Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Optimizing Multidisciplinary Workforce Sustainability: The Interplay of Job Strain, Workplace Hazards, and Organizational Support on Work Engagement Among Registered Nurses and Practical Nurses and Nursing Assistants
Authors Assavanopakun P, Surawattanasakul V ![]() , Kiratipaisarl W, Siriratchadanan T, Chaithong C, Teplaor T, Thongon N
, Kiratipaisarl W, Siriratchadanan T, Chaithong C, Teplaor T, Thongon N
Received 24 February 2026
Accepted for publication 24 June 2026
Published 14 July 2026 Volume 2026:19 602020
DOI https://doi.org/10.2147/JMDH.S602020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David C. Mohr
Pheerasak Assavanopakun,1,2 Vithawat Surawattanasakul,1,2 Wuttipat Kiratipaisarl,1 Thanwarat Siriratchadanan,3 Chitsanupong Chaithong,3 Thunwalai Teplaor,3 Niti Thongon3
1Department of Community Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 2Environmental and Occupational Medicine Excellence Center, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand; 3Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Correspondence: Vithawat Surawattanasakul, Department of Community Medicine, Faculty of Medicine, Chiang Mai University, 110 Intawaroros Road, Si Phum, Muang, Chiang Mai, 50200, Thailand, Email [email protected]
Purpose: To examine the prevalence and association between work stress and work engagement among healthcare personnel.
Patients and Methods: A cross-sectional study was conducted using questionnaires among registered nurses (RNs) and practical nurses and nursing assistants (PNNAs) in a university hospital. The survey comprised three parts: 22 items on general information, 54 items from the Job Content Questionnaire assessing work stress, and 17 items from the Thai version of the Utrecht Work Engagement Scale 17 assessing work engagement. Multivariable linear regression was applied to determine factors associated with total work engagement scores.
Results: Among 694 participants (506 RNs, 188 PNNAs; 91.6% female; mean experience: 13.2 years), 25.7% had high-strain jobs, 61.0% high demand, 39.9% low control, and 51.6% high hazards. PNNAs scored significantly higher than RNs in median overall engagement (76 (59, 87) vs. 67 (51, 81); p < 0.01) and all subdomains: vigor (28 vs. 27; p = 0.02), dedication (21.5 vs. 18; p < 0.01), and absorption (25 vs. 23; p < 0.01). Regression showed high-strain jobs reduced engagement for RNs (β = − 12.2, 95% CI: − 16.0, − 8.5) and PNNAs (β = − 16.7, 95% CI: − 24.6, − 8.9). Greater support increased engagement for RNs (β = 5.0, 95% CI: 1.2, 8.8) and PNNAs (β = 9.2, 95% CI: 1.8, 16.6). High workplace hazards further decreased engagement specifically in RNs (β = − 3.9, 95% CI: − 7.2, − 0.6).
Conclusion: RN experienced higher job stress and hazards, while PNNAs demonstrated greater engagement. Strengthening organizational support may mitigate stress and enhance engagement, guiding strategies to improve work environments and personnel well-being.
Keywords: work-related stress, work engagement, registered nurse, practical nurses and nursing assistants
Introduction
Work-related stress is defined by the World Health Organization as a response to work demands and pressures that exceed an individual’s knowledge, abilities, and capacity to cope.1 It stems from interrelated factors, including the nature of work, organizational management, and the workplace environment.2 While optimal pressure can enhance motivation and productivity, excessive stress surpasses individual thresholds, adversely affecting employee health and job effectiveness.2–4
Healthcare professionals are highly vulnerable to occupational stress due to daily clinical responsibilities and persistent exposure to critical patient situations.5 Key predictors include heavy workloads, inadequate resources, workplace conflicts, and low job satisfaction.6 Within this sector, the nursing profession encompasses diverse roles such as registered nurses (RNs) and practical nurses and nursing assistants (PNNAs), distinguished by their scopes of practice and training durations.7 Despite working within the same multidisciplinary setting, the occupational descriptions of RNs and PNNAs might exhibit varying levels of work stress. Registered nurses have more specific scopes of practice and longer training periods, which might face higher psychological distress.8,9 In contrast, nursing assistants, who primarily provide supportive care, are documented to experience greater physical labor pressures, including high frequencies of manual patient handling and repetitive physical tasks.10 Such occupational stress compromises service quality, decreases patient satisfaction, and increases turnover.11 The workplace constitutes a statistically significant source of stress for employees owing to excessive workloads, psychological harassment, work procedures, encounters with patients’ families, professional and administrative obligations, resource limitations, and insufficient management support.12 Work-related stress can also lead to burnout, diminished job satisfaction, and reduced work engagement among employees within the organization.13,14 Work engagement is characterized as a positive and fulfilling psychological state related to work, encompassing three dimensions: vigor, which reflects energy; dedication, indicating involvement; and absorption, representing a state of happiness in work activities.15 Existing literature indicates that diminished work engagement correlated with a decline in the safety and quality of clinical operations, encompassing lower levels of care quality, decreased patient satisfaction, heightened adverse events, and a contagion effect on patients. The operational and financial viability of healthcare companies was related to heightened turnover intentions, absenteeism, lateness, and negative cultural contagion.16,17
Tertiary hospitals represent high-risk environments for stress due to their complex, multi-departmental structures18 making nursing a profession highly susceptible to compassion fatigue.19 While work strain and low engagement are global challenges, these issues are notably prevalent within the healthcare systems of Southeast Asia. Studies conducted in the Philippines and Vietnam investigated job-related aspects and work engagement among nurses, revealing concerns associated with administrative components and their consequent effects on patient care outcomes.20,21 In Thailand, empirical evidence indicates that approximately 15–20% of hospital personnel experience significant job stress, which is often associated with critical work factors such as nursing shortages, extended shifts, insufficient income, and poor social support.22,23 Investigating a multidisciplinary nursing workforce in Thailand addresses a critical regional gap where empirical evidence is limited. Thus, this study examines the prevalence of occupational stress, degrees of work engagement, and the relationship between these variables among healthcare professionals in a medical university hospital.
The study’s theoretical framework is grounded in Karasek’s model of occupational stress, which balances psychological demands against decision latitude,24 to assess diverse occupational risks. Additionally, the Job Demands-Resources theory conceptualizes work engagement as a distinct state independent of burnout.25,26 Work engagement should be regarded solely as being separate from burnout. This concept posits that, theoretically, an employee who is not experiencing burnout may exhibit either high or low levels of engagement, whereas an engaged employee may demonstrate either high or low levels of burnout. We evaluate occupational stress and work engagement through questionnaires rooted in a theoretical framework to investigate and clarify the association between these variables among study participants.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted via an on-site survey from 15 April 2023 to 31 May 2023. This study utilized a total population sampling approach, where all eligible RNs and PNNAs across all clinical and administrative departments of the participating university hospital were invited to participate. Of the total distributed questionnaires, a response rate of approximately 30% was achieved. A survey was distributed to 2329 RN and PNNAs who have been employed as the hospital permanent workers for at least 6 months. The sample size determination reveals that a minimum of 532 samples must be assembled, according to calculations by the n4Studies application regarding finite sample mean estimation at Confidence interval was set to 95% (alpha 0.05) without cluster sampling with a pre-specified Utrecht Work Engagement Scale.
