Back to Journals » International Journal of Women's Health » Volume 15
Outcome of Different Endometrial Preparation Protocols Prior to Frozen-Thawed Embryo Transfer on Pregnancy Outcomes in Women with Repeated Implantation Failure
Authors Xiu YL, Sun KX, Zhang Q, Xiao YH, Bai X, Chen Y, Zhao MS, Yu YX ![]()
Received 2 August 2023
Accepted for publication 8 November 2023
Published 24 November 2023 Volume 2023:15 Pages 1835—1844
DOI https://doi.org/10.2147/IJWH.S433640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Yin-Ling Xiu, Kai-Xuan Sun, Qian Zhang, Yu-Hong Xiao, Xue Bai, Yong Chen, Meng-Si Zhao, Yue-Xin Yu
Center of Reproductive Medicine, General Hospital of Northern Theatre Command, Shenyang, 110016, People’s Republic of China
Correspondence: Yue-Xin Yu, Center of Reproductive Medicine, General Hospital of Northern Theater Command, No. 83, Wenhua Road, Shenhe District, Shenyang, 110016, People’s Republic of China, Tel +86-18809881296, Email [email protected]
Aim: To compare the pregnancy outcomes of frozen-thawed embryo transfer (FET) cycles among women with repeated implantation failure (RIF) treated with various endometrial preparation protocols.
Methods: A total of 605 women with RIF were retrospectively recruited between January 2017 and December 2020 from Northern Theater General Hospital. Patients were divided into natural cycles, hormone replacement therapy (HRT) cycles, depot gonadotropin-releasing hormone (GnRH) agonist-HRT, and endometrial scratching (ES) plus depot GnRH agonist-HRT. The primary endpoint was clinical pregnancy rate, while secondary endpoints included live birth rate and pain assessment.
Results: Of the 605 recruited patients, 63 were undergoing natural cycles, 281 were treated with HRT cycles, 141 treated with depot GnRH agonist-HRT, and 120 treated with ES combined with depot GnRH agonist-HRT. There were significant differences among protocols on clinical pregnancy rate (P=0.029), while no significant difference was observed among protocols on live birth rates (P=0.108). Multivariate analyses suggested that HRT (odds ratio [OR]: 0.50; 95% confidence interval [CI]: 0.28– 0.89; P=0.019) and depot GnRH agonist-HRT (OR: 0.49; 95% CI: 0.27– 0.91; P=0.021) cycles were associated with a lower clinical pregnancy rate as compared with natural cycles, while no significant difference between ES combined with depot GnRH agonist-HRT and natural cycles for clinical pregnancy rates (OR: 0.72; 95% CI: 0.38– 1.36; P=0.313). Moreover, the HRT (OR: 0.70; 95% CI: 0.39– 1.28; P=0.239), depot GnRH agonist-HRT (OR: 0.67; 95% CI: 0.35– 1.29; P=0.229), and ES combined with depot GnRH agonist-HRT (OR: 1.11; 95% CI: 0.58– 2.14; P=0.754) cycles had no significant effects on live birth rate as compared with natural cycles. A total of 87.50% patients treated with ES combined with depot GnRH agonist-HRT reported pain during the procedure.
Conclusion: ES and depot GnRH agonists could be considered for RIF women with high-quality blastocysts, 14 days after verified transplantation failure.
Keywords: endometrial scratching, depot GnRH agonist, repeated implantation failure, blastocysts, clinical pregnancy rate, live birth rate
Introduction
Infertility has become a major disease in young couples and is the third most common health issue.1 Currently, nearly 10% of people face difficulties in conceiving naturally and are in need of fertility therapies, such as assisted reproductive technology (ART), especially in developed countries.2 Moreover, the number of ART cycles has increased by 20% since 2011, and this increase is mainly centered on frozen-thawed embryo transfer (FET), oocyte donation, preimplantation genetic testing, and single embryo transfer (SET).3 Despite technical advances in in vitro fertilization (IVF) and the increasing application of FET, the incidence of recurrent implantation failure (RIF) in women undergoing IVF embryo transfer (ET) remains high, ranging from 10–15%.4,5
Currently, RIF poses a greater clinical challenge for women undergoing ART, and no international consensus for the diagnostic criteria for RIF or standard treatments has been established.6,7 Nearly 23–45% of ART specialists recommended that RIF be defined as having more than two transplantation failures.5 The etiology of RIF involves underlying diseases, uterine abnormalities, and embryonic factors.8 Despite controlling for these factors, RIF still occurs.9 Therefore, additional effective treatment protocols should be applied to improve pregnancy outcomes in women undergoing RIF.
