")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Outcome of Diabetic Keto Acidosis Treatment and Associated Factors Among Adult Patients Admitted to Emergency and Medical Wards at St. Paul’s Hospital, Addis Ababa Ethiopia, 2023: A Cross-Sectional Study
Authors Derse TK , Haile MT, Chamiso TM
Received 18 August 2023
Accepted for publication 21 October 2023
Published 3 November 2023 Volume 2023:16 Pages 3471—3480
DOI https://doi.org/10.2147/DMSO.S432220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Tsegamlak Kuemlachew Derse,1 Michael Tamene Haile,2 Tekalign Markos Chamiso3
1Department of Critical and Emergency Nursing, St. Paul’s Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Pediatrics and Child Health Nursing, St. Paul’s Millennium Medical College, Addis Ababa, Ethiopia; 3Department of Cardiovascular Nursing, St. Paul’s Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Tsegamlak Kuemlachew Derse; Tekalign Markos Chamiso, St.Paul’s Hospital MMC, Addis Ababa, Ethiopia, Email [email protected]; [email protected]
Background: Diabetic ketoacidosis is a potentially fatal disease that affects adults. Therefore, rapid detection and treatment are required to decrease mortality rates. Most of the earlier research on diabetic ketoacidosis in Ethiopia concentrated on its prevalence and associated factors. This study aimed to assess the treatment outcomes of diabetic ketoacidosis and its associated factors in adult patients admitted to St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, in 2023.
Methods: This institution-based retrospective cross-sectional study was conducted with a sample size of 357. The data were entered in Epidata version 4.6 and exported to the Statistical Package for the Social Sciences (SPSS) version 25 for analysis. Adjusted Odds Ratio (AOR) with a 95% confidence interval was estimated to determine its association with outcome of treatment.
Results: Three hundred fifty-seven diabetic ketoacidosis patients’ charts were reviewed. Fourteen (3.9%) diabetic ketoacidosis (DKA) patients had died. Those Patients with diabetic ketoacidosis who had acute comorbidity (presence of sepsis) (AOR = 3.24, 95% CI: 1.20– 10.2), international unit (IU) insulin administration in the 1st 24 hours (AOR = 8.046, 95% CI: 3.881– 25.32), fluid replacement in the 1st 24 hours (AOR = 5.84, 95% CI: 1.53– 10.07), and potassium replacement (AOR = 3.08, 95% CI: 1.835– 5.817) were independently associated with treatment outcome of diabetic ketoacidosis. Insulin administration for the first 24 hours more than > 60 IU insulin showed improvement in treatment outcome by 8.04 times more likely than less < 60 IU insulin administration for the first 24 hours. More > 6 liters fluid replacement in the first 24 hours had improvement in treatment outcome by 5.84 times more likely than < 6 liters fluid replacement.
Conclusion: A considerable proportion of the patients with diabetic ketoacidosis died at St. Paul’s hospital millennium medical college. Stakeholders must emphasize the treatment of patients with diabetes (diabetic ketoacidosis), according to the recommendations of local and international guidelines.
Keywords: morbidity, die, replacement, improvement and mortality
Introduction
Diabetic Ketoacidosis (DKA) is a life-threatening acute hyperglycemic complication associated with diabetes mellitus (DM).1 With a blood sugar level of at least 14.0 mmol/l, presence of urine or plasma ketones, and serum bicarbonate level of less than 18 mmol/l required for the diagnosis of DKA. It appears that DKA still has a high fatality rate during inpatient therapy.1 DKA may be triggered by medications that alter carbohydrate metabolism, including corticosteroids, thiazides, sympathetic mimetic drugs, and pentamidine. Both conventional and atypical antipsychotic medications are associated with a low risk of hyperglycemia and DKA.2
Typically, a fruity odor is detectable upon inspection, and breathing is typical of DKA, such as rapid, shallow Kussmaul breathing, or other polycythemia-related symptoms. Numerous other symptoms, including anorexia, nausea, vomiting, stomach discomfort, and weight loss may also be reported.3 Increases in counter-regulatory hormones and decreased peripheral glucose utilization, such as glucagon, are related to it. These factors lead to hyperglycemia and hyperosmolality, resulting in electrolyte loss and osmotic diuresis.4
DKA can be treated with the administration of fluids like normal saline, ringer lactate, and dextrose in water because it results in fluid loss through osmosis.5,6 With the right care, DKA can be successfully treated within 12 to 36 hours, preventing complications and effectively reducing mortality.7 Since DKA is a severe acute complication of diabetes mellitus, it should be treated as quickly as possible with 10–20mL/kg of 0.9% normal saline and 0.5–0.1 unit/kg of insulin drip for the first hour, followed by 0.45% of normal saline plus continued insulin drip and addition of 20mEQ/l of potassium phosphate and acetate until the resolution of DKA for the following two hours, and addition of 0.5% of DW if the blood glucose level reaches 250 mg/dl.8
DKA, which is associated with considerable morbidity and mortality in patients with type 1 and type 2 DM, is the most serious hyperglycemic emergency. In a study conducted by the American Diabetes Association (Hyperglycemia Crises in Adult Patients with Diabetes During treatment of DKA treatment), the average treatment time until blood glucose is 250 mg/dl and ketoacidosis, bicarbonate >18 mmol/l is corrected to 6 and 12 hours, respectively.9 Hyperglycemia is cured more quickly than ketoacidosis. Five percent dextrose should be administered to replacement fluids after the plasma glucose is below 200 mg/dl to allow for sustained insulin treatment until ketonemia is under control while also preventing hypoglycemia.2,5
