Back to Journals » International Journal of General Medicine » Volume 17
Oxidative Products of Catecholamines During Heightened Sympathetic Activity Due to Congestive Heart Failure: Possible Role of Antioxidants
Authors Ganguly P ![]()
Received 24 November 2023
Accepted for publication 14 February 2024
Published 11 March 2024 Volume 2024:17 Pages 919—923
DOI https://doi.org/10.2147/IJGM.S449688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Paul Ganguly
College of Medicine, Alfaisal University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Paul Ganguly, College of Medicine, Alfaisal University, Riyadh, Kingdom of Saudi Arabia, Tel +966503092964, Email [email protected]
Abstract: The past several decades have shown the functional status of sympathetic activity in congestive heart failure. The results, particularly through clinical and basic studies in heart failure, indicate an increased sympathetic neural activity. The definitive and compelling evidence of the involvement of catecholamines is the demonstration that many drugs that are therapeutically useful in the treatment of heart failure also affect the sympathetic nervous system at various sites, including its synthesis, release and uptake of catecholamines and a decreased plasma norepinephrine level. Although it is not surprising that the sympathetic system is altered as cardiac function is compromised in heart failure, it now appears that this system may overreact in chronic situations. The detrimental cardiovascular problems result in the production of aminochrome and free radicals. Antioxidant therapy to target the production of aminochrome from autooxidation of catecholamines should provide an insight into the future therapeutic goal in situations like congestive heart failure.
Keywords: aminochrome, congestive heart failure, antioxidants, cardiac dysfunction, intracellular mechanisms
Introduction
Heart failure can be defined as a condition of decreased cardiac function to maintain systemic circulation appropriate to the body’s need under physiological conditions or during increased demand, and is often associated with irregular heart rate, enlarged heart, ischemia, and cell death. Despite advances in understanding of the pathophysiology and treatment, heart failure continues to be a challenge in the scientific community as it is a major cause of morbidity and mortality worldwide. Proven through a variety of molecular approaches for studying human sympathetic neural function, many studies have now shown that the activation of the sympathetic nervous system is a hallmark of congestive heart failure.1,2 Heart failure is associated with an initial decrease in pumping capacity of the heart. During this time, a variety of compensatory mechanisms are activated, including the adrenergic nervous system, the renin-angiotensin system, and the cytokine system. In the short term these systems allow the restoration of cardiovascular function to a normal homeostatic range, with the result that the patient may remain free from major symptoms. However, over time the chronic activation of these systems can lead to secondary end-organ damage within the ventricle and subsequent cardiac dysfunction with decreased cardiac contractility. As a result of the worsening of cardiac decompensation, patients go from asymptomatic to symptomatic heart failure. In particular, the adrenergic overdrive in heart failure is associated with effector organs, such as the downregulation of beta-receptors at the cardiac level which exerts negatively on the cardiovascular system.1,2 Defective sodium-calcium exchange can also contribute to the contractility of the heart. Given the fact that heart failure and sympathetic activation are closely related, the adrenergic overdrive has become a target of therapeutic interventions.3 The purpose of this article is to summarise the fact that; a) sympathetic activity is increased in congestive heart failure, b) oxidant and free radical species have been involved and c) newer antioxidants specially targeting molecules such as aminochrome derived from heightened sympathetic activity are the future therapeutic goal in this disease.
