Back to Journals » Journal of Pain Research » Volume 19
Orofacial Pain at a Tertiary Clinic: Comorbidities and Psychological Conditions Using the International Classification of Orofacial Pain (ICOP) Criteria
Authors Brauckhoff LL ![]() , Haavik CM, Haug SR
, Haavik CM, Haug SR ![]() , Rosén A
, Rosén A ![]()
Received 27 January 2026
Accepted for publication 20 May 2026
Published 3 June 2026 Volume 2026:19 595369
DOI https://doi.org/10.2147/JPR.S595369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rune Häckert Christensen
Lise Lotte Brauckhoff,1,* Celine Messaoudi Haavik,1,* Sivakami Rethnam Haug,1 Annika Rosén1,2
1Department of Clinical Dentistry, University of Bergen, Bergen, Norway; 2Department of Oral and Maxillofacial Surgery, Haukeland University Hospital, Bergen, Norway
*These authors contributed equally to this work
Correspondence: Annika Rosén, Department of Clinical Dentistry, University of Bergen, Årstadveien 19, PO Box 7804, Bergen, 5020, Norway, Tel +4755586481, Email [email protected]
Purpose: To characterize a patient group with refractory orofacial pain (OFP) at a tertiary pain clinic with emphasis on subtype distribution, comorbidities, sex differences and psychological factors.
Patients and Methods: This retrospective study reviewed 98 consecutive patients assessed at the National Unit of Orofacial Pain, Haukeland University Hospital, Bergen, Norway (2017– 2021). All patients were investigated by an interdisciplinary team that used a structured clinical interview and assessments and patients completed a series of standardized questionnaires that formed the basis for the final diagnosis and treatment plan. The International Classification of Orofacial Pain (ICOP-2020) was launched later and therefore retrospectively used forming the basis for this study. Five primary subtypes were analyzed: primary myofascial orofacial pain (pMOP), post-traumatic trigeminal neuropathic pain (PTTNP), persistent idiopathic facial pain (PIFP), trigeminal neuralgia (TN) and burning mouth syndrome (BMS). Secondary MOP (sMOP) was recorded when myalgia co-occurred with another primary diagnosis. Descriptive statistics, χ2-tests and one-way ANOVA was performed.
Results: The most frequent diagnosis was pMOP (60.2%), followed by PTTNP (20.4%), PIFP (14.3%), TN (4.1%), and BMS (3.1%). Twenty-five patients had more than one diagnosisa(aPercentages do not sum to 100%. A total of 25 patients with overlapping diagnoses, including 23 patients with secondary MOP and 2 patients with dual primary diagnoses.). Significantly more women (82.6%) had OFP (p< 0.05). Patients with pMOP experienced longest mean pain duration (9.9 years) and reported comorbidities such as body pain, headaches and arthritis more frequently than non-MOP groups (p < 0.05). sMOP was present in 75% of PTTNP cases (p = 0.0038). Psychometric and functional measures varied across subtypes: patients with pMOP exhibited the highest scores on HADS (15.3), MFIQ (14.4), and RS (7.0).
Conclusion: Refractory OFP is dominated by pMOP and female patients. The strong association between PTTNP and sMOP suggests early combined management of neuropathic- and muscle pain which may limit chronification. Together, our findings support a personalized, interdisciplinary approach to OFP that can improve diagnostic precision and optimize long-term patient outcomes.
Plain Language Summary: We conducted this study to better understand people living with long-lasting pain in the face or mouth who had not improved after earlier treatment. We wanted to identify the types of pain they experienced, what other health problems they reported, and how the pain affected daily life.
The study included 98 adults examined at Norway’s National Unit for Orofacial Pain. Most participants had experienced pain for many years. Each person was assessed by a multidisciplinary team that provided a diagnosis and treatment plan. Diagnoses were based on the International Classification of Orofacial Pain (ICOP).
The most common diagnosis was primary myofascial orofacial pain, meaning pain originating from the jaw muscles. Around 60% of participants had this condition. About 20% had neuropathic pain caused by nerve injury, while fewer had other types of facial pain.
Many individuals with nerve injury also had jaw muscle pain, suggesting that nerve damage may contribute to the later development of muscle pain. Participants with jaw muscle pain frequently reported headaches, widespread body pain, and arthritis.
Symptoms of anxiety and depression were also common, highlighting how persistent pain can affect both physical and mental health.
These findings suggest that people with long-lasting orofacial pain need early, coordinated, and multidisciplinary care. Treatment should address not only nerve and muscle pain, but also associated health conditions and psychological well-being, with a focus on the whole person rather than isolated symptoms.
