Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Overcoming Barriers in Nurse-Pharmacist Collaborations on Wards – Qualitative Expert Interviews with Nurses and Pharmacists
Authors Wakob I, Schiek S, Bertsche T
Received 13 February 2023
Accepted for publication 20 March 2023
Published 5 April 2023 Volume 2023:16 Pages 937—949
DOI https://doi.org/10.2147/JMDH.S408390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ines Wakob,1,2 Susanne Schiek,1,2 Thilo Bertsche1,2
1Clinical Pharmacy, Institute of Pharmacy, Medical Faculty, Leipzig University, Leipzig, Germany; 2Drug Safety Center, Faculty of Medicine, University Hospital of Leipzig and Leipzig University, Leipzig, Germany
Correspondence: Thilo Bertsche, Clinical Pharmacy, Institute of Pharmacy, Medical Faculty, Leipzig University and Drug Safety Center, University Hospital of Leipzig and Leipzig University, Bruederstr. 32, Leipzig, 04103, Germany, Tel +49 3 41 97- 11800, Email [email protected]
Purpose: Interprofessional collaboration in healthcare is an essential element in promoting patient safety. However, little research is available on the collaboration between nurses and pharmacists. To optimize processes, mutual understanding is needed, which can be gained by examining the perspectives of those collaborating professional groups. We aimed to identify barriers to the interprofessional collaboration of nurses and pharmacists as well as preconditions and solution strategies to devise approaches for optimizing teamwork in inpatient settings.
Methods: We recruited pairs of collaborating nurses and pharmacists from different hospitals in German-speaking countries and conducted qualitative expert interviews by phone with each of them individually. Transcribed interviews were assessed using qualitative content analysis.
Results: We conducted 12 interviews each with the collaborating nurses and pharmacists. The most frequently mentioned barriers to optimal collaboration were “skepticism due to perception as controller” (reported mainly by pharmacists), “organizational implementation”, and “limited (possibilities of) presence” (reported by both professional groups). A solution strategy proposed to overcome such barriers was “explaining added value”. This added value was found in “clinical-pharmaceutical activities as complement by additional perspective” and “reducing workload in tasks distant from the patient”.
Conclusion: Nurses, pharmacists and hospital management should recognize the added value of intensifying their collaboration regarding patient-related services. A combination of logistical and clinical-pharmaceutical activities should be established at the level of drug application since interviewees endorsed collaboration. A stepwise process must be anticipated to address existing barriers, including some redefinition of professional roles.
Keywords: interprofessional collaboration, interprofessional health teams, pharmacist, nurses, qualitative research
Introduction
Strengthening the professional dialogue between healthcare professionals has resulted in measurable patient benefits by optimizing their pharmacotherapy and avoiding potential adverse drug reactions.1,2 Collaboration between physicians and nurses forms an essential element in this regard. Apart from this, qualitative methodology has been used to investigate collaborations between physicians and pharmacists in the outpatient sector.3
In contrast, inpatient care can be assumed to involve an exceptionally high degree of collaboration not only between pharmacists and physicians but especially between pharmacists and nurses. The involvement of pharmacists on wards is now required by law in a federal state in Germany.4 This will increase the number of pharmacists on the wards, and collaboration with nurses will become even more significant. Internationally, the involvement of pharmacists on the therapeutic team, also collaborating with nurses, has already been established and analyzed in diverse settings.5–10 To derive optimal benefit to the patient from the collaboration, it is necessary to investigate attitudes, barriers and opportunities for the interprofessional collaboration of both nurses and pharmacists. Scant data about the mutual attitudes and expectations of this collaboration have been published so far, especially in the German-speaking countries with comparatively few pharmacists already employed on wards compared to the Anglo-American countries. For this reason, this qualitative study was carried out to identify barriers to collaboration between nurses and pharmacists and possible solution strategies to devise approaches for improving synergetic joint work under the routine conditions of healthcare systems.
Materials and Methods
Study Design
Individual qualitative expert interviews were conducted by phone from April to September 2019. Interviewed experts were a pharmacist and a directly collaborating nurse on the ward in each hospital.
Data Collection
According to the legal regulations, an ethics vote was not required since we did not collect patient-related data or examine existing patient-related data. All data protection regulations were adhered to. Data were collected anonymously after matching the pharmacist-nurse pair. Nurses and pharmacists were invited to take part voluntarily. Informed consent was obtained for participation, recording and transcription of the interviews and publication of anonymized responses. We asked for socio-demographic data, followed by the interview´s main part consisting of open questions. All interviews were conducted by the same person (IW). We developed interview guides containing leading questions for each group (nurses and pharmacists) based on the current status of literature on pharmaceutical activities on wards.6–8,11 The leading questions of the interview guide included topics concerning framework conditions, barriers, solution strategies and future potential for optimization (Table 1). The interviewer trained on handling the interview guides in advance. The results obtained in this context were not included in the evaluation of the main study.
