Back to Journals » Infection and Drug Resistance » Volume 15
Outcomes and Risk Factors of Bloodstream Infections Caused by Carbapenem-Resistant and Non-Carbapenem-Resistant Klebsiella pneumoniae in China
Authors Liang X, Chen P, Deng B, Sun FH, Yang Y, Yang Y, He R, Qin M, Wu Y, Yang F, Tian GB, Dai M
Received 23 March 2022
Accepted for publication 3 June 2022
Published 17 June 2022 Volume 2022:15 Pages 3161—3171
DOI https://doi.org/10.2147/IDR.S367588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xiaoxue Liang,1,* Ping Chen,2,* Baoguo Deng,2,* Feng-Hui Sun,1,* Yongqiang Yang,3– 5 Yanxian Yang,3,4 Ruowen He,3,4 Mingyang Qin,2 Yiping Wu,3,4 Fan Yang,2 Guo-Bao Tian,3,4 Min Dai1
1School of Laboratory Medicine, Chengdu Medical College, Chengdu, Sichuan Province, People’s Republic of China; 2School of Basic Medical Science, Xinxiang Medical University, Xinxiang, Henan Province, People’s Republic of China; 3Department of Microbiology, Zhongshan School of Medicine, Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China; 4Key Laboratory of Tropical Diseases Control (Sun Yat-sen University), Ministry of Education, Guangzhou, Guangdong Province, People’s Republic of China; 5School of Pharmaceutical Sciences (Shenzhen), Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Min Dai, School of Laboratory Medicine, Chengdu Medical College, Chengdu, Sichuan Province, People’s Republic of China, Tel +86 28-62739128, Email [email protected]
Purpose: To compare antimicrobial resistance, virulence, clinical characteristics, and risk factors between carbapenem-resistant K. pneumoniae (CRKP) and carbapenem-susceptible K. pneumoniae (CSKP) isolates from patients with bloodstream infections (BSIs) in China.
Patients and Methods: The clinical data of 103 patients with K. pneumoniae BSI from 10 hospitals were retrospectively analyzed. The minimum inhibitory concentrations of 15 antibiotics against the bacteria were determined. A Galleria mellonella infection model was used to evaluate virulence of the isolates. Kaplan–Meier curves were calculated to evaluate the 28-day and in-hospital survival rates of the isolates. The risk factors for CRKP and CSKP infection and respective mortality rate were evaluated by univariate analysis, and independent risk factors were evaluated using the multivariate logistic regression model.
Results: Our results indicated that CRKP isolates were more resistant to most tested antibiotics than CSKP isolates. The G. mellonella infection model was used to demonstrate that CRKP isolates were more virulent than CSKP isolates. We found that in-hospital deaths occurred in 39.3% (22/56) of patients with CRKP BSIs and were significantly higher than those in patients with CSKP infections (19.1%, 9/47). Patients infected with CRKP isolates had poorer outcomes than those infected with the CSKP strains. For in-hospital mortality of CRKP BSIs, the independent risk factors included carbapenem-resistant Enterobacterales bacteremia and length of hospitalization after the onset of BSI.
Conclusion: Our findings confirm that CRKP isolates are more drug-resistant than CSKP isolates and are associated with poorer outcomes. To prevent CRKP infection, strict infection control strategies and active surveillance should be implemented in hospitals.
Keywords: Klebsiella pneumoniae, bloodstream infections, virulence, antimicrobial resistance
Introduction
Klebsiella pneumoniae is the most common pathogen that causes bloodstream infections (BSIs), pneumonia, peritonitis, and urinary tract infections.1 The China Antimicrobial Resistance Surveillance Network revealed that the isolation rate of K. pneumoniae ranked second among gram-negative bacteria in 2020. The first case of carbapenem-resistant K. pneumoniae (CRKP) was reported in the 1990s.2 In the following decades, CRKP was reported in the USA,3 Israel,4 Europe,5,6 and China.7–9 Notably, public health is threatened by BSIs caused by CRKP. The mortality rates caused by CRKP infections in Europe, South America, Asia, and North America are reportedly 50.06%, 46.71%, 44.82%, and 33.24%, respectively.5 In addition, the medical costs of CRKP-infected patients are higher than those of carbapenem-susceptible K. pneumoniae (CSKP)-infected patients during hospitalization.10
Previous researchers paid attention to the monitoring of long-term antibiotics of Klebsiella pneumoniae,11 the predictors of CRKP strain infection12,13 and the effect of CRKP isolates on patients’ clinical relevance,6,14–16 however, few studies have compared the differences between CRKP and CSKP strains in BSIs. Here, we conducted a retrospective case-control study in Guangdong Province, China. In this study, 103 strains were collected from 10 hospitals between 2010 and 2018. The antimicrobial resistance, virulence, clinical characteristics, and risk factors of the CRKP and CSKP isolates from patients with BSIs were clarified.
Materials and Methods
Isolated Bacteria
Between 2010 and 2018, 103 K. pneumoniae isolates were collected from the blood of patients with BSIs in 10 tertiary hospitals in Guangdong Province, China. The isolates were cultured, and species were identified by 16S rRNA sequencing and MALDI-TOF MS (Bruker Daltonik GmbH, Bremen, Germany). Universal primer 27F (5’-AGRGTTYGATYMTGGCTCAG-3’) and 1492R (5’-RGYTACCTTGTTACGACTT-3’) were used to amplify the full-length 16S rRNA gene.17
Patient Demographics
Information regarding demographics, comorbidities (hypertensive, diabetes diseases, coronary heart disease, hematogenous tumor cancer, and other chronic diseases), location before admission, health-care exposures before BSI onset (previous hospitalization within 12 months, or intensive care unit [ICU] admission, surgery, immunosuppressive therapy, or antibiotic exposure within 30 days), or underlying diseases were collected as primary data; Sources of infection (central-line; pneumonia or ventilator; infections of cardiovascular or gastrointestinal systems, surgical sites, urinary tract, skin and soft tissue, reproductive tract; mechanical ventilation; central vein catheterization; septic shock; change in antibiotic treatment after positive culture results; or carbapenem-including treatment) were also collected together with microbiological data, length of hospitalization, antimicrobial therapies, and patient outcomes.
