Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Optimizing Recovery After Carpal Tunnel Syndrome Release Surgery: The Role of Counseling in Pain Management and Perioperative Functional Enhancement
Authors Dawod MS ![]() , Alswerki MN
, Alswerki MN ![]() , Al Ja’ar SM, Keilani DZ, Keilani LZ, Alani MA, Saimeh TH, AL-Tamimi S
, Al Ja’ar SM, Keilani DZ, Keilani LZ, Alani MA, Saimeh TH, AL-Tamimi S ![]() , Al-Shibly SM, Saimeh ZH, Al-Juboori MA, Alelaumi A
, Al-Shibly SM, Saimeh ZH, Al-Juboori MA, Alelaumi A ![]() , Alsheikh FT, Kamal TW, Khanfar A
, Alsheikh FT, Kamal TW, Khanfar A ![]()
Received 26 November 2023
Accepted for publication 26 February 2024
Published 4 March 2024 Volume 2024:17 Pages 971—980
DOI https://doi.org/10.2147/JMDH.S451008
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Moh’d said Dawod,1 Mohammad N Alswerki,2 Sarah M Al Ja’ar,3 Dana Z Keilani,3 Lana Z Keilani,3 Maryam A Alani,3 Tamara H Saimeh,3 Shatha AL-Tamimi,3 Sulaf Moh Al-Shibly,4 Zaid H Saimeh,3 Mohammed Ahmed Al-Juboori,3 Ahmad Alelaumi,2 Farah T Alsheikh,3 Tala W Kamal,3 Aws Khanfar5
1Mutah University, Faculty of Medicine, Karak, Jordan; 2Jordan University Hospital, Orthopedic Department, Amman, Jordan; 3Jordan University Hospital, Amman, Jordan; 4Jordan University of Science and Technology School of Medicine, Irbid, Jordan; 5Upper limb & Orthopedic Surgery Consultant, Jordan University Hospital, Amman, Jordan
Correspondence: Mohammad N Alswerki, Department of Orthopedic Department, Jordan University Hospital, P.O. Box 13046, Amman, Jordan, Email [email protected]
Background: Preoperative patient education is pivotal in improving patient outcomes during the perioperative phase, involving a thorough explanation of what patients can expect. This enhances adherence and reduces perioperative anxiety. In orthopedics, carpal tunnel syndrome, a common and painful hand condition, is effectively managed through surgical release under local anesthesia. Inadequate counseling before such procedures may intensify intraoperative anxiety and increase pain responses. Thus, this research aims to investigate the effects of comprehensive preoperative counseling on various parameters in carpal tunnel release surgery.
Methods: A case-control study design was adopted for this study. A retrospective analysis of patients who underwent carpal tunnel release surgery was performed. These patients were categorized into two distinct groups: one group received comprehensive counseling during their clinic visits, while the other group reported receiving less effective counseling. Evaluation encompassed patient-related factors, disease-related aspects, and perioperative variables for both groups.
Results: The study comprised 681 participants, with 526 (77.2%) being females, 421 (61.8%) undergoing surgery on the right side, and 519 (76.2%) employed in non-manual occupations. Moreover, 559 (82.1%) were non-smokers, while approximately two-thirds of the cohort had both diabetes and hypertension. The average age of participants was 52 years, and they reported a mean functional disability score of 7.2 out of 10. The comprehensive preoperative counseling group consisted of 333 patients, while the other group included 348 patients. The analysis revealed statistically significant differences between the two groups, including reduced intra-procedural anxiety (p = 0.043), decreased intraoperative pain (p = 0.005), lower rates of wound complications (p = 0.022), and improved self-reported pain relief (p = 0.3).
Conclusion: Our study emphasizes the crucial role of preoperative counseling in improving patient experiences during perioperative care, leading to reduced anxiety, milder pain responses, fewer complications, decreased reliance on postoperative pain medication, and increased self-reported pain relief.
Level of Evidence: Level III, Case-control retrospective study.
Keywords: carpal tunnel syndrome, carpal tunnel release, preoperative counselling, patient’s education, intraoperative anxiety, patient-reported outcomes, improved peri-operative care
Introduction
Counseling of patients constitutes a pivotal component within the domain of preventive medicine.1,2 Its significance is particularly pronounced during the perioperative phase, as it serves a dual purpose: firstly, to apprise patients of what to anticipate in the perioperative context, and secondly, to contribute to a seamless and efficacious postoperative convalescence.3,4 Consequently, counseling stands as a potent means to substantially mitigate the perioperative anxiety frequently experienced by patients undergoing various surgical procedures.5–8
Counseling assumes a pivotal role in efficiently mitigating perioperative stress, which has far-reaching clinical implications.9 Its effectiveness extends to improved clinical and patient-reported outcomes, encompassing enhanced postoperative pain relief and self-reported functional amelioration.7 By addressing the emotional and psychological aspects of surgery, counseling equips patients with coping strategies and a better understanding of the perioperative period, fostering empowerment and confidence.10 These positive outcomes not only benefit patients but also hold broader clinical significance. This includes reducing reliance on medications through enhanced pain management, minimizing side effects, and expediting recovery via improved self-reported functional outcomes, thus diminishing the need for extended rehabilitation.11,12
Carpal tunnel syndrome represents a frequently encountered orthopedic condition characterized by hand pain and numbness in the radial three and a half digits, often accompanied by distressing nocturnal symptoms.13 These manifestations can have a significant impact on the patient’s occupational and functional capabilities, particularly when the dominant hand is affected.14 Typically, patients seek orthopedic care due to the dual burden of pain and functional limitations associated with this condition.15 Initial management strategies generally involve conservative approaches, with surgical intervention considered if conservative measures yield no improvement.16,17 Carpal tunnel release surgery is typically performed on a day-case basis, frequently under local anesthesia.18,19
Counseling, typically performed in the clinic visit, is an integral part of the patient’s visit, encompassing comprehensive explanations of the surgical procedure and the corresponding perioperative period.12,20 This educational component aligns with the overarching goal of improving patients’ comprehension and confidence throughout their surgical experience, ultimately leading to enhanced clinical and self-reported outcomes.
