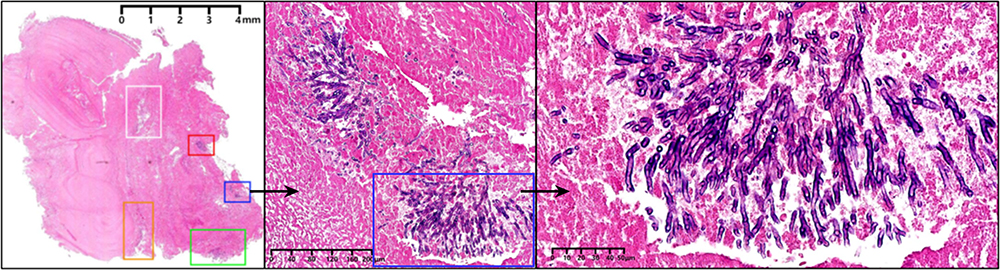 |
Figure 2 Histopathological examination of the vegetation by HE staining. The boxes with different colors represent the presence of Aspergillus lesions, and the black arrow is used to point to the enlarged image of Aspergillus lesion in the blue box. |
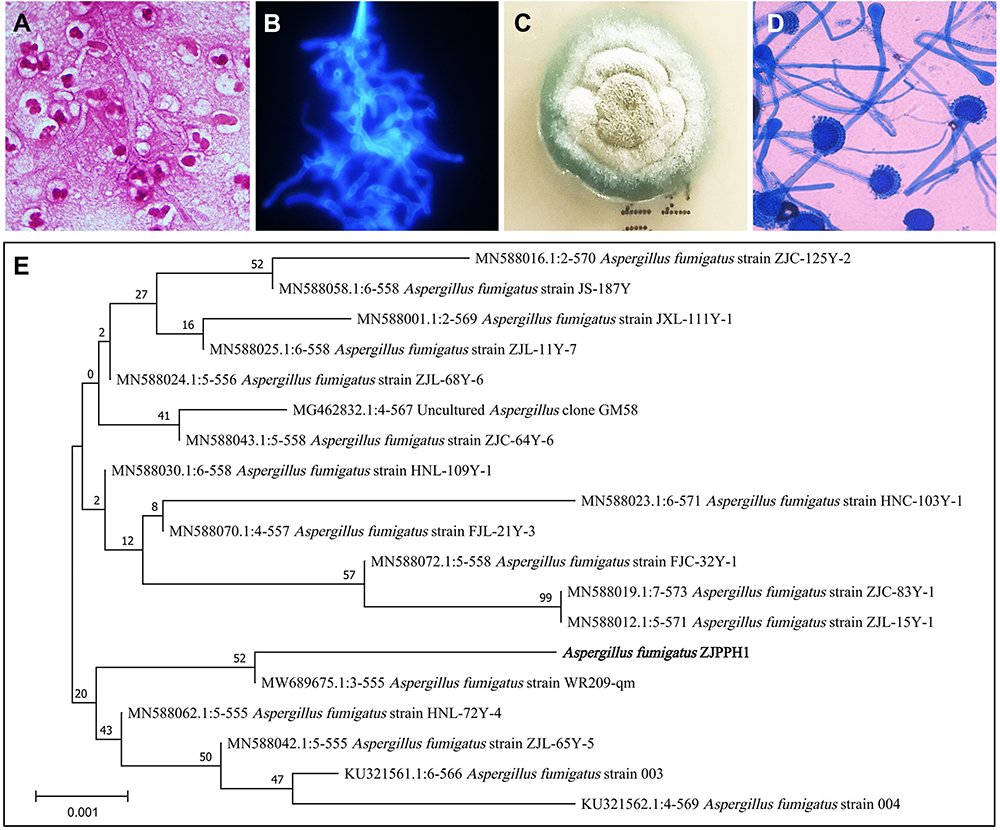 |
Figure 3 Pathogenic identification. (A) Antler-like filamentous hyphae in a background of several inflammatory cells by Gram staining of the vegetation. (B) Blue septate hyphae with branches at acute angles by fluorescence staining of the vegetation. (C) A greyish-green and velutinous colony after culture on fungal medium. (D) Lactophenol cotton blue staining of the colony. (E) Phylogram of the ITS sequence of isolating strain Aspergillus fumigatus ZJPPH1 along with 18 available sequences with the highest homology retrieved from GenBank by MEGA11. |
Discussion
Aspergillus endocarditis caused by hyphae invading pulmonary arterioles and blood dissemination is becoming an emerging life-threatening infection due to population aging and the increase in patients with transplantation, invasive surgery, immunodeficiency and metabolic dysfunction as well as the extensive application of chemotherapeutics, immunosuppressants, and broad-spectrum antibiotics worldwide. AE is a relatively rare disease, accounting for 0.2% of all cases of IE, and has rarely been recognized by doctors in the past.10 AE accounted for 0.2% of 4528 patients with IE in a national multicenter cohort (2008–2018) and mainly affected previous valvular surgery or solid organ transplant recipients. Furthermore, embolisms occurred in 54%, and the main isolated species were Aspergillus fumigatus (47.5%) and Aspergillus flavus (24.6%).10 AE accounted for 31 of 374 patients with IE enrolled from 2005–2016 in a tertiary referral university hospital, and fever was present in 67.7% of the AE patients. Aspergillus was the most common fungus in FE (31/43; 72.1%), and the authors suggested that the absence of fever, health care-associated endocarditis, prosthetic valve endocarditis, and aortic abscess/pseudoaneurysm were strong predictors of AE.11 The diagnosis of bacterial endocarditis and the treatment of multidrug resistant bacteria have been well described;12 however, it is mainly problematic and lacks diagnostic criteria, treatment guidelines and data for cases of filamentous fungal endocarditis, including AE. Although the diagnostic criteria of EORTC/MSGERC 2020 have defined possible, probable and proven invasive aspergillosis, the diagnostic criteria are mainly for pulmonary aspergillosis, as most invasive aspergillosis is mainly involved in the lungs.13 However, AE is a special and serious type of invasive aspergillosis. In fact, the diagnostic guidelines for AE remain unclear. In addition, AE often does not conform to the conventional clinical standard of IE; most patients have negative blood culture and do not have fever, and even CRP only slightly increases.11 In this case, the patient had fever, increased infection indices, pulmonary embolism and abnormal coagulation function, but the blood culture was negative. According to our clinical experience, valvular vegetation, aortic abscess or pseudoaneurysm accompanied by fever of unknown origin and sterile blood culture are important clinical features of AE. The attributable mortality rate of AE is approximately 90%, and the clinical diagnosis and treatment of AE are complicated with challenges.8 We hope that clinicians and researchers can obtain valuable information from our case to address cases of AE in the future. The positive