")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Oral Isotretinoin and Its Uses in Dermatology: A Review
Authors Paichitrojjana A , Paichitrojjana A
Received 25 June 2023
Accepted for publication 20 August 2023
Published 25 August 2023 Volume 2023:17 Pages 2573—2591
DOI https://doi.org/10.2147/DDDT.S427530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Anon Paichitrojjana,1 Anand Paichitrojjana2
1School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, Bangkok, Thailand; 2Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Anon Paichitrojjana, School of Anti-Aging and Regenerative Medicine, Mae Fah Luang University, 36/87-88 PS Tower 25Fl, Asoke Road, Sukhumvit 21, Klong Toey Nua, Wattana, Bangkok, 10110, Thailand, Tel +66-81-9343050, Email [email protected]
Abstract: In 1982, the Food and Drug Administration (FDA) of the United States of America approved isotretinoin (13-cis-retinoic acid), a retinoid derivative of vitamin A, to treat severe recalcitrant acne vulgaris. Apart from its prescribed use for severe acne, evidence suggests that isotretinoin is commonly used off-label to treat mild-to-moderate acne, inflammatory skin conditions, genodermatoses, skin cancer, and other skin disorders. This is due to its anti-inflammatory, immunomodulatory, and antineoplastic properties. Some “off-label” use is successful, while others are ineffective. Therefore, this information is essential to clinicians for deciding on the appropriate use of isotretinoin. In this article, we aim to review the most updated evidence-based data about the use of oral isotretinoin in dermatology.
Keywords: isotretinoin, acne vulgaris, rosacea, skin cancer, dermatology
Introduction
Isotretinoin (13-cis-retinoic acid) is a retinoid derivative of vitamin A approved by the FDA of the United States and Europe (excluding Sweden) in 1982 and 1983, respectively. Its primary use is for treating severe recalcitrant cases of acne vulgaris.1,2
Isotretinoin is a highly effective acne treatment. It works by reducing the size of sebaceous glands, lowering sebum excretion, regulating cell proliferation, and decreasing keratinization. Isotretinoin can alter the microenvironment of the follicles, resulting in a decrease in the number of Cutibacterium acnes.3,4 Additionally, it possesses anti-inflammatory and immunomodulatory properties by reducing monocyte TLR-2 expression, minimizing the inflammatory cytokine response, and antineoplastic properties, making it a valuable treatment option for various skin diseases.5,6
According to data, a lot of isotretinoin is being utilized off-label to treat mild-to-moderate acne, inflammatory skin diseases, genodermatoses, skin cancer, and other skin disorders.7–9 Some “off-label” use is successful, while others are ineffective. Therefore, this information is essential to clinicians for deciding on the appropriate use of isotretinoin. This review aims to review the most updated evidence-based data about the use of oral isotretinoin in dermatology.
Use of Oral Isotretinoin in Acne
Although isotretinoin is labeled by FDA only for treating severe recalcitrant acne, there is a consensus among the expert’s opinion that patients with less severe acne who do not respond to conventional therapy and patients with scarring acne that causes severe psychologic distress may also be good candidates for this drug.10
Prognostic factors which should be considered for the early use of isotretinoin include a family history of severe acne, early onset of acne, hyper seborrhea, truncal acne, scarring acne, psychosocial problems, and persistent acne.11
The conventional dosage of isotretinoin is 0.5 to 1 mg/kg/day in two divided doses with a standard cumulative dosage of 120 to 150 mg/kg/course. Managing patients with acne can vary based on different guidelines and consensus. The recommended daily dosage ranges from 0.3 to 0.5 mg/kg in European guidelines, while US guidelines suggest up to 1 mg/kg. However, only the European guidelines recommend a minimum treatment duration of six months.12
Isotretinoin treatment should begin with a dose of 0.5 mg/kg; if the patient is well tolerated, increase the amount to 1/mg/kg, but if side effects cannot be taken, low dose or intermittent therapy can be used.13 The duration of therapy is about four to six months, depending on the daily dose that can be adjusted by clinical response and the side effects. Treatment discontinuation should be considered when the clinical severity score of acne has improved more than 90% compared to the beginning of treatment for one to two months.3
Clinical data suggest that the long-term cure rate after a course of isotretinoin may be lower than reported, especially in younger patients who have a chance to relapse more than older ones.3,14,15 A course of isotretinoin therapy can completely clear acne in 61% of patients, 39% relapsed within the first 18 months after treatment, and 23% required an additional course of isotretinoin.14 A study that followed 299 patients for five years after treatment revealed that 17% required two courses, 5% required three, and 1% required four to five courses of treatment. Contributing factors for more than one course of isotretinoin therapy included lower dose treatment regimens, severe acne, female over 25, and long history of acne.16
Despite the reports of relapses, this conventional regimen is still highly effective while at the same time causing several dose-related side effects. Therefore, micro-dose, mini-dose, low-dose, and intermittent treatment regimens with better tolerance and lower incidence of adverse effects have been introduced.12,17–25
Although low-dose isotretinoin regimens are not yet the standard of care, several studies have reported their usage. However, due to the heterogeneity of these studies, there are no definitive criteria for determining the appropriate dosage of low-dose isotretinoin. Palmer defined micro-dose as continuous treatment with a single 20 mg isotretinoin tablet, taken once or twice weekly (0.04–0.11 mg/kg/day).24 Amichai similarly used a mini-dose regimen by treating patients with 20 mg of isotretinoin weekly.25 Strauss classified three different dosing levels of isotretinoin into low-daily dose (0.1 mg/kg/day), intermediate-daily dose (0.5 mg/kg/day), and high-daily dose (1 mg/kg/day).26 Al Muqarrab described a low-daily dose regimen as a short course of 0.1–0.3 mg/kg/day and the pulsed dose regimen as the intermittent use of isotretinoin (every other day low dose or monthly low dose pulses).27
A systemic review and meta-analysis of ten randomized controlled trials (RCTs) involving 809 patients with acne vulgaris that compared low-daily doses with a conventional dose showed an overall favorable benefit of conventional dose (SMD 0.35, 95% CI - 0.29–0.99, p = 0.28) with a better effect on preventing relapse (OR 1.63, 95% CI 0.51–5.21, p = 0.02).26
Contrarily, a systemic review of fifteen studies, comprising 3 prospective, 2 retrospective, 8 RCTs, and 2 articles with unspecified details, has confirmed that daily dosages ranging from 0.1 to 0.3 mg/kg can be recommended as a viable option for the treatment of acne vulgaris, considering their minimal side effects and cost-effectiveness, albeit with a higher probability of relapse. For greater effectiveness, oral isotretinoin should be combined with topical medications such as tretinoin, adapalene, and clindamycin.28
Other literature reviews demonstrated that the efficacy and relapse rates of low-dose regimen in mild-to-moderate grades of acne are comparable with the conventional regimen (1 mg/kg/day), which is given in the severe grade of acne vulgaris.21,29,30 An RCT revealed that the conventional (0.5–0.7mg/kg/day) and low-dose (0.25–0.4mg/kg/day) regimens have similar efficacy, while intermittent treatment (0.5–0.7mg/kg/day for one week out of every four weeks) had less effective than conventional or low-dose regimens.31
Different results could be from different study methodologies and the heterogeneity of the study groups. Further RCTs with adequate sample sizes, longer follow-up periods, and analysis outcomes regarding the cumulative dose rather than the daily dose of isotretinoin in mild-to-moderate acne patients are required.27 While there is still no definitive conclusion on the effectiveness of low-dose isotretinoin therapy for mild-to-moderate acne vulgaris, extensive evidence suggests that a low-dose regimen over a longer period of time has shown more significant outcomes and long-term remission, highlighting the need for higher cumulative doses.21,27,30
In addition to conventional-dose and low-dose regimens, high-dose regimens and regimens that adjust treatment according to the patient’s response have also been proposed. A prospective, observational intervention study in 80 patients with nodulocystic acne treated with high-dose isotretinoin with a mean daily dose of 1.6 mg/kg for an average of 178 days (cumulative dose 290 mg/kg) showed all patients were resolved from acne upon completion of treatment. During the three-year follow-up period, only ten patients (12.5%) developed a relapse that required an additional course of isotretinoin.32
Coincided by another study that included 116 acne patients in the 12-month follow-up survey indicated that the relapse rate was 47.4% in the lower-dose treatment group (accumulative dose <220 mg/kg) compared with 26.9% in the high-dose group (accumulative dose ≥220 mg/kg) (P = 0.03). Although almost 100% of the patients in both groups developed cheilitis and xerosis during treatment, this study suggests that significantly higher doses of isotretinoin are effective for treating acne and decreasing relapse rates.33
Adjusting treatment according to the patient’s response regimens was studied in 132 patients. Every patient was treated with isotretinoin 0.75 mg/kg/day until all active inflammatory lesions were cured, followed by a maintenance dose of 20 mg/day for one more month. Treatment was continued for 6.6 ± 2.5 months with a cumulative dose of 111.5 + 33.9 mg/kg. The mean final improvement rate was 96.7% (95% CI, 84.9% to 108.5%). Only 18.35% of the patients experienced relapse after a mean interval of 1.28 years.34
Isotretinoin is poor water solubility that limits oral bioavailability and requires a high-fat (50gm fat) and high-calorie (800–1000 calories) meal for better absorption.35 The bioavailability of isotretinoin increased 1.5 to 2 times more significantly when the dose was administered 1 hour before, concomitantly with, or 1 hour after a meal than when it was taken during a complete fast.36 This recommendation cannot be followed in many patients, which may result in poor treatment efficacy.
Two new formulations of isotretinoin can increase gastrointestinal absorption by a lipid-based drug delivery system resembling a fatty meal (Lidose-isotretinoin) and accelerating dissolution by particle micronization (Micronized-isotretinoin).37 When taken with food, Micronized-isotretinoin 32 mg and Lidose-isotretinoin 40 mg have the same bioequivalence. However, when taken in a fasted state, Micronized-isotretinoin 32 mg is absorbed at approximately twice the rate of Lidose-isotretinoin 40 mg.38 A randomized, multicenter, double-blind study in 600 patients with severe recalcitrant nodular acne demonstrated that once-daily use of the Micronized isotretinoin (0.4mg/kg/day) under fasted conditions is clinically comparable to the conventional dose isotretinoin (1mg/kg/day) under fed conditions.39 New formulations enhanced the absorption and bioavailability of isotretinoin with food independence helping patients achieve optimal cumulative dosing that reduces acne lesions and relapse rates.40
While there may be variations in the guidelines and consensus regarding the treatment of acne patients,12 the accumulative dose over the entire course of treatment was found to be a significant factor in preventing relapse.41,42 According to a study on the factors that contribute to relapse after undergoing oral isotretinoin treatment (dosage of 0.3–1 mg/kg/day for a minimum of four months), it was discovered that the relapse rate stands at 37.3%. Patients who are younger than 20 years old, have macrocomedone-type acne or have remaining lesions after treatment are more likely to experience a relapse. The median time for relapse is ten months.43
Evidence from RCTs of isotretinoin in acne treatment is summarized in Table 1.