Our study aimed to investigate the impact of patient counseling on mitigating intraoperative anxiety levels, alleviating postoperative pain, and enhancing postoperative functional recovery.
Patients and Methods
In our retrospective study, we examined a cohort of 681 patients who had undergone carpal tunnel release surgery at two major hospitals between January 2015 and December 2022 in Jordan. We retrospectively asked these patients for information regarding the adequacy of preoperative patient counseling during their preoperative clinic visits. Additional details about patient’s health profiles were obtained by an authorized access of the patient’s health records. The primary objective of our study was to assess the impact of preoperative patient counseling on various outcome parameters, notably intra-procedural experience, pain levels during the procedure, postoperative analgesic requirements, and self-reported pain relief. Secondary objectives encompassed the identification of patient health profiles, as well as the evaluation of symptomatology and disease presentations.
In our research, the term proper counseling was defined as the counseling provided to patients before undergoing surgery, which sufficiently addressed their concerns, the objective of the surgery, perioperative care, relevant complications, treatment alternatives, and associated benefits. The formulation of this definition has been derived from existing literature that examines the topic of preoperative patient counseling.21–24 Patients who did not receive all these elements and expressed confusion regarding certain aspects were categorized as belonging to the inadequate counseling group for the purpose of our analysis.
The study’s inclusion criteria were formulated to encompass individuals who had undergone primary carpal tunnel release surgery within the predefined study timeframe. Conversely, exclusion criteria were applied to patients who had received surgery beyond the specified study period, those who had undergone revision surgery, individuals with significant cognitive impairments that might compromise the reliability of data, patients who declined participation in the study, and patients who had undergone concurrent hand or wrist procedures. Furthermore, supplementary data, considered pertinent to the research question, were systematically categorized into three distinct domains: patient-related demographic parameters, disease-specific symptomatology, and perioperative variables, contributing to a comprehensive data set for analysis.
The variables related to patients encompassed factors such as age, side of surgery, handedness, and body mass index (BMI), alongside medical comorbidities such as diabetes mellitus and hypertension. Moreover, disease-specific variables included parameters such as hand pain, paresthesia along the distribution of the median nerve, nocturnal discomfort, weakened hand grip, and the utilization of splints.
The perioperative variables under consideration comprised preoperative gabapentin use, the patient’s experience during the procedure, occurrence of heightened pain during the procedure, wound complications, prolonged postoperative analgesic consumption, and time required for maximal improvement. Intraoperative experience was operationally defined as the patient’s subjective state during surgery, categorized as feeling either anxious or irritable, or relaxed and comfortable Intraoperative pain was classified as either exaggerated, necessitating additional local anesthetic for alleviation, or minimal and tolerable. Wound complications encompassed instances of infection, dehiscence, and oozing. Prolonged postoperative analgesic use was delineated as the utilization of analgesia for a duration exceeding one month following the procedure. Time to maximum improvement denoted the period required by patients to resume their customary activities of daily living and function without experiencing pain.
An examination was conducted on a cohort of 1260 patients who underwent carpal tunnel release procedures at our institution from 2015 to 2022. Following application of inclusion and exclusion criteria, a refined cohort of 681 patients emerged. Analysis of our study findings was performed via the Statistical Package for Social Sciences (SPSS) version 23. Quantitative variables such as age, weight, height, and BMI were evaluated using student-test, means and standard deviations. Categorical variables including intra-procedural experience, wound complications, and prolonged postoperative analgesia were assessed utilizing the Chi-square test.
Appropriate Institutional Review Board (IRB) for this study was obtained by the Jordan University Medical Research Office, IRB number (2023/25,128). Appropriate informed consents were obtained from all participants of the study. The Code of Ethics of the World Medical Association (Declaration of Helsinki) was followed while conducting the study. Figure 1 is a flowchart summary of the study.