results of serum galactomannan (1.13 μg/L) and 1,3-β-D-glucan (243.63 pg/mL) assisted the diagnosis to a certain extent in this patient, and both levels significantly decreased after 42 consecutive days of treatment with caspofungin (serum galactomannan was 0.79 μg/L and 1,3-β-D-glucan was 14.87 pg/mL). Detection of serum galactomannan and 1,3-β-D-glucan was of positive diagnostic and follow-up value in this patient. Galactomannan is a cell wall component released by Aspergillus in the process of proliferation in hosts.14 False negative results may occur in patients with nonneutropenia, as galactomannan can be cleared by neutrophils.15 Although this patient had nonneutropenia, serum galactomannan was positive, and it is recommended to apply serum galactomannan in the auxiliary diagnosis of AE. EORTC/MSGERC 2020 suggested that galactomannan should not be recommended as the diagnostic basis for proven invasive aspergillosis, but a threshold value was given for the diagnosis of probable cases, and this value was consistent among children and adults meeting any one of the following criteria: single plasma or serum ≥ 1.0, bronchoalveolar lavage fluid ≥ 1.0, single serum or plasma ≥ 0.7, bronchoalveolar lavage fluid ≥ 0.8, and cerebrospinal fluid ≥ 1.0.16–19 It has generally been reported that 1,3-β-D-glucan has low specificity, but serum 1,3- β-D-glucan has not been included in clinical trials with patients to diagnose invasive aspergillosis, nor has it been used as mycological evidence to diagnose invasive mycosis.13 Serum samples should be taken at least twice consecutively, and 1,3-β-D-glucan ≥ 80 ng/L after excluding other causes can be used as a diagnostic basis for possible cases.13 However, it was found that serum 1,3-β-D-glucan decreased significantly after antifungal treatment in our case, suggesting that 1,3-β-D-glucan is valuable for the follow-up of the antifungal efficacy of AE. It is usually traumatic and difficult to obtain heart tissue for pathogenic examination, and it takes a long time to identify positive results of Aspergillus by culture (typical colonies need 3 days or longer to grow). Delayed or mistaken diagnosis of AE is extremely common, and many diagnoses are made postmortem. In fact, in 2016, the Infectious Disease Society of America (IDSA) recommended the GM assay as a useful adjunctive diagnostic method for patients with invasive aspergillosis who did not receive antifungal treatment, but this has not been studied in the setting of endocarditis.19 Therefore, we suggest that serum G and GM assays should be used as the primary screening methods for suspected AE in clinical practice. In this case, histopathology clearly indicated the basis of filamentous fungal infection, and we finally identified the exact strain as Aspergillus fumigatus through culture and ITS sequencing. Next-generation sequencing (NGS) is widely used by clinical laboratories because of its advantages of being able to quickly detect a variety of pathogenic microorganisms and its applicability to the detection of tissues, blood samples, body fluids and other types of clinical specimens.20 NGS should be considered for patients with critical illness when specific pathogens cannot be identified, although it has some limitations, including identifying and distinguishing true pathogens from environmental contaminants.21 However, because NGS is not presently included in the medical insurance in our region, the family member of this patient declined the use of NGS in consideration of the cost. We finally obtained the results by ITS sequencing of the colony after 2 days of culture.