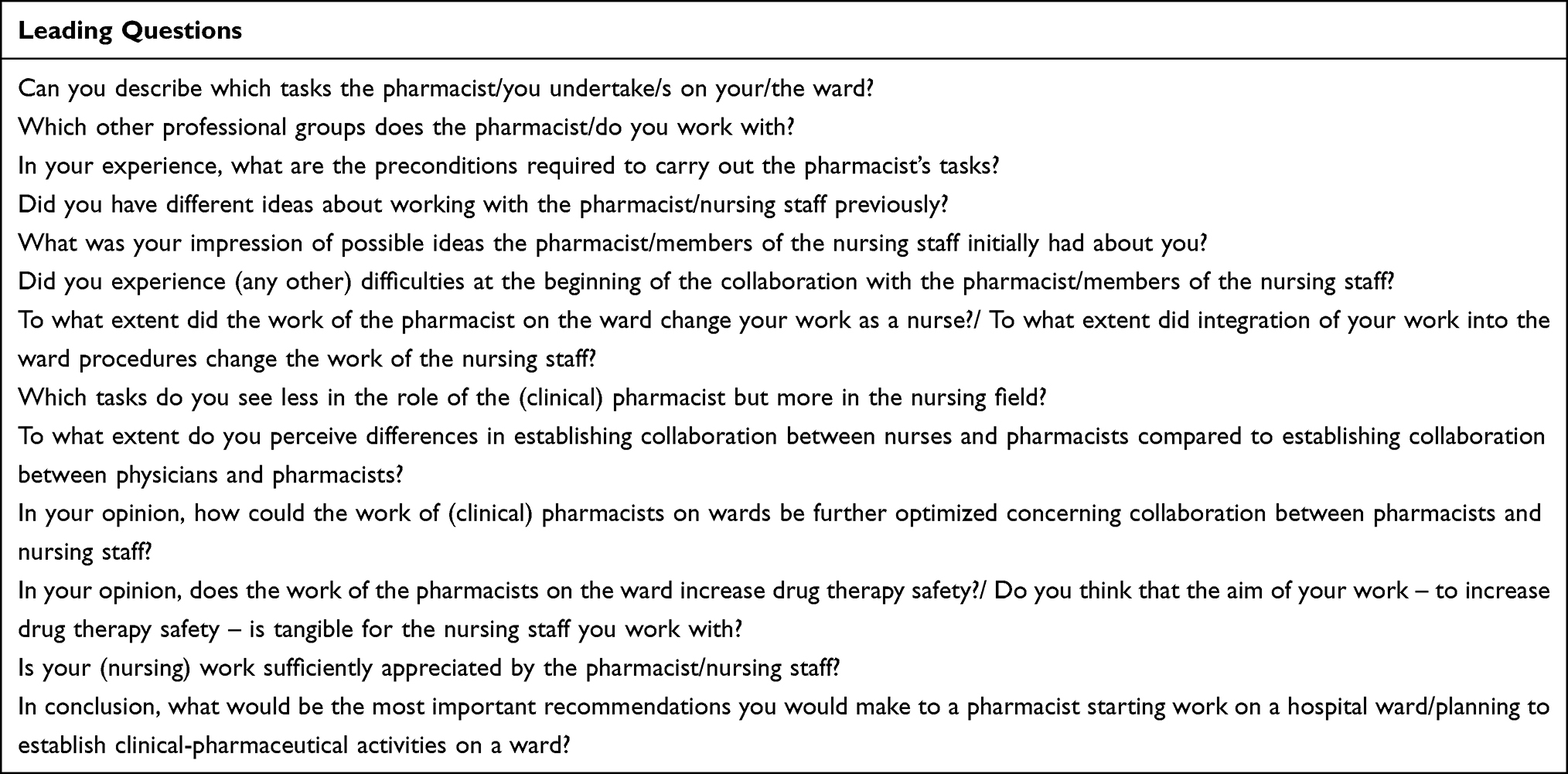 |
Table 1 Interview Guide. Respective Questions to Nurses and Pharmacists Were Mostly Equivalent. Deviations are Shown in the Table. Further (Ad Hoc) Questions Were Possible According to the Qualitative Approach |
Recruitment
Collaborating pairs of nurses and pharmacists in hospitals from German-speaking countries were invited to participate. Recruitment was carried out by phone or email. We aimed to include participants from different regions and a wide range of settings according to the number of beds, from about 300 to more than 1000, representing different levels of hospital care and the progress of interprofessional collaborations. Recruitment was performed in pairs, while each participant was interviewed separately. Pairs of pharmacists and nurses were invited to participate according to our knowledge of their clinical-pharmaceutical activities on wards by personal contacts or visiting respective homepages. The first contact was made with the pharmacist, who then suggested which nurse to recruit.