Keywords: atypical facial pain, myalgia, temporomandibular disorder, post-traumatic trigeminal neuropathic pain, trigeminal neuralgia, burning mouth syndrome, persistent idiopathic facial pain
Introduction
Orofacial pain (OFP) comprises of a heterogeneous group of chronic pain conditions affecting the face, jaw, and oral cavity.1 These conditions may arise from musculoskeletal, neuropathic, and idiopathic mechanisms and are frequently accompanied by physical and psychological comorbidities.2 As a result, OFP imposes a substantial burden on affected individuals, leading to functional impairment, emotional distress, and diminished quality of life.3 Despite its significant clinical impact, OFP remains frequently underdiagnosed and inconsistently treated in clinical practice.4
A major advancement in the field occurred in 2020 with the introduction of the International Classification of Orofacial Pain (ICOP), which established standardized diagnostic criteria for OFP. ICOP integrates elements from established classification systems, including the International Classification of Headache Disorders (ICHD-3) and Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), with the aim of improving diagnostic consistency across both research and clinical settings.5,6
From a clinical perspective, OFP challenges traditional boundaries between medicine and dentistry, often resulting in fragmented care pathways, diagnostic delays, and suboptimal treatment outcomes.4,7 Gender-related differences and mental health factors further complicate assessment and prognosis.8,9 Although existing literature consistently reports a high prevalence of anxiety, depression, and somatic comorbidities among individuals with OFP, the specific associations between OFP subtypes, psychological distress, and systemic conditions particularly in refractory cases remain insufficiently elucidated.10–12
Despite the introduction of the ICOP as a standardized framework for diagnosing orofacial pain conditions, important gaps in knowledge remain. Overlap between diagnostic categories continues to complicate clinical decision-making where its implementation in routine practice may be limited, as clinicians often require support from an interdisciplinary expert team. The novelty of this study lies in the application of the ICOP, a standardized and internationally recognized diagnostic framework, to a field that has historically been inconsistent and difficult to compare across studies. Furthermore, the study is strengthened by its setting within a national multidisciplinary pain unit, where collaboration among specialists underscores the clinical complexity of these conditions and highlights the substantial psychological and emotional burden experienced by affected patients.
This exploratory study investigated a cohort of patients with refractory OFP referred to a national unit for orofacial pain in Norway that had been investigated by an interdisciplinary specialist team. The primary aim was to characterize the distribution of OFP subtypes and to examine their associations with medical comorbidities, psychological distress, and gender, using ICOP-based diagnoses in conjunction with focus on the comprehensive clinical and psychological assessments.
Methods
Study Design and Presentation of National Unit for Orofacial Pain
This retrospective, questionnaire-based clinical study was conducted at the National Unit for Orofacial Pain (NUOP), Haukeland University Hospital (HUH), Bergen, Norway. The NUOP is a tertiary pain clinic where patients can be referred to after that they have been assessed and treated in the specialist health care system, but pain remain. The referred patients at NUOP answered questionnaires, were clinically examined by an interdisciplinary team with extensive experiences. They received an explanation of why they had pain, diagnoses and a treatment plan. Between 2017 and 2021, a total of 150 patients were evaluated, of these, 110 patients initially consented to participate, and 98 completed all clinical assessments and questionnaires, 65%, and were therefore included in the final analysis (Figure 1). In our study, we reviewed the patients’ medical records and classified them according to ICOP retrospectively, similar to the study by Handa et al13. The final sample comprised 98 consecutive patients among those who provided informed consent. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.14
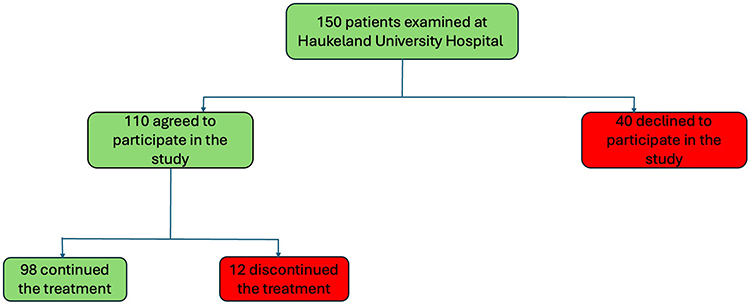 |
Figure 1 Flowchart displaying the number of patients. Of 150 patients assessed, 40 declined participation and 12 were lost to follow-up, leaving 98 in the final sample. |
At NUOP, each patient was evaluated thoroughly by an interdisciplinary team consisting of six specialists, both dental and medical, with more than 10 years of experience in pain medicine: an oral and maxillofacial surgeon, a dental specialist in orofacial pain (OFP), a physician specialized in pain medicine, a clinical specialist psychologist, a physiotherapist specialized in pain medicine, and radiologists specialized in MRI and in CBCT/CT. Prior to the investigation a comprehensive questionnaire was filled in by the patient. The clinical assessments were comprehensive and included anamnesis including pain history, severity of symptoms, duration of symptoms and consequences such as extended periods of sick-leave and disability pension, psychosocial factors, physical functioning, a history of adverse events, previous treatments.15 At the initial consultation orthopantomogram (OPG) and blood tests are taken, and eventually MRI and/or CT/CBCT are taken. The patient is seen on three separate days by dental specialists, radiologists and members of the pain clinic team. At the final consultation a dynamic feedback meeting takes place to present the results and treatment recommendations for the patient and their relatives.
Attrition Analysis
Twelve patients (10 women and 2 men: mean age 41 years) were excluded due to discontinuation of the diagnostic process or incomplete data. Although specific reasons for discontinuation were not systematically recorded, comparative demographic analyses revealed no significant differences between excluded individuals and those included in the final cohort.
Ethics
The research study was approved by the Regional Committees for Medical and Health Research Ethics West, Norway (REK 86004) and by the Department of Clinical Dentistry. All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants for the use of their personal data. The study fully complied with all applicable European Union (EU) and European Economic Area (EEA) General Data Protection Regulation (GDPR) requirements.
