Back to Journals » Infection and Drug Resistance » Volume 16
Outcomes and Predictors of Severe Community-acquired Pneumonia Among Adults Admitted to the University of Gondar Comprehensive Specialized Hospital: A Prospective Follow-up Study
Authors Kassaw G ![]() , Mohammed R, Tessema GM, Yesuf T, Lakew AM
, Mohammed R, Tessema GM, Yesuf T, Lakew AM ![]() , Tarekegn GE
, Tarekegn GE ![]()
Received 15 October 2022
Accepted for publication 16 January 2023
Published 28 January 2023 Volume 2023:16 Pages 619—635
DOI https://doi.org/10.2147/IDR.S392844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Getasew Kassaw,1 Rezika Mohammed,1 Getahun Mengistu Tessema,1 Tesfaye Yesuf,1 Ayenew Molla Lakew,2 Gebrekidan Ewnetu Tarekegn2
1Department of Internal Medicine, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia; 2Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Gebrekidan Ewnetu Tarekegn, Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P.O. Box. 196, Gondar, Ethiopia, Tel +251 930781289, Email [email protected]
Background: Severe community-acquired pneumonia is a common life-threatening infection with a high rate of unfavorable outcome. This study aimed to assess the outcomes and predictors of hospitalized severe community-acquired pneumonia patients at University of Gondar comprehensive specialized hospital.
Methods: A prospective follow-up study was conducted at University of Gondar comprehensive specialized hospital from May 1 to September 31, 2021. The data was collected by reviewing patients’ charts and interviewing the patients themselves. Descriptive statistics, binary and multivariable logistic regression analysis were performed accordingly. Variables with p-value < 0.2 on binary logistic regression were analyzed using multivariable logistic regression and variables with p< 0.05 were considered to have significant association.
Results: A total of 239 admitted patients with severe community-acquired pneumonia were enrolled in the study. An unfavorable outcome was observed in 105 (44%) patients; 24.27% was in-hospital all-cause mortality, 12.5% was nonresolution, 5.8% was complicated cases, and 1.26% were gone against medical care for poor prognosis. After analyzing multivariable logistic regression, confusion (OR= 4.84; 95%CI: 1.47– 15.88), anemia (OR= 2.36; 95%CI: 1.01– 5.52), leukopenia (OR=4.38; 95%CI: 1.26– 15.25), leukocytosis (OR=3.15; 95%CI: 1.23– 7.96), elevated creatinine (OR=5.67; 95%CI: 1.72– 18.65), intubation (OR=7.27; 95%CI: 1.58– 33.37) and antibiotic revision during treatment for a different reason (OR=0.02; 95%CI: 0.01– 0.07) were variables significantly associated with unfavorable outcome.
Conclusion: Unfavorable outcome was high among hospitalized severe community acquired pneumonia patients, and confusion, elevated creatinine, anemia, leukopenia, leukocytosis, intubation during admission, and antibiotic revision during the course were independent predictors associated significantly with the unfavorable outcome. It is important to consider the development of a treatment protocol for the hospital and to further research incorporating the microbiologic profile of the patients.
Keywords: pneumonia, unfavorable outcome, community-acquired pneumonia, Ethiopia
Background
Pneumonia is one of the life-threatening infections of the lung parenchyma characterized by acute onset of symptoms like cough, pleuritic chest pain, fever, sputum production, and shortness of breath alone or in combination with variable degree of physical (crepitation, bronchial breath sound, effusion sign., etc), and radiologic findings (consolidation, infiltrations, effusion, etc).1
Pneumonia can be classified in different ways: based on the origin of the site of patient, exposure to the infecting agent, it can be classified as community acquired or hospital acquired. The second way of classification is by using etiology and can be categorized as bacterial, viral, fungal, or parasitic. Using the anatomy of the affected lung parts, it is possible to classify as lobar, interstitial, or bronchial. Taking clinical presentation in to account, it can be also categorized as typical or atypical, mild (walking pneumonia), or severe. Community-acquired pneumonia (CAP) is a pneumonia with a source of infection in the community.2–6
Community-acquired pneumonia severity ranges from mildly ambulating to severe necrotizing pneumonia with septic shock or requiring mechanical ventilation. The degree of severity affects the patients’ outcome in the short- and long-term.7 There are many different well-defined predictor scores developed so far, including Infectious Disease Society Association/American Thoracic Society (IDSA/ATS) severity score, confusion, urea, respiratory rate, blood pressure and age >65 (CURB-65), pneumonia severity index (PSI) scores, etc, and these are helpful for proper management of a patient.2,8
Community-acquired pneumonia is widespread infectious disease of the lung parenchyma caused by various etiologies like bacteria, viruses, fungi, and parasitic agents affecting the world population but proportionally it is rampant among low- and middle-income countries, mainly sub-Saharan Africa countries including Ethiopia.9–11
In Africa, SCAP is related to in-hospital mortality of 6–15% from hospital-based reports11–13 of which more than four million pneumonia episodes and more than 200,000 deaths occur in sub-Saharan Africa. Secondary data analyzed in the US from 2014 to 2016 among 7449 patients admitted with a diagnosis of community-acquired pneumonia showed 77% of the patients improvement and nonresolving pneumonia was documented in 3% at the end of one week of therapy and 30-day mortality was 6%.14
The 2019 IDSA/ATS severity criteria define severe CAP by the presence of one of the two major criteria (septic shock requiring vasopressor support and requirement for mechanical ventilation) or presence of ≥3 minor criteria (respiratory rate ≥30 breaths/min, arterial oxygen tension / fractional inspired oxygen ratio (PaO2/FiO2) ≤250.
