Back to Journals » Cancer Management and Research » Volume 18

Optimizing Left-Sided Breast Cancer Radiotherapy: Strategy-Dependent Trade-Offs Among VMAT and Hybrid Techniques
Authors Mottareale R, Buonanno F ![]() , d'Alesio V, Falivene S, Serra M, Arrichiello C, Ametrano G, Ferraioli P, Gagliardo G
, d'Alesio V, Falivene S, Serra M, Arrichiello C, Ametrano G, Ferraioli P, Gagliardo G ![]() , Di Franco R, Mercogliano S, Muto P, Ravo V
, Di Franco R, Mercogliano S, Muto P, Ravo V ![]()
Received 23 December 2025
Accepted for publication 11 March 2026
Published 22 May 2026 Volume 2026:18 591060
DOI https://doi.org/10.2147/CMAR.S591060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Rocco Mottareale,1 Francesca Buonanno,1 Valentina d’Alesio,1 Sara Falivene,1 Marcello Serra,1 Cecilia Arrichiello,1 Gianluca Ametrano,1 Piera Ferraioli,1 Gaetano Gagliardo,2 Rossella Di Franco,1 Simona Mercogliano,1 Paolo Muto,2 Vincenzo Ravo1
1Department of Radiation Oncology, Istituto Nazionale Tumori - IRCCS - Fondazione G. Pascale, Napoli, Italy; 2Fondazione Muto ETS, Napoli, Italy
Correspondence: Rocco Mottareale; Francesca Buonanno, Department of Radiation Oncology, Istituto Nazionale Tumori - IRCCS - Fondazione G. Pascale, Napoli, Italy, Email [email protected]; [email protected]
Purpose: To compare dosimetric trade-offs among two full-VMAT and two hybrid 3D-CRT/VMAT strategies for left-sided whole-breast irradiation (WBI), and to evaluate the influence of planning strategy, introducing a novel tangential hybrid approach (H-tVMAT).
Patients and Methods: Twenty patients with left-sided breast cancer treated with WBI (40.05 Gy in 15 fractions) were retrospectively analyzed. For each patient, four plans were generated within a single treatment planning system under free-breathing conditions: large-angle VMAT, tangential VMAT (tVMAT), Hybrid VMAT (H-VMAT), and the novel tangential Hybrid tVMAT (H-tVMAT). Primary dosimetric endpoints included heart and pulmonary structures and the contralateral breast, with dedicated evaluation of low-dose exposure. Target conformity, homogeneity index (HI), and monitor units (MUs) were also assessed.
Results: All strategies achieved clinically acceptable target coverage and homogeneity. Hybrid configurations consistently reduced cardiac, pulmonary, and contralateral low-dose exposure compared with full-VMAT solutions. Among the evaluated strategies, H-tVMAT provided the most favorable balance between heart/LAD sparing, low-dose containment, and target coverage. Appropriately configured tangential VMAT achieved dosimetric results close to hybrid solutions, underscoring the importance of arc geometry. No statistically significant differences in delivery complexity were observed across strategies.
Conclusion: Dosimetric performance in left-sided WBI is strongly influenced by planning implementation rather than nominal technique category alone. Hybrid tangential VMAT achieved the most balanced dosimetric profile, while optimized tangential VMAT provided comparable results. These findings support a strategy-specific approach to technique selection, emphasizing the central role of implementation choices in breast radiotherapy planning.
Keywords: whole breast irradiation, hybrid VMAT, tangential VMAT, cardiac sparing
Introduction
Radiation therapy (RT) plays a central role in the management of breast cancer,1–5 with whole breast irradiation (WBI) representing a standard adjuvant approach after breast-conserving surgery, particularly in early-stage disease.6 The widespread adoption of hypofractionated regimens has increased the need for rigorous dosimetric control, given the complex breast anatomy and its proximity to critical organs at risk (OARs), especially the heart and lungs.7 Conventional three-dimensional conformal radiotherapy (3D-CRT) with tangential fields has long been the reference technique for WBI.8 While this approach is characterized by limited low-dose exposure to surrounding healthy tissues,9 it is often associated with suboptimal target homogeneity, especially in patients with larger breast volumes, potentially leading to increased acute skin toxicity.10 The introduction of field-in-field techniques partially addressed these limitations by improving dose uniformity through subfield modulation.11 More recently, advanced intensity-modulated techniques such as volumetric modulated arc therapy (VMAT) have been increasingly adopted in breast RT due to their ability to enhance target conformity and homogeneity.12–17 However, the use of VMAT for WBI remains controversial. Gains in target dose distribution are frequently accompanied by a substantial increase in low-dose exposure to large volumes of healthy tissues.6,14 This so-called “low-dose bath” has been associated with an increased risk of radiation-induced cardiac and pulmonary toxicity, as well as a potential rise in secondary malignancy risk.15 These concerns are particularly relevant in left-sided WBI, where cardiac exposure represents a key determinant of long-term treatment-related morbidity.18,19 Current planning recommendations provide limited guidance on balancing target coverage, homogeneity, and OARs sparing, leaving clinicians with uncertainty regarding optimal strategy selection for individual patients.
In this evolving clinical and technical landscape, optimization of breast radiotherapy can no longer rely solely on maximizing target conformity. Instead, there is growing emphasis on planning strategies capable of balancing dosimetric quality with long-term safety, minimizing unnecessary low-dose exposure while preserving adequate target coverage and homogeneity. Hybrid approaches combining 3D-CRT and VMAT have therefore been proposed to exploit the robustness and favourable low-dose characteristics of tangential fields while using a limited VMAT component to improve dose homogeneity and conformity.20–28 Despite the increasing adoption of hybrid approaches for left-sided WBI, current evidence remains heterogeneous and challenging to translate into robust planning recommendations. Most published studies rely on comparisons between a single hybrid implementation and a full-VMAT solution, offering limited insight into how different planning configurations within the same technique category may influence target homogeneity, OARs sparing, and low-dose exposure. Consequently, key controversies remain unresolved regarding which hybrid configurations optimally balance these trade-offs, and whether reported advantages reflect intrinsic technique properties or are implementation dependent. Understanding how implementation-dependent factors influence these trade-offs is therefore essential to support informed technique selection beyond nominal technique classification.