Data Collection and Diagnostic Process
All patients underwent a structured interview and standardized clinical examination. The assessments focused on myofascial pain, temporomandibular joint (TMJ) function, (including range of motion), and occlusion. The diagnostic protocol included radiographic imaging to identify structural abnormalities, as well as standardized measures of pain intensity.
To ensure diagnostic accuracy and consistency, the multidisciplinary team conducted consensus meetings in which all clinical findings and imaging results were reviewed. Final diagnoses were assigned based on majority agreement in the team. In this retrospective study all patients were later classified according to the ICOP-2020 criteria.5,15
The following variables were collected and analyzed:
Pain variables: Pain duration and intensity were assessed using the General Pain Intensity (GPI) index and the Numeric Rating Scale (NRS: 0–10).16
Psychometric instruments: Hospital Anxiety and Depression Scale (HADS): Assessment of symptoms of anxiety and depression.17,18
Coping Strategies Questionnaire (CSQ): Evaluation of pain catastrophizing using the validated 2-item version.19
Roland Morris Disability Scale (RMS): Measurement of pain-related physical disability using the 24-item scale.20
Mandibular Function Impairment Questionnaire (MFIQ): Classification of the severity of mandibular functional impairment.21
ICOP-2020 Diagnoses: Diagnoses included Trigeminal Neuralgia (TN),5,22 Primary and Secondary Myofascial Orofacial Pain (MOP),5 Burning Mouth Syndrome (BMS),5,23,24 Persistent idiopathic facial pain (PIFP)5,25 and Post-traumatic trigeminal neuropathic pain (PTTNP).2,5
Statistical Analysis
Descriptive statistics were calculated in Microsoft Excel 2023. Inferential statistical analyses were performed with SPSS software (version 29.0.2.0, IBM Corp). Categorical variables were analyzed using the chi-square test (α = 0.05), with Fisher’s exact test applied when expected cell counts were less than 5. Continuous variables were compared across diagnostic groups using one-way analysis of variance (ANOVA), followed by Tukey’s post hoc test for pairwise comparisons, with statistical significance set at α = 0.05.
Results
Diagnostic Distribution and Overlap