In-hospital mortality in DKA was found to be 10% in 2015 according to a prospective study conducted in a tertiary care facility in Karnataka, India.9 In a study conducted in Riyadh, Saudi Arabia, at King Abdul-Aziz Medical City, majority (98.2%) of the admitted DKA patients improved and were discharged.10 In Africa, DKA was high mortality rate. According to studies from Kenya, Tanzania, and Ghana, there is an unacceptability high mortality rate, with a fatality rate of 26 to 29%.11 In Malaysia and Zambia, the mortality rates were 16.7% and 17.6%, respectively.12 A retrospective study was conducted at Debre Tabor General Hospital most majority 95.6% of the patients improved and discharged, whereas 4.4% patients died in the hospital.13 Patients who participated in the trial at Jimma University Specialized Hospital had a 74% in-hospital improved and discharge from DKA.14
Generally, understanding the factors associated with diabetic ketoacidosis treatment outcomes is crucial for identifying patients at risk of this complication. Therefore, this study describes the treatment outcomes and factors associated with diabetic ketoacidosis in the emergency and medical wards.
Methods and Materials
Study Area and Study Period
This study was conducted at St. Paul’s hospital millennium medical College. The institution was selected using a simple random sampling procedure.
Although the medical school opened in 2007, the hospital was established in 1968 by late Emperor Haile Selassie II. Currently, the hospital provides services to more than 5 million people as a catchment area. It provides both specialty and subspecialty services including pediatrics, surgery, gynecology, obstetrics, and internal medicine. The hospital has more than 700 beds. The flow rate of patients ranges from 600 to 800 per day. The weekly diabetic follow-up clinic service to 500–600 patients per month. On average, approximately 1300 DKA patients have been admitted to the emergency department and medical wards per year.15
The study was a three years retrospective chart review from January 01/2020 to December 30/2022. This study was conducted between February 1/2023 and April 20/2023.
Study Design and Population
This institutional retrospective cross-sectional study was conducted to assess the outcomes of diabetic ketoacidosis and its associated factors at St. Paul’s hospital millennium medical college, Addis Ababa, Ethiopia. All patients admitted with diabetic ketoacidosis at Addis Ababa public hospitals were the source population, and all patients admitted with diabetic ketoacidosis at St. Paul’s hospital millennium medical college were study population. Charts of patients with diabetic ketoacidosis who were reviewed during the collection period at St. Paul’s hospital millennium medical college were used as the study units.
Inclusion and Exclusion Criteria
The patients’ charts reviewed from February 01/2020 to March 30/2023, and patients aged 18 years and above who had been diagnosed with DKA and received treatment in the hospital’s emergency room and medical ward were included.
Sample Size Determination and Sampling Procedure
The sample size was determined by using a single-population proportion formula. According to study that was done on acute management of diabetic ketoacidosis in Addis Ababa at Tikur Anbessa hospital’s adult emergency department and medical wards, 51.8% of the patients were discharged with improvement.16 The desired precision of 5% and 95% confidence intervals were used for the calculation; the sample size was 384. With finite population correction formula, the final sample size was set to 357. A simple random sampling procedure was used to select one hospital from the 11 governmental hospitals (Figure 1). Therefore, 357 study participants were sampled from the hospital using a systematic sampling method from the emergency and medical DKA registry sheets using the patient’s medical registration number sampling frame.
 |
Figure 1 The schemes presentation of sampling procedure to select study participants from Addis Ababa governmental hospitals, 2023. |
Data Collection and Procedure
Data were collected using a pretested checklist prepared in English. The questionnaire/checklist was adapted by reviewing the literature and similar previous studies.10,14 Medical data were obtained from patient records. Five data collectors and one supervisor were recruited from among the healthcare providers who worked in emergency departments and medical wards.
Data Quality Control and Management
One day of training for five nurses and one physician was provided on data collection methods, and a pretest was performed using 5% (18) of patients’ charts at Tirunesh Beijing General Hospital. The purpose of the pre-test was to ascertain the data collectors’ understanding of the items in the chart, appropriateness of responses, and time required to fill out the questionnaire/checklist. A reliability estimate was conducted, and the Cronbach’s alpha was 0.8 for the ketoacidosis outcome and associated factor measurement tools. Daily supervision was conducted by the lead investigator and supervisor, and during data collection, data were checked for completeness on a daily basis.