BSI onset was defined as the date of collection of an isolate that resulted in a positive blood culture. BSI can be divided into community-acquired (CA) and hospital-acquired (HA), based on the location of onset. CA-BSI patients were defined as blood culture-positive patients who had been hospitalized for <48 h and had not been hospitalized in the past 6 months. On the contrary, HA-BSI was defined as a positive blood culture from a patient 48 hours after hospitalization or a positive blood culture from a patient hospitalized for <48 h but who had been hospitalized within the past 6 months.4
Antimicrobial Susceptibility Testing (AST)
The agar dilution method was used for AST, and the breakpoints of polymyxin B and tigecycline were explained based on the breakpoints of the European Committee on Antimicrobial Susceptibility Testing (EUCAST) and those of other antimicrobials were based on the Clinical and Laboratory Standards Institute guidelines (CLSI).18
The 15 antimicrobial agents tested were cefotaxime, ceftazidime, cefepime, colistin, tigecycline, imipenem, ertapenem, meropenem, ciprofloxacin, fosfomycin, trimethoprim-sulfamethoxazole, piperacillin-tazobactam, amikacin, gentamicin, and aztreonam. Isolates with imipenem and/or meropenem minimum inhibitory concentrations (MICs) ≥4 μg/mL or ertapenem MICs ≥2 μg/mL were defined as CRKP.19
Construction of a Galleria Mellonella Infection Model
Virulence of the CRKP and CSKP strains was measured using a G. mellonella model.20,21 11 strains were randomly selected from the CRKP and CSKP groups respectively, and the larvae were infected with the concentrations of 1×104 CFU/mL. Escherichia coli MG1655 was used as the non-toxic control and K. pneumoniae strain Hvkp4 as the highly toxic control as previously reported.21 The wax moth larvae were incubated in a dark room at 37 °C, and the survival rate was recorded every 12 h for 7 days.
Statistical Analysis
Statistical analyses of the data were performed using IBM SPSS. Categorical variables are presented as numbers and percentages and compared using the chi-square or Fisher’s exact test. In addition, continuous variables are indicated by the median and interquartile range (IQR; non-normally distributed data) or standard deviation (SD; normally distributed data) and mean. Continuous variables were compared according to their distributions using the nonparametric Mann–Whitney U-test or Student’s t-test. The results of the univariate analysis are indicated by P values and odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance (two-tailed) was defined as P<0.05.