A total of 98 patients with OFP were included in the study. Diagnostic overlap was identified in 25 patients (25.5%). Of these, 23 patients presented with myalgia classified as secondary myofascial orofacial pain (sMOP) in addition to a primary diagnosis, including persistent idiopathic facial pain (PIFP), post-traumatic trigeminal neuropathic pain (PTTNP), or trigeminal neuralgia (TN). Additionally, two patients received overlapping primary diagnoses: one with concomitant PIFP and PTTNP, and another with PIFP and burning mouth syndrome (BMS) (Table 1).
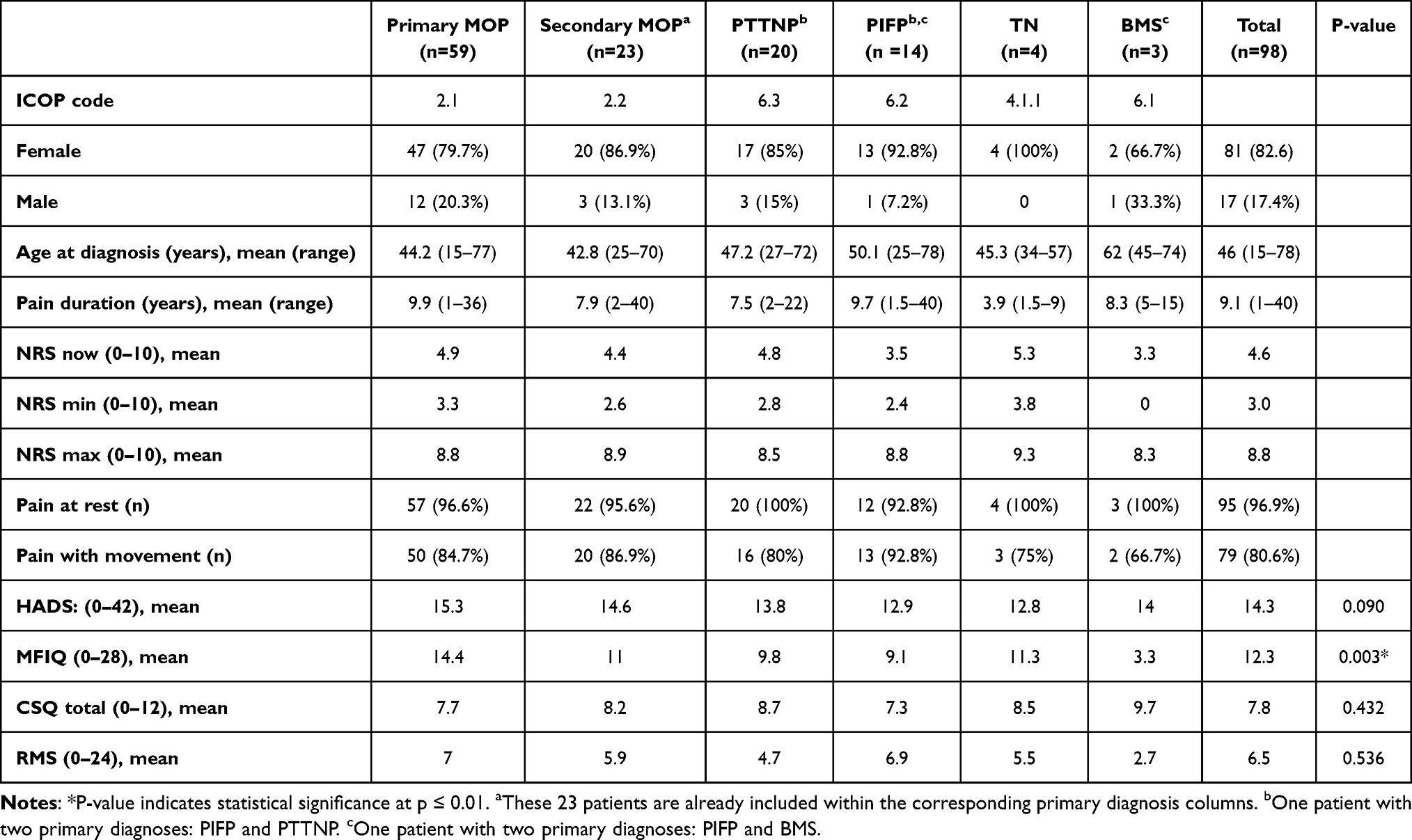 |
Table 1 Demographic Characteristics |
According to the ICOP-2020 classification, 60.2% of patients met the diagnostic criteria for primary myofascial orofacial pain (pMOP), followed by PTTNP (20.4%), PIFP (14.3%), TN (4.1%), and BMS (3.1%). Because two patients received more than one primary diagnosis, the cumulative percentages exceed 100% (Figure 2).
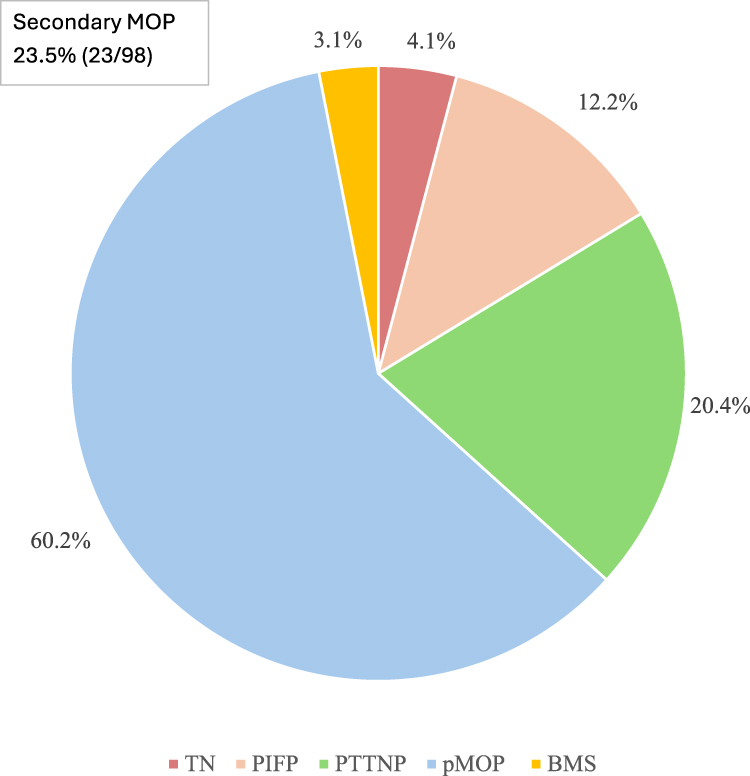 |
Figure 2 The call-out box indicates that 23 patients (23.5%) also met criteria for secondary myofascial orofacial pain (sMOP) in addition to their primary diagnosis. |
Associations and Comorbidities
A statistically significant diagnostic overlap was observed between neuropathic injury and secondary muscle pain, as 75% of patients diagnosed with PTTNP also fulfilled the criteria for sMOP (p < 0.01) (Table 2). Secondary MOP arises when a patient develops muscle tenderness in response to underlying neuropathic pain. In contrast, primary myalgia represents a classic painful temporomandibular disorder (pTMD), in which the pain originates directly from the masticatory muscles. In contrast, no significant association was found between PIFP and myofascial orofacial pain (Table 2).
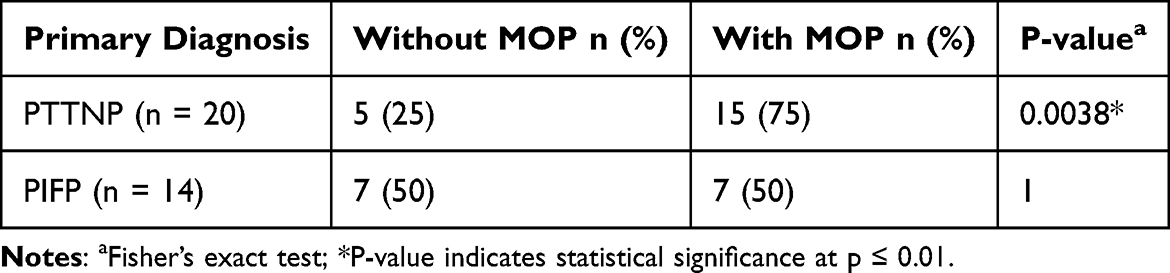 |
Table 2 Association Between Primary Diagnosis and sMOP |
Analysis of comorbidities across diagnostic groups demonstrated that patients with pMOP exhibited a significantly higher burden of systemic conditions compared with non-pMOP groups (Table 3). Specifically, these patients reported higher prevalences of widespread body pain (p = 0.018), headache disorders (p = 0.037), and arthritis (p = 0.025) (Table 3). No statistically significant differences were observed among the primary diagnostic groups with respect to respiratory, cardiovascular, or psychiatric comorbidities (Table 3).