(UWES-17) score consisting of standard deviation of 1.30 and absolute error (d) of 0.1. Of 883 responses, 694 (78.6%) participants completed all the questions. The two target occupational groups within the multidisciplinary workforce are defined based on national healthcare regulations in Thailand. RN possess a minimum of a four-year bachelor degree in nursing, are licensed by the Thailand Nursing and Midwifery Council, and are legally responsible for advanced clinical judgment, patient care management, and administrative supervision. The secondary comparative group is collectively designated as PNNAs. Practical nurses complete a formalized one-year certificate program in practical nursing under accredited institutions, operating within a structured supportive clinical scope under the supervision of registered nurses. Nursing assistants typically undergo short-term vocational training lasting from three to six months, focusing primarily on basic patient hygiene, ambulation assistance, and routine physical labor tasks. These distinct educational requirements and operational boundaries underpin the rationalization of evaluating variations in job strain, decision latitude, and workplace hazards between the two cohorts.7
Questionnaire
The participants were asked about their Socio-demographic, working conditions, stress from work, and work engagement. The questionnaire consisted of four sections:
Part 1: Socio-demographic of the participants such as age, gender, education, marital status, number of children, financial status, physical and mental health conditions, and average nightly sleep duration.
Part 2: Working conditions such as job position, type of employment, work experience, patient contact.
Part 3: Thai Job Content Questionnaire (JCQ) 54 items, developed by Pitchaya Parkthongsuk et al.27,28 To ensure linguistic and cultural appropriateness, the research instruments underwent a rigorous adaptation process. The original English scales were translated into Thai using a standard forward-and-backward translation procedure by independent bilingual translators. Subsequently, the Thai version was evaluated for content validity and cultural relevance by a panel of nursing and healthcare management experts. Items were refined based on expert consensus to ensure that the terminology aligned with the daily practice and organizational structure of Thai university hospitals. The questionnaire is divided into 6 areas:
- Job control refers to the perception of one’s ability to control work and the freedom to make decisions regarding various work-related matters (Questions 1–11).
- Regarding psychological job demands, it refers to the mental perception related to the responsibilities of performing the job (Questions 12–23).
- Regarding physical job demands, it refers to the physical perception related to the responsibilities of the job (Questions 24–29).
- Regarding job security, it refers to the perception of stability in the job being performed (Questions 30–34).
- Social support refers to the perception of support in job performance from supervisors (supervisor support) and co-workers (co-worker support) (Questions 35–42).
- Hazard at work refers to the perception of risks or dangers that may arise from performing tasks (Questions 43–54).
The questionnaire predominantly comprises a Likert scale. Questions 1–42 utilized four Likert scales as follows. Strongly agree (4 points), agree (3 points), disagree (2 points), and strongly disagree (1 point). For questions 43–54, which are evaluations of hazards or occupational risks, the responses are classified into three tiers. The three levels are “no problem,” “some/a few problems,” and “many problems,” corresponding to scores of 1, 2, and 3, respectively.
Assessing occupational stress and the prevalence of work-related stress in accordance with the Job Demand-Control Model. The model created by Karasek will take into account the scores derived from job control or decision-making authority (questions 1–11) and psychological job demand (questions 12–23). By dividing the scores obtained from these two components into 2 groups, high and low, using the cut point at the 50th percentile. We utilized the established cut off threshold reported the previous study in similar setting. The JCQ were categorized as high in the following cut off threshold. Job control (≥17), psychological demand (≥34), physical demand (≥15), job security (≥16), social support at work (≥36) and hazards at work (≥17).29 Can assess work-related stress in four types as follows.
- Low-strain job or relaxed job: high job control low psychological job demand
- Passive job: low job control, low psychological job demand
- Active job: high job control, high psychological job demand
- High-strain job: low job control, high psychological job demand
The content of this questionnaire section has already passed the validity test. Internal consistency reliability: Cronbach’s alpha coefficient was adequate for decision latitude scale (0.82), psychological demand (0.76), social support (0.81), physical demand (0.71), and work hazards (0.86) but moderately adequate for job security (0.55). Permission was obtained from the original developers to include it in the study’s questionnaire.27,28
Part 4: Work engagement: The Utrecht Work Engagement Scale, Thai language version, (UWES-17-TH). The UWES, consisting of 17 items, uses a Likert-type response format with scores ranging from 0 (never) to 6 (always, every day). Three subscales are included: vigor (6 items), dedication (5 items), and absorption (6 items).30 The Utrecht Work Engagement Scale, Thai language version, has already passed the validity test, with Cronbach’s alpha coefficient for overall work engagement as 0.93, absorption as 0.79, dedication as 0.88, and vigor as 0.84.31 The interpretation of the tool used will use the median as the criterion. If the score is lower than the median, it will be categorized as low. If the score is higher than or equal to the median, it will be categorized as high.
Statistical Analysis
All statistical analyses were conducted using statistical packages in the Stata software version 18.0 (StataCorp, TX, USA). Descriptive statistics were provided by frequency and percentage for categorical data, a mean with standard deviation (SD) for the parametric data and a median with interquartile range (IQR) for the non-parametric data. One-sample Kolmogorov–Smirnov test of normality was used to assess the outcome distribution for normality including UWES-17 and three subdomains. The non-parametric rank-sum test (Mann–Whitney U-test) was utilized to evaluate the statistical significance of between-group differences in total work engagement sum scores and its respective subdomains (vigor, dedication, and absorption) between RNs and PNNAs. Exploratory analysis using a multivariable linear regression with robust standard error correction was performed to determine factors associated with UWES-17 sum of scores and its subdomains: vigor, dedication, and absorption. The paper questionnaire was distributed through the head of each department office and manually entered by trained personnel into spreadsheet software by two person and cross-validate for any discrepancies. All discrepancy was traced back to hardcopy and resolved for any typographic error in data entry. Extreme values were prevented by specifying ranges for ages (20–60 years old), sleep (2–12 hours) in both data gathering and entry process; value outsides the range were treated as missing values. No missing data imputation was made due to missing completely at random assumption (MCAR), identified using sensitivity analysis of samples: 1) complete response (n = 506) and 2) partially completed response across three subdomains of UWES-17 (n = 516 to n = 518). The results of this study were reported in accordance with the strengthening of the reporting of observational studies in Epidemiology (STROBE) checklist. All statistical analyses were two-sided, and a p-value ≤ 0.05 was considered statistically significant.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki guidelines, and the protocol was approved by the Research Ethics Committee, Faculty of Medicine, Chiang Mai University, Thailand (No. 120/2023). All participants read the Informed Consent form carefully and provided their consent before starting to complete the questionnaire. The study objectives and procedures were clearly explained, and participants were informed of their right to withdraw at any time.