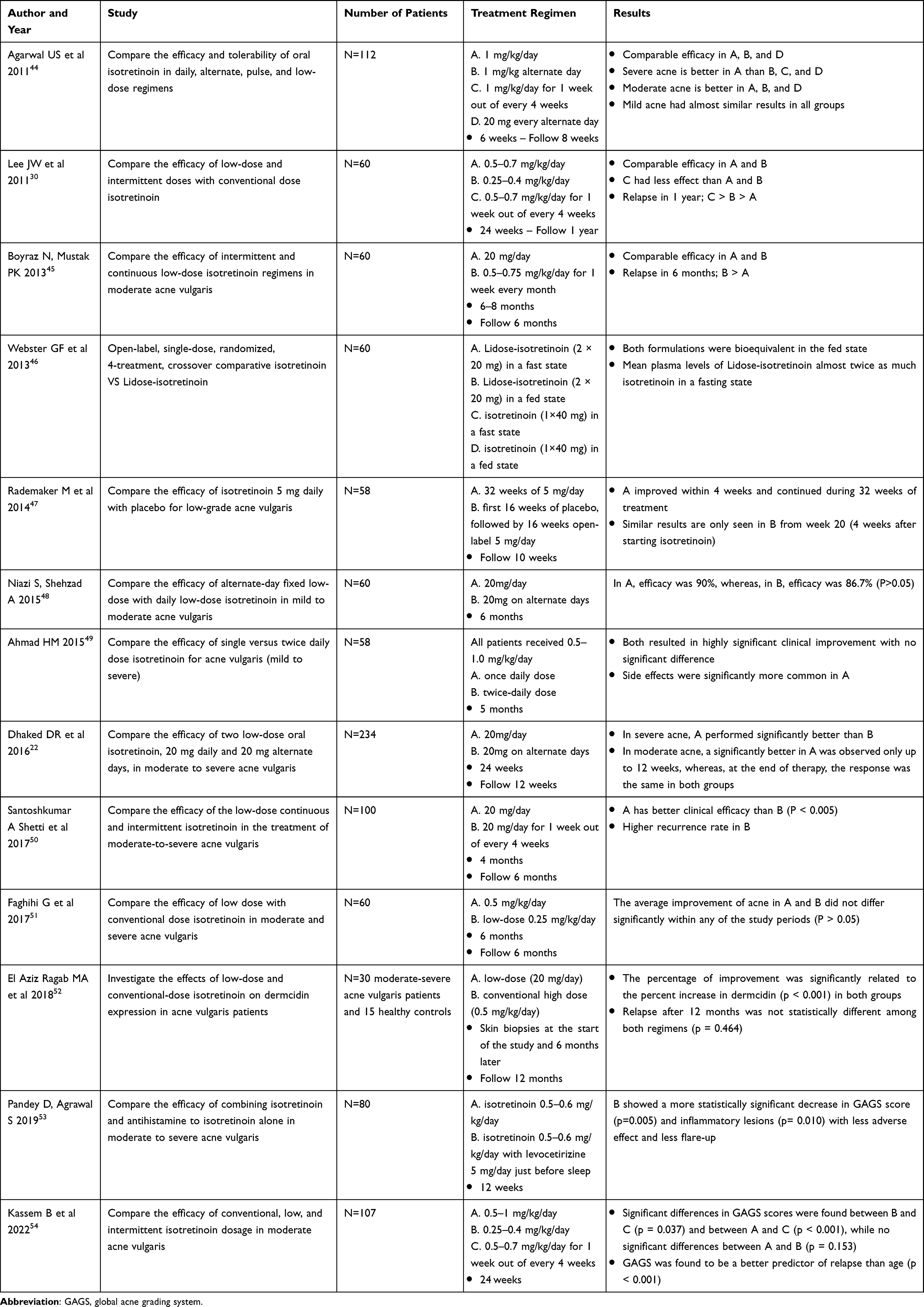 |
Table 1 Oral Isotretinoin and Its Uses in Acne |
Use of Oral Isotretinoin in Inflammatory Skin Diseases
Rosacea
Rosacea is a chronic inflammatory skin disease characterized by recurrent flushing, persistent erythema, papules, pustules, and telangiectasia on facial skin and eyes. Inflammatory pathways associated with rosacea pathogenesis include immune system dysregulation and neurocutaneous mechanism.55 Isotretinoin can be used in treating rosacea because it reduces sebocyte proliferation, sebum production, inflammation process, and telangiectasia on the skin.3–5,56 Also, isotretinoin modifies the skin microenvironment and changes the density of Demodex folliculorum, which is associated with rosacea.57 A review of 15 studies with a total of 991 patients who were treated with isotretinoin for rosacea confirmed its effectiveness. The dosages ranged from 0.22 to 1 mg/kg/day, with 0.3 mg/kg/day being the most effective in achieving complete remission after 12 weeks of therapy.8 Studies proved that isotretinoin is more effective in decreasing rosacea symptoms than placebo, topical tretinoin, doxycycline, and minocycline.58–61 A retrospective study demonstrated that low-dose isotretinoin (40 mg/week) was more effective than minocycline (100 mg/day) for severe rosacea, achieving a complete response in 62.5% of patients after 4–7 months of treatment.61 A study found that patients with mild-to-moderate papulopustular rosacea who were treated with a very low dose of isotretinoin (10–20 mg once to five times a week, equivalent to 5 mg/day) for 57 weeks experienced a 91% clearance of their rosacea.62 However, it was also reported that high relapse rates (45–58.3%) occurred within 11 months after isotretinoin treatment in rosacea.60,63
Recently, patients with Morbihan disease, a rare complication of rosacea that results in an erythematous, edematous plaque on the face, have been reported to experience complete recovery without recurrence when taking oral isotretinoin at a daily dosage of 20–80mg.64
Evidence from RCTs of isotretinoin in rosacea is summarized in Table 2.
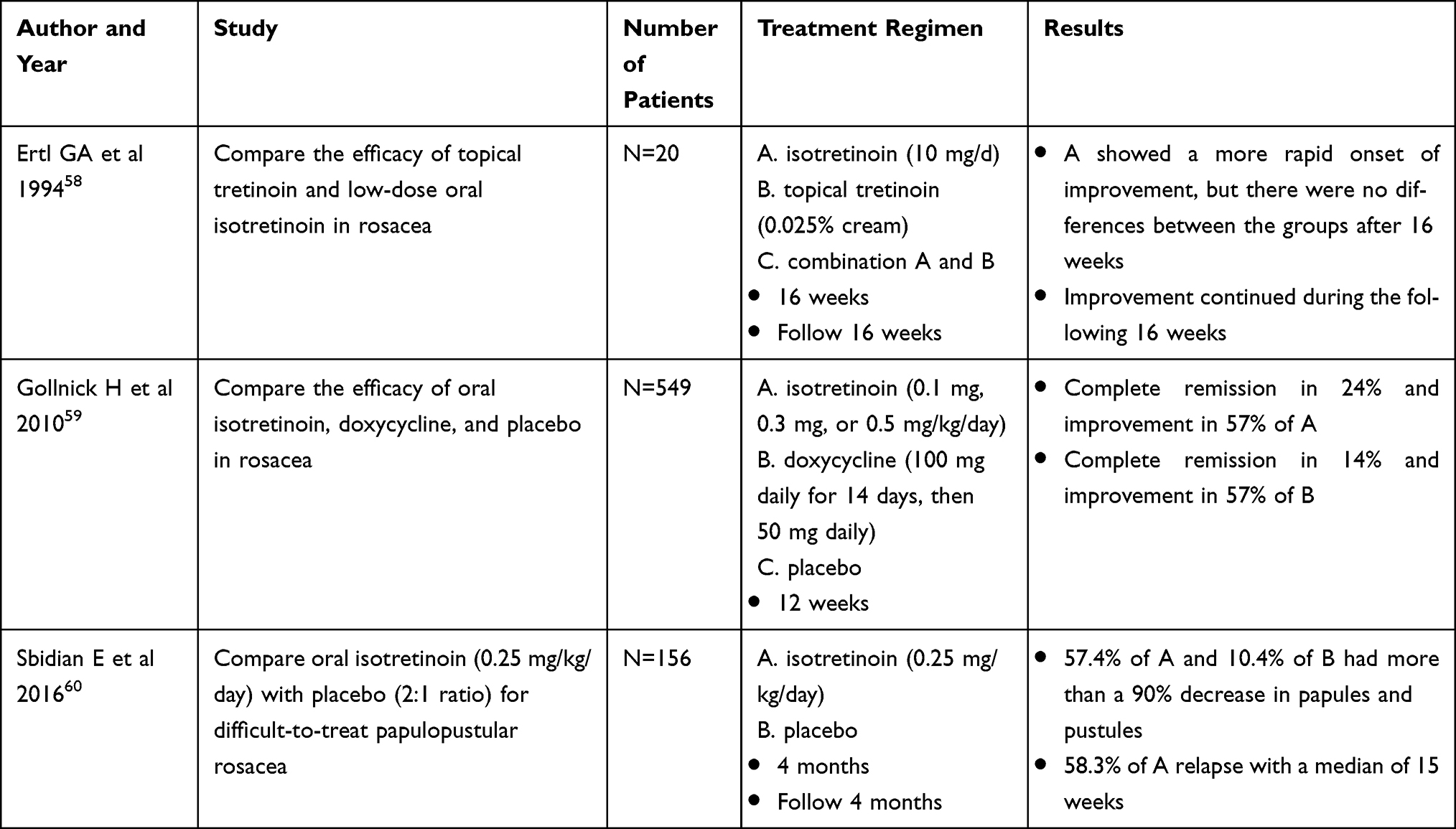 |
Table 2 Oral Isotretinoin and Its Uses in Rosacea |
Hidradenitis Suppurativa (HS)
It has been proposed for a long time that apocrine glands play a significant role in causing HS, but there is a lack of conclusive evidence to support this hypothesis. HS is a chronic inflammatory skin disease of the pilosebaceous unit in intertriginous body areas, such as the axilla and groin, and is characterized by persistent abscesses, comedones, fistulas, scars, and keloids. It is traditionally thought that HS and acne are closely related, and because of this, isotretinoin has also been used in treating HS. There is an assumption that oral isotretinoin effectively treats HS by reducing follicular plugging.65
There have been variable responses of HS to isotretinoin in the literature. Three retrospective studies showed that 15.9–68% of patients had clinical improvement as early as four months, especially female gender, and acne history was associated with a positive response to oral isotretinoin doses ranging from 0.45 mg/kg/day to140mg/day.66–68 A recent retrospective study revealed that 35.9% of patients responded to treatment and had a positive association with pilonidal cyst history but not associated with the patient’s BMI, Hurley stage, or history of acne.69
On the contrary, some patients reported worsening HS by increasing several inflammatory nodules following isotretinoin treatment.67,70 Eight patients with severe acne treated with isotretinoin and subsequently developed HS have been reported.71
However, there is evidence demonstrating that isotretinoin could be used as an effective alternative or adjunctive therapy in early inflammatory lesions of HS.66–68,72
Folliculitis Decalvans (FD)
FD is a chronic neutrophilic inflammation of hair follicles characterized by irregular scarring alopecia, follicular hyperkeratosis, multiple pustules, perifollicular crusts, and tufted hair folliculitis on the scalp. Pathophysiology is unknown but considered an abnormal immune response to Staphylococcus aureus. Isotretinoin plays a role in FD treatment through the direct immunomodulatory effect that can inhibit the migration of neutrophils into the skin.