Synchronization of blastocyst development with receptivity of the endometrium is important for FET because endometrium is the destination of embryo implantation.10 Therefore, an appropriate endometrial preparation protocol can promote implantation; however, the optimal protocol remains controversial. Currently, natural cycles, ovarian stimulation cycles, and hormone replacement therapy (HRT) cycles are widely used for the preparation of the endometrium before FET. Moreover, studies have indicated that endometrial scratching (ES) in the cycle preceding IVF could improve endometrial receptivity.11–14 The potential mechanism underlying the procedure could involve improving impaired endometrial receptivity through the partial normalization of estrogen and progesterone receptor expression, as well as pinopode proliferation.15 Decidualization of the endometrium could be initiated by ES, thus increasing the probability of implantation of a replaced embryo.16 Furthermore, inflammatory and immune processes could be influenced by ES, leading to the promotion of embryo implantation.17–20 In addition, studies have demonstrated that the use of gonadotropin-releasing hormone (GnRH) prior to FET could regulate the expression of the enzymes and cytokines, which play a directly impact on endometrial receptivity markers.21,22 However, whether ES combined with depot GnRH agonists provides better pregnancy outcomes than depot GnRH agonists for women with RIF undergoing HRT remains unclear. This study aimed to compare natural cycles and three HRT protocols prior to FET for pregnancy outcomes in women with RIF.
Materials and Methods
Study Design and Patient Recruitment
This study was designed as a retrospective cohort, recruiting patients who presented at the Department of Reproductive Medicine, Northern Theater General Hospital, between January 2017 and December 2020. The Ethics Committee of Northern Theater General Hospital approved this study (registration number: 202H2019PJ003). The study was performed following the Declaration of Helsinki. The requirement for informed consent was waived owing to the retrospective design of the study and the data did not contain any identifying information. Patients were included if they met the following criteria: (1) had ≥3 fresh or frozen cycles, which did not reach clinical pregnancy after transplantation of ≥4 high-quality embryos. Implantation failures were not caused by chromosomal, anatomical, endocrine, or other etiological factors; (2) needed performed FET, and >1 high-quality embryo was transferred; (3) aged <40.0 years; (4) with infertility ≤10 years; and (5) not caused by chromosomal abnormalities.23 The exclusion criteria were as follows: (1) women with known endometriosis, endometriomas, adenomyosis, uterine malformations, endometrial abnormalities, severe male-factor infertility, uterine polyps, fibroids, or hydrosalpinx; (2) chromosomal abnormalities in one or both of the couples; (3) a history of diabetes, thyroid disease, mental disease, or autoimmune disease; and (4) reduced ovarian reserves (anti-Mullerian hormone [AMH] ≤1.1 μg/L), including premature ovarian failure and insufficiency. After screening the potentially included patients, a total of 605 women with RIF treated with HRT, depot GnRH agonist-HRT, or ES combined with GnRH agonist-HRT prior to FET were identified (Figure 1).
 |
Figure 1 Patients recruited according to inclusion and exclusion criteria. |
Endometrial Preparation Protocols
According to the endometrial preparation protocols, patients were divided into natural cycles, HRT cycles, depot GnRH agonist (HRT), and ES combined with depot GnRH agonist (HRT). The endometrium was prepared with estrogen and progesterone for all FET cycles.
In the HRT cycle group, estrogen and progesterone were sequentially administered prior to FET to prepare the endometrium. Daily oral estrogen (4 mg) was started on the fifth day of the menstrual period. After 1 week, transvaginal ultrasonography was performed to detect endometrial thickness, serum estradiol (E2), luteinizing hormone (LH), and progesterone (P) levels. Subsequently, the estrogen dose was adjusted according to endometrial thickness and hormone levels. An intrauterine infusion of 4.5iu GH (Human Growth Hormone for Injection, Anhui Anke) was administered on day 8 of estrogen treatment.24,25 Before 3–5 days of the FET, the progesterone (40 mg/day) was intramuscular injected, and the dose of progesterone was reduced after 42 days of FET, until stopped at 56 days of FET. Simultaneously, 4 mg of estrogen were added every day.
In the depot GnRH agonist-HRT group, GnRH downregulation was observed by subcutaneous injection of 3.75 mg of leuprolide acetate (Beijing Boen) on day 3 or 5 of the menstrual cycle. After 28–32 days, the patients returned to the hospital for re-examination, ultrasonography to detect endometrial thickness, and serum E2, LH, and P level measurements. The patients then underwent HRT with sequential administration of estrogen and progesterone prior to FET to prepare the endometrium, and the regimen was consistent with that of the HRT cycle group (intrauterine infusion of 4.5iu GH was administered on day 8 of estrogen treatment).