Results
Patient Demographics
In this study, 103 K. pneumoniae strains were collected from patients with BSIs between 2010 and 2018 (Figure 1A and Table 1). Based on the AST results (Table 2), of the 103 strains included, 56 (54.4%) were CRKP and 47 (45.6%) were CSKP. 73 (70.87%) patients were male (37.87% and 33.01% in the CRKP and CSKP groups, respectively), and 30 (29.13%) were female (Table 1). The median age of CRKP-infected patients was 27 years (IQR 0–61) and CSKP patients was 10 years (IQR 0–61) (P = 0.48); almost half of the CRKP group was 0–17 years old (48%), followed by 41–65 years (29%) and ≥ 66 years (18%) (Figure 1B). CSKP isolates were mainly detected in 0–17 years old, 41–65 years old (58%), and ≥ 66 years old (58%, 21%, and 17%, respectively) (Figure 1C).
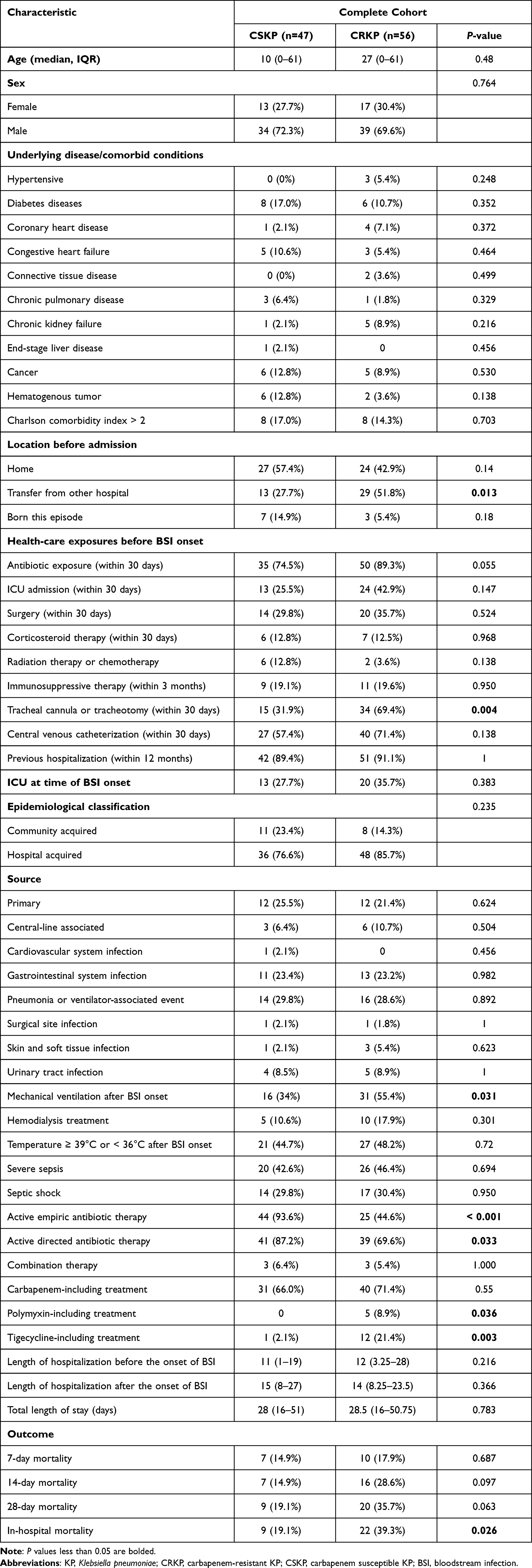 |
Table 1 Characteristics of Patient Cohorts |
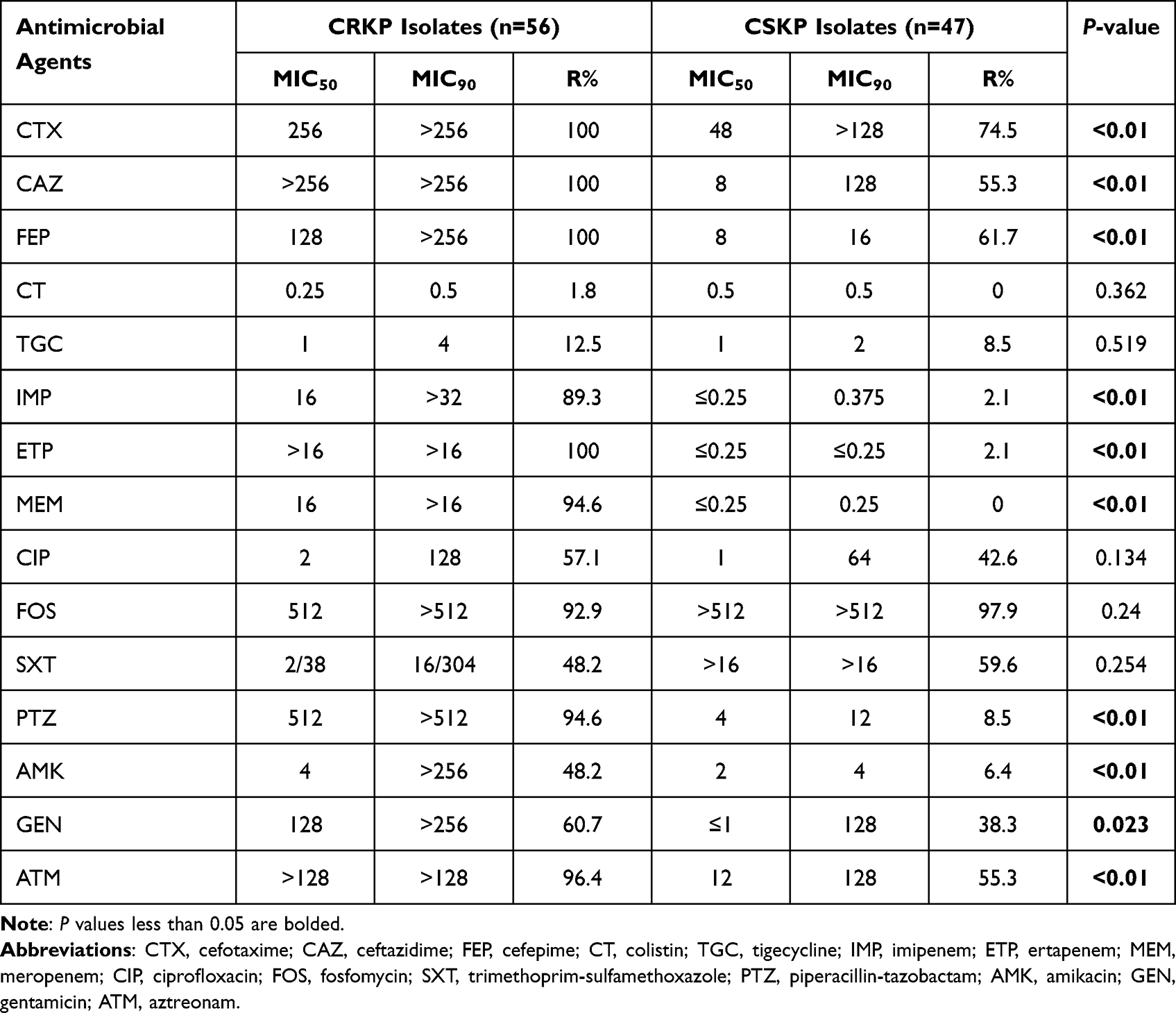 |
Table 2 Antimicrobial Spectrum Evaluation Percentage of Carbapenem-Resistant Klebsiella pneumoniae Isolates Resistance to Various Antibiotics |
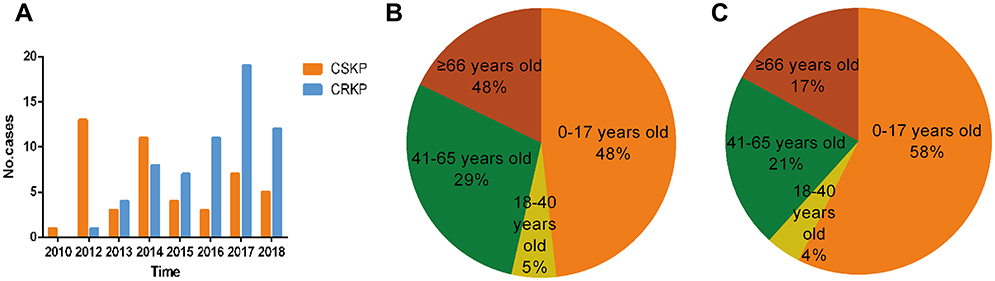 |
Figure 1 (A) Isolation of CRKP and CSKP over the past 9 years. CRKP isolates increased almost every year, and most strains were isolated in 2017. (B) Age distribution of patients with CRKP strains. (C) Age distribution of patients with CSKP strains. Abbreviations: KP, Klebsiella pneumoniae; CRKP, carbapenem-resistant KP; CSKP, carbapenem-susceptible KP. |
CRKP Strains Were More Resistant to Most Antibiotics Compared with CSKP Strains
All 103 K. pneumoniae strains were tested for susceptibility against 15 antibiotics (Figure 2, Table 2). In addition to carbapenem resistance, the CRKP group had a higher resistance rate among other antibiotics than the CSKP group, except for FOS, among which cephalosporins showed 100% non-susceptibility rates. The lowest non-sensitive rates in the CRKP group were for colistin (1.8%) and tigecycline (12.5%) (Figure 2). The value of MIC50 and MIC90 of the CRKP group were higher than those of the CSKP group (Table 2). The resistance rates to cefotaxime, cefepime, imipenem, ertapenem, meropenem, piperacillin-tazobactam, amikacin, aztreonam, and gentamicin in the CRKP group were higher than those in the CSKP group (P < 0.01) (Table 2).