Data Analysis Procedure
After data collection was completed, the data were checked for properly collected, recorded, coded, entered, and cleaned into Epi Data version 4.6 and exported to the Statistical Package for the Social Sciences (SPSS) version 25 for analysis. Descriptive statistics, including frequency, proportion, and mean of variables, were used to report the descriptive results. Variables with a p-value <0.25 in bi-variable logistic regression analysis were fitted with multiple logistic regression analysis. In the multivariate logistic regression model, fitness was tested using the Hosmer–Lemeshow goodness-of-fit. Adjusted odds ratio (AOR) with a 95% confidence interval was estimated to assess the strength of the association with the outcome of ketoacidosis treatment. Statistical significance was set at p <0.05. Finally, the processed data were presented by creating frequencies and percentages using tables, texts, and graphs.
Result
Socio-Demographic Characteristics of the Study Participants
In total, the charts of 357 DKA patients were reviewed. Majority of the respondents (39.8) were found to be in the age category of 18–30 years, 193 (54.1%) of the respondents were male, and 205 (57.4%) were urban residents. From the reviewed charts, 14 (3.9%) DKA patients had poor outcome that was death (Table 1).
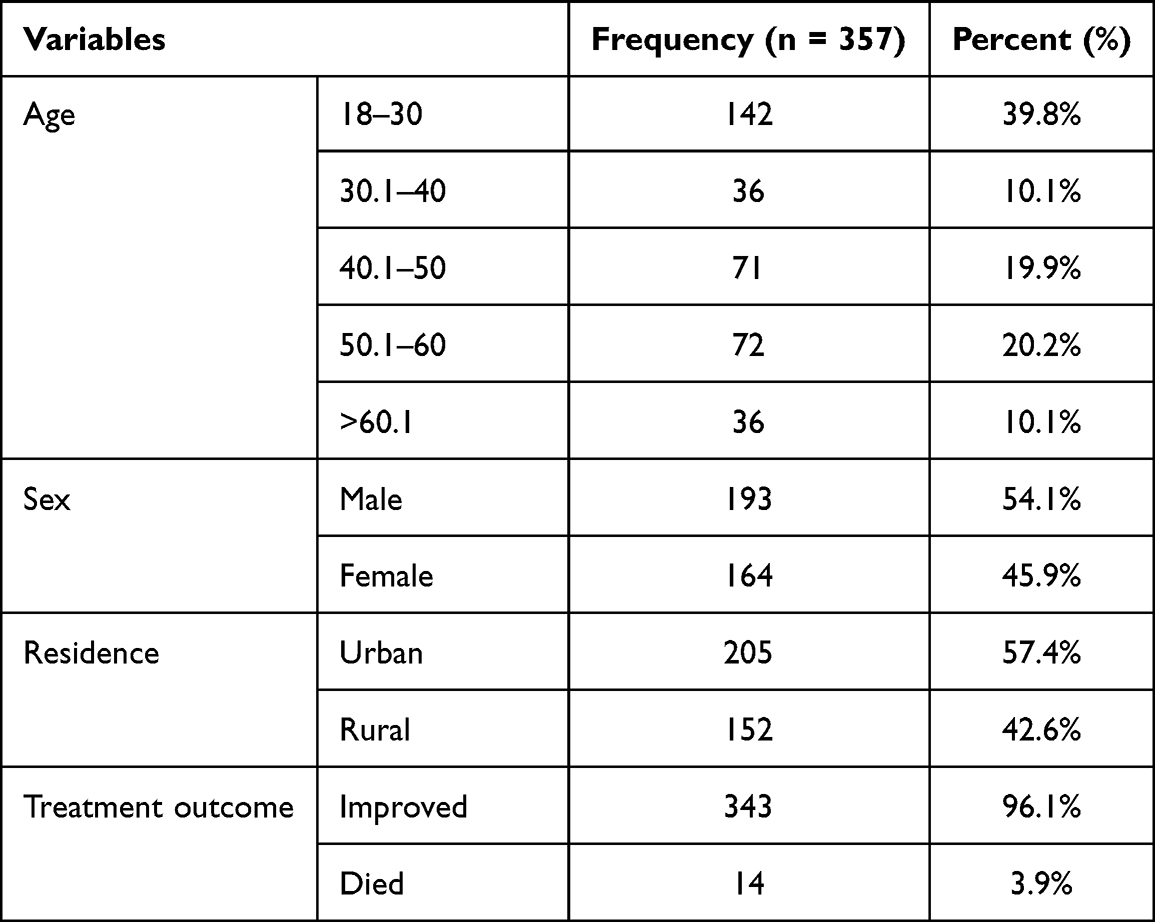 |
Table 1 Socio-Demographic Characteristics of DKA Patients and Their Outcome Admitted to SPHMMC Emergency Department and Medical Ward, Addis Ababa, Ethiopia, 2023 (n = 357) |
Clinical Profile of Participants
Regarding the biochemical profile of the adults admitted with DKA in emergency and medical ward, among 357 adults with DKA, poly symptoms (87.1%) were reported by most patients with DKA, followed by abdominal pain (31.7%). Hyponatremia occurred in 92 (25.8%) and hypokalemia (serum concentration of potassium less than 3.5 mmol/l) 90 (25.2%) and random blood glucose level 425.17 ± 75.45. Majority of the adults 311 (87.1%) had been diagnosed with type 1 DM (Tables 1 and 2).