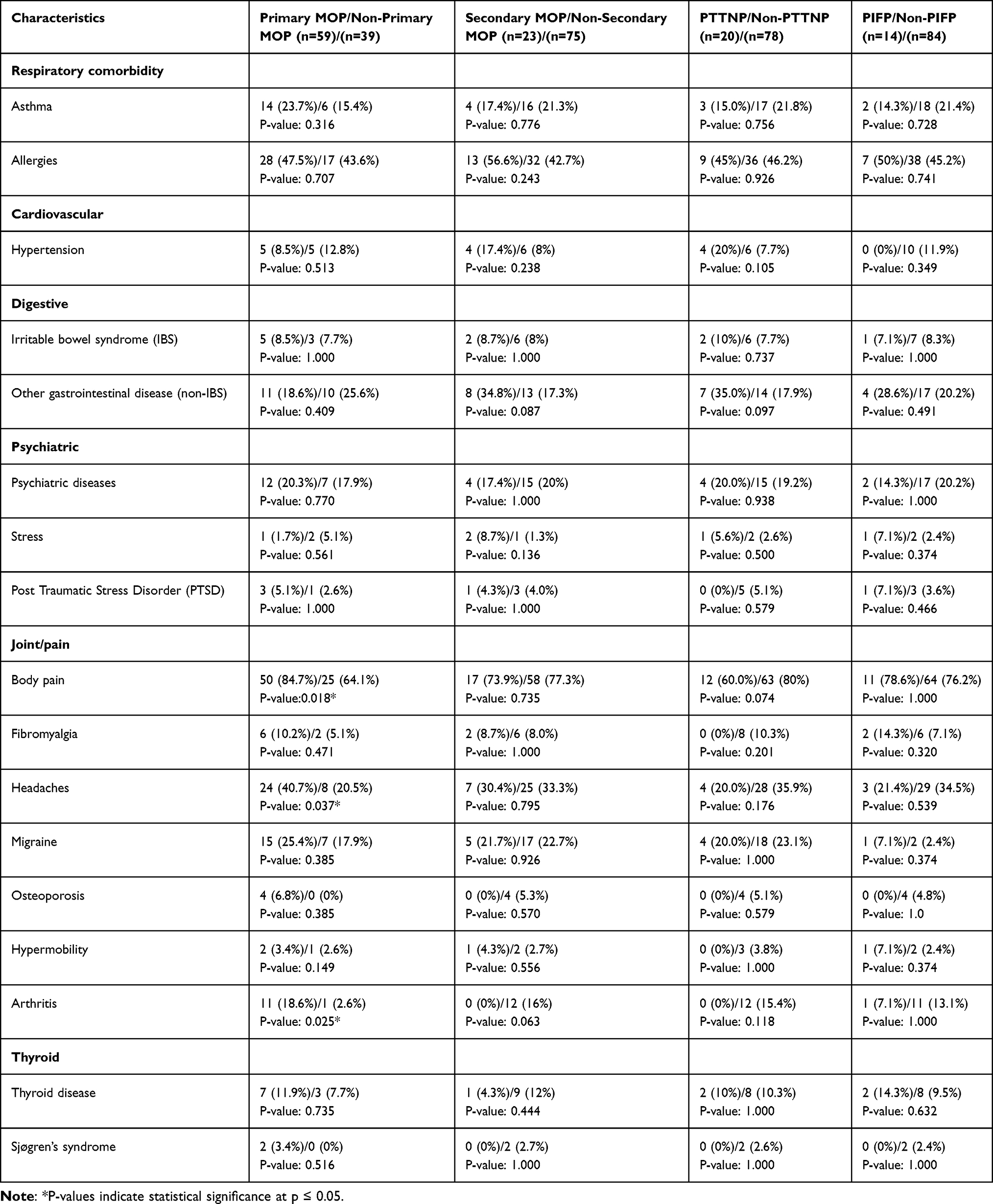 |
Table 3 Systemic Comorbidities |
Discussion
We characterized a cohort of patients investigated in a tertiary specialist orofacial pain clinic using the ICOP-2020 classification framework,5 allowing for direct comparison with international data such as the series by Handa et al13 While Handa et al identified PTTNP and PIFP as the most prevalent diagnoses in their study,13 pMOP dominated our referral-based Norwegian cohort. The transition from “atypical facial pain” to the ICOP-2020 “persistent idiopathic facial pain” (PIFP) represents a pivotal advancement in diagnostic precision.5,25 While “atypical” implies deviation without specificity, PIFP explicitly defines criteria based on temporal persistence, idiopathic nature, and facial localization, which facilitates more targeted clinical management.25
Our findings reveal that pMOP frequently co-occurs with PTTNP, a pattern consistent with the progression from persistent trigeminal nociceptive input to central sensitization with secondary myogenous involvement.2,5 We propose that sustained nociceptive barrage from injured trigeminal fibers induces neuroplastic changes in the spinal trigeminal nucleus, lowering activation thresholds and expanding receptive fields. This heightened central excitability manifests clinically as secondary myofascial pain, as innocuous masticatory muscle activity triggers pain responses. Maladaptive motor strategies, such as protective jaw posturing or nocturnal bruxism, may further exacerbate this musculoskeletal component.2,26 These findings highlight the necessity of early, multidisciplinary interventions that address both neuropathic and musculoskeletal factors.