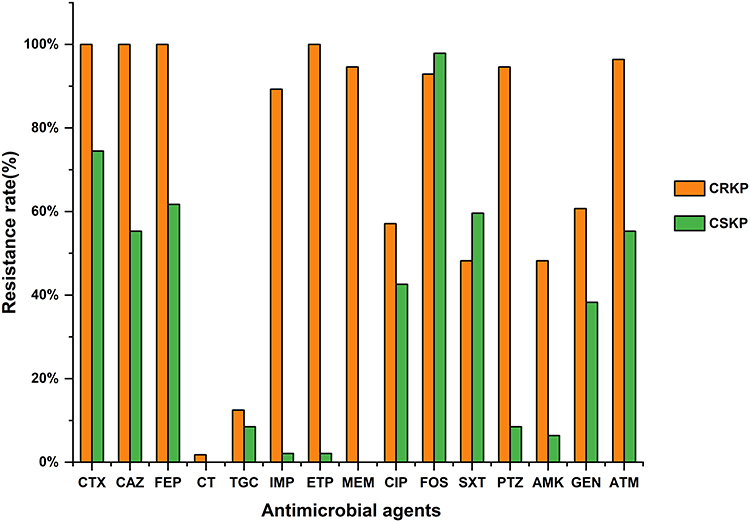 |
Figure 2 Resistance rate of CRKP and CSKP to antimicrobial agents. Abbreviations: CTX, cefotaxime; CAZ, ceftazidime; FEP, cefepime; CT, colistin; TGC, tigecycline; IMP, imipenem; ETP, ertapenem; MEM, meropenem; CIP, ciprofloxacin; FOS, fosfomycin; SXT, trimethoprim-sulfamethoxazole; PTZ, piperacillin-tazobactam; AMK, amikacin; GEN, gentamicin; ATM, aztreonam. |
CRKP Strains Had Higher Pathogenicity Than CSKP Strains
Using the G. mellonella infection model to predict the toxicity of strains, we randomly selected 11 strains from both the CRKP and CSKP groups. The results showed that the survival rate of the CRKP group was significantly lower than that of the CSKP group (P < 0.05; Figure 3A). The fatality rate of the CRKP group was significantly higher than that of the CSKP group from 12 to 168 h (P < 0.05; Figure 3B). The highly virulent K. pneumoniae strain Hvkp4 was used as a positive control. The survival curve revealed that the survival rate of the CRKP group was lower than those of K. pneumoniae strain Hvkp4 at different time points. The mortality rate of G. mellonella injected with some isolates was approximately 100% during the first 24 h (Figure 3C). In contrast, the survival rate of most strains in the CSKP group was higher than that of K. pneumoniae strain Hvkp4 (Figure 3D). Taken together, we have demonstrated in this study that the CRKP strain is to some extent more virulent than the CSKP strain.
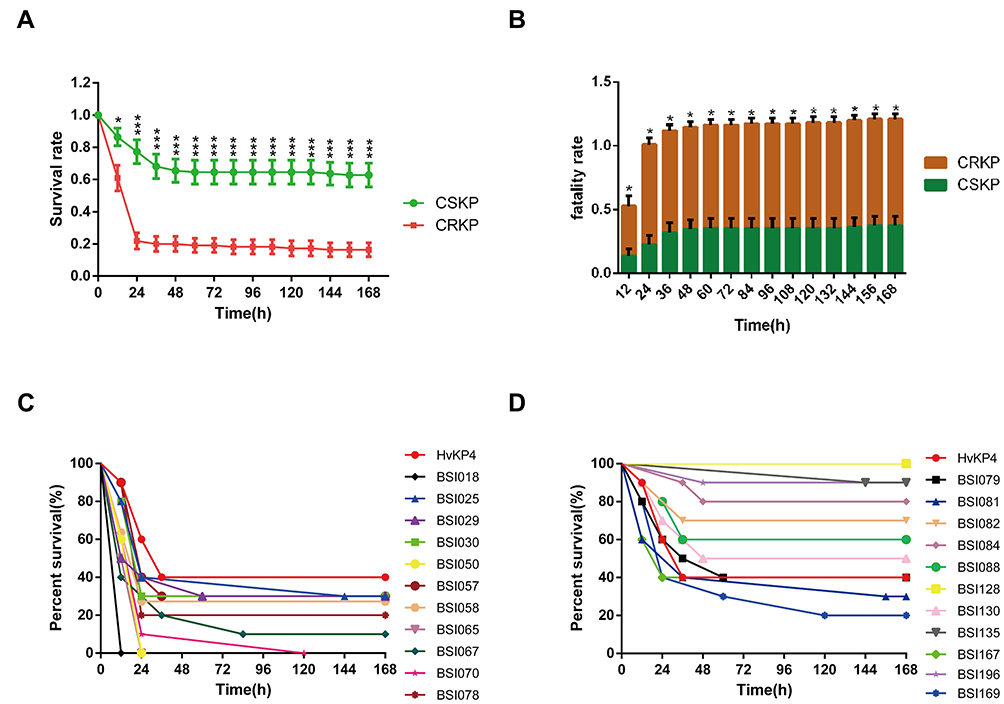 |
Figure 3 (A) Survival rates between CRKP and CSKP infections with G. mellonella infection model. (B) Fatality rates between CRKP and CSKP infections with G. mellonella infection model. (C) Kaplan–Meier survival curves of CRKP infections (11 strains) with G. mellonella infection model. (D) Kaplan–Meier survival curves of CSKP infections (11 strains) with G. mellonella infection model. Klebsiella pneumoniae strain HvKP4 as a positive control. *Means P < 0.05, ***Means P < 0.001. |
The Patients Infected by the CRKP Group Had Higher Mortality Than the CSKP Group
In-hospital deaths occurred in 22 (39.3%) of 56 CRKP BSIs and were significantly higher than those in CSKP infections (9/47 [19.1%] cases, P = 0.026, χ2 test) (Table 1). The mortality rates in the CRKP group were 17.9% at 7 days, 28.6% at 14 days, and 35.7% at 28 days, compared to 14.9% at 7 days, 19.1% at 14 days, and 19.1% at 28 days in the CSKP group (P = 0.687, 0.097, and 0.063, respectively) (Table 1).