The aim of the present study is to address these gaps by systematically comparing two full-VMAT and two hybrid 3D-CRT/VMAT planning strategies for left-sided WBI. Unlike previous dosimetric investigations based on binary technique comparisons, this multi-strategy design enables the assessment of intra-technique variability and provides a more comprehensive characterization of clinically relevant dosimetric trade-offs. By explicitly analyzing the balance between target dose conformity, OARs sparing, and low-dose exposure, this work seeks to provide clinically meaningful evidence to support technique selection in routine practice, with particular attention to long-term treatment-related safety. Within this framework, we evaluated the feasibility and effectiveness of the two distinct hybrid VMAT arrangements in comparison with two pure VMAT solutions. To our knowledge, this is the first study to investigate the hybridization of tangential VMAT (tVMAT) with 3D-CRT within the Monaco treatment planning system (TPS), a configuration referred to as hybrid tVMAT (H-tVMAT), providing novel insight into how implementation choices shape the dosimetric behavior of hybrid planning strategies and inform clinical decision-making in left-sided WBI.
Materials and Methods
Patient Data Set and Contouring
Twenty patients with left-sided breast cancer receiving adjuvant whole breast radiotherapy after conservative surgery were retrospectively selected. All patients were immobilized supine with arms raised using a dedicated breast board to ensure setup reproducibility throughout treatment. Free-breathing planning images were acquired with a 3-mm slice thickness on a Toshiba Aquilion CT scanner (Toshiba Medical Systems, Tokyo, Japan) from the mandibular level to the umbilicus. The clinical target volume (CTV) was delineated following institutional guidelines and international recommendations.29–31 To account for setup uncertainties and respiratory motion, the planning target volume (PTV) was obtained by applying a 5 mm isotropic expansion to the CTV. PTV was then cropped 3 mm from patient surface. The contoured OARs included the heart, left anterior descending coronary artery (LAD), ipsilateral and contralateral lungs, and contralateral breast. A total dose of 40.05 Gy was prescribed in daily fractions of 2.67 Gy for all patients.
Treatment Planning
Each patient was planned with 6 MV photon beams using the Monaco v6.1 TPS employing the Monte Carlo (MC) and collapsed cone convolution (CCC) algorithms for VMAT and 3D-CRT, respectively. For MC, a statistical uncertainty of 1% was applied, and the dose calculation grid resolution was set to 3 mm for both MC and CCC algorithms. All plans were designed for a VersaHD linear accelerator (Elekta AB, Stockholm, Sweden) equipped with 5-mm Agility MLC. Four treatment approaches were considered: VMAT, Hybrid VMAT (H-VMAT), tangential VMAT (tVMAT) and Hybrid tVMAT (H-tVMAT), the latter obtained by hybridizing tVMAT with 3D-CRT, as suggested by evidence of improved OARs sparing using two narrow coplanar arcs over large VMAT arcs.20,21,32 For each patient, the same isocenter was maintained to ensure a consistent comparison between the planning techniques. All plans were considered clinically acceptable after review by two experienced medical physicists and approval by a radiation oncologist.
VMAT and tVMAT
The VMAT technique involves a maximum of two semi-arcs. According to the patient’s anatomy and PTV coverage, the start angle was set to 316°±10° with an arc length of 220° and an arc segment step size of 20°. The collimator angle was fixed to 10°. Optimization parameters included a maximum of 300 control points per arc, a minimum segment width of 1 cm, and high fluence smoothing. For tVMAT plans, two narrow coplanar arcs of 55° each were used, maintaining the same angular orientation as the two tangential beams in the 3D-CRT approach. The arc segment step size was reduced to 11° to enhance modulation of the dose distribution as the gantry moved through the arc. A dedicated template for cost functions was created within the Monaco IMRT Constraints module (Table 1). The optimization process was conducted to satisfy the clinical constraints reported in Table 2.
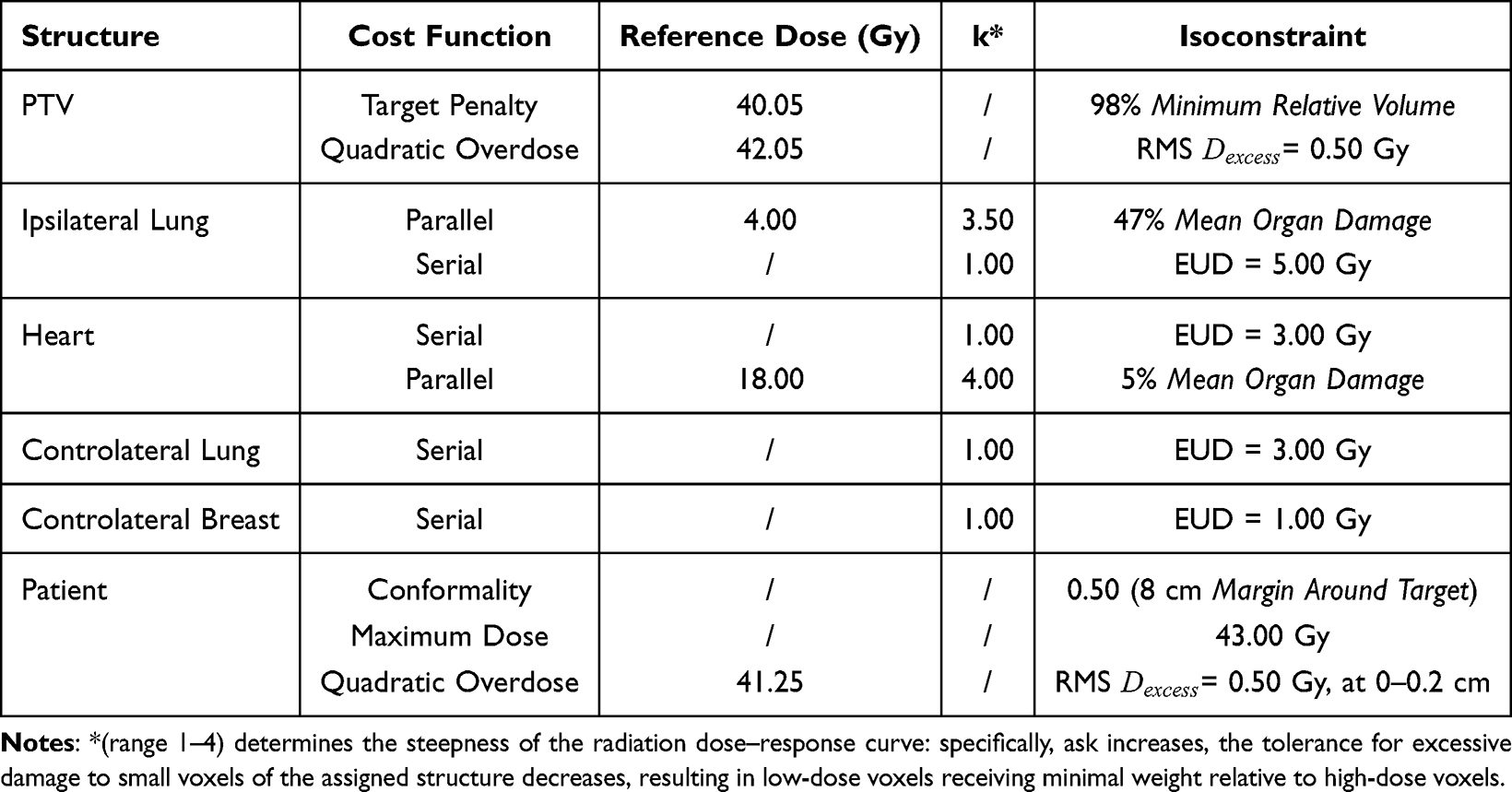 |
Table 1 List of the IMRT Constraints Used for the Inverse Planning Optimization of Both VMAT and tVMAT, for the Planning Target Volume (PTV) and Organs at Risk (OARs): Ipsilateral Lung, Heart, Left Anterior Descending Artery (LAD), Contralateral Breast, Contralateral Lung and External Patient Volume (Outside the PTV) |
 |
Table 2 List of Dosimetric Constraints Used in Planning Optimization for Both Planning Target Volume (PTV) and Organs at Risk (OARs): Ipsilateral Lung, Heart, Left Anterior Descending Artery (LAD), Contralateral Breast, and Contralateral Lung |
H-VMAT and H-tVMAT
The H-VMAT and H-tVMAT plans were developed by integrating a 3D-CRT plan with a modulated arc-based component. The 3D-CRT plan utilized two opposed tangential fields, with the gantry positioned at 316°±10° for the internal beam and 136°±10° for the external beam. This initial 3D-CRT plan was normalized to 70% of the prescribed dose, ensuring coverage of at least 95% of the PTV. The 3D-CRT plan represents a bias dose contribution for the VMAT/tVMAT component. The bias-corrected VMAT/tVMAT plan was normalized to 30% of the prescribed dose, ensuring optimized PTV coverage with the specific objectives V95% > 95% and V107% < 2%.