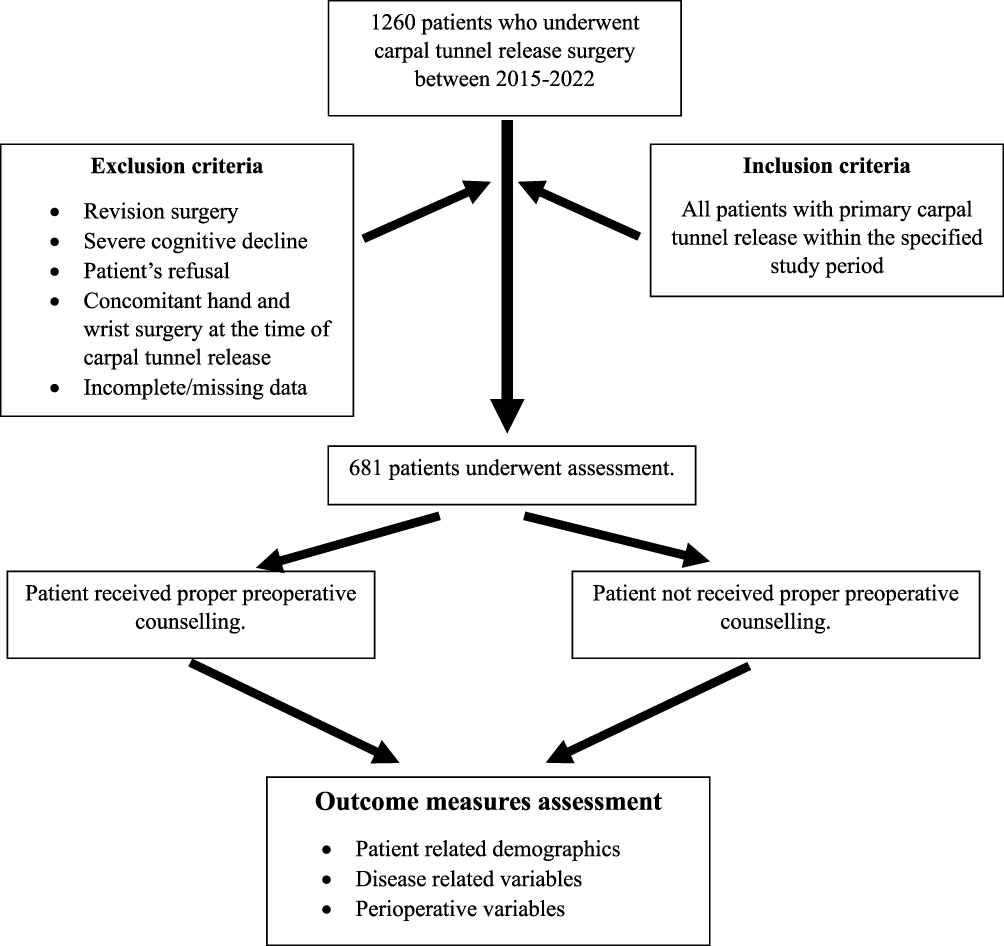 |
Figure 1 Flowchart summary of the study methodology. |
Results
Considering patient demographic characteristics, a predominant proportion of the study cohort consisted of females, accounting for 526 patients (77.2%). The mean age of patients was 52 years. A significant proportion, representing 519 patients (76.2%), were engaged in non-manual occupations according to their occupational status. Approximately two-thirds of the patients underwent carpal tunnel release surgery for their right hand (421 patients or 62%), while the remaining 260 patients (38%) underwent the procedure for their left hand. Furthermore, most individuals within the study cohort exhibited right-hand dominance (92.7%). Smoking was reported by a relatively small subset, comprising 122 patients (17.9%) of the total cohort. (Table 1)
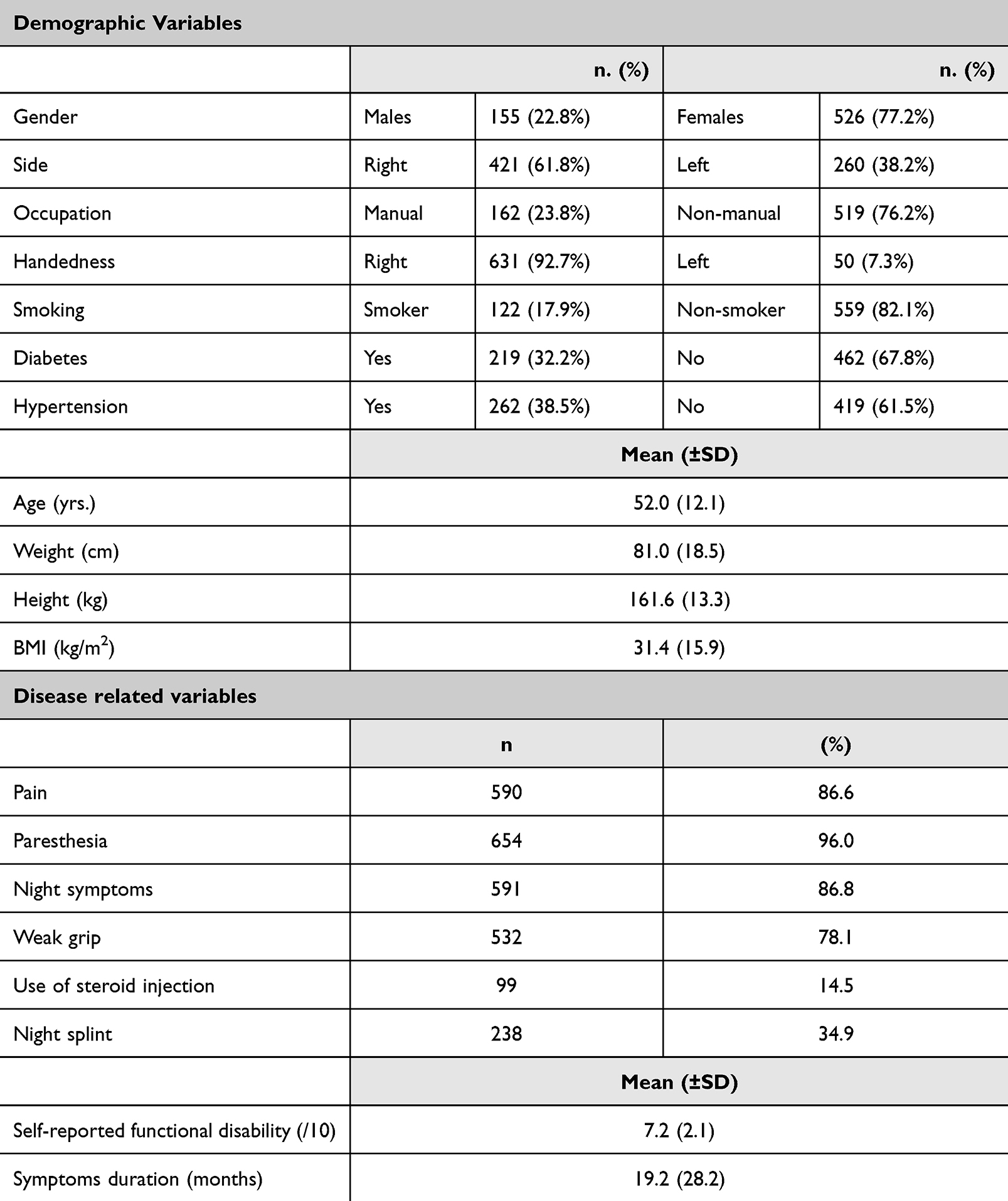 |
Table 1 Summary of the Demographic and Disease Related Variables |
In terms of educational achievement, patients were classified into four educational categories, namely middle school, high school, graduate, and postgraduate. Notably, a substantial proportion of patients fell within the high school and graduate categories, collectively constituting more than 70% of the study cohort. In the context of medical comorbidities, a significant portion of the patient cohort demonstrated specific health conditions: hypertension was prevalent in 419 patients (61.5%), diabetes mellitus was observed in 462 patients (67.8%), and ischemic heart disease was present in 93 patients (13.7%). Furthermore, the cohort exhibited certain anthropometric characteristics, with a mean weight of 81.01 kilograms, a mean height of 161.6 centimeters, and an average body mass index (BMI) of 31.4 kilograms per square meter (kg/m^2) (Table 1).
Regarding the disease symptoms displayed by our cohort, 654 patients (96.0%) reported paresthesia affecting the three and a half radial digits, while 590 patients (86.6%) reported hand pain. Additionally, 591 patients (86.8%) reported significant and disruptive nocturnal symptoms. Furthermore, 532 patients (78.1%) reported diminished grip strength in the affected hand. A subset of the study participants had previously sought conservative treatments before undergoing surgery, with 99 patients (14.5%) opting for steroid injections, 238 patients (34.9%) employing night splints, and 167 patients (24.5%) undergoing gabapentin therapy preoperatively for pain management (Table 1).