Data Analysis
Transcripts of each interview were prepared via “f4transkript” (Dr. Dresing & Pehl GmbH, Marburg, Germany). Qualitative content analysis following Kuckartz12 was applied to analyze the transcripts. Categories were developed in a deductive-inductive procedure, and the definitions of the eight main categories are listed in Appendix 1. Subcategories were created inductively based on assigned text passages. The analysis and structured evaluation were supported by “f4analyse”. A comparison of similarities and differences in attitudes and perspectives of each professional group was carried out by comparing the frequency of responses in subcategories.
Results
Sample
We conducted 24 interviews with 12 pairs of nurses and pharmacists in different clinical facilities. Five other hospital pharmacists did not respond to a participation request, and one refused to participate. For data describing the study sample, see Table 2.
 |
Table 2 Study Sample |
Current Fields of Activity and Cooperation Partners
Nurses and pharmacists reported especially medication reviews and the pharmacits´ function as consultants and contact persons of nurses and physicians in the current fields of activity of the pharmacist. In addition, the accompaniment on ward rounds was mentioned 14 times. The pharmacist´s participation in interprofessional morning meetings or nursing handovers was reported 3 times (exclusively by nurses). Integration of pharmacists into the admission or discharge management and direct information and counseling for patients were mentioned fewer times than medication reviews or accompaniment on ward rounds. Furthermore, information and counseling represented a field of activity for nursing staff while the pharmacist was assigned to
Train the trainers. (P09)
Regarding side effect management, the subcategory “observation of side effects by nursing staff (proximity to patient)” was emphasized by both nursing staff and pharmacists.
Beyond fields of activity in collaboration with nursing staff, physicians particularly were named as cooperation partners during the on-ward participation of pharmacists in the units.
Differences in Collaboration with Various Cooperation Partners
Pharmacists, as well as nurses, consider the pharmacist to be both a “controller” and a “supporter”. The pharmacist´s collaboration with various healthcare professionals was considered to be different:
The first thing coming to mind when I think about the development of collaboration with nursing staff is rather to show them that we are on the same level and I am not above them. And for physicians, it´s the other way around, to demonstrate to the physicians that I am not below them but that I am indeed on the same level as they are. (P06)
“Level of collaboration”, mentioned especially by pharmacists and “willingness to cooperate” were other topics. Levels of collaboration distinguished were a technical content-related “prescription level” with physicians and an executive “process and application level” with nurses. In addition, the “gap” resulting from the delegation of certain activities from physicians to nurses was thematized as a field of activity for a clinical pharmacist.
Concerning the subcategory “patient orientation”, pharmacists were assigned a “theoretical, specific view of the patient and his therapy”, and physicians and nurses were assigned a “practical, comprehensive, more patient-individual view”. This subcategory was mainly made a subject of discussion by nurses. (For more differences in frequency of statements see Appendix 2.)
Preconditions for Exercising Clinical-Pharmaceutical Activities on a Ward
Participants of both professional groups mentioned preconditions regarding the “support of hospital management” and “resources”:
The recognition of the need. Because I don´t think that […] management levels of many hospitals do even see the need. And the need definitely exists. (N09)
Yes, so you should [...] be given the posts. So just full-time equivalents, they’re important. You can’t just do it alongside, on top of your normal job; it’s difficult, depending on what department you’re in. (P12)
Furthermore, “organization” and “interprofessionality” were mentioned as preconditions:
Start from scratch, in a way that you don´t want too much right away, but instead begin at one ward. (P01)
Most important is that […] social interaction is a major concern to [the pharmacist]. That he integrates himself […] into the team. (N06)
Preconditions concerning the pharmacist himself were “pharmacist´s experience” as well as “pharmacist´s soft skills” and “pharmacist´s hard skills”:
That, if necessary, one also sits in again before starting somewhere, preferably in the department he will work in afterward. (P10)
Communication is also quite important because simply identifying drug-related problems is not sufficient to be able to solve them in a sustainable way for the patient. (P03)
The ´specialist pharmacist for clinical pharmacy´ is not necessarily [required] because you indeed have to provide clinical-pharmaceutical services for the practical tasks, and the workshops are partly also quite good, but depending on the specialty, or depending on the discipline, you need much more in-depth knowledge than the specialist pharmacist can impart. So, I think a specialization in one discipline or in various disciplines makes sense. (P10)
Barriers
Most prominent barriers were “skepticism due to perception as controller” (especially among pharmacists) as well as “organizational implementation” with “restructuring of stable, established processes” (mentioned by five pharmacists and nurses each) and “limited (possibilities of) presence” (mentioned by six pharmacists and three nurses). Subcategories are presented in Figure 1. Illustrative quotations for the different subcategories are given in Table 3.