A total of 89 patients with FD were included in four retrospective studies and two case reports. They were treated with oral isotretinoin for 5–7 months, with doses ranging from 0.1 to 1.02 mg/kg/day. In many cases, the treatment was combined with antibiotics such as clindamycin, cephalexin, minocycline, rifampicin, and dapsone or prednisolone.73–78 Most patients (82–90%) reached a partial or complete response within three months and remained in remission for four months to two years.73,74 In a retrospective study, it was found that oral isotretinoin monotherapy led to complete healing in 82% of patients. Those who took oral isotretinoin at a dosage of ≥0.4 mg/kg/day for more than three months had a better response rate. Of the responders, 66% never experienced a relapse.74 However, an isotretinoin refractory case of FD has been reported after treatment up to 60 mg/day for three months but successfully with biosimilar adalimumab.77
Dissecting Cellulitis (DCS)
DCS is characterized by perifollicular, follicular pustules and nodules that develop into tracts coalescing into chronically inflamed tissue that end up with scarring alopecia. The effectiveness of isotretinoin may be due to its sebaceous gland suppression, anti-inflammatory effect, and normalization of follicular keratinization.79
A review and meta-analysis included five retrospective studies from 2004 to 2018, demonstrating that the overall efficacy of isotretinoin for DCS was estimated to be 0.9 with a 95% CI (0.81–0.97). Most patients improved or completed remission. Recurrence was seen in 24% (6/25) of patients.80 The most successful treatment study used a 0.5–0.8 mg/kg/day dosage with an average treatment duration of 3 months.81 The relapse of DCS is a common finding for those who undergo successful treatment. Retreatment with isotretinoin after relapse is still effective.82 Maintenance therapy with 0.75–1 mg/kg/day has been proposed to prevent the high recurrence rates.83 Similar results have been found in two systematic reviews. The first review from 57 articles, including 90 patients, revealed that approximately 54% of all patients treated with isotretinoin showed significant improvement, but 19% eventually relapsed.84 The second review from 14 studies with 76 patients reported most patients (71.1%) had significant clinical improvement with isotretinoin dosages ranging from 0.27 to 1 mg/kg/day for several months, while 29.9% had no improvement, and relapse was reported in two patients.8 Successful treatment with low-dose isotretinoin (0.25 to 0.5 mg/kg/day) has also been reported in 65 out of 72 (90.3%) patients with DCS.85
Seborrheic Dermatitis (SD)
There are few studies on the treatment of SD with oral isotretinoin. A retrospective study demonstrated that all 48 patients with moderate-to-severe SD treated with either 20 mg or 10 mg daily of oral isotretinoin for 2 to 6 months showed a significant reduction in the symptom scale of seborrheic dermatitis score compared with baseline. Additionally, there was no significant difference between the outcomes of these two groups.86 An RCT compared isotretinoin 10 mg every other day and topical treatment in 45 patients with moderate-to-severe SD revealed that isotretinoin significantly decreased scalp pruritus, sebum production, and increased quality of life than topical treatment.87 Recently, a systematic review showed that isotretinoin treatment is more effective than oral itraconazole, anti-fungal shampoo, or salicylic acid-containing soap in improving SD symptoms, even at low doses. Isotretinoin is a potentially effective treatment for moderate-to-severe SD and is generally well tolerated and safe.88
On the contrary, a retrospective study has revealed that 5 patients who underwent effective isotretinoin therapy for their acne subsequently suffered from seborrheic dermatitis-like skin eruptions.89
Psoriasis
Psoriasis is a chronic inflammatory skin disease classified as plaque, pustular, and erythrodermic. Isotretinoin can modulate abnormal hyperproliferation, differentiation of keratinocytes, and inflammatory cells in psoriasis.8 A prospective cohort study compared the efficacy of isotretinoin (30 mg twice daily) with methotrexate (5 mg thrice weekly) in patients with moderate-to-severe plaque psoriasis for 12 weeks revealed that isotretinoin is effectively less than methotrexate when compared with the mean percentage reduction in PASI score (52.78 ± 7.34 and 70.23 ± 6.78).90 Successful treatment of plaque-type psoriasis with combination therapy between isotretinoin and phototherapy has been reported in two RCTs. The first study compared narrow-band ultraviolet B (NBUVB) + isotretinoin (0.5 mg/kg/day) with the control group receiving NBUVB + placebo demonstrated that isotretinoin + NBUVB could reduce the number of phototherapy sessions and cumulative NBUVB dose.91 The second study showed that combining isotretinoin (0.5 mg/kg/day) with oral psoralen + sun exposure (PUVAsol) is more effective than PUVAsol alone for treating chronic plaque psoriasis.92 A case series documented that five individuals with generalized pustular psoriasis did not respond to conventional therapy but were effectively treated with isotretinoin (1.5–2 mg/kg/day) within a short treatment period.93 A comparative study revealed that even though the efficacy of isotretinoin and etretinate in treating generalized pustular psoriasis was comparable, isotretinoin was less effective than etretinate in treating chronic plaque psoriasis.94
Pityriasis Rubra Pilaris (PRP)
PRP refers to skin conditions characterized by follicular hyperkeratotic papules and reddish-orange scaling patches with well-defined borders. The effectiveness of isotretinoin can be attributed to its ability to normalize keratinization.
According to a review of eleven studies, 122 patients were treated with oral isotretinoin at doses ranging from 0.5 to 4 mg/kg/day. The results showed that most patients (82%) responded well to treatment with 50–90% lesion clearance. These positive outcomes were observed over treatment periods ranging from 1 to 6 months. However, relapse was seen between 4 and 12 weeks after the end of treatment.8 There has been a report of two cases of PRP following the administration of the ChAdOx1 (COVID-19) vaccine were successfully treated with a combination of isotretinoin (20 to 30mg) and emollients for three months, resulting in complete remission.95 Same as a recent case series report revealed the effective use of isotretinoin (10–20 mg/day for 6–12 weeks) in treating two cases of PRP that were initially misdiagnosed as atopic dermatitis.96
Cutaneous Lupus Erythematosus (CLE)
CLE is classified as acute, subacute, and chronic. Isotretinoin can be used by decreasing inflammatory processes and reducing abnormal hyperproliferation of keratinocytes.
A study demonstrated that 86.9% of 24 patients with chronic or subacute CLE treated with isotretinoin 0.15–0.5 mg/kg/day showed improvement or clearing of clinical lesions and histopathology within 16 weeks. Better results were seen in patients with chronic CLE.97 A review of seven studies on isotretinoin monotherapy (10 to 50 mg/day) in 19 patients with CLE showed that 90% of the skin lesions displayed signs of improvement within one to three months.8 Combination therapies isotretinoin (0.5 to 1.5 mg/kg/day) with hydroxychloroquine, prednisone, topical clobetasol propionate, and fluocinonide also showed high efficacy of treatment by all patients showed 90% improvement in only three weeks.98–100
However, it has been reported in a case series of six patients that discontinuing treatment resulted in a rapid recurrence of lesions.99
Lichen Planus (LP)
Isotretinoin may be effective in lichen planus by regulating cellular proliferation and differentiation of keratinocytes.
According to various reports, mucocutaneous LP has shown a positive response to oral isotretinoin at a dosage of 0.25–1 mg/kg/day, with noticeable clinical improvement within two months of treatment.8 However, two reports showed relapse in five patients within two months after discontinuing treatment.101,102 Successful prevention of relapse by oral isotretinoin 20 mg alternate days for another month has been reported.103 A prospective study of the efficacy of fixed low-dose isotretinoin (20 mg/day) for six months in oral and cutaneous lichen planus pigmentosus showed moderate improvement (25–50%) and good improvement (>50%) in 55.7% and 21.8% of the patients, respectively.104
Lichen Planopilaris (LPP)
LPP is an uncommon inflammatory condition characterized by lymphocytic infiltration and fibrosis that can lead to cicatricial alopecia. One form is frontal fibrosing alopecia (FFA), which affects the frontotemporal hairline with facial papules. Isotretinoin may play a role by normalization of follicular keratinocyte antigen expression and reducing inflammatory cellular infiltrate.105
A review, including three retrospective cohort studies and three case series, has shown that oral isotretinoin can effectively treat LPP. Successful outcomes have been observed with dosages ranging from 10 mg every other day to 40 mg/day and treatment durations ranging from 2 to 24 months.8 A comparative study showed no further progression of LPP in 76% of patients and no relapse in 72% after isotretinoin treatment (20mg/day) for 12 months.106 According to an RCT, patients with facial LPP showed greater improvement when taking oral isotretinoin (20 mg/day) than those using topical 0.05% isotretinoin gel.107 Combining Isotretinoin with 5-alpha reductase inhibitors, finasteride, spironolactone, pimecrolimus cream, and vitamins has proven to be highly effective in treating both LPP and FAA.108,109
Granuloma Annulare (GA)
GA is a common inflammatory skin disease that may be caused by a delayed hypersensitivity reaction in the dermis, typified clinically by annular, smooth, purplish papules and plaque. Isotretinoin has a role in GA through its anti-inflammatory effect and altered cellular proliferation.110
Sixteen patients with GA, including generalized, localized, and perforating types, showed 90% clinical improvement after being treated with isotretinoin for three months to 1 year at a dosage of 0.5–1 mg/kg/day.8 However, recurrence occurred in 25% of all patients followed-up after discontinued treatment.111–113
There have been reported cases of resistance to isotretinoin. It is recommended to only use isotretinoin for patients with disseminated or refractory GA.110
Use of Oral Isotretinoin in Skin Cancer
Basal Cell Carcinoma (BCC)
BCC is the most common, locally invasive skin cancer. According to various reports, BCC lesions experienced a 36–50% reduction, partially or completely, after undergoing treatment with oral isotretinoin monotherapy 0.2–8.2 mg/kg/day lasting two months to one year.8 In terms of skin cancer prevention, an RCT involving 981 patients with two or more previous BCC treated with 10 mg/day oral isotretinoin for 36 months showed no differences compared to the placebo in the cumulative percentage of patients with BCC at a new site or the annual rate of BCC formation existed.114 Concurred by another RCT in 525 patients with a history of BCCs and SCCs showed no difference between those who received retinol (25,000 units), isotretinoin (5–10 mg), or the placebo daily for three years in the time to the first occurrence or the total number of BCC or SCC reported.115
Squamous Cell Carcinoma (SCC)
SCC is a common type of invasive skin cancer derived from cells within the epidermis that can metastasize. Oral isotretinoin monotherapy dosages ranging from 0.5 to 3 mg/kg/day are used in many case reports for SCC treatment. Regression in 35.3% of SCC lesions can be observed as soon as two weeks after treatment.8 In a prospective study, thirty-two patients with inoperable SCC were treated with a combination of oral isotretinoin (1 mg/kg/day) and subcutaneous recombinant human IFN alpha-2a (3 million units/day) for at least two months showed a response rate 93% (13 of 14) in patients with advanced local disease (six complete responses), 67% (4 of 6) in patients with the regional disease (no complete responses), and 25% (2 of 8) in patients with distant metastases (one complete response).116 The similar result was observed in another clinical trial, isotretinoin (0.6–1 mg/kg/day) combined with alpha-IFN (6 × 106 I.U./day) for three months in 35 patients with SCC demonstrated a response rate in 41% of cases (13/32 evaluable patients) with five complete and eight partial responses.117
Leukoplakia
Leukoplakia appears as thick, white patches on the oral mucosa and can also be a sign of precancerous lesions in the mouth. An RCT has revealed that isotretinoin at a 2 mg/kg/day dose for three months is significantly more effective than a placebo in treating oral leukoplakia. The treatment resulted in a remarkable reduction in lesion size (67% vs 10%) and histologic dysplasia (54% vs 10%). However, after the treatment ended, relapse was observed in 56% (9 out of 16) of patients within three months.118
A clinical trial shows that low-dose isotretinoin (0.5 mg/kg/day) is more effective than beta-carotene (30 mg per day) in preventing leukoplakia. After nine months, 92% of patients using isotretinoin had stable lesions, while only 45% of patients using beta carotene had the same outcome.119 Recently, a systematic review and meta-analysis study of 8 RCTs conducted from 2008 to 2016 found no significant difference in clinical responses between chemo-preventive agents, like isotretinoin, and placebo for oral leukoplakia prevention.120
Keratoacanthoma (KA)
KA is a rapidly growing destructive skin tumor that clinically may be indistinguishable from well-differentiated SCC. A case report of recurrent KA after surgical excision showed complete clinical resolution confirmed by skin biopsy after being treated with isotretinoin 1 mg/kg/day for 12 weeks.121 According to other reports, five patients with different types of KA (such as multiple KAs, giant KA, and KA centrifugum marginatum) were treated with oral isotretinoin 0.5–6 mg/kg/day and experienced regression as early as two weeks. However, it was common for this condition to recur within 8–12 weeks after the therapy was stopped.122–126 There have been reports of successful use of isotretinoin 0.25 mg/kg/day as a maintenance therapy to prevent new KA.125
Cutaneous T-Cell Lymphoma (CTCL)
CTCL is the most common type of primary cutaneous lymphoma in which malignant T-cells are initially increased in the skin. Isotretinoin may play a role by changing multiple signaling pathways in cellular differentiation and apoptosis.