Studies done globally showed that many sociodemographic, clinical related, laboratory related variables were significantly associated with unfavorable outcomes for SCAP. Among those variables age, sex, residence, educational level, occupation, marital status, smoking status, alcoholism, diabetics, HIV, cardiac diseases, nutritional status, elevated creatinine, chronic liver disease, stroke, residual physical disability, CURB65, pregnancy, tachypnea, blood pressure, tachycardia, temperature, and other variables were significantly associated with the unfavorable treatment outcomes of SCAP patients.2,8,15–23
The hypothesis of this study was that there are different predicting factors to the unfavorable outcome of SCAP as it is still costing the lives of many despite advances are made in diagnostics and treatment in modern medicine and this problem is cumbersome in developing countries including Ethiopia.
The implementation of safe, effective, and affordable interventions toward these predictors may reduce the unfavorable outcomes of SCAP in the risky populations.24 Therefore, knowing predictors of unfavorable outcome in SCAP has paramount benefit from individual patient level to country level in many aspects. In terms of patient care, it will guide physicians to have targeted evaluation and timely interventions.
However, little is known about the outcomes and associated factors of severe community-acquired pneumonia among adults in a developing country, specifically in Ethiopia. Therefore, this study aims to assess outcomes and predictors of severe community acquired pneumonia among adults admitted to the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2021.
Methods and Materials
Study Design, Setting, and Period
A hospital-based prospective follow-up study was conducted in the University of Gondar comprehensive specialized Hospital (UoGCSH) from May 1, 2021 to September 31, 2021. It is located at the middle of Gondar city in the northwestern part of the country. It is also one of the largest referral hospitals with easy access to about more than five million people and one of the oldest academic institutions in Ethiopia. Internal medicine department provides services for both rural and urban populations and includes outpatient clinics, emergency service wards, and adult medical intensive care unit (ICU). The department has 25–30 senior internists, more than 55 residents, more than 15 general practitioner (GPs) and other health-care providers.
Population
All adults admitted with the diagnosis of severe community acquired pneumonia in University of Gondar comprehensive specialized hospital during the study period were included in this study. Patients who have risk of hospital-acquired pneumonia, aspiration pneumonia, and significant immunosuppression making them at risk of opportunistic infections were excluded from the study.
Sample Size and Sampling Procedure
Sample Size Determination and Sampling Procedure
The required sample size to conduct the study was estimated by a single population proportion formula. By considering 95% confidence level, 5% margin of error (d), and by taking 18% proportion (P) of unfavorable outcome of SCAP from previous study.22 By assuming the above assumptions, the required sample size (n) was calculated using the formula  . By adding a 5% of nonresponse rate, the final sample size was 239.
. By adding a 5% of nonresponse rate, the final sample size was 239.
The required sample was taken by enumerating all patients during the study period (from May 1, 2021 to September 31, 2021) consecutively until the required sample size was secured.
Data Collection Methods and Instruments
The data sources for the study were patients’ medical records, care givers or guardians and physicians. A structured and pretested questionnaire was used to collect the raw data. Trained interns, GPs and residents collected the data after training was provided on the objectives of the study and how to collect the data. Data collection involved both patient interview and chart review. Focused history was asked addressing sociodemographic characteristics, duration of symptoms, previous pneumonia diagnosis, and antibiotics used and for the presence of smoking, alcohol drinking, and other substance abuse. Focused physical examination (day one, findings of mental status, mid-upper arm circumference, and vital signs) was documented on the chart or performed. Laboratory findings of complete blood count, renal function test, serum electrolyte, and COVID-19 test, PICT, and chest radiography results were documented. Type of treatment and any antibiotic revision during treatment were also recorded.
Study Variables
The outcome variable of the study was the outcomes of SCAP. It was defined as favorable outcome or unfavorable outcome. Favorable outcome was defined as a patient who improved and discharged ultimately, and unfavorable outcome was defined as all-in-hospital death, complications, nonresolutions, and went against medical care. And the possible independent variables for this study were sociodemographic variables like (age, sex, residency, religion, education level, marital status, cigarette smoking), comorbidity, and clinical related variables.