The current IDSA guidelines recommend voriconazole and amphotericin B as the initial treatment for AE and consider lifelong antifungal therapy after surgical debridement.19,22 Previous studies have shown that voriconazole is associated with improved survival and less nephrotoxicity, electrolyte abnormalities, and infusion-related events than amphotericin B.9 In this patient, serious side effects of hepatorenal toxicity occurred after the use of voriconazole; however, the patient was tolerant to caspofungin. In fact, in the clinical practice of invasive mycosis, many specifications remain to be standardized. In previous reports, all patients without recurrence received antifungal treatment with voriconazole or isavuconazole for more than 6 months, but there are no statistics on echinocandins due to a lack of data.4 In this case, the classic first choice of antifungal drugs, voriconazole, was not used for antifungal treatment. This article provides a case of caspofungin antifungal treatment for patients who have a strong reaction to voriconazole. Surgical debridement is mandatory for all patients, and secondary embolism is the most frequent complication and major cause of death from AE.23 Our patient also suffered from embolism and underwent surgery.
Limitations
Presently, the detection of in vitro drug susceptibility of fungi is limited to yeast, including Candida and Cryptococcus, and the drug susceptibility of filamentous fungi, including Aspergillus, has not been routinely carried out in clinical practice, as it usually requires the inspector to purchase corresponding drug sensitivity reagents at his own expense. Although we isolated an Aspergillus fumigatus strain from the patient, an in vitro fungal susceptibility test was not performed, and we do not know the specific antifungal drug phenotype of this strain. With the increase in the incidence rate of mycosis, we suggest that the drug sensitivity test of filamentous fungi in vitro should be routinely performed in clinical practice to standardize and accurately guide clinical medication administration. There is no standard for the appropriate duration of antifungal therapy. Currently, the duration of medication and whether life-long suppressive treatment is needed largely depends on the experience of the doctor. Patients with bloodstream infections of pathogens such as Bartonella and Coxiella that do not grow in routine culture also appear to have apparent negative blood culture results. Therefore, these pathogens were not excluded in the diagnosis and treatment of this patient.
Conclusion
Early diagnosis of emerging life-threatening infections caused by AE remains a daunting challenge. Here, we report a case of a 68-year-old male with a history of dilated cardiomyopathy and pacemaker implantation who had a repeated fever with failed antibacterial treatment and sterile blood culture. He developed endocarditis, and the culture and biopsy of vegetation tissue showed the abundant presence of septate hyphae, which was subsequently identified as Aspergillus fumigatus by ITS sequencing. Although the patient had serious side effects from voriconazole, he had a good prognosis following surgery and prolonged caspofungin antifungal therapy of 42 consecutive days. GM assay and NGS are recommended for the timely establishment of the diagnosis. Early surgical intervention combined with prompt antifungal therapy appears significant for survival. Additional clinical cases and studies of AE with unusual clinical features of invasive pulmonary aspergillosis are needed to improve the efficiency of antifungal treatment and management.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author Yumei Ge on reasonable request.
Ethics Approval and Consent to Participate
This study was supported by the Ethics Committee of Zhejiang People’s Hospital (Ethics Committee Approval of Biomedical Research Involving Humans, Approval No.:2022JS008) and was carried out in accordance with the ethical standards of the Declaration of Helsinki.
Consent for Publication
Written and informed consent was obtained from the patient for publication of this Case Report and any accompanying images.
Acknowledgments
We thank all members of the microbiology laboratory of Zhejiang Provincial People’s Hospital for their help in the collection of clinical data.