In the ES combined with depot GnRH agonist-HRT group, ES was performed for non-pregnant women, 14 days after transplantation failure by the same operators. The cervix was dilated to size 5 with a cervical dilator and a size 4 curette was used to superficially scratch all surfaces of the endometrium. Subsequently, a subcutaneous injection of 3.75 mg leuprolide acetate (Beijing Boen) was administered for pituitary downregulation. After 28–32 days, women were re-admitted to the hospital for re-examination, ultrasonography to detect endometrial thickness, and serum measurements of E2, LH, and P levels. HRT was administered approximately 4 weeks after the GnRH agonist dose,26 and patients underwent HRT with sequential administration of estrogen and progesterone prior to FET to prepare the endometrium. Luteal support was provided at 10 weeks of gestation after pregnancy.
Embryo Quality Assessment
All the transferred embryos were cryopreserved by vitrification and transferred after thawing. Embryo morphology was assessed on days 3, 5, and 6. Cleavage-stage embryos with at least seven blastomeres and <20% fragmentation were considered to be high-quality embryos. Blastocysts were scored according to the Gardner and Schoolcraft grading system and recorded as high quality if they reached at least expansion stage 3 with an A or B (3BB) inner cell mass and trophectoderm.27–29 The laboratory procedures and conditions remained constant with fixed operators. All FET patients underwent endometrial receptivity testing on the morning of embryo transfer. Endometrial thickness,30 endometrial morphology,31 and endometrial blood flow32 were measured by professional sonographers in our center using the same ultrasound machine (Voluson E8; GE Healthcare, Chicago, IL, USA).
Data Collection
The general demographics and characteristics of all patients were collected from the electronic medical record system, including maternal age, years of infertility, basal follicle-stimulating hormone (FSH), basal AMH, basal E2, body mass index ([BMI], calculated as weight (kg) divided by height (meters) squared), basal number of antral follicles, number of previous embryo transfers, type of infertility, endometrial thickness, endometrial type (A: the endometrium is in the early proliferative phase, with a thickness of generally 4–6 mm, and the echogenicity appears as low echogenicity; B: the endometrium is in the late proliferative phase, showing homogeneous moderate echogenicity. However, the midline of the uterine cavity echoes intermittently unclear, and the thickness is generally around 9–12 mm), amount of sub-endometrial blood, endometrial blood flow type (I: blood vessels pass through the low echogenic zone on the outer side of the endometrium, but they have not reached the high echogenic outer edge of the endometrium; II: blood vessels pass through the high echogenic outer edge of the endometrium but have not entered the low echogenic zone of the endometrium; III: the blood vessels have entered the low echogenic zone of the endometrium), days of embryo transfer, embryo transfer type, and number of transferred embryos.
Outcome Measurements
The primary endpoint was clinical pregnancy, defined as a gestational sac visible on transvaginal ultrasound.33 The secondary endpoints were live birth, pain assessment, and complications.34
Statistical Analysis
Patient characteristics were assigned as continuous and categorical data. Continuous data are described as mean (standard deviation) and median (interquartile range) according to data distribution, while categorical data are shown as frequency and proportion. The differences among the three groups were assessed using one-way analysis of variance and the Kruskal–Wallis test for continuous data, and categorical data were compared using chi-square tests. Multivariate logistic regression analyses were performed to compare the effects of endometrial preparation protocols on the incidence of clinical pregnancy and live birth rates. Odds ratios (OR) with 95% confidence intervals (CI) were calculated as effect estimates. Moreover, the pain assessment in women treated with ES combined with a depot GnRH agonist-HRT was recorded. All reported P values were two-sided, and the significance level was 0.05. Statistical analyses were performed using SPSS Statistics for Windows version 19.0 (IBM Corp., Armonk, NY, USA).
Results
Patient Characteristics
The demographic and clinical characteristics of the patients in the four groups are shown in Table 1. Of the 605 recruited patients, 63 were natural cycles, 281 were treated with HRT cycles, 141 with depot GnRH agonist-HRT, and 120 with ES combined with depot GnRH agonist-HRT. There were no significant differences among the four protocols for maternal age (P=0.382), years of infertility (P=0.682), basal FSH level (P=0.374), basal AMH level (P=0.066), BMI (P=0.052), type of infertility (P=0.559), endometrial thickness (P=0.117), endometrial type (P=0.285), amount of sub-endometrial blood (P=0.311), days of embryo transfer (P=0.540), and number of transferred embryos (P=0.403). However, we noted significant differences among the four protocols for basal E2 (P<0.001), basal number of antral follicles (P=0.013), number of previous embryo transfers (P<0.001), and endometrial blood flow type (P=0.023).