Operational Definition of Some Variables
Desaturation – oxygen saturation <90% and tachypnea defined as >16 breaths/min; malnourished – MUAC<23 cm; bradycardia and tachycardia defined heart rate <60 and >90 bpm, respectively; hypertension defined as systolic BP ≥130 mmHg and/or diastolic BP ≥90 mmHg; hypotension defined as systolic BP ≥90 mmHg and/or diastolic BP <60 mmHg; fever and hypothermia defied as axillary temperature measurement of >37.2 and <35.5°C respectively; leukocytosis and leukopenia defined as ≥11,000 and <4000/µL, respectively; lymphocytosis and lymphopenia defined as >40% and <20%, respectively; thrombocytosis and thrombocytopenia defied >450,000 and <150,000/µL respectively; hypernatremia >145 and hyponatremia <135 mEq/L, hyperkalemia >5.5 mEq/L and hypokalemia <3.5 mEq/L.25–27
Data Quality Management
The questionnaire was evaluated with the pretesting tool, training was given for data collectors, checking the completeness of filled questionnaires, daily supervision, and checkup was done as planned, and finally, double data entry was performed.
Data Processing and Analysis
Each completed data was checked for consistency before data entry. Then the data were coded and entered in to a computer by using EpiData version 4.6 and further clean-ups were made to check the accuracy and consistency. Then the data was exported to STATA version 16 for detail analysis. Bivariable analysis was carried out first to observe the crude association between independent and dependent variable. Multivariable logistic regression model was analyzed to identify covariates significantly associated with the outcome variables. All statistical inference were made at 5% level of significance. Both statistical and clinical significance of the variable were assessed. The independent variables with p-value <0.05 were considered statistically associated with the unfavorable outcomes of the patients. The model goodness of fitness was checked using Hosmer–Lemeshow. This result supports the model were well fitted to the data (p-value >0.05).
Ethical Considerations
After getting permission from the Internal medicine department, the study proposal was submitted to the Institutional Review Board (IRB) of the College of Medicine, University of Gondar. The study was done after approval was obtained from the board and hospital administration written informed consent was presented to the participants before the study was conducted.
Results
Sociodemographic and Behavioral Characteristics
A total of 239 patients hospitalized with SCAP were involved in the study, 129 (53.97%) were females. The median age was 52 years. The majority 167 (69.87%) were from urban areas, 119 (49.79%) had no formal education (Table 1).
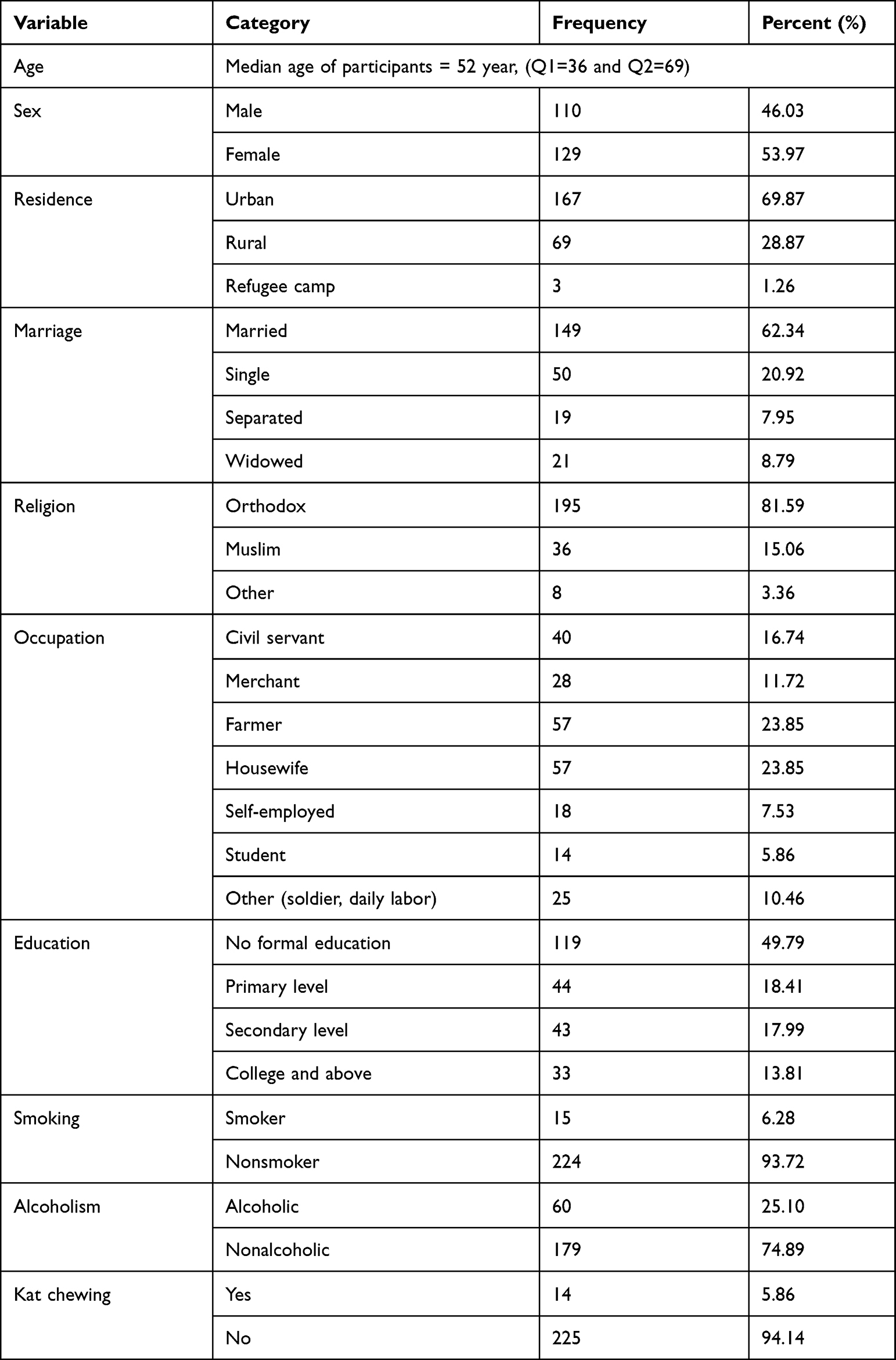 |
Table 1 Sociodemographic and Behavioral Characteristics of Patients Admitted to SCAP, UoGCSH, 2021 (n=239) |
Comorbidities
Among all enrolled participants, 66% had one or more comorbidities. Diabetes, hypertension, cardiac disease, and malnutrition were the most commonly identified (Table 2).