In the context of perioperative variables assessment, it is noteworthy that 269 patients (39.5%) reported experiencing anxiety during the release surgery, which was conducted under local anesthesia, while a majority of 412 patients (60.5%) underwent the procedure without significant discomfort. In terms of the quality of preoperative counseling, 333 patients (48.9%) acknowledged having received comprehensive counseling during their preoperative clinic visit, contrasting with 348 patients (51.1%) who reported receiving suboptimal or brief counseling. Encouragingly, a relatively limited number of patients, specifically 46 (6.8%), reported encountering mild wound complications following surgery. Extended use of analgesia after the surgical intervention was reported by 303 patients (44.5%). Notably, prior to the procedure, the cohort exhibited a mean patient-reported hand disability score of 7.2 on a scale of 10, while the mean patient-reported pain relief score was 8.1, denoting substantial improvement after the surgery (Table 2).
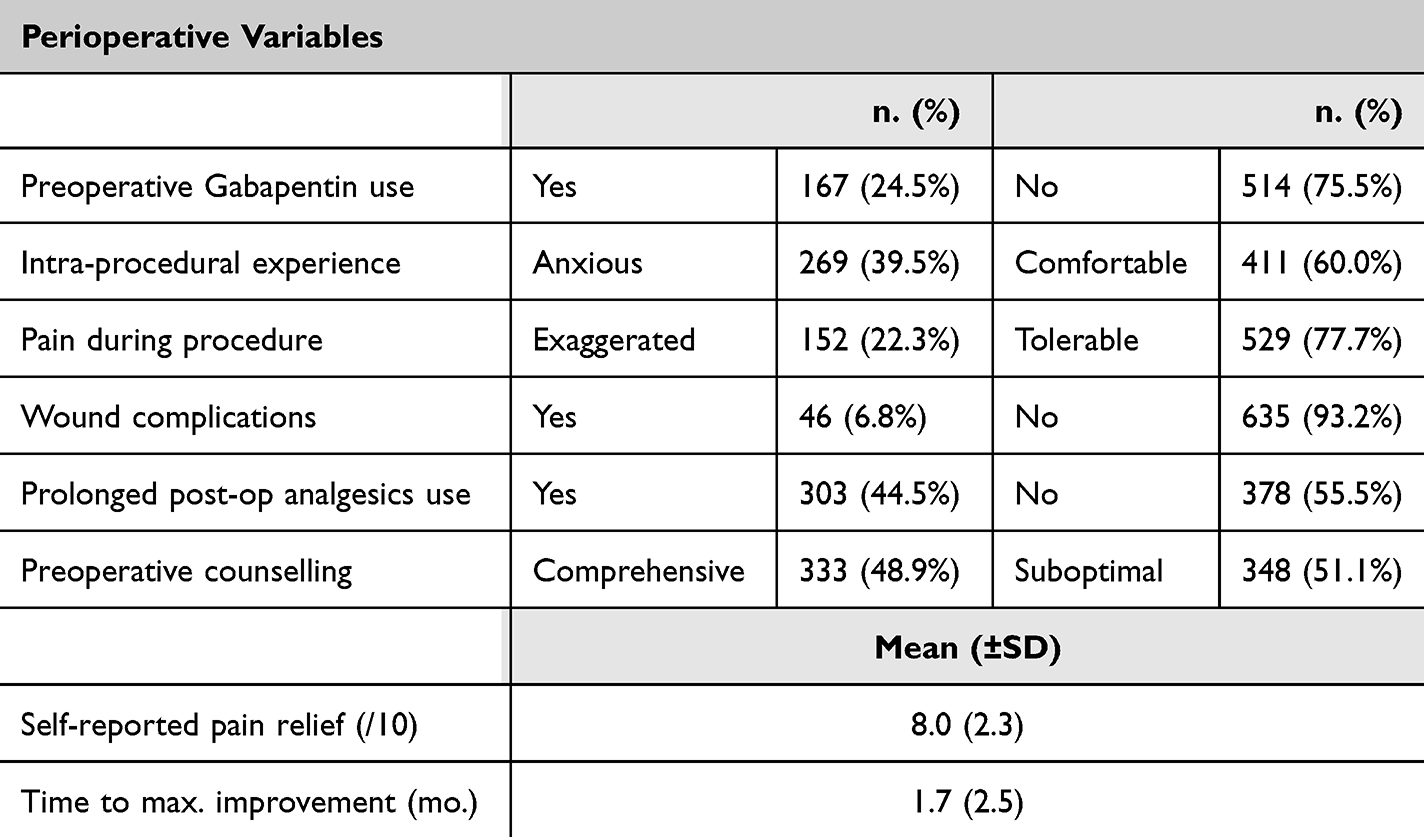 |
Table 2 Summary of the Perioperative Variables |
Analysis utilizing the chi-square tests for categorical variables while plotting the group of comprehensive vs suboptimal counseling yielded the following results: 117 patients in the comprehensive counseling group and 152 in the suboptimal counseling group reported anxiety during the procedure. Conversely, 216 patients who received comprehensive counseling reported comfort during surgery, while 195 in the suboptimal counseling group did so (chi-square = 6.30, p-value = 0.04), indicating the impact of counseling quality on patients’ reported anxiety during surgery. A similar statistical difference was also observed when plotting the two groups in terms of intraoperative increased pain during the procedure, with 59 patients in the counseling group reporting pain vs 93 patients in the suboptimal counseling group (chi-square = 7.6, p = 0.005) (Table 3).
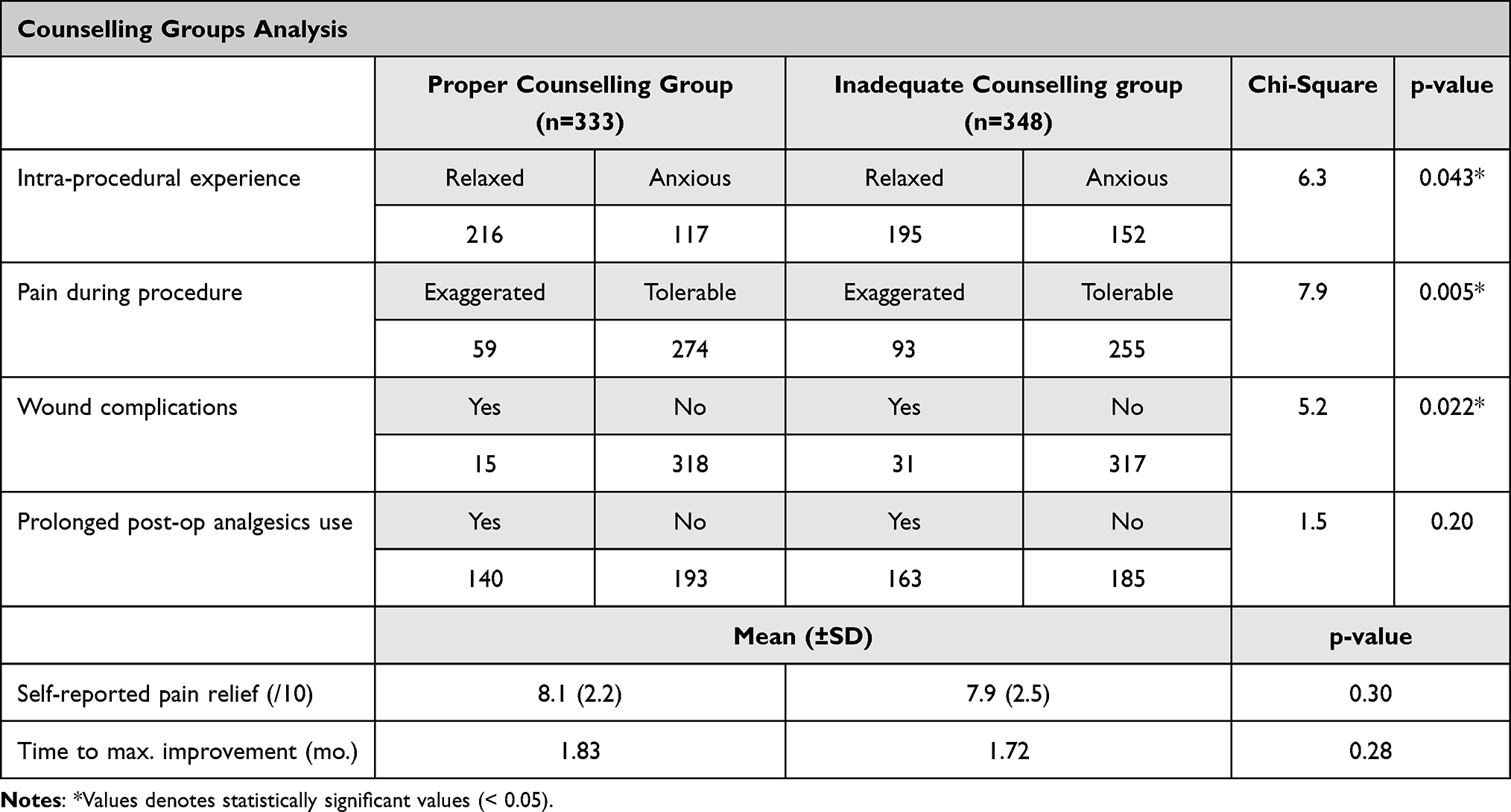 |
Table 3 Comparative Analysis Between Counselling Groups Using the Chi-Square Statistical Test for Categorical Variables Analysis. Student’s t-Test Was Used for Continuous Variables |
Discussion