In contrast, we found no clear association between PIFP and sMOP,27 suggesting a distinct pathophysiological pathway where nerve injury is not the central trigger. Instead, mechanisms such as small-fiber neuropathy (SFN) of A-delta and C-fibers have been proposed for PIFP.27 This is consistent with Handa et al,27 who reported higher rates of dysautonomia in TMD patients and similar findings in BMS where SFN is a recognized underlying factor.28
We observed a significant female predominance (82.6%), aligning with previous epidemiological studies.8,9 Hormonal fluctuations, particularly estrogen, likely influence nociception and may intensify psychological distress during menopause.9,26 Furthermore, pMOP showed a strong association with systemic musculoskeletal conditions, widespread pain, and arthritis.26 The high prevalence of headaches among these patients supports existing literature linking MOP to migraines through shared anatomical pathways, potentially perpetuating a bidirectional pain cycle.29–34
Psychological distress was elevated across all OFP subtypes, mirroring previous findings by Staniszewski et al and Willassen et al35,36 and has also been pointed out by Salinas Fredricson et al37 where sick leave and disability pension were common among TMD patient treated in a hospital setting. Notably, these studies underscore the societal burden for these patients.35,36 Furthermore, the perception of OFP and headache, and are often associated with poor subjective sleep quality, insomnia, and daytime sleepiness contributing to the psychological distress.30–40
Elevated HADS scores41,42 underscore the substantial psychological burden of chronic OFP. Compared with Norwegian population norms (HADS-A ≈ 4–5: HADS-D ≈ 3) our cohort showed higher mean HADS scores. HADS did not differ by sex, indicating that the female predominance reflects epidemiology rather than disproportionate psychological morbidity. Functional impact was most severe in pMOP, as evidenced by MFIQ scores,20,36 while pain intensity peaked in TN patients.21 The long pain duration observed in PIFP highlights the ongoing diagnostic challenges,43 while the high CSQ scores in BMS point to increased pain catastrophizing thinking.44
BMS and PIFP had moderately high scores, consistent with continuous, burning, or dull pain. High CSQ scores in BMS point to increased pain catastrophizing thinking. The unclear etiology behind BMS likely contributes to anxiety and depression thus leading to pain catastrophizing thinking.44 Pain duration also varied where PIFP had the longest mean duration, reflecting diagnostic challenges.43 Long pain duration was associated with greater disability and psychological strain. PTTNP had a shorter duration, but its strong association with MOP suggests musculoskeletal consequences even in moderate chronicity. NRS scores showed that TN patients reported the highest mean pain intensity, reflecting the severe and episodic nature of TN.21
This study has several limitations that should be considered. As a retrospective study, it relies on preexisting medical records and data from clinical examinations and questionnaires, which may lead to variable data quality, recall bias, and missing information. The sample is restricted to patients examined at HUH over a four-year period (2017–2021), potentially limiting the generalizability of the findings to other populations. Additionally, the use of self-reported data from questionnaires may introduce biases related to patient interpretation or incomplete responses. There is also a risk of selection bias, as the included patients may represent a group with more complex cases. The lack of a control group further complicates causal inferences. Furthermore, the uneven distribution of patients across different OFP subgroups and the underrepresentation of men compared to women may skew the results. Lastly, despite the application of standardized ICOP criteria, the interpretation of the results may be influenced by subjectivity.
Conclusion
This study confirms the multifaceted character of orofacial pain (OFP) and the diagnostic utility of the ICOP-2020 criteria in a tertiary clinical setting. The strong link we identified between PTTNP and sMOP underscores the importance of early, multidisciplinary intervention that addresses both neuropathic and musculoskeletal components to prevent central sensitization. Furthermore, the high prevalence of comorbid widespread body pain, headaches, and arthritis in pMOP patients points to shared systemic mechanisms that clinicians must consider during treatment planning.
Elevated psychological distress across all diagnostic groups demonstrates the necessity of embedding mental health support within routine OFP care to address the substantial psychosocial burden identified. Finally, the pronounced female predominance, observed without sex-based differences in anxiety or depression, suggests that while epidemiology is gender linked, the requirement for psychological screening remains universal for all patients. Together, our findings support a personalized, interdisciplinary approach to OFP that can improve diagnostic precision and optimize long-term patient outcomes.