Heightened Sympathetic Activity
There are many published reports4,5 indicating the heightened sympathetic tone in patients with congestive heart failure and provided evidence that there is a direct correlation between plasma norepinephrine and prognosis of the disease. Heightened sympathetic activity has been proposed to play a major role in the progression of the disease and outcome through its effect on myocardial cells, arrhythmia, and possible excitation-contraction coupling.1,2 Most patients with heart failure show increased sympathetic activity as evidenced from increased plasma norepinephrine levels either in rest or during exercise. However, in spite of higher plasma norepinephrine levels, the heart rate of these patients was not increased, and signs of vasoconstriction werre not evident. Such observations clearly indicate that some adaptation to prolonged sympathetic activity occurs. In fact, the response of failing hearts to both exogenous and endogenous catecholamines become markedly attenuated. It has been suggested that the down regulation of beta-adrenergic receptors is primarily responsible for such an effect.1,2 Other studies have shown that the catecholamine resistance is due to a defect in the guanylate nucleotide complex that is tied up with the beta receptor to adenylate cyclase.4,5
Aminochrome/Adrenochrome Hypothesis
Generally, catecholamines are metabolized by two pathways using two different enzymes, catechol-O-methyl transferase (COMT) and monoamine oxidase (MAO). However, it has been suggested6 that under chronic stressful conditions when these systems are overburdened by increased levels of circulating catecholamine, they bypass enzyme-induced metabolic pathways and ultimately auto-oxidize. In fact, the oxidation of catecholamines has been demonstrated to result in the formation of aminochrome/adrenochrome and adrenolutin. Out of all metabolites that form through autooxidation of catecholamines, aminochrome is the most unstable substance and known to be highly reactive as a toxic metabolite. This aminochrome is converted by further oxidation to a stable and inactive metabolite, aminolutin. Thus, aminochrome can be measured in plasma in the form of proportional increase of aminolutin. We have shown earlier that the concentration of plasma aminochrome, measured as adrenolutin, was found to increase several folds by injecting epinephrine. Studies have suggested that the oxidation of catecholamines results in the production of oxygen free radicals. The importance of oxyradical generation and the development of oxidative stress in cardiovascular diseases warrant further investigation.
Is increased plasma norepinephrine concentration injurious to myocardium? Is heightened sympathetic activity an obvious etiology or an effect? Does a common mechanism explain the cardiac dysfunction in heart failure? Although many more studies are needed for these answers, it is now generally accepted that chronic stressful conditions are associated with increased levels of circulating catecholamines and possibly heart disease. Although numerous investigators7,8 have contributed substantially to our understanding of the biochemical basis for the cardiotoxic action of catecholamines, such as defective Ca2+ transport mechanisms and Ca2+ overload, the present hypothesis is intriguing.9 The mechanism of catecholamine-induced myocardial injury mediated via aminochrome, one of the oxidation products of catecholamines and free radicals, is regarded as a possible cardiotoxic factor during the presence of excess levels of catecholamines in the circulation. The accumulation of oxidation products of catecholamines in the myocardium through various molecular mechanisms damages myocardial cells. In fact, earlier studies have shown that aminochrome impaired the contractile function of the heart. These studies confirm that excess aminochrome produces arterial spasm, irregularities of the heart, structural damage, and decreased ventricular function. The toxic influence of adrenochrome on the myocardium and its modification by various agents support the participation of this oxidation product in the pathogenesis of catecholamine-induced cardiotoxicity.10
Aminochrome disappears in circulation,11 an observation that indicates that blood cells may be involved in the oxidation of aminochrome to other metabolites such as aminolutin. By using high-performance liquid chromatography, an adrenolutin assay technique was developed.11 We showed earlier that the formation of adrenolutin from epinephrine was dose-dependent. It is thus, possible that the level of adrenolutin in plasma may reflect the extent of oxidation of circulating catecholamines. High levels of plasma adrenolutin in various species may suggest the presence of an efficient mechanism for the oxidation of catecholamines. Because the turnover of dopamine is associated with cellular oxidant, increased neuronal activity could also be triggered by oxidative stress. Thus, one may reasonably hypothesize the participation of the oxidative products of catecholamines, such as aminochrome, in the pathophysiologic process in congestive heart failure.9 It is logical to believe that a persistent oxidative stress resulting from heightened sympathetic activity, coupled with other etiologic factors, may produce significant abnormalities in the failing heart.
Other Sources of Oxidant Stress
Thomson et al 12 reported that a heightened renin-angiotensin-aldosterone system is one of the main biological pathways involved in oxidant stress in heart failure. In fact, nitric oxide generates reactive oxygen species and promotes heart failure through multiple mechanisms such as stimulation of xanthine oxidase, uncoupling of nitric oxide synthase and mitochondrial leakage. The authors conclude that a certain antioxidant monotherapy is necessary to challenge specific heart failure aetiology and progression. Although these observations are interesting, it may be pointed out that, as discussed above, the heightened sympathetic activity remains the hallmark in heart failure and thus many drugs are targeted to reduce the activity by decreasing the production of catecholamines or by acting on catecholamine receptors. This is complicated by the fact that, till today, we have failed to understand the entire oxidant burden, neither knowing the source of these oxidants or the free radical species.