Plan Analysis and Dosimetric Evaluation
For quantitative analysis dose–volume histograms (DVHs) of the PTV and OARs were extracted. To assess PTV coverage, for each plan Conformity Index (CI) and Homogeneity Index (HI) were calculated following the RTOG definitions:22

where PIV95 is the isodose volume corresponding to 95% of the prescribed dose (Dp) and TV is the target volume. This value ranges from 0 to 1 with CI = 1 indicating an ideal conformation of the irradiated volume to the reference isodose;

where D2% and D98% are the near maximum and the near minimum of the PTV dose, respectively, and Dp is the prescription dose. An ideal HI of 0 indicates perfect dose homogeneity within the PTV. Minimizing the HI ensures that the target volume receives the prescription dose as uniformly as possible, with fewer regions of underdose or overdose.
Furthermore, relevant PTV and OARs metrics were retrieved in terms of dose received by X percentage of volume (DX) and mean dose (Dmean). PTV coverage was evaluated in terms of D95%, D2%, and Dmean. OARs sparing was assessed using the following criteria: D15%, D20%, D35%, and D50% for the ipsilateral lung; D15%, D20%, and Dmean for the heart; D1% and Dmean for the LAD; D15%, D20%, and Dmean for the contralateral lung; D15%, D20%, D35%, D50%, and Dmean for the contralateral breast.
Low-dose spillage was evaluated by considering the spread of low doses in normal tissue through the percentage of normal tissue (patient body minus PTV) receiving doses ranging from 1 to 25 Gy. In addition, the number of monitor units (MU) used in each plan was recorded to assess delivery efficiency.
Statistical Analysis
For each dosimetric parameter, normality for each patient across the four techniques was assessed using the Shapiro–Wilk test. Paired t-tests were applied for normally distributed pairs of techniques, and Wilcoxon signed-rank tests were applied otherwise, to account for the repeated-measures design. Six pairwise comparisons were performed per parameter (corresponding to all possible pairs among the four techniques), and p-values were adjusted using the Bonferroni correction to control for multiple testing (α/6 = 0.0083). P-values exceeding this threshold are indicated as NS (not significant). Statistical significance was considered at p < 0.0083 after Bonferroni correction.
Results