Results
The majority of participants were women (636, 91.6%), held a bachelor’s degree (460, 66.3%), were single (416, 59.9%), and had no children (447, 64.4%). Most reported no underlying physical (469, 67.6%) or psychiatric (676, 97.4%) conditions and described their financial status as more than adequate (360, 51.9%). The average sleep duration was 6 hours per night, and mean work experience was 13 years. Statistically significant differences between subgroups were observed in marital status (p = 0.011), parenthood (p = 0.013), and sleep duration (p = 0.002). Highly statistically significant differences were found in education level, financial status, and employment type (p < 0.001) (Table 1).
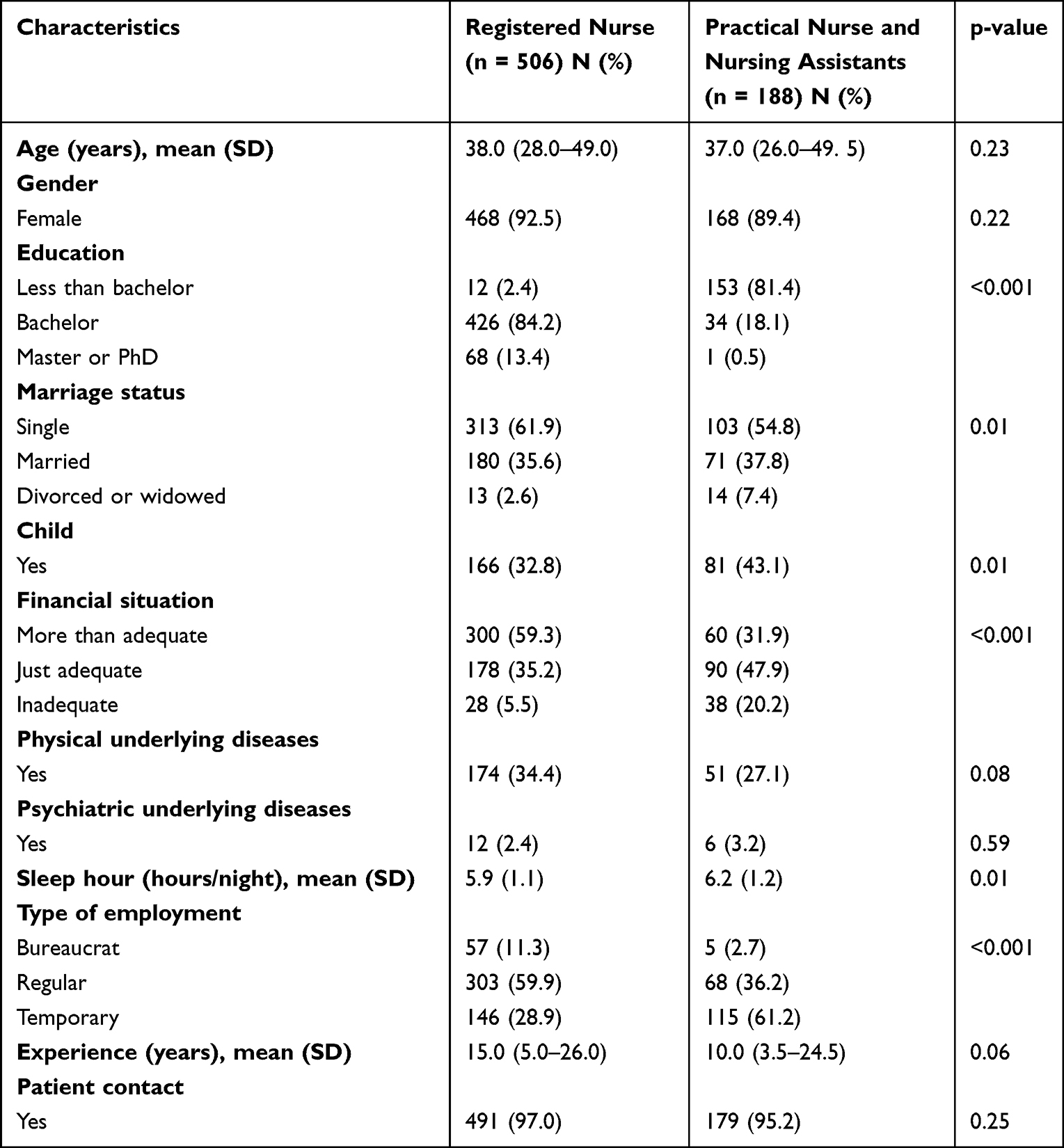 |
Table 1 Sociodemographic Characteristics and Working Conditions of Eligible Participants |
Participants reported low job control (277, 39.9%), high psychological demand (423, 61%), high physical demand (434, 62.5%), low support (146, 21%), and high job hazard (358, 51.6%) (data not shown). Comparison of Job Content Questionnaire results showed statistically significant differences in psychological demand, physical demand, and job hazard between RN and PNNAs groups (Figure 1).
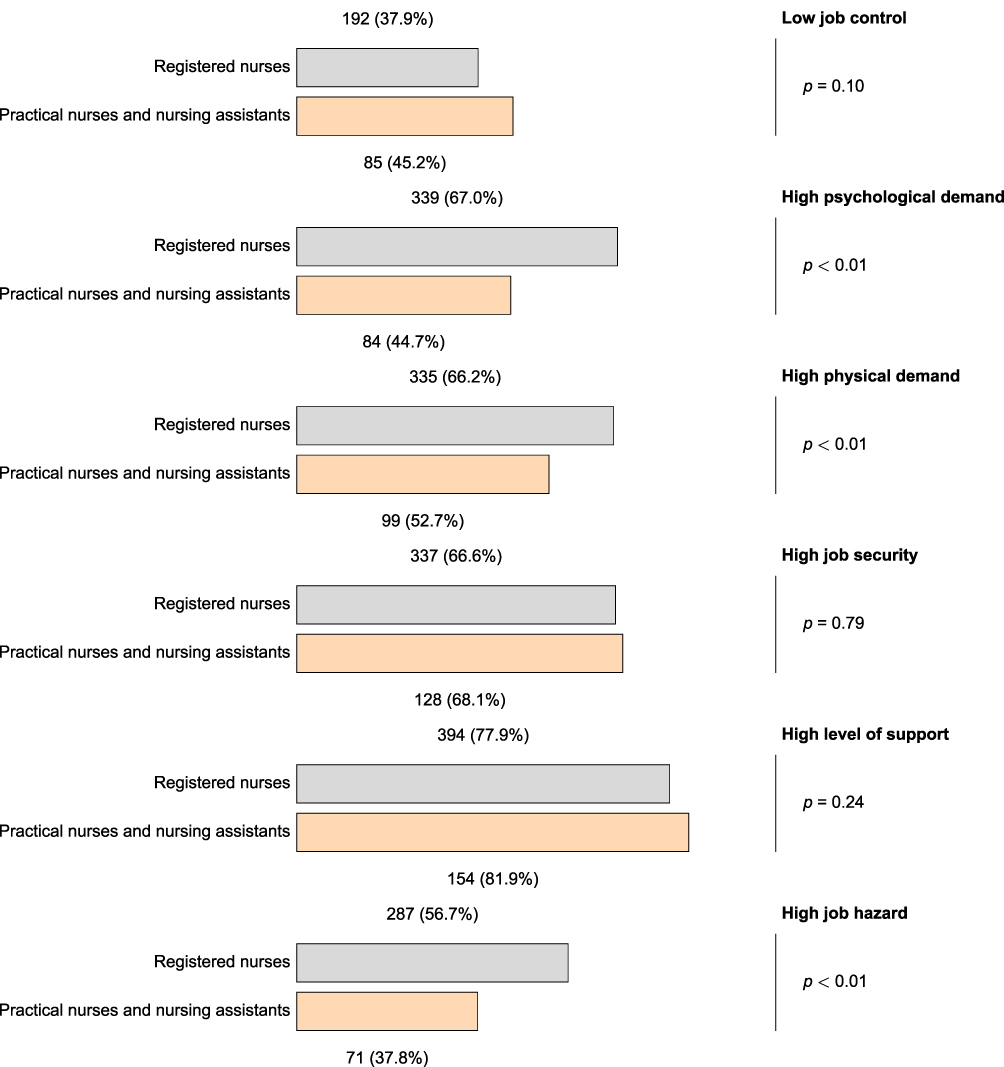 |
Figure 1 The descriptive bar plots demonstrate subdomains of the 54-item Job Content Questionnaire (JCQ) across occupation: 1) registered nurses (gray) and 2) practical nurses and nursing assistants (Orange); descriptive statistics presented in frequency and percentage, n (%); p-value was derived from the Chi square test of two independent proportions. |
Using the job control-demand matrix, most participants (253, 41.3%) were classified as having an Active job, followed by High-strain (157, 25.7%), Relaxed (127, 20.8%), and Passive (75, 12.3%) jobs (data not shown). The detailed distribution and descriptive parameters of occupational categories for both RN and PNNAs are presented comprehensively in Figure 2.