 |
Table 1 The Demographic and Clinical Characteristics of Recruited Patients |
Clinical Pregnancy Rate
The clinical pregnancy rates in natural, HRT, depot GnRH agonist-HRT, and ES plus depot GnRH agonist-HRT cycles were 60.32, 41.99, 43.26, and 51.67%, respectively, and the differences of clinical pregnancy rate among four protocols were statistically significant (P=0.029; Table 1). After adjusted potential confounder factors, we noted HRT (OR: 0.50; 95% CI: 0.28–0.89; P=0.019) and depot GnRH agonist-HRT (OR: 0.49; 95% CI: 0.27–0.91; P=0.021) cycles were associated with a lower clinical pregnancy rate as compared with natural cycles, while no significant difference was observed between ES combined with depot GnRH agonist-HRT and natural cycles for clinical pregnancy rates (OR: 0.72; 95% CI: 0.38–1.36; P=0.313) (Table 2).
 |
Table 2 Multivariate Analyses for Pregnancy Outcomes Among Endometrial Preparation Protocols |
Live Birth Rate
The live birth rates in natural, HRT, depot GnRH agonist-HRT, and ES plus depot GnRH agonist-HRT cycles were 38.10, 27.76, 29.08, and 38.33%, respectively, and the differences among four protocols were not statistically significant (P=0.108; Table 1). The results of multivariate regression analyses suggested that HRT (OR: 0.70; 95% CI: 0.39–1.28; P=0.239), depot GnRH agonist-HRT (OR: 0.67; 95% CI: 0.35–1.29; P=0.229), and ES combined with depot GnRH agonist-HRT (OR: 1.11; 95% CI: 0.58–2.14; P=0.754) cycles showed no statistically significant differences in live birth rate as compared with natural cycles (Table 2).
Pain Assessment in ES Combined with Depot GnRH Agonist-HRT Group
Table 3 shown the details of pain and complications in women in the ES combined with depot GnRH agonist-HRT group. All patients underwent routine follow-up after ES, and 105 (87.5%) reported feeling pain during surgery, of which 65 (61.9%) reported pain similar to dysmenorrhea, 15 (14.29%) felt sharp pain, 14 (13.33%) contraction-like pain, and 11 (10.48%) felt mild pain. Most of the patients considered this pain to be tolerable which resolved quickly after the operation. Only nine patients still felt pain 24 hours after the operation. Three patients had post-ES bleeding three days after the surgery, and two had abnormal leucorrhea postoperatively.
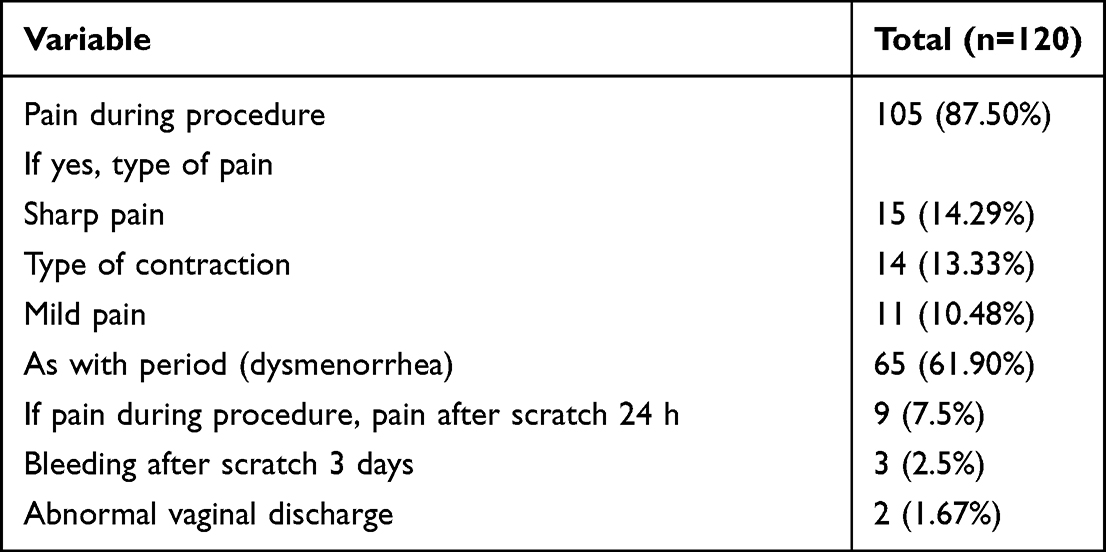 |
Table 3 Pain Assessment and Complications for Patients Treated with Endometrial Scratching Plus Depot Gonadotropin-Releasing Hormone Agonist-HRT |
Discussion
Numerous studies recommend using ES to improve embryo implantation in patients with RIF,35–40 but whether ES combined with existing endometrial preparation protocols could improve pregnancy outcomes in women with RIF remains controversial. The current study recruited 605 women with RIF, and the demographic and clinical characteristics of the patients in the four groups were relatively well balanced. After adjusted for potential confounders, we noted that HRT and depot GnRH agonist-HRT cycles were associated with lower clinical pregnancy rate as compared with natural cycles, while the difference between ES plus depot GnRH agonist-HRT and natural cycles was not statistically significant. Moreover, there was no significant difference among four protocols for live birth rates. Moreover, most of the pain that occurred during ES was tolerable and quickly relieved.