Funding
This study was supported by the New Project of Zhejiang Provincial People’s Hospital entitled “Construction of Rapid Nucleic Acid Detection Platform for Invasive Fungi” (20211214).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Prattes J, Koehler P, Hoenigl M; ECMM-CAPA Study Group. COVID-19 associated pulmonary aspergillosis: regional variation in incidence and diagnostic challenges. Intensive Care Med. 2021;47(11):1339–1340. doi:10.1007/s00134-021-06510-2
2. Dagenais TR, Keller NP. Pathogenesis of Aspergillus fumigatus in invasive aspergillosis. Clin Microbiol Rev. 2009;22(3):447–465. doi:10.1128/CMR.00055-08
3. Glampedakis E, Cassaing S, Fekkar A, et al. Invasive aspergillosis due to Aspergillus section usti: a multicenter retrospective study. Clin Infect Dis. 2021;72(8):1379–1385. doi:10.1093/cid/ciaa230
4. Born T, Aruanno M, Kampouri E, et al. Aspergillus tubingensis endocarditis: a case report and review of the literature. Mycopathologia. 2022;187(2–3):249–258. doi:10.1007/s11046-022-00621-0
5. El-Hamamsy I, Durrleman N, Stevens LM, et al. Aspergillus endocarditis after cardiac surgery. Ann Thorac Surg. 2005;80(1):359–364. doi:10.1016/j.athoracsur.2004.08.070
6. Tattevin P, Revest M, Lefort A, et al. Fungal endocarditis: current challenges. Int J Antimicrob Agents. 2014;44(4):290–294. doi:10.1016/j.ijantimicag.2014.07.003
7. Pasha AK, Lee JZ, Low SW, et al. Fungal endocarditis: update on diagnosis and management. Am J Med. 2016;129(10):1037–1043. doi:10.1016/j.amjmed.2016.05.012
8. McCormack J, Pollard J. Aspergillus endocarditis 2003–2009. Med Mycol. 2011;49(Suppl 1):S30–S34. doi:10.3109/13693786.2010.498449
9. Kalokhe AS, Rouphael N, El Chami MF, et al. Aspergillus endocarditis: a review of the literature. Int J Infect Dis. 2010;14(12):e1040–e1047. doi:10.1016/j.ijid.2010.08.005
10. Valerio M, Camici M, Machado M, et al. Aspergillus endocarditis in the recent years, report of cases of a multicentric national cohort and literature review. Mycoses. 2022;65(3):362–373. doi:10.1111/myc.13415
11. Meshaal MS, Labib D, Said K, et al. Aspergillus endocarditis: diagnostic criteria and predictors of outcome, A retrospective cohort study. PLoS One. 2018;13(8):e0201459. doi:10.1371/journal.pone.0201459
12. Singh V, Chibale K. Strategies to combat multi-drug resistance in tuberculosis. Acc Chem Res. 2021;54(10):2361–2376. doi:10.1021/acs.accounts.0c00878
13. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European organization for research and treatment of cancer and the Mycoses Study Group Education and research consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
14. Ghazaei C. Molecular insights into pathogenesis and infection with Aspergillus fumigatus. Malays J Med Sci. 2017;24(1):10–20. doi:10.21315/mjms2017.24.1.2
15. He H, Ding L, Chang S, et al. Value of consecutive galactomannan determinations for the diagnosis and prognosis of invasive pulmonary aspergillosis in critically ill chronic obstructive pulmonary disease. Med Mycol. 2011;49(4):345–351. doi:10.3109/13693786.2010.521523
16. D’Haese J, Theunissen K, Vermeulen E, et al. Detection of galactomannan in bronchoalveolar lavage fluid samples of patients at risk for invasive pulmonary aspergillosis: analytical and clinical validity. J Clin Microbiol. 2012;50(4):1258–1263. doi:10.1128/JCM.06423-11
17. Leeflang MM, Debets-Ossenkopp YJ, Wang J, et al. Galactomannan detection for invasive aspergillosis in immunocompromised patients. Cochrane Database Syst Rev. 2015;2015(12):CD007394. doi:10.1002/14651858.CD007394.pub2
18. Mennink-Kersten MA, Donnelly JP, Verweij PE. Detection of circulating galactomannan for the diagnosis and management of invasive aspergillosis. Lancet Infect Dis. 2004;4(6):349–357. doi:10.1016/S1473-3099(04)01045-X
19. Patterson TF, Thompson GR, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases Society of America. Clin Infect Dis. 2016;63(4):e1–e60. doi:10.1093/cid/ciw326
20. Peng Y, Dong X, Zhu Y, et al. A rare case of pulmonary nocardiosis comorbid with Sjogren’s syndrome. J Clin Lab Anal. 2021;35(9):e23902. doi:10.1002/jcla.23902
21. Dai T, Hu Q, Xie Z, et al. Case report: infective endocarditis caused by Aspergillus flavus in a hemodialysis patient. Front Med. 2021;8:655640. doi:10.3389/fmed.2021.655640
22. Walsh TJ, Anaissie EJ, Denning DW, et al. Treatment of aspergillosis: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2008;46(3):327–360. doi:10.1086/525258
23. Meena DS, Kumar D, Agarwal M, et al. Clinical features, diagnosis and treatment outcome of fungal endocarditis: a systematic review of reported cases. Mycoses. 2022;65(3):294–302. doi:10.1111/myc.13398
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.