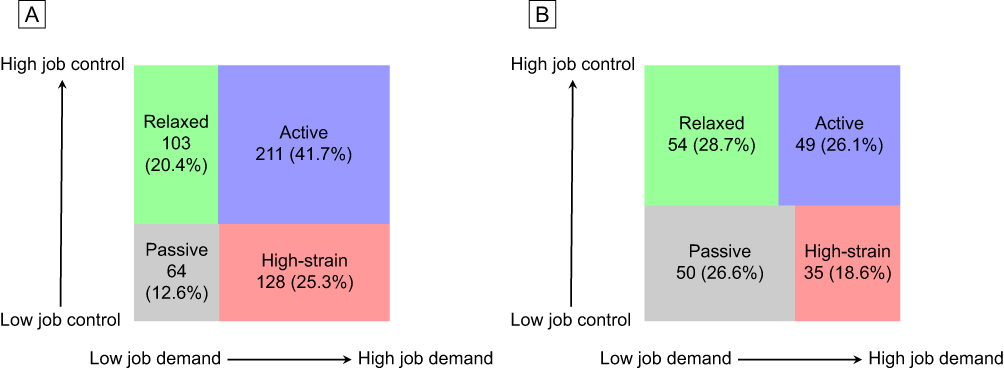 |
Figure 2 The descriptive mosaic plots demonstrate four phenotypes of job control-demand matrix: 1) active (blue), 2) high-strain (red), 3) relaxed (green), and 4) passive (gray); descriptive statistics presented in frequency and percentage, n (%); (A) registered nurses (n = 506); (B) practical nurses and nursing assistants (n = 188). |
For work engagement, One-sample Kolmogorov–Smirnov test of normality was used on the data of UWES-17 and three subdomains resulting in presence of non-normality (p < 0.01). PNNAs exhibited a significantly higher overall work engagement sum score compared to RNs (Median: 76 (Q1=59, Q3=87) vs 67 (Q1=51, Q3=82), p < 0.01). Consistent with the global score, statistically significant differences were observed across all three subdomains. Specifically, PNNAs reported higher scores than RNs in vigor (Median: 28 (Q1=24, Q3=31) vs 27 (Q1=21, Q3=30), p = 0.02), dedication (Median: 21.5 (Q1=14.5, Q3=26) vs 18 (Q1=12, Q3=24), p < 0.01), and absorption (Median: 25 (Q1=18, Q3=30) vs 23 (Q1=16, Q3=28), p < 0.01). Between-group comparisons showed statistically significant differences in overall engagement, dedication, and absorption (Figure 3).
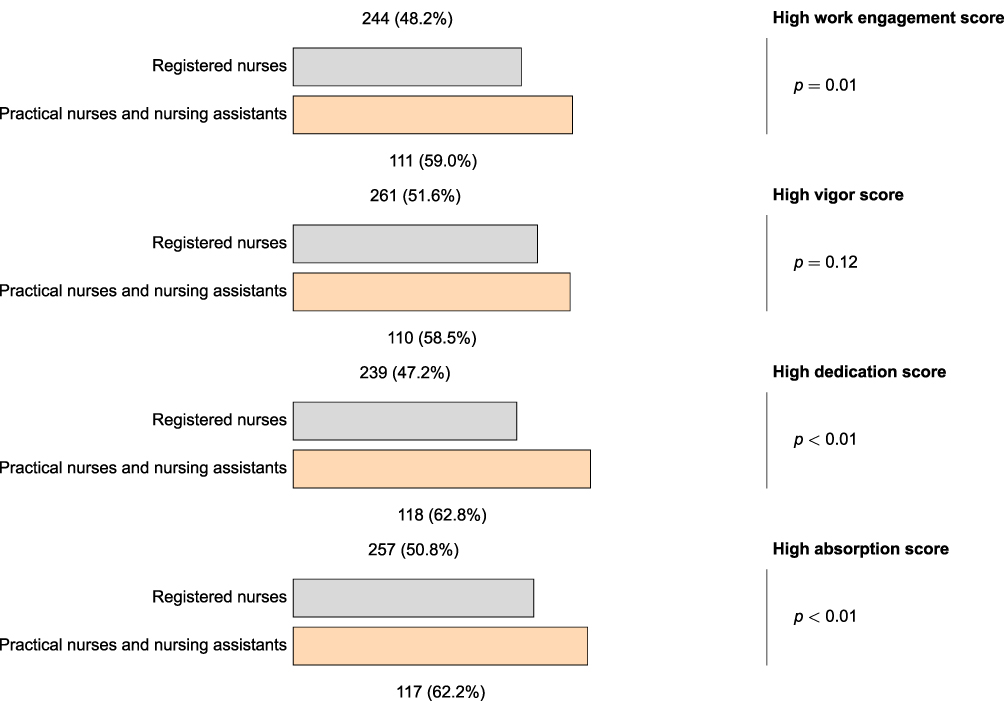 |
Figure 3 The descriptive bar plots demonstrate subdomains of the 17-item Utrecht Work Engagement Scale (UWES-17) across occupation: 1) registered nurses (gray) and 2) practical nurses and nursing assistants (Orange); descriptive statistics presented in frequency and percentage, n (%); p-value was derived from the Chi square test of two independent proportions. |
Multivariable linear regression identified factors associated with work engagement and its subdomains (Tables 2 and 3). High-strain jobs were linked to lower engagement across all domains in both groups, while high support was associated with higher engagement and vigor. Among PNs, older age, high job hazard, and high physical demand were associated with lower engagement or dedication. In the PNNAs group, high job hazard reduced absorption scores, whereas high support increased dedication scores. The completed response analysis is presented in Tables S1 and S2.