In this study, we have revealed a clinically significant connection between the provision of comprehensive preoperative counseling in the clinic setting and a remarkable reduction in patient anxiety levels during carpal tunnel release surgery. The process of undergoing any surgical procedure can be a source of substantial distress and apprehension for patients, often leading to exaggerated perceptions of pain and discomfort during the surgery itself. Our findings illuminate the crucial role that preoperative counseling plays in alleviating this anxiety and subsequently improving the overall patient experience during carpal tunnel release surgery.
Proper preoperative education consistently demonstrates significant benefits, as supported by various studies. In the field of cardiac surgery, Boga et al conducted a comprehensive review that highlights the crucial role of preoperative education in enhancing patients’ experiences and overall outcomes.25 The analysis underscores the multifaceted nature of this education, which encompasses the provision of essential healthcare information, equipping patients with coping strategies, and offering vital psychosocial support. The results consistently demonstrate the positive impact of preoperative education in mitigating postoperative complications, shortening hospital stays, and facilitating patients’ recovery. These findings align with our own research, which emphasizes the tangible benefits of preoperative patient education and counseling, particularly in reducing intraoperative anxiety and pain.
Shifting to the domain of abdominal surgery, Brodersen et al investigated the influence of preoperative patient education on postoperative recovery.26 Their thorough exploration, involving a review of 12 relevant studies, reveals a promising landscape. Patients who receive preoperative education experience encouraging trends, including shorter hospital stays, reduced postoperative complications, and decreased psychological distress. These results strongly echo our own findings, which highlight the potential advantages of comprehensive preoperative patient education programs.
However, the landscape of preoperative education is not without its complexities. Tom et al, in their systematic review on preoperative supplementary educational videos, uncover varying impacts on patients’ knowledge, preparedness, satisfaction, and overall psychological and physical well-being.27 While some studies demonstrate significant positive differences associated with educational videos, others present contrasting results, showing no discernible distinctions. Nonetheless, Tom et al advocate for the integration of videos into routine preoperative education, suggesting the need for the evolution of traditional patient education methods.