 |
Table 3 Sample Quotations for Subcategories of Main Category “Barriers” |
 |
Figure 1 Barriers. The hierarchical subcategory system is presented as a concept map for the main category “barriers”; decreasing intensity of grey levels = decreasing hierarchy levels. Thematic subcategories with apparent professional group-specific differences in the frequency of interviewees with mentions are presented in bold bordered. (“Skepticism due to perception as controller” was mentioned by 3 nurses versus 10 pharmacists; “Pharmacist first needs to prove his expertise to physicians and nursing staff” was not mentioned by any nurse, but 4 pharmacists; 1 nurse and 7 pharmacists mentioned “missing reward”). |
Solution Strategies
Solution strategies most frequently mentioned (by at least one-third of all participants) were “explaining added value”, “patience”, “clarification of the main focus on support/completion”, “availability as contact person”, and “communication methods”. Subcategories are presented in Figure 2. Illustrative quotations for the different subcategories are given in Table 4.
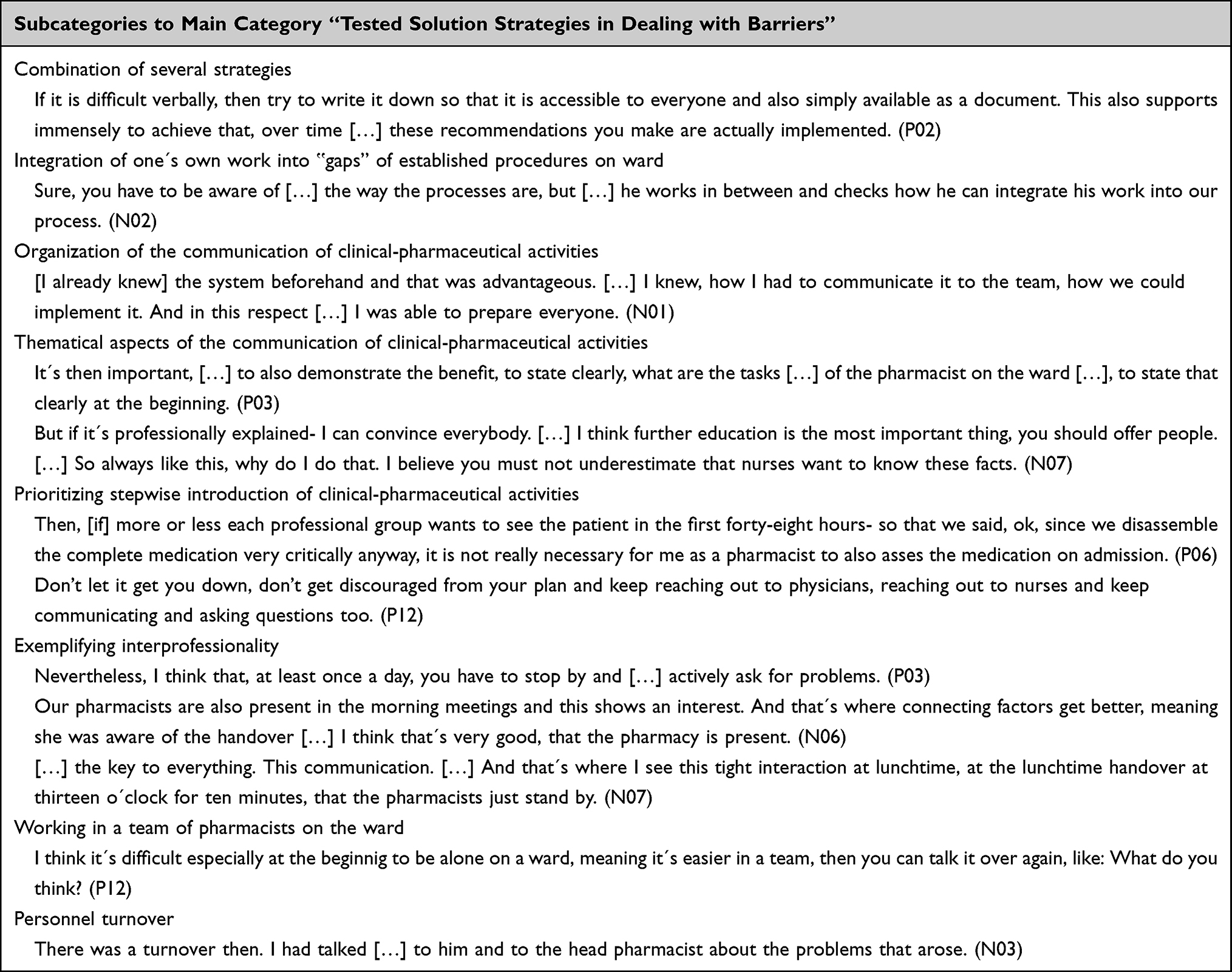 |
Table 4 Sample Quotations for Subcategories of Main Category “Tested Solution Strategies in Dealing with Barriers” |
 |
Figure 2 Solution strategies to barriers. The hierarchical subcategory system is presented as a concept map for the main category “tested solutions in dealing with barriers”; decreasing intensity of grey levels = decreasing hierarchy levels. Thematic subcategories with conspicuous professional group-specific differences in the frequency of interviewees with mentions are presented in bold bordered. (“Patience” was mentioned by 2 nurses and 8 pharmacists; “Explaining added value” was mentioned by 2 nurses and 6 pharmacists; and “Optimized communication of errors” was mentioned by 3 nurses and 8 pharmacists). |
Added Value
The added value was considered in two domains: Clinical-pharmaceutical activities as “complement by additional perspective” and in “reducing workload in tasks distant from the patient” (Figure 3).
 |
Figure 3 Added value. Subcategories of category “Added values for/from the point of view of nursing staff by the clinical pharmacist on the ward”; black: number of nurses with mentions; shaded: number of pharmacists with mentions. |
Potential for Optimization
The subcategories defined as optimization potential are “focusing on collaboration with nursing staff in general”, “more service-offering by pharmacy”, “supply of clinical-pharmaceutical activities at patient level”, “development of technological conditions”, “support of basic conditions promoting interprofessionality”, “enhanced pharmaceutical-technical dialogue with nursing staff” and “organization of dialogue with nursing staff” itself:
I would imagine making flying visits as a pharmacist in the morning. It would be that way every morning, one or two hours, each of us is assigned to one ward, goes there and discusses problems. That, at least in principle. (P04)
Such an “increasing the pharmacist´s presence on the ward/in the charge office” was requested by nursing staff and pharmacists with similar frequency, although concerns were expressed twice:
One should not lose touch with the pharmacy. To be on the ward exclusively means you lose the basis or roots a little bit. Then you might no longer incorporate recommendations of your colleagues in the pharmacy, but you are working only with physicians, and you possibly also adopt their opinion, which is actually not supposed to be the intention, but you should approach the situation from a different point of view. (P10)
I think if […] the pharmacist was always sitting here for eight hours, people would feel controlled. […] Well, they know he´s available, they know, he´s always available for us, and that´s quite good enough. (N10)
Presence is also linked to the subcategory “fixed person” within the main category “added value for/from the point of view of nursing staff by the clinical pharmacist on the ward”, which has been mentioned by nurses and pharmacists with equal frequency.
Concerning the development of technological conditions, pharmacists particularly wish for the electronic patient file to be established. Nevertheless, they remark on the risk of a decreasing presence on the ward.
Occasionally, pharmacists identified the potential for optimization in “strengthened accompaniment of the individual patient´s process by the pharmacist”.
Discussion
Studies on the interprofessional collaboration of pharmacists currently focus mainly on pharmacists’ relationships with physicians rather than nurses. However, close collaboration between nurses and pharmacists is essential since nurses are usually involved at the end of the medication process for administration. We, therefore, explored a wide range of clinical facilities and performed a qualitative approach. By this, we identified various experiences concerning collaboration to identify preconditions, current fields of activities, barriers and solution strategies to overcome them, as well as added value and optimization potential.
Our findings support the optimization of interprofessional collaboration between nurses and pharmacists.
Both professional groups endorse collaboration. However, it may only work out after a period of time. So the need for patience during implementation towards nursing staff and pharmacists was mentioned. On the one hand, it is necessary to change the routine procedures of nursing staff over a more extended time and overcome resistance from the nursing staff. On the other hand, pharmacists also have to plan time to adjust to working with nursing staff and recognize and address their needs. Overall, therefore, implementation will take time to take place and should be carried out step by step in small stages. Our study indicates the need to define the pharmacist’s role on the ward and combine the different perspectives. Beyond the role of the logistician and “controller”, in which pharmacists predominantly perceive themselves, the challenges in the pharmacist’s current patient-centered professional practice necessitate specifying their position as a health care professional increasingly providing pharmaceutical services. Both professional groups see added value in “reducing workload in tasks distant from the patient”, as was identified in our interviews.