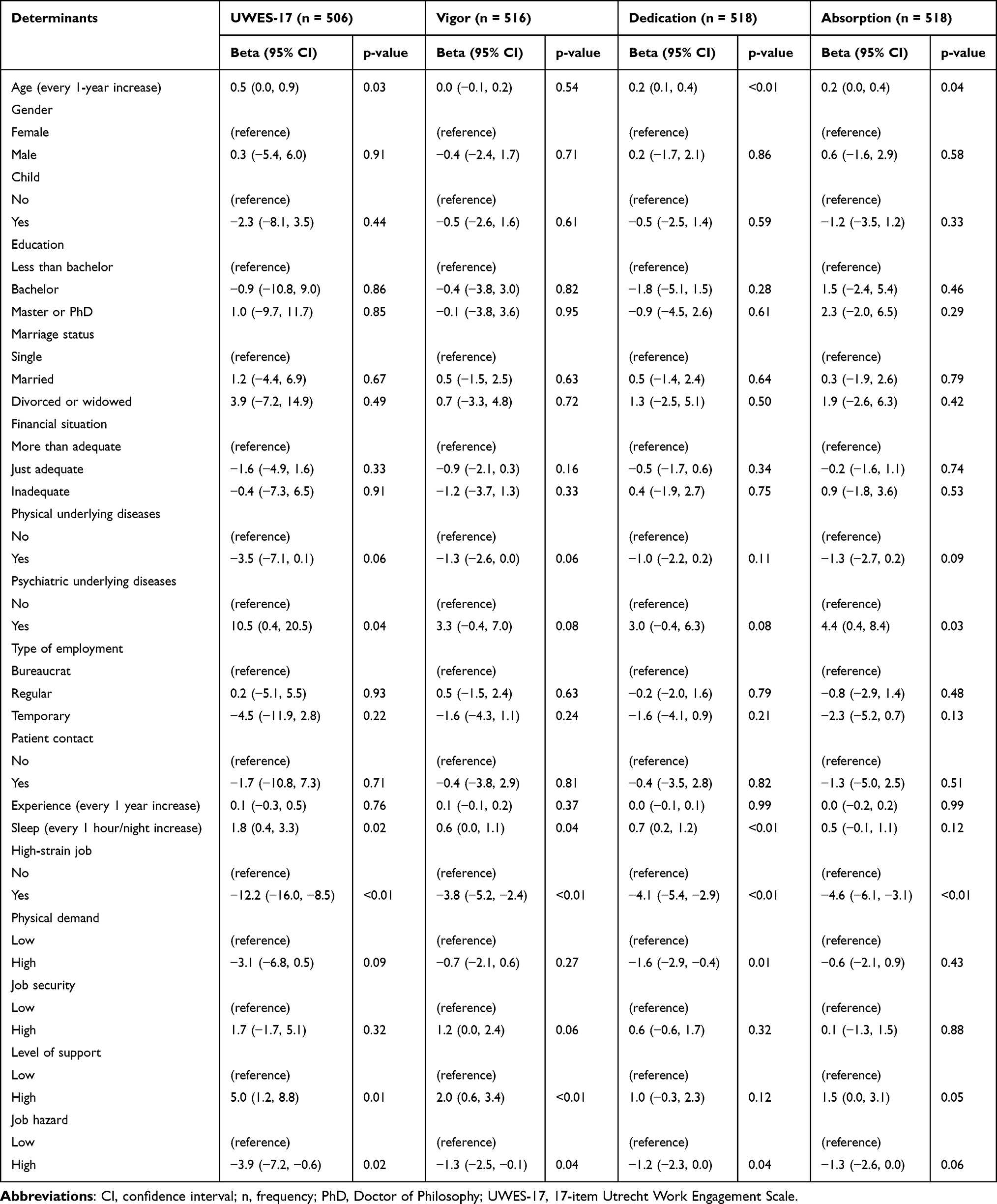 |
Table 2 Multivariable Linear Regression Demonstrating the Association of Determinants with Work Engagement Score and Its Subdomains in Registered Nurses |
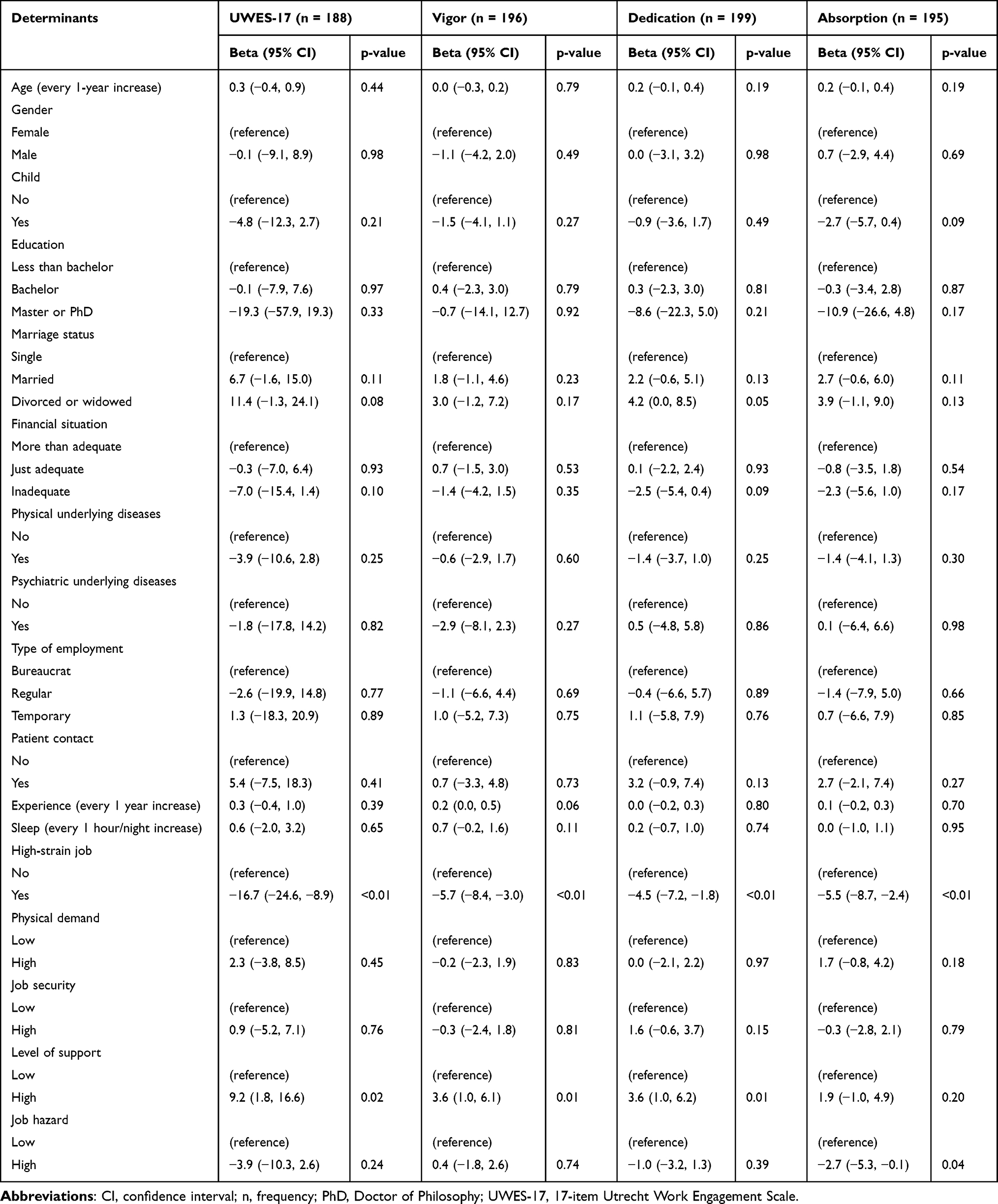 |
Table 3 Multivariable Linear Regression Demonstrating the Association of Determinants with Work Engagement Score and Its Subdomains in Practical Nurses and Nursing Assistants |
Discussion
The study’s first objective revealed that the RN study population predominantly occupied active and high-strain jobs, collectively comprising over half of the RN cohort. This indicates a higher proportion of high-strain jobs compared to previous findings in similar and different Thai hospital contexts, including urban tertiary and private institutions.29,32,33 Conversely, the PNNAs group was characterized mostly by relaxed and passive jobs. Despite sharing direct patient care responsibilities, considerable disparities in job characteristics are obvious between these populations. These RN job characteristics align with prior research indicating that RNs rank highest among professions for job stress.34 Additionally, different sleep durations between groups are associated with work-related stress, as inadequate sleep relates to physiological stress in the workplace.35
Regarding work engagement, over half of all participants exhibited a high overall level, though the proportion was lower within the RN group than the PNNAs group. Statistically significant differences were found in the proportions of high total, dedication, and absorption scores between the two cohorts. This high engagement level aligns with previous evidence among health professionals.13 The distinct dedication and absorption scores in the RN group compared to the PNNAs group relate to differing inherent decision-making processes,36 since decision latitude is associated with dedication, which in turn links to absorption.37
The secondary objective investigated the relationship between work stress and engagement. In both cohorts, high-strain jobs significantly associated with lower scores in overall work engagement and all subdomains. Elevated demands in high-strain jobs serve as a significant mediating factor for adverse health outcomes, with burnout subsequently demonstrating a negative association with engagement.38,39 Conversely, high support significantly associated with increased overall engagement and vigor, consistent with studies showing job demand and control positively correlate with engagement.40,41 Within the various socio-demographic and professional traits linked to engagement,42 only age and sleep hours showed significant associations among RNs. This aligns with research proving age positively correlates with nurses’ engagement.21,43 Conversely, sleep duration lacked sufficient evidence to establish a direct link with engagement; only one study indicated that Daylight Saving Time linked to reduced engagement through decreased sleep quality rather than length.44 Nonetheless, sleep duration reflects overall well-being and quality of life,45 both positively connected to engagement.42 The greater sleep amount observed here may suggest improved sleep quality, contributing to a positive relationship with engagement among RNs.
Our findings indicate high physical demands negatively associated with RNs’ dedication, showing that elevated physical burdens coexist with diminished professional dedication. Additionally, high support significantly correlated with nearly all engagement dimensions, except for dedication and absorption among PNNAs. High workplace hazards linked to almost all engagement dimensions in RNs, except for a marginal correlation with absorption; conversely, in PNNAs, hazards significantly associated with absorption. These variations are linked to distinct hazards, psychological demands, physical demands, and workloads between groups, as heavy workloads and hazards demonstrate strong associations with diminished engagement.46 Workplace hazards affect work engagement by depleting employees’ cognitive and emotional resources, prompting a transition from a focus on development to self-preservation. Psychological theories indicate that adverse situations serve as stressors, increasing burnout and diminishing job satisfaction.47,48 Furthermore, physical demands involving non-ergonomic activities, such as prolonged high-risk procedures, heavy lifting, or awkward postures49,50 explain why participants facing high physical burdens exhibit poor overall dedication. To improve engagement, strategies must focus on reducing stress, optimizing physical demands, minimizing hazards through occupational monitoring, and strengthening team support. Additionally, implementing Decision Support Systems can mitigate psychological demands by addressing communication and decision-making obstacles.51–53