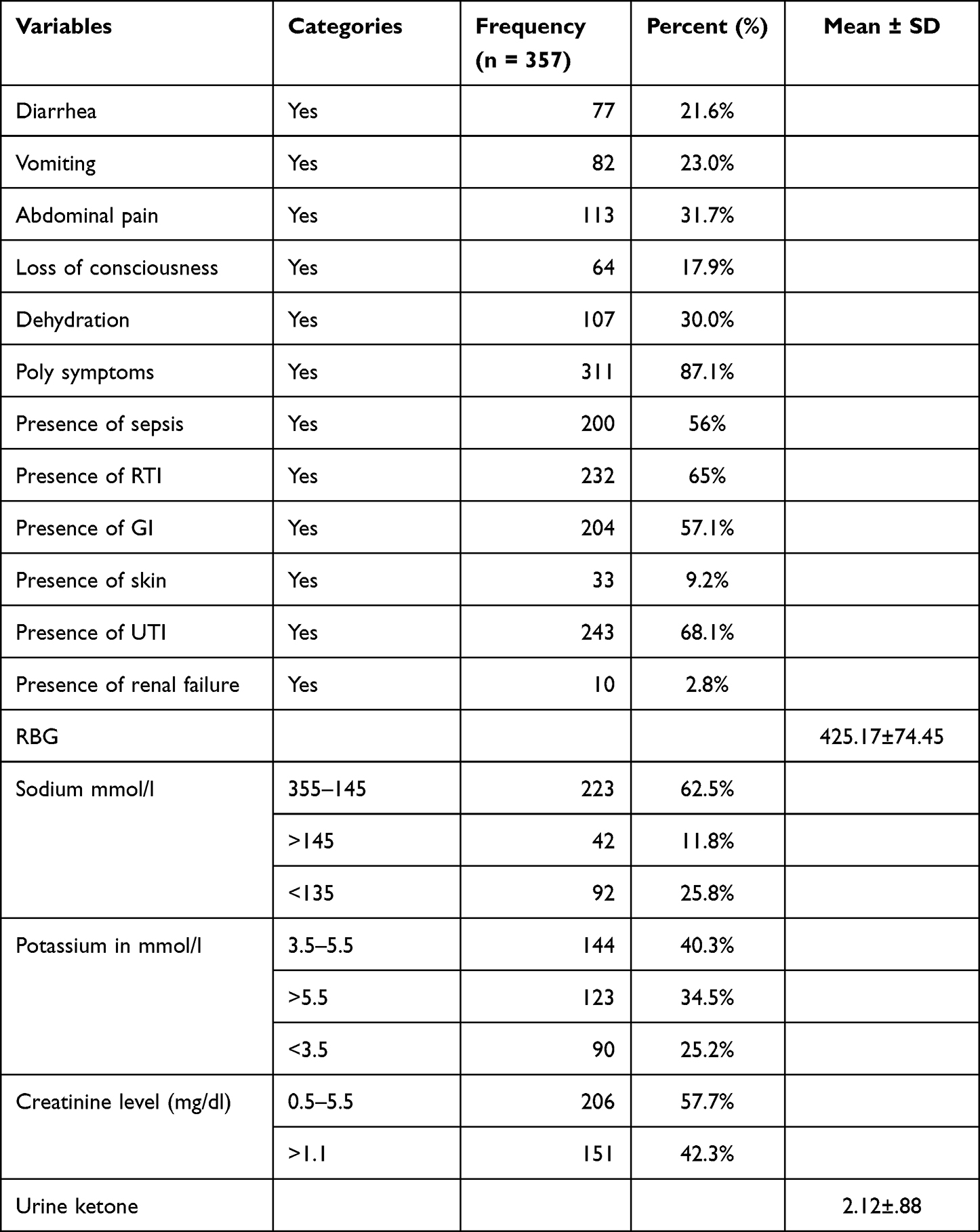 |
Table 2 Clinical Features DKA Patients Admitted to SPHMMC Emergency Department and Medical Ward, Addis Ababa, Ethiopia, 2023 (n = 357) |
Among 357 adults with DKA, approximately 200 (56.0%) had presence of sepsis, 232 (65%) had respiratory tract infections, urinary tract infection accounts for 243 (68.1%) and gastrointestinal infections 204 (57.1) (Table 2). Approximately 22 (6.2%) of them had 00 and trace urine ketone levels, 53 (14.8%) of them had urine ketone level +1, 142 (39.78%) of them had urine ketone level +2 the rest and 140 (39.22%) of had urine ketone level +3 (Figure 2).
 |
Figure 2 The urine ketone level of DKA patients admitted to SPHMMC emergency department and medical ward, Addis Ababa, Ethiopia, 2023 (n=357). |
Concerning the management protocol of DKA patients, the most common type of fluid used for bolus was 0.9% normal saline 147 (41.2%) and 158 (44.3%) of respondents took above 6 litters of total fluid. Of the total insulin administered in the first 24 h, 147 (41.2%) were taken 40IU–60IU and 306 (85.7%) received potassium replacement, and also 213 (59.7%) had 3–5 days of hospital stay (Table 3).