Studies on oral isotretinoin monotherapy for CTCL have shown that 1–2 mg/kg/day for 2–3 months is the most effective for achieving clinical remission. In combination therapy, a dosage of 1 mg/kg/day for 3–4 months has been found to be the most effective.8 In a clinical trial, isotretinoin and etretinate were compared in treating CTCL. After two months of treatment with isotretinoin at a dosage of 0.2–2 mg/kg/day, complete remission was observed in 21% of patients, while partial remission was in 38%. The study found that isotretinoin and etretinate had the same effectiveness in treating CTCL. However, despite continued therapy, 25% of patients experienced a relapse.127 The combination of isotretinoin (0.5–1.5 mg/kg/day), etretinate, and PUVA therapy showed better results. The treatment led to complete remission in 73% of patients and partial remission in 27%.128 A case study has confirmed the efficacy of using isotretinoin (20mg/day) as part of combination therapy with methotrexate and PUVA for early-stage refractory CTCL.129 Additionally, six patients with advanced refractory folliculotropic mycosis fungoides have been successfully treated with IFN-γ in combination with low-dose oral isotretinoin (10–20mg/day), topical carmustine ointment, and phototherapy.130
Use of Oral Isotretinoin in Genodermatosis
Xeroderma Pigmentosum (XP)
XP is a skin condition sensitive to ultraviolet light, leading to premature aging of the skin and an increased risk of developing skin cancer. Five XP patients were treated with oral isotretinoin at 2 mg/kg/day in a three-year controlled prospective study. The study found a 63% decrease in tumor occurrence during the two years of treatment. However, 60% of patients experienced an 8.5-fold increase in annual tumor occurrence within three months after treatment discontinuation.131
Successful treatment of combination therapy with isotretinoin (1 mg/kg/day) and chemotherapy in two cases of XP by completely resolved SCC without recurrence have been reported.132,133 High-dose oral isotretinoin (2 mg/kg/day) can reduce the number of skin tumors in XP and should only be used in patients with an exceptionally high number of newly developed skin tumors, while some cases may respond to an intermediate dose (1 mg/kg/day) or a lower dose (0.5 mg/kg/day) of oral isotretinoin with fewer adverse effects.134
Ichthyosis
Ichthyosis is a genetic skin disorder that can cause dry, itchy, scaly, rough, and red skin. Symptoms can vary in intensity. A multicenter clinical trial demonstrated that almost all patients with lamellar ichthyosis and epidermolytic hyperkeratosis could be improved with oral isotretinoin (mean dosage 2mg/kg/day). More significant improvement was seen in the group of patients with lamellar ichthyosis.135 A case report revealed that isotretinoin treatment from day 7 of life could increase survival in a patient with harlequin ichthyosis.136 The beneficial effects of isotretinoin in ichthyosis are dose-dependent. The mean dosing from the studies was 1.8 to 2.1 mg/kg/day, given the cutaneous and extracutaneous toxicities. A lower dose of 0.5–1 mg/kg/day is recommended for maximal clearing and maintenance with minimal side effects.137
Darier’s Disease (DD)
DD is an autosomal dominant genetic disorder with scaly crusted papules in a seborrheic distribution and skin folds. Isotretinoin may be efficacious by reducing abnormal proliferation and differentiation of the keratinocyte.
In eight studies involving 119 patients who used oral isotretinoin at doses of 0.5 to 4 mg/kg/day, it was observed that there was a significant improvement in lesions, ranging from 75% to 100%, within 4 weeks to 3 months. However, every patient who was followed up reported a relapse of lesions, ranging from 80% to 100%, within seven days to 6 months after stopping treatment.8 A comprehensive review of the therapeutic option for DD from 113 studies identified grade B evidence quality support for isotretinoin and suggested that taking isotretinoin continuously on maintenance dosing may be necessary to prevent a recurrence.138
Use of Oral Isotretinoin in Cutaneous HPV Infections
Wart
Oral isotretinoin can be used in cutaneous HPV infections from the immunomodulatory effect inducing apoptosis, down-regulating HPV transcription in affected keratinocytes, and affecting epithelial differentiation and proliferation.139
There has been a first report about an immunosuppressed patient who had developed persistent warts on their hands and feet after undergoing chemotherapy and showed clinical improvement after a 28-week treatment with oral isotretinoin at 1 mg/kg/day.140 Complete remission was reported in fourteen patients with recalcitrant warts by combining low-dose isotretinoin (0.1–0.2 mg/kg/day) and topical therapy for 3 months with no sign of relapse for up to 3 years.141 The successful treatment of extensive and recalcitrant warts in an immunocompetent patient using isotretinoin monotherapy at 1mg/kg/day for six weeks has been reported. The patient remained in complete remission for 23 months with no signs of relapse.139 An RCT demonstrated a statistically significant difference in the therapeutic response between the isotretinoin and the placebo groups, with complete clearance in 60% and 0% of the patients, respectively.142 A systematic review and meta-analysis revealed that combinations of systemic isotretinoin with intralesional immunotherapy yield higher complete clearance rates with lower recurrence.143 Different results were found in a comparative study that showed no statistically significant difference between the combination of intralesional purified protein derivative (PPD) with a low dose isotretinoin and PPD alone regarding the therapeutic response.144
Flat Wart
Several patients have reported positive outcomes from treatment with oral isotretinoin in the range of 0.1 to 0.5 mg/kg/day for flat warts.8 According to three RCTs, isotretinoin has proven to be effective. In one study,16 patients treated with 30 mg/day of isotretinoin showed complete clearance of all recalcitrant flat warts within 12 weeks, while there was no improvement in the placebo group.145 In the second study, patients who received a daily dose of oral isotretinoin at 0.5 mg/kg showed complete remission in 69% of cases. In contrast, only 38% of patients treated with topical isotretinoin 0.05% showed the same results after three months.146 The third study found that 44.4% of patients in the oral isotretinoin alone group (0.3 mg/kg/day) experienced complete clearance of flat warts, compared to 38.8% in the combination therapy with the Candida antigen group.147
Condyloma Acuminata
Several studies reported favorable outcomes from isotretinoin treatment (0.5–1 mg/kg/day) in patients with condyloma acuminata that resist conventional therapy. High-dose oral isotretinoin (0.6 mg/kg/day) is more effective than low-dose (0.3 mg/kg/day) in treating cutaneous and genital warts, with 76% of patients achieving complete clearance compared to 46%.148 Isotretinoin provides significantly better results than a placebo, and combination therapy was superior to isotretinoin monotherapy.8 An average of 96% of patients treated with isotretinoin combined with IFN alfa-nl or IFN alfa-2a exhibited complete remission compared to 61.72% of those treated with isotretinoin monotherapy. Additionally, combination therapy decreased the treatment duration and the recurrence rate in this group of patients.149–153
Evidence from RCTs of isotretinoin in condyloma acuminata treatment is summarized in Table 3.
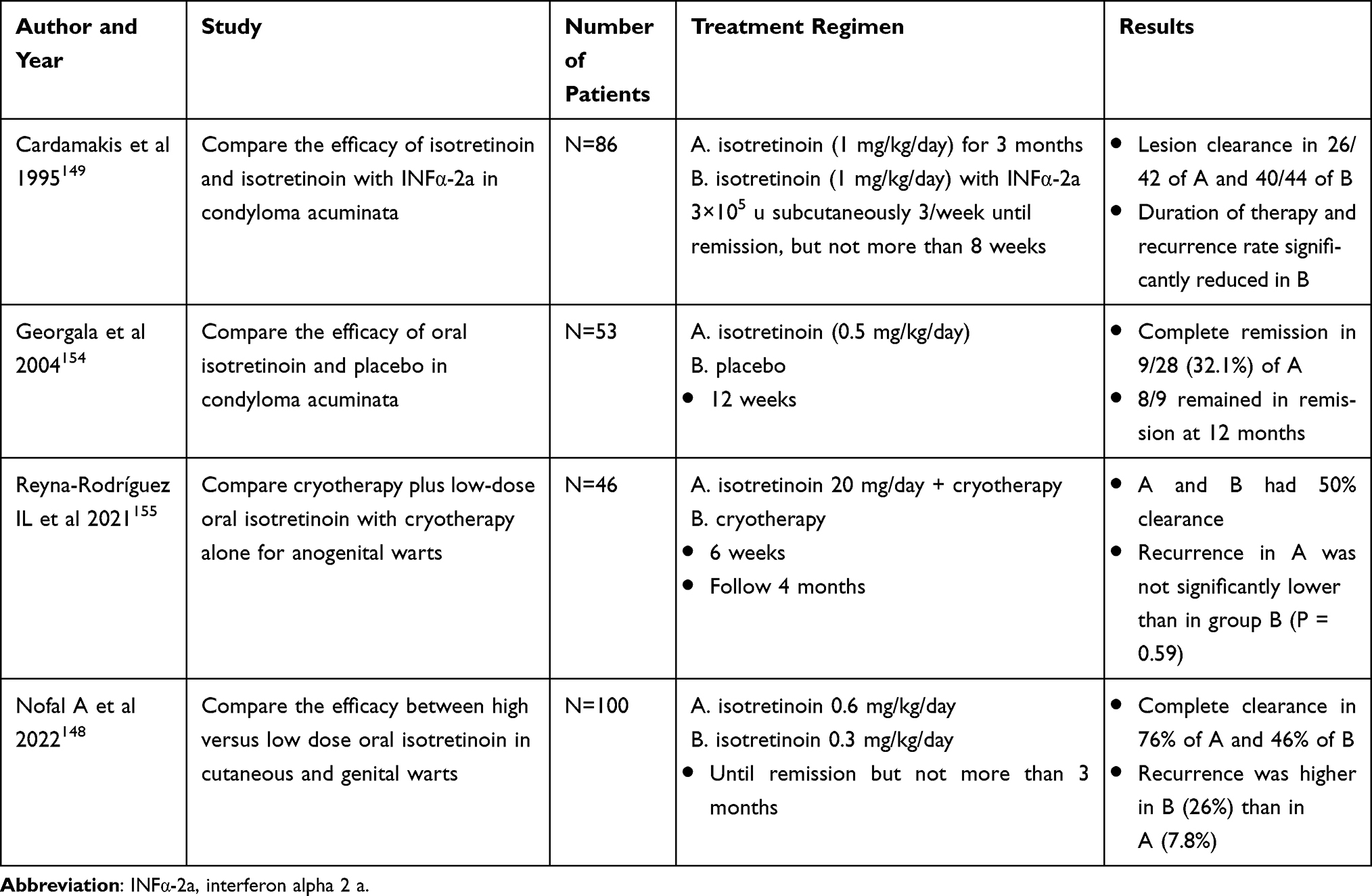 |
Table 3 Oral Isotretinoin and Its Uses in Condyloma Acuminata |
Use of Oral Isotretinoin in Aesthetic Dermatology
Photoaging Skin
The most widely used treatments for photoaging skin are topical products, and evidence on the benefits of oral isotretinoin is still debated. The outcomes of aging skin following treatment with systemic isotretinoin remain mixed. Two RCTs demonstrated that 20 mg of isotretinoin daily does not significantly improve photoaging skin compared to topical retinoic acid or moisturizer/sunscreen by clinical, histology, and quality of life scores.156,157 Another two studies demonstrated a statistically significant increase in collagen fibers and overall skin improvement (wrinkle, skin texture, and coloration) in the treatment group with either 10 or 20 mg isotretinoin thrice weekly for three months.158,159 A literature review from 6 studies involving 251 patients summarized that isotretinoin might be useful in treating photoaging, but there is currently insufficient evidence to support its use when weighing the potential risks.160
Evidence from RCTs of isotretinoin in photoaging treatment is summarized in Table 4.