These factors relate to varying individual perceptions of job demands54 alongside organizational factors where disparate management systems connect with employee perceptions.55 Given the complexity of examining work involvement via institutional frameworks, future applications of advanced theories, such as the Person-Situation Approach, Multilevel JD-R Theory, or healthcare-specific frameworks like Convergent Care Theory, may yield deeper insights into the association between occupational stress and work engagement.56,57
This study’s strength lies in its pioneering exploration of psychosocial outcomes among healthcare personnel working in the complex context of a medical university hospital. This research offers insights into work-related stress levels and work engagement, defined in detail in each module, and focuses on comparing specific job groups, in contrast to other studies that focus on a broad workforce. Furthermore, our findings can be utilized to formulate policies and cultivate an organizational culture that enhances employee job engagement. Several limitations must be acknowledged when interpreting this study. First, the cross-sectional design precludes establishing causality and introduces potential reverse causality. For instance, staff with lower baseline engagement might experience decreased situational awareness, increasing their susceptibility to hazards and administrative strain over time. Future longitudinal research is required to clarify these temporal directions. Second, profession heterogeneity and non-random recruitment mean the sample may not fully represent the institutional population. Notably, the low response rate (29.8%) introduces potential non-response and self-selection bias. Overworked or severely burned-out staff likely lacked time to participate, potentially biasing work engagement estimates upward. Therefore, these descriptive findings warrant cautious interpretation. Third, relying entirely on self-report questionnaires (JCQ and UWES) subjects the findings to information, social desirability, and common method biases, which may distort the true relationships among variables. Fourth, this study lacked individual-level data on shiftwork configurations, failing to fully isolate scheduling-related stress. In typical Thai tertiary hospitals, RNs and PNNAs predominantly rotate through continuous 8-hour shifts (morning, afternoon, night). Because shift rotation strongly correlates with fatigue, this omission is a limitation. Residual confounding from unmeasured variables (eg., baseline burnout) may also persist, necessitating detailed scheduling parameters in future research. Finally, the single-hospital, single-country design limits generalizability to other healthcare tiers, private sectors, or different cultural contexts. Future studies should broaden their scope to explore wider predictors, utilize advanced analytical approaches, and investigate concurrent mental health conditions like anxiety and depression.
Conclusion
This study highlights marked differences in stress and engagement between RNs and PNNAs; RNs reported higher demands, while PNNAs showed greater engagement. Across both groups, high-strain jobs reduced engagement, whereas high support increased it. Importantly, regression analysis identified organizational support as the primary intervention target with the most significant impact, followed by job strain, sleep duration, and workplace hazards. Consequently, interventions must be tailored for practical operability. For RNs, strategies should optimize workflows and establish peer-support programs to reduce decision-making pressure. For PNNAs, priority must be given to ergonomic training and safety protocols to mitigate physical labor. Regarding generalizability, these findings offer substantial reference value for comparable secondary and tertiary hospitals across Thailand. Despite cross-sectional limitations, these insights effectively inform policies for a healthier, more engaged healthcare workforce.