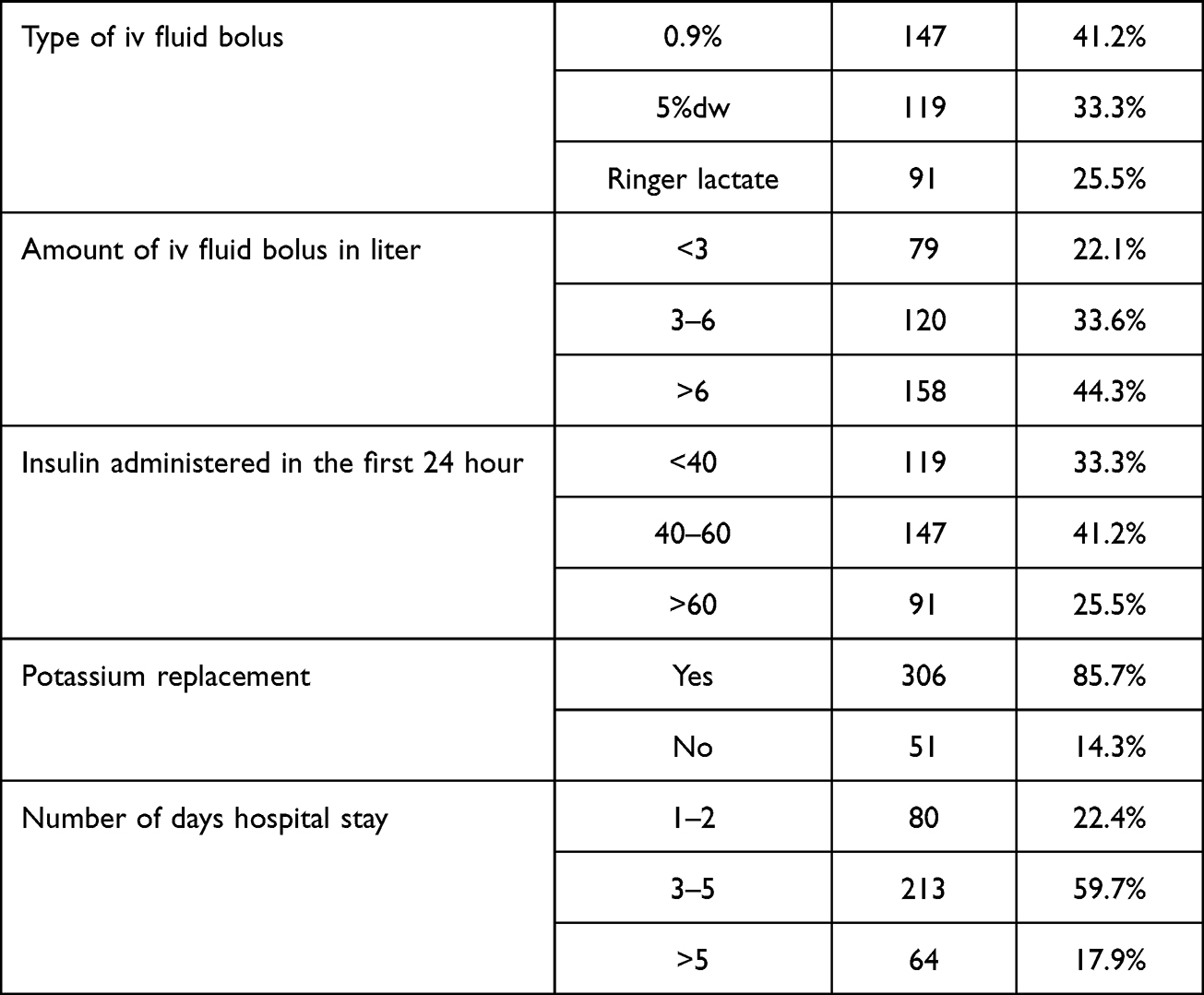 |
Table 3 Biochemical Profile and Management Protocol DKA Patients Admitted to SPHMMC Emergency Department and Medical Wards, Addis Ababa, Ethiopia, 2023 (n = 357) |
Factors Associated with Treatment Outcome (Death) of Adult Patient with DKA
Bi-variable logistic regression analysis indicated that polysymptoms, presence of sepsis, presence of skin infection, presence of pulmonary edema, insulin administration for the first 24 hours, and amount of IV fluid bolus in liter and potassium replacement therapy were variables that qualified the assumption (p < 0.25) and were considered candidates for multi-variable analysis.