Several studies have addressed the effects of ES on improving pregnancy outcomes. A prospective Israeli study found that ES through a biopsy catheter on days 8, 12, 21, and 26 in spontaneous menstrual cycles before IVF-ET treatment could increase women’s chances of conceiving in subsequent treatment cycles. Moreover, they pointed out that ES could improve the rates of implantation (27.7 vs 14.2%), clinical pregnancy (66.7 vs 30.3%), and live birth (48.9 vs 23.6%).41 A meta-analysis performed by Vitagliano et al, including 10 trials, found that ES can improve pregnancy outcomes in IVF patients with at least two previous embryo transfer failures.42 However, whether ES can improve pregnancy outcomes in patients with RIF remains unclear due to limitations in sample size and study quality. The potential beneficial effect of performing ES in patients with RIF may positively affect endometrial receptivity by normalizing marker expression in most but not all endometrial cells, thereby increasing ongoing pregnancy rates.15 However, some scholars have pointed out that endometrial mechanical stimulation does not improve the clinical pregnancy rate in patients with RIF and found that ES did not improve implantation and pregnancy rates.43 One potential reason for this could be that the endometrium had not sufficiently recovered because the interval between ES and embryo implantation was short. In this study, we noted that in the ES plus depot GnRH agonist-HRT group, there was no significant difference between clinical pregnancy rate and live birth rate, which could explained by the following: ES 14 days after verified transplantation failure and women with high-quality embryos who failed a third transfer were selected. Moreover, the use of ES required straightforward communication with the patients and notification of their condition, which reflects real world comparisons of endometrial preparation protocols on pregnancy outcomes in women with RIF.
The use of FET could improve the reproductive outcomes in women with RIF,44 but whether undergoing a natural cycle, using an HRT cycle, or a depot GnRH agonist combined with an HRT cycle is more effective in FET, especially in patients with RIF, remains unclear. Studies have shown that GnRH agonists may restore the secretion of endometrial implantation-related factors such as homeobox A10 and leukemia inhibitory factor, which could then regulate endometrial development and allow embryo implantation and decidual growth.21,45,46 In our study, we noted GnRH agonist-HRT cycles was associated with lower clinical pregnancy rate as compared with natural cycles, while the difference between ES plus depot GnRH agonist-HRT and natural cycles for clinical pregnancy rate was statistically significant. Moreover, we did not find significant differences among the four protocols in live birth rates in women with RIF. However, considering the marginal 95% CI, the conclusion was not robust and needs further verification. Finally, although the live birth rate in the ES combined with depot GnRH agonist-HRT group was higher than that in the GnRH agonist-HRT and HRT groups in women who received a thawing blastocyst embryo transfer cycle, the analyses was based on a smaller number of included patients and crude data; thus, this result might have been overestimated.
Pain during surgery was reported in most patients who received ES combined with a depot GnRH agonist-HRT group. On follow-up, none of the patients regretted the procedure. ES does not require clamping of the cervix because the catheter used is thin with a short procedure time. The resulting cervical stimulation is negligible when entering and exiting the uterine cavity. The operator can better and uniformly use a catheter to stimulate and remove the endometrium from all sides of the uterine cavity and promote the proliferation and differentiation of epithelial and stromal cells, resulting in increased endometrial blood flow. Consequently, most pain symptoms or complications are tolerable and resolve quickly, although the effect of ES on pregnancy outcomes requires further large-scale prospective studies.
Several limitations of this study should be acknowledged. First, this study was designed as a retrospective cohort, and selection or recall biases could confound the conclusions. Second, background therapies for RIF were not addressed, which might have affected pregnancy outcomes in women with RIF. Third, the infertility cause were not available in most patients, which might have played an important role on pregnancy outcomes. Fourth, data on adverse pregnancy outcomes, such as biochemical pregnancies and miscarriages were not available in most patients, which needed further explorations. Finally, the analysis was based on a small number of included patients, and further stratified analyses should be performed based on variables that could affect pregnancy outcomes, such as the amount of sub-endometrial blood and days of embryo transfer.