Abbreviations
ICOP, International Classification of Orofacial Pain; HUH, Haukeland University Hospital; NUOP, national unit of orofacial pain; MOP, myofascial orofacial pain; pMOP, primary myofascial orofacial pain; sMOP, secondary myofascial orofacial pain; PTTNP, post-traumatic trigeminal neuropathy pain; TN, trigeminal neuralgia; BMS, burning mouth syndrome; PIFP, persistent idiopathic facial pain; ICHD, International Classification of Headache Disorders; DC/TMD, Diagnostic Criteria for Temporomandibular Disorders; TMJ, temporomandibular joint; NRS, numeric rating scale; GPI, general pain intensity; HADS, hospital anxiety depression scale; HADS-A, Hospital anxiety depression scale part considering anxiety; HADS-D, Hospital anxiety depression scale part considering depression; CSQ, coping strategies questionnaire; RMS, Roland Morris scale; MFIQ, mandibular function impairment; SFN, small fiber neuropathy.
Acknowledgments
A special note of appreciation goes to Professor Stein Atle Lie for his generous help and expertise with SPSS and statistical analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Labanca M, Gianò M, Franco C, Rezzani R. Orofacial pain and dentistry management: guidelines for a more comprehensive evidence-based approach. Diagnostics. 2023;13(17):2854. doi:10.3390/diagnostics13172854
2. Baad-Hansen L, Benoliel R. Neuropathic orofacial pain: facts and fiction. Cephalalgia. 2017;37(7):670–10. doi:10.1177/0333102417706310
3. Shueb SS, Nixdorf DR, John MT, Alonso BF, Durham J. What is the impact of acute and chronic orofacial pain on quality of life? J Dent. 2015;43(10):1203–1210. doi:10.1016/j.jdent.2015.06.001
4. Xiao X, Jiang L, Liu L, Chai G, Luo F. Challenges of misdiagnosis and suboptimal treatment of persistent idiopathic facial pain and atypical odontalgia: a retrospective multi-centric cross-sectional investigation. J Pain Res. 2020;13:2853–2860. doi:10.2147/JPR.S269329
5. International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia. 2020;40(2):129–221. doi:10.1177/0333102419893823
6. Pigg M, Nixdorf DR, Law AS, et al. New international classification of orofacial pain: what is in it for endodontists? J Endod. 2021;47(3):345–357. doi:10.1016/j.joen.2020.12.002
7. Renton T. Refractory orofacial pain: is it the patient or the pain? J Oral Facial Pain Headache. 2021;35(4):317–325. doi:10.11607/ofph.3009
8. Häggman-Henrikson B, Liv P, Ilgunas A, et al. Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain. 2020;161(8):1768–1775. doi:10.1097/j.pain.0000000000001872
9. Casale R, Atzeni F, Bazzichi L, et al. Pain in women: a perspective review on a relevant clinical issue that deserves prioritization. Pain Ther. 2021;10(1):287–314. doi:10.1007/s40122-021-00244-1
10. Giannakopoulos NN, Keller L, Rammelsberg P, Kronmüller KT, Schmitter M. Anxiety and depression in patients with chronic temporomandibular pain and in controls. J Dent. 2010;38(5):369–376. doi:10.1016/j.jdent.2010.01.003
11. Hoffmann RG, Kotchen JM, Kotchen TA, Cowley T, Dasgupta M, Cowley AW. Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. 2011;27(3):268–274. doi:10.1097/AJP.0b013e31820215f5
12. Karamat A, Smith JG, Melek LNF, Renton T. Psychologic impact of chronic orofacial pain: a critical review. J Oral Facial Pain Headache. 2022;36(2):103–140. doi:10.11607/ofph.3010
13. Handa S, Keith DA, Abou-Ezzi J, Rosèn A. Neuropathic orofacial pain: characterization of different patient groups using the ICOP first edition, in a tertiary level Orofacial Pain Clinic. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;132(6):653–661. doi:10.1016/j.oooo.2021.07.021
14. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
15. Berge T, Schjødt B, Bell RF, et al. Assessment of patients with severe temporomandibular disorder in Norway — a multidisciplinary approach. Den Nor Tannlegeforen Tid. 2016;126(9):748–754.