The dose distributions for one representative patient with the four investigated field arrangements are illustrated in Figure 1. Table 3 summarizes the dosimetric results as median values and ranges for each metric across all patients, along with their statistical comparisons. The average DVHs are shown in Figures 2 and 3.
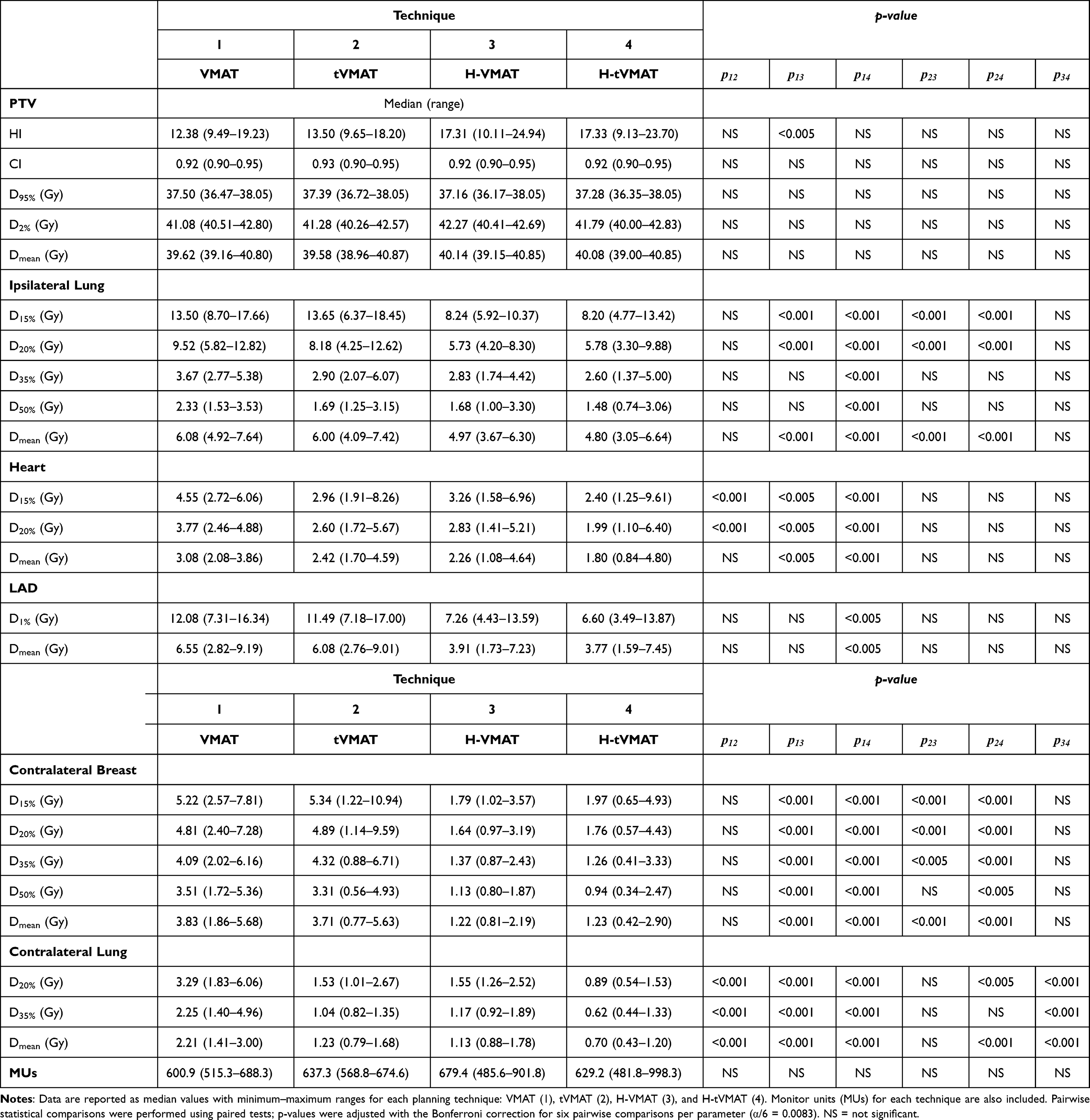 |
Table 3 Dosimetric Parameters for the Planning Target Volume (PTV) and Organs at Risk (OARs): Ipsilateral Lung, Heart, Left Anterior Descending Artery (LAD), Contralateral Breast, and Contralateral Lung |
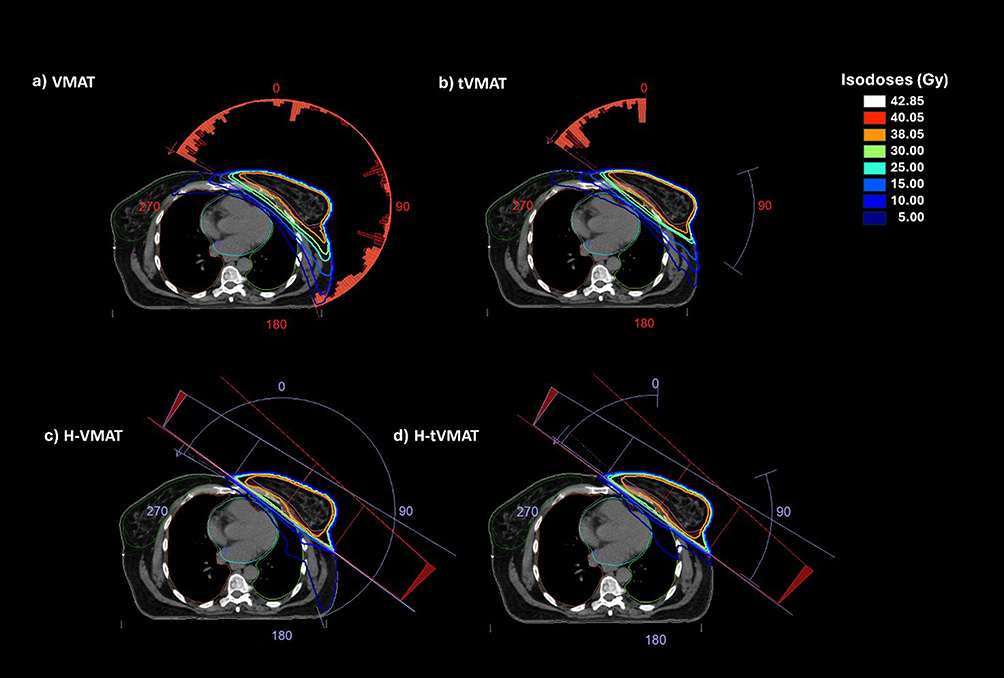 |
Figure 1 Dose distributions for a representative patient with the four investigated field arrangements are shown: (a) VMAT, (b) tVMAT, (c) H-VMAT, and (d) H-tVMAT. Isodose lines, expressed as percentages of the prescription dose (40.05 Gy delivered to the PTV in 15 fractions), are displayed on an axial CT slice at isocenter. Organs at risk are delineated as follows: heart (blue), LAD (red), ipsilateral lung (light green), contralateral lung (Orange), and contralateral breast (dark green). |
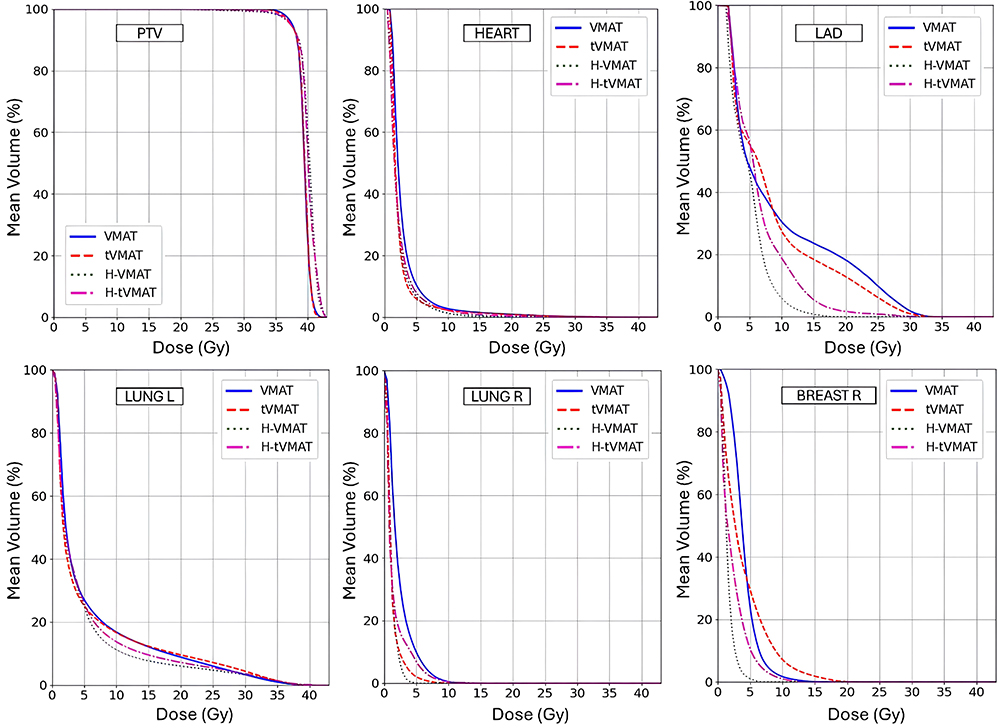 |
Figure 2 Mean dose–volume histograms (DVHs) illustrating the average percentage volume as a function of dose (Gy) for the PTV and organs at risk: ipsilateral lung, heart, LAD, contralateral breast, and contralateral lung. Each curve corresponds to one of the evaluated techniques: VMAT, tVMAT, H-VMAT, and H-tVMAT. |
 |
Figure 3 Comparison of low-dose volumes (1–25 Gy) for VMAT, tVMAT, H-VMAT, and H-tVMAT. Data are presented as the mean percentage of irradiated external patient volume (outside the PTV) corresponding to each dose level (Gy). |
Target Coverage and Dose Homogeneity
No statistically significant differences were found among the investigated techniques in terms of CI and target coverage (D95%), since the comparison was conducted under equivalent target volume coverage (V95% > 95%). However, VMAT showed a significant improvement in the HI, indicating a more uniform dose distribution compared with the hybrid plans H-VMAT and H-tVMAT (p < 0.005 and p < 0.05, respectively). Similarly, tVMAT demonstrated a significantly lower HI than H-VMAT (p < 0.05). No significant differences were observed in HI between VMAT and tVMAT, tVMAT and H-tVMAT and in the comparison between the two hybrid techniques, suggesting comparable dose target homogenity. Among the planning techniques, H-VMAT exhibited the highest D2% value, which nevertheless fulfilled the PTV constraint V105% < 5–7%.