 |
Table 2 Comorbidities of Patients Hospitalized for SCAP at UoGCSH from May to September 2021 (n=239) |
Clinical Related Factors
Among the 239 participants, 50 (20.92%) and 59 (24.69%) patients had pneumonia diagnosis and antibiotic exposure in the past three months, respectively. The median duration of symptoms was 6 days with the shortest and longest duration being 1 and 60 days, respectively.
Complete blood count, renal function test, and chest X-ray was done for all patients. Serum electrolyte (sodium and potassium) was done for 187 and 185 patients, respectively. COVID-19 test was done for 105 (43.93%) patients but only 42 (17.57%) were positive. Leukocytosis, leukopenia, anemia, thrombocytopenia were seen in 78 (32.99%), 43 (17.99%), 70 (29.29%), and 79 (33.05%) respectively. Among all, 33 (13.81%) and 182 (76.15%) patients had elevated creatinine and urea levels in order. Hypokalemia and hyponatremia were seen among 69 (37.3%) and 72 (38.5%) patients, respectively. On chest X-ray, 83 (34.73%) had pneumonia 76 (31.80%) had pneumonia with one or more of the following: effusion, obstructive airway disease, fibrosis and cardiomegaly; 64 (26.80) had multifocal or multilobe pneumonia and 16 (6.69%) had different reports including normal, obstructive airway disease, fibrosis or effusion alone. CURB65 score was done for all participants and 154 (64.44%) patients had ≤2 and 85 (35.56%) patients had ≥3 values. Regarding the antibiotic treatment, patients were given ceftriaxone combined with either vancomycin, azithromycin, or doxycycline for 102 (42.68%) patients, 71 (29.7%) patients and 31 (12.97%) patients, respectively and antibiotic revision was made in 55 (23%) of the cases during treatment (Table 3).
 |
Table 3 Clinical Features of Patients Hospitalized for SCAP at UoGCSH from May to September 2021 (n=239) |
Outcomes of Severe Community Acquired Pneumonia
Composite unfavorable outcomes of patients hospitalized with SCAP in this study were 105 (44%; 95%CI: 37.59–50.27) (Figure 1).
 |
Figure 1 Outcomes of hospitalized patients with SCAP at UoGCSH from May to September 2021 (n=239). |
Unfavorable Outcomes by Sociodemographic and Behavioral Characteristics of the Patients
The proportion of patient’s age above 65 years with unfavorable outcome were 35 (14.6%). Males had 22.6% and females had 21.6% unfavorable outcome. Among all, 76 (31.8%), 59 (24.7%), and 56 (23.4%) patients with unfavorable outcome were from urban areas, were unemployed and had no formal education, respectively (Table 4).
 |
Table 4 Sociodemographic and Behavioral Characteristics as a Predictor of Unfavorable Outcome Among Hospitalized SCAP Patients at UoGCSH, May to September 2021 (n=239) |
Unfavorable Outcome by Comorbidity
The proportion of patients having DM comorbidity with unfavorable outcome was 19 (7.95%), patients having hypertension comorbidity had 10.46% and HIV comorbidity had 10.58% unfavorable outcome (Table 5).
 |
Table 5 Comorbidities as Predictor of Unfavorable Outcome Among Hospitalized SCAP Patients at UoGCSH, May to September 2021 (n=239) |
History and Physical Examination Findings as Predictors
Unfavorable outcome was identified in 24 (10%) of patients who reported pneumonia diagnosis and 30 (12.6%) of patients who used antibiotics in the past three months. Similarly, unfavorable outcome was also identified in 40 (16.7%), 47 (19.7%), 18 (7.5%), 20 (8.4%), 75 (31.4%), 95 (39.7%) patients who altered mental status, fever, hypothermia, oxygen saturation less than 70%, respiratory rate greater than 30 and tachycardic patients respectively. Among all participants, 11 (4.6%) and 12 (5%) patients with diastolic and systolic hypotension also had an unfavorable outcome (Table 6).
 |
Table 6 History and Physical Exam Findings Related to Unfavorable Outcome Among Hospitalized SCAP Patients at UoGCSH, May to September 2021 (n=239) |
Laboratory Findings of the Patients
Unfavorable outcome was observed in 59 (24.68%) anemic, 43 (17.99%) thrombocytopenic, and 24 (10.04%) leukopenic patients, respectively. Unfavorable outcome was seen in 9 (3.77%) patients with elevated creatinine. Patients with elevated urea had a favorable outcome in 95 (39.75%) of cases. Similarly, 40 (21.39%), 34 (18.34%), and 67 (28.03%) with hyponatremia, hypokalemia, and COVID-19 positivity in the listed order had unfavorable outcomes (Table 7).