16. Lundeberg T, Lund I, Dahlin L, et al. Reliability and responsiveness of three different pain assessments. J Rehabil Med. 2001;33(6):279–283. doi:10.1080/165019701753236473
17. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
18. Michopoulos I, Douzenis A, Kalkavoura C, et al. Hospital anxiety and depression scale (Hads): validation in a Greek general hospital sample. Ann Gen Psychiatry. 2008;7:4. doi:10.1186/1744-859X-7-4
19. Jensen MP, Keefe FJ, Lefebvre JC, Romano JM, Turner JA. One- and two-item measures of pain beliefs and coping strategies. Pain. 2003;104(3):453–469. doi:10.1016/S0304-3959(03)00076-9
20. Stratford PW, Riddle DL. A roland morris disability questionnaire target value to distinguish between functional and dysfunctional states in people with low back pain. Physiother Can. 2016;68(1):29–35. doi:10.3138/ptc.2014-85
21. Su N, Poon R, Wang C, Darling M, Grushka M. Clinical application of the Mandibular Function Impairment Questionnaire. Oral Surg Oral Med Oral Pathol Oral Radiol. 2022;133(5):e119. doi:10.1016/j.oooo.2021.08.047
22. Cruccu G, Finnerup NB, Jensen TS, et al. Trigeminal neuralgia: new classification and diagnostic grading for practice and research. Neurology. 2016;87(2):220–228. doi:10.1212/WNL.0000000000002840
23. Momin S. Burning mouth syndrome — a frustrating problem. JAMA Otolaryngol Head Neck Surg. 2021;147(6):580. doi:10.1001/jamaoto.2021.0177
24. Wu S, Zhang W, Yan J, Noma N, Young A, Yan Z. Worldwide prevalence estimates of burning mouth syndrome: a systematic review and meta-analysis. Oral Dis. 2022;28(6):1431–1440. doi:10.1111/odi.13868
25. Schweiger V, Nocini R, De Santis D, et al. Persistent Idiopathic Facial Pain (PIFP) in patients referred to a multidisciplinary centre in Italy: a retrospective observational study. J Clin Med. 2022;11(13):3821. doi:10.3390/jcm11133821
26. LeResche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med. 1997;8(3):291–305. doi:10.1177/10454411970080030401
27. Handa S, Heffernan MR, Tan S, Keith DA, Rosén A, Cheng HT. Correlation between orofacial pain and sensory and autonomic neuropathies. J Pain Res. 2024;17:3287–3295. doi:10.2147/JPR.S475528
28. Kouri M, Adamo D, Vardas E, et al. Small fiber neuropathy in burning mouth syndrome: a systematic review. Int J Mol Sci. 2024;25(21):11442. doi:10.3390/ijms252111442
29. Ballegaard V, Thede-Schmidt-Hansen P, Svensson P, Jensen R. Are headache and temporomandibular disorders related? A blinded study. Cephalalgia. 2008;28(8):832–841. doi:10.1111/j.1468-2982.2008.01597.x
30. International Association of Headache Disorders. ICHD-3: the International Clas- sification of Headache Disorders, 3rd edition. 2020. Available from: https://ichd-3.org/.
31. Di Paolo C, D’Urso A, Papi P, et al. Temporomandibular disorders and headache: a retrospective analysis of 1198 patients. Pain Res Manag. 2017;2017:3203027. doi:10.1155/2017/3203027
32. Yakkaphan P, Elias LA, Ravindranath P, et al. Is painful temporomandibular disorder a real headache for many patients? Br Dent J. 2024;236:475–482. doi:10.1038/s41415-024-7178-1
33. Abouelhuda AM, Kim HS, Kim SY, Kim YK. Association between headache and temporomandibular disorder. J Korean Assoc Oral Maxillofac Surg. 2017;43(6):363–367. doi:10.5125/jkaoms.2017.43.6.363
34. Byun SH, Min C, Yoo DM, Yang BE, Choi HG. Increased risk of migraine in patients with temporomandibular disorder: a longitudinal follow-up study using a national health screening cohort. Diagnostics. 2020;10(9):724. doi:10.3390/diagnostics10090724
35. Staniszewski K, Lygre H, Bifulco E, et al. Temporomandibular disorders related to stress and HPA-axis regulation. Pain Res Manag. 2018;2018:7020751. doi:10.1155/2018/7020751
36. Willassen L, Johansson AA, Kvinnsland S, Staniszewski K, Berge T, Rosén A. Catastrophizing has a better prediction for TMD than other psychometric and experimental pain variables. Pain Res Manag. 2020;2020:7893023. doi:10.1155/2020/7893023
37. Salinas Fredricson A, Krüger Weiner C, Adami J, et al. Sick leave and disability pension among TMD patients with musculoskeletal diseases, mental and behavioural disorders - a SWEREG-TMD population-based cohort study. BMC Public Health. 2023;23(1):852. doi:10.1186/s12889-023-15815-4
38. Orzeszek S, Martynowicz H, Smardz J, et al. Assessment of sleep quality in patients with orofacial pain and headache complaints: a polysomnographic study. Dent Med Probl. 2024;61(4):549–562. doi:10.17219/dmp/177008
39. Orzeszek S, Martynowicz H, Smardz J, et al. Assessment of the relationship between sleep bruxism, reported pain and headache, selected health factors, and general health conditions among temporomandibular disorder patients: a preliminary report. Dent Med Probl. 2025;62(2):393–399. doi:10.17219/dmp/192824
40. Orzeszek S, Martynowicz H, Smardz J, et al. Relationship between pain, quality of sleep, sleep bruxism and patients’ personality among individuals with reported orofacial pain. Sci Rep. 2025;15(1):25009. doi:10.1038/s41598-025-09978-w
41. Stordal E, Bjartveit Krüger M, Dahl NH, Krüger Ø, Mykletun A, Dahl AA. Depression in relation to age and gender in the general population: the Nord-Trøndelag Health Study (HUNT). Acta Psychiatr Scand. 2001;104(3):210–216. doi:10.1034/j.1600-0447.2001.00130.x
42. Grønli OK, Bramness JG, Wynn R, Høye A. Depressive symptoms in the general population: the 7th Tromsø Study. J Affect Disord Rep. 2022;8:100322. doi:10.1016/j.jadr.2022.100322
43. Zakrzewska JM. Differential diagnosis of facial pain and guidelines for management. Br J Anaesth. 2013;111(1):95–104. doi:10.1093/bja/aet125
44. Pereira JV, Normando AGC, Rodrigues-Fernandes CI, Rivera C, Santos-Silva AR, Lopes MA. The impact on quality of life in patients with burning mouth syndrome: a systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;131(2):186–194. doi:10.1016/j.oooo.2020.11.019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.