The Kaplan–Meier curve showed the survival of the CRKP and CSKP groups after bloodstream infections (Figure 4). The 28-day cumulative survival showed a significant difference between the CRKP and the CSKP groups (P = 0.0303). The in-hospital cumulative survival showed a significant difference between the CRKP and CSKP groups (P = 0.0125). These data suggest that patients infected with CRKP have poorer outcomes than those infected with the CSKP isolates.
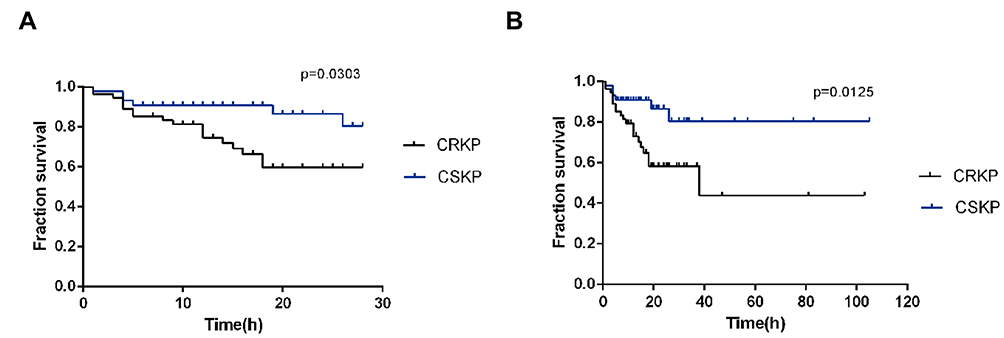 |
Figure 4 (A) Survival curve between CRKP and CSKP on Days from BSI onset. (B) Survival curve between CRKP and CSKP on Length of hospitalization after the onset of BSI. Abbreviations: KP, Klebsiella pneumoniae; CRKP, carbapenem-resistant KP; CSKP, carbapenem-susceptible KP. |
Risk Factors for Infections by CRKP and CSKP Strains
The median length of hospital stay was 28.5 days for CRKP patients compared with 28 days for CSKP patients. Most BSI patients (84/103; 81.55%) were healthcare-associated, whereas the rest (19/103; 18.45%) were community-acquired. Before BSI onset, access to healthcare was more frequent among CRKP patients than among CSKP patients. More patients with CRKP BSIs were treated with ICU admission, antibiotics, surgery within 30 days before BSI onset, immunosuppressive therapy, and previous hospitalization (Table 1). Carbapenems were the most frequently used antibiotics in subsequent therapy for both CRKP BSIs (71.4%, 40/56) and CSKP BSIs (66.0%, 31/47).
Univariate analysis showed that transfer from other hospitals, tracheal cannula or tracheotomy (within 30 days), mechanical ventilation after BSI onset, active empiric antibiotic therapy, active directed antibiotic therapy, polymyxin treatment, and tigecycline treatment were associated with CRKP BSIs (Table 1). Multivariable logistic regression analysis showed that tracheal cannula or tracheotomy (within 30 days) (OR = 0.295; 95% CI = 0.102–0.852, P = 0.024), active empiric antibiotic therapy (OR = 0.008; 95% CI = 0.001–0.118, P < 0.01), and tigecycline treatment (OR = 0.061; 95% CI = 0.004–0.855, P = 0.038) were independent risk factors for CRKP BSIs (Table 3).