Conclusions
This study found that endometrial preparation using natural cycles was associated with a higher clinical pregnancy rate compared to HRT cycles and depot GnRH agonist-HRT cycles. Moreover, patients with unexplained RIF, who still have high-quality blastocysts, may consider undergoing ES and depot GnRH agonist injection, 14 days after verified transplantation failures, which may be associated with elevated live birth rates. Given the limitations of this study, the use of ES combined with the depot GnRH agonist-HRT for women with RIF require further large-scale prospective studies.
Abbreviations
ART, Assisted reproductive technology; FET, Frozen embryo transfer; SET, Single embryo transfer; IVF, in vitro fertilization; RIF, recurrent implantation failure; ET, embryo transfer; HRT, hormone replacement therapy; ES, endometrial scratching; GnRH, gonadotropin-releasing hormone; AMH, anti-Mullerian hormone; E2, serum estradiol; LH, luteinizing hormone; P, progesterone; FSH, follicle-stimulating hormone; BMI, body mass index; OR, odds ratios; CI, confidence intervals.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
The Ethics Committee of Northern Theater General Hospital approved this study (registration number: 202H2019PJ003). The study was performed following the Declaration of Helsinki. The requirement for informed consent was waived owing to the retrospective design of the study and the data did not contain any identifying information.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was funded by the Umbilical cord mesenchymal stem cell therapy based on mechanical stimulation improves fertility in early-onset ovarian dysfunction (no: 2020JH2/10300118).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Momenimovahed Z, Taheri S, Tiznobaik A, Salehiniya H. Do the fertility drugs increase the risk of cancer? A review study. Front Endocrinol. 2019;10:313. doi:10.3389/fendo.2019.00313
2. La marca A, Sunkara SK. Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: from theory to practice. Hum Reprod Update. 2014;20(1):124–140. doi:10.1093/humupd/dmt037
3. de Mouzon J, Chambers GM, Zegers-Hochschild F, et al. International committee for monitoring assisted reproductive technologies world report: assisted reproductive technology 2012dagger. Hum Reprod. 2020;35(8):1900–1913. doi:10.1093/humrep/deaa090
4. Sun Y, Zhang Y, Ma X, Jia W, Su Y. Determining diagnostic criteria of unexplained recurrent implantation failure: a retrospective study of two vs three or more implantation failure. Front Endocrinol. 2021;12:619437. doi:10.3389/fendo.2021.619437
5. Cimadomo D, Craciunas L, Vermeulen N, Vomstein K, Toth B. Definition, diagnostic and therapeutic options in recurrent implantation failure: an international survey of clinicians and embryologists. Hum Reprod. 2021;36(2):305–317. doi:10.1093/humrep/deaa317
6. Ben Rafael Z. Repeated implantation failure (RIF): an iatrogenic meaningless definition that generates unnecessary and costly use of add-on procedures. Hum Reprod. 2020;35(7):1479–1483. doi:10.1093/humrep/deaa134
7. Rozen G, Rogers P, Teh WT, Stern CJ, Polyakov A. An algorithm to personalise the diagnosis of recurrent implantation failure based on theoretical cumulative implantation rate. Hum Reprod. 2021;36(6):1463–1468. doi:10.1093/humrep/deab091
8. Fu M, Zhang X, Liang Y, Lin S, Qian W, Fan S. Alterations in vaginal microbiota and associated metabolome in women with recurrent implantation failure. mBio. 2020;11(3). doi:10.1128/mBio.03242-19
9. Ruiz-Alonso M, Blesa D, Diaz-Gimeno P, et al. The endometrial receptivity array for diagnosis and personalized embryo transfer as a treatment for patients with repeated implantation failure. Fertil Steril. 2013;100(3):818–824. doi:10.1016/j.fertnstert.2013.05.004
10. Valdes CT, Schutt A, Simon C. Implantation failure of endometrial origin: it is not pathology, but our failure to synchronize the developing embryo with a receptive endometrium. Fertil Steril. 2017;108(1):15–18. doi:10.1016/j.fertnstert.2017.05.033