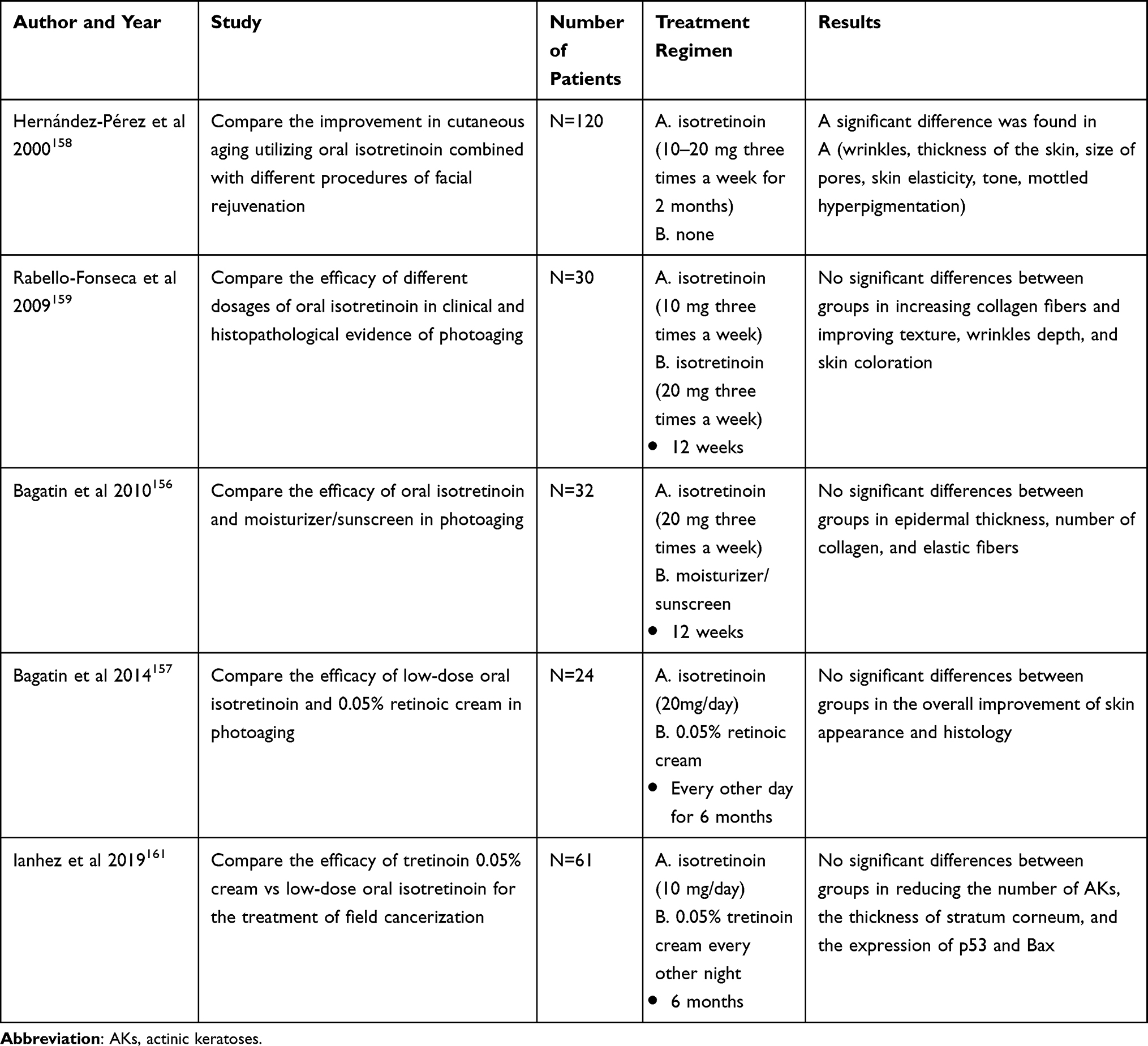 |
Table 4 Oral Isotretinoin and Its Uses in Photoaging |
Sebaceous Hyperplasia (SGH)
SGH is characterized by enlarged sebaceous glands on the forehead or cheeks of middle-aged and older people causing unsightly and bothersome. Isotretinoin can reduce sebaceous gland size and inhibit sebum production.
According to one prospective study and eight case reports, it is possible to achieve complete or near-complete clearance of SGH by taking oral isotretinoin at a dosage of 0.14 to 1 mg/kg/day within 1 to 12 weeks.8 However, prior studies showed a high relapse rate in patients who do not receive consistent therapy.162,163 Several patients maintained their dosage of either isotretinoin 20 mg/day or 40 mg every other day to prevent relapse.164,165 To enhance the efficacy of treating SGH, isotretinoin can be used in conjunction with lasers and photodynamic therapy.166
Oily Skin (Hyper Seborrhea)
Face looking like an oily mess by noon and difficulty with makeup are problems in people with hyper seborrhea. Isotretinoin has been proven to be the highest reduction of sebum secretion among all treatment options for hyper seborrhea.
A prospective study revealed that sebum excretion rates were profoundly reduced after a 4-month course of isotretinoin at 1 mg/kg/day (79–83%) and remained significantly low one year following therapy (43–36%).167 Even with a low dosage of isotretinoin (2.5–5mg/day), a reduction in sebum production of up to 64% can be observed. Additionally, biopsies have shown a 51% decrease in the size of sebaceous glands following a 6-month course of this therapy.168 But a lower dose of isotretinoin is associated with a higher relapse rate of acne and hyper seborrhea.169
Conclusion
Isotretinoin has increasingly been used to treat various dermatological conditions, in addition to its primary indication for severe acne vulgaris. Success stories of effectiveness in these conditions have expanded its potential usage beyond previously known. However, it is important to note that most studies are limited to case reports, case series, or prospective studies. Therefore, it is still necessary to conduct randomized controlled trials to confirm the effectiveness of isotretinoin in treating these conditions. When considering treatment options, carefully evaluating the potential benefits and drawbacks is crucial. For instance, it is important to consider the possible side effects of isotretinoin, especially for women of childbearing age.
Data Sharing Statement
Unavailable data, but the reader can personally request access via Dr. Anon Paichitrojjana; E-mail: [email protected].
Acknowledgments
All authors thank the School of Antiaging and Regenerative Medicine, Mae Fah Luang University, and the Faculty of Medicine, Ramathibodi Hospital, Mahidol University, for their research facilities.
Funding
This study did not receive any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. FDA. FDA approved drug products: accutane oral capsule; 2023. Available from: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=018662.
2. European Medicines Agency. Roaccutane was registered in all EU member states, except Sweden, from 1983; 2023. Available from: https://www.ema.europa.eu/en/medicines/human/referrals/roaccutane.
3. Layton A. The use of isotretinoin in acne. Dermatoendocrinol. 2009;1(3):162–169. doi:10.4161/derm.1.3.9364
4. Nelson AM, Gilliland KL, Cong Z, et al. 13-cis Retinoic acid induces apoptosis and cell cycle arrest in human SEB-1 sebocytes. J Invest Dermatol. 2006;126(10):2178–2189. doi:10.1038/sj.jid.5700289
5. Dispenza MC, Wolpert EB, Gilliland KL, et al. Systemic isotretinoin therapy normalizes exaggerated TLR-2-mediated innate immune responses in acne patients. J Invest Dermatol. 2012;132(9):2198–2205. doi:10.1038/jid.2012.111
6. Meyskens FL, Gilmartin E, Alberts DS, et al. Activity of isotretinoin against squamous cell cancers and preneoplastic lesions. Cancer Treat Rep. 1982;66(6):1315–1319.
7. Wysowski DK, Swann J, Vega A. Use of isotretinoin (Accutane) in the United States: rapid increase from 1992 through 2000. J Am Acad Dermatol. 2002;46(4):505–509. doi:10.1067/mjd.2002.120529
8. Chu S, Michelle L, Ekelem C, et al. Oral isotretinoin for the treatment of dermatologic conditions other than acne: a systematic review and discussion of future directions. Arch Dermatol Res. 2021;313(6):391–430. doi:10.1007/s00403-020-02152-4
9. Bagatin E, Costa CS, Rocha MADD, et al. Consensus on the use of oral isotretinoin in dermatology - Brazilian Society of Dermatology. An Bras Dermatol. 2020;95(Suppl 1):19–38. doi:10.1016/j.abd.2020.09.001
10. Johnson BA, Nunley JR. Use of systemic agents in the treatment of acne vulgaris.. Am Fam Physician. 2000;62(8):1823–1836.
11. Layton AM, Dreno B, Gollnick HP, et al. A review of the European Directive for prescribing systemic isotretinoin for acne vulgaris. J Eur Acad Dermatol Venereol. 2006;20(7):773–776. doi:10.1111/j.1468-3083.2006.01671.x
12. Dessinioti C, Zouboulis CC, Bettoli V, et al. Comparison of guidelines and consensus articles on the management of patients with acne with oral isotretinoin. J Eur Acad Dermatol Venereol. 2020;34(10):2229–2240. doi:10.1111/jdv.16430
13. Goulden V, Clark SM, McGeown C, et al. Treatment of acne with intermittent isotretinoin. Br J Dermatol. 1997;137(1):106–108. doi:10.1046/j.1365-2133.1997.17771864.x
14. Layton AM, Knaggs H, Taylor J, et al. Isotretinoin for acne vulgaris-10 years later; a safe and successful treatment. Br J Dermatol. 1993;129(3):292–296. doi:10.1111/j.1365-2133.1993.tb11849.x
15. Azoulay L, Oraichi D, Bérard A. Isotretinoin therapy and the incidence of acne relapse: a nested case-control study. Br J Dermatol. 2007;157(6):1240–1248. doi:10.1111/j.1365-2133.2007.08250.x
16. Stainforth JM, Layton AM, Taylor JP, et al. Isotretinoin for the treatment of acne vulgaris: which factors may predict the need for more than one course? Br J Dermatol. 1993;129(3):297–301. doi:10.1111/j.1365-2133.1993.tb11850.x
17. Kaymak Y, Ilter N. The effectiveness of intermittent isotretinoin treatment in mild or moderate acne. J Eur Acad Dermatol Venereol. 2006;20(10):1256–1260. doi:10.1111/j.1468-3083.2006.01784.x
18. Seukeran DC, Cunliffe WJ. Acne vulgaris in the elderly: the response to low-dose isotretinoin. Br J Dermatol. 1998;139(1):99–101. doi:10.1046/j.1365-2133.1998.02321.x
19. Mandekou-Lefaki I, Delli F, Teknetzis A, et al. Low-dose schema of isotretinoin in acne vulgaris. Int J Clin Pharmacol Res. 2003;23(2–3):41–46.