Institutional Review Board Statement
This study was conducted following the Declaration of Helsinki, and the protocol was approved by the Research Ethics Committee, Faculty of Medicine, Chiang Mai University, Thailand (No. 120/2023, approved on 28 March 2023). Informed consent was obtained from all participants prior to study commencement. Participants were informed that their participation was voluntary and that they could withdraw from the study at any time without any negative consequences.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
This research work was partially supported by Chiang Mai University. This work would not have been possible without the operational support from the support unit offices and the nursing service organization. We would like to express our sincere gratitude to the Vice Director of the Nursing Department (Research), Maharaj Nakorn Chiang Mai Hospital, Faculty of Medicine, Chiang Mai University, for her valuable support in public relations and facilitating the data collection process. We would also like to thank Peewara Kanta for her assistance in the data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report there are no competing interests to declare for this work.
References
1. Leka S, Griffiths A, Cox T. Work organisation and stress: systematic problem approaches for employers, managers and trade union representatives. World Health Organization. 2003.
2. Chen B, Wang L, Li B, Liu W. Work stress, mental health, and employee performance. Front Psychol. 2022;13:1006580. doi:10.3389/fpsyg.2022.1006580
3. Restrepo J, Lemos M. Addressing psychosocial work-related stress interventions: a systematic review. Work. 2021;70(1):53–13. doi:10.3233/wor-213577
4. Kaewboonchoo O, Saleekul S, Usathaporn S. Factors related to work ability among Thai workers. Southeast Asian J Trop Med Public Health. 2011;42(1):225–230.
5. Ferrari S, Cuoghi G, Mattei G, et al. Young and burnt? Italian contribution to the international BurnOut Syndrome Study (BOSS) among residents in psychiatry. La Medicina del lavoro. 2015;106(3):172–185.
6. Catapano P, Cipolla S, Sampogna G, et al. Organizational and individual interventions for managing work-related stress in healthcare professionals: a systematic review. Medicina. 2023;59(10):1866. doi:10.3390/medicina59101866
7. Thailand Nursing Council. Announcement of the thailand nursing council: nursing council policy on nursing team staffing. 2018.
8. Harnyoot O. Nursing process and implications. J Royal Thai Army Nurs. 2015;15(3):137–143.
9. Sukdisthanon S. Advance practice nurse: APN. Maharat Nakhon Ratchasima Hospital J. 2024;28(1):59–66.
10. Walton AL, Rogers B. Workplace hazards faced by nursing assistants in the United States: a focused literature review. Int J Environ Res Public Health. 2017;14(5):544. doi:10.3390/ijerph14050544
11. Park SA, Ahn SH. Relation of compassionate competence to burnout, job stress, turnover intention, job satisfaction and organizational commitment for oncology nurses in Korea. Asian Pac J Cancer Prev. 2015;16(13):5463–5469. doi:10.7314/apjcp.2015.16.13.5463
12. Bryant C, Fairbrother G, Fenton P. The relative influence of personal and workplace descriptors on stress. Br J Nurs. 2000;9(13):876–880. doi:10.12968/bjon.2000.9.13.5517
13. Lourenção LG, Sodré PC, Gazetta CE, Silva AGD, Castro JR, Maniglia JV. Occupational stress and work engagement among primary healthcare physicians: a cross-sectional study. Sao Paulo Med J. 2022;140(6):747–754. doi:10.1590/1516-3180.2021.0644.R1.10012022
14. Bernales-Turpo D, Quispe-Velasquez R, Flores-Ticona D, et al. Burnout, professional self-efficacy, and life satisfaction as predictors of job performance in health care workers: the mediating role of work engagement. J Prim Care Community Health. 2022;13:21501319221101845. doi:10.1177/21501319221101845
15. Bakker AB, Schaufeli WB. Work engagement. Wiley Encyclopedia Manage. 1–5.
16. Moisoglou I, Katsiroumpa A, Katsapi A, Konstantakopoulou O, Galanis P. Poor nurses’ work environment increases quiet quitting and reduces work engagement: a Cross-Sectional Study in Greece. Nurs Rep. 2025;15(1). doi:10.3390/nursrep15010019
17. Çaylak E, Altuntaş S. Organizational silence among nurses: the impact on organizational cynicism and intention to leave work. J Nurs Res. 2017;25(2):90–98. doi:10.1097/jnr.0000000000000139
18. Salem EA, Ebrahem SM. Psychosocial work environment and oxidative stress among nurses’. J Occup Health. 2018;60(2):182–191. doi:10.1539/joh.17-0186-OA
19. Xie W, Chen L, Feng F, et al. The prevalence of compassion satisfaction and compassion fatigue among nurses: a systematic review and meta-analysis. Int J Nurs Stud. 2021;120:103973. doi:10.1016/j.ijnurstu.2021.103973
20. Minh DV, Akkadechanunt T, Chitpakdee B. Job Demands, job resources and work engagement among nurses in tertiary care hospitals, Thanh Hoa Province, The Socialist Republic of Vietnam. Nursing J CMU. 2019;46(1):166–179.
21. Falguera CC, Labrague LJ, De Los Santos JAA, Firmo CN, Tsaras K. Predictive roles of organizational and personal factors in work engagement among nurses. Front Nurs. 2022;9(4):379–387. doi:10.2478/fon-2022-0048
22. Thaomor W. Factors associated to job stress among officers in a General Hospital. research article. Buddhachinaraj Med J. 2020;37(1):49–59.
23. Palasak I, Suppapitiporn S. Occupational stress and related factors among registered nurses at Relief and Community Health Bureau, Thai Red Cross Society. Chulalongkorn Med J. 2022;66(4):457–464. doi:10.58837/CHULA.CMJ.66.4.10
24. Karasek RA. Job Demands, Job Decision Latitude, and Mental Strain: implications for Job Redesign. Adm Sci Q. 1979;24(2):285–308. doi:10.2307/2392498
25. Bakker AB, Demerouti E, Sanz-Vergel AI. Burnout and work engagement: the JD–R approach. Ann Rev Organizat Psychol Organizat Behav. 2014;1(1):2014):389–411. doi:10.1146/annurev-orgpsych-031413-091235
26. Schaufeli WB, Salanova M, González-romá V, Bakker AB. The measurement of engagement and burnout: a two sample confirmatory factor analytic approach. J Happiness Stud. 2002;3(1):71–92. doi:10.1023/A:1015630930326
27. Phakthongsuk P, Apakupakul N. Psychometric properties of the thai version of the 22-Item and 45-Item karasek job content questionnaire. Int J Occup Med Environ Health. 2008;21:331–344. doi:10.2478/v10001-008-0036-6
28. Phakthongsuk P. Construct validity of the Thai version of the job content questionnaire in a large population of heterogeneous occupations. J Med Assoc Thailand. 2009;92:564–572.