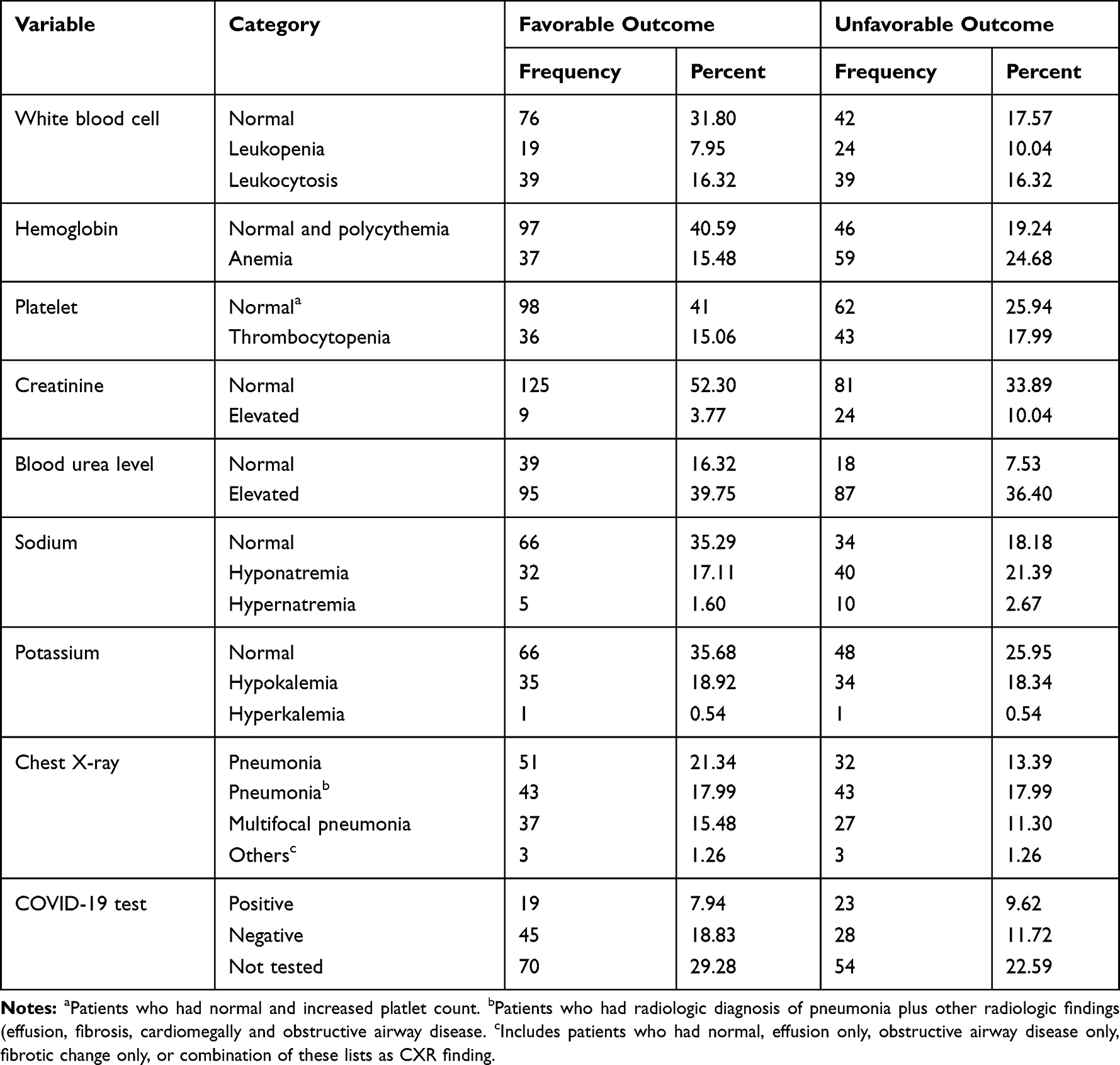 |
Table 7 Investigation Findings as Predictors of Unfavorable Outcome Among Hospitalized SCAP Patients at UoGCSH, May to September 2021 (n=239) |
Patient Management Related Characteristics of the Patients
Among patients with CURB-65 score of ≥3, 53 (22.18%) had unfavorable outcomes. Similarly, unfavorable outcomes occurred in 48 (20%) of patients after antibiotic revision. A total of 29 (12.13%) patients were intubated during admission and an unfavorable outcome was noted in 20 (8.37%) of them. Antibiotic revision was made for 55 patients of which 48 (20%) were having an unfavorable outcome. A total of 27 patients were treated with vasopressors for septic shock during admission of which 20 (74%) had an unfavorable outcome (Table 8).