20. Amichai B, Shemer A, Grunwald MH. Low-dose isotretinoin in the treatment of acne vulgaris. J Am Acad Dermatol. 2006;54(4):644–646. doi:10.1016/j.jaad.2005.11.1061
21. Sardana K, Garg VK. Efficacy of low-dose isotretinoin in acne vulgaris. Indian J Dermatol Venereol Leprol. 2010;76(1):7–13. doi:10.4103/0378-6323.58672
22. Rao PK, Bhat RM, Nandakishore B, et al. Safety and efficacy of low-dose isotretinoin in the treatment of moderate to severe acne vulgaris. Indian J Dermatol. 2014;59(3):316. doi:10.4103/0019-5154.131455
23. Dhaked DR, Meena RS, Maheshwari A, et al. A randomized comparative trial of two low-dose oral isotretinoin regimens in moderate to severe acne vulgaris. Indian Dermatol Online J. 2016;7(5):378–385. doi:10.4103/2229-5178.190505
24. Palmer RA, Sidhu S, Goodwin PG. ‘Microdose’ isotretinoin. Br J Dermatol. 2000;143(1):205–206. doi:10.1046/j.1365-2133.2000.03626.x
25. Amichai B. Long-term mini-doses of isotretinoin in the treatment of relapsing acne. J Dermatol. 2003;30(7):572. doi:10.1111/j.1346-8138.2003.tb00437.x
26. Strauss JS, Rapini RP, Shalita AR, et al. Isotretinoin therapy for acne: results of a multicenter dose-response study. J Am Acad Dermatol. 1984;10(3):490–496. doi:10.1016/s0190-9622(84)80100-0
27. Al Muqarrab F, Almohssen A. Low-dose oral isotretinoin for the treatment of adult patients with mild-to-moderate acne vulgaris: systematic review and meta-analysis. Dermatol Ther. 2022;35(4):e15311. doi:10.1111/dth.15311
28. Sadeghzadeh-Bazargan A, Ghassemi M, Goodarzi A, et al. Systematic review of low-dose isotretinoin for treatment of acne vulgaris: focus on indication, dosage, regimen, efficacy, safety, satisfaction, and follow up, based on clinical studies. Dermatol Ther. 2021;34(1):e14438. doi:10.1111/dth.14438
29. Torzecka JD, Dziankowska-Bartkowiak B, Gerlicz-Kowalczuk Z, et al. The use of isotretinoin in low doses and unconventional treatment regimens in different types of acne: a literature review. Postepy Dermatol Alergol. 2017;34(1):1–5. doi:10.5114/ada.2017.65614
30. Rademaker M. Isotretinoin: dose, duration and relapse. What does 30 years of usage tell us? Australas J Dermatol. 2013;54(3):157–162. doi:10.1111/j.1440-0960.2012.00947.x
31. Lee JW, Yoo KH, Park KY, et al. Effectiveness of conventional, low-dose and intermittent oral isotretinoin in the treatment of acne: a randomized, controlled comparative study. Br J Dermatol. 2011;164(6):1369–1375. doi:10.1111/j.1365-2133.2010.10152.x
32. Cyrulnik AA, Viola KV, Gewirtzman AJ, et al. High-dose isotretinoin in acne vulgaris: improved treatment outcomes and quality of life. Int J Dermatol. 2012;51(9):1123–1130. doi:10.1111/j.1365-4632.2011.05409.x
33. Blasiak RC, Stamey CR, Burkhart CN, et al. High-dose isotretinoin treatment and the rate of retrial, relapse, and adverse effects in patients with acne vulgaris. JAMA Dermatol. 2013;149(12):1392–1398. doi:10.1001/jamadermatol.2013.6746
34. Ghaffarpour G, Mazloomi S, Soltani-Arabshahi R, et al. Oral isotretinoin for acne, adjusting treatment according to patient’s response. J Drugs Dermatol. 2006;5(9):878–882.
35. Leyden JJ, Del Rosso JQ, Baum EW. The use of isotretinoin in the treatment of acne vulgaris: clinical considerations and future directions. J Clin Aesthet Dermatol. 2014;7(2 Suppl):S3–S21.
36. Colburn WA, Gibson DM, Wiens RE, et al. Food increases the bioavailability of isotretinoin. J Clin Pharmacol. 1983;23(11–12):534–539. doi:10.1002/j.1552-4604.1983.tb01800.x
37. Bellomo R, Brunner M, Tadjally E. New formulations of isotretinoin for acne treatment: expanded options and clinical implications. J Clin Aesthet Dermatol. 2021;14(12 Suppl 1):S18–S23.
38. Madan S, Kumar S, Segal J. Comparative pharmacokinetic profiles of a novel low-dose micronized-isotretinoin 32 mg formulation and lidose-isotretinoin 40 mg in fed and fasted conditions: two open-label, randomized, crossover studies in healthy adult participants. Acta Derm Venereol. 2020;100(4):adv00049. doi:10.2340/00015555-3381
39. Strauss JS, Leyden JJ, Lucky AW, et al. A randomized trial of the efficacy of a new micronized formulation versus a standard formulation of isotretinoin in patients with severe recalcitrant nodular acne. J Am Acad Dermatol. 2001;45(2):187–195. doi:10.1067/mjd.2001.115965
40. Del Rosso JQ, Stein Gold L, Segal J, et al. An open-label, phase IV study evaluating lidose-isotretinoin administered without food in patients with severe recalcitrant nodular acne: low relapse rates observed over the 104-week post-treatment period. J Clin Aesthet Dermatol. 2019;12(11):13–18.
41. Del Rosso JQ. Status report on oral isotretinoin in the management of acne vulgaris: why all the discussion about drug absorption and relapse rates? Curr Dermatol Rep. 2013;2(3):177–180.
42. Tolino E, Skroza N, Proietti I, et al. Efficacy and safety of systemic isotretinoin treatment for moderate to severe acne (insights from the real-life clinical setting). Dermatol Ther. 2020;33(6):e14392. doi:10.1111/dth.14392
43. Demirci Saadet E. Investigation of relapse rate and factors affecting relapse after oral isotretinoin treatment in patients with acne vulgaris. Dermatol Ther. 2021;34(6):e15109. doi:10.1111/dth.15109
44. Agarwal US, Besarwal RK, Bhola K. Oral isotretinoin in different dose regimens for acne vulgaris: a randomized comparative trial. Indian J Dermatol Venereol Leprol. 2011;77(6):688–694. doi:10.4103/0378-6323.86482
45. Boyraz N, Mustak PK. Comparison of the efficacies of intermittent and continuous low-dose isotretinoin regimens in the treatment of moderate acne vulgaris. Int J Dermatol. 2013;52(10):1265–1267. doi:10.1111/j.1365-4632.2012.05853.x
46. Webster GF, Leyden JJ, Gross JA. Comparative pharmacokinetic profiles of a novel isotretinoin formulation (isotretinoin-Lidose) and the innovator isotretinoin formulation: a randomized, 4-treatment, crossover study. J Am Acad Dermatol. 2013;69(5):762–767. doi:10.1016/j.jaad.2013.05.036
47. Rademaker M, Wishart JM, Birchall NM. Isotretinoin 5 mg daily for low-grade adult acne vulgaris--a placebo-controlled, randomized double-blind study. J Eur Acad Dermatol Venereol. 2014;28(6):747–754. doi:10.1111/jdv.12170
48. Niazi S, Shehzad A. Comparison of efficacy of fixed low-dose regimens (daily vs alternate day) of oral isotretinoin in mild to moderate acne vulgaris. J Pak Assoc Dermatol. 2016;25(4):291–297.
49. Ahmad HM. Analysis of clinical efficacy, side effects, and laboratory changes among patients with acne vulgaris receiving single versus twice daily dose of oral isotretinoin. Dermatol Ther. 2015;28(3):151–157. doi:10.1111/dth.12213
50. Shetti SA, Nagesh HN, Hanumantharaya N. A randomized, open-label, comparative study of efficacy of low-dose continuous versus low-dose intermittent oral isotretinoin therapy in moderate-to-severe acne vulgaris. Natl J Physiol Pharm Pharmacol. 2017;7(9):941–946. doi:10.5455/njppp.2017.7.0305804052017
51. Faghihi G, Mokhtari F, Fard NM, et al. Comparing the efficacy of low dose and conventional dose of oral isotretinoin in treatment of moderate and severe acne vulgaris. J Res Pharm Pract. 2017;6(4):233–238. doi:10.4103/jrpp.JRPP_17_30
52. Aziz Ragab MA E, Omar SS, Collier A, et al. The effect of continuous high versus low dose oral isotretinoin regimens on dermcidin expression in patients with moderate to severe acne vulgaris. Dermatol Ther. 2018;31(6):e12715. doi:10.1111/dth.12715
53. Pandey D, Agrawal S. Efficacy of isotretinoin and antihistamine versus isotretinoin alone in the treatment of moderate to severe acne: a randomised control trial. Kathmandu Univ Med J. 2019;17(65):14–19.
54. Kassem B, Ismail M, Hassan F. Evaluation of the efficacy and relapse rates of treatment protocols for moderate acne using isotretinoin based on the global acne grading system: randomized, controlled, comparative study. Dermatol Ther. 2022;35(12):e15974. doi:10.1111/dth.15974
55. van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22(4):457–465. doi:10.1007/s40257-021-00595-7
56. Guruvayoorappan C, Kuttan G. 13 cis-retinoic acid regulates cytokine production and inhibits angiogenesis by disrupting endothelial cell migration and tube formation. J Exp Ther Oncol. 2008;7(3):173–182.
57. Paichitrojjana A, Paichitrojjana A. Successful treatment of ivermectin refractory demodicosis with isotretinoin and permethrin cream. JAAD Case Rep. 2022;26:98–100. doi:10.1016/j.jdcr.2022.06.017
58. Ertl GA, Levine N, Kligman AM. A comparison of the efficacy of topical tretinoin and low-dose oral isotretinoin in rosacea. Arch Dermatol. 1994;130(3):319–324.
59. Gollnick H, Blume-Peytavi U, Szabó EL, et al. Systemic isotretinoin in the treatment of rosacea - doxycycline- and placebo-controlled, randomized clinical study. J Dtsch Dermatol Ges. 2010;8(7):505–515. doi:10.1111/j.1610-0387.2010.07345.x
60. Sbidian E, Vicaut É, Chidiack H, et al. A randomized-controlled trial of oral low-dose isotretinoin for difficult-to-treat papulopustular Rosacea. J Invest Dermatol. 2016;136(6):1124–1129. doi:10.1016/j.jid.2016.01.025
61. Shemer A, Gupta AK, Kassem R, et al. Low-dose isotretinoin versus minocycline in the treatment of rosacea. Dermatol Ther. 2021;34(4):e14986. doi:10.1111/dth.14986
62. Rademaker M. Very low-dose isotretinoin in mild to moderate papulopustular rosacea; a retrospective review of 52 patients. Australas J Dermatol. 2018;59(1):26–30. doi:10.1111/ajd.12522
63. Uslu M, Şavk E, Karaman G, et al. Rosacea treatment with intermediate-dose isotretinoin: follow-up with erythema and sebum measurements. Acta Derm Venereol. 2012;92(1):73–77. doi:10.2340/00015555-1204
64. Mayur O, Martinez R, McNichol MC, et al. Clinical and histological features and treatment outcomes of patients with Morbihan disease: a systematic review. Arch Dermatol Res. 2023:1. doi:10.1007/s00403-023-02621-6
65. Boer J. Oral retinoids for hidradenitis suppurativa. In: Jemec GBE, Revuz J, Leyden J, editors. Hidradenitis suppurativa. Heidelberg: Springer; 2006:128–134.
66. Boer J, van Gemert MJ. Long-term results of isotretinoin in the treatment of 68 patients with hidradenitis suppurativa. J Am Acad Dermatol. 1999;40(1):73–76. doi:10.1016/s0190-9622(99)70530-x
67. Soria A, Canoui-Poitrine F, Wolkenstein P, et al. Absence of efficacy of oral isotretinoin in hidradenitis suppurativa: a retrospective study based on patients’ outcome assessment. Dermatology. 2009;218(2):134–135. doi:10.1159/000182261
68. Huang CM, Kirchhof MG. A new perspective on isotretinoin treatment of hidradenitis suppurativa: a retrospective chart review of patient outcomes. Dermatology. 2017;233(2–3):120–125. doi:10.1159/000477207
69. Patel N, McKenzie SA, Harview CL, et al. Isotretinoin in the treatment of hidradenitis suppurativa: a retrospective study. J Dermatolog Treat. 2021;32(4):473–475. doi:10.1080/09546634.2019.1670779
70. Jørgensen AR, Thomsen SF, Ring HC. Isotretinoin and hidradenitis suppurativa. Clin Exp Dermatol. 2019;44(4):e155–e156. doi:10.1111/ced.13953
71. Gallagher CG, Kirthi SK, Cotter CC, et al. Could isotretinoin flare hidradenitis suppurativa? A case series. Clin Exp Dermatol. 2019;44(7):777–780. doi:10.1111/ced.13944
72. Boer J. Are there indications for isotretinoin treatment of hidradenitis suppurativa? Dermatology. 2017;233(2–3):111–112. doi:10.1159/000477615
73. Tietze JK, Heppt MV, von Preußen A, et al. Oral isotretinoin as the most effective treatment in folliculitis decalvans: a retrospective comparison of different treatment regimens in 28 patients. J Eur Acad Dermatol Venereol. 2015;29(9):1816–1821. doi:10.1111/jdv.13052
74. Aksoy B, Hapa A, Mutlu E. Isotretinoin treatment for folliculitis decalvans: a retrospective case-series study. Int J Dermatol. 2018;57(2):250–253. doi:10.1111/ijd.13874
75. Bunagan MJ, Banka N, Shapiro J. Retrospective review of folliculitis decalvans in 23 patients with course and treatment analysis of long-standing cases. J Cutan Med Surg. 2015;19(1):45–49. doi:10.2310/7750.2014.13218
76. Miguel-Gómez L, Rodrigues-Barata AR, Molina-Ruiz A, et al. Folliculitis decalvans: effectiveness of therapies and prognostic factors in a multicenter series of 60 patients with long-term follow-up. J Am Acad Dermatol. 2018;79(5):878–883. doi:10.1016/j.jaad.2018.05.1240
77. Shireen F, Sudhakar A. A case of isotretinoin therapy-refractory folliculitis decalvans treated successfully with Biosimilar adalimumab (exemptia). Int J Trichol. 2018;10(5):240–241. doi:10.4103/ijt.ijt_34_18
78. Gemmeke A, Wollina U. Folliculitis decalvans of the scalp: response to triple therapy with isotretinoin, clindamycin, and prednisolone. Acta Dermatovenerol Alp Pannonica Adriat. 2006;15(4):184–186.