Furthermore, an additional perspective was reported as a result of this study to be a great advantage of the extended collaboration. Therefore, it is reasonable that respondents requested pharmacists’ hard skills, such as specialist knowledge acquired from pure factual knowledge. But in addition, when implementing these services on the ward, soft skills and the integration of pharmaceutical expertise with the proximity of the nursing staff to the patient are mentioned as valuable. They are crucial to devising recommendations for increasing individual patients´ pharmacotherapy safety.
To exploit these potential benefits, interviewees stated that the enhancement of time and technical resources is a primary requirement for implementing enduring, beneficial collaboration of nurses and pharmacists on wards.
Different and Shared Perspectives of Pharmacists and Nurses on Collaboration
We identified that pharmacists perceived a barrier in “skepticism due to perception as controller”, such as legally required inspections of wards and demands for certain drugs, which are often linked to economic aspects.13
This barrier existing in the perception of the pharmacist as a controller was less frequently mentioned by nursing staff, and it is rather conspicuous that they even appreciated additional control. Furthermore, only pharmacists noted that the pharmacist first must prove his expertise to physicians and nursing staff. This contrasts with nurses, who favored having research tasks taken off their hands and reported that gaining background knowledge themselves on a drug-information-based level was an added value. The pharmacists seem less aware of this view of nursing staff because it was hardly mentioned. They might need to take advantage of the opportunity to use this potential way to build cooperation and strengthen their role as a healthcare professional.
The fact that pharmacists consider their role of controller to be such a barrier may also explain why they emphasized the following approaches to overcoming barriers more often than the interviewed nurses: “optimized communication of errors”, “explaining added value”, and “patience”. Differences (person-related) in readiness for collaboration must be expected.14 So, more general strategies were referred to, such as the need for patience, among others involving acceptance by nurses. This is generally known from change management processes in various organizations,15 even concretely in the introduction of clinical pharmacists on wards.16 Individual components might be expressed by rejection as the stable, established processes of the daily routine of the ward and time schedules of the nursing staff are restructured when a pharmacist is integrated into the team, which initially seems uncomfortable This prevents the added value from being immediately grasped.
To facilitate, our results indicate the need for a precise definition of the activities of the clinical pharmacist, which is in line with other studies.5,16 Our interviewees reported mediators from the nursing team to support establishing clinical-pharmaceutical activities. In addition, they mentioned the benefit of regular meetings. The literature emphasizes their necessity as concepts should be constantly re-evaluated and revised in an iterative improvement process – the plan-do-check-act model.17
Duration of the implementation process is also determined by the pharmacist´s soft skills, which were referred to, and according to the time of pharmacists’ presence on site. This was desired to be increased by both professional groups. International studies confirm the presence of the pharmacist on the ward as beneficial.16 Therefore, the collaboration between nurses and pharmacists should be strengthened by regular appointments explicitly between these professional groups and by one pharmacist being a fixed contact person. Omitting a fixed assignment of the pharmacist to the ward may complicate proceedings.18 On the other hand, rotation principles can offer better sustainability through substitution arrangements, which can also ensure consistency and thus facilitate change management. This is a multifactorial decision and, therefore, can be different for each specific hospital.
Role of the Pharmacist as a Healthcare Professional on the Ward
According to our results, logistical activities can open doors to initiating collaboration with nursing staff on the ward and thus pave the way for future clinical-pharmaceutical activities. Initial expectations towards the pharmacist are predominantly linked to logistical aspects.6 We found that assistance with tasks such as these, which are distant from the patient, was cited as an additional value. Therefore, a total separation of logistical and clinical-pharmaceutical activities is not appropriate. Pharmacists also emphasized that they should keep in touch with the pharmacy in the drug supply sector.
The focus of current clinical-pharmaceutical activities identified by the interviewees of our study is the establishment of medication reviews. Involvement in crucial admission and discharge procedures, for example, is less likely to be implemented, which is in line with the results of other studies.19,20 This may be due to the comparatively time saving implementation because medication reviews can be performed independently of ward workflows at more flexible times by the pharmacist – especially with the implementation of digital patient records. This way, the initial objective is to address the prescription level in collaboration with the physician, similar to pharmacists accompanying physicians’ ward rounds, which was also mentioned quite often. On the other hand, counseling and training of nursing staff are reported as general tasks. Still, data collected suggest this is more likely to be an activity often carried out on the side in everyday life. More detailed concepts of pharmaceutical-nursing collaboration are desirable, including the drug-information-based and patient-individual levels. In this context, management of adverse drug events might offer opportunities due to the frequently emphasized proximity of nursing staff to the patient in our interviews.