The multivariable logistic regression analysis results indicated that the presence of sepsis, insulin administration for the first 24 h, amount of intravenous fluid bolus in litters, and potassium replacement variables were associated with the treatment outcome of DKA (death).
In a multivariable logistic regression analysis, participants who had acute co-morbidity (presence of sepsis) 3.24 times (AOR = 3.24, 95% CI: 1.20–10.2, p < 0.024) more likely to die as compared to those patients who had no presence of sepsis. Study participants who took insulin administration for the first 24 hours more than >60 IU insulin showed improvement in treatment outcome by 8.04 times (AOR = 8.046, 95% CI: 3.881–25.32, p < 0.007) more likely than less <60 IU insulin administration for the first 24 hours. Study participants who treated with more >6 liters fluid replacement in the first 24 hours had an improvement in treatment outcome by 5.84 times (AOR = 5.84, 95%, CI: 1.53–10.07, p < 0.031) more likely than <6 liters fluid replacement. Similarly, the participant patient who did not receive potassium as a replacement 3.08 times (AOR = 3.08, 95% CI: 1.835–5.817 p < 0.006) more likely to die as compared to those patient who received potassium as replacement (Table 4).
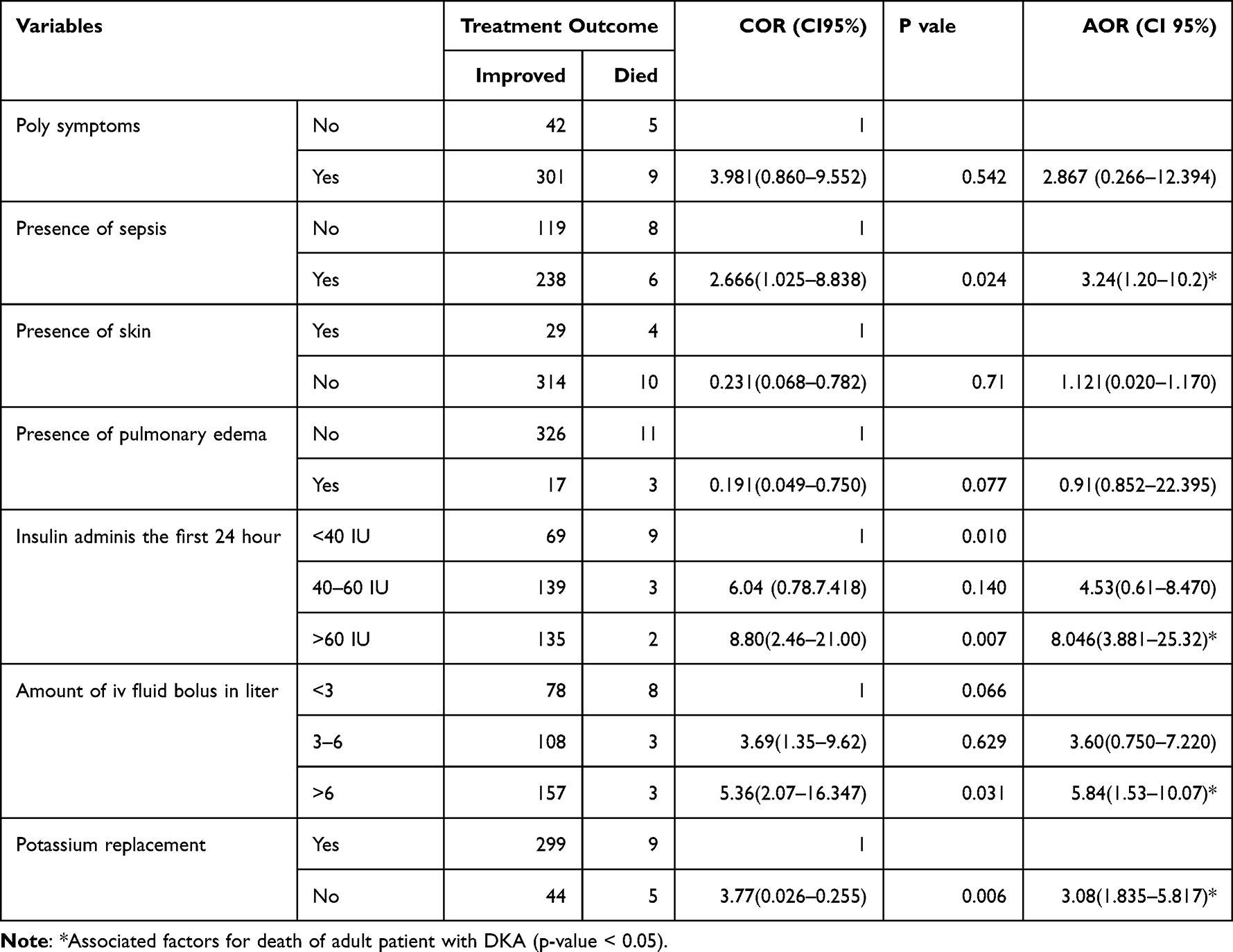 |
Table 4 Factors Associated with Treatment Outcome of DKA Patients Admitted to SPHMMC Emergency Department and Medical Ward, Addis Ababa, Ethiopia, 2023 (n=357) |
Discussion
This facility-based cross-sectional study was designed to determine ketoacidosis treatment outcomes at a selected governmental hospital (St. Paul’s Hospital Millennium Medical College) in Addis Ababa. This study also addressed the socio-demographic characteristics, clinical profiles, comorbidity, complication, management protocol, and treatment outcome of patients with DKA. The results address the main and specific objectives of this study.