 |
Table 8 Treatment Related Characteristics of Unfavorable Outcome Among Hospitalized SCAP Patients at UoGCSH, May to September 2021 (n=239) |
Predictors of Unfavorable Outcome in Hospitalized Patients with SCAP
Among variables patient’s occupation, asthma, respiratory rate, oxygen saturation, level of consciousness, CURB65, hemoglobin, platelet count, white blood cell count, creatinine, urea, antibiotic revision and intubation status were having an association with the unfavorable outcome. After analyzing multivariable binary logistic regression, the level of consciousness, hemoglobin, white blood cells, creatinine, intubation status, and antibiotic revision were significantly associated with the occurrence of unfavorable outcomes.
The odds of unfavorable outcome were five, two, four, three, six, and seven times higher among patients who had confusion, anemia, leukopenia, leukocytosis, elevated creatinine, and those who required intubation compared to conscious, normal hemoglobin, WBC, creatinine and those who were not intubated, respectively. The odds value of unfavorable outcome was reduced by 98% antibiotics revision compared to those for who no antibiotic revision was made (Table 9).
 |
Table 9 Bivariable and Multivariable Logistic Regression Analysis of SCAP Patients Hospitalized at UoGCSH, 2021 (n=239). |
Discussion
The present study showed increased rates of unfavorable patient outcomes following admission due to SCAP with over all composite unfavorable outcome of 44% of which all-cause-in-hospital mortality accounted for 24.27%, nonresolution cases were 12.55% and complication in the course of treatment was 5.86%.
The result of in-hospital mortality from this study was higher than the findings from the studies conducted in USA, Spain, Netherlands.14,20,28 This difference was most likely ascribed to the level of better care provided in these high-income countries with better health-care infrastructure which includes early case detection, early treatment initiation, advanced supportive treatment options; early care-seeking behavior by patients may also contribute. This finding, however, was consistent with studies done in Spain, Portuguese, and Egypt.29–31 The finding in this study was higher than from the finding from the study conducted previously in Ethiopia22 and the possible explanation is that this study included critical patients admitted to ICU admissions in addition to ward admitted patients, who have better outcome comparatively.
For a similar explanation mentioned above, this study showed increased rates of nonresolution cases compared to the study done in the USA14 which was consistent with findings from the study done in China from secondary data.20
The complications in the course of treatment in this study were fewer than in the study done in Ethiopia previously;22 the likely reason is that the patients in this study included critical cases requiring ICU admission who are at risk of higher in-hospital mortality once they develop the complications compared to patients who were not critically sick, admitted in the ward from the previous study.
In this study, presence of unfavorable outcome was significantly associated with the presence of confusion during admission. Patients with confusion were having the unfavorable outcome five times more than conscious patients during admission. This result is consistent with the finding of the study done in Barcelona, Spain.15 This might be explained by patients who had confusion at admission being likely to have severe hypoxia, hypo perfusion, acidosis, inflammation, and other end organ damage with metabolic complications that results in altered level of mental status.
The presence of anemia at admission had significantly increased the occurrence of unfavorable outcomes. Patients who had anemia, hemoglobin level <12 mg/dL for both sexes during admission were 2.36 times more at risk of having unfavorable outcomes compared to those with normal and above hemoglobin levels. This finding was consistent with studies done in the US, Switzerland, Pakistan, and Singapore.16,19,28,32 The presence of anemia compromise the already sick patient who is hypoxic, hypo perfused, and severely inflamed.
The presence of leukocytosis at admission had a significant association with unfavorable outcomes. Patients who had leukocytosis >11,000 during admission were 3.15 times more at risk of having unfavorable outcomes compared to those with normal white blood cells. This finding was in agreement with studies done in China and Singapore.20,32,33 Leukocytosis is the body’s immune response, predominantly the polymorph nuclear type, as a means to control the infection. However, the presence of an extremely high white cells may tell the underlying leukemia or leukemoid reaction.
The presence of leukopenia at admission had a significant association with unfavorable outcomes. Patients who had leukocytosis <4000 during admission were 4.38 times more at risk of having unfavorable outcomes as compared to those with normal white blood cells. This finding was in line with the finding in the study done in Singapore.32 The presence of leukopenia tells the presence of intense inflammation suppressing leukocyte production in the bone marrow or increasing their destruction. It may also occur with the effect of the underlying comorbidity or cause of pneumonia, like some viruses can cause leukopenia.
Patients with SCAP who had elevated creatinine >1.3 mg/dL during admission had an increased risk of unfavorable outcome 5.3 times compared to SCAP patients who had a serum creatinine level <1.3 mg/dL. Different studies done in Ethiopia and Spain22,31 showed consistent evidence. This might explain the presence of bacteremia (sepsis).