The pharmacist assessing the patient case on a theoretical level, as reported by the interviewees, and thus adding the pharmaceutical perspective as an additional one, ought to be the aim. Nonetheless, the pharmacists´ lack of patient orientation in everyday clinical practice mentioned by both professional groups in our study is not negligible. In this regard, the pharmacist should recognize nursing staff as partners and utilize increased collaboration to assess better his pharmaceutical activity’s clinical relevance in the individual patient case.
However, to implement such interprofessional projects of nurses and pharmacists, support by hospital managements and resources were emphasized as preconditions in our study. Furthermore, missing rewards and limited possibilities for the presence on wards were cited as barriers.
Limitations in resources are a barrier to clinical-pharmaceutical activity.20,21 Despite some international studies, the problem of recording cost reductions by a clinical pharmacist still needs to be solved.22,23 Therefore, resources for implementing clinical-pharmaceutical activities on wards will remain restricted, especially without specific legal requirements.
Outlook
Concerning the clinical-pharmaceutical activities of pharmacists in hospitals, the benefits for patient safety in practice and clinical trials are increasingly recognized.24–27
It should be further explored how pharmacotherapy on a patient-individual level might be improved by structuring collaboration between professional groups of pharmacists and nurses exceeding logistics. Furthermore, it has to be evaluated how the adaption of concepts to the needs and resources of individual settings can be managed.
Limitations
Since the nurse-pharmacist pairs interviewed had already implemented collaborations, it can be assumed that they were particularly motivated to collaborate. Furthermore, pharmacists suggested nurses to recruit and likely named cooperative nurses. They may already have overcome potential barriers, which may limit the general applicability of the results to other settings. However, this was not an aim of the qualitative approach. But due to recall bias, certain barriers may be underrepresented.
Interviews were conducted by a pharmacist, as specific prior knowledge of the work situation on the ward was required to perform the interviews. To counteract potential uncertainty among the nursing staff, it was emphasized in the introduction of each interview that answers are analyzed anonymously and not judged.
Interviews were carried out by phone, making it impossible to capture gestures and facial expressions. However, it was the most practical way to conduct the interviews widely across the German-speaking regions. We do not assume any substantial restriction of data quality for our purpose since carrying out the interviews worked out easily in this way.
Acknowledgments
We thank all participating nurses and pharmacists for contributing to the study, for taking the time for the interviews, and for the valuable experiences that were shared. We thank Katharine Worthington for the language editing of the manuscript.
Funding
We acknowledge support from Leipzig University for Open Access Publishing.
Disclosure
The authors report no conflict of interest in this work.
References
1. Langebrake C, Hilgarth H. Clinical pharmacists´ interventions in a German university hospital. Pharm World Sci. 2010;32:194–199. doi:10.1007/s11096-010-9367-z
2. Hahn M, Ritter C, Roll SC. Validation of pharmacist-physician collaboration in psychiatry: the Eichberger-model. Int J Clin Pharm. 2018;40(5):1001–1004. doi:10.1007/s11096-018-0664-2
3. Weissenborn M, Haefeli WE, Peters-Klimm F, Seidling HM. Interprofessional communication between community pharmacists and general practitioners: a qualitative study. Int J Clin Pharm. 2017;39(3):495–506. doi:10.1007/s11096-017-0450-6
4. Law amending the lower saxony hospital law and other regulations. Nds GVBl. 2018;14:214–216.
5. Sjölander M, Gustafsson M, Gallego G. Doctors’ and nurses’ perceptions of a ward-based pharmacist in rural northern Sweden. Int J Clin Pharm. 2017;39:953–959. doi:10.1007/s11096-017-0488-5
6. Halvorsen KJ, Stensland P, Granas AG. A qualitative study of physicians´and nurses´experiences of multidisciplinary collaboration with pharmacists participating in case conferences. Int J Pharm Pract. 2011;19:350–357. doi:10.1111/j.2042-7174.2011.00129.x
7. Bell HT, Granas AG, Enmarker I, Omli R, Steinsbekk A. Nurses´and pharmacists´ learning experiences from participating in interprofessional medication reviews for elderly in primary health care – a qualitative study. BMC Fam Pract. 2017;18:30. doi:10.1186/s12875-017-0598-0
8. Wilbur K, Kelly I. Interprofessional impressions among nursing and pharmacy students: a qualitative study to inform interprofessional education initiatives. BMC Med Educ. 2015;15(1):53. doi:10.1186/s12909-015-0337-y
9. Austin Z, Ensom MHH. Education of pharmacists in Canada. Am J Pharm Educ. 2008;72(6):128. doi:10.5688/aj7206128
10. Baqir W, Crehan O, Murray R, Campbell D, Copeland R. Pharmacist prescribing within a UK NHS hospital trust: nature and extent of prescribing, and prevalence of errors. Eur J Hosp Pharm. 2015;22:79–82. doi:10.1136/ejhpharm-2014-000486
11. Shemeili SJ, Klein S, Strath A, Fares S, Stewart D. An exploration of health professionals´ experiences of medicines management in elderly, hospitalised patients in Abu Dhabi. Int J Clin Pharm. 2016;38:107–118. doi:10.1007/s11096-015-0212-2