Organs at Risk
Ipsilateral Lung
No significant differences were observed between VMAT and tVMAT in terms of D15% and D20%. H-VMAT and H-tVMAT significantly reduced D15% and D20% when compared with VMAT and tVMAT (p < 0.001). VMAT exhibited higher median values of D35% and D50% compared with tVMAT or hybrid techniques (p < 0.05 vs. tVMAT and H-VMAT; p < 0.001 vs. H-tVMAT). However, there were no statistically significant differences between tVMAT and the hybrid techniques for D35% and D50%. Additionally, no significant differences were found between the two hybrid techniques for any of the considered dosimetric indicators related to the left lung, suggesting that both provided an equal sparing of this OAR.
Heart and LAD
VMAT delivered the highest dose values to the heart compared with all other techniques. The use of narrow coplanar arc pairs significantly reduced D15%, D20%, and Dmean compared with VMAT (p < 0.001 for D15% and D20% and p < 0.05 for Dmean). A similar trend was observed for the hybrid techniques, which showed significantly lower values for these dosimetric metrics than full VMAT approaches (p < 0.005 and p < 0.001 for H-VMAT and H-tVMAT, respectively).
While no significant differences were found between tVMAT and H-VMAT, H-tVMAT plans achieved significantly lower median values for heart Dmean (p < 0.05). No significant differences were observed between H-VMAT and H-tVMAT.
Regarding LAD involvement, both VMAT and tVMAT exhibited the highest maximum dose (D1%), whereas H-VMAT and H-tVMAT achieved significantly lower D1% values than VMAT (p < 0.05 and p < 0.005, respectively). The mean LAD dose was significantly higher in VMAT compared with hybrid techniques (6.55 Gy for VMAT, 3.91 Gy and 3.77 Gy for H-VMAT and H-tVMAT, respectively), with no statistically significant differences between the two hybrid techniques.
Contralateral Breast
No significant differences were observed between VMAT and tVMAT. Both hybrid techniques had significantly lower D15%, D50%, and Dmean compared with VMAT and tVMAT (p < 0.001, p < 0.001, p < 0.005, respectively). The contralateral breast Dmean was significantly lower for both H-VMAT and H-tVMAT compared with both VMAT and tVMAT. No statistically significant differences were found between the two hybrid techniques.
Contralateral Lung
tVMAT resulted in significantly lower values of D20%, D35%, and Dmean compared with VMAT (p < 0.001). VMAT also showed significantly higher values compared with hybrid techniques (p < 0.001). No significant differences were found between tVMAT and H-VMAT. However, H-tVMAT resulted in significantly lower doses compared with tVMAT (p < 0.005 for D20%, p < 0.05 for D35%, and p < 0.001 for Dmean). Additionally, when comparing the two hybrid techniques, H-tVMAT produced significantly lower dose values than H-VMAT (p < 0.001), indicating superior sparing of the contralateral lung.
Low-Dose Volumes
Figure 3 and Table 4 show the percentage volumes of the normal tissue receiving doses ranging from 1 to 25 Gy for each of the four planning techniques.
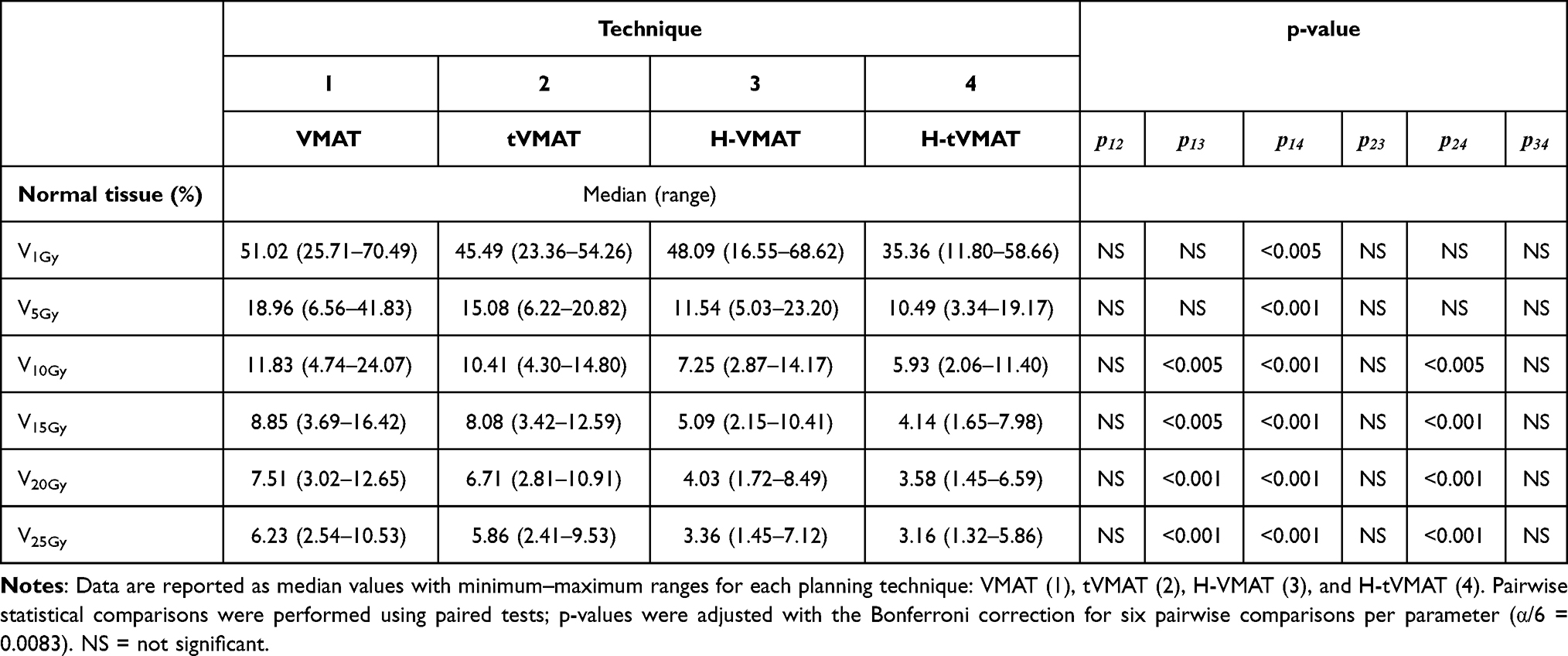 |
Table 4 Low-Dose Spillage Expressed as the Percentage of External Patient Volume (Outside the PTV) Receiving 1–25 Gy |
The comparison of VMAT and tVMAT revealed no statistically significant differences in the V1Gy–V25Gy range, with tVMAT showing slightly lower median values. However, VMAT plans resulted in significantly higher irradiated patient volumes than both hybrid techniques, particularly in the 5–25 Gy range (p < 0.05 to p < 0.001). When comparing tVMAT and H-VMAT, no significant differences emerged in the 1–10 Gy range, but at higher dose levels (15–25 Gy), H-VMAT demonstrated superior dose sparing (p < 0.05). Meanwhile, H-tVMAT consistently outperformed tVMAT across the 5–25 Gy range (p < 0.05 to p < 0.001), enhancing its effectiveness in reducing radiation exposure to healthy tissues. The two hybrid techniques showed no significant differences in the 5–25 Gy range, except for V1Gy, where H-tVMAT resulted in significantly lower irradiated volumes than H-VMAT (p < 0.05).
Delivery Efficiency
The median number of MUs (Table 3) was 601 (range, 515.3–688.3) for VMAT, 637.3 (range 568.8–674.6) for tVMAT, 679.4 (range, 485.6–901.8) for H-VMAT and 629.2 (range, 481.8–998.3) for H-tVMAT. No statistical differences were observed between the techniques.
Discussion