11. El-Toukhy T, Sunkara S, Khalaf Y. Local endometrial injury and IVF outcome: a systematic review and meta-analysis. Reprod Biomed Online. 2012;25(4):345–354. doi:10.1016/j.rbmo.2012.06.012
12. Potdar N, Gelbaya T, Nardo LG. Endometrial injury to overcome recurrent embryo implantation failure: a systematic review and meta-analysis. Reprod Biomed Online. 2012;25(6):561–571. doi:10.1016/j.rbmo.2012.08.005
13. Nastri CO, Polanski LT, Raine-Fenning N, Martins WP. Endometrial scratching for women with repeated implantation failure. Hum Reprod. 2014;29(12):2855–2856. doi:10.1093/humrep/deu257
14. Nastri CO, Lensen SF, Gibreel A, et al.Endometrial injury in women undergoing assisted reproductive techniques. Cochrane Database Syst Rev. 2015;3:CD009517. doi:10.1002/14651858.CD009517.pub3
15. Tumanyan A, Gemilyan M, Hambartsoumian E. Single and double endometrial scratching (ES) in infertile women with strict criteria of recurrent implantation failure (RIF). Gynecol Endocrinol. 2019;35(sup1):11–14. doi:10.1080/09513590.2019.1632085
16. Aflatoonian A, Baradaran Bagheri R, Hosseinisadat R. The effect of endometrial injury on pregnancy rate in frozen-thawed embryo transfer: a randomized control trial. Int J Reprod Biomed. 2016;14(7):453. doi:10.18502/ijrm.v14i7.768
17. Granot I, Gnainsky Y, Dekel N. Endometrial inflammation and effect on implantation improvement and pregnancy outcome. Reproduction. 2012;144(6):661–668. doi:10.1530/REP-12-0217
18. Dekel N, Gnainsky Y, Granot I, Mor G. Inflammation and implantation. Am J Reprod Immunol. 2010;63(1):17–21. doi:10.1111/j.1600-0897.2009.00792.x
19. Gnainsky Y, Granot I, Aldo P, et al. Biopsy-induced inflammatory conditions improve endometrial receptivity: the mechanism of action. Reproduction. 2015;149(1):75–85. doi:10.1530/REP-14-0395
20. Gnainsky Y, Granot I, Aldo PB, et al. Local injury of the endometrium induces an inflammatory response that promotes successful implantation. Fertil Steril. 2010;94(6):2030–2036. doi:10.1016/j.fertnstert.2010.02.022
21. Xu B, Geerts D, Hu S, et al. The depot GnRH agonist protocol improves the live birth rate per fresh embryo transfer cycle, but not the cumulative live birth rate in normal responders: a randomized controlled trial and molecular mechanism study. Hum Reprod. 2020;35(6):1306–1318. doi:10.1093/humrep/deaa086
22. Song J, Sun X, Qian K. Endometrial but not ovarian response is associated with clinical outcomes and can be improved by prolonged pituitary downregulation in patients with thin and medium endometrium. Reprod Sci. 2019;26(11):1409–1416. doi:10.1177/1933719118816835
23. Coughlan C, Ledger W, Wang Q, et al. Recurrent implantation failure: definition and management. Reprod Biomed Online. 2014;28(1):14–38. doi:10.1016/j.rbmo.2013.08.011
24. Altmae S, Mendoza-Tesarik R, Mendoza C, Mendoza N, Cucinelli F, Tesarik J. Effect of growth hormone on uterine receptivity in women with repeated implantation failure in an oocyte donation program: a randomized controlled trial. J Endocr Soc. 2018;2(1):96–105. doi:10.1210/js.2017-00359
25. Altmae S, Aghajanova L. Growth hormone and endometrial receptivity. Front Endocrinol. 2019;10:653. doi:10.3389/fendo.2019.00653
26. Karimzade MA, Oskouian H, Ahmadi S, Oskouian L. Local injury to the endometrium on the day of oocyte retrieval has a negative impact on implantation in assisted reproductive cycles: a randomized controlled trial. Arch Gynecol Obstet. 2010;281(3):499–503. doi:10.1007/s00404-009-1166-1
27. Cummins JM, Breen TM, Harrison KL, Shaw JM, Wilson LM, Hennessey JF. A formula for scoring human embryo growth rates in in vitro fertilization: its value in predicting pregnancy and in comparison with visual estimates of embryo quality. J in vitro Fert Embryo Transf. 1986;3(5):284–295. doi:10.1007/BF01133388
28. Gardner DK, Lane M, Schoolcraft WB. Physiology and culture of the human blastocyst. J Reprod Immunol. 2002;55(1–2):85–100. doi:10.1016/S0165-0378(01)00136-X
29. Zhang J, Liu H, Mao X, et al. Effect of body mass index on pregnancy outcomes in a freeze-all policy: an analysis of 22,043 first autologous frozen-thawed embryo transfer cycles in China. BMC Med. 2019;17(1):114. doi:10.1186/s12916-019-1354-1