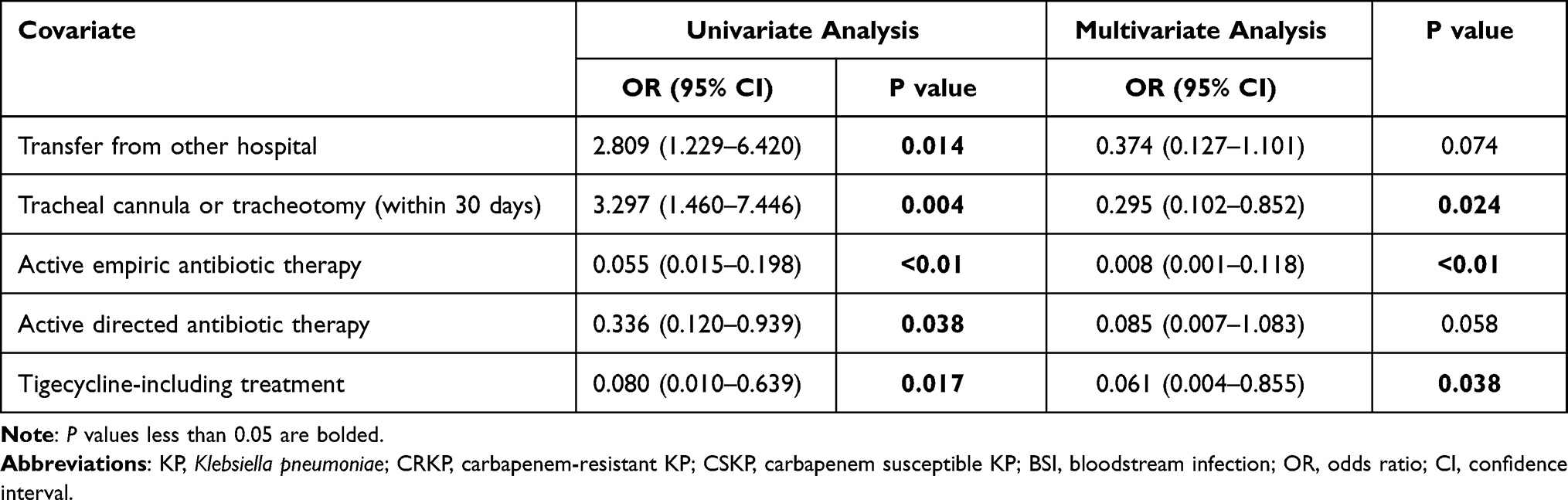 |
Table 3 Risk Factors for CRKP BSIs with Multivariate Logistic Regression Analysis |
Risk Factors of Mortality of CRKP, and CSKP BSIs
Univariate analysis of risk factors for 28-day mortality (Supplementary Material Table S1) and in-hospital mortality (Supplementary Material Table S2) among the CRKP and CSKP groups was conducted. According to the results of the univariate analysis, variables with statistical differences between the death and survival groups were included in the multivariable logistic regression model. Multivariate analysis revealed that tracheal cannula or tracheotomy (within 30 days) (P = 0.018, OR = 0.014), severe sepsis (P = 0.048, OR = 0.012), and length of hospitalization after the onset of BSI (P = 0.004, OR = 0.699) were independent risk factors for 28-day mortality of CRKP BSIs (Table 4). Multivariate analysis showed that carbapenem-resistant Enterobacterales bacteremia (P = 0.023, OR = 0.009) and length of hospitalization after the onset of BSI (P = 0.018, OR = 0.816) were independent risk factors for in-hospital mortality of CRKP BSIs (Table 4).
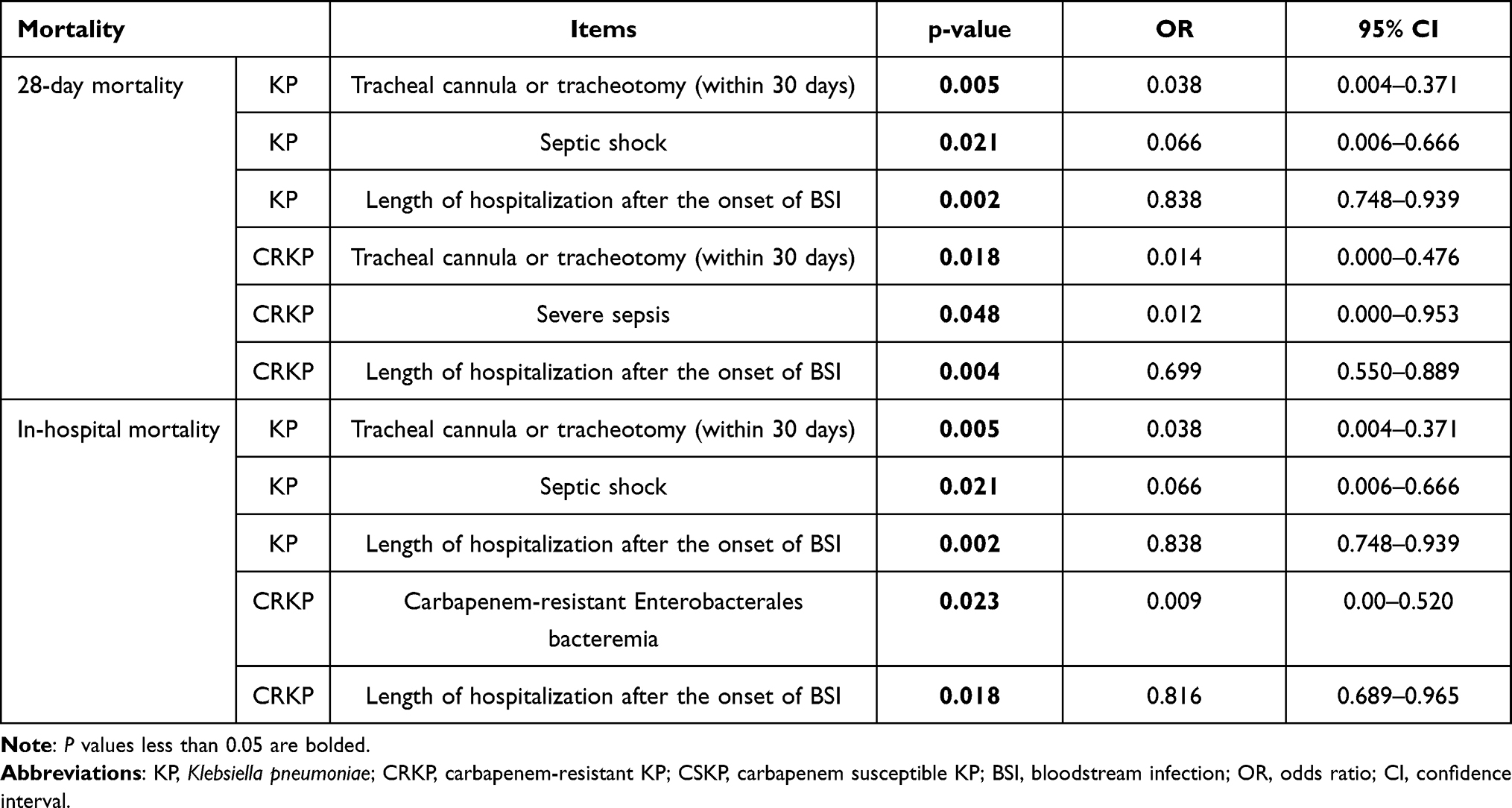 |
Table 4 Risk Factors for Mortality of KP, CRKP and CSKP BSI with Multivariate Logistic Regression Analysis |
Discussion
Carbapenems are therapeutic antimicrobials for severe bacterial infections including those caused by K. pneumoniae and the last line of treatment for many other infections following antibiotic failure.22 We conducted a retrospective study involving 103 K. pneumoniae BSI cases that occurred between 2010 and 2018 in 10 hospitals. We found that the separated CRKP showed an upward trend, not only in Guangdong but also in other parts of China.23 (http://www.carss.cn/Report/Details?aId=770). Meanwhile, we found that the resistance rate to carbapenems and other antibiotics in K. pneumoniae is increasing.24 According to the data on the drug-resistant bacteria monitoring network, the drug resistance rate of K. pneumoniae to carbapenems was 10.9% nationwide, up 0.8% compared to 2018. Our data showed that the resistance rate of the CRKP group to cephalosporins was 100%. In addition to FOS, the antibiotic resistance of the CRKP group was higher than that of the CSKP group. There were significant differences between the two groups in antibiotics, such as CTX, CAT, FEP, IPM, ETP, MEM, PTZ, AMK, GEN, and ATM. This demonstrated that the CRKP isolates harbored more severe antimicrobial resistance profiles than the CSKP isolates.