This study presents a systematic dosimetric evaluation of multiple VMAT and hybrid 3D-CRT/VMAT planning strategies for left-sided WBI within a unified planning framework. By adopting a multi-strategy approach, our analysis extends beyond conventional binary comparisons and demonstrates that dosimetric differences are not solely attributable to technique category but are strongly dependent on planning configuration and implementation. These findings challenge the assumption that VMAT and hybrid techniques represent homogeneous entities and emphasize the critical role of strategy-specific design choices in shaping clinically relevant dosimetric trade-offs.
Previous dosimetric studies investigating hybrid VMAT-based approaches for WBI have reported heterogeneous results, reflecting substantial methodological variability rather than intrinsic inconsistencies in technique performance. Several investigations compared a single hybrid configuration with a full-VMAT solution, generally reporting improved target homogeneity and reduced low-dose exposure to selected organs at risk.23,24 An overview of key methodological features and dosimetric outcomes reported in recent hybrid VMAT studies is provided in Table 5, highlighting the substantial heterogeneity in planning configurations, platforms, and reported metrics. While these studies established the feasibility and potential advantages of hybrid planning, they predominantly adopt a binary comparison framework in which hybrid planning is represented by a single implementation defined by fixed dose-weighting and arc geometry choices. As a result, they provide limited insight into how dosimetric outcomes may vary as a function of planning implementation rather than technique category alone. The present results indicate that these differences are largely driven by implementation-dependent factors, particularly arc geometry and modulation strategy, rather than by the hybrid concept per se.
 |
Table 5 Comparative Analysis of Previously Published Studies on Hybrid VMAT Techniques, Reporting Planning Approaches, Dose Prescription, Dosimetric Outcomes, and Main Findings in Relation to the Present Work |
Most available investigations rely on hybrid implementations characterized by a predominant 3D-CRT component, commonly adopting an approximate 80% tangential field and 20% VMAT contribution, as reported by Venjakob et al,24 Cilla et al,23 Bi et al,26 and Iga Racka et al27 While this paradigm has demonstrated favorable low-dose characteristics, it inherently constrains the degrees of freedom available for modulation and may limit optimization flexibility. In contrast, the present study explored alternative hybrid implementations using a 70/30 dose-weighting scheme and systematically evaluated different arc geometries, thereby expanding the parameter space typically investigated in the literature.
Additional heterogeneity across published studies arises from differences in prescription regimens, use of simultaneous integrated boost, breathing management strategies, and TPS. Prior investigations predominantly employed Eclipse24,26–28 or Pinnacle23,25 platforms, whereas the present analysis was performed using the Monaco TPS, whose optimization framework differs substantially in terms of cost-function handling and fluence modulation. These factors limit the interpretability of direct numerical comparisons and reinforce the need for multi-strategy evaluations performed within a single, controlled planning environment.
Breathing management further complicates cross-study comparisons, particularly for cardiac and coronary artery dosimetry. Several reports achieving very low cardiac doses relied on deep inspiration breath hold,24,25,27,28 whereas the present work was conducted entirely under free-breathing conditions. Moreover, despite the growing recognition of the LAD as a critical structure in left-sided breast irradiation, many dosimetric studies either do not report LAD-specific metrics or restrict the analysis to global heart parameters. Within this context, the heart and LAD doses observed in the present study compare favorably with previously reported free-breathing data,28 reinforcing the clinical relevance of a more detailed and consistent evaluation of cardiac substructures.
Within this heterogeneous landscape, the present analysis demonstrates that differences observed between VMAT and hybrid approaches are primarily driven by arc geometry and modulation strategy. In particular, constraining arc geometry through tangential narrow arcs resulted in a consistent reduction of low-dose exposure to contralateral organs and selected cardiac structures while preserving clinically acceptable target coverage.