In this study, the presence of unfavorable outcomes was significantly associated with invasive mechanical ventilation. Patients who were managed invasively with mechanical ventilation were 7.27 times at risk of having the unfavorable outcome compared to those who were not intubated. This result was in agreement with the prospective observational study done in Barcelona and other studies also show similar evidence.15,30,34 This may be due to the complication of mechanical ventilation including barotrauma, pneumothorax, ventilator-associated pneumonia, etc. Conversely, patients who are treated with invasive mechanical ventilation likely do have severe infection and end organ damage.
The odds of unfavorable outcome were reduced by 98% in those for whom antibiotic revision was made compared to those for whom change was not done. This finding suggests that initial empiric antibiotic choice may be discordant. The result is consistent with the study done in Portuguese, Ethiopia, Spain, and China.15,20,22,30 Subsequent escalation or de-escalation of antibiotics may require covering different etiologies and resistant organisms, if possible, guided by culture.
Strength and Limitations of the Study
This study was conducted using a prospective study design, which clarifies the temporal sequence of the outcome. This outcome is possible because researchers can observe definitive behaviors or characteristics. However, this study had limitations, including the lack of a microbiologic profile of the patients due to resource constraints, the failure to address specific causes of death and complications, and the fact that some variables, such as CXR reading, were inconsistent due to varying levels of training.
Conclusion
Hospitalized patients with SCAP had high in-hospital mortality and clinical nonresolution cases. Confusion, high creatinine, anemia, leukopenia, leukocytosis, intubation during admission and antibiotic revision during the course were independent predictors that were significantly associated with the unfavorable outcome. It is better the clinicians prepare SCAP treatment protocol considering the unfavorable outcome.
Abbreviations
AIDS, acquired immunodeficiency syndrome; AOR, adjusted odds ratio; ATS, American Thoracic Society; ART, anti-retroviral therapy; CAP, community-acquired pneumonia; CBC, complete blood count; CI, confidence interval; CURB 65, confusion, urea, respiratory rate, blood pressure and age >65; COPD, chronic obstructive pulmonary disease; CLD, chronic liver disease; CKD, chronic kidney disease; ED, emergency department; EMCC, emergency medicine and critical care; FIO2, fraction of inspired oxygen; GCS, Glasgow coma scale; GP, general practitioner; UOGCSH, University of Gondar Comprehensive Specialized Hospital; HIV, human immunodeficiency virus; ICU, intensive care unit; IDSA, Infectious Disease Society Association; ILD, interstitial lung disease; IQR, interquartile range; MUAC, mid-upper arm circumference; p, probability-value; PCCM, pulmonologist and critical care management; PSI, pneumonia severity index; PaO2, partial arterial oxygen; RCT, randomized control trial; US, United States; WBC, white blood count.
Data Sharing Statement
The datasets supporting the conclusions of this article are available upon request to the primary/corresponding author.
Acknowledgments
The authors would like to acknowledge University of Gondar college of Medicine and Health Science, School of Medicine for giving us the opportunity to conduct this study. Our acknowledgment would also extend to health professionals who work at the Department of Internal Medicine for their cooperativeness in the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
All authors declare that they have no conflicts of interest in relation to this work.
References
1. Somberg J. Harrisons Princiole of Internal Medicine.
2. Ramirez JA. Overview of community-acquired pneumonia in adults; 2019.
3. Ewig S, Welte T, Chastre J, Torres A. Rethinking the concepts of community-acquired and health-care-associated pneumonia. Lancet Infect Dis. 2010;10(4):279–287. doi:10.1016/S1473-3099(10)70032-3
4. Bohte R, van Furth R, van den Broek PJ. Aetiology of community-acquired pneumonia: a prospective study among adults requiring admission to hospital. Thorax. 1995;50(5):543–547. doi:10.1136/thx.50.5.543
5. Lanks CW, Musani AI, Hsia DW. Community-acquired pneumonia and hospital-acquired pneumonia. Med Clin. 2019;103(3):487–501. doi:10.1016/j.mcna.2018.12.008
6. Shoar S, Musher DM. Etiology of community-acquired pneumonia in adults: a systematic review. Pneumonia. 2020;12(1):1–10. doi:10.1186/s41479-020-00074-3
7. Ewig S, Schafer H, Torres A. Severity assessment in community-acquired pneumonia. Eur Respir J. 2000;16(6):1193–1201. doi:10.1034/j.1399-3003.2000.16f27.x
8. Li HY, Guo Q, Song WD, et al. Modified IDSA/ATS minor criteria for severe community-acquired pneumonia best predicted mortality. Medicine. 2015;94:36.
9. Ferreira-Coimbra J, Sarda C, Rello J. Burden of community-acquired pneumonia and unmet clinical needs. Adv Ther. 2020;2020:1–17.