We found that the death rate was significantly higher in patients with CRKP infections than in those with CSKP infections, and some studies have shown that carbapenem resistance leads to 26–44% deaths.25 To date, the impact of carbapenem resistance on health outcomes in Chinese patients with BSI has been evaluated in only a few studies.26–28 Our study demonstrated that the in-hospital mortality of patients was significantly higher in CRKP BSIs than in CSKP BSIs. CRKP-infected patients had more frequent healthcare experiences before the onset of BSI. More patients with CRKP BSIs had been admitted to the ICU, antibiotics, surgery within 30 days before BSI onset, immunosuppressive therapy, and previous hospitalization. ICU admission within 30 days, transfer from other hospitals, tracheal cannula or tracheotomy (within 30 days), change in antibiotic treatment after positive culture, and central vein catheterization were associated with the development of CRKP BSIs. Studies have shown a 15–79% mortality rate for K. pneumoniae BSI.29–32 In this study, the in-hospital mortality rate in the CRKP group was 39.3%. The data suggest that the survival rate of the CRKP group was lower than that of K. pneumoniae strain HvKP4 in G. mellonella infection model. In addition, we found that the survival rate of the CRKP group was lower than that of the CSKP group according to the Kaplan–Meier curve after the onset of BSI. Previous studies have reported an association between carbapenem resistance and BSIs.4,26 We further clarified that carbapenem resistance is a crucial factor in the clinical treatment of CRKP BSI.
Conclusion
In conclusion, we found that the antimicrobial resistance and mortality rate of the CRKP group were higher and broader than those of the CSKP group. The survival curve showed that the outcome and prognosis of the CRKP group were worse than those of the CSKP group were. Our data provide novel information to compare antimicrobial resistance, virulence, and outcomes between CRKP and CSKP isolates.
Ethical Approval
Ethical approval for this study was given by Zhongshan School of Medicine of Sun Yat-sen University under approval number 068.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant number 82061128001, 81830103, and 81902123), Guangdong Natural Science Foundation (grant number 2017A030306012), National Key Research and Development Program (grant number 2017ZX10302301), Project of high-level health teams of Zhuhai at 2018 (The Innovation Team for Antimicrobial Resistance and Clinical Infection), 111 Project (grant number B12003), China Postdoctoral Science Foundation (grant number 2019M653192), Science, Technology & Innovation Commission of Shenzhen Municipality (grant number JCYJ20190807151601699).
Disclosure
None of the authors have any conflicts of interest related to this article.
References
1. Martin RM, Bachman MA. Colonization, infection, and the accessory genome of Klebsiella pneumoniae. Front Cell Infect Microbiol. 2018;8:4. doi:10.3389/fcimb.2018.00004
2. MacKenzie FM, Forbes KJ, Dorai-John T, Amyes SG, Gould IM. Emergence of a carbapenem-resistant Klebsiella pneumoniae. Lancet. 1997;350(9080):783. doi:10.1016/S0140-6736(05)62567-6
3. Clancy CJ, Chen L, Shields RK, et al. Epidemiology and molecular characterization of bacteremia due to carbapenem-resistant Klebsiella pneumoniae in transplant recipients. Am J Transplant. 2013;13(10):2619–2633. doi:10.1111/ajt.12424
4. Hussein K, Raz-Pasteur A, Finkelstein R, et al. Impact of carbapenem resistance on the outcome of patients’ hospital-acquired bacteraemia caused by Klebsiella pneumoniae. J Hosp Infect. 2013;83(4):307–313.
5. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16(1):18. doi:10.1186/s12941-017-0191-3
6. Zarkotou O, Pournaras S, Tselioti P, et al. Predictors of mortality in patients with bloodstream infections caused by KPC-producing Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clin Microbiol Infect. 2011;17(12):1798–1803. doi:10.1111/j.1469-0691.2011.03514.x
7. Zheng S-H, Cao S-J, Xu H, et al. Risk factors, outcomes and genotypes of carbapenem-nonsusceptible Klebsiella pneumoniae bloodstream infection: a three-year retrospective study in a large tertiary hospital in Northern China. Infect Dis. 2018;50(6):443–451. doi:10.1080/23744235.2017.1421772
8. Hu Y, Ping Y, Li L, Xu H, Yan X, Dai H. A retrospective study of risk factors for carbapenem-resistant Klebsiella pneumoniae acquisition among ICU patients. J Infect Dev Ctries. 2016;10(3):208–213. doi:10.3855/jidc.6697
9. Wu D, Cai J, Liu J. Risk factors for the acquisition of nosocomial infection with carbapenem-resistant Klebsiella pneumoniae. South Med J. 2011;104(2):106–110. doi:10.1097/SMJ.0b013e318206063d
10. Huang W, Qiao F, Zhang Y, et al. In-hospital medical costs of infections caused by carbapenem-resistant Klebsiella pneumoniae. Clin Infect Dis. 2018;67(suppl_2):S225–S230. doi:10.1093/cid/ciy642
11. Zhang Z, Sun Z, Tian L. Antimicrobial resistance among pathogens causing bloodstream infections: a multicenter surveillance report over 20 years (1998–2017). Infect Drug Resist. 2022;15:249–260. doi:10.2147/IDR.S344875
12. Lou T, Du X, Zhang P, et al. Risk factors for infection and mortality caused by carbapenem-resistant Klebsiella pneumoniae: a large multicentre case-control and cohort study. J Infect. 2022;84:637–647. doi:10.1016/j.jinf.2022.03.010
13. Cao Z, Yue C, Kong Q, et al. Risk factors for a hospital-acquired carbapenem-resistant bloodstream infection: a five-year retrospective study. Infect Drug Resist. 2022;15:641–654. doi:10.2147/IDR.S342103
14. Pan H, Lou Y, Zeng L, et al. Infections caused by carbapenemase-producing Klebsiella pneumoniae: microbiological characteristics and risk factors. Microb Drug Resist. 2019;25(2):287–296. doi:10.1089/mdr.2018.0339
15. Giacobbe DR, Del Bono V, Trecarichi EM, et al. Risk factors for bloodstream infections due to colistin-resistant KPC-producing Klebsiella pneumoniae: results from a multicenter case-control-control study. Clin Microbiol Infect. 2015;21(12):
16. Ben-David D, Kordevani R, Keller N, et al. Outcome of carbapenem resistant Klebsiella pneumoniae bloodstream infections. Clin Microbiol Infect. 2012;18(1):54–60. doi:10.1111/j.1469-0691.2011.03478.x
17. Callahan BJ, Wong J, Heiner C, et al. High-throughput amplicon sequencing of the full-length 16S rRNA gene with single-nucleotide resolution. Nucleic Acids Res. 2019;47(18):e103. doi:10.1093/nar/gkz569
18. CLSI. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
19. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
20. McLaughlin MM, Advincula MR, Malczynski M, Barajas G, Qi C, Scheetz MH. Quantifying the clinical virulence of Klebsiella pneumoniae producing carbapenemase Klebsiella pneumoniae with a Galleria mellonella model and a pilot study to translate to patient outcomes. BMC Infect Dis. 2014;14:31. doi:10.1186/1471-2334-14-31
21. Gu D, Dong N, Zheng Z, et al. A fatal outbreak of ST11 carbapenem-resistant hypervirulent Klebsiella pneumoniae in a Chinese hospital: a molecular epidemiological study. Lancet Infect Dis. 2018;18(1):37–46. doi:10.1016/S1473-3099(17)30489-9
22. Livermore DM. The impact of carbapenemases on antimicrobial development and therapy. Curr Opin Investig Drugs. 2002;3(2):218–224.
23. Hu Y, Liu C, Shen Z, et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant in patients from Zhejiang, China, 2008–2018. Emerg Microbes Infect. 2020;9(1):1771–1779. doi:10.1080/22221751.2020.1799721
24. Nordmann P, Cuzon G, Naas T. The real threat of Klebsiella pneumoniae carbapenemase-producing bacteria. Lancet Infect Dis. 2009;9(4):228–236. doi:10.1016/S1473-3099(09)70054-4
25. Falagas ME, Tansarli GS, Karageorgopoulos DE, Vardakas KZ. Deaths attributable to carbapenem-resistant Enterobacteriaceae infections. Emerg Infect Dis. 2014;20(7):1170–1175. doi:10.3201/eid2007.121004
26. Zheng X, Wang J-F, Xu W-L, Xu J, Hu J. Clinical and molecular characteristics, risk factors and outcomes of Carbapenem-resistant bloodstream infections in the intensive care unit. Antimicrob Resist Infect Control. 2017;6:102. doi:10.1186/s13756-017-0256-2
27. Zhang Y, Guo LY, Song WQ, Wang Y, Dong F, Liu G. Risk factors for carbapenem-resistant K. pneumoniae bloodstream infection and predictors of mortality in Chinese paediatric patients. BMC Infect Dis. 2018;18:248. doi:10.1186/s12879-018-3160-3
28. Tian L, Tan R, Chen Y, et al. Epidemiology of Klebsiella pneumoniae bloodstream infections in a teaching hospital: factors related to the carbapenem resistance and patient mortality. Antimicrob Resist Infect Control. 2016;5:48. doi:10.1186/s13756-016-0145-0
29. Liu YM, Li BB, Zhang YY, et al. Clinical and molecular characteristics of emerging hypervirulent Klebsiella pneumoniae bloodstream infections in mainland China. Antimicrob Agents Chemother. 2014;58(9):5379–5385. doi:10.1128/AAC.02523-14
30. Falcone M, Russo A, Iacovelli A, et al. Predictors of outcome in ICU patients with septic shock caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin Microbiol Infect. 2016;22(5):444–450. doi:10.1016/j.cmi.2016.01.016
31. Liu Q, Li W, Du X, et al. Risk and prognostic factors for multidrug-resistant Acinetobacter baumannii complex bacteremia: a retrospective study in a tertiary hospital of West China. PLoS One. 2015;10(6):e0130701. doi:10.1371/journal.pone.0130701
32. da Silva KE, Maciel WG, Sacchi FPC, et al. Risk factors for KPC-producing Klebsiella pneumoniae: watch out for surgery. J Med Microbiol. 2016;65(6):547–553. doi:10.1099/jmm.0.000254
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.