The comparison between the two hybrid strategies investigated in this study, H-VMAT and H-tVMAT, provides insight into how arc geometry and modulation extent influence dosimetric outcomes in left-sided whole-breast irradiation. Tangential VMAT was originally introduced by Virèn et al21 to preserve the favorable beam geometry of conventional tangential fields while exploiting arc-based modulation to improve dose homogeneity. Building on this rationale, the hybrid tVMAT configuration evaluated here combines tangential 3D-CRT fields with narrow tangential arcs, aiming to further constrain beam entrance angles outside the tangential sector and reduce dose spillage toward contralateral organs while maintaining sufficient modulation capability. Compared with the wider-arc hybrid approach (H-VMAT), H-tVMAT showed reduced exposure of contralateral organs and selected cardiac structures while preserving clinically acceptable target coverage. Among the evaluated strategies, H-tVMAT achieved the most favorable overall balance between cardiac sparing, low-dose containment, and target coverage. Conversely, the wider-arc H-VMAT configuration provided increased degrees of freedom for dose shaping but resulted in broader low-dose exposure. Variability in reported PTV homogeneity among hybrid VMAT studies reflects differences in optimization priorities as well as the lack of standardized definitions of homogeneity metrics. While some investigations prioritize homogeneity, others accept higher heterogeneity in exchange for improved organ-at-risk sparing. The intermediate homogeneity index values observed in the present study reflect this trade-off and underscore the importance of interpreting dosimetric results within the context of planning objectives rather than relying on isolated metrics.
Within this framework, H-tVMAT may represent a pragmatic compromise in selected clinical scenarios where limiting low-dose exposure to critical structures is prioritized, although this potential advantage must be weighed against planning and delivery considerations.
Beyond dosimetric performance, planning complexity and deliverability represent relevant practical aspects when comparing VMAT and hybrid strategies. Importantly, the dosimetric advantages observed for H-tVMAT were not associated with a statistically significant increase in delivery complexity, as reflected by comparable monitor unit values across strategies. However, it is important to note that these observations are specific to the Monaco TPS and free-breathing conditions; extrapolation to other platforms or breathing protocols should be done cautiously. These findings highlight that technique selection should balance dosimetric benefit with implementation complexity and institutional workflow considerations.
This study has several limitations. The analysis is retrospective and purely dosimetric, and no clinical outcome data were available to correlate dose differences with toxicity or tumor control Additionally, the exclusive use of a single treatment planning system and free-breathing conditions may limit generalizability, and absolute dosimetric values could differ on alternative platforms or with DIBH strategies. Finally, although multiple planning configurations were investigated, the sample size remains limited, and larger multi-institutional studies would be valuable to confirm these findings.
Overall, this analysis demonstrates that hybrid VMAT techniques should not be regarded as a single, uniform approach but rather as a spectrum of planning solutions characterized by different balances between target conformity, dose homogeneity, OARs sparing, and delivery complexity. By systematically evaluating multiple VMAT and hybrid configurations within a single planning framework, this study provides evidence that planning implementation—particularly arc geometry—plays a decisive role in determining dosimetric performance and should be explicitly considered in technique selection.
Conclusion
This study shows that dosimetric differences in left-sided whole-breast irradiation are not determined by technique category alone, but are strongly influenced by planning implementation, particularly arc geometry and modulation strategy. Among the evaluated approaches, hybrid tangential VMAT (H-tVMAT) appeared to provide a favorable balance between cardiac and contralateral organ sparing, low-dose containment, and target coverage. However, appropriately configured tangential VMAT achieved dosimetric results close to hybrid solutions, indicating that similar performance may be obtained through careful planning design. Importantly, the dosimetric advantages observed for H-tVMAT were not associated with a statistically significant increase in delivery complexity. These results suggest that, within the limits of a dosimetric study, careful consideration of planning implementation can inform technique selection and may guide decision-making in routine clinical workflows, allowing clinicians to balance target coverage, OAR sparing, and low-dose exposure effectively. Overall, the findings support a strategy-specific, cost–benefit approach to technique selection, emphasizing that implementation details are central to optimizing breast radiotherapy rather than reliance on nominal technique classification alone.
Data Sharing Statement
The research data supporting the findings of this study are openly available in the Zenodo repository at https://doi.org/10.5281/zenodo.18957912. Further information can be obtained from the corresponding authors, Rocco Mottareale and Francesca Buonanno.
Ethic Statement
This study was conducted within the DREAMS trial prot. 52/25, approved by the Ethics Committee CAMPANIA 1 of the Istituto Nazionale Tumori – IRCCS - Fondazione G. Pascale of Napoli (Italy) on 03.09.2025 (D. n. 1411 of 17.09.2025). All patients provided written informed consent prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Authors thank Alessandra Trocino, librarian at the Istituto Nazionale Tumori di Napoli, IRCCS “G. Pascale”, Italy, for bibliographic assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Italian Ministry of Health Ricerca Corrente funds “LINEA 4/15_25”, Istituto Nazionale Tumori-IRCCS-Fondazione G. Pascale.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Berbers J, Van Baardwijk A, Houben R, et al. ‘Reconstruction: before or after postmastectomy radiotherapy?’ A systematic review of the literature. Eur J Cancer. 2014;50(16):2752–16. doi:10.1016/j.ejca.2014.07.023
2. Balaji K, Subramanian B, Yadav P, Anu Radha C, Ramasubramanian V. Radiation therapy for breast cancer: literature review. Med Dosim. 2016;41(3):253–257. doi:10.1016/j.meddos.2016.06.005