30. Dickey RP, Olar TT, Taylor SN, Curole DN, Matulich EM. Relationship of endometrial thickness and pattern to fecundity in ovulation induction cycles: effect of clomiphene citrate alone and with human menopausal gonadotropin. Fertil Steril. 1993;59(4):756–760. doi:10.1016/S0015-0282(16)55855-5
31. Gonen Y, Casper RF. Prediction of implantation by the sonographic appearance of the endometrium during controlled ovarian stimulation for in vitro fertilization (IVF). J in vitro Fert Embryo Transf. 1990;7(3):146–152. doi:10.1007/BF01135678
32. Applebaum M. The uterine biophysical profile. Ultrasound Obstet Gynecol. 1995;5(1):67–68. doi:10.1046/j.1469-0705.1995.05010067.x
33. Zegers-Hochschild F, Adamson GD, de Mouzon J, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520–1524. doi:10.1016/j.fertnstert.2009.09.009
34. Bodian CA, Freedman G, Hossain S, Eisenkraft JB, Beilin Y. The visual analog scale for pain: clinical significance in postoperative patients. Anesth. 2001;95(6):1356–1361. doi:10.1097/00000542-200112000-00013
35. Lensen S, Sadler L, Farquhar C. Endometrial scratching for subfertility: everyone’s doing it. Hum Reprod. 2016;31(6):1241–1244. doi:10.1093/humrep/dew053
36. Bar G, Harlev A, Alfayumi-Zeadna S, et al. Recurrent implantation failure: which patients benefit from endometrial scratching prior to IVF? Arch Gynecol Obstet. 2020;301(3):817–822. doi:10.1007/s00404-019-05424-1
37. Mak JSM, Chung CHS, Chung JPW, et al. The effect of endometrial scratch on natural-cycle cryopreserved embryo transfer outcomes: a randomized controlled study. Reprod Biomed Online. 2017;35(1):28–36. doi:10.1016/j.rbmo.2017.04.004
38. Yeung TW, Chai J, Li RH, Lee VC, Ho PC, Ng EH. The effect of endometrial injury on ongoing pregnancy rate in unselected subfertile women undergoing in vitro fertilization: a randomized controlled trial. Hum Reprod. 2014;29(11):2474–2481. doi:10.1093/humrep/deu213
39. Dain L, Ojha K, Bider D, et al. Effect of local endometrial injury on pregnancy outcomes in ovum donation cycles. Fertil Steril. 2014;102(4):1048–1054. doi:10.1016/j.fertnstert.2014.06.044
40. van Hoogenhuijze NE, Mol F, Laven JSE, et al. Endometrial scratching in women with one failed IVF/ICSI cycle-outcomes of a randomised controlled trial (SCRaTCH). Hum Reprod. 2021;36(1):87–98. doi:10.1093/humrep/deaa268
41. Barash A, Dekel N, Fieldust S, Segal I, Schechtman E, Granot I. Local injury to the endometrium doubles the incidence of successful pregnancies in patients undergoing in vitro fertilization. Fertil Steril. 2003;79(6):1317–1322. doi:10.1016/S0015-0282(03)00345-5
42. Vitagliano A, Di Spiezio Sardo A, Saccone G, et al. Endometrial scratch injury for women with one or more previous failed embryo transfers: a systematic review and meta-analysis of randomized controlled trials. Fertil Steril. 2018;110(4):687–702 e682. doi:10.1016/j.fertnstert.2018.04.040
43. Levin D, Hasson J, Cohen A, et al. The effect of endometrial injury on implantation and clinical pregnancy rates. Gynecol Endocrinol. 2017;33(10):779–782. doi:10.1080/09513590.2017.1318369
44. Magdi Y, El-Damen A, Fathi AM, et al. Revisiting the management of recurrent implantation failure through freeze-all policy. Fertil Steril. 2017;108(1):72–77. doi:10.1016/j.fertnstert.2017.04.020
45. Du H, Taylor HS. The role of Hox genes in female reproductive tract development, adult function, and fertility. Cold Spring Harb Perspect Med. 2015;6(1):a023002. doi:10.1101/cshperspect.a023002
46. Hu L, Li H, Huang CL, Chen H, Zhu G, Qian K. Regulation of myeloid ecotropic viral integration site 1 and its expression in normal and abnormal endometrium. Fertil Steril. 2014;102(3):856–863 e852. doi:10.1016/j.fertnstert.2014.05.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gonadotropin Releasing Hormone Agonists Combined with Hormone Replacement Therapy Significantly Improves Reproductive Outcomes for Patients with Thin Endometrium and Intramural Fibroids in Frozen Embryo Transfer Cycles
Wei L, Tian B, Wang S, Xu S, Zhang C
Drug Design, Development and Therapy 2025, 19:173-183
Published Date: 10 January 2025