10. Heo JY, Seo YB, Jeong HW, et al. Epidemiology of community-acquired pneumonia in the era of extended serotype-covering multivalent pneumococcal conjugate vaccines. Vaccine. 2020;38(49):7747–7755. doi:10.1016/j.vaccine.2020.10.046
11. Aston R, Rylance J. Community-acquired pneumonia in sub-Saharan Africa.
12. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
13. Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2197–2223. doi:10.1016/S0140-6736(12)61689-4
14. Peyrani P, Arnold FW, Bordon J, et al. Incidence and mortality of adults hospitalized with community-acquired pneumonia according to clinical course. Chest. 2020;157(1):34–41. doi:10.1016/j.chest.2019.09.022
15. Garcia-Vidal C, Fernández-Sabé N, Carratalà J, et al. Early mortality in patients with community-acquired pneumonia: causes and risk factors. Eur Respir J. 2008;32(3):733–739. doi:10.1183/09031936.00128107
16. Elsener C, Beeler PE, Battegay E, Bello B, Thienemann F. Risk factors of in-hospital mortality in patients treated for pneumonia at a tertiary care centre in Switzerland. Respiration. 2020;99(8):637–645. doi:10.1159/000508666
17. Thomsen RW, Kasatpibal N, Riis A, Nørgaard M, Sørensen HT. The impact of pre-existing heart failure on pneumonia prognosis: population-based cohort study. J Gen Intern Med. 2008;23(9):1407–1413. doi:10.1007/s11606-008-0672-3
18. Rumbus Z, Matics R, Hegyi P, et al. Fever is associated with reduced, hypothermia with increased mortality in septic patients: a meta-analysis of clinical trials. PLoS One. 2017;12(1):e0170152. doi:10.1371/journal.pone.0170152
19. Iqbal N, Irfan M, Siddique F, Arshad V, Zubairi ABS. Factors predicting in‐hospital mortality among patients admitted with community acquired pneumonia at a tertiary care hospital Karachi, Pakistan. Clin Respir J. 2020;14(4):328–334. doi:10.1111/crj.13137
20. Han X, Liu X, Chen L, et al. Disease burden and prognostic factors for clinical failure in elderly community acquired pneumonia patients. BMC Infect Dis. 2020;20(1):1–9. doi:10.1186/s12879-020-05362-3
21. Khalil R, Sinno L, HJJoR R, Disorders H. Outcome of hospitalized pneumonia patients with and without COVID-19: a retrospective cohort study. J Ren Nutr Dis. 2022;6(1):17–23. doi:10.15586/jrenhep.v6i1.132
22. Fenta T, Engidawork E, Amogne W, Berha AB. Evaluation of current practice of antimicrobial use and clinical outcome of patients with pneumonia at a tertiary care hospital in Ethiopia: a prospective observational study. PLoS One. 2020;15(1):e0227736. doi:10.1371/journal.pone.0227736
23. Bartlett JG, Mundy LM. Community-acquired pneumonia. N Engl J Med. 1995;333(24):1618–1624. doi:10.1056/NEJM199512143332408
24. Isturiz RE, Luna CM, Ramirez J. Clinical and economic burden of pneumonia among adults in Latin America. Int J Infect Dis. 2010;14(10):e852–e6. doi:10.1016/j.ijid.2010.02.2262
25. Greene DN, McPherson GW, Rongitsch J, et al. Hematology reference intervals for transgender adults on stable hormone therapy. Clin Chim Acta. 2019;492:84–90. doi:10.1016/j.cca.2019.02.011
26. Kratz A, Ferraro M, Sluss PM, Lewandrowski KB. Normal reference laboratory values. N Engl J Med. 2004;351(15):1548–1563. doi:10.1056/NEJMcpc049016
27. Kellett J. The assessment and interpretation of vital signs. In: Textbook of Rapid Response Systems. Springer; 2017:63–85.
28. Reade MC, Weissfeld L, Angus DC, Kellum JA, Milbrandt EB. The prevalence of anemia and its association with 90-day mortality in hospitalized community-acquired pneumonia. BMC Pulm Med. 2010;10(1):1–10. doi:10.1186/1471-2466-10-15
29. Elshamly M, Nour MO, Omar AM. Clinical presentations and outcome of severe community-acquired pneumonia. J Chest Dis Tuberc. 2016;65(4):831–839. doi:10.1016/j.ejcdt.2016.06.002
30. Pereira J, Paiva J, Baptista J, Froes F, Gonçalves-Pereira JJCC. Severe community-acquired pneumonia: risk factors for in-hospital mortality. Crit Care. 2012;16(1):1–189.
31. Sirvent JM, de la Torre MC, Lorencio C, et al. Predictive factors of mortality in severe community-acquired pneumonia: a model with data on the first 24 h of ICU admission. Med Intensiva. 2013;37(5):308–315. doi:10.1016/j.medin.2013.03.003
32. Balakrishnan I, Crook P, Morris R, Gillespie S. Early predictors of mortality in pneumococcal bacteraemia. Int J Infect. 2000;40(3):256–261. doi:10.1053/jinf.2000.0653
33. Xu L, Ying S, Hu J, et al. Pneumonia in patients with cirrhosis: risk factors associated with mortality and predictive value of prognostic models. Respir Res. 2018;19(1):1–11. doi:10.1186/s12931-018-0934-5
34. Ito A, Ishida T, Tokumasu H, et al. Prognostic factors in hospitalized community-acquired pneumonia: a retrospective study of a prospective observational cohort. BMC Pulm Med. 2017;17(1):1–10. doi:10.1186/s12890-017-0424-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.