79. Marquis K, Christensen LC, Rajpara A. Dissecting cellulitis of the scalp with excellent response to isotretinoin. Pediatr Dermatol. 2017;34(4):e210–e211. doi:10.1111/pde.13143
80. Guo W, Zhu C, Stevens G, et al. Analyzing the efficacy of isotretinoin in treating dissecting cellulitis: a literature review and meta-analysis. Drugs RD. 2021;21(1):29–37. doi:10.1007/s40268-020-00335-y
81. Badaoui A, Reygagne P, Cavelier-Balloy B, et al. Dissecting cellulitis of the scalp: a retrospective study of 51 patients and review of literature. Br J Dermatol. 2016;174(2):421–423. doi:10.1111/bjd.13999
82. Qi S, Zhao Y, Zhang X, et al. Clinical features of primary cicatricial alopecia in Chinese patients. Indian J Dermatol Venereol Leprol. 2014;80(4):306–312. doi:10.4103/0378-6323.136833
83. Khaled A, Zeglaoui F, Zoghlami A, et al. Dissecting cellulitis of the scalp: response to isotretinoin. J Eur Acad Dermatol Venereol. 2007;21(10):1430–1431. doi:10.1111/j.1468-3083.2007.02239.x
84. Thomas J, Aguh C. Approach to treatment of refractory dissecting cellulitis of the scalp: a systematic review. J Dermatolog Treat. 2021;32(2):144–149. doi:10.1080/09546634.2019.1642441
85. Melo DF, Trüeb RM, Dutra H, et al. Low-dose isotretinoin as a therapeutic option for dissecting cellulitis. Dermatol Ther. 2020;33(6):e14273. doi:10.1111/dth.14273
86. Yanfei Z, Xiaoying N, Dingwei Z, et al. Efficacy and safety of oral isotretinoin in the treatment of moderate to severe seborrheic dermatitis: a retrospective study. Int J Dermatol. 2023;62(6):759–763. doi:10.1111/ijd.16582
87. de Souza Leão Kamamoto C, Sanudo A, Hassun KM, et al. Low-dose oral isotretinoin for moderate to severe seborrhea and seborrheic dermatitis: a randomized comparative trial. Int J Dermatol. 2017;56(1):80–85. doi:10.1111/ijd.13408
88. King A, Tan MG, Kirshen C, et al. Isotretinoin for the management of moderate-to-severe seborrheic dermatitis: a systematic review. J Am Acad Dermatol. 2023;2023(23):1351. doi:10.1016/j.jaad.2023.07.010
89. Barzilai A, David M, Trau H, et al. Seborrheic dermatitis-like eruption in patients taking isotretinoin therapy for acne: retrospective study of five patients. Am J Clin Dermatol. 2008;9(4):255–261. doi:10.2165/00128071-200809040-00005
90. Paul S, Das A, Ghosh C. Efficacy and safety of isotretinoin in comparison to methotrexate in the patients suffering from moderate-to-severe plaque psoriasis: a prospective cohort study. Asian J Med Sci. 2022;13(4):66–72. doi:10.3126/ajms.v13i4.41610
91. Mortazavi H, Khezri S, Hosseini H, et al. A single blind randomized clinical study: the efficacy of isotretinoin plus narrow band ultraviolet B in the treatment of psoriasis vulgaris. Photodermatol Photoimmunol Photomed. 2011;27(3):159–161. doi:10.1111/j.1600-0781.2011.00581.x
92. Gahalaut P, Soodan PS, Mishra N, et al. Clinical efficacy of psoralen + sunlight vs combination of isotretinoin and psoralen + sunlight for the treatment of chronic plaque-type psoriasis vulgaris: a randomized hospital-based study. Photodermatol Photoimmunol Photomed. 2014;30(6):294–301. doi:10.1111/phpp.12125
93. Sofen HL, Moy RL, Lowe NJ. Treatment of generalised pustular psoriasis with isotretinoin. Lancet. 1984;1(8367):40. doi:10.1016/s0140-6736(84)90196-x
94. Moy RL, Kingston TP, Lowe NJ. Isotretinoin vs etretinate therapy in generalized pustular and chronic psoriasis. Arch Dermatol. 1985;121(10):1297–1301.
95. Criado PR, Ianhez M, Rocha PS, et al. Pityriasis rubra pilaris (type I) following ChAdOx1 COVID-19 vaccine: a report of two cases with successful treatment with oral isotretinoin. J Eur Acad Dermatol Venereol. 2022;36(7):e508–e510. doi:10.1111/jdv.18055
96. Al Khalifa N, Alsabbagh M, Raees M, et al. Misdiagnosed pityriasis rubra pilaris successfully managed with isotretinoin: a case series. Cureus. 2023;15(5):e38657. doi:10.7759/cureus.38657
97. Vena GA, Coviello C, Angelini G. Impiego dell’isotretinoina orale nel trattamento del lupus eritematoso cutaneo [Use of oral isotretinoin in the treatment of cutaneous lupus erythematosus]. G Ital Dermatol Venereol. 1989;124(6):311–315. Italian.
98. Rubenstein DJ, Huntley AC. Keratotic lupus erythematosus: treatment with isotretinoin. J Am Acad Dermatol. 1986;14(5 Pt 2):910–914. doi:10.1016/s0190-9622(86)70111-4
99. Shornick JK, Formica N, Parke AL. Isotretinoin for refractory lupus erythematosus. J Am Acad Dermatol. 1991;24(1):49–52. doi:10.1016/0190-9622(91)70008-p
100. Richardson TT, Cohen PR. Subacute cutaneous lupus erythematosus: report of a patient who subsequently developed a meningioma and whose skin lesions were treated with isotretinoin.. Cutis. 2000;66(3):183–188.
101. Camisa C, Allen CM. Treatment of oral erosive lichen planus with systemic isotretinoin. Oral Surg Oral Med Oral Pathol. 1986;62(4):393–396. doi:10.1016/0030-4220(86)90288-4
102. Woo TY. Systemic isotretinoin treatment of oral and cutaneous lichen planus. Cutis. 1985;35(4):385–393.
103. Rahman A, Hafeez D. Successful treatment of exanthematous lichen planus in a young adult with low dose oral corticosteroid and isotretinoin. Dermatol Online J. 2022;28(4):
104. Muthu SK, Narang T, Saikia UN, et al. Low-dose oral isotretinoin therapy in lichen planus pigmentosus: an open-label non-randomized prospective pilot study. Int J Dermatol. 2016;55(9):1048–1054. doi:10.1111/ijd.13293
105. Pham CT, Hosking A-M, Cox S, et al. Therapeutic response of facial papules and inflammation in frontal fibrosing alopecia to low-dose oral isotretinoin. JAAD Case Rep. 2020;6(5):453–456. doi:10.1016/j.jdcr.2020.01.030
106. Rakowska A, Gradzińska A, Olszewska M, et al. Efficacy of isotretinoin and acitretin in treatment of frontal fibrosing alopecia: retrospective analysis of 54 cases. J Drugs Dermatol. 2017;16(10):988–992.
107. Saber M, Bahraminejad M, Fatemi Naeini F, et al. Comparison of systemic and topical isotretinoin in the treatment of facial lichen planopilaris: a randomized controlled trial. J Cosmet Dermatol. 2022;21(9):3896–3904. doi:10.1111/jocd.14730
108. Babahosseini H, Tavakolpour S, Mahmoudi H, et al. Lichen planopilaris: retrospective study on the characteristics and treatment of 291 patients. J Dermatolog Treat. 2019;30(6):598–604. doi:10.1080/09546634.2018.1542480
109. Pedrosa AF, Duarte AF, Haneke E, et al. Yellow facial papules associated with frontal fibrosing alopecia: a distinct histologic pattern and response to isotretinoin. J Am Acad Dermatol. 2017;77(4):764–766. doi:10.1016/j.jaad.2017.04.1118
110. Looney M, Smith KM. Isotretinoin in the treatment of granuloma annulare. Ann Pharmacother. 2004;38(3):494–497. doi:10.1345/aph.1D312
111. Ratnavel RC, Norris PG. Perforating granuloma annulare: response to treatment with isotretinoin. J Am Acad Dermatol. 1995;32(1):126–127. doi:10.1016/0190-9622(95)90210-4
112. Tang WYM, Chong L-Y, Lo -K-K. Resolution of generalized granuloma annulare with isotretinoin therapy. Int J Dermatol. 1996;35(6):455–456. doi:10.1111/j.1365-4362.1996.tb03034.x
113. Pasmatzi E, Georgiou S, Monastirli A, et al. Temporary remission of disseminated granuloma annulare under oral isotretinoin therapy. Int J Dermatol. 2005;44(2):169–171. doi:10.1111/j.1365-4632.2005.02229.x
114. Tangrea JA, Edwards BK, Taylor PR, et al. Long-term therapy with low-dose isotretinoin for prevention of basal cell carcinoma: a multicenter clinical trial. isotretinoin-Basal Cell Carcinoma Study Group. J Natl Cancer Inst. 1992;84(5):328–332. doi:10.1093/jnci/84.5.328
115. Levine N, Moon TE, Cartmel B, et al. Trial of retinol and isotretinoin in skin cancer prevention: a randomized, double-blind, controlled trial. Southwest Skin Cancer Prevention Study Group. Cancer Epidemiol Biomarkers Prev. 1997;6(11):957–961.
116. Lippman SM, Parkinson DR, Itri LM, et al. 13-cis-retinoic acid and interferon -2a: effective combination. Therapy for advanced squamous cell carcinoma of the skin. J Natl Cancer Inst. 1992;84(4):235–241. doi:10.1093/jnci/84.4.235
117. Toma S, Palumbo R, Vincenti M, et al. Efficacy of recombinant alpha-interferon 2a and 13-cis-retinoic acid in the treatment of squamous cell carcinoma. Ann Oncol. 1994;5(5):463–465. doi:10.1093/oxfordjournals.annonc.a058881
118. Hong WK, Endicott J, Itri LM, et al. 13- cis -retinoic acid in the treatment of Oral Leukoplakia. N Engl J Med. 1986;315(24):1501–1505. doi:10.1056/NEJM198612113152401
119. Lippman SM, Batsakis JG, Toth BB, et al. Comparison of low-dose isotretinoin with beta carotene to prevent oral carcinogenesis. N Engl J Med. 1993;328(1):15–20. doi:10.1056/NEJM199301073280103
120. Xie A, Liu J. Chemoprevention of oral cancer in leukoplakia patients: a systematic review and meta-analysis. J Pak Med Assoc. 2017;67(9):1415–1419.