In the pursuit of enhancing the surgical journey, Balakrishnan et al’s Randomized Control Trial stands as a beacon of clarity, unequivocally affirming the profound impact of preoperative educational counseling on patients’ overall surgical experience. This intervention yields tangible results by instilling patients with higher levels of confidence and satisfaction.28 Similarly, Burgess et al’s systematic review delves into the extensive potential of preoperative education sessions, providing insights into clinical, psychological, and economic outcomes in elective spinal surgery.29 While not every aspect exhibits significant differences, the study underscores the promising potential of preoperative education in spinal surgery. These collective findings align with our own positive results, where effective counseling consistently demonstrates a significant reduction in intraoperative anxiety and pain, emphasizing the multifaceted advantages of comprehensive preoperative education and support.
Effective preoperative counseling is a critical component in the endeavor to minimize postoperative wound complications. Through comprehensive patient education, individuals gain a profound understanding of the surgical process, preoperative requirements, and the expectations for their postoperative care. This heightened awareness empowers patients to become active participants in their recovery journey, ensuring strict adherence to hygiene and wound care protocols. Moreover, preoperative counseling addresses the psychological aspects of patient preparation, assuaging anxiety and stress, which can significantly influence the immune response and subsequent wound healing. The combination of patients who are well-informed and compliant, along with their psychological readiness, highlights the crucial importance of thorough preoperative counseling in significantly decreasing the probability of wound complications after surgery. In our cohort, the group who received comprehensive counseling showed a statistically significant decrease in wound complication rates, a finding that was not previously reported in the literature, according to the author’s best knowledge.