Antioxidants as Treatment in Heart Failure
It is generally accepted that under normal physiological conditions, reactive oxygen species levels are regulated by antioxidant enzymes, such as superoxide dismutase, catalase, and glutathione peroxidase, and the oxidative stress is followed by a transient or a persistent increase of reactive oxygen radicals. The low concentrations of these enzymes, as found in heart failure, trigger a chain-reaction that destroys the myocardial homeostatic and defensive mechanisms. Such pathological stimulus also leads to altered signaling pathways and modifies cellular constituents. These results are interpreted to mean that reactive oxygen species are the key pathophysiological player in cardiac hypertrophy, remodeling, and the development of heart failure.9 Although a therapeutic trial of antioxidants to slow the progression of cardiac abnormalities may be considered in the future, the question remains whether we have; a) newer antioxidants, b) agents that have nutritional value similar to Vitamin E and, finally, c) agents that can effectively target aminochrome-induced free radicals originating from the oxidation products of catecholamines. Figure 1 demonstrates the possible mechanism related to the role of antioxidants in congestive heart failure.
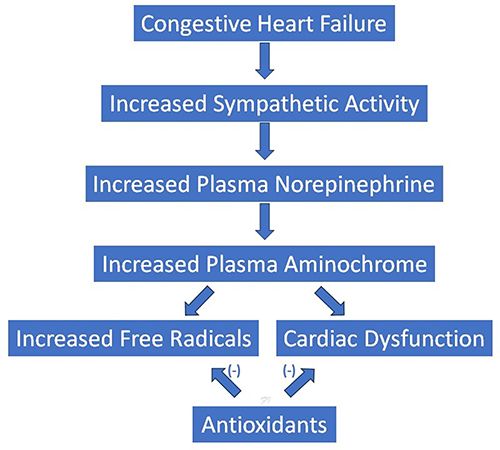 |
Figure 1 The diagrammatic representation of the role of antioxidants in congestive heart failure. It is proposed that the newer antioxidants can combat the ill effect of aminochrome and free radicals originated from heightened sympathetic activity and increased plasma catecholamines. |
The use of antioxidants or anti-inflammatory agents in the treatment of heart failure yielded different kinds of results. A possible explanation is that unselective inflammatory suppression may be harmful in heart failure because it also damages many of the essential cellular protective mechanisms, such as cellular signalling pathways, immune defence, and mitochondrial energy production.12 Thus, it is possible to conclude that not all antioxidants or anti-inflammatory reagents can be useful in heart failure. These results justify that interventions directed to the more specific and balanced inhibition of oxidative/inflammatory mechanisms in heart failure may be more beneficial and warrants further investigation. Milinkovic et al,12 in recent trials showed additional selective agents which produced promising results. Further research along the same line is needed. In addition, strategies aimed at preventing the renin-angiotensin system, cytokines or stimulating endogenous antioxidant systems should also prove beneficial. It is felt that further investigation on this line may pave the pathway to suggest that “the best is yet to come with further research”. Those agents will selectively work on potential anti-inflammatory or antioxidant interventions and pinpoint the aetiology and pathophysiology of heart failure relevant to complex intracellular compartments.13
As indicated above, multiple antioxidative stress therapies have been tested through; a) inhibition of oxidative stress producers, b) improvement of endogenous antioxidant concentration, and c) improvement of antioxidants by adding exogenous antioxidants. However, the results from these studies suggest that although targeting oxidative stress is theoretically logical, most of the current strategies fail to improve clinical outcomes. The results obtained using drugs with anti-inflammatory, antioxidative stress and antidiabetic properties appear to be very promising. In this regard, sodium-glucose cotransporter two inhibitors, a novel class of antidiabetic drugs, appear to be promising in reducing reactive oxygen species in experimental animals.14 The question therefore arises as to why antioxidant therapy has failed to cause significant benefit in the treatment of heart failure? Till we have the pharmacokinetic results of all newer agents, it is difficult to answer such a question. This is complicated by the fact that no single antioxidant agent has yet proved to be beneficial in combating the entire pathophysiology of heart failure and the ill effects of oxidative stress and inflammation, activation of the sympathetic nervous system activity and renin–angiotensin–aldosterone system, and defective sodium-calcium exchange.