The overall number of deaths in this study was 14 (3.9%). When compared with studies that were done in different countries, the studies that were conducted in Kenya, Malaysia, and Zambia, the mortality rates were 26%, 16.7%, and 17.6%, respectively.5,17,18 In Ethiopia, a retrospective study carried out at Shashemene Referral Hospital and Adama General Hospital were 12% and (15.1%), respectively.6,19 There was a higher percentage of improvement in treatment outcomes in Riyadh, Saudi Arabia, and King Abdul-Aziz Medical City (98.2%).14 The variability in the outcome of treatment may reflect the different systems in which this study was conducted; factors may influence treatment, study designs, study times, and multi-specialized hospitals.
Sepsis was positively associated with diabetic ketoacidosis death outcomes. This finding is agreed with a study conducted in Jimma Zone Hospital and Saudi Arabia.10,20 This might be because sepsis results in the production of counter-regulatory hormones, such as adrenaline and cortisol, which decrease the effect of insulin on glucose regulation.12
DKA patients treated with less than six liters fluid replacement in the 1st 24 hours had a positive association with the outcome of treatment. This finding was supported by a study conducted in Adama and East Africa.6,12 This may be because further fluid therapy should be administered at a rate sufficient to maintain adequate blood pressure, urine output, and mental status to correct the estimated water deficit over 24 h.
In addition, DKA in patients who did not receive potassium replacement was significantly associated with treatment outcomes. Different findings also support that, adding 20–40 mmol/l KCl would usually result in adequate replacement, keeping the serum potassium around 4.5 mmol/l.12 This might be because if potassium replacement therapy is not administered to adult patients, hypokalemia leads to cardiac conduction problems, such as cardiac dysthymia. Therefore, unless the patient exhibits hyperkalemia or anuria, potassium should be added to the intravenous fluids at the beginning of the second hour of therapy.
Conclusion
The overall treatment outcome of the patients with DKA admitted to emergency department and medical ward was 14 (3.9%). There was a high in-hospital mortality rate owing to correctable causes. After adjusting for other confounding variables, the main factors for the DKA treatment outcome of death were the presence of sepsis, less insulin administration for the first 24 hours, less bolus IV fluid administration, and lack of potassium replacement.
Abbreviations
AKI, acute kidney injury; AMI, Acute Myocardial Infraction; AOR, Adjusted Odds Ratio; BPH, Benign Prostate Hyperplasia; COR, Crude Odds Ratio; DKA, Diabetic Ketoacidosis; DM, Diabetic Mellitus; E.C, Ethiopian Calendar; HW Workers; ICU, Intensive Care Unit; LOS, Length of Stay; MOH, Minister of Health; SD, Standard Deviation; SPHMMC, St. Paul’s Hospital Millennium Medical College.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Before data collection, ethical clearance was obtained from St. Paul’s hospital millennium medical college Institutional Review Board. Permission to conduct the study was obtained from St. Paul’s Hospital Millennium Medical College. This is in line with the Helsinki Declaration which is stated as “medical research using identifiable human material or data, physicians must normally seek consent for the collection, analysis, storage and/or reuse. There may be situations where consent would be impossible or impractical to obtain for such research or would pose a threat to the validity of the research. In such situations, the research may be done only after consideration and approval of a research ethics committee”.21 The data were anonymous and informed consent was waived by the approving Institutional Review Board because of the retrospective nature of the study.
Consent for Publication
All authors agreed that this paper is eligible for publication.
Acknowledgment
We thank St. Paul’s Hospital Millennium Medical College Research Office and the School of Nursing for providing the opportunity to prepare for this study. We thank the medical registration staff, supervisors, and data collectors for their time and voluntary facilitation of the data-collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting and revising, gave final approval of the paper to be published, agreed on the journal to which the article had to be submitted, and agreed to be accountable for all aspects of the work.
Funding
No funding to perform the study.
Disclosure
The authors declared that they have no competing interests in this work.