Emphasis and Scope of Investigation: The Significance of a Patient-Centered Approach
This study places paramount importance on exploring the transformative potential of comprehensive preoperative counseling within the context of carpal tunnel release surgery. At its core, this research underscores the critical need for a patient-centered approach in healthcare, particularly in the perioperative context. By acknowledging and recognizing of distinct patient requirements and concerns, we aim to shed light on the profound impact that individualized preoperative counseling can have on patient-reported outcomes, ultimately offering a comprehensive perspective on the surgical experience.
The crux of this study lies in recognizing the profound implications of patient anxiety during surgery. Surgical procedures inherently evoke apprehension, and patients’ anxiety levels can significantly affect their perception of pain and discomfort during surgery. Our investigation illuminates how comprehensive preoperative counseling acts as a potent instrument for alleviating this anxiety, thereby fostering a patient-centered ethos where the patient’s emotional well-being and comfort take precedence in the care process.
Moreover, this study is in perfect harmony with the fundamental tenet of patient-centered care, emphasizing the importance of open and honest communication, well-informed decision-making, and the proactive resolution of patients’ concerns and expectations. By prioritizing the enhancement of the overall surgical experience through patient-centered preoperative counseling, this study bridges the gap between theory and practice, offering tangible insights that healthcare providers can employ to refine their care delivery. Ultimately, our endeavor seeks to amplify the quality of care within surgical settings, yielding practical benefits for both patients and healthcare professionals.
Conclusion
The outcomes of our investigative study elucidate a pivotal aspect of patient-centered care within the perioperative domain, namely, the role of preoperative counseling. Our research delineates a significant association between preoperative counseling and multifaceted enhancements in the patient experience, encompassing reductions in patient-reported intraoperative anxiety, mitigated extremes of pain response, decreased incidence of wound complications, diminished reliance on prolonged postoperative analgesic use, and amplified self-reported pain relief in the postoperative phase.
Bridging Research to Practice: Unaddressed Scientific Inquiries and Clinical Repercussions
The clinical implications of our findings are substantial and hold the promise of enhancing patient care in the perioperative setting, especially within the context of carpal tunnel release surgery. Our research underscores the pivotal role of comprehensive preoperative counseling as an effective tool for reducing patient-reported intraoperative anxiety, mitigating extreme pain responses, lowering the incidence of wound complications, decreasing reliance on prolonged postoperative analgesics, and amplifying self-reported pain relief in the postoperative phase. These outcomes are not only beneficial for individual patients but also bear broader implications for healthcare providers and the healthcare system as a whole. By prioritizing patient-centered care and integrating robust preoperative counseling protocols, clinicians can significantly improve the overall surgical experience, enhance patient satisfaction, and potentially reduce healthcare costs associated with prolonged recovery and complications.
While our study provides valuable insights, several limitations warrant consideration. Firstly, the retrospective nature of our study design precludes the establishment of causality. Future interventional studies are warranted to definitively ascertain causal relationships. Furthermore, our investigation focused solely on carpal tunnel release surgery, necessitating caution in extrapolating these findings to other surgical procedures. The substantial number of excluded patients may have impacted the statistical power of our analysis. Moreover, the absence of specific content analysis of counseling sessions presents a gap for future research to address. Additionally, our study did not directly assess long-term outcomes beyond the immediate postoperative phase. Future research endeavors could investigate the enduring effects of preoperative counseling on patients’ overall well-being and recovery.
Data Sharing Statement
The data that support the findings of this study are available upon appropriate request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgment
We acknowledge the cooperation of the IT office to facilitate the collection of data from electronic and archived files.
Funding
The authors received no financial support for the preparation, research, authorship, and publication of this manuscript.
Disclosure
The authors report no potential conflicts of interest for this manuscript.
References
1. Flach SD, McCoy KD, Vaughn TE, Ward MM, BootsMiller BJ, Doebbeling BN. Does patient-centered care improve provision of preventive services? J Gen Intern Med. 2004;19(10):1019. doi:10.1111/J.1525-1497.2004.30395.X
2. Krist AH, Tong ST, Aycock RA, Longo DR. Engaging patients in decision-making and behavior change to promote prevention. Stud Health Technol Inform. 2017;240:284. doi:10.3233/978-1-61499-790-0-284
3. Samnani SS, Umer MF, Mehdi SH, Farid FN. Impact of preoperative counselling on early postoperative mobilization and its role in smooth recovery. Int Sch Res Not. 2014;2014:1–5. doi:10.1155/2014/250536
4. Cheng JYJ, Wong BW, Chin YHet al. Preoperative concerns of patients undergoing general surgery. Patient Educ Couns. 2021;104(6):1467–1473. doi:10.1016/J.PEC.2020.11.010
5. Agüero-Millan B, Abajas-Bustillo R, Ortego-Maté C. Efficacy of nonpharmacologic interventions in preoperative anxiety: a systematic review of systematic reviews. J Clin Nurs. 2023;32(17–18):6229–6242. doi:10.1111/JOCN.16755
6. Abate SM, Chekol YA, Basu B. Global prevalence and determinants of preoperative anxiety among surgical patients: a systematic review and meta-analysis. Int J Surg Open. 2020;25:6–16. doi:10.1016/J.IJSO.2020.05.010
7. Akkamahadevi P, Subramanian VV. The efficacy of different methods of pre-operative counselling on perioperative anxiety in patients undergoing regional anaesthesia. Indian J Anaesth. 2016;60(1):58. doi:10.4103/0019-5049.174812
8. Ji W, Sang C, Zhang X, Zhu K, Bo L. Personality, preoperative anxiety, and postoperative outcomes: a review. Int J Environ Res Public Health. 2022;19(19):12162. doi:10.3390/IJERPH191912162
9. Ito J. Cochlear implantation: preoperative counselling and postoperative problems. Auris Nasus Larynx. 1994;21(2):98–102. doi:10.1016/S0385-8146(12)80027-7
10. Karimlou V, Charandabi SMA, Malakouti J, Mirghafourvand M. Effect of counselling on health-promoting lifestyle and the quality of life in Iranian middle-aged women: a randomised controlled clinical trial. BMC Health Serv Res. 2019;19(1):1–9. doi:10.1186/S12913-019-4176-0/FIGURES/3
11. Khorfan R, Shallcross ML, Yu B, et al. Preoperative patient education and patient preparedness are associated with less postoperative use of opioids. Surgery. 2020;167(5):852–858. doi:10.1016/J.SURG.2020.01.002
12. Butkus JM, Awosanya S, Scott ER et al. Multimodal analgesia and patient education reduce postoperative opioid consumption in otology. Otolaryngol Head Neck Surg. 2023;169(1):120–128. doi:10.1002/OHN.229