Conclusions
The above hypothesis, if correct, may have a significant role in many pathophysiological situations where plasma catecholamines are expected to be significantly increased, such as in pheochromocytoma.8 Nevertheless, it is tempting to strengthen the view that newer antioxidants targeted by oxidative products of catecholamines may be beneficial, particularly in heart failure where the activity is increased several fold. Future studies on this issue are warranted to strengthen the present hypothesis.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Zhang DY, Anderson AS. The sympathetic nervous system and heart failure. Cardiol Clin. 2014;32(1):33–45. doi:10.1016/j.ccl.2013.09.010
2. Ganguly PK, Shao Q, Dhalla KS, Dhalla NS, Dhalla NS. Differential changes in sympathetic activity in left and right ventricles in congestive heart failure after myocardial infarction. Am Heart J. 1997;133(3):340–345. doi:10.1016/S0002-8703(97)70230-8
3. Ganguly PK. Antioxidant therapy in congestive heart failure: is there any advantage? J Int Med. 1991;229(3):205–209. doi:10.1111/j.1365-2796.1991.tb00333.x
4. Ganguly PK. Catecholamines and cardiovascular disorders: pathophysiologic considerations. Am Heart J. 1989;118(4):868–872. doi:10.1016/0002-8703(89)90610-8
5. Kaneko M, Chapman DC, Ganguly PK, Beamish RE, Dhalla NS. Modification of cardiac adrenergic receptors by oxygen free radicals. Am J Physio. 1991;260:H821–H826.
6. Ganguly PK. Impaired inotropic responses to adrenergic stimulation following aortic constriction: role of oxidation product of catecholamines. Angiology. 1991;42(2):133–139. doi:10.1177/000331979104200207
7. Ganguly PK, Sherwood GR. Norepinephrine turnover and metabolism in myocardium following aortic constriction in rats. Cardiovasc Res. 1991;25:579–585. doi:10.1093/cvr/25.7.579
8. Ganguly PK, Beamish RE, Dhalla NS. cardio pheoch. Am Heart J. 1989;117(6):1399–1400. doi:10.1016/0002-8703(89)90435-3
9. Dhalla NS. Formation of aminochrome leads to cardiac dysfunction and sudden cardiac death. Circ Res. 2018;123(4):409–411. doi:10.1161/CIRCRESAHA.118.313416
10. Ganguly PK. Neuropeptide Y level in hypothalamus of experimental diabetic rats: correlation with sympathetic activity and body weight. Intern J Gen Med. 2010;3:321–325. doi:10.2147/IJGM.S7749
11. Dhalla KS, Ganguly PK, Rupp H, Beamish RE, Dhalla NS. Measurement of adrenolutin as an oxidation product of catecholamines in plasma. Mol Cell Biochem. 1989;87(1):85–92. doi:10.1007/BF00421086
12. Thomson MJ, Frenneaux MP, Kaski JC. Antioxidants treatment for heart failure. Q J Med. 2009;102:305–310. doi:10.1093/qjmed/hcn160
13. Singh RB, Fedacko J, Pella D, et al. High exogenous antioxidant, restorative treatment (heart) for prevention of the six stages of heart failure: the heart diet. Antioxidants. 2022;11:1464–1468. doi:10.3390/antiox11081464
14. Lahnwong S, Chattipakorn SC, Chattipakaron N. Potential mechanisms responsible for cardioprotective effects of sodium-glucose co-transporter 2 inhibitors. Cardiovasc Diabet. 2018;17:101. doi:10.1186/s12933-018-0745-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.