References
1. Wolfsdorf J, Glaser N, Sperling MA. Diabetic ketoacidosis in infants, children, and adolescents: a consensus statement from the American Diabetes Association. Diabetes Care. 2006;29(5):1150–1159. doi:10.2337/dc06-9909
2. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009;32(7):1335–1343. doi:10.2337/dc09-9032
3. Lizzo JM, Goyal A, Gupta V. Adult diabetic ketoacidosis. In: StatPearls [Internet]. StatPearls Publishing; 2022.
4. Wolfsdorf JI, Glaser N, Agus M, et al. ISPAD clinical practice consensus guidelines 2018: diabetic ketoacidosis and the hyperglycemic hyperosmolar state. Pediatr Diabetes. 2018;19:155–177. doi:10.1111/pedi.12701
5. Mbugua P, Otieno C, Kayima J, Amayo A, McLigeyo S. Diabetic ketoacidosis: clinical presentation and precipitating factors at Kenyatta National Hospital, Nairobi. East Afr Med J. 2005;82(12). doi:10.4314/eamj.v82i12.9381
6. Kassaye DA, Girsha WD, Guto GJ, Deybasso HA. Diabetic ketoacidosis treatment outcome and associated factors among adult patients admitted to medical wards of Adama Hospital Medical College, Oromia, Ethiopia. Am J Intern Med. 2018;6(2):34–42.
7. Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL. Harrison’s Principles of Internal Medicine. McGraw-Hill Companies, Inc; 2005.
8. Sampson M, Jones C. Joint British Diabetes Societies for Inpatient Care: clinical guidelines and improving inpatient diabetes care. Diabet Med. 2018;35(8):988–991. doi:10.1111/dme.13672
9. Seth P, Kaur H, Kaur M. Clinical profile of diabetic ketoacidosis: a prospective study in a tertiary care hospital. J Clin Diagnostic Res. 2015;9(6):OC01. doi:10.7860/JCDR/2015/8586.5995
10. Alotaibi A, Aldoukhi A, Albdah B, Alonazi JA, Alseraya AS, Alrasheed N. Diabetic ketoacidosis treatment outcome and associated factors among adult patients admitted to the emergency department and medical wards at King Abdulaziz Medical City, Riyadh, Saudi Arabia. Cureus. 2020;12(8). doi:10.7759/cureus.10067
11. McLigeyo SO, Mbugua P, Otieno C, Kayima J, Amayo A. Diabetic ketoacidosis: clinical presentation and precipitating factors at Kenyatta National Hospital, Nairobi. East Afr Med J. 2005;82(12 Suppl):S191–6.
12. Otieno C, Kayima J, Omonge EO, Oyoo GO. Diabetic ketoacidosis: risk factors, mechanisms and management strategies in sub-Saharan Africa: a review. East Afr Med J. 2005;82(12). doi:10.4314/eamj.v82i12.9382
13. Mekonnen GA, Gelaye KA, Gebreyohannes EA, Abegaz TM. Treatment outcomes of diabetic ketoacidosis among diabetes patients in Ethiopia. Hospital-based study. PLoS One. 2022;17(4):e0264626. doi:10.1371/journal.pone.0264626
14. Worku D, Hamza L, Woldemichael K. Patterns of diabetic complications at Jimma University specialized hospital, southwest Ethiopia. Ethiop J Health Sci. 2010;20(1):33–39. doi:10.4314/ejhs.v20i1.69424
15. Bayisa T, Berhane A, Kedir S, Wuletaw T. Admission patterns and outcomes in the medical intensive care unit of St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Ethiop Med J. 2017;55(1):19–26.
16. Adem A, Demis T, Feleke Y. Trend of diabetic admissions in Tikur Anbessa and St. Paul’s University Teaching Hospitals from January 2005-December 2009, Addis Ababa, Ethiopia. Ethiop Med J. 2011;49(3):231–238.
17. Usman A, Sulaiman SAS, Khan AH, Adnan AS. Profiles of diabetic ketoacidosis in multiethnic diabetic population of Malaysia. Trop J Pharm Res. 2015;14(1):179–185. doi:10.4314/tjpr.v14i1.25
18. Kakusa M, Kamanga B, Ngalamika O, Nyirenda S. Comatose and noncomatose adult diabetic ketoacidosis patients at the University Teaching Hospital, Zambia: clinical profiles, risk factors, and mortality outcomes. Indian J Endocrinol Metab. 2016;20(2):199. doi:10.4103/2230-8210.176358
19. Taye GM, Bacha AJ, Taye FA, Bule MH, Tefera GM. Diabetic ketoacidosis management and treatment outcome at medical ward of Shashemene Referral Hospital, Ethiopia: a retrospective study. Clin Med Insights Endocrinol Diabetes. 2021;14:11795514211004957. doi:10.1177/11795514211004957
20. Desse T, Eshetie T. Determinants of long hospital stay among diabetic patients admitted with diabetic ketoacidosis at Jimma University Specialized Hospital. J Trauma Stress Disor Treat. 2016;6(1):2.
21. Portaluppi F, Smolensky MH, Touitou Y. Ethics and methods for biological rhythm research on animals and human beings. Chronobiol Int. 2010;27(9–10):1911–1929. doi:10.3109/07420528.2010.516381
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.