12. Kuckartz U. Qualitative content analysis. Methods, practice, computer support. Beltz Juvent. 2018;4:95.
13. Johnston A, Asmar R, Dahlöf B, et al. Generic and therapeutic substitution: a viewpoint on achieving best practice in Europe. Br J Clin Pharmacol. 2011;72:727–730. doi:10.1111/j.1365-2125.2011.03987.x
14. Kendall S, Deacon-Crouch M, Raymond K. Nurses’ attitudes toward their role in patient discharge medication education and toward collaboration with hospital pharmacists: a staff development issue. J Nurses Staff Dev. 2007;23(4):173–179. doi:10.1097/01.NND.0000281416.04731.3e
15. Elrod PD, Tippett DD. The “Death valley” of change’. J Organ Chang Manag. 2002;15(3):273–291. doi:10.1108/09534810210429309
16. Lindqvist MH, Gustafsson M, Gallego G. Exploring physicians, nurses and ward-based pharmacists working relationships in a Swedish inpatient setting: a mixed methods study. Int J Clin Pharm. 2019;41(3):728–733. doi:10.1007/s11096-019-00812-8
17. Johnson CN. The benefits of PDCA. Qual Prog. 2002;35(5):120.
18. Bryant R, Chaar B, Schneider C. Differing clinical pharmacy service models: quantitative and qualitative analysis of nurse perceptions of support from pharmacists. Int J Nurs Stud. 2018;86:90–98. doi:10.1016/j.ijnurstu.2018.04.003
19. Schulz C, Fischer S, Fischer A, et al. Survey on status quo of the work of clinical pharmacists in German hospital pharmacies.
20. Grandt D, Löffert S, Steffen P, et al. AMTS und der Einsatz von Apothekern im Krankenhaus. [Medication safety in hospitals in Germany and contribution of pharmacists]. Krankenhauspharmazie. 2022;43:320–325. German.
21. Frontini R, Miharija-Gala T, Sykora J, Survey EAHP. 2010 on hospital pharmacy in Europe: part 1. General frame and staffing. Eur J Hosp Pharm. 2012;19:385–387. doi:10.1136/ejhpharm-2012-000162
22. Jourdan JP, Muzard A, Goyer I, et al. Impact of pharmacist interventions on clinical outcome and cost avoidance in a university teaching hospital. Int J Clin Pharm. 2018;40(6):1474–1481. doi:10.1007/s11096-018-0733-6
23. Dawoud DM, Smyth M, Ashe J, et al. Effectiveness and cost effectiveness of pharmacist input at the ward level: a systematic review and meta-analysis. Res Social Adm Pharm. 2019;15(10):1212–1222. doi:10.1016/j.sapharm.2018.10.006
24. De Winter S, Spriet I, Indevuyst C, et al. Pharmacist- versus physician-acquired medication history: a prospective study at the emergency department. Qual Saf Health Care. 2010;19(5):371–375. doi:10.1136/qshc.2009.035014
25. Rothschild JM, Churchill W, Erickson A, et al. Medication errors recovered by emergency department pharmacists. Ann Emerg Med. 2010;55(6):513–521. doi:10.1016/j.annemergmed.2009.10.012
26. Chiu PKC, Lee WK, See YW, Chan HW. Outcomes of a pharmacist-led medication review programme for hospitalized elderly patients. Hong Kong Med J. 2018;24(2):98–106. doi:10.12809/hkmj176871
27. Seiberth S, Mannell H, Birkenmaier C, et al. Benefit of medication reviews by renal pharmacists in the setting of a computerized physician order entry system with clinical decision support. J Clin Pharm Ther. 2022;47(10):1531–1538. doi:10.1111/jcpt.13697
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
What It Takes to Manage Change: A Qualitative Study of Healthcare Managers’ Role Perceptions in Supporting and Sustaining TeamSTEPPS Implementation
Lüchinger R, Blondon K, Junod Perron N, Audétat MC
Journal of Healthcare Leadership 2026, 18:584769
Published Date: 30 April 2026