13. Sevy JO, Varacallo M. Carpal tunnel syndrome; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448179/.
14. Genova A, Dix O, Saefan A, Thakur M, Hassan A. Carpal tunnel syndrome: a review of literature. Cureus. 2020;12(3):316–320. doi:10.7759/CUREUS.7333
15. Assmus H, Antoniadis G, Bischoff C. Carpal and cubital tunnel and other, rarer nerve compression syndromes. Dtsch Arztebl Int. 2015;112(1–2):14. doi:10.3238/ARZTEBL.2015.0014
16. Pace V, Marzano F, Placella G. Update on surgical procedures for carpal tunnel syndrome: what is the current evidence and practice? What are the future research directions? World J Orthop. 2023;14(1):6. doi:10.5312/WJO.V14.I1.6
17. Steinberg DR. Surgical release of the carpal tunnel. Hand Clin. 2002;18(2):291–298. doi:10.1016/S0749-0712(01)00011-7
18. Orhurhu V, Orman S, Peck J, et al. Carpal tunnel release surgery- a systematic review of open and endoscopic approaches. Anesthesiol Pain Med. 2020;10(6):1–12. doi:10.5812/AAPM.112291
19. Tulipan JE, Ilyas AM. Carpal tunnel syndrome surgery: what you should know. Plast Reconstr Surgery Glob Open. 2020;8(3):e2692. doi:10.1097/GOX.0000000000002692
20. Sanati KA, Mansouri M, MacDonald D, Ghafghazi S, MacDonald E, Yadegarfar G. Surgical techniques and return to work following carpal tunnel release: a systematic review and meta-analysis. J Occup Rehabil. 2011;21(4):474–481. doi:10.1007/S10926-011-9310-8
21. Raju B, Reddy K. Are counseling services necessary for the surgical patients and their family members during hospitalization? J Neurosci Rural Pract. 2017;8(1):114. doi:10.4103/0976-3147.193551
22. Liaqat Adam Albalushi S, Khraim F, Al-Tawafsheh AMM, Forgrave D. “Effect of pre-operative education on post-operative pain management among adult patients undergoing elective surgery: an integrative review”. Australian College of Perioperative Nurses. 2023;2023:1. doi:10.26550/2209-1092.1246
23. Ziegelmann M, Köhler TS, Bailey GC, Miest T, Alom M, Trost L. Surgical patient selection and counseling. Transl Androl Urol. 2017;6(4):609. doi:10.21037/TAU.2017.07.19
24. Balakrishnan S, Kurian FS, Jojo JE. ” Effect of preoperative educational counselling about routine elements of peri-operative care on patient’s experience through their first surgical journey: a randomised control trial”. medRxiv. 2023;2023:1. doi:10.1101/2023.01.09.23284099
25. Boga SM. The healing power of preoperative education in patients undergoing cardiac surgery. J Clin Nurs Pract. 2020;2(3):1–3.
26. Brodersen F, Wagner J, Uzunoglu FG, Petersen-Ewert C. Impact of preoperative patient education on postoperative recovery in abdominal surgery: a systematic review. World J Surg. 2023;47(4):937–947. doi:10.1007/S00268-022-06884-4/TABLES/4
27. Tom K, Phang PT. Effectiveness of the video medium to supplement preoperative patient education: a systematic review of the literature. Patient Educ Couns. 2022;105(7):1878–1887. doi:10.1016/J.PEC.2022.01.013
28. Matti H. Uber die behandlung der navicularfracture und der refractura patellae durch Plombierung mit spongiosa. Zentralbl Chir. 1936;1997:1.
29. Burgess LC, Arundel J, Wainwright TW. ThE effect of preoperative education on psychological, clinical and economic outcomes in elective spinal surgery: a systematic review. Healthcare. 2019;7(1):48. doi:10.3390/HEALTHCARE7010048
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Analysis of a New Device-Assisted Mini-Incision Versus Conventional Surgery for Carpal Tunnel Syndrome: A Retrospective Study of 109 Cases
Guo T, Li C, Tian D, Gao R, Yu K, Sun N, Yang J, Bai J
Therapeutics and Clinical Risk Management 2025, 21:511-522
Published Date: 23 April 2025