121. Wong WINONAYL, Kolbusz RV, Goldberg LH, et al. Treatment of a recurrent keratoacanthoma with oral isotretinoin. Int J Dermatol. 1994;33(8):579–583. doi:10.1111/j.1365-4362.1994.tb02902.x
122. Feldman RJ, Maize JC. Multiple keratoacanthomas in a young woman: report of a case emphasizing medical management and a review of the spectrum of multiple keratoacanthomas. Int J Dermatol. 2007;46(1):77–79. doi:10.1111/j.1365-4632.2006.02948.x
123. Haydey RP, Reed ML, Dzubow LM, et al. Treatment of Keratoacanthomas with oral 13- cis -retinoic acid. N Engl J Med. 1980;303(10):560–562. doi:10.1056/NEJM198009043031005
124. Levine N. Oral isotretinoin therapy. Use in a patient with multiple cutaneous squamous cell carcinomas and keratoacanthomas. Arch Dermatol. 1984;120(9):1215–1217. doi:10.1001/archderm.1984.01650450097029
125. Shaw JC, White CR. Treatment of multiple keratoacanthomas with oral isotretinoin. J Am Acad Dermatol. 1986;15(5):1079–1082. doi:10.1016/s0190-9622(86)70268-5
126. Schaller M, Korting HC, Wolff H, et al. Multiple keratoacanthomas, giant keratoacanthoma and keratoacanthoma centrifugum marginatum: development in a single patient and treatment with oral isotretinoin. Acta Derm Venereol. 1996;76(1):40–42. doi:10.2340/00015555764042
127. Molin L, Thomsen K, Volden G, et al. Oral retinoids in mycosis fungoides and Sézary syndrome: a comparison of isotretinoin and etretinate. A study from the Scandinavian Mycosis Fungoides Group. Acta Derm Venereol. 1987;67(3):232–236.
128. Thomsen K, Hammar H, Molin L, et al. Retinoids plus PUVA (RePUVA) and PUVA in mycosis fungoides, plaque stage. A report from the Scandinavian Mycosis Fungoides Group. Acta Derm Venereol. 1989;69(6):536–538.
129. Woo YR, Lee HM, Lee JS, et al. Long-term follow-up of refractory mycosis fungoides which achieved remission with the addition of isotretinoin to methotrexate and psoralen plus ultraviolet a therapy. Ann Dermatol. 2013;25(2):259–260. doi:10.5021/ad.2013.25.2.259
130. Del Guzzo CA, Jariwala NN, Haun PL, et al. Pilot study of a novel therapeutic approach for refractory advanced stage folliculotropic mycosis fungoides. Acta Derm Venereol. 2020;100(13):adv00187. doi:10.2340/00015555-3443
131. Kraemer KH, DiGiovanna JJ, Moshell AN, et al. Prevention of skin cancer in xeroderma pigmentosum with the use of oral isotretinoin. N Engl J Med. 1988;318(25):1633–1637. doi:10.1056/NEJM198806233182501
132. Saade M, Debahy NE, Houjeily S. Clinical remission of xeroderma pigmentosum-associated squamous cell carcinoma with isotretinoin and chemotherapy: case report. J Chemother. 1999;11(4):313–317. doi:10.1179/joc.1999.11.4.313
133. Zaman S, Gillani JA, Nabeela N, et al. Role of isotretinoin in cancer prevention and management in malignancies associated with xeroderma pigmentosum. J Ayub Med Coll Abbottabad. 2014;26(2):255–257.
134. Leung AK, Barankin B, Lam JM, et al. Xeroderma pigmentosum: an updated review. Drugs in Context. 2022;11:2022–2025. doi:10.7573/dic.2022-2-5
135. Baden HP, Buxman MM, Weinstein GD, et al. Treatment of ichthyosis with isotretinoin. J Am Acad Dermatol. 1982;6(4):716–720. doi:10.1016/s0190-9622(82)70062-3
136. Chang LM, Reyes M. A case of harlequin ichthyosis treated with isotretinoin. Dermatol Online J. 2014;20(2):
137. Zaenglein AL, Levy ML, Stefanko NS, et al. Consensus recommendations for the use of retinoids in ichthyosis and other disorders of cornification in children and adolescents. Pediatr Dermatol. 2021;38(1):164–180. doi:10.1111/pde.14408
138. Hanna N, Lam M, Fleming P, Lynde CW. Therapeutic options for the treatment of Darier’s disease: a comprehensive review of the literature. J Cutan Med Surg. 2022;26(3):280–290. doi:10.1177/12034754211058405
139. Pasmatzi E, Badavanis G, Kapranos N, et al. Extensive and recalcitrant common warts in an immunocompetent patient: rapid and complete remission after oral isotretinoin monotherapy. Acta Dermatovenerol Alp Pannonica Adriat. 2020;29(1):35–37. PMID: 32206821.
140. Katz RA. Isotretinoin treatment of recalcitrant warts in an immunosuppressed man. Arch Dermatol. 1986;122(1):19–20. doi:10.1001/archderm.1986.01660130021014
141. Dave DD, Abdelmaksoud A. Low dose isotretinoin as an adjuvant therapy for treatment of different clinical variants of warts: a case series. Dermatol Ther. 2019;32(2):e12836. PMID: 30663177. doi:10.1111/dth.12836
142. Nofal A, Fawzy MM, Eldeeb F, et al. Oral isotretinoin versus Acitretin in male patients with multiple recalcitrant common warts: a randomized, double-blinded placebo-control study. J Cosmet Dermatol. 2022;21(11):5895–5901. PMID: 35726506. doi:10.1111/jocd.15173
143. Salman S, Shehata M, Ibrahim AM, et al. Efficacy of retinoids alone or in combination with other remedies in the management of warts: a systematic review and network meta-analysis. Dermatol Ther. 2021;34(2):e14793. PMID: 33480148. doi:10.1111/dth.14793
144. Diab N, Atef H, Salah E. Comparative efficacy of using a combination of intralesional purified protein derivative with low dose isotretinoin in the treatment of recalcitrant common warts. Dermatol Ther. 2022;35(6):e15457. PMID: 35297138. doi:10.1111/dth.15457
145. Olguin-García MG, Jurado-Santa Cruz F, Peralta-Pedrero ML, et al. A double-blind, randomized, placebo-controlled trial of oral isotretinoin in the treatment of recalcitrant facial flat warts. J Dermatolog Treat. 2015;26(1):78–82. doi:10.3109/09546634.2013.869302
146. Kaur GJ, Brar BK, Kumar S, et al. Evaluation of the efficacy and safety of oral isotretinoin versus topical isotretinoin in the treatment of plane warts: a randomized open trial. Int J Dermatol. 2017;56(12):1352–1358. PMID: 28901534. doi:10.1111/ijd.13727
147. Nofal A, Khedr A, Fathy M. Combined oral isotretinoin and Candida antigen versus either agent alone in the treatment of plane warts. J Dermatolog Treat. 2022;33(1):342–347. doi:10.1080/09546634.2020.1754325
148. Nofal A, Fawzy MM, Eldeeb F, et al. High versus low dose oral isotretinoin in the treatment of cutaneous and genital warts. Dermatol Ther. 2022;35(12):e15964. doi:10.1111/dth.15964
149. Cardamakis E, Kotoulas IG, Relakis K, et al. Comparative study of systemic interferon alfa-2a plus isotretinoin versus isotretinoin in the treatment of recurrent condyloma acuminatum in men. Urology. 1995;45(5):857–860. doi:10.1016/S0090-4295(99)80094-6
150. Cardamakis EK, Kotoulas IG, Dimopoulos DP, et al. Comparative study of systemic interferon alfa-2a with oral isotretinoin and oral isotretinoin alone in the treatment of recurrent condylomata accuminata. Arch Gynecol Obstet. 1996;258(1):35–41. doi:10.1007/BF01370930
151. Olsen EA, Kelly FF, Vollmer RT, et al. Comparative study of systemic interferon alfa-nl and isotretinoin in the treatment of resistant condylomata acuminata. J Am Acad Dermatol. 1989;20(6):1023–1030. doi:10.1016/s0190-9622(89)70127-4
152. Pasmatzi E, Kapranos N, Monastirli A, Melachrinou M, Georgiou S, Tsambaos D. Large benign condyloma acuminatum: successful treatment with isotretinoin and interferon alpha. Acta Derm Venereol. 2012;92(3):249–250. doi:10.2340/00015555-1257
153. Yildirim M, Inaloz HS, Baysal V, et al. A case of condyloma acuminatum treated successfully with low-dose isotretinoin and interferon. Int J Clin Pract. 2004;58(9):889–891. doi:10.1111/j.1742-1241.2004.00071.x
154. Georgala S, Katoulis AC, Georgala C, et al. Oral isotretinoin in the treatment of recalcitrant condylomata acuminata of the cervix: a randomised placebo controlled trial. Sex Transm Infect. 2004;80(3):216–218. doi:10.1136/sti.2003.006841
155. Reyna-Rodríguez IL, Chavez-Alvarez S, Garza-Rodríguez V, et al. Cryotherapy plus low-dose oral isotretinoin vs cryotherapy only for the treatment of anogenital warts: a randomized clinical trial. Arch Dermatol Res. 2021;313(10):815–827. doi:10.1007/s00403-020-02182-y
156. Bagatin E, Parada MO, Miot HA, et al. A randomized and controlled trial about the use of oral isotretinoin for photoaging. Int J Dermatol. 2010;49(2):207–214. doi:10.1111/j.1365-4632.2009.04310.x
157. Bagatin E, Guadanhim LR, Enokihara MM, et al. Low-dose oral isotretinoin versus topical retinoic acid for photoaging: a randomized, comparative study. Int J Dermatol. 2014;53(1):114–122. doi:10.1111/ijd.12191
158. Hernandez-Perez E, Khawaja HA, Alvarez TY. Oral isotretinoin as part of the treatment of cutaneous aging. Dermatol Surg. 2000;26(7):649–652. doi:10.1046/j.1524-4725.2000.99210.x
159. Rabello-Fonseca RM, Azulay DR, Luiz RR, et al. Oral isotretinoin in photoaging: clinical and histopathological evidence of efficacy of an off-label indication. J Eur Acad Dermatol Venereol. 2009;23(2):115–123. doi:10.1111/j.1468-3083.2008.02947.x
160. Honeybrook A, Bernstein E. Oral isotretinoin and photoaging: a review. J Cosmet Dermatol. 2020;19(7):1548–1554. doi:10.1111/jocd.13467
161. Ianhez M, Pinto SA, Miot HA, et al. A randomized, open, controlled trial of tretinoin 0.05%9 cream vs low-dose oral isotretinoin for the treatment of field cancerization. Int J Dermatol. 2019;58(3):365–373. doi:10.1111/ijd.14363
162. Ranasinghe GC, Friedman AJ. Eruptive sebaceous hyperplasia: a rare consequence of systemic corticosteroids. J Drugs Dermatol. 2018;17(1):118–120.
163. Tagliolatto S, Santos Neto Ode O, Alchorne MM, et al. Sebaceous hyperplasia: systemic treatment with isotretinoin. An Bras Dermatol. 2015;90(2):211–215. doi:10.1590/abd1806-4841.20153192
164. Burton CS, Sawchuk WS. Premature sebaceous gland hyperplasia: successful treatment with isotretinoin. J Am Acad Dermatol. 1985;12(1 Pt 2):182–184. doi:10.1016/s0190-9622(85)80013-x
165. Gupta V, Mridha AR, Sharma VK. Sebaceous hyperplasia and sebaceous adenomas presenting as leonine facies and improving with oral isotretinoin. Clin Exp Dermatol. 2016;41(8):923–924. doi:10.1111/ced.12918
166. Hussein L, Perrett CM. Treatment of sebaceous gland hyperplasia: a review of the literature. J Dermatolog Treat. 2021;32(8):866–877. doi:10.1080/09546634.2020.1720582
167. Hughes BR, Cunliffe WJ. A prospective study of the effect of isotretinoin on the follicular reservoir and sustainable sebum excretion rate in patients with acne. Arch Dermatol. 1994;130(3):315–318.
168. Geissler SE, Michelsen S, Plewig G. Very low dose isotretinoin is effective in controlling seborrhea. J Dtsch Dermatol Ges. 2003;1(12):952–958. doi:10.1046/j.1365-2303.2003.00108.x-i1
169. Endly DC, Miller RA. Oily skin: a review of treatment options. J Clin Aesthet Dermatol. 2017;10(8):49–55.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.