29. Thitaree K, Chaiwong W. A study on prevalence of work-related stress and relating factors among staff in a private hospital. Thammasat Med J. 2019;19(1):115–132.
30. Schaufeli W. The Utrecht Work Engagement Scale (UWES). Test Manual. 2017.
31. Tatha O, Shimazu A, Watanabe K, Kawakami N, Schaufeli WB. Measuring work engagement in Thailand: development and validation testing of the Utrecht Work Engagement Scale-Thai version (UWES-TH). Ind Health. 2024;62(3):182–194. doi:10.2486/indhealth.2023-0017
32. Kaewboonchoo O, Yingyuad B, Rawiworrakul T, Jinayon A. Job stress and intent to stay at work among registered female nurses working in Thai hospitals. J Occup Health. 2014;56(2):93–99. doi:10.1539/joh.12-0204-oa
33. Vimonvattana A, Benjakul N. The work engagement among nurses in an urban-based tertiary hospital. Nursing Rep. 2025;15(7):241. doi:10.3390/nursrep15070241
34. Wahab A, Mohd Hairon S, Shafei MN, Ibrahim MI, Mahmud N. Exploring job stress among public health workforce in Northeastern Malaysia. Cureus. 2023;15(11):e49083. doi:10.7759/cureus.49083
35. Chen J, Davis LS, Davis KG, Pan W, Daraiseh NM. Physiological and behavioural response patterns at work among hospital nurses. J Nurs Manag. 2011;19(1):57–68. doi:10.1111/j.1365-2834.2010.01210.x
36. Boblin S, Baxter P, Alvarado K, Baumann A, Akhtar-Danesh N. Registered nurses and licensed/registered practical nurses: a description and comparison of their decision-making process. Nurs Leadersh. 2008;21(4):56–72. doi:10.12927/cjnl.2008.20288
37. Van Bogaert P, van Heusden D, Timmermans O, Franck E. Nurse work engagement impacts job outcome and nurse-assessed quality of care: model testing with nurse practice environment and nurse work characteristics as predictors. Front Psychol. 2014;5:1261. doi:10.3389/fpsyg.2014.01261
38. Kohnen D, De Witte H, Schaufeli WB, Dello S, Bruyneel L, Sermeus W. What makes nurses flourish at work? How the perceived clinical work environment relates to nurse motivation and well-being: a cross-sectional study. Int J Nurs Stud. 2023;148:104567. doi:10.1016/j.ijnurstu.2023.104567
39. Bonsaksen T, Thørrisen MM, Skogen JC, Aas RW. Who reported having a high-strain job, low-strain job, active job and passive job? The WIRUS Screening study. PLoS One. 2020;14(12):e0227336. doi:10.1371/journal.pone.0227336
40. Adriaenssens J, Hamelink A, Bogaert PV. Predictors of occupational stress and well-being in first-line nurse managers: a cross-sectional survey study. Int J Nurs Stud. 2017;73:85–92. doi:10.1016/j.ijnurstu.2017.05.007
41. Schaufeli WB, Bakker AB, Van Rhenen W. How changes in job demands and resources predict burnout, work engagement, and sickness absenteeism. J Organizational Behav. 2009;30(7):893–917. doi:10.1002/job.595
42. Aungsuroch Y, Gunawan J, Juanamasta IG, Montayre J. Updating factors influencing nurse work engagement in the hospital settings: a systematic review. J Healthc Leadersh. 2024;16:157–176. doi:10.2147/jhl.S451056
43. Pericak A, Hogg CW, Skalsky K, Bourdeanu L. What influences work engagement among registered nurses: implications for evidence-based action. Worldviews Evid Based Nurs. 2020;17(5):356–365. doi:10.1111/wvn.12469
44. Völker J, Kühnel J, Feinäugle F, Barnes CM. Being robbed of an hour of sleep: the impact of the transition to daylight saving time on work engagement depends on employees’ chronotype. Sleep Health. 2023;9(5):579–586. doi:10.1016/j.sleh.2023.06.004
45. Kudrnáčová M, Kudrnáč A. Better sleep, better life? Testing the role of sleep on quality of life. PLoS One. 2023;18(3):e0282085. doi:10.1371/journal.pone.0282085
46. Fiabane E, Giorgi I, Sguazzin C, Argentero P. Work engagement and occupational stress in nurses and other healthcare workers: the role of organisational and personal factors. J Clin Nurs. 2013;22(17–18):2614–2624. doi:10.1111/jocn.12084
47. Rasool SF, Wang M, Tang M, Saeed A, Iqbal J. How toxic workplace environment effects the employee engagement: the mediating role of organizational support and employee wellbeing. Int J Environ Res Public Health. 2021;18(5):2294. doi:10.3390/ijerph18052294
48. Pires ML. The effects of job insecurity on psychological well-being and work engagement: testing a moderated mediation model. Behav Sci. 2025;15(7):979. doi:10.3390/bs15070979
49. Ayvaz Ö, Özyıldırım BA, Işsever H, Öztan G, Atak M, Özel S. Ergonomic risk assessment of working postures of nurses working in a medical faculty hospital with REBA and RULA methods. Sci Prog. 2023;106(4):368504231216540. doi:10.1177/00368504231216540
50. Kaewcharern U, Arphorn S, Kaewboonchoo O, Chaikittiporn C, Pruktharathikul V, Siriwong W. Ergonomic risk factors and work ability among registered nurses in operating rooms, Bangkok, Thailand. J Health Res. 2017;25(1):39–43.
51. Yiengprugsawan V, Strazdins L, Lim LL, Kelly M, Seubsman SA, Sleigh AC. Physically and psychologically hazardous jobs and mental health in Thailand. Health Promot Int. 2015;30(3):531–541. doi:10.1093/heapro/dat080
52. Eid J, Brattebø G, Jacobsen JK, Espevik R, Johnsen BH. Distributed team processes in healthcare services: a scoping review. Front Med. 2023;10:1291877. doi:10.3389/fmed.2023.1291877
53. Dehghani Soufi M, Samad-Soltani T, Shams Vahdati S, Rezaei-Hachesu P. Decision support system for triage management: a hybrid approach using rule-based reasoning and fuzzy logic. Int J Med Inform. 2018;114:35–44. doi:10.1016/j.ijmedinf.2018.03.008
54. Borst RT, Knies E. Well-Being of public servants under pressure: the roles of job demands and personality traits in the health-impairment process. Rev Public Personnel Administration. 2023;43(1):159–184. doi:10.1177/0734371x211052674
55. Bakker AB, Demerouti E. Multiple levels in job demands-resources theory: implications for employee well-being and performance. In: Handbook of Well-Being. Noba Scholar; 2018.
56. Bakker AB, Demerouti E, Sanz-Vergel A. Job demands–resources theory: ten years later. Ann Rev Organizat Psychol Organizat Behav. 2023;10(10):2023):25–53. doi:10.1146/annurev-orgpsych-120920-053933
57. Wei H. The development of an evidence-informed convergent care theory: working together to achieve optimal health outcomes. Int J Nurs Sci. 2022;9(1):11–25. doi:10.1016/j.ijnss.2021.12.009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.