3. Moo T-A, Sanford R, Dang C, Morrow M. Overview of breast cancer therapy. PET Clin. 2018;13(3):339–354. doi:10.1016/j.cpet.2018.02.006
4. Mottareale R, Frascogna C, La Verde G, et al. Impact of ionizing radiation on cell-ECM mechanical crosstalk in breast cancer. Front Bioeng Biotechnol. 2024;12:1408789. doi:10.3389/fbioe.2024.1408789
5. Frascogna C, Mottareale R, La Verde G, et al. Role of the mechanical microenvironment on CD-44 expression of breast adenocarcinoma in response to radiotherapy. Sci Rep. 2024;14(1):391. doi:10.1038/s41598-023-50473-x
6. Chung E, Corbett JR, Moran JM, et al. Is there a dose-response relationship for heart disease with low-dose radiation therapy? Int J Radiat Oncol Biol Phys. 2013;85(4):959–964. doi:10.1016/j.ijrobp.2012.08.002
7. Rudat V, Shi Y, Zhao R, Yu W. Setup margins based on the inter- and intrafractional setup error of left-sided breast cancer radiotherapy using deep inspiration breath-hold technique (DIBH) and surface guided radiotherapy (SGRT). J Applied Clin Med Phys. 2024;25(6):e14271. doi:10.1002/acm2.14271
8. Xie X, Ouyang S, Wang H, et al. Dosimetric comparison of left-sided whole breast irradiation with 3D-CRT, IP-IMRT and hybrid IMRT. Oncol Rep. 2014;31(5):2195–2205. doi:10.3892/or.2014.3058
9. Kim J, Forouzannia A, Saini A, Hwang C. Hypofractionated whole-breast radiotherapy using a three-dimensional conformal technique: toxicity comparison in different breast sizes. Prec Radiat Oncol. 2018;2(4):119–124. doi:10.1002/pro6.54
10. Barnett GC, West CML, Dunning AM, et al. Normal tissue reactions to radiotherapy: towards tailoring treatment dose by genotype. Nat Rev Cancer. 2009;9(2):134–142. doi:10.1038/nrc2587
11. Jha B, Lamichhane HP, Prasiko G, Srivastava RP. Clinical experience and dosimetry outcome in treating breast cancer with field-in-field technique. ABCR. 2021;10(03):35–43. doi:10.4236/abcr.2021.103003
12. Yu CX, Tang G. Intensity-modulated arc therapy: principles, technologies and clinical implementation. Phys Med Biol. 2011;56(5):R31–R54. doi:10.1088/0031-9155/56/5/R01
13. Pasler M, Lutterbach J, Björnsgard M, Reichmann U, Bartelt S, Georg D. VMAT techniques for lymph node-positive left sided breast cancer. Zeitschrift für Medizinische Physik. 2015;25(2):104–111. doi:10.1016/j.zemedi.2014.03.008
14. Hall EJ. Intensity-modulated radiation therapy, protons, and the risk of second cancers. Int J Radiat Oncol Biol Phys. 2006;65(1):1–7. doi:10.1016/j.ijrobp.2006.01.027
15. Kang Z, Chen S, Shi L, He Y, Gao X. Predictors of heart and lung dose in left-sided breast cancer treated with VMAT relative to 3D-CRT: a retrospective study.Xue J, editor. PLoS One. 2021;16(6):e0252552. doi:10.1371/journal.pone.0252552
16. Roy S, Salerno KE, Citrin DE. Biology of radiation-induced lung injury. Sem rad oncol. 2021;31(2):155–161. doi:10.1016/j.semradonc.2020.11.006
17. Keffer S, Guy CL, Weiss E. Fatal radiation pneumonitis: literature review and case series. Adv Radiat Oncol. 2020;5(2):238–249. doi:10.1016/j.adro.2019.08.010
18. Darby SC, Ewertz M, McGale P, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N Engl J Med. 2013;368(11):987–998. doi:10.1056/NEJMoa1209825
19. Borger JH, Hooning MJ, Boersma LJ, et al. Cardiotoxic effects of tangential breast irradiation in early breast cancer patients: the role of irradiated heart volume. Int J Radiat Oncol Biol Phys. 2007;69(4):1131–1138. doi:10.1016/j.ijrobp.2007.04.042
20. Karpf D, Sakka M, Metzger M, Grabenbauer GG. Left breast irradiation with tangential intensity modulated radiotherapy (t-IMRT) versus tangential volumetric modulated arc therapy (t-VMAT): trade-offs between secondary cancer induction risk and optimal target coverage. Radiat Oncol. 2019;14(1):156. doi:10.1186/s13014-019-1363-4
21. Virén T, Heikkilä J, Myllyoja K, Koskela K, Lahtinen T, Seppälä J. Tangential volumetric modulated arc therapy technique for left-sided breast cancer radiotherapy. Radiat Oncol. 2015;10(1):79. doi:10.1186/s13014-015-0392-x
22. Shaw E, Scott C, Souhami L, et al. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: final report of RTOG protocol 90-05. Int J Radiat Oncol Biol Phys. 2000;47(2):291–298. doi:10.1016/S0360-3016(99)00507-6
23. Cilla S, Romano C, Macchia G, et al. Automated hybrid volumetric modulated arc therapy (HVMAT) for whole-breast irradiation with simultaneous integrated boost to lumpectomy area: a treatment planning study. Strahlenther Onkol. 2022;198(3):254–267. doi:10.1007/s00066-021-01873-3
24. Venjakob A, Oertel M, Hering DA, Moustakis C, Haverkamp U, Eich HT. Hybrid volumetric modulated arc therapy for hypofractionated radiotherapy of breast cancer: a treatment planning study. Strahlenther Onkol. 2021;197(4):296–307. doi:10.1007/s00066-020-01696-8
25. Lamprecht B, Muscat E, Harding A, et al. Comparison of whole breast dosimetry techniques – from 3DCRT to VMAT and the impact on heart and surrounding tissues. J of Med Radiat Sci. 2022;69(1):98–107. doi:10.1002/jmrs.541
26. Bi S, Zhu R, Dai Z. Dosimetric and radiobiological comparison of simultaneous integrated boost radiotherapy for early stage right side breast cancer between three techniques: IMRT, hybrid IMRT and hybrid VMAT. Radiat Oncol. 2022;17(1):60. doi:10.1186/s13014-022-02009-2
27. Racka I, Majewska K, Winiecki J, Kiluk K. Hybrid planning techniques for early-stage left-sided breast cancer: dose distribution analysis and estimation of projected secondary cancer-relative risk. Acta Oncologica. 2023;62(8):932–941. doi:10.1080/0284186X.2023.2238553
28. Yeh H-L, Lin J-F. The Impact of Deep Inspiration Breath Hold (DIBH) Implementation on the hybrid technique in left-sided whole breast irradiation: a dosimetric characteristic study of 3D-CRT hybrid VMAT in DIBH and free breathing conditions, and VMAT in free breathing conditions. BCTT. 2023;15:683–693. doi:10.2147/BCTT.S426903
29. Li XA, Tai A, Arthur DW, et al. Variability of target and normal structure delineation for breast cancer radiotherapy: an RTOG multi-institutional and multiobserver study. Int J Radiat Oncol Biol Phys. 2009;73(3):944–951. doi:10.1016/j.ijrobp.2008.10.034
30. Offersen BV, Boersma LJ, Kirkove C, et al. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer. Radiother Oncol. 2015;114(1):3–10. doi:10.1016/j.radonc.2014.11.030
31. Ciabattoni A, Gregucci F, De Rose F, et al. AIRO breast cancer group best clinical practice 2022 update. Tumori J. 2022;108(2_suppl):1–144. doi:10.1177/03008916221088885
32. Chen X, Li W, Song S, Qin N, Wu X, Cai H. Dosimetric comparison of hybrid IMRT and different arc techniques VMAT after breast-conserving surgery for left-sided breast cancer. J Applied Clin Med Phys. 2025;26(9):e70257. doi:10.1002/acm2.70257
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.